Back to Journals » International Journal of Women's Health » Volume 14
Women’s Risk Perceptions and Willingness to Engage in Risk-Reducing Interventions for the Prevention of Obesity-Related Endometrial Cancer
Authors Derbyshire AE, MacKintosh ML, Pritchard CM, Pontula A, Ammori BJ, Syed AA ![]() , Beeken RJ, Crosbie EJ
, Beeken RJ, Crosbie EJ ![]()
Received 17 October 2021
Accepted for publication 19 January 2022
Published 28 January 2022 Volume 2022:14 Pages 57—66
DOI https://doi.org/10.2147/IJWH.S326417
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Elie Al-Chaer
Abigail E Derbyshire,1 Michelle L MacKintosh,1 Christina M Pritchard,1 Arya Pontula,2 Basil J Ammori,3,4 Akheel A Syed,4,5 Rebecca J Beeken,6 Emma J Crosbie1,2
1Department of Obstetrics and Gynaecology, Manchester University NHS Foundation Trust, Manchester, UK; 2Division of Cancer Sciences, University of Manchester, Manchester, UK; 3Department of Surgery, Salford Royal NHS Foundation Trust, Salford, UK; 4Division of Diabetes, Endocrinology and Gastroenterology, University of Manchester, Manchester, UK; 5Department of Obesity Medicine, Diabetes & Endocrinology, Salford Royal NHS Foundation Trust, Salford, UK; 6Leeds Institute of Health Sciences, University of Leeds, Leeds, UK
Correspondence: Emma J Crosbie
Division of Cancer Sciences, University of Manchester, Manchester, UK
, Tel +44 161 701 6942
, Email [email protected]
Introduction: Endometrial cancer rates are rising in parallel with the global obesity epidemic. Our aim was to assess the willingness of women at greatest risk of obesity-related endometrial cancer to engage with risk-reducing strategies and establish perceived barriers that may preclude their participation in a randomized controlled trial of primary endometrial cancer prevention.
Materials and Methods: Women attending gynecology, obesity and sleep apnea clinics in Manchester Academic Health Sciences Centre-affiliated hospitals with obesity classes II (BMI 35– 39.9kg/m2) and III (BMI ≥ 40kg/m2) were invited to participate in a cross-sectional survey. We asked women about their perceived risk, knowledge of risk factors and willingness to engage with endometrial cancer risk-reducing interventions.
Results: Seventy-four women with a median age of 51 years (range 22– 73) and BMI of 47kg/m2 (range 34– 81) took part in the study. Two-thirds (65.6%) knew that obesity was a risk factor for endometrial cancer but few were able to recall other major risk factors. Just over half (53.5%) perceived their risk of developing endometrial cancer to be higher than average. Women were prepared to lose weight (94%), eat healthily (91%), exercise more (87%), take a pill every day (74%) or receive an intra-uterine device (49%) for primary endometrial cancer prevention. Perceived barriers included cost, forgetting, willpower, finding time, physical fitness, social anxiety, possible side effects and previous bad experiences.
Conclusion: Women at highest risk of obesity-related endometrial cancer may not always appreciate their susceptibility. However, willingness to engage in risk-reducing strategies suggests recruitment to a randomized controlled trial for primary endometrial cancer prevention could be feasible.
Keywords: endometrial cancer, obesity, risk reducing interventions, weight loss, exercise, chemoprevention, levonorgestrel-releasing intrauterine system, metformin
Introduction
Endometrial cancer is the most common gynecological cancer in the United Kingdom (UK), affecting around 9000 women every year.1 Over the past two decades, the incidence of endometrial cancer has increased, and more women are now dying of the disease despite improvements in long-term survival rates.2 This is partly because the prevalence of obesity, defined as a body mass index (BMI) of ≥30 kg/m2, has reached unprecedented levels, with around 29% of all women and 36% of those in mid to late adulthood in England now classified as obese.3,4 Obesity is the strongest risk factor for endometrial cancer,5 with every 5kg/m2 increment in BMI associated with a 60% increased risk of the disease.6 Women with obesity classes II and III (BMI 35–39.9 and ≥40 kg/m2, respectively) are at highest risk, particularly of Bokhman type I or endometrioid endometrial cancer, the most common histological subtype.7 If obesity rates remain at current levels, it is predicted that there will be additional 3700 new cases diagnosed and 850 further deaths from the disease each year in England and Wales by 2030.8
Attempts to understand the biological relationship between obesity and endometrial cancer have concluded that several influences are at play.9 An excess of endogenous estrogen synthesized from adipose tissue and unopposed by progesterone in women who are postmenopausal or who have anovulatory menstrual cycles is thought to be the major driver,7 but insulin resistance10 and a pro-inflammatory microenvironment are other key contributors.11 Advances in our understanding of endometrial carcinogenesis have prompted the proposal of several risk reducing interventions that may decrease obesity levels and/or inhibit the tumor-promoting consequences of obesity in the endometrium.12 These include bariatric surgery and diet-induced weight loss,13,14 exercise programs,15 oral or intrauterine progestins16 and metformin.17 Such risk reducing interventions may have additional health benefits, including treatment or prevention of other obesity-related conditions, such as type 2 diabetes mellitus, hypertension and ischemic heart disease, and with generally low toxicity profiles. Risk reducing interventions have yet to be tested in high quality randomized controlled trials, but their potential as primary endometrial cancer prevention tools has been suggested by laboratory, biomarker and epidemiological studies.18 If effective, and appropriately targeted at those with the greatest risk, these interventions could offer an opportunity to halt current trends in endometrial cancer rates.
Key to the success of any intervention is engagement from those likely to benefit. According to models of health behavior, knowledge of risk factors and perceived personal risk, alongside beliefs about the ability to change that risk, are important factors that influence a person’s capability and motivation to change their behavior.19 Previous work has shown that public awareness of the link between obesity and endometrial cancer risk is low,20,21 but no studies have asked women whether they are interested in reducing their endometrial cancer risk and what interventions would be acceptable to them. The aim of this study was to assess the willingness of women at greatest risk of obesity-related endometrial cancer to engage in risk-reducing strategies and to establish any barriers that may prevent their participation in a randomized controlled trial of primary prevention.
