Back to Journals » Clinical Interventions in Aging » Volume 13
Whose advocacy counts in shaping elderly patients’ satisfaction with physicians’ care and communication?
Authors Kahana B, Yu J, Kahana E, Langendoerfer KB
Received 13 February 2018
Accepted for publication 12 April 2018
Published 25 June 2018 Volume 2018:13 Pages 1161—1168
DOI https://doi.org/10.2147/CIA.S165086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Boaz Kahana,1 Jiao Yu,2 Eva Kahana,2 Kaitlyn Barnes Langendoerfer2
1Department of Psychology, Cleveland State University, 2Department of Sociology, Case Western Reserve University, Cleveland, OH, USA
Purpose: The purpose of this article was to examine the relative importance of patients’ self-advocacy and perceived physicians’ advocacy for impacting patients’ satisfaction in terms of physician communication and physician–patient relationship. We also examine the influence of physicians’ emotional support and patients’ demographic as well as health characteristics on patients’ satisfaction.
Sample: Our sample includes interviews with 806 community dwelling older adults (mean age =77.82 years, SD=8.41). The sample included residents of a large retirement community in Clearwater, FL, USA. Respondents were also included from representative samples of older adults living in Orlando and Miami, FL, USA, and Cleveland, OH, USA.
Methods and results: Using multiple hierarchical regression analyses, we found that patients’ age and functional limitations were negatively associated with their care satisfaction. When compared with White patients, African-American patients were less satisfied with their physicians while Latino patients expressed greater satisfaction with their medical care. We found limited evidence of patients’ self-advocacy and such advocacy did not serve as a significant predictor of satisfaction with physicians. In contrast, patients’ perception of physicians’ readiness to act as patient advocates was a significant predictor of patients’ satisfaction. Emotional support of physicians was also associated with patients’ satisfaction.
Conclusion: These findings raise questions about consumer empowerment among older adults and underscore their desire for and appreciation of physicians’ advocacy. Findings are discussed in the context of power imbalance between elderly patients and their doctors.
Keywords: physicians’ emotional support, patient proactivity, patient-centered care, evaluations of medical care, paternalistic model of primary care
Introduction
Determinants of patients’ satisfaction have been extensively studied but pose unique challenges for understanding the primary care of older patients.1 For elderly patients, good communication with health care providers assumes particular importance.2 With more chronic illnesses and health challenges, information sharing and supportive care received from physicians can play a significant role in ensuring patients’ well-being.3
In considering older patients’ preferences and perspectives, older patients, those who are sicker (i.e., report more chronic health conditions) and minorities who have less access to health care, have been found to face particular challenges in obtaining responsive care.4,5 However, there has been little focus on the relative importance of physicians’ advocacy in contributing to patients’ satisfaction with communication and medical care in primary care situations. Beyond responsive communication with patients, physicians’ advocacy is recognized as an important physician responsibility.6 However, there is lack of consensus about parameters of physicians’ advocacy and prevalence of physicians engaging in patients’ advocacy.7 The medical model of health care is based on a paternalistic view of care wherein physicians offer support, advice, and care to their patients. Such physician-driven models for health care are especially prevalent in treating older patients.8
A paternalistic model of care offers opportunities for physicians to advocate for patients and champion their concerns, preferences, and well-being.9 Patients’ advocacy, reflecting professional initiatives on behalf of patients, has received attention both in medicine and in nursing.10 On one hand, the desirability of social responsibility of health care providers for patients’ well-being is recognized.7 On the other hand, health care providers’ advocacy may be viewed as limiting patient autonomy.10 Engagement of physicians in advocacy on their patients’ behalf has been advocated in medical education11 even as the costs involved in such advocacy may pose a problem.12 Nevertheless, it is noteworthy that research on patients’ desire for physicians’ advocacy has not been undertaken. One qualitative study has identified patients’ desire for involved physicians that might point to positive views of physicians’ advocacy.13 Furthermore, there are useful suggestions about the value of similarities in patient and physician orientations to shared decision making.14 Examination of patient preferences for physicians’ advocacy is still lacking and requires study.
