")
Back to Journals » Clinical Ophthalmology » Volume 17
Work Intensity of Postoperative Care Following Implantation of Presbyopia-Correcting versus Monofocal Intraocular Lenses
Authors Maloney RK, Doane J, Weinstock R, Donaldson KE
Received 21 April 2023
Accepted for publication 27 June 2023
Published 17 July 2023 Volume 2023:17 Pages 1993—2001
DOI https://doi.org/10.2147/OPTH.S418128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Robert K Maloney,1 John Doane,2 Robert Weinstock,3 Kendall E Donaldson4 On behalf of AECOS Postoperative Care Study Group
1Maloney-Shamie Vision Institute, Los Angeles, CA, USA; 2Discover Vision Centers, Kansas City, MO, USA; 3The Eye Institute of West Florida, Saint Petersburg, FL, USA; 4Bascom Palmer Eye Institute, Plantation, FL, USA
Correspondence: Robert K Maloney, Maloney-Shamie Vision Institute, 10921 Wilshire Blvd, Suite 900, Los Angeles, CA, 90024, USA, Tel +1 310-208-3937, Fax +1 310-208-8058, Email [email protected]
Purpose: To compare the work intensity of postoperative care following implantation of presbyopia-correcting intraocular lenses (IOLs) to that of standard monofocal IOLs.
Patients and Methods: This open-label, multicenter, comparative study retrospectively reviewed the case records of cataract surgery patients who underwent bilateral implantation of either presbyopia-correcting IOLs (presby-IOL group; N=177) or standard monofocal IOLs (monofocal group; N=177). Outcome measures included the total time the patient spent in the office, number of visits, mean duration of visits, and the number of procedures and diagnostic tests during the first postoperative year. Outcome measures were compared between the first 90 days and days 91– 365 after surgery.
Results: Mean (±SD) time spent in the office during the first postoperative year was 5:50 ± 3:35 hours (H:MM) over 6.6 ± 2.9 visits in the presby-IOL group, compared to 3:38 ± 1:36 hours over 4.9 ± 1.6 visits in the monofocal IOL group (p < 0.001). During the first 90 days, a presby-IOL patient spent 40 minutes longer in the office than a monofocal IOL patient (3:39 ± 1:38 hours vs 2.59 ± 1:13 hours) (p < 0.001). During days 91– 365, time in the office was 1:32 hours longer (p < 0.001), and the mean visit duration was 8 minutes longer for the presby-IOL patients (p=0.002) than those with monofocal IOL. In addition, the presby-IOL patients underwent more procedures and diagnostic tests (p ≤ 0.001) as compared with standard monofocal cataract surgery patients.
Conclusion: Patients implanted with presbyopia-correcting IOLs require significantly more clinic time, diagnostic testing, and procedures postoperatively as compared with standard monofocal cataract surgery patients.
Keywords: AECOS, presbyopia-correcting IOLs, multifocal IOLs, cataract surgery, work intensity of postoperative care
Introduction
Cataract surgery has evolved from simple removal of a cataract into a procedure that can provide patients with a high level of independence from distance and near spectacles. However, the use of a presbyopia-correcting intraocular lens (IOL) can place more demands on the patient and the surgeon, both pre-operatively and post-operatively.1 The use of these lenses can require additional surgical interventions such as earlier or more frequent Neodymium-doped yttrium aluminium garnet (Nd:YAG) capsulotomies, or refractive enhancements.2,3 Presbyopia-correcting IOL patients require a return to the operating room to perform an IOL exchange, rotation, or enhancement more frequently than standard monofocal IOL patients.2,3 Presbyopia-correcting lenses may also require more intensive treatment postoperatively for dry eye or other ocular surface problems perhaps due to higher expectations and greater sensitivity from ocular surface irregularities with multifocal technology.4 Patients with presbyopia-correcting IOLs can require more postoperative counseling because of higher expectations, positive and negative dysphotopsias, or dissatisfaction with the quality of vision.5,6 All these challenges can translate to additional postoperative work for the patient and the surgeon.
