Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Why the COPD Microbiome Matters: How Airway Microbes Shape Disease Severity and Treatment Response
Authors Jia S, Liu P, Zhang H, Zeng H, Chen G, Zhao L
Received 5 November 2025
Accepted for publication 13 February 2026
Published 17 March 2026 Volume 2026:21 531521
DOI https://doi.org/10.2147/COPD.S531521
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Shuying Jia,1 Panpan Liu,2 Huali Zhang,2 Haizhu Zeng,2 Guo Chen,3 Lei Zhao2
1School of Gongli Hospital Medical Technology, University of Shanghai for Science and Technology, Shanghai, People’s Republic of China; 2Department of Pulmonary and Critical Care Medicine, Shanghai Pudong New Area Gongli Hospital, Shanghai, People’s Republic of China; 3Department of Emergency Medicine, Shanghai Pudong New Area Gongli Hospital, Shanghai, People’s Republic of China
Correspondence: Lei Zhao, Department of Pulmonary and Critical Care Medicine Shanghai Pudong New Area Gongli Hospital, Shanghai, People’s Republic of China, Tel +86 21-58858730-5339, Email [email protected] Guo Chen, Department of Emergency Medicine, Shanghai Pudong New Area Gongli Hospital, Shanghai, People’s Republic of China, Tel +86 21-58858730, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is a heterogeneous disease caused by multiple factors, with diverse clinical manifestations leading to varying treatment outcomes. Dysbiosis of the respiratory microbiome is one of the key contributors to this variability.
Objective and Methods: Due to differences in microbial detection technologies and sample collection methods, studies on the characteristics of respiratory prokaryotic microbiota and how these microbes influence host functions in COPD patients have yielded variable results. In this review, we conducted a comprehensive search of relevant literature from PubMed, ScienceDirect, and Elsevier, summarizing studies on the characteristics and functional analyses of prokaryotic microbiota under various technical approaches. The goal was to identify common patterns of microbiota changes in COPD across different disease states, as well as individual microbial influences on host functions.
Results: Compared with healthy adults, in stable-phase COPD patients, the relative abundance of Prevotella species in the Bacteroidetes phylum is significantly reduced. During acute exacerbations, the predominant microbiota is composed of Moraxella, Haemophilus, and Streptococcus species from the Proteobacteria and Firmicutes phyla. Clinical indicators in COPD patients are correlated with the abundance of Streptococcus (Firmicutes) and Prevotella (Bacteroidetes) species. Furthermore, the different phyla of respiratory prokaryotic microbiota are associated with innate immunity, metabolism, and inflammation factors related to COPD.
Conclusion: This review summarizes evidence on dynamic changes in the airway prokaryotic microbiome during COPD progression. It highlights the dual role of these microbial changes as biomarkers of disease progression and modifiable targets for personalized care. Observed patterns—such as reduced Prevotella abundance in stable disease and the dominance of Moraxella, Haemophilus, and Streptococcus during acute exacerbations—provide a basis for stratifying patients and designing individualized treatment plans. Microbiome analysis may aid in early identification of high-risk patients for preventive strategies, guide pathogen-specific antimicrobial or immunomodulatory therapy, and allow treatment response to be monitored through microbial shifts. By linking distinct microbial profiles to host immune and inflammatory pathways, this approach supports the development of tailored interventions to restore microbial balance. These strategies could improve clinical outcomes and advance precision medicine in COPD management.
Keywords: chronic obstructive pulmonary disease, COPD, airway microbiome, prokaryotic microorganisms, dysbiosis, disease endotype, microbial composition, airway inflammation, host-microbiome interaction
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic respiratory disease caused by abnormalities in the airways and/or alveolar structures, primarily characterized by symptoms such as breathlessness, cough, and sputum production.1 COPD is one of the leading causes of death worldwide, with approximately 3 million people dying from COPD each year. With the continued exposure to risk factors and the aging global population, it is expected that by 2060, the number of COPD-related deaths will exceed 5.4 million,2,3 posing significant challenges to global economies and societies.
COPD is primarily diagnosed and assessed for risk stratification through pulmonary function tests, chest imaging, relevant laboratory tests, symptom evaluation, and the GOLD grading system.4 With the continuous advancement of medical standards, patients can alleviate their symptoms through various treatments such as medications (eg, bronchodilators, inhaled corticosteroids), oxygen therapy, pulmonary rehabilitation, surgical interventions, and vaccination.5 Moreover, as research into the molecular mechanisms of the disease progresses, new therapeutic approaches such as biologics (eg, dupilumab) and pharmacogenomics are gradually coming into focus.6 The development of COPD involves multiple mechanisms, including inflammation, oxidative stress, imbalance of protease/antiprotease, cell death and apoptosis, genetic and environmental factors, microbial infections, immune dysfunction, and metabolic disorders. The pathological process reflects the complex interplay of multiple factors, pathways, and levels. Despite advances in the study of COPD mechanisms, effective treatments for inhibiting disease progression and addressing the physiological decline, fatigue, and frailty associated with COPD are still lacking.
The heterogeneity of COPD presents a significant challenge in clinical management. This heterogeneity manifests in phenotypes such as frequent exacerbations and rapid lung function decline, which are associated with distinct patterns of airway microbiota dysbiosis. Phenotype-specific dysbiosis—ranging from a loss of microbial antagonistic networks to an increased pathogen burden—directly correlates with clinical severity. Mechanistically, dysbiosis perpetuates the disease through sustained activation of innate immune pathways. Upregulation of TLR4 and NOD1/2 by microbial ligands drives NF-κB–dependent inflammation, while a dysbiosis-induced Th17/IL-17 axis exacerbates neutrophilic influx and remodeling. Concomitant alterations in immunomodulatory microbial metabolites further disrupt host homeostasis.7 Elucidating these microbe–host interactions establishes a critical framework for advancing personalized management strategies in COPD.
Dysbiosis of the respiratory microbiota has been shown to play a key role in various chronic respiratory diseases, including COPD, asthma, bronchiectasis, and idiopathic pulmonary fibrosis (IPF).3 These diseases often involve impaired airway clearance, leading to microbial imbalance in the airways, which exacerbates inflammation and drives disease progression.8,9 Studies indicate that the respiratory tract hosts not only bacteria but also fungi, viruses, and other microbial communities. The structure of these microbial communities and their metabolic products can modulate the host’s immune response and inflammation levels,10 and are closely linked to the risk of acute exacerbation, disease severity, and mortality. The interaction between microbial communities and the host may provide potential therapeutic targets for improving the progression of chronic respiratory diseases. Recent studies suggest that microbial therapies, such as probiotics, antibiotic interventions, or microbial modulation, may have a positive impact on the treatment of COPD, particularly in regulating immune function and alleviating inflammation, offering new insights and methods for COPD management.
