Back to Journals » Patient Preference and Adherence » Volume 15
Exit-Knowledge About Dispensed Medications and Associated Factors Among Patients Attending the Outpatient Pharmacy of Ambo General Hospital, Western Ethiopia
Authors Eticha EM ![]() , Gemechu WD
, Gemechu WD
Received 14 October 2020
Accepted for publication 22 December 2020
Published 6 January 2021 Volume 2021:15 Pages 1—8
DOI https://doi.org/10.2147/PPA.S286700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Johnny Chen
Endalkachew Mekonnen Eticha,1 Workineh Diriba Gemechu2
1Department of Pharmacy, Ambo University, Ambo, Oromia, Ethiopia; 2School of Medicine, Jigjiga University, Jigjiga, Somali, Ethiopia
Correspondence: Endalkachew Mekonnen Eticha
Department of Pharmacy, Ambo University, Ambo, Oromia, Ethiopia
Tel +251967344420
Email [email protected]
Background: Insufficient knowledge of patients about their dispensed medications may result in inappropriate use of medication which can lead to treatment failure and poor therapeutic outcome.
Purpose: This study aimed to determine the exit-knowledge level and its determinants among patients attending outpatient pharmacy of the Ambo General Hospital.
Patients and Methods: Hospital-based cross-sectional study was conducted on 400 study participants who visited the outpatient pharmacy in Ambo General Hospital from October to December 2019. Face-to-face interview was conducted using structured questionnaires to assess the exit-knowledge of the patients about their dispensed medication at the pharmacy exit. A binary logistic regression was employed to determine factors associated with the exit-knowledge. The association was statistically significant at 95% of confidence interval with a p-value less than 0.05.
Results: A total of 400 patients participated in the study with a 100% response rate. Of the total, 222 (55.5%) patients had sufficient exit-knowledge about their dispensed medication. Patients in the age group of 19– 29 (AOR=3.1; 95% CI (1.7– 5.6) and 49 − 59 (AOR = 3.7; 95% CI (2.3– 6.0)) had greater exit-knowledge than the elderly participants (> 60 years). Participants who reported the comfort of the waiting area was not suitable had lower odds of sufficient exit-knowledge (AOR= 0.7; 95% CI (0.2– 3.0)) in comparison to those who reported a suitable waiting area. Lower odds of sufficient exit-knowledge (AOR=0.4; 95% CI (0.3– 0.7)) was determined among those who responded fairly clarity of the dispensers guidance in comparison with those reported clear guidance. The gender and the residence of the participants were also had a significant association with the exit-knowledge level.
Conclusion: Modest number of the patients had sufficient exit-knowledge of their dispensed medication. Age, gender, residence, perceived comfort of the waiting area and perceived clarity of the pharmacists’ guidances were significantly associated with the exit-knowledge.
Keywords: exit-knowledge, outpatient pharmacy, patients
Introduction
Appropriate use of medicines is essential for treatment to be effective in ensuring better health care for patients and the community as a whole.1 The World Health Organization (WHO) defines the rational use of medicines as ensuring that a patient receives medications appropriate to their clinical needs, in the right doses, for an adequate duration of therapy, and at the right cost to the patient and their community.2–4 To overcome the challenges in delivering appropriate medication, a good dispensing practice that includes strong pharmacists-patient interaction is required.5–8
A strong pharmacist–patient relationship is essential to ensure the safe use of drug and prevent the occurrence of drug therapy problems.9–12 The pharmacist should provide sufficient to patients about the name of the medication and counsel them about, the frequency and duration of therapy, the route of administration, and the potential toxicities the medication dispensed.7 Several factors affect the dispensing practice of pharmacists, such as the language barrier, the pharmacists’ commitments, knowledge and experience and the dispensing room environment.13–16
Patients’ knowledge about the prescribed medications is the essential pre-requisites for the optimal use of medicines.17 Insufficient knowledge about the dispensed medications may result in inappropriate use of medication in the patients, which can lead to treatment failure and poor therapeutic outcome.18 Most of the studies on patients’ knowledge of the dispensed medications are from developed countries19 and some are from developing countries.13,14,20 Despite, some studies were conducted in the Ethiopia, there is discrepancies of the results. Therefore, this study aimed to identify factors affecting patients’ exit-knowledge about their dispensed medications at the outpatient pharmacy of Ambo General Hospital (AGH).
Patients and Methods
The Study Design, Setting and Participants
A hospital-based cross-sectional study was conducted from October to December 2019 in AGH which is located 126 km west of Addis Ababa, the capital city of Ethiopia. The hospital is one of the governmental hospitals in western Ethiopia. The hospital has more than 183 healthcare professionals and 240 administrative and supportive staff. It provides services for approximately greater than 20,000 populations annually with a total of 150 beds.
