Back to Journals » Patient Preference and Adherence » Volume 19
Why We Keep Going: A Qualitative Longitudinal Study of the Motivation and Engagement Among Patients with COPD During a Long-Term Danish Tele-Rehabilitation Program
Authors Olsen M ![]() , Nielsen C, Emme C
, Nielsen C, Emme C ![]() , Godtfredsen NS
, Godtfredsen NS ![]() , Hansen H
, Hansen H ![]()
Received 24 June 2025
Accepted for publication 16 October 2025
Published 12 November 2025 Volume 2025:19 Pages 3573—3587
DOI https://doi.org/10.2147/PPA.S549332
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Maria Olsen,1 Christina Nielsen,1 Christina Emme,2 Nina Skavlan Godtfredsen,1,3 Henrik Hansen1,3,4
1Respiratory Research Unit and Department of Respiratory Medicine, Copenhagen University Hospital – Hvidovre, Hvidovre, 2650, Denmark; 2Department of Quality and Education, Copenhagen University Hospital – Bispebjerg, Copenhagen, 2400, Denmark; 3Institute for Clinical Medicine, University of Copenhagen, Copenhagen, 2200, Denmark; 4Institute of Rehabilitation Sciences, University of Antwerp, Antwerpen, 2000, Belgium
Correspondence: Christina Nielsen, Email [email protected]
Introduction: Pulmonary tele-rehabilitation (PTR) is an effective treatment for patients with chronic obstructive pulmonary disease (COPD). However, determinants of sustained motivation and adherence have been sparsely investigated.
Aim: This study examined how motivation and engagement evolved throughout 25 weeks of a maintenance PTR program in patients with moderate to very severe COPD.
Methods: In a qualitative study with a longitudinal recurrent cross-sectional design, 11 individual semi-structured interviews were conducted after 10 week of Homebased Pulmonary Rehabilitation (HPR) or PTR intervention and 10 interviews were conducted after 25 weeks into the maintenance PTR program with 16 patients participating in a randomized controlled trial on pulmonary tele-rehabilitation at Hvidovre Hospital, Denmark. The interview guide and initial coding framework were directed by the Theoretical Domains Framework in a deductive content analysis. An unconstrained matrix, based on inductive principles, was used to capture categories across multiple domains.
Results: Three main categories emerged: (1) Acceptance and Hope, (2) Physical Factors, and (3) External Support. Over time, participants developed greater acceptance of COPD, transitioning from fear-driven motivation to sustained engagement through improved coping strategies. Easy PTR access, continuous therapist, and peer support were key factors in maintaining adherence.
Conclusion: Over the course of 25 weeks, motivation evolved from fear-driven to autonomous, reflective engagement. The results emphasize the importance of external support and tailored environments like remote delivery methods for long-term adherence to maintenance PTR programs.
Keywords: telerehabilitation, COPD, motivation, engagement, longitudinal research, qualitative, interviews, TDF
Introduction
Globally, Chronic Obstructive Pulmonary Disease (COPD) is one of the top four leading cause of death and is characterized by persistent airway obstruction and symptoms like breathlessness, cough, increased mucus production, and fatigue.1,2 Pulmonary Rehabilitation (PR) is essential in COPD management3 and defined by American Thoracic Society/European Respiratory Society as:
A comprehensive intervention based on a thorough patient assessment followed by papatient-tailored herapies that include, but are not limited to, exercise training, education, and behavior change, designed to improve the physical and psychological condition of people with chronic respiratory disease and to promote the long-term adherence to health-enhancing behaviors.4
However, less than 30% of patients with COPD complete PR due to barriers such as transportation, mobility issues, exacerbations, and low motivation.5–8 Thus, emerging PR methods like Home-based Pulmonary Rehabilitation (HPR) and Pulmonary Tele-Rehabilitation (PTR) are proposed, offering outcomes comparable to traditional center-based rehabilitation, and achieving higher participation rates.9 Especially, the COVID-19 pandemic has accelerated the interest to utilize these new PR delivery methods as they address several of the well-known barriers to traditional center-based PR programs like transportation and mobility barriers while still maintaining communication between patient and health professionals.10 HPR consists of PR in the patients’ home while PTR is PR performed via a technological device such as a tablet screen, also often from the patients’ home.9,11,12
While short-term PR benefits are well-documented, studies indicate that health gains decline after 12 months without continued supervised exercise.13,14 Maintenance programs can support long-term improvements but face adherence challenges, with dropout rates increasing over time from 27% to 53%.14–17 Qualitative studies have shown that lack of motivation for physical exercise, long commute to a rehabilitation center, daily fluctuating respiratory symptoms, and frequent exacerbations, especially those requiring hospitalization, are emphasized as main factors affecting motivation and adherence negatively.17,18
To address these challenges, new models of delivering short-term PR and maintenance programs have been proposed with the use of health care technology like tablet-based video-conference calls.19 Studies emphasize the role of health benefits, self-efficacy, independence, and user-friendly technology in sustaining long-term adherence and managing COPD challenges.18,20 However, they also underscore significant challenges and the current lack of knowledge regarding whether and how these tablet-based maintenance programs can be successfully integrated into patients’ everyday lives following a short-term PR program.19 A key factor in this integration is patients’ sustained motivation and engagement, as these processes are central to maintaining participation in long-term PR.21,22 Motivation is defined as a process aimed at creating and maintaining a specific behavior to achieve a particular outcome, and engagement refers to being interested, emotionally involved, and/or committed to something.23,24 Yet, the evolvement of long-term motivational factors within supervised group-based exercise maintenance programs via a tablet, particularly following HPR or PTR, remains unexplored. To the authors knowledge no other studies have qualitatively investigated this specifically on a group of patients with COPD who are unable to attend center-based PR. Therefore, this study aimed to examine how perceptions of motivation and factors related to engagement evolve over a 25-week period during a 65-week maintenance group-based tele-rehabilitation program for patients with moderate to very severe COPD who have declined traditional center-based rehabilitation.
Materials and Methods
This qualitative study is registered at osf.io, https://osf.io/74sja and was conducted as part of a randomized controlled trial (RCT) examining the effects of a 10-week intervention with either structured home-based pulmonary rehabilitation (HPR) or group supervised tele-pulmonary rehabilitation (PTR) delivered via tablet (video-conference system), followed by a 65-week maintenance group-based PTR program offered to all the participants merging the two groups to one. The tablet enables all participants to see each other during exercise and communicate. All participants proceeded with their usual medication regimen. The details on the RCT-study can be found in the protocol published December 22nd 2022 at Clinicaltrials.gov, ID: NCT05664945,25 no deviations made to the protocol. This qualitative study used a longitudinal recurrent cross-sectional design,26,27 with semi-structured interviews conducted in two blocks after the 10-week HPR or PTR intervention program and again 25 weeks into the maintenance PTR program. This design was chosen to examine the evolvement in motivation and engagement over time, ensuring reliable data and achieving data saturation in a patient group prone to lower attendance and dropouts during prolonged interventions.18,28 By using a longitudinal recurrent cross-sectional design, we were also able to address the challenges posed by high attrition and clinical vulnerability in COPD populations, thereby ensuring an efficient use of research resources and minimizing the ethical risk of performing interviews not used as would be the risk of a trajectory design.