Although progress has been made in the study of respiratory microbiota, research on COPD remains predominantly focused on bacterial communities, and inconsistencies across studies are often due to differences in the techniques and sampling methods used. Current research mainly employs techniques such as 16S rRNA sequencing, metagenomics, transcriptomics, and metabolomics to analyze the composition of prokaryotic microbiota in the respiratory tract and their interactions with the host.11–13 However, differences in analytical methods and sampling can lead to varied conclusions across studies. Therefore, this review aims to systematically search databases such as PubMed, ScienceDirect, and Elsevier using the keywords “COPD, microbiota, respiratory tract,” to integrate the findings from different studies, explore the role of respiratory prokaryotic microbiota in COPD, and provide insights into the mechanisms of microbial imbalance in COPD for further investigation, early diagnosis, and the development of therapeutic strategies.
Characteristics of Respiratory Prokaryotic Microbiota in Stable and Acute Exacerbation Stages of COPD
Respiratory Prokaryotic Microbiota Diversity in Stable COPD Patients
At the genus level, a study by Rong Wang on sputum samples from 52 stable COPD patients revealed that the most common prokaryotic microbiota were Streptococcus (29.32%) and Gemella (6.74%) from the phylum Firmicutes, Granulicatella (4.68%) from the phylum Firmicutes, Rothia (22.31%) from the phylum Actinobacteria, and Leptotrichia (4.30%) from the phylum Fusobacteria.14 In another study by Hazra et al, sputum samples from 29 COPD patients 12 with moderate COPD and 17 with severe COPD and healthy individuals showed that in the moderate COPD cohort, the five most common genera were Streptococcus (28.2%), Rothia (11.4%), Prevotella (8.3%), Porphyromonas (7.9%), and Neisseria (6.2%).15 In the severe COPD cohort, the dominant genera were Streptococcus (20.2%), Prevotella (11.7%), Porphyromonas (10.1%), Leptotrichia (5.9%), and Rothia (5.3%). In contrast, Prevotella (16.5%) was the most common genus in healthy individuals, followed by Streptococcus (13.0%), Neisseria (7.1%), Fusobacterium (6.6%), and Bacteroides (6.2%).16,17
Bouquet et al18 analyzed microbial load in 446 spontaneous sputum samples from stable COPD patients, finding that Prevotella, Veillonella, Haemophilus, and Streptococcus were the most common genera. Notably, microbiota dominated by Prevotella displayed higher respiratory microbial diversity. Studies by Wang Z (2020),13 Wang J (2020),19 Dicker A. J. (2021),20 and Yang C. Y. (2021)21 also reported a significant reduction in the relative abundance of Prevotella in sputum samples from COPD patients.
Ramsheh et al22 analyzed 546 bronchial brush samples from healthy individuals and COPD patients, with 214 healthy individuals showing a relative abundance of Prevotella (45.3%), Streptococcus (7.7%), and Moraxella (0.39%). In 360 stable COPD patients, the relative abundance of Prevotella was 33.2%, Streptococcus 12.2%, and Moraxella 2.3%. This study highlighted that Prevotella (Bacteroidetes), Streptococcus (Firmicutes), and Moraxella (Proteobacteria) were the most distinguishing genera between COPD patients and healthy individuals. Compared with healthy individuals, COPD patients showed a significant decrease in Prevotella and a significant increase in Streptococcus and Moraxella. Both genus-level and phylum-level studies indicate that while there is no significant difference in the phylum-level microbiota of stable COPD patients compared to healthy individuals, there are differences in the relative abundance of different phyla. At the genus level, however, the composition and abundance of microbial communities show significant differences.