All patients aged ≥15 years and received at least one drug from the outpatient pharmacy were included in the study. Patients refused to provide oral consent, unconscious and severely ill patients who received greater than three medications were excluded from the study. The latter two were excluded, since information recall and retention abilities of such individuals were thought to be affected by the disease condition and the number of medications dispensed to them, respectively.
Sample Size Determination and Sampling Technique
The sample size was calculated using the single population proportion formula (N = Z (α/2)2 (pq)/d2). Where n=required sample size; p=0.386 from the study conducted in Hiwotfana specialized University Hospital; Z=standard value of Z distribution at 95% confidence interval (CI) and d=0.05 margin of error. Accordingly, 364 sample size was calculated. Finally, a sample size of 400 participants was estimated adding 10% (n=36) of contingency for non-response. Participants eligible for the study were consecutively added until the required sample size was achieved.
Data Collection Tools and Method
A data collection tool for the patient interview was developed from previously conducted studies.6,16,21–23 Questionnaires were translated to local language Afan Oromo and Amharic in collaboration with Afan Oromo and Amharic Departments of Ambo University, respectively. The newly translated and refined items were administered to small samples (10 participants) as with a typical set of participants. Two trained clinical pharmacists working in Ambo General Hospital were involved in data collection. The pre-test was done on 10%20 of the study population to guarantee the quality of data collection, in which they were excluded from the study.
The tool consisted of parameters to measure socio-demographic characteristics of the patients, perception of patients for the pharmacists’ service and the exit-knowledge. Patients’ exit-knowledge indicates patients recall ability about the pharmacists counselling and guidance on their dispensed medication at the exit of outpatient pharmacy.
