Back to Journals » Clinical Ophthalmology » Volume 17
YAG Capsulotomy Rates in Patients Following Cataract Surgery and Implantation of New Hydrophobic Preloaded Intraocular Lens in an Australian Cohort: 3-Year Results
Authors Agarwal S ![]() , Thornell E
, Thornell E ![]()
Received 22 September 2023
Accepted for publication 26 October 2023
Published 23 November 2023 Volume 2023:17 Pages 3637—3643
DOI https://doi.org/10.2147/OPTH.S437537
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Smita Agarwal,1,2 Erin Thornell1
1Wollongong Eye Specialists, Wollongong, NSW, Australia; 2Graduate School of Medicine, University of Wollongong, Wollongong, NSW, Australia
Correspondence: Erin Thornell, Wollongong Eye Specialists, Level 2, 2 Victoria St, Wollongong, NSW, Australia, Tel +61 2 4227 6388, Email [email protected]
Purpose: To assess the risk of posterior capsular opacification (PCO) following implantation of the Clareon lens.
Materials and Methods: Retrospective analysis was performed for 484 consecutive eyes that had undergone phacoemulsification and implantation of a monofocal lens (CNA0T) between April 2018 and February 2020. Eyes with other ocular pathology that may affect outcomes, previous refractive surgery or eyes corrected for a near target were excluded. Incidence of PCO and YAG capsulotomy was recorded and regression analysis was performed to determine risk factors associated with PCO formation.
Results: Overall incidence of PCO following implantation of the CNA0T monofocal lens was 3.7% (18 eyes) at 1 year with 1.9% (9 eyes) undergoing YAG capsulotomy. At 3 years, 8.7% (42 eyes) had developed PCO and 4.1% (20 eyes) had undergone YAG capsulotomy cumulatively. Primary open angle glaucoma (POAG; OR = 6.53; 95% CI = 18.68, 2.28; P = 0.0005), age-related macular degeneration (AMD; OR = 2.35; 95% CI = 5.21, 1.06; P = 0.036), vitreomacular traction (VMT; OR = 7.32; 95% CI = 45.08, 1.19; P = 0.032), retinal vein occlusion (RVO; OR = 8.42; 95% CI = 38.99, 1.82; P = 0.006) and history of anti-VEGF therapy (OR = 3.22; 95% CI = 10.26, 1.01; P = 0.048) were positively associated with an increased risk of PCO.
Conclusions: Incidence of PCO requiring YAG capsulotomy was relatively low. However, certain co-morbidities were found to increase the risk of PCO development, most significantly POAG and RVO.
Keywords: capsulotomy, posterior capsule opacification, phacoemulsification
Introduction
Posterior capsular opacification (PCO) is a common complication following cataract surgery that can compromise visual outcomes. It has been proposed that the wound-healing response triggered by surgery causes lens epithelial cells to proliferate and migrate towards the posterior capsule, where they undergo fibre regeneration and epithelial-to-mesenchymal transition.1
With the use of registries that directly access and store electronic medical records, an abundance of data has been made available in recent years regarding prevalence of PCO following cataract surgery. The American Academy of Ophthalmology IRIS® (Intelligence Research in Sight) Registry was established as a centralized repository for patient data. A recent study reported an overall PCO incidence of 28% and YAG capsulotomy incidence of 10.3% at 1 year2 in patients that had undergone cataract surgery. Findings reported from data stored via a Finnish registry reported an overall cumulative YAG capsulotomy incidence of 13.2% at 5 years, although it was noted that incidence varies by lens implanted, varying from 9.6% to 18.1%.3
Patient factors that have been reported to increase the risk of PCO include dry eye disease, glaucoma, previous uveitis, age-related macular degeneration (AMD), hyperlipidemia, peptic ulcers, liver disease, younger age at the time of surgery (<60 years), diabetes, lens nucleus hardness and previous vitrectomy.4,5 In addition to patient factors, lens design and material are highly influential in PCO development. The CNA0T monofocal intraocular lens (IOL) is an asymmetric biconvex lens that features a sharp edge design which may help inhibit the migration of epithelial cells.6 The hydrophobic acrylate/methacrylate copolymer material also features a relatively high water content that may help to enhance visual clarity while minimizing glistening formation, surface haze and roughness.7,8 Specifications of the CNA0T lens are included in Table 1.