The United States Centers for Medicare and Medicaid Services (CMS) permits patient billing for the additional costs involved in the implantation and perioperative care of presbyopia-correcting IOLs, as do many jurisdictions around the globe.7 An understanding of the time and effort involved in the care of these patients may help surgeons to plan their clinical time and determine a charge for the extra services. One study examined the additional work required preoperatively,8 but there has been no systematic study of the additional postoperative time and work required for implanting presbyopia-correcting IOLs. This retrospective multicenter study compares the work intensity of postoperative care during the first year after surgery for patients who received bilateral presbyopia-correcting IOLs (presby-IOL group) to a control group of patients who received bilateral standard monofocal IOLs (monofocal IOL group) in the same practices, performed by the same surgeons.
Materials and Methods
This multicenter, open-label, retrospective, comparative study enrolled two groups of patients who underwent bilateral cataract surgery. The presby-IOL group included patients who received presbyopia-correcting IOLs in both eyes. The monofocal group included patients who received spherical monofocal IOLs with no additional refractive services, such as limbal relaxing incisions. Patients underwent bilateral cataract surgery performed by an experienced cataract surgeon at one of 18 participating practices in the USA (Appendix A). De-identified patient data were collected and analyzed in accordance with the tenets of the Declaration of Helsinki and its amendments. The study protocol was approved by Salus Independent Review Board (Austin, TX, USA) with a waiver of informed consent as data were collected as part of normal medical practice.
The primary outcome measure was the mean total time spent in the office during the first year after surgery in the presby-IOL group compared to the monofocal IOL group. Secondary outcome measures were mean duration per visit, number of visits, and number of tests and procedures during the first postoperative year. Additionally, these outcome measures were analyzed for days 1–90 and days 91–365 after surgery.
Eligible patients in either group were at least 18 years old, and underwent bilateral successive uncomplicated cataract surgery, with the second eye surgery performed within 30 days of the first eye surgery.
Patients excluded from both groups included those whose care (for either eye) was comanaged outside the practice; those who had cataract surgery in either eye as part of a clinical study; those whose surgery in either eye was combined with any other ocular procedure; those who had a preoperative diagnosis of glaucoma, diabetes, keratoconus, subclinical keratoconus or forme fruste keratoconus; who had prior ocular surgery, including refractive surgery; those who required the intraoperative use of a pupil expansion device; in whom capsule staining with trypan blue or other agents was performed; or those who had any intraoperative complication. In addition, patients were excluded if, in the investigator’s opinion, their postoperative best spectacle-corrected acuity based on the preoperative exam was expected to be worse than 20/20 in either eye due to pre-existing ocular comorbidities. The intention was to exclude patients with other disorders that might require additional care unrelated to the cataract surgery but still permit enrollment of patients with mild macular degeneration or mild dry eye disease that was not visually significant.
Patients were eligible for inclusion in the presby-IOL group if they had a presbyopia-correcting IOL implanted in both eyes. For this study, a presbyopia-correcting IOL was defined as an IOL with Food and Drug Administration (FDA) labeling that the lens provides a greater range of vision than a monofocal IOL. This included multifocal lenses (spherical and toric models), extended depth of focus (EDOF) lenses (spherical and toric models), and the Crystalens (Bausch + Lomb, Rochester, NY) (spherical and toric models). Monofocal toric IOLs not labeled to provide an increased range of vision, such as the Trulign lens (Bausch + Lomb) or the Light-Adjustable Lens (RxSight, Aliso Viejo, CA), were excluded from the study. Femtosecond laser use and intraoperative incisions for the correction of astigmatism were permitted in this group.
Patients were eligible for inclusion in the monofocal IOL group if they had bilateral implantation of spherical monofocal IOLs and had no intraoperative refractive services such as aberrometry measurement or astigmatic incisions. Patients who had femtosecond laser treatment in either eye were also excluded from this group.
