")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Work-Related Musculoskeletal Disorders Among Hospital Midwives in Chenzhou, Hunan Province, China and Associations with Job Stress and Working Conditions
Authors Cao W, Hu L, He Y, Yang P, Li X, Cao S
Received 25 December 2020
Accepted for publication 14 April 2021
Published 3 September 2021 Volume 2021:14 Pages 3675—3686
DOI https://doi.org/10.2147/RMHP.S299113
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Wenjing Cao,1 Lin Hu,2 Yongmei He,3 Ping Yang,4 Xiaoling Li,5 Shunwang Cao6
1Nursing School of Xiang Nan University, Chenzhou, Hunan, People’s Republic of China; 2School of Public Health of Xiang Nan University, Chenzhou, Hunan, People’s Republic of China; 3Department of Nursing, The Affiliated Hospital of Xiangnan University, Chenzhou, Hunan, People’s Republic of China; 4Department of Gastroenterology, The Affiliated Hospital of Xiangnan University, Chenzhou, Hunan, People’s Republic of China; 5Rehabilitation School of Xiang Nan University, Chenzhou, Hunan, People’s Republic of China; 6Department of Laboratory Medicine, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, Guangdong, People’s Republic of China
Correspondence: Shunwang Cao
Department of Laboratory Medicine, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, Guangdong, People’s Republic of China
Tel +86 15625053283
Email [email protected]
Background: Midwives have a high risk of work-related musculoskeletal disorders (WMSDs), which are the leading cause of pain and disability. However, the association between job stress and WMSDs among midwives has not been studied. The aim of this project was to specifically describe relationships between the job stress and WMSDs among a sample of hospital midwives in Chenzhou, Hunan Province, China.
Methods: We conducted a cross-sectional study among a sample of 769 eligible midwives in the city of Chenzhou in Hunan Province, China from May 2018 to January 2019. All participants completed a questionnaire regarding the presence and severity of different pain symptoms and job stress assessed by the Korean occupational stress scale.
Results: A total of 597 participants responded (77.6%), and 491 (82.2%) reported that they had experienced WMSDs at some time over a 12-month period. The most common pain site was low back (72.7%), followed by the neck (52.8%) and shoulders (42.7%). We revealed that various aspects of job stress were associated with WMSDs in the current study, namely “Owing to my workload, I always feel time pressure” (OR, 2.05; 95% CI: 1.28– 3.28), “My job has become increasingly overbearing” (OR, 2.34; 95% CI: 1.46– 3.77), “My work requires long lasting concentration” (OR, 3.50; 95% CI: 2.13– 5.74), “I have to do various jobs simultaneously”, (OR, 3.15; 95% CI: 1.93– 5.14)), “My work requires creativity” (OR, 2.15; 95% CI: 1.31– 3.54), “My work requires a high level of skill or knowledge” (OR, 2.83; 95% CI: 1.67– 4.80), “My supervisor is helpful in getting the job done” (OR, 0.53; 95% CI: 0.33– 0.84), “I have someone who understands my difficulties at work” (OR, 0.53; 95% CI: 0.34– 0.85), “Undesirable changes (ie, downsizing) will come to my job” (OR, 3.28; 95% CI: 2.01– 5.77), “My company provides me with sufficient organizational support” (OR, 0.47; 95% CI: 0.29– 0.74), “Departments cooperate each other without conflicts” (OR, 0.50; 95% CI: 0.32– 0.80), “I am provided with the opportunity to develop my capacity” (OR, 0.57; 95% CI: 0.36– 0.91) and “My company climate is authoritative and hierarchical” (OR: 3.21; 95% CI: 1.97-5.23).
Conclusion: Overall, this study suggests that job stress has an important influence on WMSDs among a sample of hospital midwives in Chenzhou, Hunan Province, China. Given the multifaceted nature of identified risk, a comprehensive approach to reduce this risk is clearly required and a job stress management program will be essential.
Keywords: midwife, work-related musculoskeletal disorders, job stress
Background
Musculoskeletal disorders (MSDs) are a leading cause of disease burden globally, producing discomfort, damage or persistent pain in body structures.1 MSDs can be work-related. The Global Burden of Disease (GBD) has reported that MSDs were the second most common work-related problems worldwide.2,3 WMSDs are defined as MSDs caused or worsened by occupational risk factors significantly, though not exclusively.4–6
Studies have shown that health-care workers are susceptible to work-related musculoskeletal disorders (WMSDs). Midwives are considered the group of the high-risk occupations for WMSDs.7 This is expected given that the nature of midwives’ job that requires prolonged standing, awkward positions, high attention and concentration, stooping, and repetitive actions.7,8 In addition, it is also important to bear in mind that midwifery workforce shortage may have contributed to WMSDs. It should be noted that there is a global shortage of midwives,9 which may pose a desperate burden on work load for the rest of the workforce to bridge gaps in personnel and resulting in increased musculoskeletal symptoms. The prevalence of WMSDs among midwives has been documented in different studies and varies across countries.8 In a cross-sectional study investigating 637 midwives in the United Kingdom reported very high prevalence of musculoskeletal symptoms (91%) in the last 12 months.10 Long MH et al found that a substantial proportion of Australian midwives are troubled by low back and neck discomfort, demonstrating annual prevalence rates of 40.8% for neck and nearly 30% for low back.11 In a study of Polish midwives, 67% of the participants had pain in any segment of the spine.12
As a result of WMSDs, midwives may prevented from carrying out normal activities, absent from work, leave the profession and need to be seen by the physician, which may create adverse effects on quality of life and patient safety.13–15 Furthermore, midwives with WMSDs also should take the negative effect of this impairment on their mental state into account. A previous study conducted in the Northeast United States reported that the prevalence of the comorbidity of MSDs and depression was 14.5% in a sample of nurses,16 and this may be true of midwives as well due to the fact that midwives are members of a unique profession sharing characteristics with nursing.