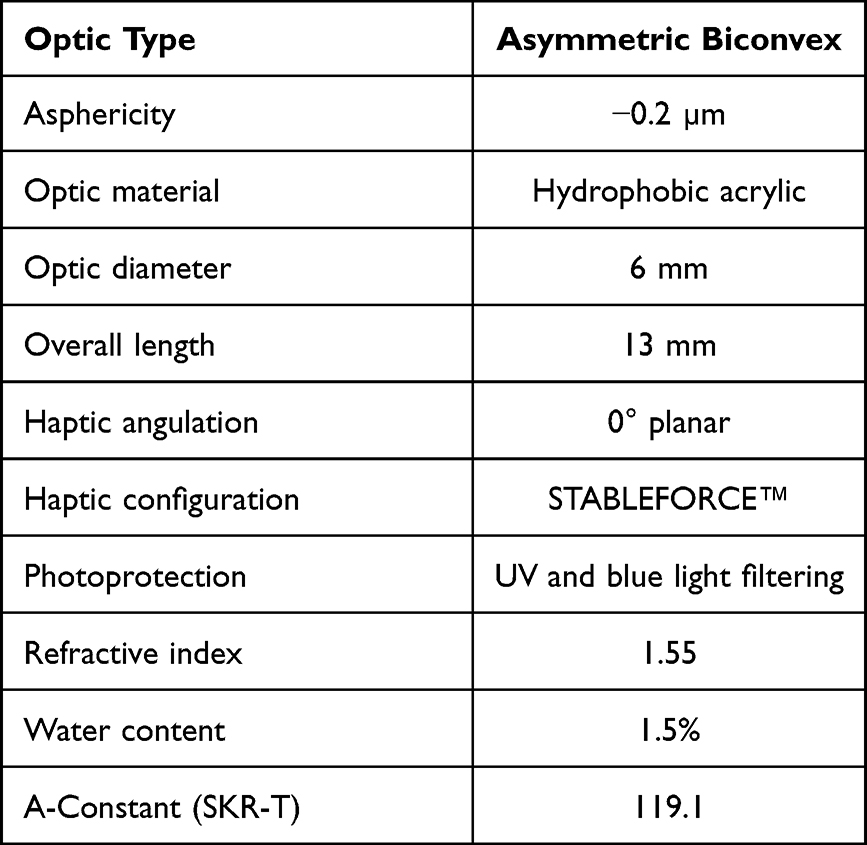 |
Table 1 Lens Specifications of the Clareon IOL |
Due to the recent availability in the American market, long-term data regarding PCO incidence with the CNA0T lens are relatively scarce. This study reports incidence of PCO and YAG capsulotomy over 3 years in eyes that have received the Clareon lens, and identifies risk factors associated with PCO development.
Methods
Retrospective analysis was performed for 484 consecutive eyes that had undergone routine phacoemulsification and IOL implantation for the treatment of cataract. All eyes that received a CNA0T (Clareon; Alcon; Geneva, Switzerland) monofocal IOL between April 2018 and February 2020 were included for analysis. Eyes with incomplete medical records or that were lost to follow up were excluded.
All surgeries were performed by a single surgeon (SA) in private hospitals in the Illawarra region, NSW, Australia. Biometry was performed preoperatively (IOLMaster 700; Zeiss), and lens power was calculated using the Barrett Universal formula with a target of plano±0.25 D spherical equivalent. Briefly, 2×1 mm paracenteses were made at 180° and a 2.3 mm main incision was made temporally. A continuous curvilinear 5.5 mm capsulorrhexis was created using a 26-gauge cystotome, followed by routine phacoemulsification and aspiration of the cortical material. Standard monofocal CNA0T IOLs were inserted through the main incision via the preloaded AutonoMe (Alcon; Geneva, Switzerland) delivery system, and the IOL and anterior capsule were polished to remove all traces of viscoelastic and lens material. Polishing of the capsule was performed using a silicone tip and polish mode on the Centurion machine using the following settings: 20 mmHg vacuum and 10 cc/min aspiration flow. Following the surgery, patients were advised to commence ofloxacin (Allergan; Ocuflox; Dublin, Ireland) and prednisolone acetate/phenylephrine hydrochloride (Allergan; Prednefrin forte; Dublin, Ireland), applying one drop every 2 hours. From the following day, the patients were advised to continue using ofloxacin and prednisolone acetate/phenylephrine hydrochloride eye drops applying one drop qid for 2 weeks and 4 weeks, respectively, and to commence using ketorolac (Allergan; Acular; Dublin, Ireland) eye drops from 1 week after surgery applying one drop qid for a further week.
