Back to Journals » Cancer Management and Research » Volume 13
Women’s Satisfaction with Cervical Cancer Screening Services and Associated Factors in Maternal Health Clinics of Jimma Town Public Health Facilities, Southwest Ethiopia
Authors Atnafu T, Daka DW ![]() , Debela TF
, Debela TF ![]() , Ergiba MS
, Ergiba MS ![]()
Received 1 July 2021
Accepted for publication 24 September 2021
Published 7 October 2021 Volume 2021:13 Pages 7685—7696
DOI https://doi.org/10.2147/CMAR.S327369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Tigist Atnafu,1 Dawit Wolde Daka,2 Tilahun Fufa Debela,2 Meskerem Seboka Ergiba2
1Department of Planning, Monitoring and Evaluation, Jimma Medical Center, Jimma, Ethiopia; 2Department of Health Policy and Management, Jimma University, Jimma, Ethiopia
Correspondence: Dawit Wolde Daka Email [email protected]
Background: Despite the existence of proven interventions for cervical cancer, low coverage and uptake of existing screening and treatment services remains the main challenge to prevention and control of cervical cancer in developing countries. This study aimed to assess women’s satisfaction with cervical cancer screening services and factors associated with it in public health facilities of Jimma town, Southwest Ethiopia.
Methods: A facility-based cross-sectional study was conducted from March 20 to May 20, 2020. All women aged between 30 and 49 years who visited health facilities during the data collection period were interviewed consecutively. Composite variables were computed from existing data for satisfaction, knowledge, and attitude. A 95% confidence interval was constructed for all outcome variables and multivariate logistic regression was used to identify predictors of satisfaction.
Results: Out of 205 interviewed women, 41% (95% CI: 34– 47) were satisfied with cervical cancer screening services. One-hundred and seventeen (57%, 95% CI: 50– 64) women had good comprehensive knowledge of cervical cancer screening and 121 (59%, 95% CI: 52– 66) had favorable attitude. Satisfaction with cervical cancer screening service was statistically associated with occupational status, religion, perceived length of waiting time to see a provider, and knowledge of cervical cancer.
Conclusion: Satisfaction with cervical cancer screening services was low in public health facilities of Jimma town. Slightly more than half of women had good knowledge and favorable attitude regarding cervical cancer screening. Among the clinical factors, only perceived length of waiting time to see a provider and women’s knowledge of cervical cancer were statistically associated with satisfaction with screening services. Therefore, efforts should be made to improve level of satisfaction, knowledge and attitude of women toward cervical cancer and screening services.
Keywords: satisfaction, knowledge, attitude, cervical cancer screening, Ethiopia
Introduction
Cervical cancer remains a major public health problem worldwide, ranking as the fourth most common cancer in women after breast cancer, colorectal cancer, and lung cancer. The global estimated age-standardized incidence rate (ASIR) of cervical cancer is 13.1 per 100,000 women and the rate varies among countries with a range of 2 to 75 per 100,000 women. In 2018 alone, there were 570,000 cases and 311,000 deaths worldwide, an increase of 8% in cases and 13% in deaths from 2008. The majority of cervical cancer cases and deaths (84 to 90%) occur in low- and-middle income countries including South Africa, India, China, and Brazil. Cervical cancer was the leading cause of cancer-related death of women in eastern, western, middle, and southern Africa. It continues to affect middle-aged women particularly in low resource settings.1–3
Primary and secondary prevention of cervical cancer has been found to be an effective strategy in averting deaths attributed to it. Human papillomavirus vaccines (HPV) and early screening services followed by treatment of precancerous lesions are effective strategies. These measures are believed to attain Sustainable Development Goal target 3.4 which states “one-third mortality reduction from non-communicable diseases in 2030” through implementing World Health Organization 90-70-90 target related to cervical cancer. The 90-70-90 target aimed to reduced ASIR of cervical cancer to less than 4 per 100,000 women worldwide by vaccinating 90% of all girls by age 15 years, screening 70% of women twice in the age range of 35–45 years, and treating at least 90% of all precancerous lesions detected during screening.1,4–7
The various screening methods recommended by World Health Organization are pap smear test, visual inspection of the cervix with acetic acid (VIA) or Lugol’s iodine (VILI), and HPV testing. VIA is highly effective and affordable as a primary screening method for low resource settings.4,6
The low coverage of screening services coupled with low uptake by women are hindering efforts toward reducing mortality caused by cervical cancer in most developing countries.8,9 Acceptability of screening services is low and vary widely across the different countries. In Ethiopia, the age standardized incidence rate of cervical cancer was 18.9/100,000 women10 and mortality from cervical cancer was estimated as 18.4/100,000 women.11,12 Cervical cancer is a major cause of mortality and morbidity of women aged 15–49 years. Uptake of cervical cancer screening services among eligible women was 13.46%12 and among HIV-positive women was 18.17%.13 Knowledge of cervical cancer and screening, history of multiple sexual partners, perceived susceptibility to cervical cancer, getting advice from health care provider, women’s educational level, and women’s attitude toward cervical cancer and screening were determinants of cervical cancer screening service uptake.12–14
Assessing satisfaction of women with cervical cancer and screening services has paramount importance programmatically. Hence, this study primarily aimed to examine women’s level of satisfaction with cervical cancer screening services and factors affecting it in public health facilities of Jimma town, Southwest Ethiopia. It also assessed knowledge and attitude of women toward cervical cancer and screening services.