Patient proactivity in communication and taking initiatives to advocate for getting good health care can also enhance the responsiveness of care received and contribute to patients’ satisfaction.15 Patient initiative and health care advocacy are recognized as increasingly important factors in the consumer age of readily retrieved health information.16 Yet, because of their vulnerability on one hand and their socialization during eras characterized by paternalistic approaches to patient care on the other hand, older patients may not fully share in patient involvement in shared decision making.3 Patient empowerment may be further limited among patients with less education and health literacy, including patients who are members of racial and ethnic minority groups.17 For example, our research with older adults who reported a prior cancer diagnosis revealed a passive orientation. Qualitative interviews indicated that these older adults were cautious in speaking up to their physicians. At the same time, they made proactive suggestions to other cancer patients to actively advocate on their own behalf.18
In this study, we explored the importance of both perceived physicians’ advocacy and patients’ self-advocacy as determinants of elderly patients’ satisfaction with physician communication and with their relationship with their physician. Physicians’ emotional support was also considered as a potential determinant of patients’ satisfaction. Additionally, we explored to what extent older patients’ demographic characteristics, health status (number of chronic health conditions), and functional abilities impacted satisfaction outcomes including overall assessment of their relationship with their physician. In terms of health status and functional abilities, we anticipated that elderly patients who exhibit more complex health problems and greater frailty would require more attention from busy physicians and may not feel that their needs were met as fully as would their healthier and less functionally limited counterparts.9
Methods
Sample
The sample for this study is drawn from a longitudinal study of successful aging conducted by the Elderly Care Research Center, which focuses on the late-life adaptation and resilience of community dwelling older adults.19 The study was conducted in four different community settings of Clearwater, Orlando, and Miami, FL, USA, and Cleveland, OH, USA. The original study was first conducted in 1990 in Clearwater, and we recruited subsequent samples from the other three sites. At wave one of the study, 3,905 households were randomly selected from residential listings of the Clearwater and Orlando retirement communities. At the baseline, 1,000 respondents, representing 908 households, were recruited. Selected households were contacted by telephone to determine if a member of the household met eligibility criteria. Eligibility criteria included 1) age 72 years or older at baseline, 2) living in the community at least 9 months out of the year, and 3) reporting that they were “sufficiently healthy” to complete a 90-minute face-to-face interview. For the other two residentially stable urban communities of Miami and Cleveland, respondents were randomly selected from census-based listings. Inclusion criteria were age 65 years or older and reporting that they were “sufficiently healthy” to complete a 90-minute face-to-face interview. The structured interviews were 60–90 minutes in duration and were conducted in respondent’s homes by trained interviewers after obtaining informed consent. The necessary ethical approval was obtained from the Institutional Review Board (IRB) of Case Western Reserve University (Protocol: 20070101), and all respondents signed written informed consent forms.
For the present study, we utilized the 2005 survey to include the respondents from wave 16 of the Clearwater sample and the samples recruited in the same year from Miami, Orlando, and Cleveland to construct an analytical data file. The effective number of patients at the completion of 2005 interviews was 806 (for all four sites). The average age of participants was 77.8 years (SD =8.41).
Measures
Outcome variables
The outcome variables in this study included patients’ satisfaction regarding communication with their primary care doctors and the doctor–patient relationship.
Doctor–patient communication satisfaction was assessed with a revised 4-item patient–physician communication satisfaction scale.20,21 Participants reported to what extent they agree with specific statements, on a scale from 1 (strongly disagree) to 5 (strongly agree). These statements include “my doctor is good about explaining the reason for medical tests”; “my doctor uses medical terms without explaining them”; “I am allowed to say what I think is important”; and “my doctor ignores what I tell her/him”. After reverse coding the second and fourth items, the summation of the scale was utilized to measure communication satisfaction. Higher scores reflect better communication between patients and physicians. The total scores ranged from 4 to 20 (SD =2.84). Cronbach’s alpha is 0.86.