In conclusion, the relative abundance of Prevotella (Bacteroidetes) is significantly reduced in the respiratory tract of stable COPD patients. Given that bronchial brush and bronchoalveolar lavage fluid samples provide deeper insight into lung microbiota, changes in the relative abundance of Prevotella are more pronounced in these samples. Nevertheless, regardless of the sampling method, an increase in the relative abundance of Streptococcus and Moraxella and a decrease in Prevotella in COPD patients may serve as potential biomarkers for diagnosing COPD (Table 1, Figures 1 and 2).
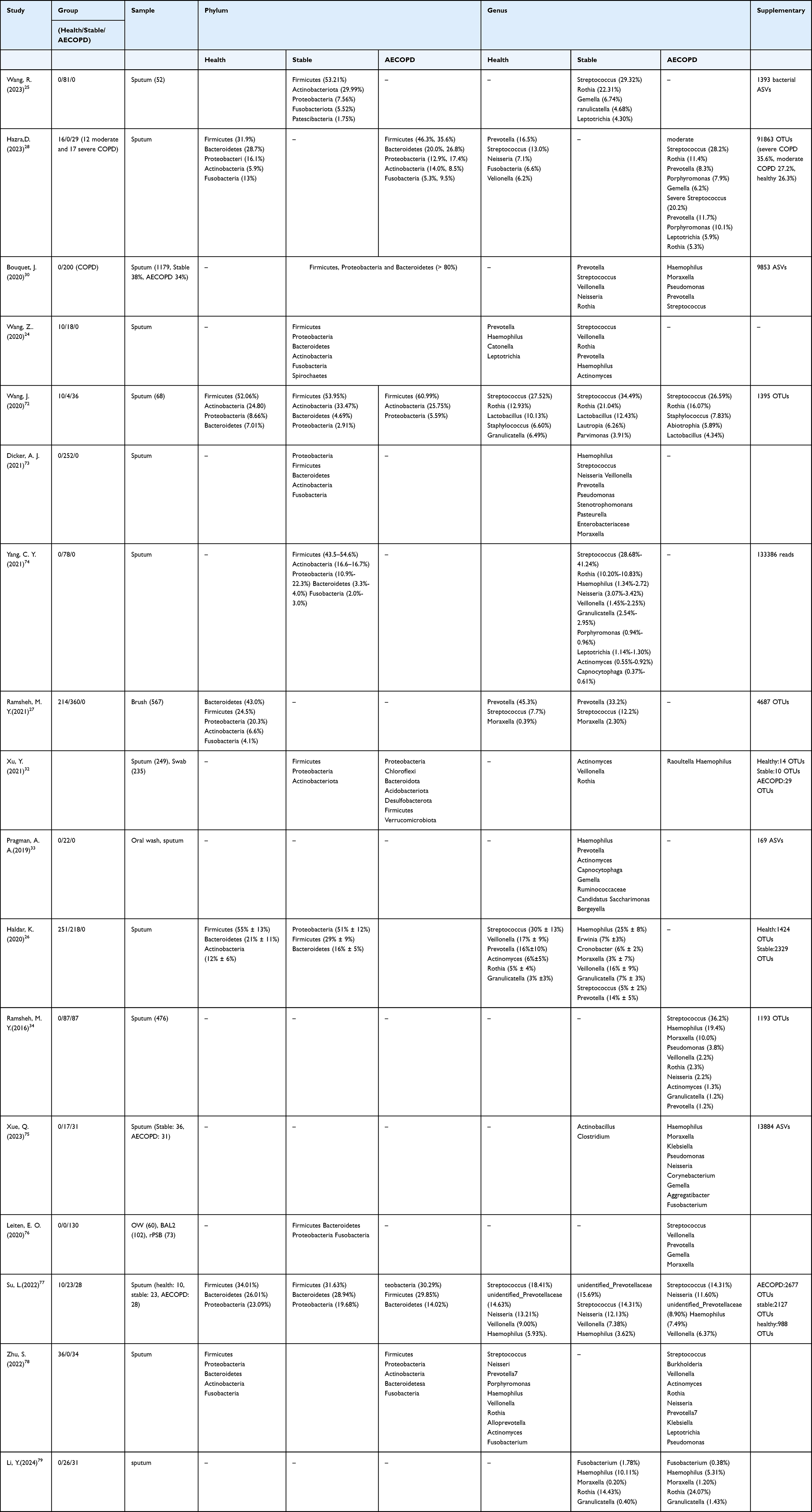 |
Table 1 List of Airway Microbiome Studies in Acute exacerbate and stable COPD |
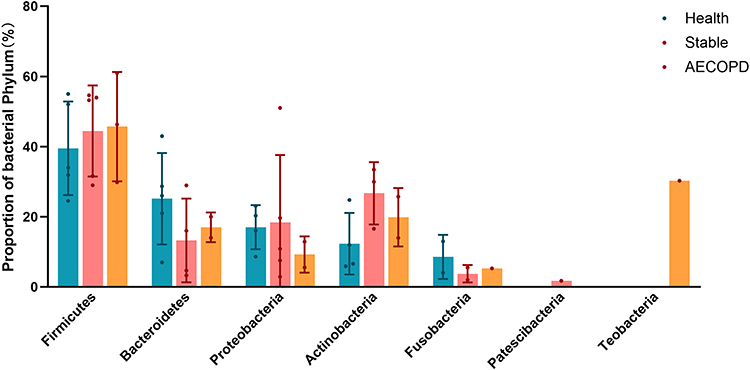 |
Figure 1 Relative abundance of major bacterial phyla in healthy, stable, and AECOPD states. |
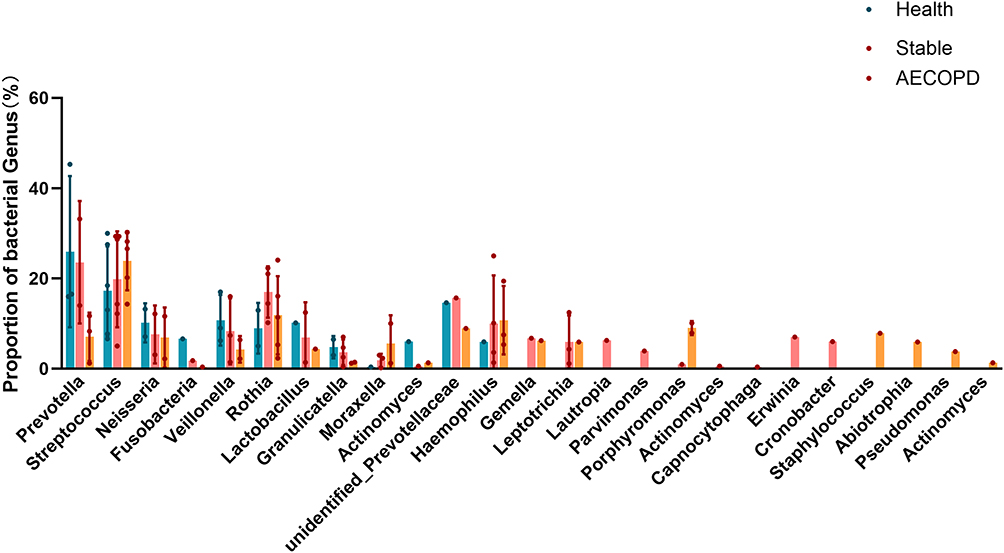 |
Figure 2 Comparison of the relative abundance of major bacterial genera in healthy, stable, and AECOPD states. |
Respiratory Prokaryotic Microbiota Diversity in Acute Exacerbation of COPD
According to the GOLD 2023 guidelines, acute exacerbation of COPD (AECOPD) is defined as an event characterized by increased shortness of breath, cough, and sputum production, lasting less than 14 days, and usually associated with increased local and systemic inflammation due to infection, pollution, or other airway damage.30 AECOPD is a leading cause of mortality in COPD patients, with Chinese COPD patients experiencing 1–4 exacerbations per year. Respiratory infections are the most common cause of AECOPD, and the microbiome plays a crucial role during this acute phase.
Yanyan Xu et al32 analyzed 249 sputum samples from six core families to investigate airway microbiome differences between healthy controls, stable COPD, and AECOPD patients. They found that compared to healthy individuals, AECOPD patients had a higher relative abundance of certain bacterial phyla, including Proteobacteria, Chloroflexi, Bacteroidota, Acidobacteriota, Desulfobacterota, Firmicutes, and Verrucomicrobiota. Specifically, within the Proteobacteria phylum, the relative abundance of Gammaproteobacteria (eg, Haemophilus) and Alphaproteobacteria was increased during AECOPD. Furthermore, at the genus level, Raoultella (Proteobacteria) and Haemophilus (Proteobacteria) showed a significant increase in AECOPD patients. Pragman, A. A.’s study33 of sputum samples from 11 patients with frequent acute exacerbations found that these patients exhibited a higher relative abundance of Gammaproteobacteria, especially Haemophilus and Moraxella, which were notably enriched in this phylum. Similarly, Koirobi Haldar et al reported that Proteobacteria accounted for 50% of the microbiota in COPD patients, with Haemophilus and Moraxella representing 25% and 3% of the microbiome, respectively, underscoring the importance of Gammaproteobacteria in COPD.15
Additionally, research by Wang, Z (2020)19 and others has shown that during AECOPD, the relative abundance of Proteobacteria increases, while that of Firmicutes decreases. Notably, Moraxella exhibits the most significant change during exacerbations, with a marked increase in relative abundance, followed by a decrease in Streptococcus and an increase in Haemophilus. Recent studies by Leiten, E. O. (2020),34 Su, L. (2022),35 Zhu, S. F. (2022),7 Qing Xue (2023),36 and Li, Y. (2024)4 also confirmed these findings, further establishing the close association between Gammaproteobacteria and acute exacerbations in COPD patients. Therefore, regular monitoring of related genera such as Haemophilus and Moraxella within Gammaproteobacteria in healthy individuals and stable COPD patients can provide valuable insights for predicting and managing AECOPD exacerbations.