Given the severe consequences of WMSDs, the relevant factors of WMSDs have been extensively studied to minimize such injuries. Factors associated with WMSDs include not only individual characteristics (eg age, sex, leisure-time exercise, BMI), but also physical risk factors that arise from a worker’s tasks (eg physical demands, handling loads, repetitive movements or vibration).17–20 Numerous previous studies have focused on occupational psychosocial risk factors (eg high psychosocial demands, low job control or inadequate social support, too much overtime) as potential causes of WMSDs.3,21,22 Besides, several studies have demonstrated a relationship between occupational injury and job stress.23,24 There is evidence that excessive job stress lead to an overall increase in the risk for occupational injuries due to the fact that it affects a worker’s ability to escape from risks, decreases risk recognition, and causes excessive fatigue.25–28 A recent study suggests that intrinsic stress is a main contributor for developing WMSDs for the midwifery profession.10 Lang et al found that stress could be a predictor of severe somatic symptoms of WMSDs.29 However, to date no study address the association between job stress and WMSDs in hospital midwives has yet been published. Hence, the impact of a broader range of job stress on midwives’ musculoskeletal health deserves research attention. The purpose of this study was to determine the status of WMSDs among a sample of hospital midwives in Chenzhou, Hunan Province, China and to investigate the existence of association between job stress and WMSDs after adjusting for confounding variables. We hypothesized that there is also an association between job stress and WMSDs.
Methods
Participants
A purposive convenience sampling method was used to recruit participate. First, with the help of Health Commission of Chenzhou, we contacted the nursing administration and human resources departments of 54 hospitals to host this study. The chief nursing officer in each hospital welcomed the research study and expressed interest in applying the findings of the study. A nurse representative from nursing administration served as the main contact and liaison between the hospital and the research team. The liaison from Nursing Administration was responsible for facilitating the Institutional Review Board (IRB) approval process, distributing recruitment flyers, recruiting midwives, and providing a list of all potential participants in study hospital. Midwives were eligible if they met the following criteria: (a) full-time registered midwives, (b) worked in midwifery profession for at least 12 months. Midwives on leave during the survey period or refusing to participate were excluded. Overall, 769 midwives met the initial eligibility criteria. Research assistant then contact those possible participants via phone for further screening to confirm inclusion/exclusion criteria. A total of 687 midwives were eligible to participate after the phone-based screening. The study was approved by the Ethics Committee of the XiangNan University.
Data Collection
We collected data from a cross-sectional survey from May 2018 to January 2019. Structured questionnaire packages, including a recruiting notice, an informed consent form, and an anonymous questionnaire, were distributed by the research team at regularly scheduled staff meetings of each study hospital, which all midwives at the hospital were required to attend. The study objectives, detailed instructions and potential benefits and risks were explained to the participants in person. All participants provided written informed consent. Every individual participating midwife was expected to take his or her own time to complete the questionnaire anonymously and return it to the designated survey collection boxes in a sealed envelope in each hospital within 1 week. The liaison from Nursing Administration in each hospital then sent the collection boxes to researchers by mail.
Survey Instrument
The survey instrument was a structured, self-administered questionnaire, which mainly required checkbox-style answers, and Likert-type scales. The questionnaire included three sections (ie, WMSDs in the previous 12-month period, Job stress and socio-demographic data).
WMSDs were measured based on the Nordic Musculoskeletal Questionnaire (NMQ), which is a valid and reliable assessment tool.30 Participants were asked to rate the severity of pain in nine body regions: neck, shoulders, upper back, elbows, wrists/hands, lower back, hips/thighs, knees, ankles/feet in the previous 12-month period. In order to highlight each part of the body for clarity, participants were provided with anatomic diagrams. The intensity of the symptoms was rated on a 5-point (1=none; 2=mild; 3=moderate; 4=severe; and 5=extreme). WMSDs was defined as “yes” for participants who reported moderate, severe, or extreme pain (≥3 on a 1–5 scale) in any region.31 The impact of such symptoms was explored with the question of “Has the trouble prevented you from carrying out normal activities (eg job, housework, hobbies) during the last 12 months?” Participants could choose between (1) yes (2) no. In addition, midwives were asked whether they had seen a physician for this condition during the last 12 months. Participants could choose between (1) yes (2) no. Besides, participants were asked if they had trouble in each body regions during the past 7 days. Participants could choose between (1) yes (2) no. The trouble was defined as prevented from carrying out normal activities or had seen a physician because of the pain in each region.
Job stress was assessed with the short form of the Korean occupational stress scale (KOSS-SF), which is commonly used to record the job stress.24 The KOSS-SF is comprised of 7 subscales and 24 items, which inquires about job demands (4 items), job control (4 items), interpersonal conflict (3 items), job insecurity (2 items), organizational system (4 items), lack of reward (3 items) and workplace environment (4 items). Each item is rated on a 4-point Likert-type scale (strongly agree, agree, disagree, strongly disagree). The KOSS-SF scale was translated into Chinese and then back-translated to validate the translation by a bilingual professional. Then, experts evaluated the Chinese version for accuracy, clarity, and readability. The Cronbach’s α score for each subscale ranged between 0.51 and 0.82, indicating a high internal consistency.23 The Cronbach’s α coefficient for subscales of job stress for this study ranged from 0.54 to 0.79.
We collected information about the midwives’ demographic and socioeconomic characteristics on hospital size, age, gender, marital status, Body Mass Index (BMI), highest educational level, practice years in midwifery, frequency of exercise (times/week), weekly working hours. Hospital size was separated into either (1) ≤399 beds, (2) ≥400 beds. Marital status was categorised as single, never married, married or domestic partnership, widowed, divorced, separated. BMI was categorised as underweight, normal weight, overweight and obese.32 Possible responses to the question about highest educational level were (1) secondary diploma, (2) associate degree, (3) bachelor’s degree/higher. When it terms to practice years in midwifery, participants could choose between: (1) ≤3 years, (2) 4–10 years, (3) >10 years. Possible responses to the question about frequency of exercise was either <3 times/week or ≥3 times/week. Participants could choose between (1) ≤40 hours, (2) >40 hours regarding the question about weekly working hours.
Statistical Analysis
We collapsed job stress items into dichotomous (agree/disagree) responses in order to simplify analysis and interpretation of the results. Respondents’ general characteristics and WMSDs were described by percentage. Age showed no normal distribution, median and interquartile range was employed.
To assess the prevalence of WMSDs in different participants, the chi-squared test (hospital size, marital status, BMI), fisher’s exact test (gender) and the Mann–Whitney U-test (age) were used. The analysis of the prevalence of WMSDs was based on the general characteristics data. The relationship of job stress and WMSDs were compared by chi-squared test.
In order to determine the association between general characteristics, job stress, and the occurrence of WMSD, we applied Univariate and multivariate logistic regression analysis. Univariate logistic regression analysis was performed with each job stress subtype as an independent variable (Model I). Multivariate logistic regression analysis was performed with hospital size, age, marital status, Body Mass Index (BMI), highest educational level, practice years in midwifery, weekly working hours as adjusted factors (Model II). P values below 0.05 were considered statistically significant throughout the analysis. All analyses were conducted with SPSS 21.0 (SPSS Inc., Chicago IL).