Patients’ exit-knowledge was referred to as a key outcome variable. To determine the exit-knowledge level, 13 questionnaires were developed. The patient was assumed to be with sufficient knowledge about the dispensed medication when he/she addressed two-thirds (≥8 out of 13) of the knowledge questionnaires. The data were collected by two trained clinical pharmacists working out of the study setting and supervised daily by the principal investigator.
Data Analysis and Interpretation
All extracted data were cleaned, coded and entered to the Statistical Package for the Social Science (SPSS) software version 20 for analysis. Categorical data were expressed in numbers and percentages. Potential variables with p-value <0.2 by univariate analysis were retained for subsequent consideration for binary logistic regression analysis. Finally, variables with p-value <0.05 were considered to have a significant association with the outcome variable.
Results
Patients Socio-Demographic Characteristics
Of the 400 participants, more than half were males, 220 (54%) and urban residents, 213 (53.3%). As shown in Table 1, most of the participants were in the age category of 45–59, 122 (30.2%). In the case of their educational background, the majority 166 (41.5%) completed tertiary school. Half of the participants, 212 (53%) visited the outpatient pharmacy only once.
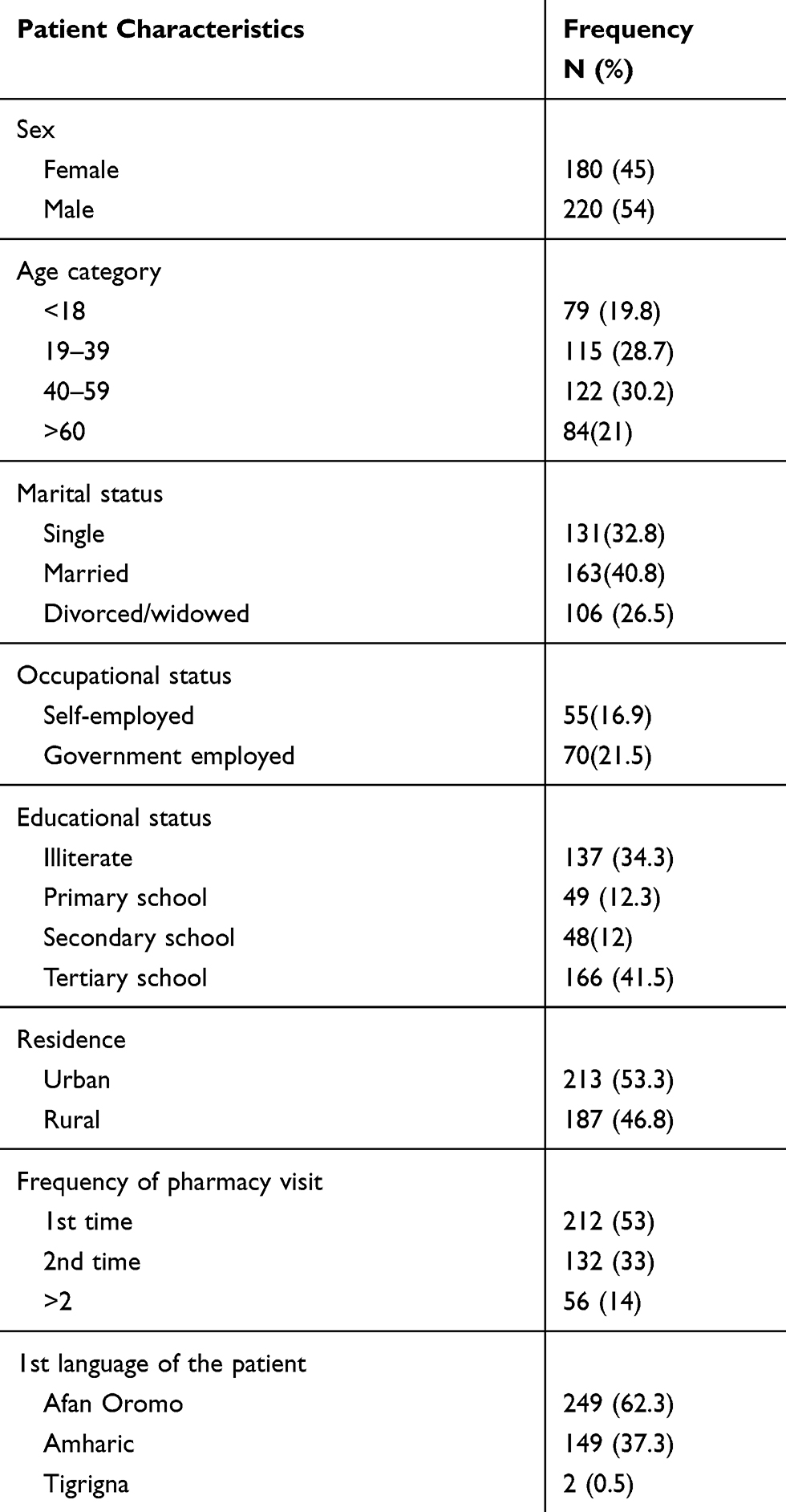 |
Table 1 Socio-Demographics Characteristics of the Patients Attending Outpatient Pharmacy of the AGH from October to December, 2019 |
Perception of the Patients on Pharmacists Service
Almost 4 out of 5 patients (83.8%) had good interaction with the pharmacist in the dispensing room. A high proportion of the participants, 375 (93.8%) reported that the ascent and the tone of the pharmacy personnel were clear and loud enough to be heard as indicated in Table 2. Regarding the clarity of the dispensers’ guidance and sufficiency of drug information service, 332 (83%) and 176 (44%) of the participants reported that they received clear guidance and enough drug information about their dispensed medication, respectively. Only 205 (51.2%) patients were comfortable with the dispensing room waiting area.