Framework
This study applied the latest validated version of Theoretical Domains Framework (TDF),29 a widely recognized framework in intervention and implementation research. The TDF consists of 14 domains and was developed by an interdisciplinary team to integrate behavior change theories into a single, accessible framework.29,30 In the present study, TDF was applied to develop interview guides, ensure data saturation, and serve as a preliminary coding framework.
Participants
Patients were recruited from five hospitals in the Capital Region of Denmark during their follow-up assessment at 10 weeks and 25 weeks into the maintenance program (1st May 2023–28th February 2024) using purposive sampling with maximal variety to ensure diversity in gender, age, socioeconomic status, attendance patterns, and personal factors (eg, marital status, severity of COPD). The study sought to achieve a gender balance, a broad age distribution, and an equal representation of participants from HPR and PTR. Eligible patients were adults (>18 years) with COPD in Global Initiative for Chronic Obstructive Lung Disease (GOLD) groups B, C, or D, unable or unwilling to access and participate in the conventional out-patient hospital- or community-based PR, due to various reasons like transportation barriers and low functional capacity, when offered during routine consultation and who had not undergone conventional PR within the past 24 months. The two physiotherapists (CN and HH) leading the interventions initially identified potential interview candidates, with final selection determined through discussions within the research team to reflect gender balance, a broad age range, representation from both HPR and PTR, and to capture a range of perspectives.
Data Generation
The individual interviews were conducted face-to-face by two female and one male physiotherapist (CN, MO, HH), all experienced in working with patients with COPD. MO had no previous experience in conducting interviews, CN had minor experience, and HH was more experienced. CN and HH had prior professional relationships with patients, while MO had no prior involvement. These prior relationships may have facilitated openness and richer responses, but also risked socially desirable answers, an effect sough balanced by MO. The location of the interviews was based on the patients’ preference. Data saturation was discussed frequently by the research team based on coverage of the TDF. To increase variation, sampling was targeted after 14 interviews to underrepresented groups, including men and participants with higher socioeconomic status, particularly for the 25-week interviews. Seven additional interviews were conducted with two interviewers present. After 21 interviews, no new information emerged despite varied interviewer constellations, focused sampling, and an adapted interview guide, indicating that data saturation had been reached. Three TDF-based interview guides, tailored to each intervention group (HPR, PTR, and maintenance PTR) were used. The questions were developed based on insights from previous studies involving patients with COPD, advise from patients, and discussions in the research team. After conducting six interviews, the 25-weeks interview guide underwent minor revisions to simplify language, based on patient feedback. The 10-week interview guides are available in supplementary material 1.
Data Analysis
The interviews were audio recorded, transcribed verbatim using Express Scribe Transcription Software version 13.24 (NCH Software, Inc., Canberra, Australia) and anonymized using pseudonyms. The analytical method applied was deductive content analysis, based on Elo and Kyngäs’ framework, focusing on manifest data.31 This flexible approach, chosen for its structured steps that enable clear, manageable analysis of large datasets, is particularly suited for longitudinal studies, allowing for category comparisons across time points.31 Each group of interviews was manually coded in the software, NVivo version 15, analyzed, and described separately, before comparing the category findings from the 10-week HPR and PTR interventions with the 25-week maintenance PTR. The initial coding phase was conducted by MO and every third interview was double coded by either CE (experienced qualitative researcher) or HH (specialist in pulmonary rehabilitation and experienced qualitative researcher) to broaden the perspective of the data. The researcher independently identified each meaning unit and analyzed into the domains in the TDF deductively. The few coding differences that arose were discussed, allowing multiple perspectives to be considered and consensus to be reached. For the categorization, an unconstrained matrix based on inductive principles was used to explore insights across multiple domains. Finally, the categories from the 10 and 25 weeks were compared to identify evolvement or fixed categories between them. An example of the analysis process is shown in Figure 1.
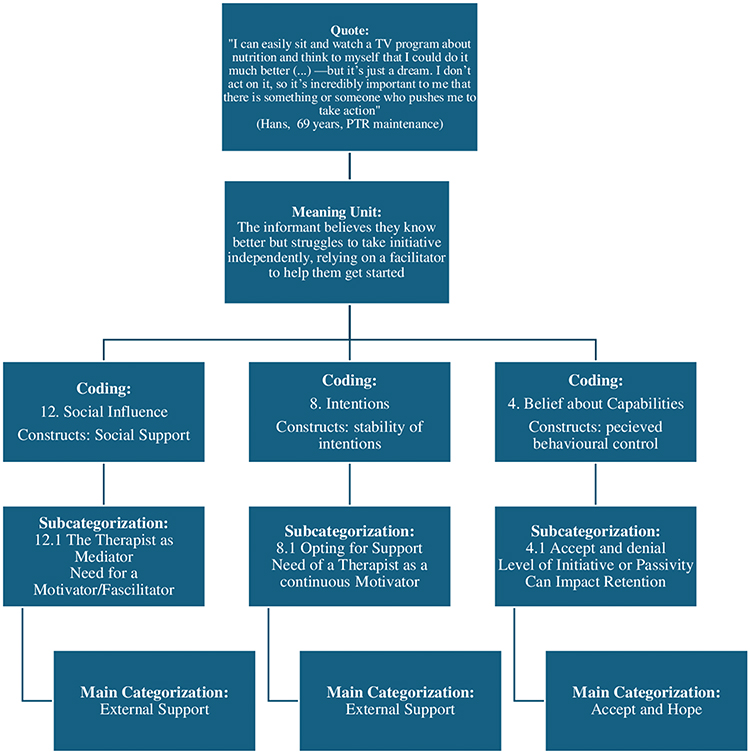 |
Figure 1 Coding Tree. Overview of the Analytical Process: From Quote to Main Category. The quote is first rewritten as a meaning unit, which is then coded into three domains and their constructs within the TDF. Next, an unconstrained matrix is applied, allowing for analysis across the domains, leading to further subcategorization and, ultimately, the main categories. |
Ethical Approval
The study was approved by the Danish Data Protection Agency (P-2022-245-13101) and the National Committee of Ethics, nr: H-22015777 the 22nd of September 2022 and carried out in accordance with the principles of the Helsinki Declaration. All patients provided written and verbal informed consent in the RCT study. Prior to the interviews, the aim of the study and the patients’ role in the research project were fully explained verbally and in writing. The patients agreed to the interviews being audiotaped with their statements anonymized and permission to use anonymized quotes and informed consent was obtained from all the patients.