Methods
Study Setting and Period
The study was conducted in public health facilities of Jimma town administration. Jimma town is located 354 Km Southwest of Addis Ababa, the capital city of Ethiopia. Jimma town is one among the town administrations in Oromia region. In the town administration there were a total of 6 public health facilities (2 hospitals and 4 health centers) and more than 15 private clinics. Out of these, cervical cancer screening services were provided in two public health facilities (Jimma Medical Center and Jimma health center) and two other non-governmental organization clinics (Marie stope international clinic and family guidance association clinic).
Jimma Medical Center is one of the specialized referral hospitals in Ethiopia. It provides health services to the town and surrounding community, and teaching services to medical and health science students. Cervical Cancer Screening services using VIA approach was introduced in the health facilities of Jimma town in 2016. The service was provided free of charge. The study was conducted from March 21 to May 20, 2020.
Study Design and Participants’ Selection
Facility-based cross-sectional study was conducted. All women aged between 30–49 years who had visited and received VIA services during the data collection period were eligible. Women who were critically ill were excluded from the study. We consecutively interviewed all women who met the eligibility criteria in both public health facilities.
Data Collection
A structured data collection questionnaire was used. The questionnaire comprised sections such as women’s background characteristics, reproductive history, service characteristics, knowledge and attitude toward cervical cancer screening and satisfaction with services. The data collection questionnaire was adapted through review of relevant literature.12,15–18 Satisfaction with services was measured using a total of 14 items with Likert scale ranging from strongly dissatisfied to strongly satisfied. The questionnaire was originally prepared in English and then translated to local languages (Afan Oromo and Amharic) by experienced translators. A pretest was conducted in another hospital located around 70 Km from Jimma town.
Four data collectors who are health professionals with a qualification of degree and above were recruited and participated in data collection. Another health professional with similar qualification participated as supervisor. All data collectors and supervisors were previously trained on cervical cancer screening with VIA and had a minimum of one year experience in the service. Two-day training was given to data collectors and supervisor on research objectives, data collection instruments, data collection techniques, interview skills, ethical issue, how to manage the data collection process, and the mechanisms to monitor the quality of data.
Data were collected from each woman during their exit from services after obtaining their consent. The supervisor closely monitored the data collection process at field level and provided feedback to data collectors.
Data Processing and Analysis
The completeness and consistency of data values were checked. Paper-based data were entered into Epidata version 3.1 and exported to SPSS version 25.0 for analysis. Data cleaning was done through running frequencies and coding of data variables was done as appropriate.
Data analysis progressed in the following way in which primarily we descriptively analyzed and presented women’s characteristics, an outcome variable and other explanatory variables. Mean value was used as a cut-off point to categorize women as satisfied and dissatisfied on each item (women who scored greater than or equal to mean value were categorized as satisfied).
The main outcome variable was satisfaction with cervical cancer screening services and secondary outcome variables were knowledge and attitude. The main outcome variable (satisfaction with cervical cancer screening services) was measured using 14 satisfaction items each containing a five-point Likert scale (1=strongly dissatisfied, 2=dissatisfied, 3=neutral, 4=satisfied, 5=strongly satisfied) and two more items asking questions related to “women’s willingness to continue treatment if tested positive” and “women’s willingness to recommend cervical screening services to relatives or another family member”. Using demarcation threshold formula [(Total highest score - Total lowest score)/2] + Total lowest score; primarily we categorized women into two categories as dissatisfied (below cut-off value) and satisfied (above cut-off value) based on the 14 satisfaction items. Women who scored 42 points out of the total satisfaction measuring score and who showed agreement on the two additional items were categorized as satisfied. Whereas those women who scored less than 42 points and did not show agreement on the two additional items were grouped as dissatisfied.
Knowledge of cervical cancer was measured using 16 items and three main categories: knowledge of preventability of cervical cancer (1 item); knowledge of risk factors (7 items) and knowledge of symptoms (8 items). The knowledge responses were coded as: “1=Yes and 0=No”. We computed the sum of the 16 scored items. Women who correctly responded to knowledge items above the median value (≥4.0) were classified as having “GOOD Knowledge” and those who responded less than the median value (<4.0) were categorized as having “POOR Knowledge”.
Attitude was measured using 14 items each containing 5-point Likert scale alternatives (1=strongly disagree, 2=disagree, 3=neutral, 4=agree, 5=strongly agree). Each of the attitude items were recoded as “1=strongly agree”, “1=agree”, “0=not sure or undecided”, “0=disagree” and “0=strongly disagree”. We computed the sum of 14 scored items. Women who responded to attitude items above the median value (≥7.0) were categorized as having “FAVORABLE Attitude” and less than median value (<7.0) as “UNFAVORABLE Attitude”.
We computed a 95% confidence interval to the outcome variable and some of the explanatory variables.