Doctor–patient relationship was measured with a single item of patient evaluation of their relationship with their primary care physicians. Patients’ assessment of the relationship was measured by asking “how would you rate your relationship with your doctor?” Ratings were made on a 5-point Likert scale rating the relationship ranging from 1 (very poor) to 5 (excellent). This item is similar to those used in other studies to measure patients’ satisfaction.4
Predictors
Physicians’ advocacy and patients’ self-advocacy are the main predictors of interest in this study. We also measured physicians’ emotional support.
Physicians’ advocacy was assessed based on responses to the question “to what extent does your doctor act as your advocate”. The responses ranged from not at all (1) to very much (5). For ease of interpretation, these variables were recoded into no (1–3) and yes (4–5).
Patients’ self-advocacy was assessed with a 6-item patients’ advocacy scale. Participants were asked how often do they do the following: “ask for a referral to a specialist from your doctor”; “request a specific medication from your physician”; “advocate for yourself, or family members to obtain better health care”; “request further explanation beyond that volunteered by your physician”; “express concerns about any aspect of your health care to your physician”; and “email to health care providers”. Each item was rated on a 5-point Likert scale ranging from 1 (not at all) to 5 (often). The summation of these items was used to assess patients’ self-advocacy. The range of self-advocacy is from 6 to 30. Cronbach’s alpha is 0.68.
Physicians’ emotional support was assessed with the Physician’s Emotional Support Scale. Participants were asked to rate to what extent their physician’s communication style was concerned, caring, respectful, supportive, enthusiastic, or hopeful. Each item was rated on a 5-point Likert scale ranging from 1 (not at all) to 5 (very). Cronbach’s alpha of this scale is 0.81.
Since we developed these evaluation items specifically for this study, we examined the factor structure and internal consistency of the items. Exploratory factor analyses provide evidence that one factor forms the basis for the five items. The single factor accounted for 64% of the item variance. We summed the six items, which were treated as a scale-level variable in our analyses to allow the estimation of variability. The range of this variable is from 6 to 30.
Patients’ characteristics include socio-demographic characteristics and health conditions of the participants. Age, gender (0= male; 1= female), education (1= less than high school; 2= high school; 3= college), marital status (0= married; 1= others), and race/ethnicity (1= non-Hispanic White; 2= African-American; 3= Hispanic; 4= others) were utilized in our analyses as sociodemographic variables. Self-rated health, instrumental activities of daily living (IADLs), and comorbidity were included in our study as indicators of patient health status. Participants were asked to report their evaluation of their health in the past year. We recoded self-rated health as “poor/fair”, “good”, and “very good”. IADLs were assessed by a 6-item IADLs’ scale that seeks information on whether participants can move from room to room, go out of doors, do housework, prepare meals, do shopping, and walk up and down stairs. Each item was rated on a 4-point Likert scale that inquired about the frequency of limitation patients experienced ranging from 1 (never) to 4 (always). The mean scores of the six items were utilized to measure objective health of participants. Higher scores reflected higher levels of functional limitations.33 We calculated a comorbidity score by counting the total number of 12 conditions (arthritis, asthma, hypertension, stomach disease, circulatory disease, diabetes, liver disease, kidney disease, heart disease, urinary tract disorder, stroke, and Parkinson’s disease).
Data analytic strategy
Multiple linear regression analyses were used to evaluate the association between patients’ perceptions of physicians’ advocacy and emotional support and patients’ reports of self-advocacy and the outcomes of patients’ satisfaction with communication and doctor–patient relationship. We also examined the influence of patients’ characteristics on their satisfaction and the doctor–patient relationship. Individual models were tested for each of the outcome variables. We modeled the prediction of doctor–patient satisfaction in three steps. Model 1 included the three major predictors, i.e., doctor’s emotional support, doctor’s willingness to act as patient advocate, and patient’s self-advocacy. In Model 2, we adjusted for patients’ health status to examine the change of the effects of the three major predictors. Model 3 included participants’ demographic characteristics. Ordinary Least Square regression and Ordinal Logit regression were used in our analyses.