Results
A total of 687 questionnaires were distributed and 608 (88.5%) were retrieved. Eleven incompletely answered the questionnaires leaving 597 (86.9%) for analysis. Table 1 contains a summary of the demographic characteristics of these midwives. The majority were female (only one male), with a mean age of 28.36 (SD=7.00) years. Mean BMI was 23.14 (SD=3.90). Regarding the weekly working hours, 89.3% of the participants reported that their weekly working hours were ≥40 hours. About 58.5% of them worked in hospitals with ≥400 beds hospital.
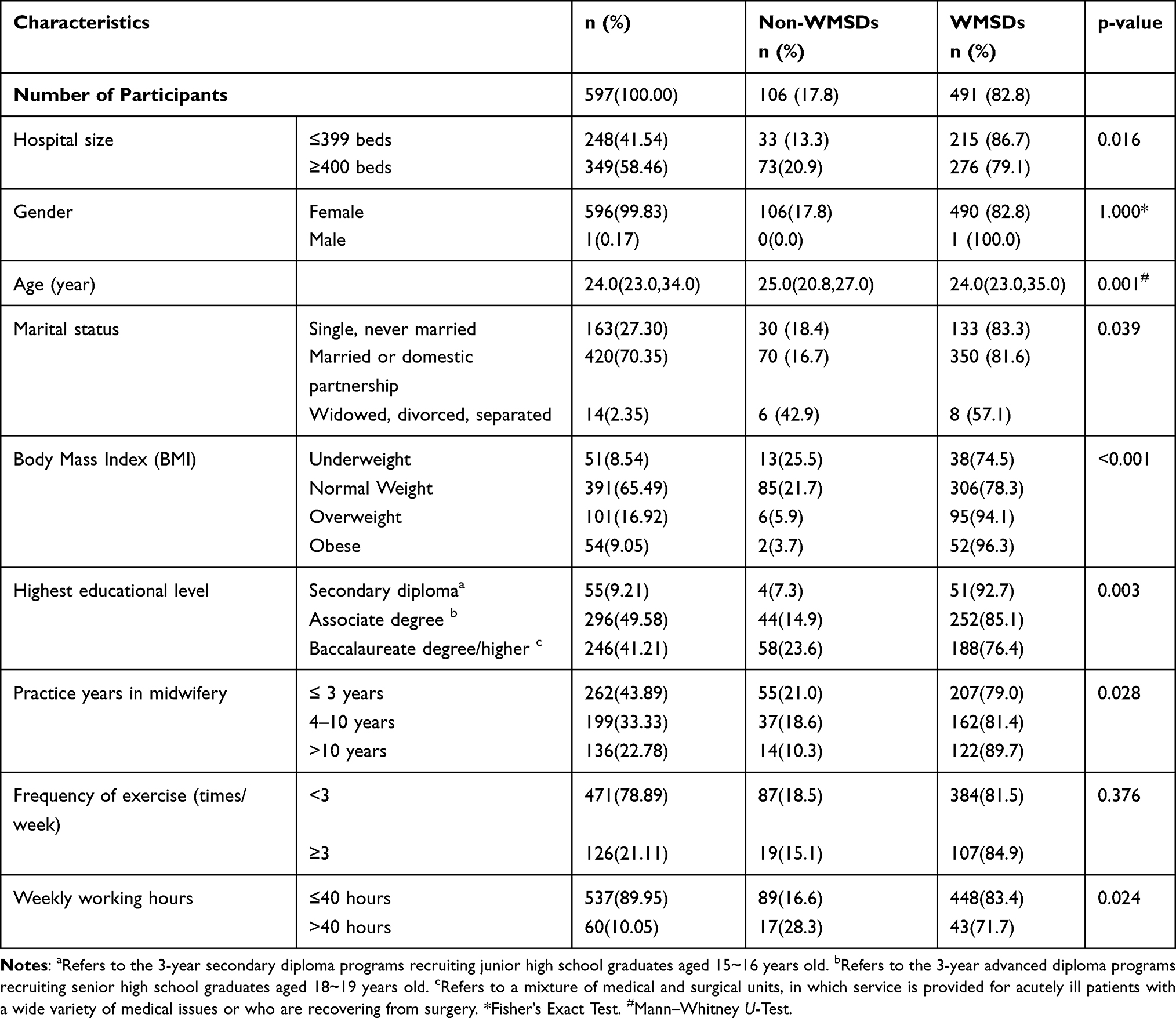 |
Table 1 Differences Between WMSDs and Non-WMSDs in Relation to Population Characteristics |
Among the participants, 491 (82.2%) reported that they had experienced WMSDs at some time over a 12-month period. There were significant differences between WMSDs versus non-WMSDs personnel with respect to hospital size, age, marital status, Body Mass Index (BMI), highest educational level, practice years in midwifery, weekly working hours (Table 1).
The Ratio and Severity WMSDs
According to participants’ answers on The NMQ, the most common pain site was low back (72.7%), followed by the neck (52.8%) and shoulders (42.7%). Of those who reported low back symptoms during the last 12 months, 24.3% had been prevented from carrying out normal activities. Those who indicated that they experienced lower back discomfort were the higher group that had seen a physician during the last 12 months (12.1%), followed by neck (4.2%). Of the participants (29.6%) reported that they experienced discomfort of their lower back during the last seven days (Table 2).