Results
Participants Characteristics
A total of 21 patients were invited to participate in the study, 16 accepted and 5 declined due to lack of interest (n=3) and hospitalization (n=2). See Figure 2 for an overview. Thus, this study included 16 patients (four males and 12 females) with COPD, with a mean Forced Expiratory Volume in 1 second (FEV1) of 43.8% (range: 22–72), corresponding to moderate to very severe airflow obstruction. The patients had a mean age of 71 years (range: 50–86). Ten patients were living alone. Six patients had never attended PR, while the remaining patients had prior experience with center-based PR. See Table 1 for further patient details. The interviews were conducted in the period from April 2023 to February 2024.
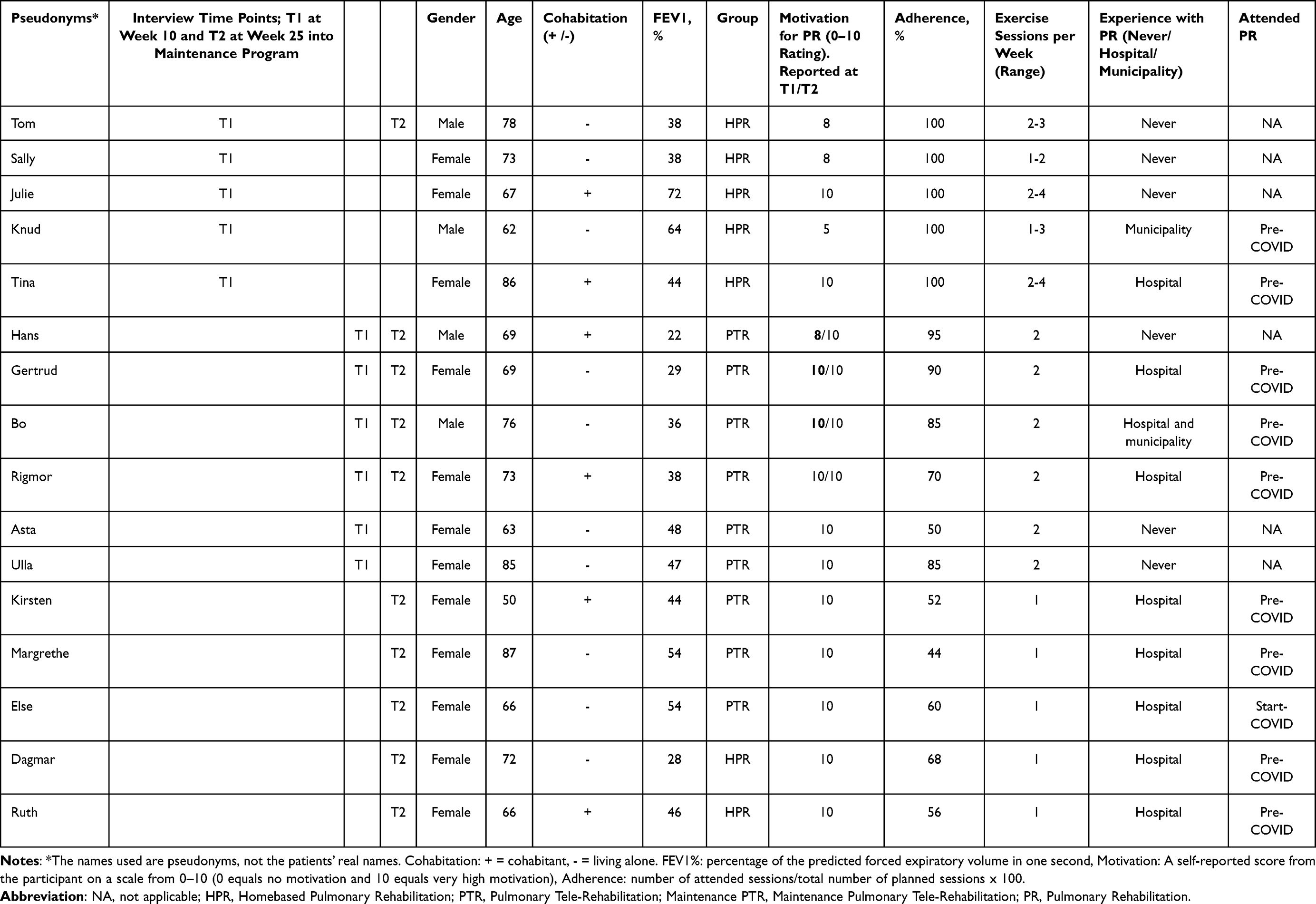 |
Table 1 Participant Characteristics |
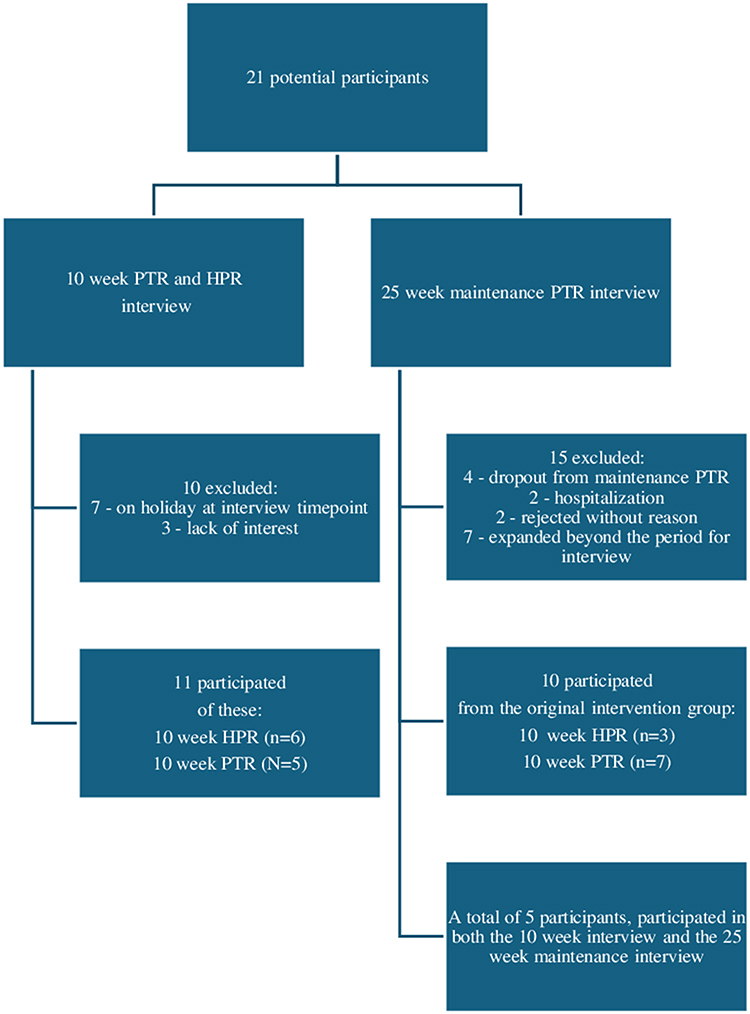 |
Figure 2 Flowchart of the recruitment process. |
Main Findings
In total, 21 interviews were conducted with the 16 participating patients as five patients took part in both the 10-week and 25-week interviews. The interviews were distributed across the groups as follows: five (HPR), six (PTR), and 10 (Maintenance). Two interviews were conducted at the hospital and 19 in patients’ homes, with an average duration of 40 minutes.