Bivariate logistic regression was used to identify associated and candidate variables to multivariate logistic regression analysis. In the multivariate logistic regression, P-value<0.05 and 95% confidence interval were used to declare the presence of statistically significant associations between main outcome variable and explanatory variables.
Ethical Consideration
Research ethical clearance was obtained from Jimma University Institute of Health research ethics committee (Reference number: IRB00051, March 2020). The research was conducted according to the Declaration of Helsinki. The research aim, benefits, and risks were explained to each research participant. Following this, written informed consent was obtained from participants. No personal identifiers were recorded and codes were used on each questionnaire. Paper-based data were kept in a locked cabinet and computer-based data were secured with confidential password. Research data will only be used for the intended aim and not shared with a third person.
Results
Socio-Demographic, Economic, and Reproductive Characteristics of Women
A total of 205 women in the age range of 30–49 years participated in the study. The average age of women was 35 years (SD 4.3). The majority of women were in the age range of 30–34 years (48%) followed by 35–39 years (37%). More than three-fourths (78%) of women were married and half (52%) of them were Muslim religion followers. More than one-third of women had secondary (38%) and tertiary (35%) educational status, and the majority (77%) of women were urban residents.
Regarding the reproductive history, six out of ten women had 2–4 children (62%) and one sexual partner in their life time (61%). Slightly more than one-third (34%) of women had life history of sexually transmitted infections (STI) and one in ten of them (12%) had family history of cervical cancer. More than two-thirds (72%) of women had ever used modern contraceptive methods and 83% ever heard about cervical cancer. Their main source of information of cervical cancer was health professionals (43%) followed by television (32%).
In the health facilities, more than half of women perceived that the length of waiting time to get medical records was “medium” (54%) and the length of time to see a provider was “long” (55%). Average length of waiting time to see a provider was 25 minutes (SD 20). Whereas, nearly six in ten (59%) women perceived that the length of consultation time with provider was “medium”. Nine in ten (89%) women had received health education on cervical cancer during their current visit to the study health facilities (Table 1).
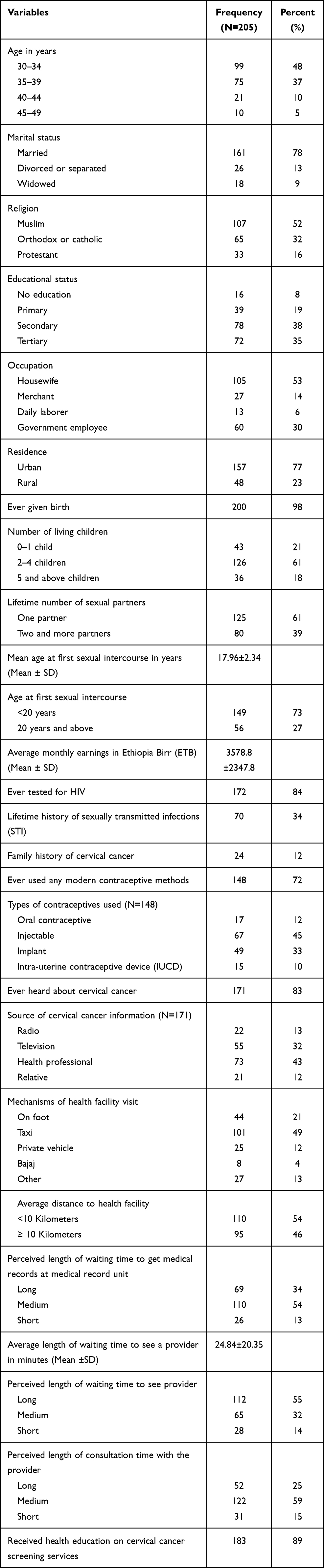 |
Table 1 Characteristics of Women at Public Health Facilities of Jimma Town, Southwest Ethiopia, 2020 |
Knowledge and Attitude
Only 17% of women knew that cervical cancer was preventable. Less than half of women had knowledge of the main risk factors of cervical cancer including having multiple sexual partners, previous family history of cervical cancer, smoking, STI, oral contraceptives and initiation of early sexual intercourse. One-third of women (31%) had replied that cervical cancer has no symptoms. Overall, 57% (95% CI: 50–64) of women had comprehensive, good knowledge of the risk factors and symptoms of cervical cancer (Table 2).