Methods
Study Participants
Women attending gynecology, obesity and sleep apnea clinics in Manchester Academic Health Sciences Centre-affiliated hospitals with obesity classes II and III (BMI ≥35kg/m2 and ≥40kg/m2) were invited to participate in this cross-sectional survey. Demographic variables (age, ethnicity) and medical history (diabetes, treated hypertension, hypercholesterolemia, obstructive sleep apnea) were recorded. Women who had previously had a hysterectomy were excluded from the study. Height was measured using a stadiometer; weight was measured using electronic scales after removal of bulky clothing, and BMI derived (kg/m2). BMI was classified according to the World Health Organisation (WHO) as obesity class I (BMI 30–34.9), class II (BMI 35–39.9) and class III (BMI ≥ 40). Waist (midpoint between lower margin of last palpable rib and top of the iliac crest, as defined by WHO, and measured with a tape measure) and hip circumference (widest portion of the buttocks) were recorded to the nearest 1 cm, and waist-to-hip ratio calculated. Blood pressure was recorded by a sphygmomanometer using a large cuff. Postcodes were used to determine socioeconomic status according to the deciles of the English Index of Multiple Deprivation 2015, with 1 the most deprived and 10 the least deprived decile.
Method of Approach
Women were approached in the waiting room prior to routine gynecology, obesity and sleep apnea clinic appointments by a member of the study team. They were provided with a participant information sheet, which gave background information about endometrial cancer, in particular its rising prevalence and the need for evidence-based primary prevention strategies. Those who agreed to participate signed a study consent form before self-completing a paper questionnaire. The questionnaire contained six items designed to assess women’s personal perception of risk, knowledge of endometrial cancer risk factors and willingness to engage with weight loss, exercise programs, oral medications and intrauterine devices for the purposes of primary endometrial cancer prevention. The six items were based on published questionnaire studies by Dillard et al22 and Stubbings et al23 that assessed cancer risk prediction and willingness to engage in risk-reducing interventions but were not specific to endometrial cancer. Question 1 asked women to indicate, “Compared to others of the same sex and age, my chances of getting womb cancer are” “much below average”, “below average”, “average”, “above average” or “much above average”, derived from Dillard et al.22 Question 2, “What things do you think affect a woman’s chance of developing womb cancer?” allowed women to write free text in the box below, and question 3 “There is not much I can do to lower my chances of getting womb cancer” followed by “strongly disagree”, “disagree”, “not sure”, “agree” and “strongly agree”, were both derived from Stubbings et al.23 Question 4 “If it would lower my chances of getting womb cancer I would be willing to … ” followed by “take a pill every day”, “have a coil fitted”, “lose weight”, “exercise more”, “eat more healthily” and choices “strongly disagree”, “disagree”, “not sure”, “agree” and “strongly agree”. Question 5 “Are there any reasons you wouldn’t want to do the following, or wouldn’t be able to do the following, to lower your chances of getting womb cancer?” with free text boxes next to each of the following “take a pill every day”, “have a coil fitted”, “lose weight”, “exercise more”, “eat more healthily”. Question 6 asked, “There are some things that can increase a woman's chance of developing womb cancer. How much do you agree that each of these can increase the chance of developing womb cancer?” followed by “not having children”, “having gone through the menopause”, “being overweight”, “being over 50 years old”, “having a close relative with womb cancer”, “having diabetes”, “doing less than 30 minutes of moderate physical activity 5 times a week” and the following choices “strongly disagree”, “disagree”, “not sure”, “agree” and “strongly agree”, adapted from Stubbings et al.23
Statistical Analysis
Data were analyzed using the statistical software package IBM Statistical Package for Social Sciences (SPSS) Version 24.0. Descriptive statistics included mean and standard deviation (SD) for normally distributed, and median and interquartile range (IQR), for non-parametric data. Free text responses were grouped into themes and scored.
Ethical Approval
All women gave written, informed consent to participate in this study. Approval was obtained from the North West Research Ethics Committee (12/NW/0050) on 23 January 2012, and the study was conducted in accordance with the Declaration of Helsinki.
Results
Seventy-four women with a median age of 51 years (range 22–73) and BMI of 47 kg/m2 (range 34–81) took part in the study (Table 1). Two thirds (65.6%) knew that obesity is a risk factor for endometrial cancer but few were able to recall other major risk factors, including those related to age, reproductive factors or genetic predisposition (Tables 2 and 3). Approximately one-fifth of participants incorrectly stated that alcohol (11.5%) and/or smoking (18%) increases endometrial cancer risk, and more than a quarter incorrectly reported that factors associated with sexual behavior, including number of partners (14.8%), history of sexually transmitted infection (4.9%), and failure to use a condom (14.8%), were important risk factors. Just over half of the women (53.5%) believed that their personal endometrial cancer risk was higher than average (Table 4). Women were prepared to lose weight (94%), eat healthily (91%), exercise more (87%), take a pill every day (74%) or receive an intra-uterine device (49%) for primary endometrial cancer prevention. Perceived barriers included willpower, finding time, poor general health, possible side effects and previous bad experiences (Table 5).