Results
Descriptive analyses
Descriptive results of study participants are provided in Table 1. Participants were predominantly White (64%). African Americans and Hispanics accounted for 13% and 15% of the participants, respectively. More than half of our participants (61%) were female, 22% of the participants were high school graduates, and 53% of the participants had at least some college education. Around half of the participants were married (53%). The mean age of the participants was 77.8 years. In terms of health status, most participants (61%) rated their health as “good” or “very good”, while 39% rated their health as “poor/fair”. Respondents reported relatively few IADL limitations, indicating that most of the participants were in good functional health.
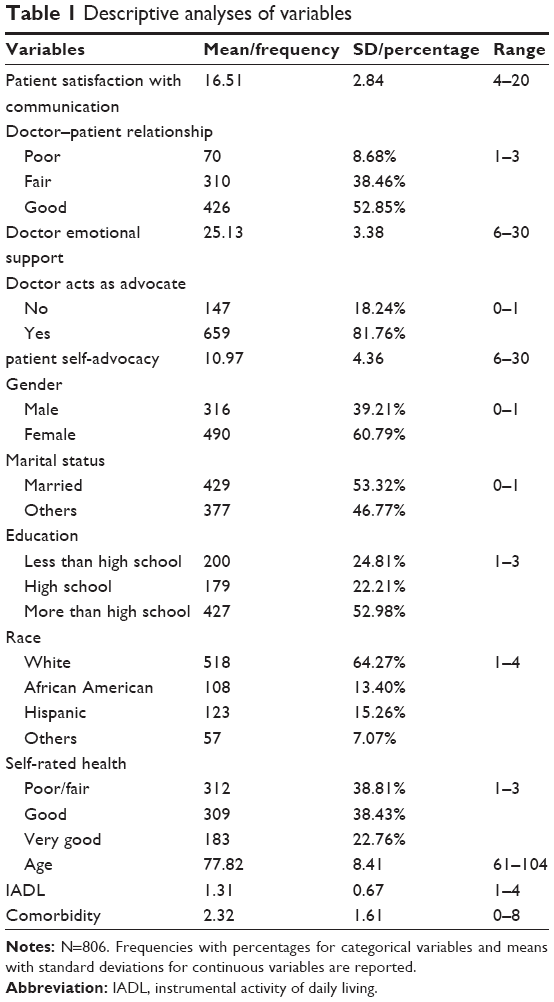 | Table 1 Descriptive analyses of variables |
As for participants’ evaluation of doctor–patient communication, 53% of our participants rated their relationship with their doctor as “good”. Only 9% of the participants reported their doctor–patient relationship as “poor”. The mean score of satisfaction regarding communication with their physicians was 16.5 (4–20), indicating that most participants were satisfied with communication with their physicians.
With respect to patients’ assessment of physicians’ characteristics, the mean score of doctors’ emotional support was fairly high, that is 25.1 (6–30). More than 81% of the participants agreed that their physicians were acting as their advocates. We found that participants who were married, younger, with less than high school education and better health status, and Hispanic race are more likely to agree that their physicians were acting as their advocates. However, patients were unlikely to advocate for themselves. The mean score of self-advocacy was merely 11 (6–30).
Regression analyses
In order to examine the relationship between the reported patient-centered care (physicians’ advocacy and emotional support) and patients’ satisfaction with communication and doctor–patient relationship, three multiple hierarchical regressions were modeled in this study. Table 2 displays the ordinary least squares regression results of patient’s satisfaction with communication after adjusting for age, gender, education, race/ethnicity, and health. We found that doctors’ emotional support and willingness to act as patient advocate were significant predictors of patients’ satisfaction with communication. Across three models, the patterns are consistent even after adjusting for patients’ social-demographic characteristics.