In the initial coding phase, 2811 meaning units were identified, with the following distribution: 10-week HPR = 525, 10-week PTR = 813, and 25-week maintenance = 1,460. During the categorization phase, three main categories emerged, each containing two and three subcategories. See Figure 3 for an overview.
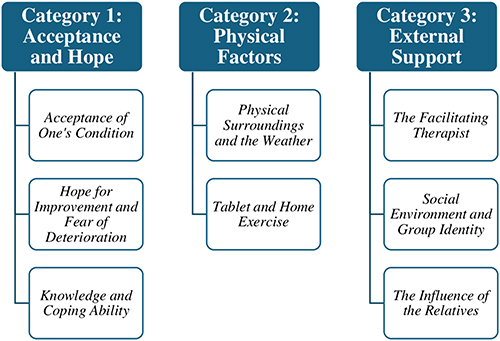 |
Figure 3 Overview of the three main categories and their respective subcategories. |
Category 1 – Acceptance and Hope
Acceptance and Hope illustrates how continued engagement and attendance during the 25-week maintenance program help patients move closer to accepting COPD and its future implications. While full acceptance may not yet be achieved, motivation evolves from being driven by fear and hope for improvement to being sustained by increased knowledge and an enhanced ability to cope with COPD.
Acceptance of One’s Condition
Being diagnosed with COPD and accepting its chronic nature are expressed as challenging for the majority of the patients both in HPR and PTR. While three patients from HPR express improved understanding and confidence, acceptance varied significantly, and several patients struggle to accept the chronic condition and its implications.
Well, yes, but it is also (pause). I haven’t yet accepted 100 %, that my lungs aren’t pink, well, they won’t be that anymore, right? (Julie, 67 years, HPR)
For the majority of patients in PTR this is also evident as many exhibited increased self-awareness, likely influenced by comparing themselves to others during group sessions. Such comparisons promote motivation to either see how others improve their physical performance or to see themselves being in a better condition than first anticipated, which fosters a deeper understanding of their health.
Well, but I have always said to myself, that you should be glad about what you can and that it could be so much worse, right? This I have said to myself a lot of times and I get it confirmed, - when I see these older women, who have a much worse pulmonary condition than me, right? (Ulla, 85 years, PTR)
During the maintenance program, nine patients develop a greater awareness of the importance of physical activity for maintaining quality of life, resulting in prioritization of the maintenance sessions, and increasing the motivation to continue attending sessions.
Well, it’s because you are ready to do something. (…) I can feel it if I skip my own training. I notice that if I’m not feeling great, it takes longer to get back to my usual level again. (Gertrud, 69 years, maintenance PTR)
They also become better at recognizing their limits, seeking help with daily tasks, declining tasks beyond their capacity and prioritizing their health.
Hope for Improvement and Fear of Deterioration
The patients who receive HPR express the motivational factors double sided as for all there is a general hope for improvement and wish to improve quality of life and their physical functioning. On the other hand, four patients had also a notable fear of worsening their condition and experience exacerbations.
Honestly, it is just as well because I am terrified to become as ill as I were when I was hospitalized over here (at the Hospital), right? (Julie, 67 years, HPR)
These ambiguous feelings are also evident in the PTR group, although three express more optimism about the future. For two, the motivation comes from the immediate benefits during the exercise sessions, while others get motivated by setting specific goals, such as walking up the stairs or performing household tasks.
Before all this, I told my husband that we might as well sign me up for a nursing home or assisted living (…) But I didn’t need that after all, because now I can, I really can, and you can do almost anything if you set your mind to it, right? (Rigmor, 73 years, PTR)
After 25 weeks in the maintenance program, eight patients maintain a positive outlook and continued commitment to exercise. Five patients envision a future, making plans beyond what they had prior to PR indicating a shift in motivation from being motivated by fear to be motivated by the future prospects, whilst three patients were motivated to maintain their current functioning levels.
I kept moving towards a space where I avoided challenging myself, right? (…) And then suddenly, (…) I could look back and see that my life looked completely different. I was saying yes to all sorts of things that I would have just said no to before. (Tom, 78 years, Maintenance PTR)
This applies to some patients both from PTR and HPR patients, with improved dyspnea management and better physical function driving their motivation.
Yes, I feel like I’ve gotten better at getting started with things at home—getting some cleaning done, tackling it bit by bit. (…) I sit down, catch my breath, and then I do it. Not because I have to, but because I’m not afraid of being out of breath anymore. That’s something I’ve learned to handle. (Rigmor, 73 years, Maintenance PTR)
Knowledge and Coping Ability
Both the HPR and PTR groups report improved control over their breathing through instruction in breathing techniques, fostering a sense of security, and serving as a consistent source of motivation throughout the maintenance program. Notably, five participants in the PTR group find breathwork education motivating, as their progressively improving skills boosted their confidence in daily activities.
Yes, absolutely. I’ve really gained a lot from learning some techniques—some tools to control my own breathing. I have my non-invasive ventilator-machine in there, right? And it definitely helps regulate my breathing. But I’ve also learned to manage without it… (Hans, 69 years, maintenance PTR)
For four patients, increased knowledge about COPD in general and in relation to exercise does not seem to affect their motivation to complete the program. However, they still acknowledge the importance of exercise.
It’s absolutely crucial for my well-being, but if I don’t participate, it’s not like I’ll die from it. Maybe I won’t live quite as long, but it’s not as if I’ll just drop dead if I don’t take part. (Hans, 69 years, PTR)
Three patients with prior negative experiences from center-based rehabilitation or fitness training report greater fear in relation to the exercise sessions which they needed to overcome to continue in the maintenance program.
You are a bit scared not to walk the distance and succeed the exercise session, because you may think that it is somewhat of a bodybuilding stuff, where you have to do a whole lot, right? (Knud, 62 years, HPR)
Category 2 – Physical Factors
Physical Factors illustrate how various physical factors remain essential prerequisites for continued engagement, without evolving in their impact on motivation and engagement throughout the program. The home-based setting is a key criterion for ongoing participation in HPR, PTR, and the maintenance program, with factors like the weather consistently influencing motivation. The category emphasizes the steady impact of the tablet-based intervention model on engagement during group-based exercise sessions.