Correlation Between Respiratory Prokaryotic Microbiota and Lung Function in COPD Patients
Studies have demonstrated a significant correlation between lung function levels and the characteristics of the respiratory microbiota in COPD patients. However, there are some discrepancies and controversies in the findings across different studies. Opron et al collected bronchial biopsy samples from 181 individuals, including non-smokers and smokers (with or without COPD), and found that the abundance of genera such as Streptococcus, Staphylococcus, Prevotella, and Gemella was negatively correlated with FEV1/FVC, FEV1, and FEF25-75%. Specifically, among ex-smokers without COPD, the abundance of Staphylococcus, Prevotella, Streptococcus, and Veillonella was negatively correlated with the FEV1/FVC ratio, FEV1% predicted value, and/or FEF25-75%.37,38 Madapoosi et al reported in a study of 126 mild stable COPD patients that the relative abundance of Streptococcus was positively correlated with FEV1, while Prevotella showed a negative correlation with FEV1.39 In contrast, Ramsheh et al analyzed bronchial brushing samples from 339 stable COPD patients and found a positive correlation between the relative abundance of Prevotella and post-bronchodilator FEV1 and FEV1/FVC ratio.22 In COPD patients with 50% ≤ FEV1 < 80%, the most common genera were Streptococcus (28.2%), Rothia (11.4%), Prevotella (8.3%), Porphyromonas (7.9%), and Gemella (6.2%).16
Erb-Downward et al analyzed lung tissue from 6 patients who had undergone lung transplantation due to advanced COPD and found that the presence of Pseudomonas was closely associated with impaired lung function.23 Millares et al analyzed sputum samples from 72 stable COPD patients and found that in those with more severe airflow limitation, the relative abundance of Pseudomonas significantly increased, while Treponema was less abundant. The observed changes in the respiratory microbiome were primarily characterized by reductions in specific genera, some of which were replaced by Pseudomonas.26 Furthermore, Ramsheh et al combined bronchial brushing samples from 9 COPD patients (aged 45–75 years) with the BODE index (including body mass index, airflow obstruction, dyspnea, and 6-minute walking distance). Their analysis revealed that the abundance of Prevotella was negatively correlated with the severity of COPD symptoms and positively correlated with exercise capacity.22
However, Pragman et al analyzed nasal swabs, throat swabs, and sputum samples from 14 COPD patients and found that bacterial biomass was site-specific, showing no significant differences related to age or FEV1% predicted, which contradicted previous findings.30
In conclusion, lung function-related indicators (such as FEV1, FEV1/FVC, and FEV1% predicted values) are significantly correlated with the relative abundance of genera such as Streptococcus (Firmicutes), Prevotella (Bacteroidota), and Pseudomonas (Proteobacteria). In particular, the relative abundance of Pseudomonas is significantly associated with more severe airflow limitation in COPD patients. Thus, future research should focus on the dynamic changes in these three genera to better clarify their relationship with lung function indicators and address the discrepancies between various study results.
Host-Microbe Interactions and Their Impact in COPD Patients
The host-microbiome relationship in the respiratory tract refers to the interaction between the host and microorganisms. Microbes produce various factors that confer virulence or promote colonization through other means, triggering molecular and cellular responses in the host, which may either help maintain health or induce disease.27 This reflects the focus of research on the dynamic interactions between the host and microbes. In COPD patients, the primary prokaryotic microorganisms involved in strong host-microbe interactions in the respiratory tract include Prevotella, Streptococcus, Pseudomonas, Lactobacillus, and Haemophilus.
Interaction Between COPD Patients and Prevotella
Prevotella is an anaerobic Gram-negative bacterium under the Bacteroidetes phylum, primarily involved in the breakdown of proteins and carbohydrates, and is considered an opportunistic pathogen. Previous studies have shown that the relative abundance of Prevotella in the respiratory tract of stable COPD patients is significantly lower compared to healthy individuals, and during the acute phase of COPD, the relative abundance of Prevotella is also significantly decreased compared to stable patients.13,19–21 Some studies suggest that Prevotella and Moraxella are significantly correlated with the host’s respiratory transcriptome profile, especially genes involved in immune and inflammatory responses, indicating that these bacteria may play a dominant role in host-microbe interactions in COPD.24
In healthy individuals, the high abundance of Prevotella is associated with the regulation of tight junction protein expression, which may promote innate immunity by directly acting on the epithelium or by upregulating Toll-like receptors (TLRs), thereby reducing the permeability of lung epithelial cells. The weak TLR-stimulating ability of Prevotella may trigger mild inflammatory responses that help clear the bacteria but also protect the lungs from pathogens and chronic diseases under balanced conditions. In addition, the abundance of Moraxella is associated with epithelial cell-derived IL-17 and TNF inflammatory features, which may be due to the effect of lipopolysaccharides on TLRs. The interaction between Prevotella and Moraxella might be related to their abundance differences and the TLR-stimulating ability caused by the different types of lipopolysaccharides they produce. The host lung gene expression profile shows a significant correlation with Prevotella and Moraxella, but not with Streptococcus.26 Studies indicate that in the case of lung dysbiosis, the pathogenic Proteobacteria increase, while Prevotella decreases. Prevotella can exert a protective role by modulating the host’s immune response.
Moreover, Prevotella can directly regulate TLR2 immune responses in lung innate immunity, inducing changes in immune system functions and development. By occupying ecological niches in the microbiome, Prevotella inhibits the colonization or infection of Proteobacteria and may act by directly killing them.24 This suggests that Prevotella and Moraxella participate in the pathogenesis of COPD by regulating the innate immunity of COPD patients.
In terms of amino acid metabolism, Prevotella is positively correlated with adenosine monophosphate (AMP) and adenosine, which regulate the volume of respiratory surface fluids.39 Studies have also shown that Prevotella can modulate adenosine metabolism and the methionine (PSC) metabolic pathway,25 and preclinical and clinical studies have explored targeted compounds for these metabolic pathways.28,40 For example, one study found that increased bacterial metabolite L-tyrosine, by elevating PSC levels, protected the host from allergic airway inflammation.29 These findings indirectly suggest that higher relative abundance of Prevotella may alleviate airway inflammation in COPD patients by modulating amino acid metabolic pathways.
Interaction Between COPD Patients and Streptococcus
The genus Streptococcus under the Firmicutes phylum consists mostly of Gram-positive cocci, with Streptococcus pneumoniae being a pathogenic species within this genus. Contrary to previous studies, some research suggests that Streptococcus, as the most common genus in COPD patients, may indirectly trigger excessive production of CXCL8/IL-8 through lung microbiome dysbiosis. The levels of CXCL8/IL-8 in sputum are associated with increased severity of COPD.31 Specifically, Streptococcus pneumoniae may play a role in patients with frequent exacerbations of COPD by damaging the TLR2 signaling pathway in alveolar macrophages.41 This indicates that Streptococcus in the respiratory tract may modulate the innate immune system and regulate the pathological process of COPD.