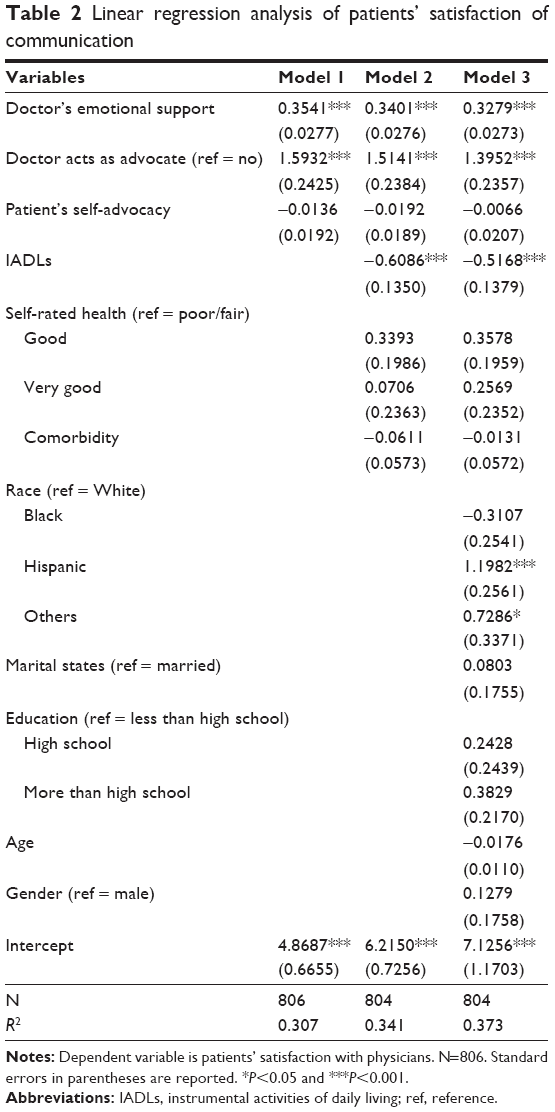 | Table 2 Linear regression analysis of patients’ satisfaction of communication |
In Model 3, we found that Hispanic patients reported more satisfaction with communicating with their doctors compared to their White counterparts (β=1.20, P<0.001). Patients with higher levels of functional impairment had more dissatisfaction with their communication with doctors (β=−0.52, P<0.001). Physicians’ emotional support (β=0.33, P<0.001) and willingness to act as patient advocates (β=1.39, P<0.001) were positively associated with patients’ satisfaction with communication. Patients’ self-advocacy was not a significant predictor of their satisfaction with communicating with their doctors.
In terms of the doctor–patient relationship, we find a similar pattern. Table 3 illustrates the Ordinal Logit regression results between physicians’ advocacy and emotional support and assessment of the doctor–patient relationship. Participants’ health and doctors’ responsiveness were significant predictors of participants’ evaluation of doctor–patient relationship. High levels of emotional support (β=0.40, P<0.001) and higher levels of willingness to act as patient advocates (β=1.56, P<0.001) were positively associated with improved patient–doctor relationship. Participants who reported higher levels of functional limitations (β=−0.25, P<0.05) were less likely to report a good relationship with their primary care doctors. Again, Hispanics reported more satisfaction in terms of doctor–patient relationship (β=0.59, P<0.05). Education was also a significant predictor of doctor–patient relationship. Participants with a college education reported a better relationship with their primary care doctors (β=0.47, P<0.05) compared with their less than high school counterparts. Older participants were less likely to assess their doctor–patient relationship as “good” (β=−0.03, P<0.05). Participants’ self-advocacy was not a significant predictor in the model.