Postoperative uncorrected distance visual acuity (UDVA), incidence of PCO and/or YAG capsulotomy, and time since surgery until PCO development or YAG capsulotomy were accessed via medical records. Logistic regression analysis was performed to calculate odds ratios for the presence of white mature cataract, complex surgery (defined as small pupil, pseudoexfoliation, previous uveitis, dense nuclear sclerosis etc), diabetes, diabetic retinopathy, posterior vitreous detachment (PVD), shallow anterior chamber, previous refractive surgery, pseudoexfoliation, Fuch’s dystrophy, geographic atrophy, primary open angle glaucoma (POAG), AMD, vitreomacular traction (VMT), retinal vein occlusion (RVO), diabetes, previous vitrectomy, history of intravitreal anti-VEGF therapy or retinopexy, and dry eyes. Correlation between type of cataract (nuclear sclerosis, cortical, posterior subcapsular or mixed) and incidence of PCO was tested using X2 correlation tests. Logistic regression and X2 correlation analysis were performed using an online calculator (available at www.socscistatistics.com) and a statistical threshold of P < 0.05. All other data analysis was performed using Excel Analysis ToolPak (Version 2302; Microsoft; USA).
This study was approved by the University of Wollongong Human Research Ethics Committee (Ethics Number 2022/309) and was conducted according to the Declaration of Helsinki. The requirement of informed consent was waived by the University of Wollongong Human Research Ethics Committee due to the retrospective nature of the study, and impracticality due to the large sample size.
Results