Physical Surroundings and the Weather
For all patients in both PTR and HPR programs, the homebased setting, logistical factors, and weather play an essential role in sustaining adherence to the maintenance program and to the amount of daily physical activity both in- and outside the home. Adverse weather conditions, particularly humidity and rain, can impair breathing, lower motivation, and increase the likelihood of non-attendance if the program was to be center-based.
Because I know that if it’s stormy and raining, I won’t be able to get out of the chair and go to the exercise class, so, well. It’s like I’m practically drenched just trying to get there. (Sally, 73 years, HPR)
The logistical benefits of exercising at home are significant for all 16 patients, as tasks such as personal hygiene, getting dressed, and transportation to public locations consume significant physical and mental resources. The ease of accessibility in the homebased setting fosters a greater adherence and enhance intrinsic motivation to “keep going”.
You can pull yourself together in the morning and say, well, I can manage this, you don’t have to go out and all that. It’s something completely different when you have to leave the house, and you’re already tired beforehand. Then you must start planning a lot more, right. (Gertrud, 69 years, Maintenance PTR)
These factors remained as a consistently important factor for ongoing engagement and a prerequisite factor to keep attending the maintenance program.
Exercise has a high priority...yes, it has… I tell my friends that they don’t have to call Tuesdays 10.30-11.30, because I’m not going to answer it. (Else, 66 years, Maintenance PTR)
With 40 weeks remaining in the maintenance phase, six patients increasingly have a focus on their future exercise settings. While two considered outdoor activities like walking, four patients with a preference for a similar tele-exercise program expressed concern about losing access to it after the study, citing logistical challenges.
Well, it is a good thing there are 40 weeks left, and I will possibly come and say that you need to give me 60 weeks more, because this is something I like to do. (Margrethe, 87 years, Maintenance PTR)
Tablet and Home Exercise
The tablet- and dumbbells-equipped program is essential for sustaining engagement in both HPR and PTR groups. For HPR patients, it offers flexible scheduling to optimize physical and mental resources, while weekly consultations and exercise logs provide structure which was especially important for three patients. Further, for four patients, easy access to equipment and home-based environment motivates to follow and complete the exercise program.
Every time I entered that room, that darn step bench was there, you know (laughs), and the weights were over there (smiles). (Julie, 67 years, HPR)
Besides, the logistical benefits for the PTR group, which was accentuated by all six patients, the three highlighted that the tablet provides a feeling of participating in a regular exercise class, normalizing the experience, and reducing self-perceived illness. Furthermore, they stressed that the tablet offers anonymity, enabling patients to feel included without being exposed which motivates to continued engagement and adherence to the group-based exercise sessions.
Well, it’s kind of like being a bit more anonymous when there’s something you can’t do. And if there’s something I can’t do or if I’m out of breath, I don’t feel as obligated to do the exercise as if I were sitting alone in front of the physiotherapist. (Hans, 69 years, Maintenance PTR)
Five patients emphasize the value of anonymity, as more have felt exposed in center-based programs often due to breathlessness or coughing which often led to dropouts.
The social aspect of having to stand in a circle and train in a room—I don’t really want that, or, I don’t know, uh… if I can avoid it, then yes, please. (Knud, 62 years, HPR)
The tablet enables greater individualization and, allows the patients to set their own boundaries more easily which is a consistent motivational factor throughout the maintenance program.
Category 3 – External Support
External Support highlights the ongoing need for external assistance to maintain motivation and sustain engagement throughout the intervention phases. The Facilitating Therapist remains important, while support from Peer Patients evolves to become more significant. Support from relatives, however, remains stable, either as a key motivational factor or with minimal influence.
The Facilitating Therapist
For all patients in both HPR and PTR programs, the therapist plays a crucial role in maintaining motivation and facilitating the development of practical skills, such as managing breathlessness in daily activities. Additionally, the therapist oversees the rehabilitation process, adjusting exercises to individual needs.
You don’t feel completely alone or left to yourself. I mean, there’s someone who follows up on what you’re doing, you know, and checks in on how you’re feeling. (Sally, 73 years, HPR)
This approach promotes a sense of security, unity, and a collaborative alliance, while cultivating a shared responsibility for adherence to the maintenance phase. This collaborative alliance is a consistent important motivational factor throughout the maintenance phase. The growing relationship with the therapist and the maintenance program enhances accountability, helping patients to stay committed and engaged throughout the maintenance phase.
The project is, in a way, (pause) like a spiritual crutch. (Margrethe, 87 years, Maintenance PTR)
Social Environment and Group Identity
The personal preferences and individual identities are being emphasized as a key factor influencing sustained adherence and engagement to the intervention program. Whilst two patients in the HPR group miss the social engagement and sense of unity in a group setting, three patients prefer the individualized nature of the exercise sessions.
Individual program has been important for me, and that has to do with the fact that I am a bit private. It’s not really my thing to seek out group activities like that. (Tom, 78 years, HPR)
All the patients in the PTR value the knowledge sharing and interaction with like-minded individuals. Some appreciate the social aspects, particularly if the disease has limited their social activities, while others prioritize the exercises. Moreover, the mirroring effect of exercising with likeminded people may serve as a motivational driver, encouraging some patients to push their physical limits and improve their performance. Throughout the maintenance phase, expectations of attendance from the therapist and peers help maintain engagement, even during fluctuations in motivation.
I must admit, some days I feel like a dishcloth, thinking I have no energy, no strength, and I don’t feel like I can get enough air (pause). (…) but still, when the time comes, I get the tablet out because there are others who expect you to show up. (Kirsten, 50 years, Maintenance PTR)
The shift to the maintenance phase presents challenges for both HPR and PTR groups. Patients in HPR must adjust from individual exercises to more structured sessions, which for some, despite less flexibility, provides increased motivation and a sense of security, encouraging them to push harder.
(…) I think it has something to do with pulling yourself together and doing it more properly in a group session. (Gertrud, 69 years, Maintenance PTR)
For two in the HPR, the transition is accompanied by fear and may potentially confront the patients with their own physical condition, which can feel intimidating, and thereby reduce their motivation.
This was also my fear for the group training - that I might not keep up because the others would be better than me. (Knud, 62 years, HPR)
In contrast, five from the PTR group struggle to initiate the frequency of self-exercises needed to sustain the previous bi-weekly exercise frequency, particularly when highly motivated by group participation.