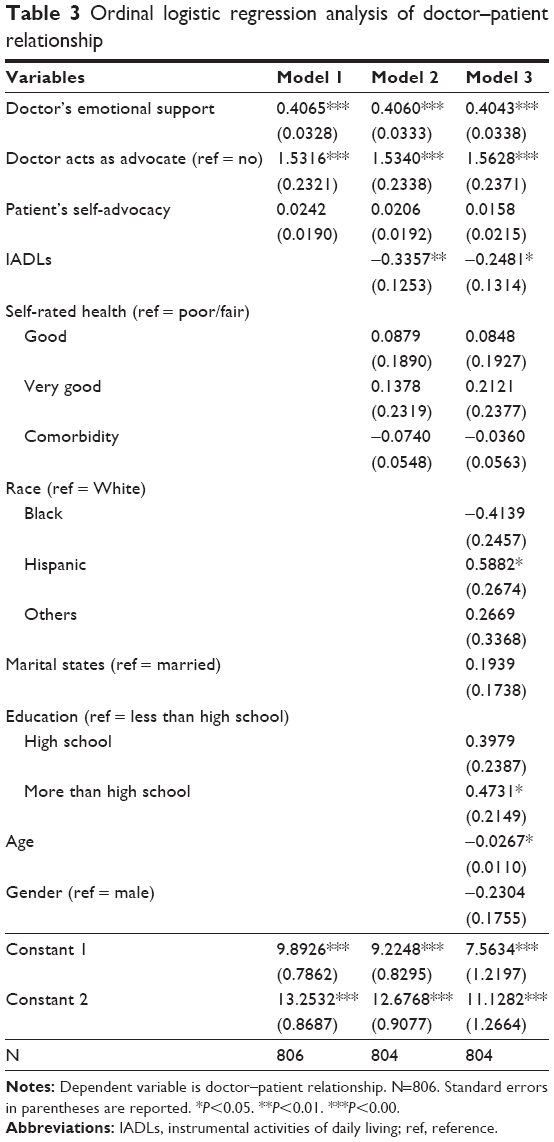 | Table 3 Ordinal logistic regression analysis of doctor–patient relationship |
In sum, after controlling patients’ socio-demographic characteristics, the reported physicians’ responsiveness (advocacy and emotional support) was a significant predictor of patients’ positive evaluation of physicians. The pattern was quite consistent across different models. Compared with patients’ self-advocacy, doctors’ perceived orientation to patient care was more important in predicting satisfaction with doctor–patient communication and with evaluation of the overall doctor–patient relationship.
Discussion
Findings of our study confirm prior research on doctor–patient communication regarding the importance of physicians’ emotional support for patients’ perception of positive communication and satisfaction with the physician.22,23 Such emotional support is likely to assume even greater importance for elderly patients who may be less confident about care that they receive due to ageism in medical care.24,25 Indeed, older patients and more impaired patients with more functional limitations expressed less satisfaction and provided less positive evaluations of their physicians in our study. Some prior research has pointed to greater satisfaction expressed by older patients. However, that research included a generally younger population.5
Sicker patients and those with greater functional impairments have been found in prior research to express less satisfaction with their medical care. This may be attributed to the direct effect of poor health on satisfaction. Another explanation is based on the belief that poorer health care is provided to sicker patients.26 Older patients’ functional limitations are likely to pose challenges during medical visits and may require that the physician spend more time to deal with complex medical issues. Consequently, satisfaction may be diminished with physicians who are unable to adequately address the patients’ complex problems.2
Our findings regarding the lower satisfaction with physicians among less educated patients and among African American respondents are consistent with observations regarding challenges faced by patients who are negotiating health care in the face of multiple vulnerabilities.1 It is notable that prior research has generally found lower satisfaction with medical care among minorities. Racism in health care has been noted as a likely underpinning of patients’ dissatisfaction.27 The greater satisfaction of Latino patients in our study may be attributed to the participation of Cuban elderly in Miami. These patients tended to receive care from Cuban physicians who were immersed in the same culture and often knew their patients outside the doctor patient encounter and interacted with them socially. It is also notable that we only included English-speaking Latino respondents in our study, and in prior research, English-speaking Latinos have shown higher levels of satisfaction with care than did their Spanish-speaking counterparts.28
Our findings indicate that older patients view their physicians as serving advocate functions on patients’ behalf. These patients appreciate and respond favorably to the advocacy of their physicians. It is remarkable that a very high proportion (87%) of our respondents reported that their physicians serve as advocates on their behalf. These findings are consistent with prior research results regarding preferences of older adults to have limited involvement in health care decision making.29 They are also consistent with prior observations that desire of older adults for shared decision making is heterogeneous30 and that the power imbalance in patient physician relationships may result in older adults’ preferences for physicians’ advocacy, rather than patients’ self-advocacy.