A total of 484 consecutive eyes were included in the analysis (average age 72.5±7.9 years; 54.4% female). Of those, 97.95% had nuclear sclerosis (477 eyes; average grade 2.78±0.77), 37.58% had cortical cataracts (183 eyes; average grade 1.58±0.57) and 8.01% had posterior subcapsular cataracts (39 eyes; average grade 2.5±0.85), with 44.15% (215 eyes) having mixed cataracts based on surgeon analysis upon slit lamp examination. White mature cataracts were found in 1.44% (7 eyes) of eyes. The most common co-morbidities were diabetes (15.9%) and AMD (11.4%) (Table 2).
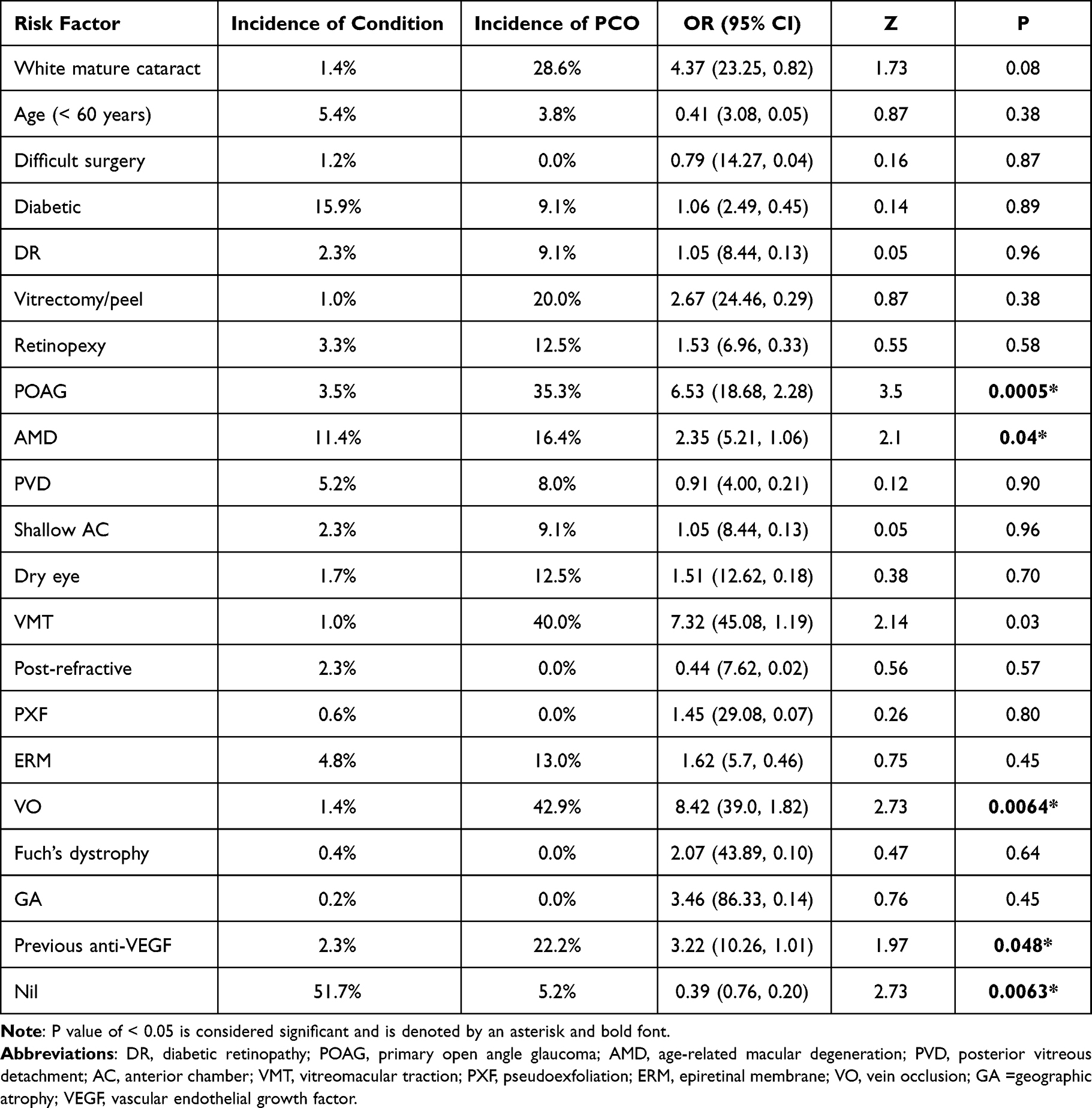 |
Table 2 Correlation Between PCO and Co-Morbidities |
Postoperative UDVA was 0.12±0.18 LogMAR at 6 weeks postoperative. Adverse events were reported for 1.03% of eyes (5 eyes); 1 eye had a small retained nuclear piece in the anterior chamber which was removed within 48 hours as per theatre availability, 3 eyes had 2+ cells in the anterior chamber due to rebound inflammation which resolved following readministration of corticosteroid eye drops (1 drop QID for 1–2 weeks) and 1 eye experienced transient Descemet folds which resolved within a week following administration of steroid eye drops (1 drop QID for 1 week). No patient experienced intraoperative complications.
At 1 year following surgery, 3.7% (18 eyes) of eyes had developed PCO with 1.8% (8 eyes) of eyes undergoing YAG capsulotomy for visually symptomatic PCO (pearl form). Posterior capsular (PC) fibrosis was found in 1.24% (6 eyes) of eyes (defined as opacification occurring within 6 weeks of surgery) with 0.2% of visually symptomatic eyes (1 eye) undergoing YAG capsulotomy for PC fibrosis alone. After 3 years, a cumulative total of 8.7% (42 eyes) of eyes had developed PCO and 3.9% (19 eyes) of eyes had undergone YAG capsulotomy. Average time till PCO diagnosis was 1.8±1.00 years from surgery and average time till first YAG capsulotomy was 1.85±0.87 years from surgery. Cumulative incidence of PCO requiring YAG capsulotomy over 3 years is shown in Figure 1.