You could say it’s easier when I only exercise once a week, but I usually work out on Fridays as well, right?. (…) But I could also end up skipping Friday. It’s harder to do it on my own. (Else, 66 years, Maintenance PTR)
The Influence of the Relatives
The role of support from relatives varies among patients in both the PTR and HPR groups but tends to stay a consistent factor for each individual throughout the maintenance program. For six patients, relatives provide strong motivation through encouragement, reminders, and shared goal setting, while for nine patients, their involvement will likely have little to no effect and may be perceived as intrusive and counterproductive.
No, my husband keeps an eye on whether I’m doing something, and he tries to encourage me, saying, ‘Aren’t you going to do.? – ‘Yes, I’ll wait until tomorrow. (Tina, 86 years, HPR)
In some cases, support from relatives may be perceived as intrusive, particularly for patients without close family, who prefer to keep their illness private.
Discussion
This study provides insight into factors that sustain long-term participation in PR. The primary finding indicates that participants’ motivation for engaging in PR transitions over time, from being driven by fear of illness progression, yet accompanied by hope for improvement of the condition, to a more autonomous and reflective engagement. A home-based setting and support from health professionals were crucial for sustaining adherence and continued involvement.
During the analysis, acceptance of the disease emerged as a recurring theme. Although exploring this aspect was not an explicit aim of the study, it was closely linked to participants’ motivation. Changes in participants’ motivation appeared to be associated with their level of acceptance regarding the significance of various components of the rehabilitation intervention, such as physical activity and symptom management in COPD.
Acceptance and motivation appear to be closely intertwined in a reinforcing cycle, with acceptance of the need for physical activity to maintain the physical function acting as a driver, which transforms and sustains motivation over time. While this connection represents a novel contribution to existing literature, related findings have been reported in previous studies. In an interprofessional intervention with group-based exercises three times a week for 26 weeks, Simonÿ et al found that a prolonged intervention period could provide a raised illness awareness and improve coping strategies.20 Furthermore, Hoaas et al found that after a two-year intervention improved coping strategies and self-efficacy was important in relation to continued engagement and adherence as it affects the cognition and emotions related to a maintenance program.18 While this study did not specifically measure self-efficacy, the TDF domain of beliefs about capabilities is relevant for understanding motivation. This study findings show similar patterns over time, despite our maintenance program being group-based and our participants older.18 Moreover, in the literature, discrepancies are found as some studies highlight hope for improvement and perceived health benefits as great motivational factors,32 while others have found lack of improvement, an increased illness level, and a higher anxiety score as barriers leading to discontinuation.33,34
The study population is accustomed to feeling stigmatized due to the visible symptoms of breathlessness, coughing, and frequent pauses in daily life.35 In contrast, the tablet- and home-based approach offers a sense of normalization and reduces the feeling of being defined by their illness, which is highly motivating and appeared to be a key factor in maintaining engagement with the exercise program. Further, the flexibility to exercise at home eliminates known barriers like transportation to a fitness or rehabilitation center6,36 and supports independence which is essential for ongoing engagement increasing the patients’ autonomy. This is especially important for the patient group included in this study as they have already declined center-based rehabilitation programs.
These factors are aligned with the findings of Cox et al who report a strong perceived autonomy in a home-based telerehabilitation environment that emphasizes support in various ways over an eight-week intervention.37 Nonetheless, direct comparison is more challenging, as our participants declined center-based PR, and our intervention differs in duration, delivery, and its focus on long-term maintenance rather than the short-term rehabilitation.
Gabriel et al explored the views and experiences of patients with COPD after the completion of a 12-month home-based pulmonary telerehabilitation program following hospital admission due to COPD exacerbation. They found that patients expressed approval of the telerehabilitation system, describing it as user-friendly38 even though our study differs regarding the delivery of PR as the interventions in our study are face-to-face, which could result in a greater emphasis on the growing importance of support from the peer patients. Slevin et al also find that using digital health technology promotes a more active role in self-management.39 This suggests that incorporating a digital component into a rehabilitation intervention can enhance its effectiveness across varying disease and symptom severities, promoting sustained adherence and motivation, especially when combined with the support of a therapist and engagement with peer patients.
Our study emphasizes that external support is a critical and consistent motivational factor for maintaining patients’ engagement in the program, which is a recurrent theme throughout the literature and is addressed in several motivational and behavioral science theories.32,34,40–42 In the literature, social support has primarily been seen in the context of traditional, center-based PR programs with face-to-face contact.33,41,43,44 Yet, emerging research highlights that social support remains a crucial factor for engagement and motivation in a home-based, telerehabilitation context.20,37,38 Also, these studies show that various forms of remote communication effectively can promote social support, proving it is not limited to physical proximity – aligning with our findings.20,37,38
Our findings differ from the current literature, in which relatives are described as having a multidimensional role in supporting patients’ self-management and motivation living with a chronic disease.45,46 While this holds true for some of our patients, others preferred to keep their relatives uninvolved. This preference may stem from either having few close relatives or a desire to maintain boundaries between personal relationships and medical treatment. Additionally, some patients viewed illness as a private matter, which influenced their decision to exclude their next of kin in the rehabilitation process. This could also explain why peer patients become increasingly important in relation to engagement in the maintenance program.
The results suggest that for this patient group has the potential for greater acceptance of continued participation in a maintenance program, if it includes peer support, therapist guidance and support, and remote program delivery methods to overcome logistical barriers, such as a tablet-based videoconferencing system.
Strengths and Limitations
Our study has strengths and limitations. To our knowledge, this is the first study to examine how perceptions of motivation and factors related to engagement evolve over time during a maintenance group-based tele-rehabilitation program for patients with moderate to very severe COPD who have declined traditional center-based PR. The TDF is a well-recognized framework to ensure a thorough and structured elaboration on factors affecting motivation and adherence. By using this framework to develop the interview guides and the initial coding we were able to explore multiple areas in a systematic and transparent way. Nevertheless, using a framework can overlook excluded elements.
Therefore, we first conducted the deductive analysis and then applied an unconstrained matrix based on inductive principles to capture perspectives crossing various domains. By not using a specific motivational theory to guide the analytical process, the study allowed for a broader range of findings and opened for new and alternative perspectives. This approach provided insights on a more structural level, highlighting how various factors important to patients influenced and evolved their level of engagement and motivation throughout the maintenance period. Furthermore, we aimed to enhance trustworthiness by double-coding every third interview, allowing for deeper insights, broader perspectives, and continuous validation of findings. However, using a specific theory might have enabled a more specific focus on motivation and potentially allowed for deeper exploration of its evolvement over time. We used a longitudinal recurrent cross-sectional design to explore motivation and engagement over time in a patient group prone to dropout and hospitalization. While this limited within-person comparisons, we prioritized interviewing the same individuals at the two time points when possible. A trajectory design could have offered deeper individual insights but was impractical due to high attrition and clinical vulnerability. Finally, it should be noted that this program was tested within the Danish healthcare system, where participation is free of charge. In settings with user fees, economic constraints may pose an additional barrier, potentially affecting patients’ motivation and engagement to continue.