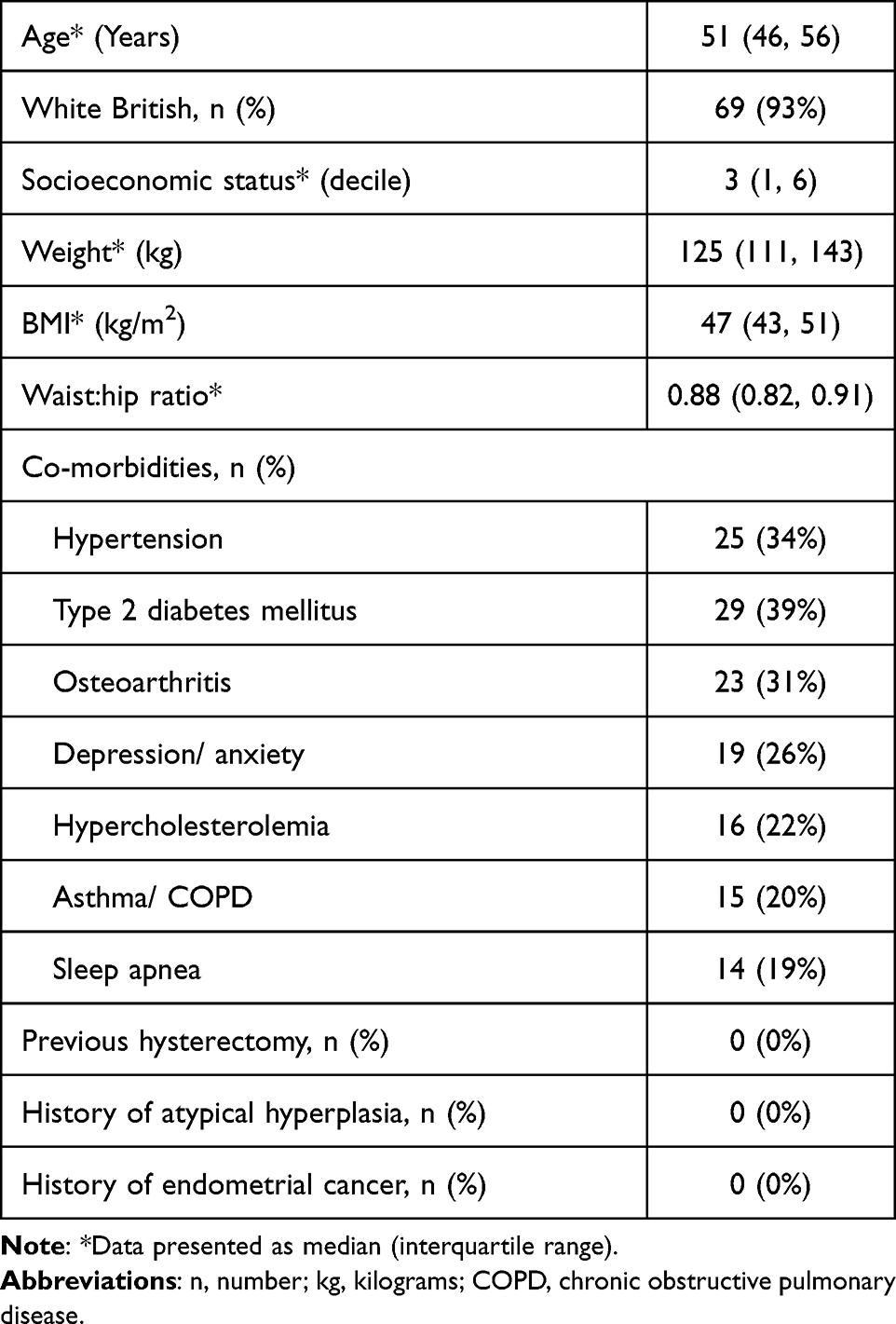 |
Table 1 Study Population Characteristics |
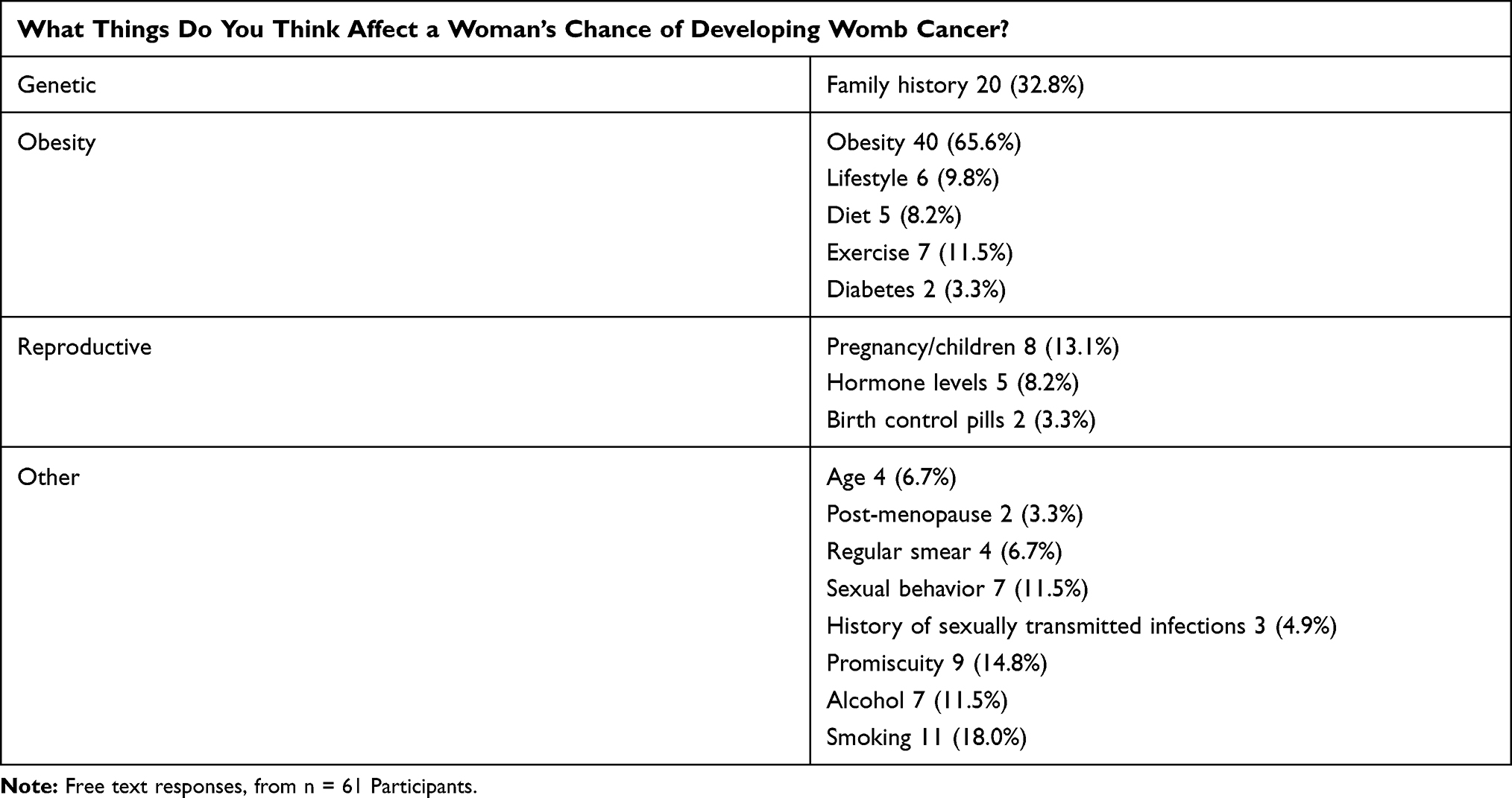 |
Table 2 Recall of Endometrial Cancer Risk Factors |
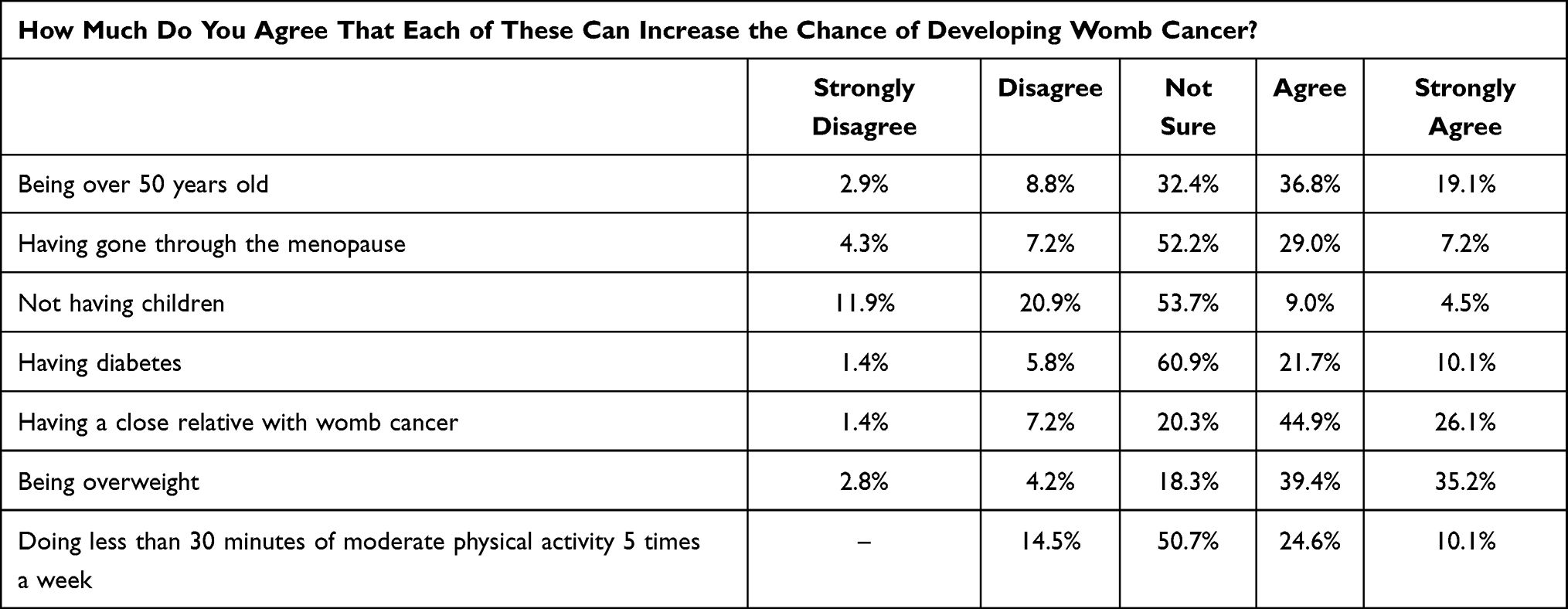 |
Table 3 Recognition of Endometrial Cancer Risk Factors |
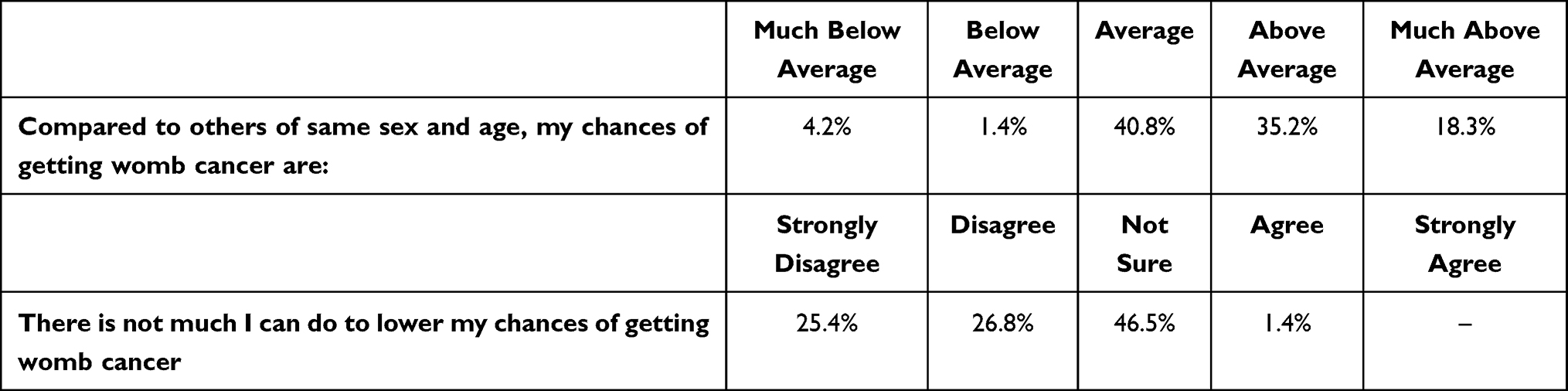 |
Table 4 Perceived Personal Risk and Opportunities to Reduce Risk of Endometrial Cancer |
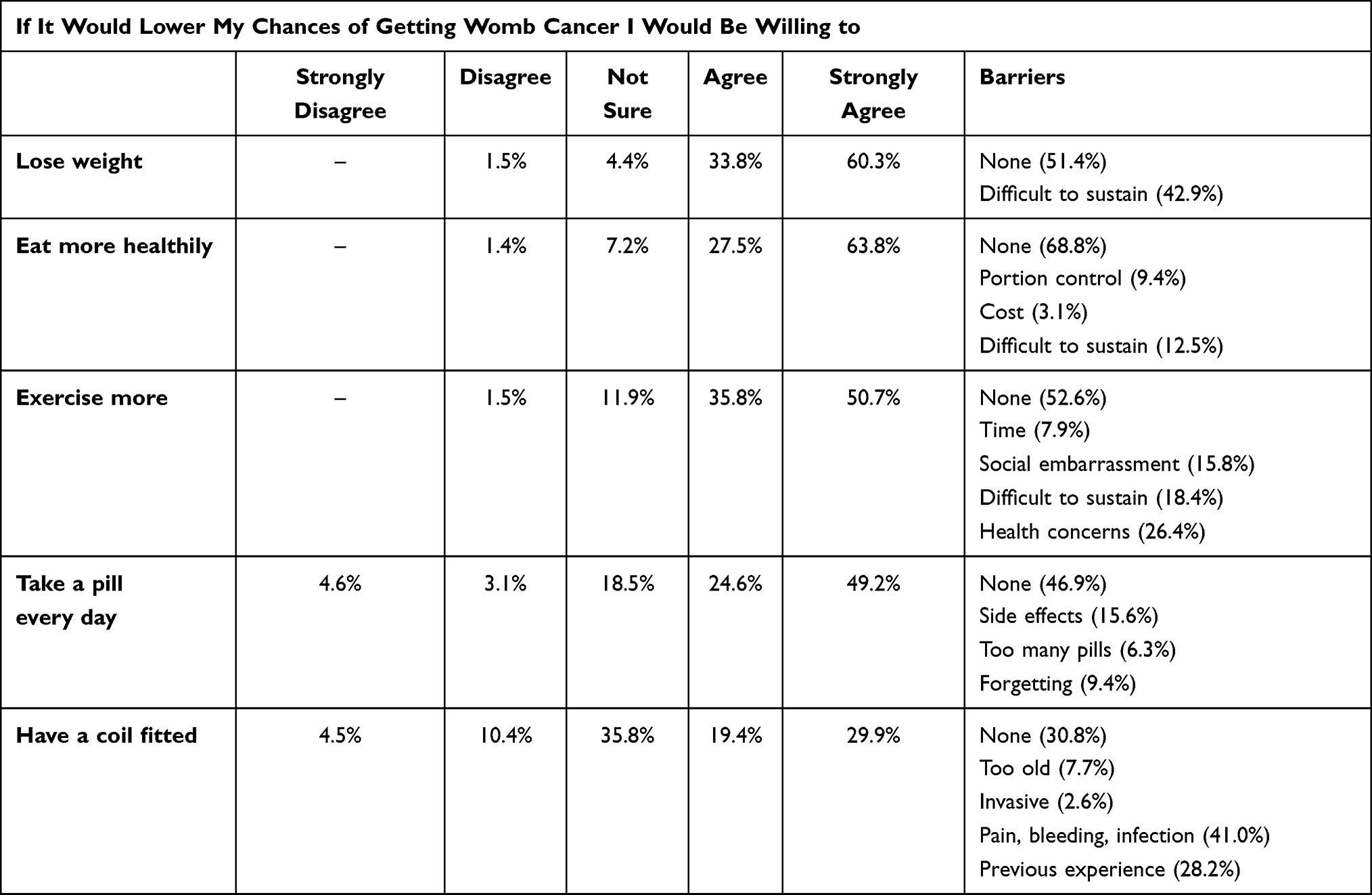 |
Table 5 Willingness to Engage in Endometrial Cancer Risk-Reducing Interventions and Perceived Barriers |
Discussion
In this study, the majority of women with obesity classes II and III knew obesity was a risk factor for endometrial cancer, but just over half perceived themselves to be at higher risk. This discrepancy may be due to a lack of self-awareness. Most women stated that they would try to change their weight management behaviors, take tablets and/or receive an intra-uterine device to reduce their risk of cancer. Willingness to engage in risk-reducing interventions was inversely proportional to their invasiveness. Perceived barriers included concerns about compliance, side effects and previous bad experiences. These data suggest that a primary endometrial cancer prevention trial that aims to reduce obesity and/or prevents its endometrial consequences could be acceptable, but would need to consider strategies to overcome some of these challenges.
Few previous studies have explored women’s understanding of the relationship between obesity and endometrial cancer risk. Two studies from the USA found 58% of 1545 women from the general population20 and 52% of 231 gynecology clinic attendees,21 respectively, were not aware that obesity increases the risk of endometrial cancer. Participant BMI did not impact awareness in either study. Other studies have focused their investigation on