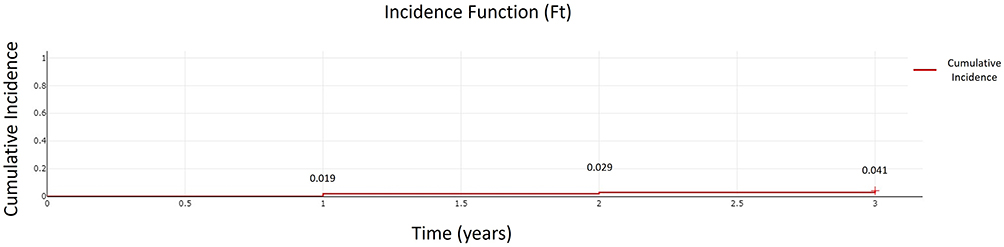 |
Figure 1 Kaplan–Meier incidence plot of PCO requiring YAG capsulotomy over 3 years following surgery. |
Outcomes of the logistic regression analysis are outlined in Table 2. Briefly, POAG (OR = 6.53; 95% CI = 18.68, 2.28; P = 0.0005), AMD (OR = 2.35; 95% CI = 5.21, 1.06; P = 0.036), VMT (OR = 7.32; 95% CI = 45.08, 1.19; P = 0.032), RVO (OR = 8.42; 95% CI = 38.99, 1.82; P = 0.006) and history of anti-VEGF therapy (OR = 3.22; 95% CI = 10.26, 1.01; P = 0.048) were positively associated with an increased risk of PCO. No correlation was found for any other risk factor, including type of cataract (X2 (3, N = 484) = 5.69, P = 0.128).
Discussion
Previously reported incidence of PCO formation following cataract surgery varies widely between studies, ranging from 2.1% to 28% at 1 year.2,9–11 These findings are skewed predominantly by inclusion of different lens types that differ in edge design, optic design and lens material. A large study of 52,162 eyes that had received either AcrySof, non-AcrySof hydrophobic or non-AcrySof hydrophilic lenses reported AcrySof lenses had a lower incidence of both PCO (4.7% versus 6.3% and 14.8% respectively) and YAG capsulotomy (2.4% versus 4.4% and 10.9% respectively) compared to both non-AcrySof hydrophobic and hydrophilic lenses after 3 years.9 Lehmann et al reported an overall PCO rate of 5.4% for CNA0T lenses after 1 year,11 while a meta-analysis of Alcon-sponsored trials reported a much lower rate of YAG capsulotomy for lenses composed of Clareon material (CNA0T) compared to lenses composed of AcrySof (SN60WF) material (1.82% versus 4.19%) after 3 years.10 One large 3-year study that reported outcomes following implantation of the CNA0T lens found zero incidence of glistenings with 92.9% of eyes having no or non-clinically significant PCO (Nuijts 2023 JCRS 49: 672–678). In another long-term study, Oshika et al reported only 5% of eyes implanted with CNA0T lenses needed YAG capsulotomy for PCO after 9 years (Oshika 2020 JCRS 46: 682–687). When compared with Tecnis monofocal eyes, CNA0T eyes had a higher incidence of PCO at 1 month after implantation (Almenara 2021 Eur J Ophthalmol 31: 3355–3366). However, a separate study that assessed outcomes at 1 year following implantation found lower rates of YAG Capsulotomy for AcrySof lenses compared to Tecnis lenses (Horn). This study reports an incidence of PCO of 3.7% within 1 year of surgery and 8.7% within 3 years of surgery, similar to rates reported in previous literature. Of those eyes that developed PCO, 42.8% developed PCO within the first year. These relatively low rates of PCO formation can be attributed to the lens material and design of the lens.
The CNA0T lens is an aspheric monofocal IOL composed of a hydrophobic acrylic material that features a high refractive index and a relatively high water content compared to other lenses. Hydrophobic materials are well known to have a lower incidence of PCO compared to hydrophilic materials due to better adherence to the capsule.12 It has been reported previously that AcrySof lens material binds to the capsule by association with fibronectin.2 The CNA0T lens, with its acrylic material, is likely to bind to the capsule in a similar manner, forming strong associations with fibronectin in the lens capsule, thereby obstructing epithelial cell migration (Linnola et al 1999 JCRS 25:1486–1491). The Clareon material differs to the AcrySof material in that it is composed of a hydrophilic polymer (hydroxyethyl methacrylate) and a hydrophobic co-polymer (phenylethyl acrylate). One study from 1982 that investigated the association of plasma fibronectin to hydrophobic and hydrophilic surfaces reported that fibronectin can bind to both surfaces but forms a higher-affinity conformation when associated with hydrophilic surfaces (Grinnell and Feld 1982 J Biol Chem 257: 4888–4893). While the relevance of this in regards to IOLs in the capsular bag would need to be further investigated, it may be possible that the addition of the hydrophilic polymer increases binding of the CNA0T lens to the lens capsule compared to AcrySof lenses.