Conclusion
Over a 25-week period, patients’ perceptions of their COPD shifted toward greater acceptance, which strengthened their motivation to stay active. What began as motivation driven by fear of decline and hope for improvement developed into a more deliberate commitment to ongoing exercise. Continued engagement was supported by therapist guidance, peer interaction, and the flexibility of home-based rehabilitation, emphasizing the crucial role of external support and a structured setting in sustaining participation in long-term programs. These factors should be taking into consideration in the design of future rehabilitation programs by addressing the individual needs, thereby optimizing the long-term benefits for patients with COPD.
Data Sharing Statement
Data access in Denmark is under strict juristic data protection law as imposed by the Danish Ministry of Justice. Any possible access or sharing demands a part application to: (1) Danish Data Protection Agency (email: [email protected]), (2) Ethics Committee of the Capital Region (email: [email protected]), (3) National Health Data Authorities (email: [email protected]). Only if the applications are approved will the data be considered available for sharing.
Acknowledgment
We sincerely thank the patients for their open-minded participation in this intervention and their generous sharing of experiences, insights, and perspectives. We thank the steering committee and all the participating departments of respiratory medicine, municipalities, departments of physiotherapy and occupational therapy for their involvement and making the necessary resources available and the conduction of this study possible. Furthermore, we thank the Danish Lung Foundation, Telemedical Center Regional Capital Copenhagen, TrygFonden, Danish Association for Physiotherapists, Jascha Fonden, Skibsreder Per Henriksen, R og Hustrus fond, Amager-Hvidovre Hospital Forskningspulje and Lundbeck Fonden for their founding support.
Disclosure
Ms Maria Olsen reports grants from Danish Lung Foundation, grants from Telemedical Center Regional Capital Copenhagen, grants from TrygFonden, grants from Danish Association for Physiotherapists, grants from Jascha Fonden, grants from Skibsreder Per Henriksen, R og Hustrus fond, grants from Amager-Hvidovre Hospital Forskningspulje, grants from Lundbeck Fonden, during the conduct of the study. Prof. Dr. Henrik Hansen reports grants from Trygfonden, grants from Lung foundation Denmark, grants from Jascha foundation, grants from Telemedicine center capital region of Copenhagen, grants from Association of Danish Physiotherapist, during the conduct of the study. No potential conflict of interest is reported by the authors.
References
1. Venkatesan P. GOLD COPD report: 2024 update. Lancet Respir Med. 2023;12(1):15.
2. Naghavi M, Ong KL, Aali A, et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet. 2024:403(10440); 2100–2132.
3. Rochester CL, Alison JA, Carlin B, et al. Pulmonary rehabilitation for adults with chronic respiratory disease: an official American Thoracic Society clinical practice guideline. Am J Respir Crit Care Med. 2023;208(4):E7–26. doi:10.1164/rccm.202306-1066ST
4. Spruit MA, Singh SJ, Garvey C, et al. An official American thoracic society/European respiratory society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–e64. doi:10.1164/rccm.201309-1634ST
5. Rochester CL, Vogiatzis I, Holland AE, et al. An Official American Thoracic Society/European Respiratory Society Policy Statement: enhancing Implementation, Use, and Delivery of Pulmonary Rehabilitation. Am J Respir Crit Care Med. 2015;192(11):1373–1386. doi:10.1164/rccm.201510-1966ST
6. Keating A, Lee A, Holland AE. What prevents people with chronic obstructive pulmonary disease from attending pulmonary rehabilitation? A systematic review. Chron Respir Dis. 2011;8(2):89–99. doi:10.1177/1479972310393756
7. Fischer MJ, Scharloo M, Abbink JJ, et al. Drop-out and attendance in pulmonary rehabilitation: the role of clinical and psychosocial variables. Respir Med. 2009;103(10):1564–1571. doi:10.1016/j.rmed.2008.11.020
8. Holland A, Dal Corso SSM. Pulmonary rehabilitation. In: Hurst JR, editor. ERS Mongraph. Vol. 1.
9. Cox NS, Dal Corso S, Hansen H, et al. Telerehabilitation for chronic respiratory disease. Cochrane Database of Systematic Reviews. 2021;2021.
10. Pimenta S, Hansen H, Demeyer H, Slevin P, Cruz J. Role of digital health in pulmonary rehabilitation and beyond: shaping the future. ERJ Open Res. 2023;9(2):00212–2022. doi:10.1183/23120541.00212-2022
11. Holland AE, Mahal A, Hill CJ, et al. Home-based rehabilitation for COPD using minimal resources: a randomised, controlled equivalence trial. Thorax. 2017;72(1):57–65. doi:10.1136/thoraxjnl-2016-208514
12. Hansen H, Bieler T, Beyer N, et al. Supervised pulmonary tele-rehabilitation versus pulmonary rehabilitation in severe COPD: a randomised multicentre trial. Thorax. 2020;75(5):413–421. doi:10.1136/thoraxjnl-2019-214246
13. Ries AL, Kaplan RM, Myers R, Prewitt LM. Maintenance after pulmonary rehabilitation in chronic lung disease: a randomized trial. Am J Respir Crit Care Med. 2003;167(6):880–888. doi:10.1164/rccm.200204-318OC
14. Blervaque L, Préfaut C, Forthin H, et al. Efficacy of a long-term pulmonary rehabilitation maintenance program for COPD patients in a real-life setting: a 5-year cohort study. Respir Res. 2021;22(1). doi:10.1186/s12931-021-01674-3
15. Silva L, Maricoto T, Costa P, Berger-Estilita J, Padilha JM. A meta-analysis on the structure of pulmonary rehabilitation maintenance programmes on COPD patients’ functional capacity. Npj Primary Care Respiratory Medicine. Nature Research. 2022;32.