endometrial cancer patients, with similar findings.24–26 There is generally a lack of knowledge about the risk factors associated with endometrial cancer even in those who have been diagnosed and treated for the disease. A recent study from the UK found that among a nationally representative sample of 3293 adults, only 21.5% were aware of the association between body weight and endometrial cancer.27 Our study suggests higher levels of awareness (two thirds stated this risk factor without prompting), which may reflect the fact that our sample was made up of women with obesity attending gynecology, obesity and sleep apnea clinics. Nonetheless, there is still scope for improvement, and particularly for increasing awareness of personal risk as a consequence of excess weight. Attempts to increase awareness must be non-stigmatizing and supportive, and accompanied by advice on strategies for risk reduction to ensure they are beneficial and avoid harm.
To our knowledge, this is the first study to ask women at greatest risk of obesity-related endometrial cancer whether they would be willing to lose weight, change their diet, exercise more, take tablets and/or have an intrauterine device fitted for endometrial protection. We also asked women to articulate any perceived barriers to uptake and compliance with these interventions. Women were almost unanimously (94%) in favor of losing weight for the purposes of endometrial cancer risk reduction, but 43% admitted that weight loss is difficult to sustain in the long term. Whilst generally still amenable, only 91% women were keen to adopt a healthy diet in order to achieve this goal, noting that maintenance, portion size and costs were significant barriers. Eighty-seven percent of women were prepared to exercise more, citing poor mobility, poor general health, lack of time, lack of willpower and