Cell migration is also inhibited by the square edge design of the lens, which forms a mechanical barrier to migration.13 Hydrophilic lenses, even those marketed as square-edged, in the hydrated environment have been reported to have a blunter angle than hydrophobic lenses, potentially allowing for greater epithelial cell migration and PCO (Werner JCRS 2009 35: 556–566; Nanavaty JCRS 2008 34: 677–686). Lens specifications regarding edge design are not often made readily available by lens manufacturers due to proprietary interests. However, a previous bench top study has reported that CNA0T has a thinner edge and smaller radius of curvature compared to the AcrySof SN60WF lens14 (Table 3). A radius of curvature less than 10 µm is known to contribute to a lower incidence of PCO. Although both below this limit, the sharper edge of the CNA0T lens compared to the SN60WF may explain the lower incidence of PCO.
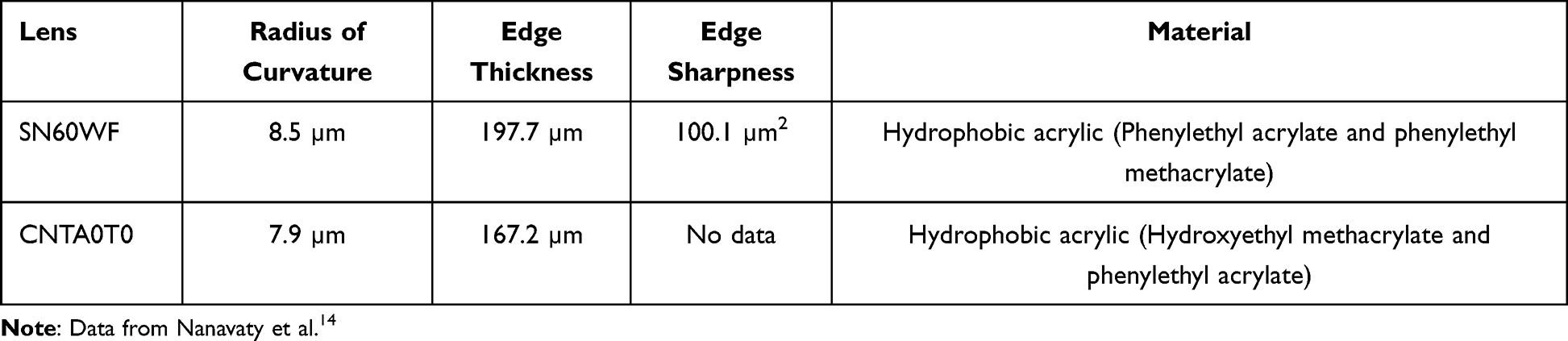 |
Table 3 Edge Parameters of the AcrySof SN60WF and Clareon CNTA0T0 Lenses |
Lens optic design also plays an important role with a large study of 89,947 eyes that received either AcrySof or Tecnis multifocal or monofocal lenses reporting a much lower incidence of YAG capsulotomy (4.1% versus 21.2% within 1 year), and a longer time to first PCO diagnosis (196.4 versus 175.3 days) for the monofocal lenses.2 In addition to lens choice, surgery type can also impact incidence of PCO, with phacoemulsification generally having a lower incidence than extracapsular extraction, with one study reporting a PCO rate of 9.1% following phacoemulsification at 6 months compared to 21.7% for extracapsular extraction (OR 0.2).15,16 Polishing of the anterior capsule following phacoemulsification and thorough aspiration of the cortical material may also help reduce risk of PCO formation, although it has been reported that the outcome may not be visually significant.17 The use of a large capsulorrhexis (ie, over 6 mm or where the capsulorrhexis does not overlap the optic) has been implicated in the early onset of PCO, with the authors suggesting primary posterior continuous curvilinear capsulorrhexis may be more beneficial in preventing PCO formation.18 However, performing a posterior continuous curvilinear capsulorrhexis may present difficulties including technical challenges and disturbance to the hyaloid interface. For this study, the surgeon aimed for a capsulorrhexis that overlapped with the lens optic completely.