To enroll patients, each site started from the last patient operated on prior to January 1, 2019, and worked backward through the list of all patients who had cataract surgery until 10 patients meeting all inclusion and exclusion criteria were identified for each group. The purpose of starting prior to January 1, 2019, was to ensure patients completed postoperative care prior to the disruption of the coronavirus disease (COVID) pandemic to avoid discontinuity of care introduced by the pandemic. Working backward from that date was designed to capture the most recent generation of presbyopia-correcting IOLs. Patients were chosen consecutively to minimize investigator bias. One site enrolled 7 patients in each group rather than 10, resulting in a study population of 177 eyes in each group.
All postoperative visits during the 12-month period (365 days) following the first eye surgery were logged, including visits unrelated to the cataract surgery. All participating practices used electronic health record (EHR) systems that logged visit start and stop times via electronic time stamps. The patient’s check-in and check-out times were recorded in hours, minutes, and seconds (HH:MM:SS). The following times were gathered from the EHR system for each patient, depending on what the investigator’s EHR system recorded: arrival time in the office (A), the time the patient was picked up from the waiting room by the technician (B), the time the patient was sent to the front desk after finishing in the clinic (C), and time the patient left the office (D).
To calculate visit duration, the time of the beginning of the visit (either A or B) was subtracted from the time at the end of the visit (either C or D). Depending on the data available in the EHR, the visit duration could be calculated by one of four possible differences: method 1 (C-B); method 2 (D-B); method 3 (C-A); or method 4 (D-A). When data were available to calculate duration by more than one method, method 1 was the most preferred, and method 4 was the least preferred. This means that at visits for which complete data (A, B, C and D) were available, the duration of the visit was always calculated as C-B (difference between the time the patient was sent to the front desk and tech pick-up time). For visits for which time stamps C or B were not available, the duration of the visit was calculated by one of the other methods, according to the order of preference provided above. The formulas used for calculating visit duration occurred with roughly equal frequency in both groups (Table 1). The differences were not statistically significant (p=0.177, chi-square test).
 |
Table 1 The Proportion of Visits with Duration Calculated by the Four Different Methods |
Surgical procedures and diagnostic tests performed on either eye or eyelid were documented. All diagnostic tests with a current procedural terminology (CPT) code (except refraction), all procedures with a CPT code, and all refractive procedures performed at each visit were recorded. Diagnostic tests performed bilaterally were considered one test. However, a surgical procedure performed on both eyes, such as bilateral laser-assisted in situ keratomileusis (LASIK) enhancement or bilateral inferior punctal plug placement, was counted as two procedures. Procedures normally performed as part of the exam, such as tonometry or refraction, were not recorded. Similarly, biometry performed on the day of surgery or between the two eye surgeries was also considered a part of preoperative work-up and was not recorded.
Statistical analysis was performed using IBM SPSS software (version 27.0). Descriptive statistics on continuous variables included mean, standard deviation, median, and range. The normality of data was checked using the Kolmogorov–Smirnov test, histograms, and quantile-quantile plots. For normally distributed data, the independent t-test was used to compare the differences between the two groups; otherwise, the Mann–Whitney U-test was used. To compare the duration per visit between the two groups, Generalized Estimating Equations (GEE) that consider the effect of correlated data within a group (multiple responses from the same patient taken at different time points) were used. For missing visit duration data, the missing values were imputed with the median value of the time spent in the office for all postop visits at that site for patients in the same IOL group. The missing visit duration data were imputed for 8 visits in the monofocal IOL group and 4 visits in the presby-IOL group. A p-value of less than 0.05 was considered statistically significant.
Results
Patient Demographics
One hundred seventy-seven patients were enrolled in each group. The mean age of the patients was 71.11 ± 8.82 years (range 48 to 100 years) in the monofocal IOL group and 66.41 ± 8.36 years (range 32 to 86 years) in the presby-IOL group. Thirty-two percent of the monofocal IOL group was male, and 33% of the presby-IOL group was male. IOLs used in the presby-IOL group were the ReSTOR multifocal IOL (Alcon, Fort Worth, TX), PanOptix multifocal IOL (Alcon, Fort Worth, TX), Symfony IOL (Johnson and Johnson Vision, Santa Ana, CA), Tecnis Multifocal IOL (Johnson and Johnson Vision, Santa Ana, CA) and Crystalens (Bausch and Lomb, Inc., Rochester, NY). Eight eyes had Crystalens, and the remainder had multifocal or EDOF lenses.