Our findings are even more remarkable when we consider the very limited reporting of self-advocacy by respondents in our study. The answer to the original question posed in the title of the study resoundingly favors physicians’ advocacy. Patients’ advocacy, in contrast, is reported to be both infrequent and as having limited relevance to elderly patients’ satisfaction with care. These findings suggest that elderly patients are comfortable viewing their doctors as their health care advocates. They appear to be far more concerned with physicians’ ability to help them navigate the system, and then, they are fearful about physicians disregarding patient autonomy. It appears that elderly patients believe in the empathic commitment of their doctors to promote patients’ well-being and trust that their physicians will represent their best interests.31
The empowerment paradigm calling for greater patients’ advocacy does not appear to be consistent with understandings and desires of the current cohort of elderly patients. According to recent qualitative research,29 preference of older adults for physicians’ advocacy may reflect a subtler form of participation that is intended to be respectful of health care providers and intended to foster partnerships with them.
There is currently a broader recognition in the field of primary care about the social responsibility of physicians to engage in health advocacy.32 Such advocacy is viewed as transcending day-to-day interactions with patients and also responds to broader societal factors that pose barriers to care. Patients’ advocacy, reflecting professional initiatives on behalf of patients, has received attention both in medicine and in nursing.10 On one hand, the desirability of social responsibility of health care providers for patients’ well-being is recognized. On the other hand, health care providers’ advocacy has been viewed as problematic as it may limit patient autonomy.
Conclusion
Our findings suggest that based on trust in their physicians, elderly patients are not overly concerned about curtailment of their autonomy. They do not seek more active roles through patients’ advocacy. There is much concern expressed currently in the nursing and medical literature about the ambiguity involved in professional roles as patient advocates. Our research suggests that older adults might offer pragmatic suggestion on the benefits they see in continued involvement of health care providers in advocacy roles.
Acknowledgment
This study was supported by NIH (grant 1 R01 NR10271).
Disclosure
The authors report no conflicts of interest in this work.
References
Clarke LH, Bennett EV, Korotchenko A. Negotiating vulnerabilities: how older adults with multiple chronic conditions interact with physicians. Can J Aging. 2014;33(1):26–37. | ||
Adelman RD, Greene MG, Ory MG. Communication between older patients and their physicians. Clin Geriatr Med. 2000;16(1):1–24. | ||
Street RL, Makoul G, Arora NK, Epstein RM. How does communication heal? Pathways linking clinician–patient communication to health outcomes. Patient Educ Couns. 2009;74(3):295–301. | ||
Zhang Y, Rohrer J, Borders T, Farrell T. Patient satisfaction, self-rated health status, and health confidence: an assessment of the utility of single-item questions. Am J Med Qual. 2007;22(1):42–49. | ||
Jackson JL, Chamberlin J, Kroenke K. Predictors of patient satisfaction. Soc Sci Med. 2001;52(4):609–620. | ||
Schwartz L. Is there an advocate in the house? The role of health care professionals in patient advocacy. J Med Ethics. 2002;28(1):37–40. | ||
Earnest MA, Wong SL, Federico SG. Perspective: physician advocacy: what is it and how do we do it? Acad Med. 2010;85(1):63–67. | ||
Emanuel EJ, Emanuel LL. Four models of the physician-patient relationship. JAMA. 1992;267(16):2221–2226. | ||
Kahana JS, Kahana E. Disability and Aging: Learning from Both to Empower the Lives of Older Adults. Boulder, CO: Lynne Rienner Publishers; 2017. | ||
Hyland D. An exploration of the relationship between patient autonomy and patient advocacy: implications for nursing practice. Nurs Ethics. 2002;9(5):472–482. | ||