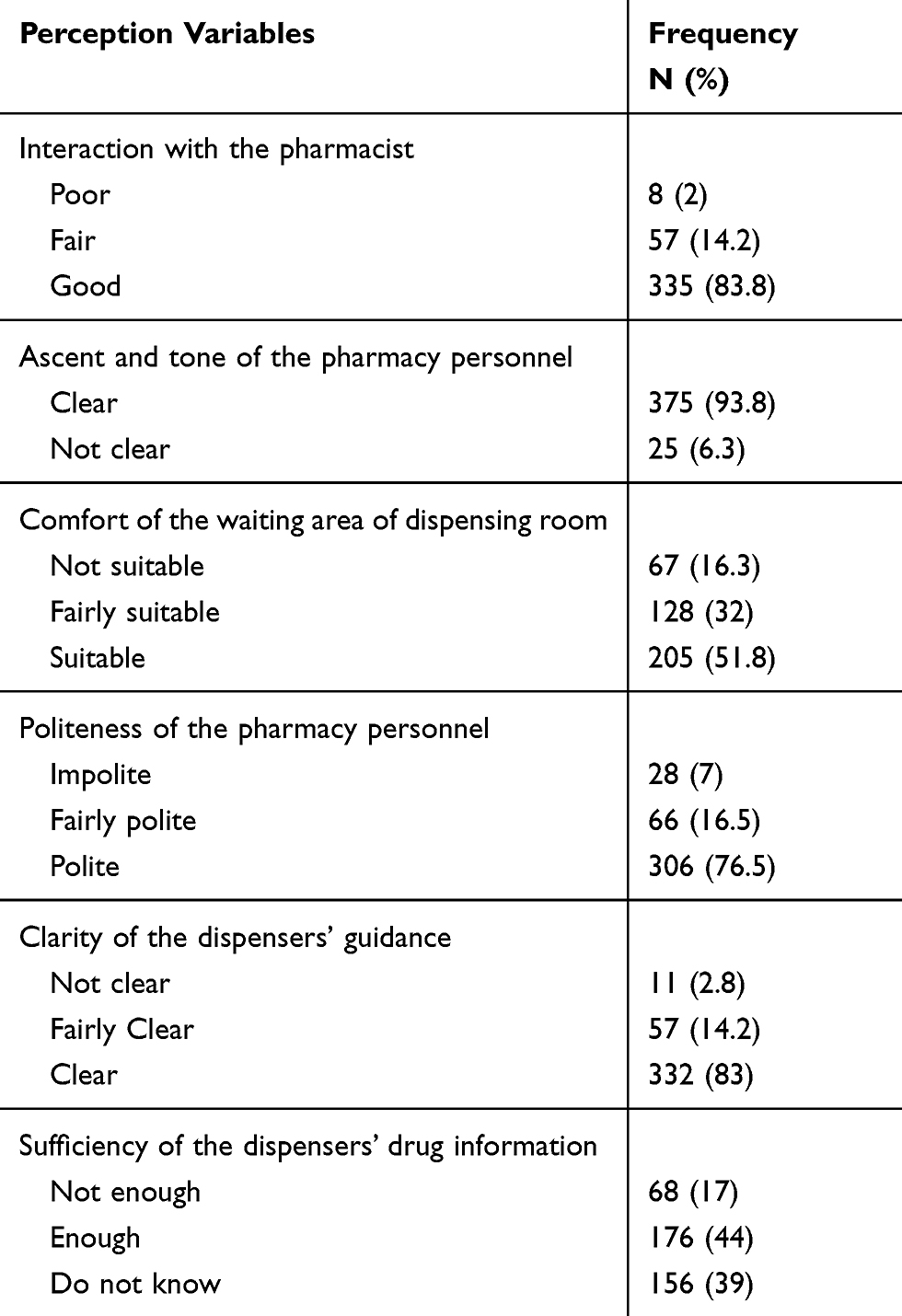 |
Table 2 Perception of the Patients on Outpatient Pharmacy Service at AGH from October to December 2019 |
Exit-Knowledge of the Patients
In this study, most of the participants recalled the name of the medication (304, 76%), drug indication (241, 60.3%), route of administration (396, 99%), the medication frequency (283, 70.8%), appropriate handling of the medication (374, 93.5%), how to use the medication (331, 82.8%), action taken for the forgotten dosage (325, 81.3%) and expected therapeutic outcome (216, 54%) as shown in Table 3. In contrast, the exit-knowledge of the participants was poor regarding the duration of therapy (178, 44.5%), the drug interaction (46, 11.5%), and potential toxicities (32, 8%) of the dispensed medication. In general, 222 (55.5%) of the patients had sufficient exit-knowledge about their dispensed medication at outpatient pharmacy exit.
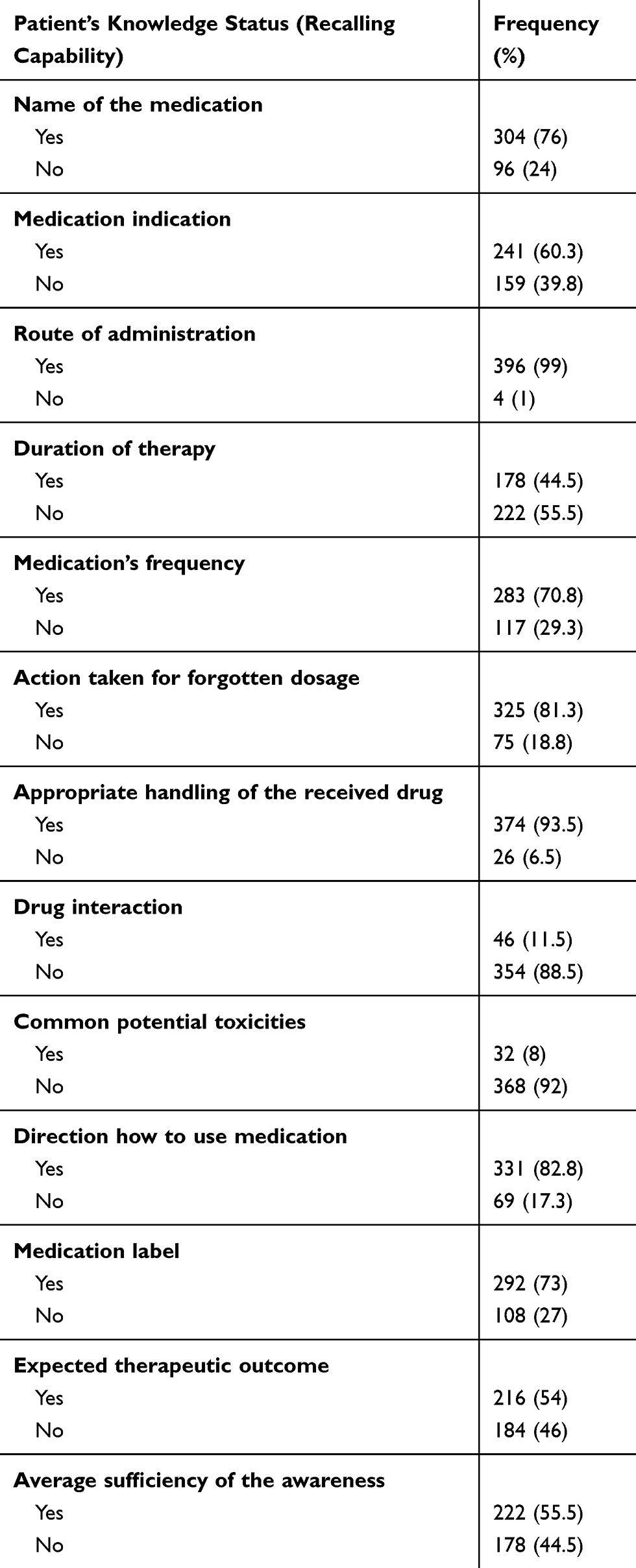 |
Table 3 Exit-Knowledge of the Patients at Outpatient Pharmacy of AGH About Their Dispensed Medication from October to December 2019 |
Factors Affecting Exit-Knowledge of the Patients
As shown in Table 4, the binary logistic regression analysis shown that several variables were found to have a significant association with the patients’ exit-knowledge. Among the socio-demographic characteristics of the participants’, age, sex, the residence of the participants significantly affects their recall potential about their dispensed medication. Patients in the age group of 19–29 (AOR=3.1; 95% CI (1.7–5.6) and 49–59 (AOR = 3.7; 95% CI (2.3–6.0) were 3.1 and 3.7 times greater exit-knowledge than the elderly patients (>60 years). Participants who were residing in the urban area were 3.7 times more likely to have sufficient knowledge of dispensed medication than those from the rural. Female patients were also less odds (AOR= 0.7; 95% CI (0.5–0.9)) of sufficient exit-knowledge than males.