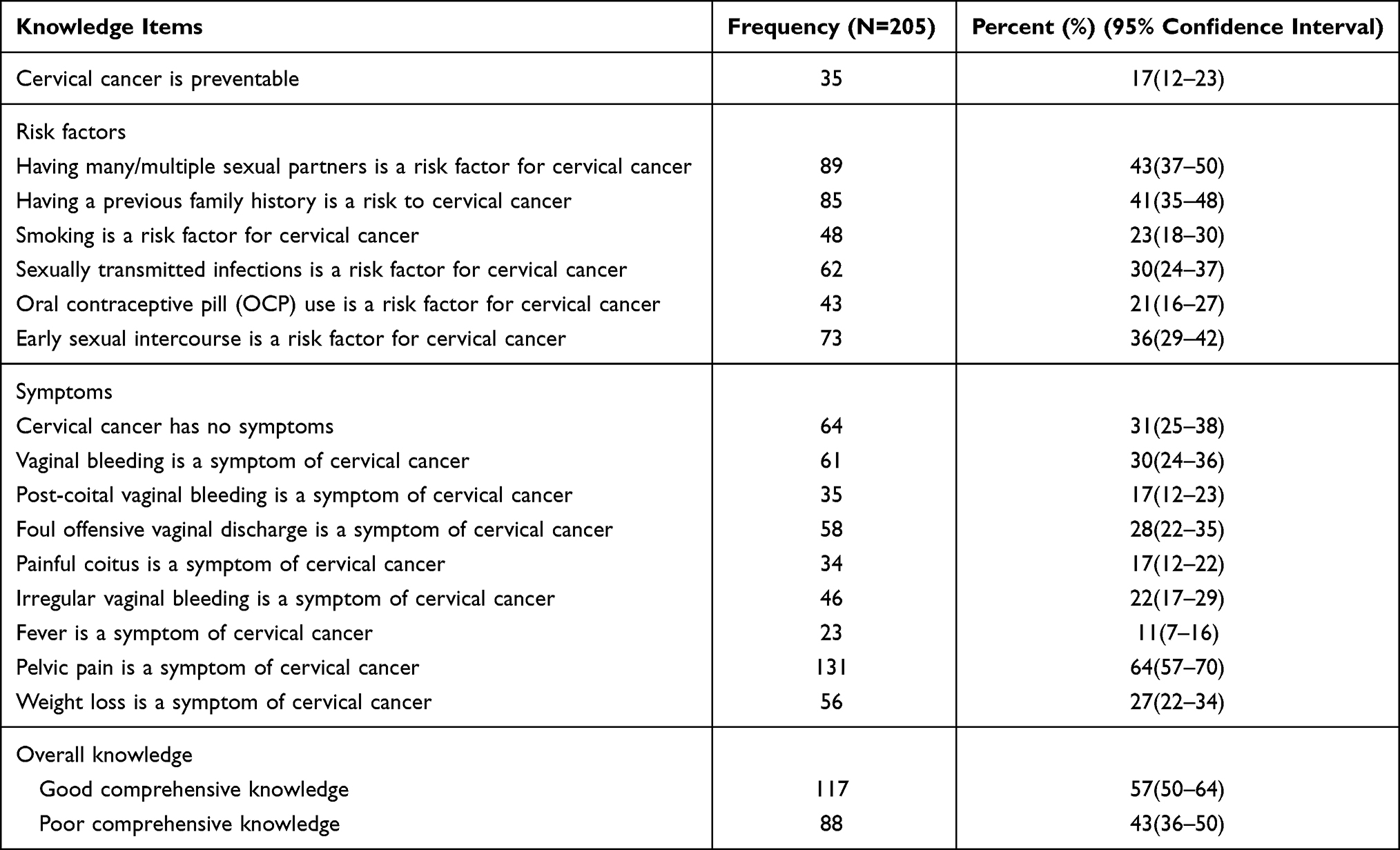 |
Table 2 Knowledge of Women of the Risk Factors and Symptoms of Cervical Cancer at Public Health Facilities of Jimma Town, Southwest Ethiopia, 2020 |
More than six out of ten women (64%) believed that they were too old to have cervical cancer examination regularly, and nearly six out of ten (59%) women thought that cervical cancer threatens their relationships and having cervical cancer exam was painful, respectively. Half of women were ashamed to sit or lie down on a gynecologic examination table and 56% of them preferred a female health worker for cervical cancer exams. Overall, nearly six in ten (59%, 95% CI: 52–66) women had favorable attitude toward cervical cancer and screening services (Table 3).
 |
Table 3 Attitude of Women toward Cervical Cancer and Screening Services at Public Health Facilities of Jimma Town, Southwest Ethiopia, 2020 |
Satisfaction
More than six out of ten women were satisfied with the clarity of provider explanation about cervical cancer, their interaction with providers, overall services provided, explanation given by provider on problem and the services given, VIA screening test experience, and consultation time with provider with satisfaction rate ranging from 60% to 69%. Eighty-two percent of women wanted to continue treatment if VIA tested positive and most (96%) of them recommended that relatives and others attend screening services given at the health facilities. The overall satisfaction of women with cervical cancer screening services was 41% (95% CI: 34–47) (Table 4).