Postoperative Time Comparison
The mean time spent in the office during the first postoperative year for a patient in the presby-IOL group was 5:50 ± 3:35 hours (mean ± SD) over 6.6 ± 2.9 visits, compared to 3:38 ± 1:36 hours over 4.9 ± 1.6 visits for a patient in the monofocal IOL group (p <0.001). The mean visit duration was 8 minutes longer for a presby-IOL patient compared to a monofocal IOL patient (p = 0.002). During the first 90 days, a presby-IOL patient spent 40 minutes longer in the office than a monofocal IOL patient (3:39 ± 1:38 hours vs 2.59 ± 1:13 hours). Time in the office was 1 hour and 32 minutes longer for the presby-IOL patient during days 91–365 (2:10 ± 2:53 hours vs 0:38 ± 0:55 hours, p <0.001) (Table 2).
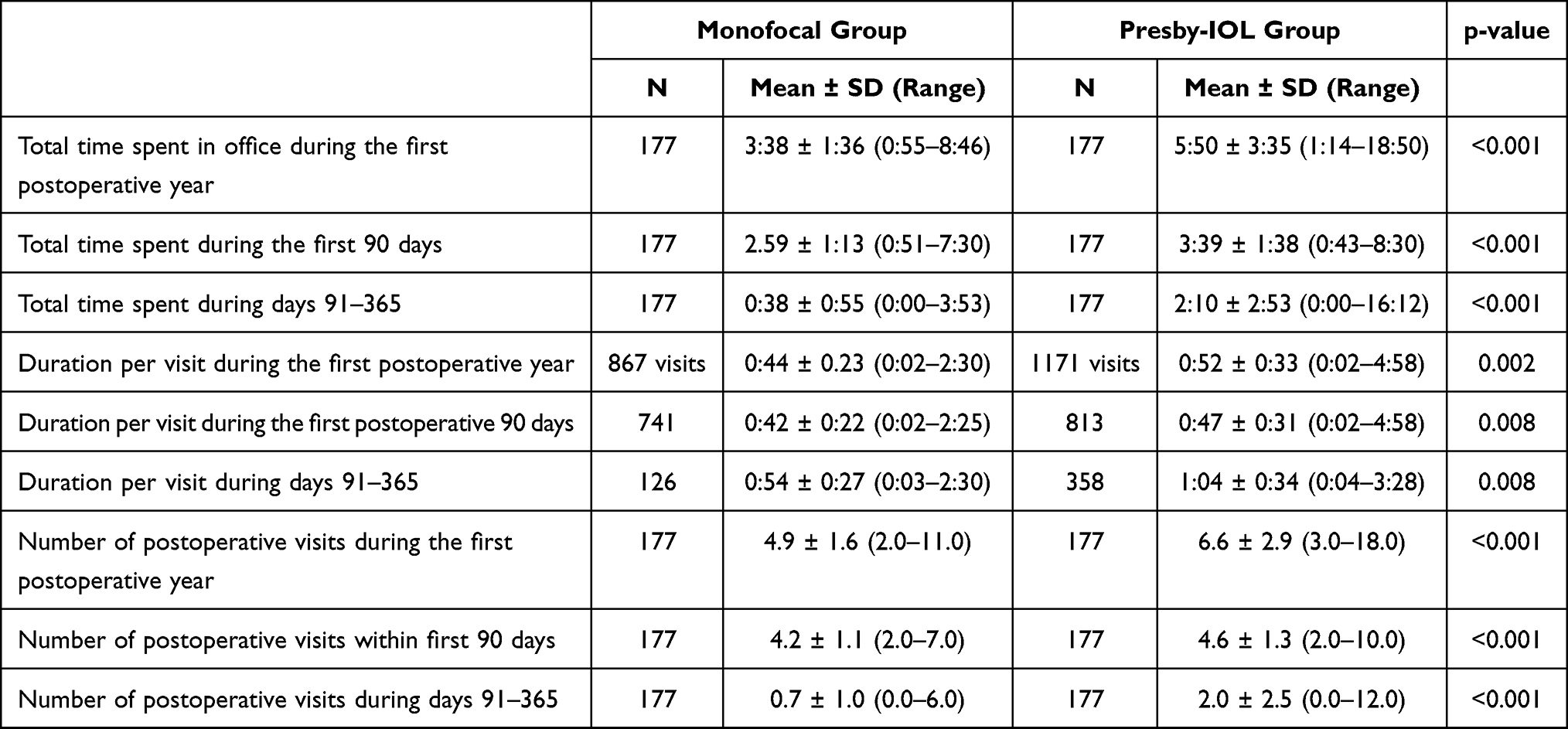 |
Table 2 Postoperative Care Time, Duration per Visit, and the Number of Postoperative Visits in the Monofocal IOL and Presby-IOL Groups |
Comparison of Frequency of Postoperative Procedures
We compared the number of procedures and diagnostic tests in the two groups. We included all diagnostic tests and surgical procedures with an associated CPT code and all refractive surgical procedures as well. A presby-IOL patient underwent a mean of 1.69 procedures and diagnostic tests during the first year, whereas a monofocal IOL patient underwent 0.51 procedures (p <0.001). The difference in the number of procedures was significant during the first 90 days (p=0.001) and days 91–365 (p <0.001) (Table 3).
 |
Table 3 Number of Procedures in the Monofocal IOL and Presby-IOL Groups |
Table 4 shows the diagnostic tests and surgical interventions performed in each group. Nd:YAG capsulotomy was the most common procedure performed in the presby-IOL group, done in 35% of patients, followed by macula optical coherence tomography (OCT) in 28% of patients. In the standard monofocal IOL group, the most common procedure was a macular OCT in 16% of patients. Sixteen percent of patients in the presby-IOL group underwent a refractive enhancement procedure, such as LASIK or limbal relaxing incisions. None of the patients in the monofocal group had a refractive enhancement procedure.
 |
Table 4 Postoperative Procedures Performed in the Monofocal IOL and Presby-IOL Groups |
Discussion