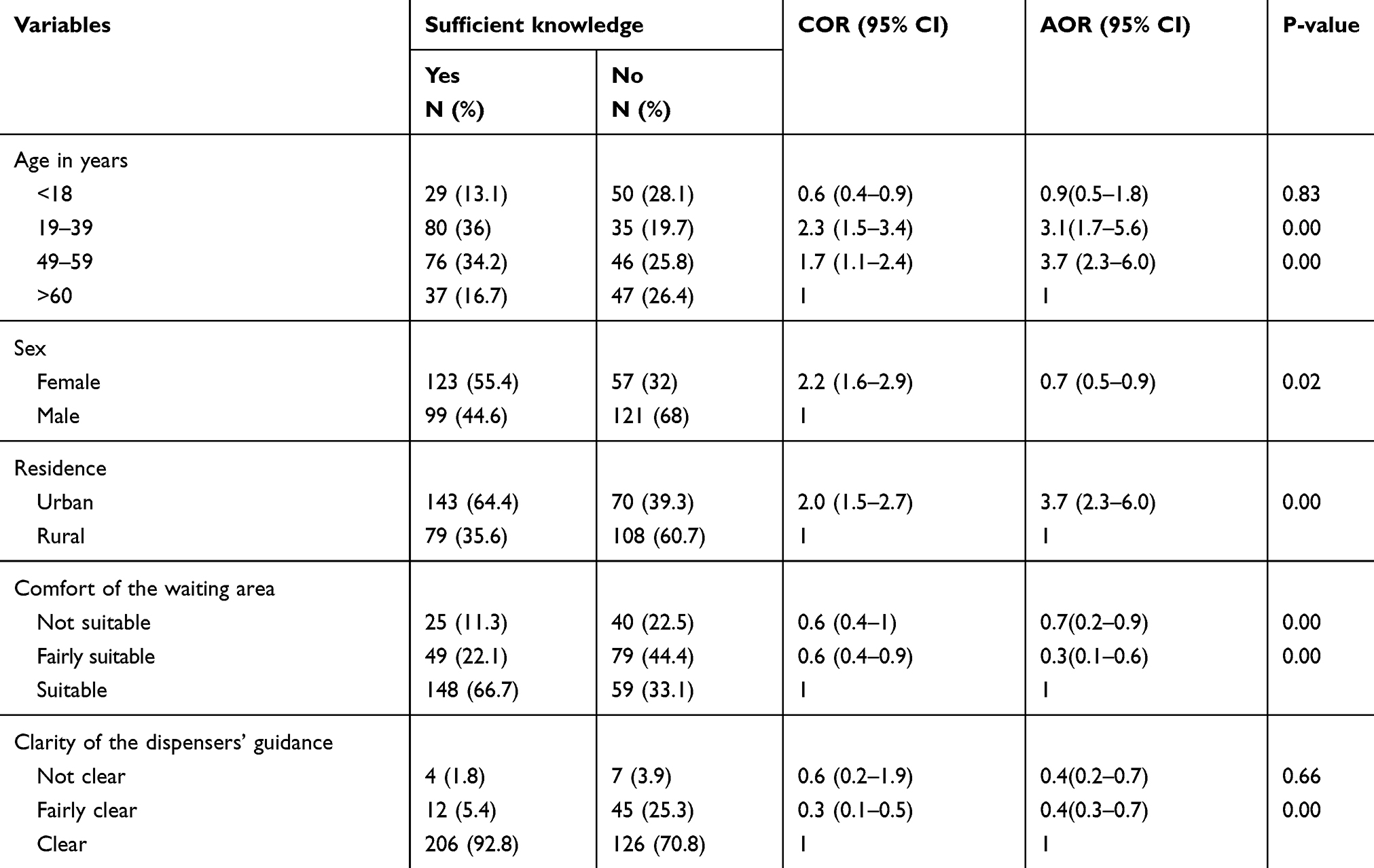 |
Table 4 Factors Affecting the Exit-Knowledge of the Patients at the Outpatient Pharmacy of AGH from October to December 2019 |
The comfort of the waiting area of the pharmacy dispensing room affected the exit-knowledge of the participants. Participants who reported the comfort of the waiting area was not suitable had lower odds of sufficient exit-knowledge (AOR= 0.7; 95% CI (0.2–3.0)) in comparison to those who reported as a suitable waiting area. A significantly reduced odds of sufficient exit-knowledge (AOR=0.4; 95% CI (0.3–0.7)) was determined among those who responded fairly clarity of the dispensers guidance in comparison with those reported clear guidance.