Moreover, the relative abundance of Streptococcus in both the respiratory and intestinal tracts of COPD patients is generally increased.38 The enrichment of Streptococcus is closely associated with increased abundance of glucosyltransferases and LPXTG-anchored adhesive domains, suggesting that enhanced adhesive capacity is a key factor driving the increase in abundance. This adhesion ability is related to specific features of Streptococcus, such as the auxiliary secretion proteins Asp1-3, which are part of the SecA2/Y2 secretion system. These glycoproteins, rich in serine, are involved in the adhesion process.38 Therefore, it can be inferred that the enrichment of Streptococcus in the respiratory tract and its involvement in amino acid metabolism may play an important role in the regulation of COPD. This further supports the close relationship between Streptococcus and COPD patients.
Interactions Between COPD Patients and Lactobacillus
Lactobacillus is a genus of non-spore-forming, Gram-positive rods under the Firmicutes phylum, known for its strong ability to metabolize carbohydrates and produce acids. Lactobacillus species are commonly found in various mucosal sites, including the respiratory tract, and have been shown to play a role in maintaining gut and lung health. In the context of COPD, Lactobacillus is believed to have potential beneficial effects by modulating the respiratory microbiome and immune responses.
Yadava et al, in their study using inhaled lipopolysaccharides and elastase to induce chronic pulmonary inflammation in mice, found that the abundance of Prevotella decreased, while the abundance of Pseudomonas and Lactobacillus increased in the affected mice.42 Lactobacillus, a Gram-positive bacterium under the Firmicutes phylum, is known for its strong metabolic ability to produce acids from carbohydrates. Regarding the relationship between Lactobacillus in the respiratory tract and COPD, Zhengzheng Yan and others, through multi-omics analysis, demonstrated that the reduction of Lactobacillus in the respiratory tract led to a higher proportion of bacterial transport systems and amino acid synthesis in neutrophilic COPD patients. The depletion of tryptophan degradation metabolism in the respiratory microbiome caused a reduction in indole-3-acetic acid (IAA) production by Lactobacillus, which in turn increased the inflammatory response, epithelial cell apoptosis, and worsened lung function. They also found that the administration of Lactobacillus and Lactobacillus salivarius to mice, along with Pseudomonas aeruginosa, significantly increased IAA in the mice’s bronchoalveolar lavage fluid, alleviating lung function decline, tissue damage, and cell apoptosis, while reducing the levels of IL-1β, IL-6, and IL-17A. These changes were observed in neutrophilic COPD patients, suggesting that the respiratory host-microbiome correlation is stronger in this patient type and that Lactobacillus colonization in the respiratory tract has a positive impact on neutrophilic COPD patients.43
At the same time, Xue Q et al conducted a study on the lung microbiome and cytokine profiles under different COPD disease states, discovering that Lactobacillus was enriched in treatment-related phenotypes, possibly exerting a potential probiotic effect.44 While some studies suggest that the enrichment of lung microbiota and the increased concentrations of microbial metabolites (such as arachidonic acid, palmitic acid, glycerol, and 4-hydroxybenzoate) can reduce alveolar macrophage TLR4 responses, leading to impaired infection clearance,45,46 these findings highlight the potential adverse effects of certain microbial metabolites on the respiratory tract. However, the research on Lactobacillus in the respiratory tract underscores the positive effects of microbial products on COPD patients, providing an encouraging response to the regulation of the respiratory microbiome for these patients.
Interactions Between COPD Patients and Haemophilus
Haemophilus is a type of Gram-negative short rod-shaped bacterium belonging to the class Gammaproteobacteria within the phylum Proteobacteria. It is widely present in the human respiratory tract and includes both non-pathogenic species and important pathogens such as Haemophilus influenzae. Haemophilus is a common pathogen in COPD patients, especially in neutrophil-dominant inflammatory phenotypes. Studies have found that the respiratory microbiome in neutrophil-dominant COPD patients is heterogeneous, with two major community types primarily dominated by Haemophilus. It has been reported that IL-1β in sputum is a reliable biomarker for predicting bacterial acute exacerbation with neutrophil increase.46
In a multi-cohort longitudinal analysis by Wang et al, they observed that in COPD patients with neutrophil proportions ≥61% and eosinophil proportions <3%, excessive expression of Haemophilus was associated with reduced microbial diversity, regardless of whether the patient was in a stable or acute exacerbation phase, and this was accompanied by elevated sputum and serum IL-17A levels.15 IL-17A further induces the production of serum amyloid A (SAA), and SAA promotes the upregulation of IL-17A and Th17-related cytokines (such as IL-6), enhancing the recruitment and activation of neutrophils. Another study further found that in sputum samples from acute exacerbation patients, not only was the relative abundance of Firmicutes altered, but the relative abundance of species within the Gammaproteobacteria class also changed significantly. This was closely related to an increase in the proportion of neutrophils in the sputum and elevated IL-1β levels in the bronchi, and this pattern was accompanied by increased serum C-reactive protein (CRP) levels and a significant decline in lung function.47 These findings highlight the important role of Haemophilus in regulating the host-respiratory microbiome interaction through inflammatory factors, playing a crucial role in the pathogenesis and progression of COPD.
The Relationship Between Immune Inflammatory Phenotypes of COPD and the Respiratory Microbiome
COPD is a highly heterogeneous disease, which can be classified into different pathological inflammatory types, including eosinophil-predominant, neutrophil-predominant, mixed inflammatory, Th1-high activation, and Th2-dominant types.48,49 Among these, eosinophil-predominant and neutrophil-predominant types are more common.
The bronchial microbiota is closely related to peripheral blood eosinophil levels. Studies have shown that patients with higher peripheral blood eosinophil percentages tend to have higher respiratory microbiota diversity. In these patients, the relative abundance of Bacteroidetes and Spirochaetes is significantly increased, while the relative abundance of Streptococcus species is lower. This microbial feature is commonly seen in COPD patients with peripheral blood eosinophil percentages ≥2%.26 The eosinophil-predominant phenotype is more common in COPD patients, and recent research has increasingly revealed its association with respiratory microbiota.