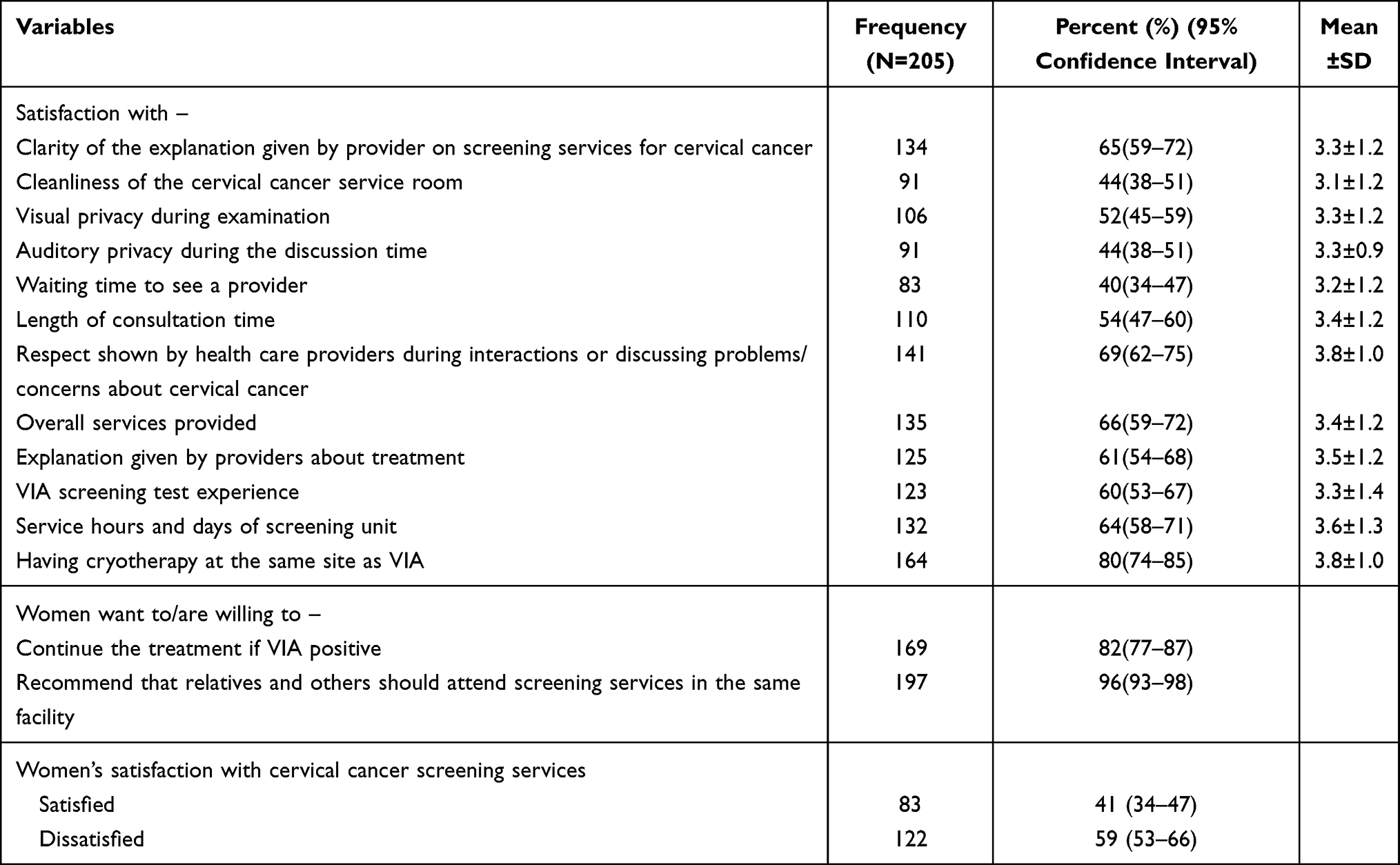 |
Table 4 Satisfaction of Women with Cervical Cancer Screening Services at the Public Health Facilities of Jimma Town, Southwest Ethiopia, 2020 |
Factors Associated with Satisfaction
In the bivariate logistic regression, marital status, educational status, occupation, religion, age at first sexual intercourse, ever heard about cervical cancer, distance from health facility, length of waiting time to get medical records, length of time to see provider, length of consultation time and knowledge of cervical cancer were candidate variables for multiple variable logistic regression with P-value<0.25. In the multivariate logistic regression, occupational status, religion, perceived length of waiting time to see care provider, and knowledge of cervical cancer were significantly associated with women’s satisfaction with cervical cancer screening services.
The interpretation of statistically significant explanatory variables follows. Satisfaction with cervical cancer screening services was 74% (AOR=0.26;95% CI 0.09–0.79) less likely among women who were merchants compared to housewives. The odds of cervical cancer screening service satisfaction were three times more likely among protestant women than Muslim women (AOR=3.04; 95% CI 1.09–8.51). Satisfaction with cervical cancer screening services was nearly three times (AOR=2.90; 95% CI 1.36–6.20) more likely among women who perceived length of waiting time to see a provider as “medium” compared to those who perceived the waiting time as “long”. The odds of screening service satisfaction were 53% (AOR=0.47; 95% CI 0.23–0.97) less likely among women who had good knowledge of cervical cancer compared to those who had poor knowledge (Table 5).
 |
Table 5 Factors Associated with Women’s Satisfaction with Cervical Cancer Screening Services at Public Health Facilities of Jimma Town, Southwest Ethiopia, 2020 |
Discussion
The study has shown that overall satisfaction with cervical cancer screening and follow-up services among women aged 30–49 years was 41%. More than half of women had good comprehensive knowledge and favorable attitude toward cervical cancer screening. In this study, occupational status, religion, perceived length of waiting time to see a provider, and knowledge of cervical cancer were identified as predictors of women’s satisfaction with cervical cancer screening services. We found no evidence that women’s level of satisfaction with the cervical cancer screening services was associated with attitude toward cervical cancer.