Various patient factors have also been associated with an elevated risk of PCO. In the current study, only ocular diseases (ie, POAG, AMD, VMT and RVO) and history of anti-VEGF therapy for either AMD or RVO were associated with an elevated risk. POAG and AMD have previously been identified as risk factors,5 although a relationship with RVO and VMT is less well documented. Due to the ambiguity surrounding the etiology of PCO, it remains unclear why compromised retinal health is a risk factor for PCO. However, there is speculation that inflammatory activation pathways may be involved.19 Inflammatory marker interleukin-6 (IL-6) has been implicated in the progression of geographic atrophy20 and also PCO development via activation of transforming growth factor β2 and extracellular matrix synthesis.21 This may also be the case in patients with history of anti-VEGF therapy with a recent case study reporting cases of PCO development in pseudophakic eyes following intravitreal injection of bevacizumab.22 However, distinguishing the effect of the injections from that of the underlying retinal disease is difficult without further analysis. Interestingly, neither diabetes nor diabetic retinal disease was associated with an elevated risk of PCO. Patients were categorised as either having diabetes or not having diabetes; HbA1C were not recorded. Diabetes may not have been identified as a risk factor if the majority of cases were well controlled with no sign of retinal changes. Patients undergoing lens replacement at a younger age (<60 years) have been reported to be more likely to develop PCO due to the higher density of lens epithelial cells at the anterior capsule.4 The current findings do not support this, although this may have been skewed by low representation within the study group of people of a younger age group; only 5.4% of patients were aged below 60 years. Similarly, in our study, previous vitrectomy or retinopexy were not associated with an elevated risk of PCO. This again contradicts literature18 and may be due to low representation of post-vitrectomy eyes in the study.
Certain limitations exist for this study. Risk factors were analysed individually and did not account for confounding of multiple co-morbidities. As eyes were recorded consecutively, some contralateral eyes were included in the study, potentially contributing to confounding of analysis. Additionally, other systemic risk factors such as hypertension and medication use were not assessed. Due to the retrospective nature of the study, available data is restricted to patients who presented with PCO within the follow-up time and therefore the exclusion of patients who did not attend appointments may have led to the potential underestimation of overall PCO rates. An assumption was made that patients who did not attend appointments had maintained their visual acuity. Future long-term studies that incorporate comparison groups with other lens types would be beneficial.
The CNA0T lens has an overall low rate of PCO and PCO requiring YAG capsulotomy, conceivably due to its optic and edge design, and its material. Certain retinal conditions and the administration of anti-VEGF therapies may increase the risk of PCO development, and this should be discussed with patients preoperatively as part of case management. Careful lens selection and procedural protocols can help mitigate the risk of PCO thereby reducing the need for further follow up and treatment.
Disclosure
Neither author has any financial or proprietary interests to disclose. No financial or material support was received for this study. Neither author has any competing interests to disclose.
References
1. Awasthi N, Guo S, Wagner BJ, Guo S, Wagner BJ, Wagner BJ. Posterior capsular opacification. Arch Ophthalmol. 2009;127(4):555–562. doi:10.1001/archophthalmol.2009.3
2. Horn JD, Fisher BL, Terveen D, Fevrier H, Merchea M, Gu X. Academy IRIS registry analysis of incidence of laser capsulotomy due to posterior capsule opacification after intraocular lens implantation. Clin Ophthalmol. 2022;16:1721–1730. doi:10.2147/OPTH.S358059
3. Lindholm J, Laine I, Tuuminem R. Five-year cumulative incidence and risk factors of Nd:YAG capsulotomy in 10044 hydrophobic acrylic 1-piece and 3-piece IOLs. Am J Ophthalmol. 2019;200:218–223. doi:10.1016/j.ajo.2019.01.010