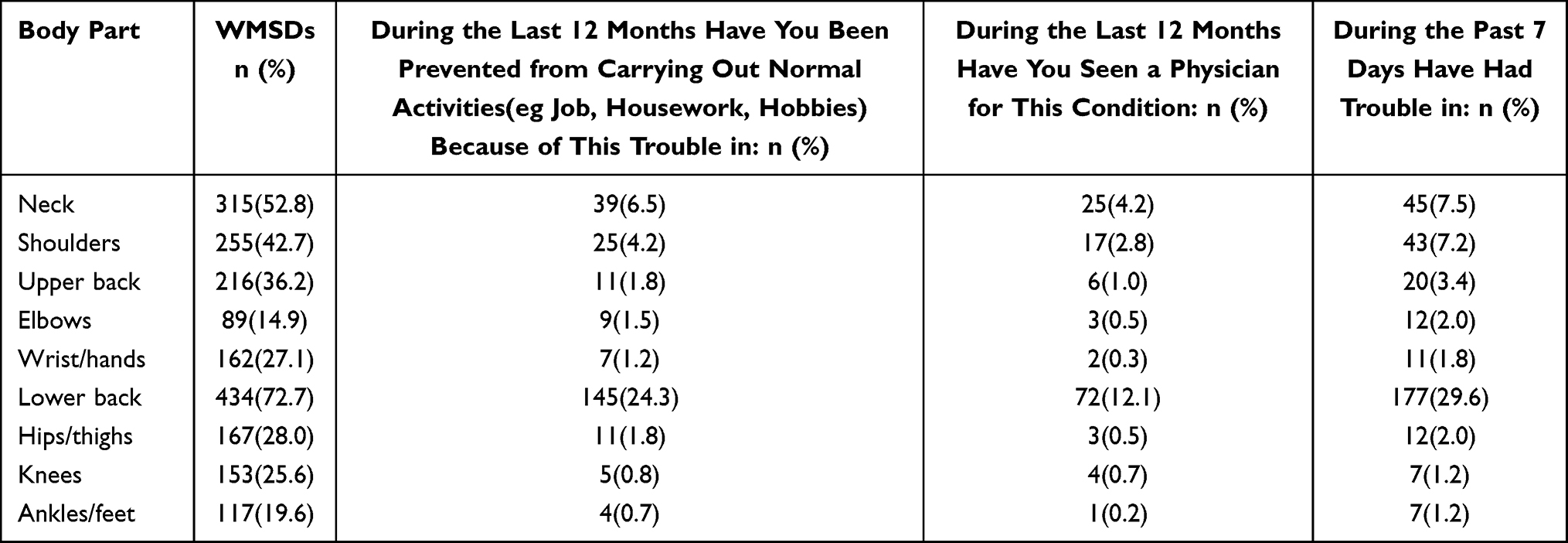 |
Table 2 Pain Location and Impact on Daily Activities and Health Care Seeking |
The Relationship Between Items of Job Stress Scale and WMSDs
Affirmative responses to the job stress Scale and their relationship with WMSDs are reported in Table 3. A total of 485 (81.2%) participants agreed with the statement “My work requires a high level of skill or knowledge”. Four hundred and thirty-four (72.7%) reported that undesirable changes (ie, downsizing) will come to their jobs and a total of 405 (67.8%) participants agree with the statement “My job has become increasingly overbearing”. Four hundred and thirty-nine (73.5%) stated that their work requires long lasting concentration. However, only 186 (31.2%) reported that the organizational policy of their company is fair and reasonable, and finally, 228 (38.2%) participants agreed with the statement “My supervisor is helpful in getting the job done”. WMSDs were associated with fourteen job stress questions.
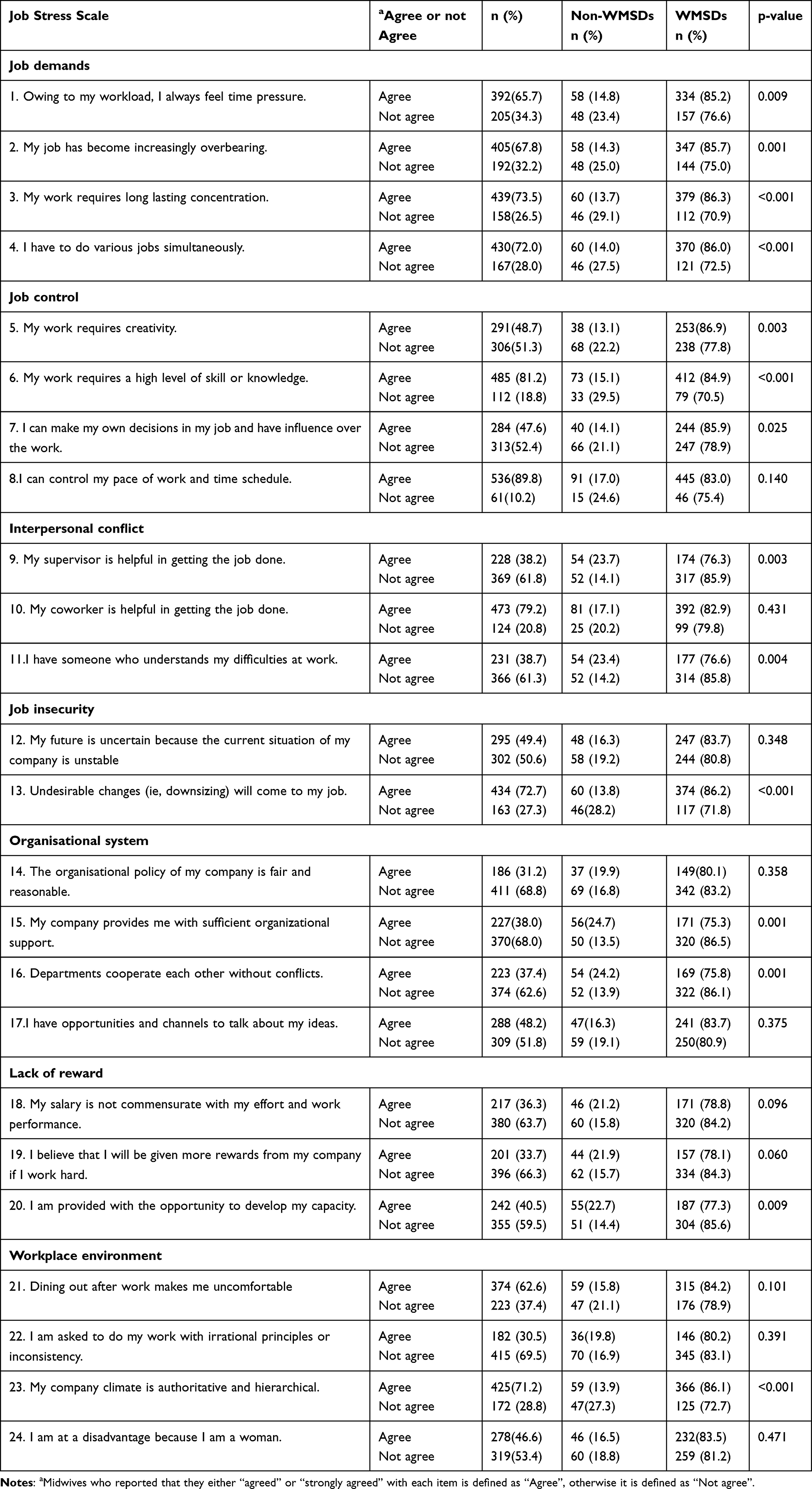 |
Table 3 Presence of WMSDs and Non-WMSDs in Relation to Job Stress Variables |
Logistic Regression Analysis of WMSDs According to Job Stress Adjusted for the Psychosocial Component
Statistical analysis revealed various associations between WMSDs and job stress, as indicated in Table 4. By adjusting the general characteristics such as hospital size, age, marital status, Body Mass Index (BMI), highest educational level, practice years in midwifery, weekly working hours; we revealed that all items from job demands were associated with the occurrence of WMSDs (eg “Owing to my workload, I always feel time pressure” (OR, 2.05; 95% CI: 1.28–3.28), “My job has become increasingly overbearing” (OR, 2.34; 95% CI: 1.46–3.77), “My work requires long lasting concentration” (OR, 3.50; 95% CI: 2.13–5.74), “I have to do various jobs simultaneously” (OR, 3.15; 95% CI: 1.93–5.14)). Meanwhile, midwives who thought that their work requires creativity were more likely to have suffered WMSDs in the previous year (OR, 2.15; 95% CI: 1.31–3.54), as well as midwives who thought that their work requires a high level of skill or knowledge (OR, 2.83; 95% CI: 1.67–4.80). In contrary, “My supervisor is helpful in getting the job done” (OR, 0.53; 95% CI: 0.33–0.84) and “I have someone who understands my difficulties at work” (OR, 0.53; 95% CI: 0.34–0.85) were less likely to have suffered WMSDs in the last 12 months. Furthermore, “Undesirable changes (ie, downsizing) will come to my job” (OR, 3.28; 95% CI: 2.01–5.77), “My company provides me with sufficient organizational support” (OR, 0.47; 95% CI: 0.29–0.74), “Departments cooperate each other without conflicts” (OR, 0.50; 95% CI: 0.32–0.80), “I am provided with the opportunity to develop my capacity” (OR, 0.57; 95% CI: 0.36–0.91) and “My company climate is authoritative and hierarchical” (OR: 3.21; 95% CI: 1.97-5.23) were also related to the occurrence of WMSDs over a 12-month period.