The level of satisfaction reported in the study area was lower than in other studies done in different parts of the world.16–21 The variation may be related to the contextual differences and the satisfaction components considered. In the study area, majority of women were willing to continue treatments if tested positive and recommended cervical cancer services to relatives or parents. The least satisfaction was related to service accommodation and convenience which was consistent with the finding reported in another study.21 Patient satisfaction is an important determinant of service uptake, adherence, and retention. It is also an important health system outcome. Poor satisfaction with available services will result in patients having a low level of trust in services and thus, low uptake and poor outcomes.22
Greater than half of women had good comprehensive knowledge of signs and symptoms, and risk factors of cervical cancer. This finding was better than that of a study conducted in Nigeria,23,24 India,25 and Nepal26 and lower than that of a study conducted in Zimbabwe27 and Democratic People’s Republic of Korea.28 The finding was also better than that of a study conducted in Adigrat town, Northern Ethiopia (46.4%), Wolayita zone hospitals (43.1%), and Gondar town, Northern Ethiopia (19.9%)15,29,30 and comparable to a study conducted in Hadiya zone, Southern Ethiopia (53.7%).31 Similarly, more than half of women had favorable attitude toward cervical cancer screening and this finding was comparable to a study done in Adigrat, Northern Ethiopia30 and higher than that of a study conducted in Wolayita zone hospitals, Southern Ethiopia (45.5%).29 The variations in the study findings might be due to contextual differences, difference in period of assessments, and knowledge and attitude components considered in the analysis. But, the findings implied that a significant proportion of women had poor comprehensive knowledge and unfavorable attitudes toward cervical cancer and related services. Better knowledge and favorable attitude toward cervical cancer screening are important factors for appropriate utilization of screening and treatment services. Women knowledge and attitude towards cervical cancer and screening services was positively associated with uptake of cervical cancer screening services.32,33 Lack of awareness of cervical cancer disease and screening services is a factor in delayed diagnosis of cervical cancer34,35 and thus, leads to advanced stage of illness during diagnosis.
There was statistically significant association between socio-demographic and economic factors (religion and occupational status) and women’s satisfaction with cervical cancer screening services. Satisfaction with cervical cancer screening services was three times more likely among protestant women compared to Muslim women and the odds of satisfaction were 74% less likely among merchant women compared to housewives. The relationship between satisfaction and socio-demographic/economic factors was reported by other studies elsewere.36,37
The study finding also indicated a significant association between service characteristics (length of waiting time to see a provider) and women’s satisfaction with screening services. Women who perceived waiting time as “medium” were nearly three times more likely to be satisfied than women who perceived waiting time as “long”. This implied that as the length of waiting time increases, women’s satisfaction declines. This finding was consistent with other studies.20,38,39 In our study, perceived length of waiting time to get medical records, perceived length of consultation time with a provider, and distance from health facility were associated with women’s satisfaction in the univariate analysis. However, these factors did not maintain the association in the multivariate analysis after controlling for confounding variables. In another study, distance from home to health facility was significantly associated with women’s satisfaction.20
Women’s knowledge of cervical cancer was significantly associated with their satisfaction with cervical cancer screening services in that women with good comprehensive knowledge were less satisfied with screening services compared to women with poor comprehensive knowledge. This might be because the women with more knowledge may expect more from services and any mismatch with their expectations will lead to less satisfaction compared to women with less knowledge about screening services. This finding was comparable to another study.20
In this study marital status, educational status, age at first sexual intercourse, and ever heard about cervical cancer were associated with women’s satisfaction with cervical cancer screening services in the univariate analysis only. Whereas, remaining variables including attitude did not show any associations in the univariate and multivariate analysis.
The study assessed women’s satisfaction with cervical cancer screening services considering a variety of components. It has also provided evidence on comprehensive knowledge and attitude of women regarding cervical cancer and screening services. The study has several limitations. The study included only women who had visited health facilities in the study period and thus, we were unable to capture the characteristics and satisfaction of women who were outside of health care settings. Interviews with women were conducted at health care settings and hence satisfaction surveys may be prone to response bias as a result of social desirability affected by the characteristics of interviewers. But, we used data collectors outside of the study area and this may have minimized response bias. All of the health facilities in the town were included in the study, however, participants were not selected randomly and it would be difficult to generalize findings to other settings. The findings should be interpreted with caution.
Conclusion
The study findings indicated that only four in ten women were satisfied with cervical cancer screening services in the public health facilities of Jimma town. Greater than half of women had comprehensive knowledge of the signs and symptoms, and preventive and treatment measures of cervical cancer. Though the majority of women expressed their willingness to continue treatments if VIA tested positive, and agreed to recommend that relatives and partners should attend screening services in the same health facility, slightly higher than half of them had favorable attitude toward screening services. The study also revealed that religion, occupational status, perceived length of waiting time to see a provider, and knowledge of cervical cancer risk factors and symptoms were predictors of women’s satisfaction.