social embarrassment as major reasons. Around three-quarters were willing to take a pill every day, although nearly half noted that side effects, forgetting and/or general dislike of taking pills were barriers. Only half the women we asked would consider having an intra-uterine device for endometrial protection; difficulties with insertion (invasive, painful, bleeding), worry about side effects and previous bad experiences were the main reasons.
The insights gained from this study are important for the design of a primary endometrial cancer prevention trial, which would aim to recruit a similar cohort of women.8 Limitations include the small sample size and recruitment from a single center, which hinders extrapolation of our findings to other healthcare settings. We did not record the number or demographics of women that declined study participation, nor did we document their reasons for declining. This hinders an assessment of selection bias. The lack of racial and ethnic diversity in our study population precludes any insight into the willingness of non-White British women to engage in risk-reducing interventions and the barriers they may experience. Approaching women attending healthcare settings where weight loss is expected/recommended may also confer selection bias. We adapted established questionnaire items for this study but formal validation was not performed beforehand. This limits the reliability of our findings. We did not ask women whether they would be willing to be randomized to different interventions nor did we detail the personal commitment, invasive procedures and long-term surveillance that a prevention trial would require. Thus, although high-risk women seem willing to engage in risk-reducing interventions, we do not know whether they would participate in a trial to establish the efficacy of these interventions.