For example, Ghebre et al proposed that the high relative abundance of Bacteroides species is closely related to eosinophilic inflammation and increased Th2-mediated CCL13 and CCL17 levels in bronchial secretions.50 Meanwhile, Xue et al found through analysis of lung microbiomes and cytokine profiles in different disease states that the abundance of Pseudomonas and Klebsiella species is significantly positively correlated with eosinophil percentages.44 Other studies have also shown a specific association between eosinophils and the respiratory microbiota.31,43 For example, some studies found that the temporal changes in Campylobacter and Prevotella species in patients are associated with shifts in inflammatory phenotypes, from neutrophil-predominant inflammation to eosinophil-predominant inflammation, which corresponds with an increase in eosinophils in sputum.51 However, Keir et al found that patients with eosinophil-predominant acute exacerbations of COPD did not show significant changes in microbiota diversity or composition.52 Perotin et al’s study also found no significant differences in the overall composition, bacterial count per sample, or α-diversity of respiratory microbiota between patients with high and low peripheral blood eosinophil levels in 59 COPD patients, and the distribution of dominant phyla (eg, Firmicutes) remained unchanged.53
In contrast, the host-microbiota correlation is more prominent in neutrophil-predominant COPD patients.53 Zhengzheng Yan et al found through multi-omics analysis that neutrophil-predominant COPD patients have a higher proportion of bacteria associated with bacterial transport systems and amino acid synthesis.43 Segal et al analyzed the sputum of 510 COPD patients and found that neutrophil-predominant COPD was associated with two main respiratory bacterial ecological patterns, both of which were dominated by Haemophilus species. The bacterial composition in Haemophilus-dominated neutrophil-predominant COPD patients was relatively stable and correlated with elevated IL-1β and TNF-α levels in sputum.54
In summary, neutrophil-predominant COPD has a stronger association with respiratory prokaryotic microbiota. Multi-omics studies have revealed that Prevotella species from Bacteroidetes, Moraxella species from Proteobacteria, Haemophilus species, and Streptococcus and Lactobacillus species from Firmicutes may participate in the onset and progression of the disease in neutrophil-predominant COPD patients through various mechanisms. This provides important clues for further research on host-microbiota interactions and their potential therapeutic targets.
Conclusion and Limits
For patients with severe conditions, up to 78% of the COPD population is affected by bacterial infections, viral infections, or a combination of both. One of the characteristics of COPD is immune dysregulation related to bacterial colonization and infection. The development of independent culturing techniques has provided new insights into the relationship between bacterial ecology and health status, further expanding our understanding of the lung microbiome. The respiratory microbiota plays an important role in the pathophysiological mechanisms of COPD, with the composition and metabolic activities of different microbiota communities closely related to the patient’s inflammatory phenotype, lung function status, and disease progression. Although differences in sampling methods may lead to variations in study results, commonalities can still be observed in analyses at the phylum and genus levels. Research has focused on phyla such as Firmicutes (eg, Streptococcus), Proteobacteria (eg, Moraxella, Haemophilus, Pseudomonas), and Bacteroidetes (eg, Prevotella).
In these common phyla and genera, immune response, inflammatory response, and metabolic mechanisms are key factors. A reduction in Prevotella species may exacerbate lung inflammation by affecting epithelial barrier function and immune regulation, while the enrichment of Streptococcus and Haemophilus species is closely associated with neutrophilic inflammation and acute exacerbations. Additionally, the respiratory microbiota characteristics in eosinophil-predominant COPD patients suggest higher microbial diversity and are associated with increased abundance of Bacteroidetes species.
The correlation between respiratory prokaryotic microbiota and lung function in COPD patients is significant. The relative abundance of Streptococcus, Prevotella, and Pseudomonas is closely related to lung function indicators such as FEV1, FEV1/FVC, and FEV1% predicted values. Pseudomonas is particularly associated with more severe airflow limitation in COPD patients. These findings highlight the importance of monitoring the dynamic changes in these microbial genera to better understand their relationship with lung function and address discrepancies in research results.
The host-microbe interactions in COPD patients play a crucial role in the pathogenesis and progression of the disease. Prevotella, Streptococcus, Pseudomonas, Lactobacillus, and Haemophilus are key microbial genera involved in these interactions. Prevotella and Moraxella are significantly correlated with the host’s respiratory transcriptome profile, especially genes involved in immune and inflammatory responses. Streptococcus may modulate the innate immune system and regulate the pathological process of COPD. Lactobacillus has potential beneficial effects by modulating the respiratory microbiome and immune responses. Haemophilus is a common pathogen in COPD patients, particularly in neutrophil-dominant inflammatory phenotypes, and plays a crucial role in regulating host-respiratory microbiome interactions through inflammatory factors.
However, there are still some limitations in existing research. First, the methods of sample collection vary widely. Current studies mainly include nasal swabs, oropharyngeal swabs,32,36 induced and spontaneous sputum samples,15,19,32,34,44 and bronchoalveolar lavage fluid,18,22,37 each of which has its own advantages and disadvantages. There are differences in microbiota composition between different sample types. Nasal and oropharyngeal swabs primarily represent upper respiratory tract microbiota, sputum samples reflect both upper and lower respiratory tract microbiota, while bronchoalveolar lavage and bronchial brushing allow for deeper sampling of lower respiratory tract microbiota. The choice of sampling method should be based on the research focus, but sputum samples are ideal for exploring the respiratory microbiota because they are easy to collect, non-invasive, well-accepted by patients, and can cover a broad range of microorganisms. Second, factors such as smoking history, treatment regimens, and long-term living environment differences may also affect microbiota diversity. Third, the sample sizes in current studies are generally small, and larger sample sizes are needed to explore more universal mechanisms. Fourth, due to the lack of long-term follow-up, the dynamic changes of the microbiota during COPD progression have not been explored in depth. Finally, current microbiota research largely relies on 16S rRNA gene sequencing and a small amount of real-time quantitative PCR, which typically only allows for analysis at the genus level, without precise species-level identification. 16S rRNA gene sequencing is a widely used and cost-effective method for detecting microbial diversity, but it can only indirectly infer microbial functions. To further improve species detection accuracy, increase diversity, and predict gene functions, metagenomic techniques, which do not require pre-culturing and can analyze microbiome resources, will become key in future research. This technology can provide species-level accuracy, discover new genes, develop novel microbial bioactive substances, reveal microbial community structure and functions, and is especially valuable in disease mechanism research.
This review was conducted through keyword searches in PubMed, ScienceDirect, and Elsevier databases, using keywords such as bacterial communication and chronic obstructive pulmonary disease. This is a narrative review, not a systematic review, aiming to cover various aspects of COPD, including different stages of the disease, sample types, lung function, and immune-inflammatory responses related to the disease. However, there are limitations to this review. First, it is based on existing literature, and due to sample size limitations and differences between studies, it may not fully reflect the comprehensive characteristics of the microbiota in COPD patients. Second, this review does not include long-term follow-up data for COPD patients, so detailed analysis of microbiota dynamics during disease progression is not provided. Finally, while metagenomic techniques offer higher accuracy for microbiota research, most studies still focus on 16S rRNA gene sequencing, with limited use of other methods, restricting the in-depth exploration of microbiota diversity and function.