In this study, we compared the intensity of postoperative care during the first year after bilateral presbyopia-correcting IOL implantation to that of bilateral standard monofocal IOL implantation. Our primary measure of work intensity was the mean time a patient spent in the office in each group during the first year. Secondary measures of work intensity were the mean number of postoperative visits, mean visit duration, and the mean number of procedures a patient underwent in each group.
By all measures of work intensity, the postoperative care of a presbyopia-correcting IOL patient is more demanding than that of a monofocal IOL patient. Presby-IOL patients required an additional cumulative postoperative care time of 2 hours and 12 minutes during the first year after surgery. The number of postoperative visits (1.7 additional), duration per visit (8 minutes longer), and the number of procedures (1.2 additional) were significantly higher in the presby-IOL group than in the monofocal IOL group.
Presbyopia-correcting lenses can cause some compromise in quality of vision to achieve an increased range of vision.2–5 These lenses may be associated with an increased incidence of visual phenomena such as glare, halos and blurry vision.2–5 Gibbons et al (2016) reviewed charts from 74 eyes of 49 patients who presented to the Bascom Palmer Eye Institute for dissatisfaction after multifocal IOL implantation.4 The most common complaint was blurry vision both for distance and near (68%). Complaints were most frequently attributed to residual refractive error (57%) and dry eye (35%). Corneal laser vision correction was done in 8% of eyes, while 7% of eyes underwent IOL exchange. The additional testing, we found in the presby-IOL group may reflect greater attention to correcting any source of degradation of quality of vision. The 29 refractive procedures performed in the presby-IOL group were done for treatment of residual refractive error. Quality of vision with presbyopia-correcting lenses is more affected by small degrees of posterior capsular opacification as compared with standard monofocal lenses.2 This likely explains the higher incidence of 62 Nd:YAG capsulotomies in the presby-IOL group as compared to the 9 in the monofocal IOL group.