Satisfaction is an important determinant for service utilization and retention in care. Knowledge and attitude play huge roles in influencing proper utilization of screening services. Therefore, effort should be made to improve the quality of health services in terms of length of waiting time to see health care provider and services in the health facilities. Moreover, awareness creation programs should be created and provided to women focusing on the signs and symptoms of cervical cancer, detection and treatment measures of cervical cancer, and the step-by-step practice of cervical cancer screening. This will increase women’s attitudes toward screening services.
Data Sharing Statement
The original data of this research are available from the corresponding author in SPSS software.
Acknowledgments
We acknowledge the different levels of administrative hierarchy and study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The funder had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The authors declared that they have no competing interests.
References
1. Arbyn M, Weiderpass E, Bruni L, et al. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health. 2020;8(2):e191–203. doi:10.1016/S2214-109X(19)30482-6
2. Hull R, Mbele M, Makhafola T, et al. Cervical cancer in low and middle income countries (review). Oncol Lett. 2020;20(3):2058–2074. doi:10.3892/ol.2020.11754
3. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021:1–41. doi:10.3322/caac.21660
4. Denny L, de Sanjose S, Mutebi M, et al. Interventions to close the divide for women with breast and cervical cancer between low-income and middle-income countries and high-income countries. Lancet. 2017;389(10071):861–870. doi:10.1016/S0140-6736(16)31795-0
5. Canfell K, Kim JJ, Brisson M, et al. Mortality impact of achieving WHO cervical cancer elimination targets: a comparative modelling analysis in 78 low-income and lower-middle-income countries. Lancet. 2020;395(10224):591–603. doi:10.1016/S0140-6736(20)30157-4
6. World Health Organisation. Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem. Vol. 2. Geneva: United Nations General Assembly; 2020:1–3.
7. Stelzle D, Tanaka LF, Lee KK, et al. Estimates of the global burden of cervical cancer associated with HIV. Lancet Glob Health. 2021;9(2):e161–9. doi:10.1016/S2214-109X(20)30459-9
8. Gupta R, Gupta S, Mehrotra R, Sodhani P. Cervical cancer screening in resource-constrained countries: current status and future directions. Asian Pac J Cancer Prev. 2017;18:1461–1467.
9. Ling Y, Gravitt P, Kheng S, Wan C, Saville M. Accelerating action on cervical screening in lower- and middle-income countries (LMICs) post COVID-19 era. Prev Med (Baltim). 2021;144:106294. doi:10.1016/j.ypmed.2020.106294
10. Bruni L, Albero G, Serrano B, et al. ICO/IARC information centre on HPV and cancer (HPV information centre). Human papillomavirus and related diseases in the world. Summary Report; January 22, 2019. Available from: https://www.hpvcentre.net/statistics/reports/XWX.pdf.
11. Wondemagegnhu T. Pattern of cancer in Tikur Anbessa specialized hospital oncology center in Ethiopia from 1998 to 2010. Int J Cancer Res Mol Mech. 2015;1(1):1–5. ISSN 2381-3318. doi:10.16966/2381-3318.103
12. Ayenew AA, Zewdu BF, Nigussie AA. Uptake of cervical cancer screening service and associated factors among age-eligible women in Ethiopia: systematic review and meta-analysis. Infect Agent Cancer. 2020;15(1):67. doi:10.1186/s13027-020-00334-3
13. Mekonnen BD. Cervical cancer screening uptake and associated factors among HIV-positive women in Ethiopia: a systematic review. Adv Prev Med. 2020;15:12–15.
14. Chidyaonga-Maseko F, Chirwa ML, Muula AS. Underutilization of cervical cancer prevention services in low and middle income countries: a review of contributing factors. Pan Afr Med J. 2015;21:231. doi:10.11604/pamj.2015.21.231.6350
15. Mengesha A, Messele A, Beletew B. Knowledge and attitude towards cervical cancer among reproductive age group women in Gondar Town, North West Ethiopia. BMC Public Health. 2020;20(1):1–10. doi:10.1186/s12889-020-8229-4
16. Sansingha K, Yamarat K. Factors effecting on women satisfaction of cervical cancer screening in Roiet province, Thailand. J Health Res. 2010;24(2):51–58.
17. Kumar Y, Mishra G, Gupta S, Shastri S. Cancer screening for women living in urban slums - acceptance and satisfaction. Asian Pac J Cancer Prev. 2011;12:1681–1685.
18. Cochran CR, Kapella S. Patient satisfaction in a statewide cervical cancer screening program. J Nevada Public Health Assoc. 2005;1(2):4.
19. Clinic S, Oludele E. Clients’ Utilization and Perceived Level of Satisfactio with Services Received at the Cervical Cancer Screening clinic. Ibadan, Nigeria: University College Hospital; 2010.