Discussion
Our cross-sectional study explores factors affecting patients’ exit-knowledge about their dispensed medication in the outpatient pharmacy of AGH. The exit-knowledge of the patients was affected by different factors includes socio-demographic characteristics and perception of the patients and healthcare-related factors.
Providing drug information to the patients about their medical conditions and drug therapy is one of the determinant components of the rational use of the drug. For this reason, patients should be informed and educated about their drug therapy. Communication barrier and inadequate interaction between patients and pharmacists on dispensed medications can lead to poor adherence and treatment failure.18,24 In this study, most of the patients perceived that their interaction with the pharmacists (83.3%), the ascent and tone (93.8%), the politeness (76.5%) and guidance (83%) of the pharmacist were sufficient enough to recall how to administer and use their medication. The result was comparable with the other studies done in Ethiopia.6,14,16
The finding of this study indicated that most of the patients (92%) did not know the potential side effects of their prescribed medication. Knowledge about the possible side effects of medicine is important for patients to recognize side effects early, and promptly report these to physicians. A study indicated that patients received appropriate medicines-related information, including side effects had adequate adherence to their drug therapy.25,26 The study from Canada25 indicated that experiencing side effects often results in discontinuation of therapy. A similar study in Ethiopia, from Mekelle (31.2%)16 and Harar (33.6%)14 indicated that less proportion of the patients know the potential side effects of their drug therapy. This might be related to the poor educational status of the patients, the high workload of the pharmacist and discomfort of dispensing room waiting area.27 Besides, the less frequent (<1) visit to the pharmacy (53%) by our study participant might be the other plausible reason. A study conducted in Saudi Arabia28 indicated that patients with a previous history of pharmacy visit had excellent knowledge about their dispensed medication.
The current study indicated that only 55.5% of the participants had a sufficient exit-knowledge about their dispensed medication. This finding is less than the study conducted in the Ayder Comprehensive Specialized Hospital, Mekelle (81%). But, it is greater than studies done in Gondar (38.3),29 eastern Ethiopia (38.6%)30 and Hiwotfana specialized University Hospital, Harar (46%).16 The discrepancy of the findings among the studies might be due to differences in the calculation of knowledge score, language barrier, counselling history, frequency of pharmacy visit and educational status of the patients. Our finding indicated that those participants not comfortable with the waiting area of the dispensing room had a high risk of insufficient exit-knowledge about their dispensed medication. Similarly, studies reported that the language barrier between pharmacist and participants were a cause of poor exit-knowledge.14,16
The binary logistic regression analysis indicated that age, sex, residence, the comfort of the waiting area and clarity of the dispensers’ guidance affected the exit-knowledge of the dispensed medication. Urban patients had 3.7 times more likely to have sufficient knowledge of dispensed medication than those from the rural. Similarly, a study form southwest of Ethiopia indicated greater exit-knowledge among urban patients than rural patients.31
The comfort of the waiting area was one of the factors affecting the exit-knowledge of the participants. Participants not suitable and fairly suitable to the dispensing room waiting area had less likely to have sufficient exit-knowledge than those comfortable in the room. WHO recommendation indicated that a good working environment promotes safe working and reduces stress levels for other staff and patients.32
Clarity of dispensers guidance also determines the recall ability of the participants about their prescribed medications. Patients who were not clear and fairly clear with the pharmacist guidance had lower exit-knowledge level than the comparators. The current study revealed that patients who responded fairly clarity of the pharmacist’s instruction how to take the medications had 60% less likely to have sufficient exit-knowledge than who got clear instruction. A study by Desta et al indicated that patients having clear instruction from pharmacist had 3.6 times greater exit-knowledge than those responded not clear. The finding of this study showed that patients in the age category of 19–39 and 40–59 years had 3.1 and 3.7 times more likely to have sufficient exit-knowledge than elderly patients, respectively. This could be explained by the fact that ageing is associated with a decline in the efficiency of cognitive processes.33
We acknowledge several limitations of the study. First, the study was a single centred study and the finding cannot be generalized to an entire country or abroad. Second, the use of self-reporting and face-to-face interview can potentially lead to recall bias by the respondents, which should be taken into consideration while interpreting the result. Besides, the exit-knowledge of the patients might be affected by the recall ability of the patients since the questions were subjective. Lastly, not to the least, exclusion of patients with poly-pharmacy may undermine the impact of poly-pharmacy on patients’ knowledge.