To our knowledge, our study is the first that attempts to quantify the postoperative time and effort required to perform presbyopia-correcting cataract surgery. In this study, we measured only postoperative work. Oshika and colleagues studied preoperative work and found that multifocal IOL patients require 64 minutes of preoperative chair time, compared to 32 minutes for monofocal IOLs.8 There can also be additional intraoperative work in implanting a presbyopia-correcting IOL, such as femtosecond laser treatment, precise centration of the IOL on the visual axis, toric axis alignment, and intraoperative aberrometry. This study did not assess the contribution of the additional preoperative and intraoperative work to the higher work intensity for presby-IOLs.
This study likely underestimates the difference in work intensity postoperatively when comparing standard cataract surgery to presbyopia correcting cataract surgery. Fifty-three additional Nd:YAG capsulotomies were performed in the presby-IOL group. Approximately half of the participating study sites performed Nd:YAG capsulotomies in a surgery center, for which the corresponding time spent on the procedure was not recorded in the practices’ EHR systems. This may also be true for other procedures, such as refractive enhancements and IOL exchanges. In addition, it is not uncommon for practices to provide a higher level of service to presby-IOL patients by giving them preferential treatment in clinic flow. While we did not study this, one could hypothesize that the actual time required for postop care of presby-IOLs would be greater than measured. For both of these reasons, the difference in postoperative care time between the groups is likely greater than the data indicates.
This study is retrospective. While prospective randomized studies generally provide more reliable data, that may not be the case in studying postoperative work intensity. It is impossible to blind surgeons and staff to the IOL implanted without impairing care. In a prospective study, it is possible that surgeons and staff would be biased by the knowledge that the patient is enrolled in a study of time and work and treat patients with presby-IOLs differently than they normally would. Since our study was done with a retrospective chart review, the care intensity of patients was unaffected by this source of bias.
In real-world clinical settings, some patients may have a presby-IOL in one eye and a monofocal IOL in the other. In this study, we included only bilateral cases in which both eyes had the same type of IOL (presby-IOL or monofocal IOL) implanted to avoid mixing different postoperative regimens. We required the two eyes to have surgery within one month to ensure that most of the postoperative care would be completed within a year of the first eye surgery. To minimize bias, the exclusion of ineligible case records was based only on the intra- and pre-operative conditions, not postoperative findings. Consecutive cases were selected for inclusion.
The calculation of precise time in the office was critical to this study. Even with the use of EHR time-stamp records, variations in practice patterns can make a multicenter study vulnerable to an error on this measure. Additionally, the common practice of a surgeon or technician reviewing and then “closing the charts” for a group of patients all at once can complicate the calculation of time spent. To avoid errors or bias in the calculation of time, four time-stamp data points were collected: The time when the patient arrived in the office; the time the patient was picked up from the waiting room by the technician; the time the patient was sent to the front desk after finishing in the clinic; and time when the patient left the office. When analyzing the duration of the visit, our first preference was to use the time elapsed between when the patient was picked up from the waiting room and when the patient was sent to the front desk after finishing in the clinic. If for any reason these time-points were not available, the time when the patient arrived in or left the office was used. There was no statistically significant difference between the two IOL groups in the frequency of methods used to calculate visit duration, suggesting that the method of calculating visit duration did not skew the data in one direction or another.
We found that presby-IOL patients require significantly more care than monofocal IOL patients, and this difference is greater after Day 90 than in the first 90 days. This may occur because surgeons wait until they perceive healing and neuroadaptation to be complete before taking a more intensive, interventional approach to managing patient complaints regarding potential sources of visual degradation.
Conclusion
To summarize, we found that patients bilaterally implanted with presbyopia-correcting IOLs require significantly more clinic time, more diagnostic testing and additional procedures during the first postoperative year as compared with patients implanted with bilateral monofocal IOLs. The present study helps to give providers a reasonable assessment of the potential additional post-operative care involved in meeting patients’ needs throughout their post-operative course.