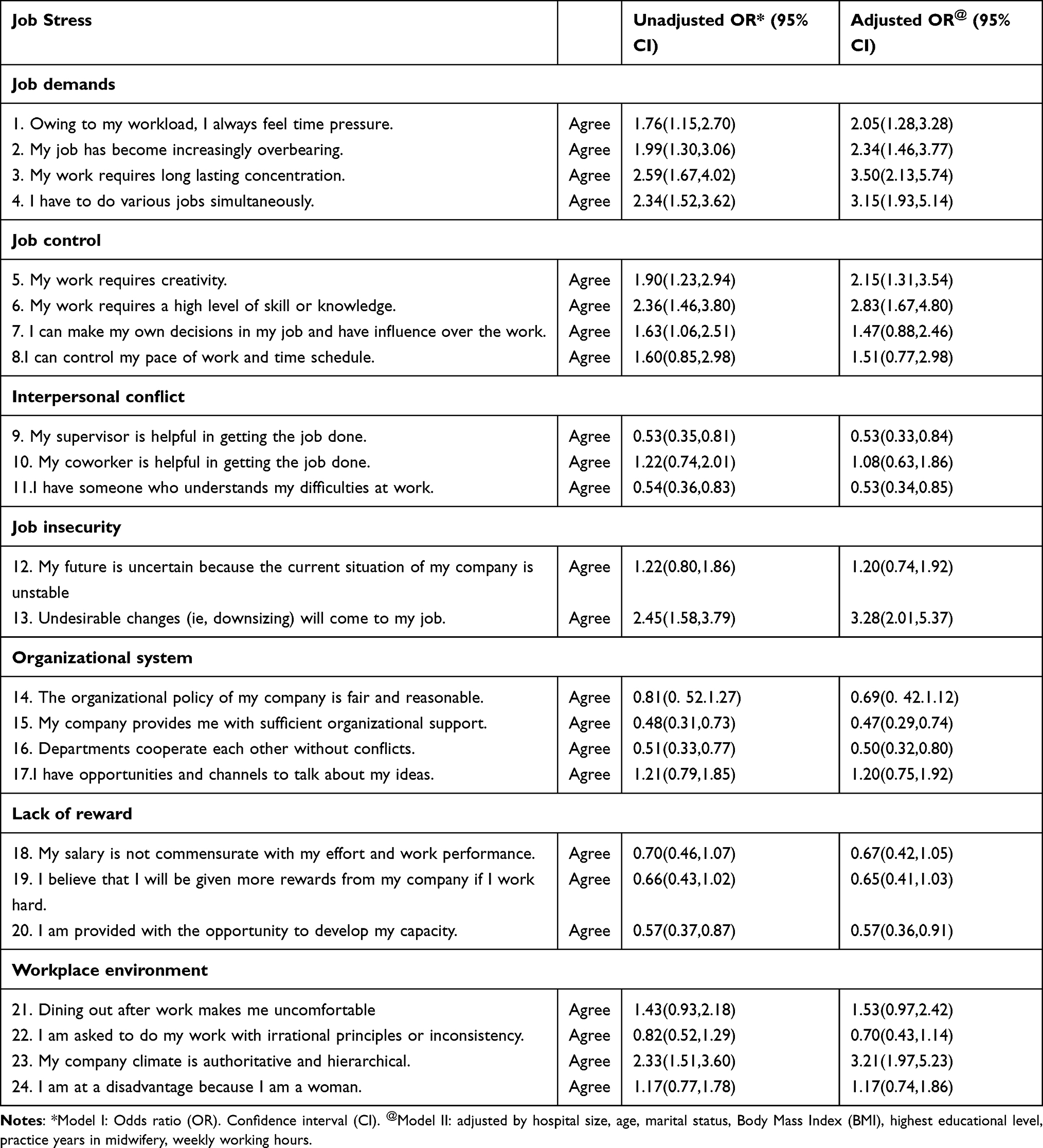 |
Table 4 Logistic Regression Analysis of WMSDs and Non-WMSDs and Job Stress Factors |
Discussion
Based on the results, the prevalence of WMSDs over a 12-month period in our sample was found to be high. The present study showed that 82.2% participants reported that they had experienced WMSDs at some time over a 12-month period. Moreover, the prevalence of lower back pain was the highest of all the parts of the body among hospital midwives, at 72.7%. This result is consistent with the result of a recent study that reported 92% of the participants reported MSDs, most commonly in the low back (71%), neck (45%) and shoulders (45%).10 WMSD prevalence rates are not very different when compared with other health-care professionals, for example, Atheer F. et al found the 12-month prevalence of WMSDs among clinical laboratory workers was 82% and to be most commonly in the low back (61%).33 One possible explanation is that hospital midwives have similar risk exposures at work with such occupations. According to this finding, of those who reported low back symptoms during the last 12 months, 24.3% had been prevented from carrying out normal activities and 12.1% had seen a physician. It is therefore very likely that the WMSDs could have critical implications for the safety and health of hospital midwives themselves and their patients, considering the fact that hospital midwives are caring two loads (mother and baby). Midwives’ emotional well-being is essential to ensure a high quality of woman-centered midwifery care.34 Therefore, efforts to prevent injuries are of great importance, particularly in light of the midwifery shortage. Our findings may highlight the need to control this problem as well as its consequences on the physical and psychological health and wellbeing of the midwifery staff.