Conclusion
The current study indicated that the participants had modest exit-knowledge level about their dispensed medications. The exit-knowledge of the patients was significantly affected by the age, the gender, the residence, the perceived clarity of the dispensers’ guidance, and the perceived comfort of the waiting area. We recommend the pharmacists and the hospital managers to provide clear and enough instruction to the patients how to take their medications and to create conducive and sufficient dispensing room.
Abbreviations
WHO, World Health Organization; AOR, adjusted odds ratio; COR, crude odds ratios; CI, confidence interval; AGH, Ambo General Hospital.
Data Sharing Statement
All data used to support the result of this research are available and researchers who need further clarification can obtain the data on reasonable request.
Ethical Approval and Consent to Participate
The study was conducted by following per under the declaration of Helsinki. Ethical approval was obtained from the Ethical Review Committee of the College of Medicine and Health Science, Ambo University with the reference number of SP\0746\19. Permission to conduct the study was also obtained from the AGH Medical Directorate. Verbal informed consent was approved by ethical review committees. Accordingly, oral informed consent was obtained from the adult patients and legal guardian oral consent was also obtained for patients under the age of 18 years before the data collection. The confidentiality of the study participants was maintained by assigning unique identifiers during data collection and analysis.
Consent to Publish
Not applicable.
Acknowledgment
We acknowledge the AGH staffs and managers for providing access to the data. We were also grateful for the data collectors and supervisors for carefully undertaking their tasks.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
No funding was obtained.
Disclosure
All authors declare they have no conflicts of interest for this work.
References
1. World Health Organization (WHO). Action Programme for Essential Drugs and Vaccines (1993). How to investigate drug use in health facilities: selected drug use indicators. World Health Organization. Available from: https://apps.who.int/iris/handle/10665/60519.
2. Butler MB. Rational use of drugs. Br Med J. 1958;2:1536. doi:10.1136/bmj.2.5111.1536-e
3. WHO. Rational use of drugs. Lancet. 1985.
4. World Health Organization. Promoting the rational use of medicines: core components. WHO Policy Perspect Med. 2002.
5. Gokcekus L, Toklu HZ, Demirdamar R, Gumusel B. Dispensing practice in the community pharmacies in the Turkish Republic of northern cyprus. Int J Clin Pharm. 2012;34:312–324. doi:10.1007/s11096-011-9605-z
6. Gudeta T, Mechal D. Patient knowledge of correct dosage regimen; the need for good dispensing practice. J Prim Care Community Heal. 2019;10:215013271987652. doi:10.1177/2150132719876522
7. Embrey M. Ensuring good dispensing practices. Managing Access Med Health Technology. 2012.
8. Siden R, Tamer HR, Skyles AJ, Weadock S, Redic K. Pharmacist-prepared dispensing guidelines for drugs used in clinical research. Am J Health-System Pharmacy. 2012;69:1021–1026. doi:10.2146/ajhp110082
9. World Health Organization (WHO). Medication without harm - global patient safety challenge on medication safety. World Heal Organ. 2017.
10. Al Aqeel S, Abanmy N, AlShaya H, Almeshari A. Interventions for improving pharmacist-led patient counselling in the community setting: A systematic review. Syst Rev. 2018;7. doi:10.1186/s13643-018-0727-4
11. Salameh LK, Farha RA, Hammour KA, Basheti I.Impact of pharmacists directed medication reconciliation on reducing medication discrepancies in a surgery ward. Case Med Res. 2019. Available from: https://clinicaltrials.gov/ct2/show/NCT03928106.
12. Karapinar-Çarkit F, Borgsteede SD, Zoer J, Smit HJ, Egberts ACG. Effect of medication reconciliation with and without patient counseling on the number of pharmaceutical interventions among patients discharged from the hospital. Ann Pharmacother. 2009;43:1001–1010. doi:10.1345/aph.1L597
13. Ameh D, Wallymahmmed A, Mackenzie G. Patient knowledge of their dispensed drugs in rural gambia. Int J Sci Basic Appl Res Int J Sci Basic Appl Res. 2014;15:1–15.