4. Wu S, Tong N, Pan L, et al. Retrospective analyses of potential risk factors for posterior capsule opacification after cataract surgery. J Ophthalmol. 2018;2018:1–7. doi:10.1155/2018/9089285
5. Chen H, Lee C, Sun C, Huang J, Lin H, Yang S. Risk factors for the occurrence of visual-threatening posterior capsule opacification. J transl Med. 2019;17(1):17. doi:10.1186/s12967-018-1755-5
6. Mencucci R, Favuzza E, Boccalini C, Gicquel J, Raimondi L. Square-edge intraocular lenses and epithelial lens cell proliferation: implications on posterior capsule opacification in an in vitro model. BMC Ophthalmol. 2015;15(1):5. doi:10.1186/1471-2415-15-5
7. Maxwell A, Suryakumar R. Long-term effectiveness and safety of a three-piece acrylic hydrophobic intraocular lens modified with hydroxy-methacrylate: an open-label, 3-year follow-up study. Clin Ophthalmol. 2018;12:2031–2037. doi:10.2147/OPTH.S175060
8. Werner L, Thattamla I, Ong M, et al. Evaluation of clarity characteristics in a new hydrophobic acrylic IOL in comparison to commercially available IOLs. J Cataract Refract Surg. 2019;45(10):1490–1497. doi:10.1016/j.jcrs.2019.05.017
9. Ursell PG, Dhariwal M, Majirska K, et al. Three-year incidence of Nd:YAG capsulotomy and posterior capsule opacification and its relationship to monofocal acrylic IOL biomaterial: a UK real world evidence study. Eye. 2018;32(10):1579–1589. doi:10.1038/s41433-018-0131-2
10. Von Tress M, Marotta JS, Lane SS, Sarangapani R. A meta-analysis of Nd:YAG capsulotomy rates for two hydrophobic intraocular lens materials. Clin Ophthalmol. 2018;12:1125–1136. doi:10.2147/OPTH.S161380
11. Lehmann R, Maxwell A, Lubeck DM, Fong R, Walters TR, Fakadej A. Effectiveness and safety of the Clareon monofocal intraocular lens: outcomes of a 12-month single-arm clinical study in a large sample. Clin Ophthalmol. 2021;15:1647–1657. doi:10.2147/OPTH.S295008
12. Wu Q, Li Y, Wu L, Wang C. Hydrophobic versus hydrophilic acrylic intraocular lens on posterior capsule opacification: a meta-analysis. Int J Ophthalmol. 2022;15(6):997–1004. doi:10.18240/ijo.2022.06.19
13. Findl O, Buehl W, Bauer P, Sycha T. Interventions for preventing posterior capsule opacification. Cochrane Database Syst Rev. 2010;17:CD003738.
14. Nanavaty MA, Zukaite I, Salvage J. Edge profile of commercially available square-edged intraocular lenses: part 2. J Cataract Refract Surg. 2019;45(6):847–853. doi:10.1016/j.jcrs.2018.12.004
15. Moulick PS, Rodrigues FEA, Shyamsundar K. Evaluation of posterior capsular opacification following phacoemulsification, extracapsular and small incision cataract surgery. MJAFI. 2009;65:225–228.
16. Li A, He Q, Wei L, et al. Comparison of visual acuity between phacoemulsification and extracapsular cataract extraction: a systematic review and meta-analysis. Ann Palliat Med. 2022;11(2):551–559. doi:10.21037/apm-21-3633
17. Sachdev GS, Soundarya B, Ramamurthy S, Laksmi C, Dandapani R. Impact of anterior capsule polishing on capsule opacification rates in eyes undergoing femtosecond laser-assisted cataract surgery. Indian J Ophthalmol. 2020;68(5):780–785. doi:10.4103/ijo.IJO_1787_19
18. Gu X, Chen X, Jin G, et al. Early-onset posterior capsule opacification: incidence, severity, and risk factors. Ophthalmol Ther. 2022;11(1):113–123. doi:10.1007/s40123-021-00408-4
19. Boyer DS, Schmidt-Erfurth U, Van Lookeren Campagne M, Henry EC, Brittain C. The pathophysiology of geographic atrophy secondary to age-related macular degeneration and the complement pathway as a therapeutic target. Retina. 2017;37(5):819–835. doi:10.1097/IAE.0000000000001392
20. Nielsen MK, Subhi Y, Molbech CR, Falk MK, Nissen MH, Sorensen TL. Systemic levels of interleukin-6 correlate with progression rate of geographic atrophy secondary to age-related macular degeneration. Invest Ophthalmol Vis Sci. 2019;60:202–208.
21. Ma B, Yang L, Jing R, et al. Effects of interleukin-6 on posterior capsular opacification. Exp Eye Res. 2018;172:94–103. doi:10.1016/j.exer.2018.03.013
22. Wahab C, Ayash J, Sayegh K, Sammouh F, Warrak EL. Hydrophilic lens opacification after intravitreal anti-VEGF injections: a case series. Case Rep Ophthalmol. 2022;13(1):134–140. doi:10.1159/000520356
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.