Results from our current study offer an interesting insight into the association between job stress and WMSDs among hospital midwives. This finding could be explained by the fact that muscle strain would be intensified if job-related psychological burdens become heavier due to work stress, which can increase the awareness of musculoskeletal symptoms or weaken the capability to manage the symptoms.35,36
We found that all items from job demands were associated with the occurrence of WMSDs. Midwives who always feel time pressure owing to their workload were more likely to have suffered WMSDs in the previous 12 months. Midwives who thought that her/his job has become increasingly overbearing reported a higher prevalence of WMSDs in the last 12 months. In addition, midwives who thought that their work requires long lasting concentration were also more likely to have suffered WMSDs in the last 12 months, as well as midwives who thought that they have to do various jobs simultaneously. It suggests that midwives experience a greater risk of WMSDs corresponding to higher job demands. There is a wealth of literature showing the association between high quantitative workloads and high cognitive demands and occupational injury.37–39 Our current study supports these findings to some extent.
Meanwhile, midwives who thought that their work requires creativity were more likely to have suffered WMSDs in the previous year as well as midwives who thought that their work requires a high level of skill or knowledge. This finding supports previous study indicating that workers had a higher risk of occupational injury when they had less job control.25 However, Nowai L et al demonstrated that an association could not be found between insufficient job control and WMSDs.23
On the other hand, midwives whose supervisor is helpful in getting the job done were nearly half as likely to have suffered WMSDs in the last 12 months; as well as midwives who have someone understand their difficulties at work. A study of the nursing workforce showed that low encouragement and help from management was associated with an decreased risk of occupational injury.40 Our results are in agreement with it, although the nature of the job was different.
Our results suggested that midwives who thought that undesirable changes (ie, downsizing) will come to her/his job were more likely to have suffered WMSDs in the last 12 months. This finding is similar to the study result of Probst TM et al, who clearly indicated that workers in insecure jobs underwent more occupational injuries compared with those in secure jobs.41 It is worrying that due to the increase in birth levels with more women being pregnant at older ages and overweight/obesity, midwives facing more undesirable changes and in more insecure jobs.
The current study suggests that midwives who were provided with sufficient organizational support were less likely to have suffered WMSDs over a 12-month period. This report is almost similar to one of a previous report in Hunan Province, China.42 To our knowledge, sufficient organizational support, like having strong support for safety programs, emphasis on environmental control, frequent safety related feedback or training, regular and open communication had profound impacts on occupational injury.43 In recent years, the impact of organizational system on health care worker’s occupational injuries has been increasingly studied.44 To the best of our knowledge, improving organizational system offers numerous benefits.45 According to this finding, these midwives whose departments cooperating each other without conflicts were less likely to have suffered WMSDs in the previous year. A study of Finish hospital personnel showed that low interpersonal conflicts was associated with an decreased risk of occupational injury.23
It should also be noted that inadequate opportunity to develop their capacities is potential antecedent for the development of WMSDs.46 Hospital midwives who provided with the opportunity to develop their capacities were less likely to have suffered WMSDs in the previous year. This seems to be consistent other research on midwives, for example Bazazan et al found an association between job satisfaction and MSD.47 One possible explanation is that satisfaction at work can be influenced by opportunities for advancement, reward, professionalism and so on.48,49
Finally, the probability of WMSDs among the midwives whose company climate is authoritative and hierarchical was increased. Musculoskeletal discomfort was previously reported to be statistically associated with poor lower company climate.50 Such findings offer an interesting insight into the association between company climate and occupational injuries. A plethora of studies have proved that poor safety climate plays a important role in occupational injuries among healthcare workers.42,51 Our current study supports these findings to some extent. Reducing WMSDs among midwives can be achieved by optimizing the climate.42
Limitations
Some limitations of this study must nevertheless be considered. First, there was possibility that the result was biased by using self-reported questionnaires without any clinical examination to confirm the presence of symptoms and exclude overestimated self-reported musculoskeletal complaints. Second, the sample size was limited to only one city in Hunan Province, China, thereby the results cannot be generalized. Finally, definitive conclusion about causal relationship between job stress and WMSDs cannot be drawn with a cross-sectional design, which allowed the interference of uncontrolled factors. Future analyses of longitudinal data would be desirable to verify the study findings.
Implications
The prevalence of, and factors associated with, WMSDs among health-care workers are well-demonstrated in the literature. Some previous studies have investigated the association between job stress and occupational injuries. However, little is known about association between job stress and WMSDs in midwives. Despite the limitations mentioned above, this study has shed light on the relationship between job stress and WMSDs among this population. This study has important implications for future research in related fields. First, given the fact that the sample size was limited to only one city in Hunan Province, China, the results of this study may not be generalized, further studies with efforts to conduct in wider areas of China are encouraged to further validate the results obtained from this study. Beyond that, further research is needed to explore how to develop strategies to manage or mitigate job stress at work in this occupational group. Lastly, there was possibility that the result was biased by using self-reported questionnaires and missing some potential confounders.
Conclusions
In summary, our study revealed that there was an association between increased job stress and WMSDs among hospital midwives. This research underscores the need for midwives and managers to reinforce risk awareness and highlights the job stress factors that should be ameliorated to prevent WMSDs among midwives. The results are crucial to promote risk-awareness and actions for risk management. Given the multifaceted nature of identified risk, a comprehensive approach to reduce WMSDs is clearly required and a job stress management program will be essential. In an effort to achieve that goal, intervention strategies should focus on decreasing work demand, improving job control, interpersonal conflicts, Job insecurity and optimizing the organisational system, reward as well as workplace environment.
Abbreviations
WMSDs, work-related musculoskeletal disorders; MSDs, musculoskeletal disorders; GBD, The Global Burden of Disease; NMQ, Nordic Musculoskeletal Questionnaire; BMI, body mass index.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of the XiangNan University (ref. 39/2018) in accordance with the Declaration of Helsinki. Written consent was obtained from all participation at the time of data collection.