The rising global incidence of obesity-related endometrial cancer is a major concern that demands innovative solutions.28 Substantial and sustained weight loss achieved through bariatric surgery not only reduces endometrial cancer risk but also has considerable benefits for cardiovascular and metabolic health, mobility and quality of life.13,29,30 Whilst providing a life-saving treatment for the most severe cases of obesity, bariatric surgery cannot be regarded as a viable public health strategy for cancer prevention given the large at-risk population, associated complications and high costs. Weight loss achieved through dietary intervention may be equally beneficial for endometrial health and total diet replacement programs demonstrate high success rates and durable responses when delivered alongside high-quality psychological support.31–33 Long-term maintenance remains a significant challenge though, and the majority of individuals participating in weight loss programs will gradually regain weight loss, with estimates that only 20% of participants are successful over the longer term.34 This has led to the development of interventions focused on weight loss maintenance. However to date, the success of these programs has been modest.35 Nonetheless, studies indicate an appreciable reduction in breast cancer risk if as little as 2.5 kg of the weight lost is kept off long term.36 Comparable studies of endometrial cancer are not yet available, although data from the Women’s Health Initiative demonstrated that intentional weight loss of ≥5% over 3 years was associated with lower endometrial cancer risk over the subsequent 11 years, particularly among women with obesity. To date, the Look AHEAD trial is the only randomized controlled trial to explore the incidence of obesity-related cancers following a behavioral intervention. The intervention lowered the incidence of obesity-related cancers by 16% in adults with overweight or obesity and type 2 diabetes. However, this effect was non-significant, likely due to a lack of power.37,38
Physical activity is an important part of most behavioral weight management interventions but also has an independent effect on endometrial cancer risk. Regular exercise reduces endometrial cancer risk by 20–30%, with even greater benefits seen with high-intensity workouts of longer duration.15 The successful incorporation of physical activity into an already busy daily routine is a major barrier and poor cardiovascular fitness, mobility issues and social embarrassment are additional obstacles that must be overcome. Interventions should draw on a growing body of evidence for successful strategies in similar populations. For example, goal setting and self-monitoring, as well as the use of a person-centered and autonomy supportive counseling approach, have been identified as important for sustained dietary and physical activity changes in adults affected by overweight and obesity.39
Pharmacological intervention may appeal to women who have struggled to lose weight through diet and exercise, as it removes some of the psychological barriers to making long-term behavioral changes. Metformin, an insulin-sensitizing drug used in the treatment and prevention of type 2 diabetes mellitus, may reduce endometrial cancer risk and even cancer-related deaths17 through systemic changes in glucose metabolism and direct inhibition of pro-proliferative PI3K-Akt-mTOR signaling in the endometrium.40 Metformin has also shown promise in the treatment of endometrial hyperplasia, a precursor lesion of obesity-related endometrial cancer, alone or in combination with progestins.41,42 A significant challenge is that many women with obesity class II/III are already on metformin; indeed, a randomized feasibility study comparing behavior change, metformin treatment and a combination of the two for endometrial protection in women with obesity failed to find sufficient numbers of women who were both eligible and interested in participating.43 The glucagon-like peptide-1 receptor agonist (GLP-1RA) class of incretin-based anti-diabetes therapies has beneficial pleiotropic effects on the diverse metabolic defects seen in insulin resistance states.44 Emerging data suggest that exenatide45 and liraglutide46 induce autophagy of endometrial cancer cells through PI3K-Akt-mTOR signaling inhibition. Liraglutide is approved for type 2 diabetes (up to 1.8 mg) and obesity (up to 3.0 mg).47 These agents could provide a novel endometrial cancer prevention strategy through direct effects on cancer cell death and indirect effects of weight reduction and amelioration of insulin resistance.
Five years or more of exposure to the combined oral contraceptive pill reduce the risk of endometrial cancer by 50%, with durable protection out to 30 years post-treatment,48 although the risks outweigh the benefits in obese women with multiple cardiovascular risk factors.49 A meta-analysis of cohort and case-control studies demonstrated a 56% reduction in endometrial cancer risk with 3 or more years of bisphosphonate use,50 a viable chemopreventive strategy in women with obesity and associated co-morbidities. The levonorgestrel-releasing intrauterine system (LNG-IUS) is associated with a 54% reduction in endometrial cancer risk, which increases to 75% if treatment is prolonged.51 It has also shown promise in the treatment of endometrial hyperplasia52 and early stage, low grade endometrial cancers,53,54 through endometrial decidualization, down-regulation of oncogenic signaling and triggering of senescence and apoptosis.55 Disadvantages of its use for endometrial protection are mostly related to the invasiveness of its insertion, but the low frequency of systemic side effects is beneficial for long-term compliance. A feasibility study of the LNG-IUS for endometrial protection in women with class II/III obesity reported an uptake of approximately 50%, no failed insertions in the outpatient setting and no adverse effects triggering withdrawal in a predominantly post-menopausal cohort.56
A primary endometrial cancer prevention trial faces many design challenges including type of study, population, sample size, trial intervention(s), primary endpoint and duration.8 There are also considerable cost implications, particularly if multiple interventions are to be trialed and endometrial cancer is the primary endpoint. The current study provides an indication that women with class II/III obesity, whilst not always appreciating their increased risk of endometrial cancer, would nevertheless be interested in behavioral and/or pharmacological interventions to reduce their risk, despite recognizing potential downsides and challenges. More sophisticated risk calculators that incorporate obesity, metabolic, reproductive and genetic factors are now needed to select high-risk women for trial participation in order to maximize the benefits and minimize the harms of risk-reducing interventions.8,57–59
In conclusion, the current study shows that women at greatest risk of obesity-related endometrial cancer may not always recognize their risk, but a willingness to engage in evidence-based risk-reducing interventions offers a potential strategy for primary prevention.
Acknowledgments
We would like to thank the women who participated in this study. We are grateful for the invaluable assistance of Gill Hesketh, who sadly passed away before this study was completed.
Funding
AED and MLM were Manchester University NHS Foundation Trust Clinical Research Fellows, EJC a National Institute for Health Research (NIHR) Clinician Scientist (NIHR-CS-012-009), and their work was supported through the NIHR Manchester Biomedical Research Centre (IS-BRC-1215-20007). RJB was supported by Yorkshire Cancer Research University Academic Fellowship funding (L389RB). This article presents independent research funded by the NIHR. The views expressed are those of the authors and not necessarily those of the NHS, NIHR, or the Department of Health.
Disclosure
The authors report no conflicts of interest.
References
1. Cancer Research UK. Uterine cancer incidence statistics; 2015. Available from: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/uterine-cancer/incidence.
2. Cancer Research UK. Uterine cancer survival statistics; 2015. Available from: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/uterine-cancer/survival.
3. NHS Digital. Statistics on obesity, physical activity and diet, England; 2020. Available from: https://digital.nhs.uk/data-and-information/publications/statistical/statistics-on-obesity-physical-activity-and-diet/england-2020.