Abbreviations
AECOS, American European Congress of Ophthalmic Surgery; IOLs, intraocular lenses; Nd:YAG, Neodymium-doped yttrium aluminium garnet; CMS, Centers for Medicare and Medicaid Services; FDA, Food and Drug Administration; EDOF, extended depth of focus; COVID, coronavirus disease; HER, electronic health record; CPT, current procedural terminology; LASIK, laser-assisted in situ keratomileusis; GEE, Generalized Estimating Equations; OCT, Optical Coherence Tomography.
Data Sharing Statement
The data used to support the findings of this study are included within the article. Clarifications or additional data used to support the findings of this study may be requested from the corresponding author.
Acknowledgments
- AECOS Postoperative Care Study Group: Bala Ambati, MD; Stephen Bylsma, MD; John Doane, MD; Eric Donnenfeld, MD; Gary Foster, MD; Damien Goldberg, MD; Tyrie Jenkins, MD; Mark Kontos, MD; Kathleen Leone, MD; Beeran Meghpara, MD; Tim Page, MD; Jay Pepose, MD; Maria Scott, MD; Jonathan Solomon, MD; William Wiley, MD; Blake Williamson, MD; Elizabeth Yeu, MD.
- The research, statistical, and editorial assistance was provided by Raman Bedi, MD (IrisARC - Analytics, Research & Consulting, Chandigarh, India) and Jan Beiting (Wordsmith Consulting, Cary, North Carolina, USA) for the preparation of this manuscript.
Funding
The study was supported by the American European Congress of Ophthalmic Surgery (AECOS) and an investigator-initiated grant from Alcon, Inc.
Disclosure
RKM is a consultant to Johnson and Johnson Vision, LENSAR, and Presbia, and an equity/stock holder of RxSight, Stroma Medical and Percept; He is also a consultant for and paid in stock options by Horizon Surgical. JD is a consultant to Zeiss and RxSight. RW is a consultant to Alcon, Bausch and Lomb, Johnson and Johnson Vision, LENSAR, and Zeiss; He also reports personal fees from Eye Point Pharma, Beyeonics, Visus (with ownership interest), BVI, Trefoil, and RxSight (with ownership interest). KED is a consultant to Alcon, Johnson and Johnson, Bausch and Lomb and Zeiss.
References
1. Xu C. Successful premium multifocal IOL surgery: key issues and pearls. Curr Cataract Surg Techniques. 2021;133.
2. Woodward MA, Randleman JB, Stulting RD. Dissatisfaction after multifocal intraocular lens implantation. J Cataract Refract Surg. 2009;35(6):992–997. doi:10.1016/j.jcrs.2009.01.031
3. Abdelghany AA, Alio JL. Surgical options for correction of refractive error following cataract surgery. Eye Vis. 2014;1:2. doi:10.1186/s40662-014-0002-2
4. Gibbons A, Ali TK, Waren DP, Donaldson KE. Causes and correction of dissatisfaction after implantation of presbyopia-correcting intraocular lenses. Clin Ophthalmol. 2016;10:1965–1970. doi:10.2147/OPTH.S114890
5. Mamalis N. Complications of multifocal intraocular lenses: what have we learned? J Cataract Refract Surg. 2021;47(10):1256–1257. doi:10.1097/j.jcrs.0000000000000777
6. Henderson B, Sharif Z, Geneva I. Presbyopia correcting IOLs: patient selection and satisfaction. In: Intraocular Lens Surgery: Selection, Complications, and Complex Cases. New York, NY: Thieme Medical; 2015:72–77.
7. Centers for Medicare & Medicaid Services. Global Surgery Data Collection. Data collection on resources used in furnishing global services. Available from: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/Global-Surgery-Data-Collection-.
8. Oshika T, Bissen-Miyajima H, Nonaka T. Comparison of preoperative chair time between monofocal and multifocal intraocular lenses. J Cataract Refract Surg. 2022;48(5):632–633. doi:10.1097/j.jcrs.0000000000000828
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.