16. Candemir İ, Ergün P, Şahin ME. Maintenance of pulmonary rehabilitation benefits in patients with COPD: is a structured 5-year follow-up program helpful? Turk J Med Sci. 2021;51(6):2915–2923. doi:10.3906/sag-2101-245
17. Güell MR, Cejudo P, Ortega F, et al. Benefits of long-term pulmonary rehabilitation maintenance program in patients with severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;195(5):622–629. doi:10.1164/rccm.201603-0602OC
18. Hoaas H, Andreassen HK, Lien LA, Hjalmarsen A, Zanaboni P. Adherence and factors affecting satisfaction in long-term telerehabilitation for patients with chronic obstructive pulmonary disease: a mixed methods study eHealth/ telehealth/ mobile health systems. BMC Med Inform Decis Mak. 2016;16(1). doi:10.1186/s12911-016-0264-9
19. Wen J, Milne S, Sin DD. Pulmonary rehabilitation in a postcoronavirus disease 2019 world: feasibility, challenges, and solutions. Current Opinion in Pulmonary Medicine. 2022;28:152–161. doi:10.1097/MCP.0000000000000832
20. Simonÿ C, Andersen IC, Bodtger U, Nyberg M, Birkelund R. Raised illness mastering–a phenomenological hermeneutic study of chronic obstructive pulmonary disease patients’ experiences while participating in a long-term telerehabilitation programme. Disabil Rehabil Assist Technol. 2022;17(5):594–601. doi:10.1080/17483107.2020.1804630
21. McNamara RJ, Dale M, McKeough ZJ. Innovative strategies to improve the reach and engagement in pulmonary rehabilitation. Journal of Thoracic Disease. AME Publishing Company. 2019;11:S2192–9. doi:10.21037/jtd.2019.10.29
22. Chevance G, Héraud N, Varray A, Boiché J. Change in explicit and implicit motivation toward physical activity and sedentary behavior in pulmonary rehabilitation and associations with postrehabilitation behaviors. Rehabil Psychol. 2017;62(2):119–129. doi:10.1037/rep0000137
23. Ryan RM, Deci EL. Intrinsic and Extrinsic Motivations: classic Definitions and New Directions. Contemp Educ Psychol. 2000;25(1):54–67. doi:10.1006/ceps.1999.1020
24. Cambridge University Press & Assessment. Engagement noun (INTEREST); 2025.
25. Nielsen C, Godtfredsen N, Molsted S, Ulrik C, Kallemose T, Hansen H. Supervised pulmonary tele-rehabilitation and individualized home-based pulmonary rehabilitation for patients with COPD, unable to participate in center-based programs. The protocol for a multicenter randomized controlled trial - the REPORT study. PLoS One. 2025;20(1):e0312742. doi:10.1371/journal.pone.0312742
26. Grossoehme D, Lipstein E. Analyzing longitudinal qualitative data: the application of trajectory and recurrent cross-sectional approaches. BMC Res Notes. 2016;9(1). doi:10.1186/s13104-016-1954-1
27. Bennett D, Kajamaa A, Johnston J. How to … do longitudinal qualitative research. The Clinical Teacher. 2020;17:489–492. doi:10.1111/tct.13203
28. Heerema-Poelman A, Stuive I, Wempe JB. Adherence to a maintenance exercise program 1 year after pulmonary rehabilitation: what are the predictors of dropout? J Cardiopulm Rehabil Prev. 2013;33(6):419–426. doi:10.1097/HCR.0b013e3182a5274a
29. Cane J, O’connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implementation Science. 2012;7(37). doi:10.1186/1748-5908-7-37
30. Atkins L, Francis J, Islam R, et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implementation Science. 2017;12(1). doi:10.1186/s13012-017-0605-9
31. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
32. Sohanpal R, Steed L, Mars T, Taylor SJC. Understanding patient participation behaviour in studies of COPD support programmes such as pulmonary rehabilitation and self-management: a qualitative synthesis with application of theory. NPJ Prim Care Respir Med. 2015;25. doi:10.1038/npjpcrm.2015.54
33. Yohannes AM, Casaburi R, Dryden S, Hanania NA. Predictors of premature discontinuation and prevalence of dropouts from a pulmonary rehabilitation program in patients with chronic obstructive pulmonary disease. Respir Med. 2022;193:106742. doi:10.1016/j.rmed.2022.106742
34. O’shea SD, Taylor NF, Paratz JD. But watch out for the weather factors affecting adherence to progressive resistance exercise for persons with COPD [Internet]. Available from: www.jcrjournal.com.
35. Halding AG, Heggdal K, Wahl A. Experiences of self-blame and stigmatisation for self-infliction among individuals living with COPD. Scand J Caring Sci. 2011;25(1):100–107. doi:10.1111/j.1471-6712.2010.00796.x
36. Skibdal KM, Emme C, Hansen HLTM. A mixed-methods study of thoughts and attitudes towards participation in pulmonary telerehabilitation among people with severe and very severe COPD who declined participation in pulmonary rehabilitation. Patient Prefer Adherence. 2022;16:2781–2798. doi:10.2147/PPA.S380832
37. Cox NS, Lee JYT, McDonald CF, et al. Perceived autonomy support in telerehabilitation by people with chronic respiratory disease: a mixed methods study. Chest. 2023;163(6):1410–1424. doi:10.1016/j.chest.2022.12.023
38. Gabriel AS, Parvanova I, Finkelstein J. Patient perspectives on long-term use of a pulmonary telerehabilitation platform: a qualitative analysis. In: Studies in Health Technology and Informatics. IOS Press BV; 2023:982–986.
39. Slevin P, Kessie T, Cullen J, Butler MW, Donnelly SC, Caulfield B. Exploring the potential benefits of digital health technology for the management of COPD: a qualitative study of patient perceptions. ERJ Open Res. 2019;5(2):00239–2018. doi:10.1183/23120541.00239-2018
40. Souto-Miranda S, Dias C, Jácome C, Melo E, Marques A. Long-term maintenance strategies after pulmonary rehabilitation: perspectives of people with chronic respiratory diseases, informal carers, and healthcare professionals. Healthcare. 2022;10(1).
41. Hellem E, Bruusgaard KA, Bergland A. Exercise maintenance: COPD patients’ perception and perspectives on elements of success in sustaining long-term exercise. Physiother Theory Pract. 2012;28(3):206–220. doi:10.3109/09593985.2011.587502
42. Karloh M, Matias TS, de Oliveira JM, et al. Breaking barriers to rehabilitation: the role of behavior change theories in overcoming the challenge of exercise-related behavior change. Brazilian Journal of Physical Therapy. Revista Brasileira de Fisioterapia. 2023;27.
43. Desveaux L, Rolfe D, Beauchamp M, Goldstein R, Brooks D. Participant experiences of a community-based maintenance program post-pulmonary rehabilitation. Chron Respir Dis. 2014;11(1):23–30. doi:10.1177/1479972313516880
44. Collado-Mateo D, Lavín-Pérez AM, Peñacoba C, et al. Key factors associated with adherence to physical exercise in patients with chronic diseases and older adults: an umbrella review. International Journal of Environmental Research and Public Health. 2021;18:1–24. doi:10.3390/ijerph18042023
45. Whitehead L, Jacob E, Towell A, Abu-Qamar M, Cole-Heath A. The role of the family in supporting the self-management of chronic conditions: a qualitative systematic review. J Clin Nurs. 2018;27(1–2):22–30. doi:10.1111/jocn.13775
46. Schulman-Green D, Feder SL, Dionne-Odom JN, et al. Family caregiver support of patient self-management during chronic, life-limiting illness: a qualitative metasynthesis. J Fam Nurs. 2021;27(1):55–72. doi:10.1177/1074840720977180
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.