4. Malik V, Willett W, Hu F. Global obesity: trends, risk factors and policy implications. Nat Rev Endocrinol. 2013;9:13–27. doi:10.1038/nrendo.2012.199
5. Raglan O, Kalliala I, Markozannes G, et al. Risk factors for endometrial cancer: an umbrella review of the literature. Int J Cancer. 2019;145(7):1719–1730. PMID: 30387875. doi:10.1002/ijc.31961
6. Crosbie E, Zwahlen M, Kitchener H, Egger M, Renehan A. Body mass index, hormone replacement therapy and endometrial cancer risk: a meta analysis. Cancer Epidemiol Biomark Prev. 2010;19(12):3119–3130. doi:10.1158/1055-9965.EPI-10-0832
7. Kaaks R, Lukanova A, Kurzer MS. Obesity, endogenous hormones, and endometrial cancer risk: a synthetic review. Cancer Epidemiol Biomarkers Prev. 2002;11(12):1531–1543.
8. Kitson SJ, Evans DG, Crosbie EJ. Identifying high-risk women for endometrial cancer prevention strategies: proposal of an endometrial cancer Risk prediction model. Cancer Prev Res. 2017;10(1):1–13. doi:10.1158/1940-6207.CAPR-16-0224
9. Calle EE, Kaaks R. Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer. 2014;4:579–591. doi:10.1038/nrc1408
10. Avgerinos KI, Spyrou N, Mantzoros CS, Dalamaga M. Obesity and cancer risk: emerging biological mechanisms and perspectives. Metabolism. 2019;92:121–135. doi:10.1016/j.metabol.2018.11.001
11. Modugno F, Ness RB, Chen C, Weiss NS. Inflammation and endometrial cancer: a hypothesis. Cancer Epidemiol Biomarkers Prev. 2005;14(12):2840–2847. doi:10.1158/1055-9965.EPI-05-0493
12. MacKintosh ML, Crosbie EJ. Prevention strategies in endometrial carcinoma. Curr Oncol Rep. 2018;20(12):101. doi:10.1007/s11912-018-0747-1
13. Ward KK, Roncancio AM, Shah NR, et al. Bariatric surgery decreases the risk of uterine malignancy. Gynecol Oncol. 2014;133(1):63–66. doi:10.1016/j.ygyno.2013.11.012
14. Mackintosh ML, Crosbie EJ. Obesity-driven endometrial cancer: is weight loss the answer? BJOG. 2013;120(7):791–794. doi:10.1111/1471-0528.12106
15. Schmid D, Behrens G, Keimling M, Jochem C, Ricci C, Leitzmann M. A systematic review and meta-analysis of physical activity and endometrial cancer risk. Eur J Epidemiol. 2015;30(5):397–412. doi:10.1007/s10654-015-0017-6
16. Gompel A. Progesterone and endometrial cancer. Best Pract Res Clin Obstet Gynaecol. 2020;69:95–107. doi:10.1016/j.bpobgyn.2020.05.003
17. Chu D, Wu J, Wang K, et al. Effect of metformin use on the risk and prognosis of endometrial cancer: a systematic review and meta-analysis. BMC Cancer. 2018;18(1):438. doi:10.1186/s12885-018-4334-5
18. Njoku K, Abiola J, Russell J, Crosbie EJ. Endometrial cancer prevention in high-risk women. Best Pract Res Clin Obstet Gynaecol. 2020;65:66–78. doi:10.1016/j.bpobgyn.2019.12.005
19. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
20. Soliman PT, Bassett RL
21. Washington CR, Haggerty A, Ronner W, Neff PM, Ko EM. Knowledge of endometrial cancer risk factors in a general gynecologic population. Gynecol Oncol. 2020;158(1):137–142. doi:10.1016/j.ygyno.2020.03.032
22. Dillard AJ, Ferrer RA, Ubel PA, Fagerlin A. Risk perception measures’ associations with behavior intentions, affect, and cognition following colon cancer screening messages. Health Psychol. 2012;31(1):106–113. doi:10.1037/a0024787
23. Stubbings S, Robb K, Waller J, et al. Development of a measurement tool to assess public awareness of cancer. Br J Cancer. 2009;101(Suppl2):S13–S17. doi:10.1038/sj.bjc.6605385
24. Haggerty AF, Sarwer DB, Schmitz KH, Ko EM, Allison KC, Chu CS. Obesity and endometrial cancer: a lack of knowledge but opportunity for intervention. Nutr Cancer. 2017;69(7):990–995. doi:10.1080/01635581.2017.1359313
25. Sekhon S, Massad LS, Hagemann AR, et al. Patients with endometrial cancer continue to lack understanding of their risks for cancer. Gynecol Oncol Rep. 2019;29:106–110. doi:10.1016/j.gore.2019.07.013
26. Wilkinson M, Murphy S, Sinclair P, Heneghan H, le Roux CW, Brennan DJ. Patient perceptions and understanding of obesity related endometrial cancer. Gynecol Oncol Rep. 2020;31(32):100545. doi:10.1016/j.gore.2020.100545
27. Hooper L, Anderson AS, Birch J, et al. Public awareness and healthcare professional advice for obesity as a risk factor for cancer in the UK: a cross-sectional survey. J Public Health. 2018;40(4):797–805. doi:10.1093/pubmed/fdx145
28. Crosbie E, Morrison J. The emerging epidemic of endometrial cancer: time to take action. Cochrane Database Syst Rev. 2014;22(12):ED000095.
29. MacKintosh ML, Derbyshire AE, McVey RJ, et al. The impact of obesity and bariatric surgery on circulating and tissue biomarkers of endometrial cancer risk. Int J Cancer. 2019;144(3):641–650. doi:10.1002/ijc.31913
30. Arterburn DE, Telem DA, Kushner RF, Courcoulas AP. Benefits and risks of bariatric surgery in adults: a review. JAMA. 2020;324(9):879–887. doi:10.1001/jama.2020.12567
31. Bischoff SC, Damms-Machado A, Betz C, et al. Multicenter evaluation of an interdisciplinary 52-week weight loss program for obesity with regard to body weight, comorbidities and quality of life - A prospective study. Int J Obes. 2012;36(4):614–624. doi:10.1038/ijo.2011.107
32. Astbury NM, Aveyard P, Nickless A, et al. Doctor Referral of Overweight People to Low Energy total diet replacement Treatment (DROPLET): pragmatic randomised controlled trial. BMJ. 2018;362:k3760.