Future research should focus on diverse sampling methods, expanding sample sizes, long-term follow-up, and the use of metagenomic techniques, with the aim of providing more comprehensive microbiome data for precision treatment of COPD and promoting the development of personalized intervention strategies based on the microbiota.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Commission Pudong New Area health and family planning commission project [PW2022A-02, PW2023A-07, PW2021A-20]. Science and Technology Development Science and Technology Development Fund of Shanghai Pudong New Area [PKJ2021-Y11], Discipline Construction Project of Shanghai Pudong New Area Health Commission (Key Discipline Group, PWZxq2022-12).
Disclosure
The author declare that they have no competing interests in this work.
References
1. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2024 Report). global initiative for chronic obstructive lung disease.
2. GBD. Mortality and causes of death collaborators (2015). Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2013;385(9963):117–15. doi:10.1016/S0140-6736(14)61682-2.
3. World Health Organization. Projections of mortality and causes of death. 2016. Available from: here:https://colinmathers.com/2022/05/10/projections-of-global-deaths-from-2016-to-2060/.
4. Cornelius T. Clinical guideline highlights for the hospitalist: GOLD COPD update 2024. J Hospital Med. 2024;19(9):818–820. doi:10.1002/jhm.13416
5. Spruit MA, Singh SJ, Garvey C, et al. ATS/ERS Task Force on Pulmonary Rehabilitation (2013). An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 188(8):e13–e64. doi:10.1164/rccm.201309-1634ST
6. Bhatt SP, Rabe KF, Hanania NA, et al. BOREAS Investigators. Dupilumab for COPD with Type 2 Inflammation Indicated by Eosinophil Counts. New Engl J Med. 2023;389(3):205–214. doi:10.1056/NEJMoa2303951
7. D’Anna SE, Dossena F, Gnemmi I, et al. Bacterial load and related innate immune response in the bronchi of rapid decliners with chronic obstructive pulmonary disease. Respir Med. 2023;215:107297. doi:10.1016/j.rmed.2023.107297
8. Wypych TP, Wickramasinghe LC, Marsland BJ. The influence of the microbiome on respiratory health. Nat Immunol. 2019;20(10):1279–1290. doi:10.1038/s41590-019-0451-9
9. Budden KF, Shukla SD, Rehman SF, et al. Functional effects of the microbiota in chronic respiratory disease. Lancet Respir Med. 2019;7(10):907–920. doi:10.1016/S2213-2600(18)30510-1
10. Chotirmall SH, Gellatly SL, Budden KF, et al. Microbiomes in respiratory health and disease: an Asia-Pacific perspective. Respirology. 2017;22(2):240–250. doi:10.1111/resp.12971
11. Drengenes C, Eagan TML, Haaland I, Wiker HG, Nielsen R. Exploring protocol bias in airway microbiome studies: one versus two PCR steps and 16S rRNA gene region V3 V4 versus V4. BMC Genomics. 2021;22(1):3. doi:10.1186/s12864-020-07252-z
12. Lin L, Yi X, Liu H, et al. The airway microbiome mediates the interaction between environmental exposure and respiratory health in humans. Nature Med. 2023;29(7):1750–1759. doi:10.1038/s41591-023-02424-2
13. Wang Z, Yang Y, Yan Z, et al. Multi-omic meta-analysis identifies functional signatures of airway microbiome in chronic obstructive pulmonary disease. ISME J. 2020;14(11):2748–2765. doi:10.1038/s41396-020-0727-y
14. Wang R, Huang C, Yang W, et al. Respiratory microbiota and radiomics features in the stable COPD patients. Respir Res. 2023;24(1):131. doi:10.1186/s12931-023-02434-1
15. Haldar K, George L, Wang Z, et al. The sputum microbiome is distinct between COPD and health, independent of smoking history. Respir Res. 2020;21(1):183. doi:10.1186/s12931-020-01448-3
16. Hazra D, Sm F, Chawla K, et al. The altered sputum microbiome profile in patients with moderate and severe COPD exacerbations, compared to the healthy group in the Indian population. F1000Research. 2023;12:528. doi:10.12688/f1000research.132220.3
17. Singh R, Mackay AJ, Patel AR, et al. Inflammatory thresholds and the species-specific effects of colonising bacteria in stable chronic obstructive pulmonary disease. Respir Res. 2014;15(1):114. doi:10.1186/s12931-014-0114-1
18. Bouquet J, Tabor DE, Silver JS, et al. Microbial burden and viral exacerbations in a longitudinal multicenter COPD cohort. Respir Res. 2020;21(1):77. doi:10.1186/s12931-020-01340-0
19. Wang J, Chai J, Sun L, Zhao J, Chang C. The sputum microbiome associated with different sub-types of AECOPD in a Chinese cohort. BMC Infect Dis. 2020;20(1):610. doi:10.1186/s12879-020-05313-y
20. Dicker AJ, Huang JTJ, Lonergan M, et al. The sputum microbiome, airway inflammation, and mortality in chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2021;147(1):158–167. doi:10.1016/j.jaci.2020.02.040
21. Yang CY, Li SW, Chin CY, et al. Association of exacerbation phenotype with the sputum microbiome in chronic obstructive pulmonary disease patients during the clinically stable state. J Transl Med. 2021;19(1):121. doi:10.1186/s12967-021-02788-4
22. Ramsheh MY, Haldar K, Esteve-Codina A, et al. Lung microbiome composition and bronchial epithelial gene expression in patients with COPD versus healthy individuals: a bacterial 16S rRNA gene sequencing and host transcriptomic analysis. Lancet Microbe. 2021;2(7):e300–e310. doi:10.1016/S2666-5247(21)00035-5
23. Erb-Downward JR, Thompson DL, Han MK, et al. Analysis of the lung microbiome in the “healthy” smoker and in COPD. PLoS One. 2011;6(2):e16384. doi:10.1371/journal.pone.0016384
24. Larsen JM, Musavian HS, Butt TM, Ingvorsen C, Thysen AH, Brix S. Chronic obstructive pulmonary disease and asthma-associated Proteobacteria, but not commensal Prevotella spp. promote Toll-like receptor 2-independent lung inflammation and pathology. Immunology. 2015;144(2):333–342. doi:10.1111/imm.12376
25. North JA, Miller AR, Wildenthal JA, Young SJ, Tabita FR. Microbial pathway for anaerobic 5’-methylthioadenosine metabolism coupled to ethylene formation. Proc Natl Acad Sci USA. 2017;114(48):E10455–E10464. doi:10.1073/pnas.1711625114
26. Millares L, Pascual S, Montón C, et al. Relationship between the respiratory microbiome and the severity of airflow limitation, history of exacerbations and circulating eosinophils in COPD patients. BMC Pulm Med. 2019;19(1):112. doi:10.1186/s12890-019-0867-x
27. Lupp C. Host–microbe interactions. Nature. 2007;449:803. doi:10.1038/449803a
28. Basu I, Locker J, Cassera MB, et al. Growth and metastases of human lung cancer are inhibited in mouse xenografts by a transition state analogue of 5’-methylthioadenosine phosphorylase. J Biol Chem. 2011;286(6):4902–4911. doi:10.1074/jbc.M110.198374
29. Wypych TP, Pattaroni C, Perdijk O, et al. Microbial metabolism of L-tyrosine protects against allergic airway inflammation. Nat Immunol. 2021;22(3):279–286. doi:10.1038/s41590-020-00856-3
30. Pragman AA, Knutson KA, Gould TJ, et al. Chronic obstructive pulmonary disease upper airway microbiome is associated with select clinical characteristics. PLoS One. 2019;14(7):e0219962. doi:10.1371/journal.pone.0219962
31. Wang Z, Locantore N, Haldar K, et al. Inflammatory endotype-associated airway microbiome in chronic obstructive pulmonary disease clinical stability and exacerbations: a multicohort longitudinal analysis. Am J Respir Crit Care Med. 2021;203(12):1488–1502.