Acknowledgments
We would like to express our deepest gratitude to all midwives who volunteered to take part in the study.
Funding
This work was supported by the Scientific research project of Traditional Chinese Medicine Bureau of Guangdong Province (20202067).
Disclosure
The authors declare no financial or non-financial conflicts interest regarding this work.
References
1. Veerman JL. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;10100(390):1260–1344.
2. Veerman JL. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;10159(392):1789–1858.
3. Bernal D, Campos-Serna J, Tobias A, Vargas-Prada S, Benavides F, Serra C. Work-related psychosocial risk factors and musculoskeletal disorders in hospital nurses and nursing aides: a systematic review and meta-analysis. Int J Nurs Stud. 2015;2(52):635–648. doi:10.1016/j.ijnurstu.2014.11.003
4. Tajvar A, Arab-Zozani M, Hassanipour S. Letter to “work-related musculoskeletal disorders in Iranian dentists: a systematic review and meta-analysis”. Saf Health Work. 2019;2(10):248–249. doi:10.1016/j.shaw.2019.03.002
5. ZakerJafari H, YektaKooshali M. Work-related musculoskeletal disorders in Iranian dentists: a systematic review and meta-analysis. Saf Health Work. 2018;1(9):1–9. doi:10.1016/j.shaw.2017.06.006
6. Davis K, Kotowski S. Prevalence of musculoskeletal disorders for nurses in hospitals, long-term care facilities, and home health care: a comprehensive review. Hum Factors. 2015;5(57):754–792. doi:10.1177/0018720815581933
7. Luan H, Hai N, Xanh P, et al. Musculoskeletal disorders: prevalence and associated factors among district hospital nurses in Haiphong, vietnam. Biomed Res Int. 2018;2018:3162564. doi:10.1155/2018/3162564
8. Long M, Johnston V, Bogossian F. Work-related upper quadrant musculoskeletal disorders in midwives, nurses and physicians: a systematic review of risk factors and functional consequences. Appl Ergon. 2012;3(43):455–467. doi:10.1016/j.apergo.2011.07.002
9. Matlala MS, Lumadi TG. Perceptions of midwives on shortage and retention of staff at a public hospital in Tshwane District. Curationis. 2019;1(42):e1–e10.
10. Okuyucu K, Gyi D, Hignett S, Doshani A. Midwives are getting hurt: UK survey of the prevalence and risk factors for developing musculoskeletal symptoms. Midwifery. 2019;79:102546. doi:10.1016/j.midw.2019.102546
11. Long MH, Johnston V, Bogossian FE. Helping women but hurting ourselves? Neck and upper back musculoskeletal symptoms in a cohort of Australian Midwives. Midwifery. 2013;29(4):359–367. doi:10.1016/j.midw.2012.02.003
12. Nowotny-Czupryna O, Naworska B, Brzęk A, et al. Professional experience and ergonomic aspects of midwives’ work. Int J Occup Med Environ Health. 2012;3(25):265–274.
13. Carriere J, Thibault P, Sullivan M. The Mediating role of recovery expectancies on the relation between depression and return-to-work. J Occup Rehabil. 2015;2(25):348–356. doi:10.1007/s10926-014-9543-4
14. Younan L, Clinton M, Fares S, Jardali F, Samaha H. The relationship between work-related musculoskeletal disorders, chronic occupational fatigue, and work organization: a multi-hospital cross-sectional study. J Adv Nurs. 2019;8(75):1667–1677. doi:10.1111/jan.13952
15. Long M, Bogossian F, Johnston V. The prevalence of work-related neck, shoulder, and upper back musculoskeletal disorders among midwives, nurses, and physicians: a systematic review. Workplace Health Saf. 2013;5(61):223–229.
16. Zhang Y, ElGhaziri M, Nasuti S, Duffy J. The comorbidity of musculoskeletal disorders and depression: associations with working conditions among hospital nurses. Workplace Health Saf. 2020;7(68):346–354. doi:10.1177/2165079919897285
17. Ribeiro T, Serranheira F, Loureiro H. Work related musculoskeletal disorders in primary health care nurses. Appl Nurs Res. 2017;33:72–77. doi:10.1016/j.apnr.2016.09.003
18. Pugh J, Cormack K, Gelder L, Williams A, Twigg D, Blazevich A. Exercise, fitness and musculoskeletal health of undergraduate nursing students: a cross-sectional study. J Adv Nurs. 2019;10(75):2110–2121. doi:10.1111/jan.13990
19. Khairy W, Bekhet A, Sayed B, Elmetwally S, Elsayed A, Jahan A. Prevalence, profile, and response to work-related musculoskeletal disorders among Egyptian physiotherapists. Open Access Macedonian j Med Sci. 2019;10(7):1692–1699. doi:10.3889/oamjms.2019.335
20. Mehdizadeh A, Vinel A, Hu Q, Schall M, Gallagher S, Sesek R. Job rotation and work-related musculoskeletal disorders: a fatigue-failure perspective. Ergonomics. 2020;4(63):461–476. doi:10.1080/00140139.2020.1717644
21. Urquhart DM, Kelsall HL, Hoe VC, Cicuttini FM, Forbes AB, Sim MR. Are psychosocial factors associated with low back pain and work absence for low back pain in an occupational cohort? Clin J Pain. 2013;12(29):1015–1020. doi:10.1097/AJP.0b013e31827ff0c0
22. Yang S, Lu J, Zeng J, Wang L, Li Y. Prevalence and Risk factors of work-related musculoskeletal disorders among intensive care unit nurses in China. Workplace Health Saf. 2019;6(67):275–287. doi:10.1177/2165079918809107
23. Kim Y, Ahn Y, Kim K, Yoon J, Roh J. Association between job stress and occupational injuries among Korean firefighters: a nationwide cross-sectional study. BMJ Open. 2016;11(6):e012002. doi:10.1136/bmjopen-2016-012002
24. Kim M, Kim K, Ryoo J, Yoo S. Relationship between occupational stress and work-related musculoskeletal disorders in Korean male firefighters. Ann Occupational Environ Med. 2013;1(25):9. doi:10.1186/2052-4374-25-9
25. Nakata A, Ikeda T, Takahashi M, et al. Impact of psychosocial job stress on non-fatal occupational injuries in small and medium-sized manufacturing enterprises. Am J Ind Med. 2006;8(49):658–669. doi:10.1002/ajim.20338
26. Swaen GM, van Amelsvoort LP, Bültmann U, Slangen JJ, Kant IJ. Psychosocial work characteristics as risk factors for being injured in an occupational accident. J Occup Environ Med. 2004;6(46):521–527. doi:10.1097/01.jom.0000128150.94272.12
27. Ajith M, Ghosh A, Jansz J. Risk factors for the number of sustained injuries in artisanal and small-scale mining operation. Saf Health Work. 2020;1(11):50–60. doi:10.1016/j.shaw.2020.01.001
28. Schreibauer E, Hippler M, Burgess S, Rieger M, Rind E. Work-related psychosocial stress in small and medium-sized enterprises: an integrative review. Int J Environ Res Public Health. 2020;20:17.