14. Hirko N, Edessa D, Sisay M. Exit-knowledge of ambulatory patients about medications dispensed in a government hospital in Eastern Ethiopia: the need for focused patient counselling. Front Public Heal. 2018;6. doi:10.3389/fpubh.2018.00254
15. Anteneh ZA, Demilew W, Gebeyehu E. Dispensing practices in health care facilities of the Bahir Dar City, Northwest Ethiopia. Infect Dis Clin Pract. 2016;24:217–223. doi:10.1097/IPC.0000000000000387
16. Desta DM, Gebrehiwet WG, Kasahun GG, Asgedom SW, Atey TM, Wondafrash TAG. Exit-knowledge about dispensed medications and associated factors among ambulatory patients attending ayder comprehensive. Patient Prefer Adherence. 2020;Volume 14:1523–1531. doi:10.2147/PPA.S267145
17. Boonstra E, Lindbaek M, Ngome E, Tshukudu K, Fugelli P. Labelling and patient knowledge of dispensed drugs as quality indicators in primary care in Botswana. Qual Saf Heal Care. 2003;12:168–175. doi:10.1136/qhc.12.3.168
18. Holloway KA. Combating the inappropriate use of medicines. Expert Rev Clin Pharmacol. 2011;4:335–348. doi:10.1586/ecp.11.14
19. Andersson K, Melander A, Svensson C, Lind O, Nilsson JLG. Repeat prescriptions: refill adherence in relation to patient and prescriber characteristics, reimbursement level and type of medication. Eur J Public Health. 2005;15:621–626. doi:10.1093/eurpub/cki053
20. Asma US, Mallesh M, Divyaja M, Sree D. Assessment of patient’s knowledge regarding dispensed medication in a south Indian government hospital. Int J Pharm Pharm Sci. 2015.
21. Tesfaye ZT, Yismaw MB, Negash Z, Ayele AG. COVID-19-related knowledge, attitude and practice among hospital and community pharmacists in Addis Ababa, Ethiopia. Integr Pharm Res Pract. 2020;Volume 9:105–112. doi:10.2147/IPRP.S261275
22. Abdelhafiz AS, Mohammed Z, Ibrahim ME, et al. Knowledge, perceptions, and attitude of egyptians towards the novel coronavirus disease (COVID-19). J Community Health. 2020;45:881–890. doi:10.1007/s10900-020-00827-7
23. Mekonen S, Samuel W, Ambelu A. Importance of labelling and patient knowledge to ensure proper care during drug dispensing: A case study from a tertiary hospital in Ethiopia. Open J Prev Med. 2014;04:1–7. doi:10.4236/ojpm.2014.41001
24. Cavaco A, Roter D. Pharmaceutical consultations in community pharmacies: utility of the Roter Interaction Analysis System to study pharmacist-patient communication. Int J Pharm Pract. 2010;18:141–148.
25. Yee D, Valiquette C, Pelletier M, Parisien I, Rocher I, Menzies D. Incidence of serious side effects from first-line antituberculosis drugs among patients treated for active tuberculosis. Am J Respir Crit Care Med. 2003;167:1472–1477. doi:10.1164/rccm.200206-626OC
26. Singh J, Singh N, Kumar R, Bhandari V, Kaur N, Dureja S. Awareness about prescribed drugs among patients attending Out-patient departments. Int J Appl Basic Med Res. 2013;3:48. doi:10.4103/2229-516X.112240
27. Saqib A, Atif M, Ikram R, Riaz F, Abubakar M, Scahill S. Factors affecting patients ’ knowledge about dispensed medicines: A Qualitative study of healthcare professionals and patients in Pakistan. PloS ONE. 2018;13(6): e0197482
28. Alkatheri AM, Albekairy AM. Do the patients’ educational level and previous counselling affect their medication knowledge? Ann Thorac Med. 2013;8:105. doi:10.4103/1817-1737.109823
29. Mekonnen GB, Gelayee DA. Low medication knowledge and adherence to oral chronic medications among patients attending community pharmacies: a cross-sectional study in a low-income country. Biomed Res Int. 2020;2020:1–8. doi:10.1155/2020/4392058
30. Hirko N, Edessa D. Factors influencing the exit-knowledge of patients for dispensed drugs at the outpatient pharmacy of Hiwot Fana specialized University Hospital, Eastern Ethiopia. Patient Prefer Adherence. 2017;Volume 11:205–212. doi:10.2147/PPA.S128658
31. Wogayehu B, Adinew A, Asfaw M.Knowledge on dispensed medications and its determinants among patients attending outpatient pharmacy at chencha primary level hospital, Southwest Ethiopia. Integr Pharm Res Pract. 2020;9:161–173. doi:10.2147/IPRP.S274406.
32. World Health Organization (WHO). Design and procurement of storage facilities. Technical Supplement to WHO Technical report series. No 961, 2014. Available from: https://www.who.int/biologicals/expert_committe/Supplement-2_TS-warehouse-design-ECSPP-ECBS.pdf.
33. Salthouse TA, Miles JD. Ageing and time-sharing aspects of executive control. Mem Cogn. 2002;30:572–582. doi:10.3758/BF03194958
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.