33. Lean ME, Leslie WS, Barnes AC, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster- randomised trial. Lancet. 2018;391(10120):541–551. doi:10.1016/S0140-6736(17)33102-1
34. Wing RR, Phelan S. Long-term weight loss maintenance. Am J Clin Nutr. 2005;82(1Suppl):222S–225S. doi:10.1093/ajcn/82.1.222S
35. Dombrowski SU, Knittle K, Avenell A, Araújo-Soares V, Sniehotta FF. Long term maintenance of weight loss with non-surgical interventions in obese adults: systematic review and meta-analyses of randomised controlled trials. BMJ. 2014;348:g2646. doi:10.1136/bmj.g2646
36. Teras LR, Patel AV, Wang M, et al. Sustained weight loss and risk of breast cancer in women 50 years and older: a pooled analysis of prospective data. J Natl Cancer Inst. 2020;112(9):929–937. doi:10.1093/jnci/djz226
37. Luo J, Chlebowski RT, Hendryx M, et al. Intentional weight loss and endometrial cancer risk. J Clin Oncol. 2017;35(11):1189–1193. doi:10.1200/JCO.2016.70.5822
38. Yeh HC, Bantle JP, Cassidy-Begay M, et al.; Look AHEAD Research Group. Intensive weight loss intervention and cancer risk in adults with type 2 diabetes: analysis of the look AHEAD randomized clinical trial. Obesity. 2020;28(9):1678–1686. doi:10.1002/oby.22936
39. Samdal GB, Eide GE, Barth T, Williams G, Meland E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int J Behav Nutr Phys Act. 2017;14(1):42. doi:10.1186/s12966-017-0494-y
40. Sivalingam VN, Myers J, Nicholas S, Balen AH, Crosbie EJ. Metformin in reproductive health, pregnancy and gynaecological cancer: established and emerging indications. Hum Reprod Update. 2014;20(6):853–868. doi:10.1093/humupd/dmu037
41. Yang BY, Gulinazi Y, Du Y, et al. Metformin plus megestrol acetate compared with megestrol acetate alone as fertility-sparing treatment in patients with atypical endometrial hyperplasia and well-differentiated endometrial cancer: a randomised controlled trial. BJOG. 2020;127(7):848–857. doi:10.1111/1471-0528.16108
42. Clement NS, Oliver TR, Shiwani H, Sanner JR, Mulvaney CA, Atiomo W. Metformin for endometrial hyperplasia. Cochrane Database Syst Rev. 2017;10(10):CD012214. doi:10.1002/14651858.CD012214.pub2
43. Yates MS, Coletta AM, Zhang Q, et al. Prospective randomized biomarker study of metformin and lifestyle intervention for prevention in obese women at increased risk for endometrial cancer. Cancer Prev Res. 2018;11(8):477–490. doi:10.1158/1940-6207.CAPR-17-0398
44. Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like peptide-1. Cell Metab. 2018;27(4):740–756. doi:10.1016/j.cmet.2018.03.001
45. Zhang Y, Xu F, Liang H, et al. Exenatide inhibits the growth of endometrial cancer Ishikawa xenografts in nude mice. Oncol Rep. 2016;35(3):1340–1348. doi:10.3892/or.2015.4476
46. Kanda R, Hiraike H, Wada-Hiraike O, et al. Expression of the glucagon-like peptide-1 receptor and its role in regulating autophagy in endometrial cancer. BMC Cancer. 2018;18(1):657. doi:10.1186/s12885-018-4570-8
47. Ammori BJ, Skarulis MC, Soran H, Syed AA, Eledrisi M, Malik RA. Medical and surgical management of obesity and diabetes: what’s new? Diabet Med. 2020;37(2):203–210. doi:10.1111/dme.14215
48. Iversen L, Sivasubramaniam S, Lee AJ, Fielding S, Hannaford PC. Lifetime cancer risk and combined oral contraceptives: the Royal College of general practitioners’ oral contraception study. Am J Obstet Gynecol. 2017;216(6):580e1–e9. doi:10.1016/j.ajog.2017.02.002
49. FSRH UK MEC. UK medical eligibility criteria for contraceptive use; 2016. Available from: https://www.fsrh.org/standards-and-guidance/external/ukmec-2016-digital-version/.
50. Ou Y-J, Chiu H-F, Wong Y-H, Yang Y-H. Bisphosphonate use and the risk of endometrial cancer: a meta-analysis of observational studies. Pharmacoepidemiol Drug Saf. 2016;25(10):1107–1115. doi:10.1002/pds.4075
51. Soini T, Hurskainen R, Grenman S, Maenpaa J, Paavonen J, Pukkala E. Cancer risk in women using the levonorgestrel-releasing intrauterine system in Finland. Obstet Gynecol. 2014;124(2 Pt 1):292–299. doi:10.1097/AOG.0000000000000356
52. Mittermeier T, Farrant C, Wise MR. Levonorgestrel-releasing intrauterine system for endometrial hyperplasia. Cochrane Database Syst Rev. 2020;9:CD012658. doi:10.1002/14651858.CD012658.pub2
53. Westin SN, Fellman B, Sun CC, et al. Prospective Phase II trial of levonorgestrel intrauterine device: nonsurgical approach for complex atypical hyperplasia and early-stage endometrial cancer. Am J Obstet Gynecol. 2020;224(2). doi:10.1016/j.ajog.2020.08.032
54. Barr CE, Ryan NAJ, Derbyshire AE, et al. Weight loss during intrauterine progestin treatment for obesity-associated atypical hyperplasia and early-stage cancer of the endometrium. Cancer Prev Res. 2021. doi:10.1158/1940-6207.CAPR-21-0229
55. Bahamondes L, Valeria Bahamondes M, Shulman LP. Non-contraceptive benefits of hormonal and intrauterine reversible contraceptive methods. Hum Reprod Update. 2015;21:640–651. doi:10.1093/humupd/dmv023
56. Derbyshire AE, Allen JL, Gittins M, et al. PROgesterone therapy for endometrial cancer protection in obese women (PROTEC) trial: a feasibility study. Cancer Prev Res. 2020;14(2):263–274. doi:10.1158/1940-6207.CAPR-20-0248
57. Bafligil C, Thompson DJ, Lophatananon A, et al. Association between genetic polymorphisms and endometrial cancer risk: a systematic review. J Med Genet. 2020;57(9):591–600. doi:10.1136/jmedgenet-2019-106529
58. O’Mara TA, Crosbie EJ. Polygenic risk score opportunities for early detection and prevention strategies in endometrial cancer. Br J Cancer. 2020;123(7):1045–1046. doi:10.1038/s41416-020-0959-7
59. Wan YL, Beverley-Stevenson R, Carlisle D, et al. Working together to shape the endometrial cancer research agenda: the top ten unanswered research questions. Gynecol Oncol. 2016;143(2):287–293. doi:10.1016/j.ygyno.2016.08.333
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.