29. Lang J, Ochsmann E, Kraus T, Lang J. Psychosocial work stressors as antecedents of musculoskeletal problems: a systematic review and meta-analysis of stability-adjusted longitudinal studies. Soc Sci Med. 2012;7(75):1163–1174. doi:10.1016/j.socscimed.2012.04.015
30. Kuorinka I, Jonsson B, Kilbom A, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;3(18):233–237. doi:10.1016/0003-6870(87)90010-X
31. Zhang Y, Duffy J, de Castillero E, Wang K. Chronotype, Sleep Characteristics, and Musculoskeletal Disorders Among Hospital Nurses. Workplace Health Saf. 2018;1(66):8–15. doi:10.1177/2165079917704671
32. Taghizadeh N, Boezen H, Schouten J, Schröder C. BMI and lifetime changes in BMI and cancer mortality risk. PLoS One. 2015;4(10):e0125261. doi:10.1371/journal.pone.0125261
33. AlNekhilan A, AlTamimi A, AlAqeel B, AlHawery A, AlFadhel S, Masuadi E. Work-related musculoskeletal disorders among clinical laboratory workers. Avicenna J Med. 2020;1(10):29–34.
34. Cull J, Hunter B, Henley J, Fenwick J, Sidebotham M. “Overwhelmed and out of my depth”: responses from early career midwives in the United Kingdom to the Work, Health and Emotional Lives of Midwives study. Women Birth. 2020;6(33):e549–e557. doi:10.1016/j.wombi.2020.01.003
35. Dick R, Lowe B, Lu M, Krieg E. Further trends in work-related musculoskeletal disorders: a comparison of risk factors for symptoms using quality of work life data from the 2002, 2006, and 2010 general social survey. J Occup Environ Med. 2015;8(57):910–928. doi:10.1097/JOM.0000000000000501
36. Bongers PM, de Winter CR, Kompier MA, Hildebrandt VH. Psychosocial factors at work and musculoskeletal disease. Scand J Work Environ Health. 1993;5(19):297–312. doi:10.5271/sjweh.1470
37. López-García J, García-Herrero S, Gutiérrez J, Mariscal M. Psychosocial and Ergonomic Conditions at Work: influence on the Probability of a Workplace Accident. Biomed Res Int. 2019;2019:2519020. doi:10.1155/2019/2519020
38. Niedhammer I, Lesuffleur T, Labarthe G, Chastang J. Role of working conditions in the explanation of occupational inequalities in work injury: findings from the national French SUMER survey. BMC Public Health. 2018;1(18):344. doi:10.1186/s12889-018-5254-7
39. Kim H, Min J, Min K, Park S. Job strain and the risk for occupational injury in small- to medium-sized manufacturing enterprises: a prospective study of 1209 Korean employees. Am J Ind Med. 2009;4(52):322–330. doi:10.1002/ajim.20673
40. Teo S, Nguyen D, Trevelyan F, Lamm F, Boocock M. Workplace bullying, psychological hardiness, and accidents and injuries in nursing: a moderated mediation model. PLoS One. 2021;1(16):e0244426. doi:10.1371/journal.pone.0244426
41. Probst T, Jiang L, Graso M. Leader-member exchange: moderating the health and safety outcomes of job insecurity. J Saf Res. 2016;56:47–56. doi:10.1016/j.jsr.2015.11.003
42. Cao W, Cao N, Gu M, et al. Prevalence of percutaneous injuries and associated factors among a sample of midwives in Hunan province, china. Workplace Health Saf. 2020;9(68):422–431. doi:10.1177/2165079920914923
43. Olds D, Aiken L, Cimiotti J, Lake E. Association of nurse work environment and safety climate on patient mortality: a cross-sectional study. Int J Nurs Stud. 2017;74:155–161. doi:10.1016/j.ijnurstu.2017.06.004
44. Julià M, Catalina-Romero C, Calvo-Bonacho E, Benavides F. The impact of job stress due to the lack of organisational support on occupational injury. Occup Environ Med. 2013;9(70):623–629. doi:10.1136/oemed-2012-101184
45. Aljabri D, Vaughn A, Austin M, et al. An investigation of healthcare worker perception of their workplace safety and incidence of injury. Workplace Health Saf. 2020;5(68):214–225. doi:10.1177/2165079919883293
46. Hampton GM, Hampton DL. Relationship of professionalism, rewards, market orientation and job satisfaction among medical professionals: the case of Certified Nurse-Midwives. J Bus Res. 2004;5:57.
47. Bazazan A, Dianat I, Bahrampour S, et al. Association of musculoskeletal disorders and workload with work schedule and job satisfaction among emergency nurses. Int Emerg Nurs. 2019;44:8–13. doi:10.1016/j.ienj.2019.02.004
48. Arkwright L, Edgar S, Debenham J. Exploring the job satisfaction and career progression of musculoskeletal physiotherapists working in private practice in Western Australia. Musculoskeletal Sci Practice. 2018;35:67–72. doi:10.1016/j.msksp.2018.03.004
49. Bulduk S, Bulduk E, Güler A. Job satisfaction among aircraft baggage handlers and their exposure to risk factors for work-related musculoskeletal disorders: a case study. Work. 2017;2(56):301–308.
50. Arcury T, O’Hara H, Grzywacz J, Isom S, Chen H, Quandt S. Work safety climate, musculoskeletal discomfort, working while injured, and depression among migrant farmworkers in North Carolina. Am J Public Health. 2012;102(S2):S272–278. doi:10.2105/AJPH.2011.300597
51. Bagheri Hosseinabadi M, Khanjani N, Etemadinezhad S, Samaei S, Raadabadi M, Mostafaee M. The associations of workload, individual and organisational factors on nurses’ occupational injuries. J Clin Nurs. 2019;28:902–911. doi:10.1111/jocn.14699
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.