32. Xu Y, et al. Upper/Lower Respiratory Tract Microbiome Changes in AECOPD and COPD. Research Square; 2021.
33. Pragman AA, Knutson KA, Gould TJ, Isaacson RE, Reilly CS, Wendt CH. Chronic obstructive pulmonary disease upper airway microbiota alpha diversity is associated with exacerbation phenotype: a case-control observational study. Respir Res. 2019;20(1):114. doi:10.1186/s12931-019-1080-4
34. Zhu SF, Wu XX, Guo Y, et al. A 16S rDNA sequencing-based analysis of airway microecology in patients with an acute exacerbation of chronic obstructive pulmonary disease: a cross-sectional study in Inner Mongolia, China. Front Med. 2022;9:946238. doi:10.3389/fmed.2022.946238
35. Li Y, Mao X, Shi P, et al. Microbiome-host interactions in the pathogenesis of acute exacerbation of chronic obstructive pulmonary disease. Front Cell Infect Microbiol. 2024;14(1386201). doi:10.3389/fcimb.2024.1386201
36. Su L, Qiao Y, Luo J, et al. Characteristics of the sputum microbiome in COPD exacerbations and correlations between clinical indices. J Transl Med. 2022;20(1):76. doi:10.1186/s12967-022-03278-x
37. Opron K, Begley LA, Erb-Downward JR, et al. Lung microbiota associations with clinical features of COPD in the SPIROMICS cohort. NPJ Biofilms and Microbiomes. 2021;7(1):14. doi:10.1038/s41522-021-00185-9
38. Bowerman KL, Rehman SF, Vaughan A, et al. Disease-associated gut microbiome and metabolome changes in patients with chronic obstructive pulmonary disease. Nat Commun. 2020;11(1):5886. doi:10.1038/s41467-020-19701-0
39. Madapoosi SS, Cruickshank-Quinn C, Opron K, et al. SPIROMICS Research Group. Lung microbiota and metabolites collectively associate with clinical outcomes in milder stage chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2022;206(4):427–439. doi:10.1164/rccm.202110-2241OC
40. LoGiudice N, Le L, Abuan I, Leizorek Y, Roberts SC. Alpha-difluoromethylornithine, an irreversible inhibitor of polyamine biosynthesis, as a therapeutic strategy against hyperproliferative and infectious diseases. Med Sci. 2018;6(1):12. doi:10.3390/medsci6010012
41. Berenson CS, Kruzel RL, Eberhardt E, et al. Impaired innate immune alveolar macrophage response and the predilection for COPD exacerbations. Thorax. 2014;69(9):811–818. doi:10.1136/thoraxjnl-2013-203669
42. Yadava K, Pattaroni C, Sichelstiel AK, et al. Microbiota promotes chronic pulmonary inflammation by enhancing il-17a and autoantibodies. Am J Respir Crit Care Med. 2016;193(9):975–987. doi:10.1164/rccm.201504-0779OC
43. Yan Z, Chen B, Yang Y, et al. Multi-omics analyses of airway host-microbe interactions in chronic obstructive pulmonary disease identify potential therapeutic interventions. Nat Microbiol. 2022;7(9):1361–1375. doi:10.1038/s41564-022-01196-8
44. Xue Q, Xie Y, He Y, et al. Lung microbiome and cytokine profiles in different disease states of COPD: a cohort study. Sci Rep. 2023;13(1):5715. doi:10.1038/s41598-023-32901-0
45. Segal LN, Alekseyenko AV, Clemente JC, et al. Enrichment of lung microbiome with supraglottic taxa is associated with increased pulmonary inflammation. Microbiome. 2013;1(1):19. doi:10.1186/2049-2618-1-19
46. Jones B, Donovan C, Liu G, et al. Animal models of COPD: what do they tell us? Respirology. 2017;22(1):21–32. doi:10.1111/resp.12908
47. Haldar K, Bafadhel M, Lau K, et al. Microbiome balance in sputum determined by PCR stratifies COPD exacerbations and shows potential for selective use of antibiotics. PLoS One. 2017;12(8):e0182833. doi:10.1371/journal.pone.0182833
48. J BP. Inflammatory endotypes in COPD. Allergy. 2019;74(7):1249–1256. doi:10.1111/all.13760
49. Zhang J, Chen FM, Wang YL, Chen YH. Early detection and prediction of acute exacerbation of chronic obstructive pulmonary disease. Chin Med J Pulm Crit Care Med. 2023;2:102–107. doi:10.1016/j.pccm.2023.04.004
50. Ghebre MA, Pang PH, Diver S, et al. Biological exacerbation clusters demonstrate asthma and chronic obstructive pulmonary disease overlap with distinct mediator and microbiome profiles. J Allergy Clin Immunol. 2018;141(6):2027–2036.e12. doi:10.1016/j.jaci.2018.04.013
51. Tworek D, Majewski S, Szewczyk K, et al. The association between airway eosinophilic inflammation and IL-33 in stable non-atopic COPD. Respir Res. 2018;19(1):108. doi:10.1186/s12931-018-0807-y
52. Keir HR, Dicker A, Lonergan M, et al. Clinical endotypes of exacerbation are associated with differences in microbial composition and diversity in COPD. Europ resp J. 2020;56(4):2000391. doi:10.1183/13993003.00391-2020
53. Perotin JM, Muggeo A, Lecomte-Thenot Q, et al. High blood eosinophil count at stable state is not associated with airway microbiota distinct profile in COPD. Int J Chronic Obstr. 2024;(19):765–771. doi:10.2147/COPD.S453526
54. Segal LN, Huang YJ. Crossing kingdoms: host-microbial endotyping and the quest to understand treatable traits in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2021;203(12):1447–1448. doi:10.1164/rccm.202101-0169ED
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
DNA Methylation Profiling in a Cigarette Smoke-Exposed Mouse Model of Airway Inflammation
Li P, Peng J, Chen G, Chen F, Shen Y, Liu L, Chen L
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2443-2450
Published Date: 1 October 2022