Croft D, Jay SJ, Meslin EM, Gaffney MM, Odell JD. Perspective: is it time for advocacy training in medical education? Acad Med. 2012;87(9):1165–1170. | ||
Pearson SD. Caring and cost: the challenge for physician advocacy. Ann Intern Med. 2000;133(2):148–153. | ||
Anderson R, Barbara A, Feldman S. What patients want: a content analysis of key qualities that influence patient satisfaction. J Med Pract Manage. 2007;22(5):255–261. | ||
Kiesler DJ, Auerbach SM. Optimal matches of patient preferences for information, decision-making and interpersonal behavior: evidence, models and interventions. Patient Educ Couns. 2006;61(3):319–341. | ||
Kahana E, Kahana B. Patient proactivity enhancing doctor–patient–family communication in cancer prevention and care among the aged. Patient Educ Couns. 2003;50(1):67–73. | ||
Wald HS, Dube CE, Anthony DC. Untangling the web – the impact of Internet use on health care and the physician–patient relationship. Patient Educ Couns. 2007;68(3):218–224. | ||
Thompson TL, Robinson JD, Beisecker AE. The older patient-physician interaction. Handb Commun Aging Res. 2004:451–477. | ||
Kahana E, Kahana B, Kelley-Moore J, et al. Toward advocacy in cancer care for older adults: survivors have cautious personal actions but bold advice for others. J Am Geriatr Soc. 2009;57(s2):S269–S271. | ||
Kahana E, Kelley-Moore J, Kahana B. Proactive aging: a longitudinal study of stress, resources, agency, and well-being in late life. Aging Ment Health. 2012;16(4):438–451. | ||
Epstein RM, Franks P, Fiscella K, et al. Measuring patient-centered communication in patient–physician consultations: theoretical and practical issues. Soc Sci Med. 2005;61(7):1516–1528. | ||
Flocke SA, Stange KC, Zyzanski SJ. The association of attributes of primary care with the delivery of clinical preventive services. Med Care. 1998;36(8):AS21–AS30. | ||
Levinson W, Roter DL, Mullooly JP, Dull VT, Frankel RM. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;277(7):553–559. | ||
Hall JA, Epstein AM, DeCiantis ML, McNeil BJ. Physicians’ liking for their patients: more evidence for the role of affect in medical care. Health Psychol. 1993;12(2):140. | ||
Greene MG, Adelman R, Charon R, Hoffman S. Ageism in the medical encounter: an exploratory study of the doctor–elderly patient relationship. Lang Commun. 1986;6(1–2):113–124. | ||
Eymard AS, Douglas DH. Ageism among health care providers and interventions to improve their attitudes toward older adults: an integrative review. J Gerontol Nurs. 2012;38(5):26–35. | ||
Hall JA, Milburn MA, Roter DL, Daltroy LH. Why are sicker patients less satisfied with their medical care? Tests of two explanatory models. Health Psychol. 1998;17(1):70. | ||
Nápoles AM, Gregorich SE, Santoyo-Olsson J, O’brien H, Stewart AL. Interpersonal processes of care and patient satisfaction: do associations differ by race, ethnicity, and language? Health Serv Res. 2009;44(4):1326–1344. | ||
Morales LS, Cunningham WE, Brown JA, Liu H, Hays RD. Are Latinos less satisfied with communication by health care providers? J Gen Intern Med. 1999;14(7):409–417. | ||
Foss C. Elders and patient participation revisited–a discourse analytic approach to older persons’ reflections on patient participation. J Clin Nurs. 2011;20(13–14):2014–2022. | ||
Joseph-Williams N, Elwyn G, Edwards A. Knowledge is not power for patients: a systematic review and thematic synthesis of patient-reported barriers and facilitators to shared decision making. Patient Educ Couns. 2014;94(3):291–309. | ||
Williams SL, Haskard KB, DiMatteo MR. The therapeutic effects of the physician-older patient relationship: effective communication with vulnerable older patients. Clin Interv Aging. 2007;2(3):453. | ||
Dharamsi S, Ho A, Spadafora SM, Woollard R. The physician as health advocate: translating the quest for social responsibility into medical education and practice. Acad Med. 2011;86(9):1108–1113. | ||
Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9(3):179–186. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.