20. Maseko FC, Chirwa ML, Muula AS. Client satisfaction with cervical cancer screening in Malawi. BMC Health Serv Res. 2014;14(1):420. doi:10.1186/1472-6963-14-420
21. Selmouni F, Zidouh A, Alvarez-Plaza C, El Rhazi K. Perception and satisfaction of cervical cancer screening by visual inspection with acetic acid (VIA) at Meknes-Tafilalet Region, Morocco: a Population-Based Cross-Sectional Study. BMC Womens Health. 2015;15(1):106. doi:10.1186/s12905-015-0268-0
22. Prakash B. Patient satisfaction. J Cutan Aesthet Surg. 2010;3(3):151–155. doi:10.4103/0974-2077.74491
23. Olubodun T, Odukoya OO, Balogun MR. Knowledge, attitude and practice of cervical cancer prevention, among women residing in an urban slum in Lagos, South West, Nigeria. Pan Afr Med J. 2019;32:1–10. doi:10.11604/pamj.2019.32.130.14432
24. Ahmed S, Ahmed R, Idris S, Sabitu K. Knowledge, attitude and practice of cervical cancer screening among market women in Zaria, Nigeria. Niger Med J. 2013;54(5):316. doi:10.4103/0300-1652.122337
25. Kokane AB, Bansal AP, Pakhare A, Kapoor N, Mehrotra R. Knowledge, attitude, and practices related to cervical cancer among adult women: a hospital-based cross-sectional study. J Nat Sci Biol Med. 2015;6(2):324–328. doi:10.4103/0976-9668.159993
26. Shilpakar O, Aacharya RP, Neupane RP, Karki B. Knowledge, attitude and practice (KAP) of women towards cervical cancer screening at a tertiary care institute in Kathmandu, Nepal. Nepal Med J. 2020;3(1):13–18. doi:10.37080/nmj.79
27. Mutambara J, Mutandwa P, Mahapa M, Chirasha V, Nkiwane S, Shangahaidonhi T. Knowledge, attitudes and practices of cervical cancer screening among women who attend traditional churches in Zimbabwe. J Cancer Res Pract. 2017;4(2):53–58. doi:10.1016/j.jcrpr.2017.02.001
28. Tran NT, Taylor R, Choe S
29. Tekle T, Wolka E, Nega B, Kumma WP, Koyira MM. Knowledge, attitude and practice towards cervical cancer screening among women and associated factors in hospitals of Wolaita Zone, Southern Ethiopia. Cancer Manag Res. 2020;12:993–1005. doi:10.2147/CMAR.S240364
30. Tsegay A, Araya T, Amare K, Gtsadik F. Knowledge, attitude, and practice on cervical cancer screening and associated factors among women aged 15–49 years in Adigrat Town, Northern Ethiopia, 2019: a Community-Based Cross-Sectional Study. Int J Womens Health. 2020;12:1283–1298. doi:10.2147/IJWH.S261204
31. Yitagesu H, Samuel Y, Tariku L. Knowledge, attitude and practice for cervical cancer prevention and control among women of childbearing age in Hossana Town, Hadiya Zone, Southern Ethiopia: Community-Based Cross-Sectional Study. PLoS One. 2017;12(7):181–200.
32. Chaowawanit W, Tangjitgamol S, Kantathavorn N, et al. Knowledge, attitudes and behavior of Bangkok Metropolitan women regarding cervical cancer screening. Asian Pac J Cancer Prev. 2016;17(3):945–952. doi:10.7314/APJCP.2016.17.3.945
33. Raychaudhuri S, Mandal S. Current status of knowledge, attitude and practice (KAP) and screening for cervical cancer in countries at different levels of development. Asian Pac J Cancer Prev. 2012;13(9):4221–4227. doi:10.7314/APJCP.2012.13.9.4221
34. Berhane A, Hailu T, Mulugeta A. Determinants of delayed diagnosis among pediatric cancer patients from Ayder comprehensive specialized hospital, Mekelle, Northern Ethiopia. BMC Pediatr. 2019;19(1):478. doi:10.1186/s12887-019-1848-1
35. Zeleke S, Anley M, Kefale D, Wassihun B. Factors associated with delayed diagnosis of cervical cancer in tikur anbesa specialized hospital, Ethiopia, 2019: Cross-Sectional Study. Cancer Manag Res. 2021;13:579–585. doi:10.2147/CMAR.S285621
36. Adhikari M, Paudel NR, Mishra SR, Shrestha A, Upadhyaya DP. Patient satisfaction and its socio-demographic correlates in a tertiary public hospital in Nepal: a Cross-Sectional Study. BMC Health Serv Res. 2021;21(1):1–10. doi:10.1186/s12913-021-06155-3
37. Djordjevic IM, Vasiljevic D. The effect of sociodemographic factors on the patient satisfaction with health care system. Serbian J Exp Clin Res. 2019;20(3):251–255. doi:10.1515/sjecr-2017-0042
38. Lee S, Groß SE, Pfaff H, Dresen A. Waiting time, communication quality, and patient satisfaction: an analysis of moderating influences on the relationship between perceived waiting time and the satisfaction of breast cancer patients during their inpatient stay. Patient Educ Couns. 2020;103(4):819–825. doi:10.1016/j.pec.2019.11.018
39. Camacho F, Anderson R, Safrit A, Jones A, Hoffmann P. The relationship between patient’s perceived waiting time and office-based practice satisfaction. N C Med J. 2006;1(67):409–413.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.