")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Who should receive treatment? Healthcare professionals’ perspectives surrounding the medical management of patients with COVID-19
Authors Almutairi AF, BaniMustafa A , Alessa YM, Alahmad G
Received 17 June 2021
Accepted for publication 19 August 2021
Published 1 September 2021 Volume 2021:14 Pages 3659—3666
DOI https://doi.org/10.2147/RMHP.S325312
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Adel F Almutairi,1 Ala’a BaniMustafa,1 Yousef M Alessa,1 Ghiath Alahmad2
1Science and Technology Unit, King Abdullah International Medical Research Center, King Saud bin Abdulaziz University for Health Sciences, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia; 2Biomedical Ethics, King Abdullah International Medical Research Center, King Saud bin Abdulaziz University for Health Sciences, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia
Correspondence: Adel F Almutairi
Science and Technology Unit, King Abdullah International Medical Research Center, King Saud bin Abdulaziz University for Health Sciences, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia
Email [email protected]
Background: The COVID-19 pandemic has resulted in unprecedented challenges for healthcare systems worldwide. This pandemic is much more than a health crisis; it has also raised many ethical challenges. The large number of infected patients amid scarce resources has placed healthcare professionals in a critical situation in which they have to make difficult decisions about how to prioritize their patients. Therefore, the aim of this study is to explore the ethical challenges experienced and perceived by healthcare professionals working in healthcare institutions and research centers in Saudi Arabia.
Methods: Semi-structured face-to-face interviews were conducted individually with frontline healthcare providers (physicians and nurses), researchers, and decision-makers involved in the management of COVID-19 cases. Each interview lasted up to 90 minutes. The thematic analysis technique was used to analyse the interview data.
Findings: The participants’ rich experiences, which revealed a number of ethical challenges concerning the provision of medical care to infected patients, were framed around four main themes: treatment challenges related to COVID-19 patients, uncertainty of the medical outcome, medical care discrimination, and decision to discontinue medical treatment.
Conclusion: The COVID-19 pandemic has posed huge ethical challenges for healthcare professionals that might lead to psychological issues given the emotional toll related to making life-and-death decisions.
Recommendation: In a situation where no reliable and certain treatment is known or well tested, establishing centralized and responsive ethical committees could help reassure and guide practitioners and address their concerns.
Keywords: coronavirus, COVID-19, ethics, medical discrimination, end of life, patients’ rights
Background
The COVID-19 pandemic resulted in unprecedented challenges for healthcare systems globally. Nearly 14% of people with COVID-19 develop severe illness that require hospitalization and oxygen support, and 5% require admission to an intensive care unit (ICU).1 Severe cases of the disease present with acute respiratory distress syndrome (ARDS), sepsis and septic shock, multi-organ failure, and cardiac injury. Being elderly with serious comorbid conditions, such as immune system disorders, have been reported as risk factors for death. COVID-19 studies in specific populations indicated that children and pregnant women do become infected, but with relatively few cases in infants.2 A review study reported that pregnant women were at a significantly higher risk compared with non-pregnant women.3 However, in children with COVID-19, the clinical presentation were less severe than in adults.4–6
The first case of COVID-19 in Saudi Arabia was reported on March 2, 2020. The number of cases is still increasing. On August 3, 2021, the Saudi Ministry of Health reported 528,952 cases and 8270 deaths confirmed in Saudi Arabia.7,8 Unfortunately, though many approaches are being tested globally, none are successful. In addition, there are still uncertainties about the virus itself.9 Decision-makers in the healthcare system in Saudi Arabia are responsible to react to the global pandemic, to prevent rapid transmission and facilitate effective containment. To achieve this goal, it is important to consider the factors playing a critical role in the spread of the disease, including population density, local evolution of COVID-19, the lifestyle of a society, and other factors.10 The population of the Kingdom of Saudi Arabia (KSA) is 35 million people, the majority (84%) are urban, resulting in urban hospitals experiencing massive pressure during the peak of the infections.11,12 Literature indicate that public collaboration with government, a robust healthcare system, and justice support the management of significant outbreaks.13
The pandemic created an international public health emergency, testing the healthcare services in every country, including wealthy industrialized nations.14 In addition, the novel coronavirus resulted in an economic, humanitarian, and human rights crises, including a host of ethical challenges.15 There are growing tension in healthcare as physicians have to balance the health of an individual patient with the health of the entire population. The increased demand for hospital beds put significant pressure on medical service providers. Approximately 9–11% of COVID-19 patients require advanced life-support in an ICU or mid-care unit, which challenged the preparedness and capacity planning of the healthcare systems and hospitals and tremendously increased the burden on them while they are dealing with this worldwide crisis.16
Globally, the majority of the healthcare systems, including the advanced emergency systems, were critically compromised and overwhelmed with COVID-19 cases. Overcrowded emergency departments struggled with the risk of losing control in managing the huge numbers of highly infectious patients.17 In many parts of the world, the demand for critical care services exceeded the supply. This scarcity of resources, coupled with the large volume of patients, challenged physicians to make crucial decisions about who should receive critical medical care, such as a ventilator, knowing that the patients who did not receive care would likely die. Physicians had to prioritize the patients who were the most likely to survive rather than patients with a limited chance of survival.
This reality stimulated a complex and difficult debate about the right of everyone to have access to healthcare. Although utilitarianism, as an ethical theory, states that an action is considered ethical and acceptable if it only has beneficial consequences, justice and equal rights as ethical principles, are still in conflict. In addition, the COVID-19 pandemic also raised other ethical issues. For example, given the urgency to obtain a vaccine or treatment for COVID-19, the slow pace of randomized controlled trials is questioned in the context of combating the virus and ensuring the patients’ best interests.18
In general, the COVID-19 pandemic caused increased stress for many people. Fears and uncertainty about the virus, with the anxiety and stress due to the lockdowns and social distancing laws resulted in various physical and psychological problems in people globally.19 Self- and family protection strategies caused frustration, dread, anxiety, and misery, all of which can disrupt an individual’s homeostasis.20
The study aimed to explore the ethical challenges experienced and perceived by healthcare professionals working in healthcare institutions and research centers in Saudi Arabia. The findings are expected to highlight the salient ethical issues arising during emergency situations to support authorities in the development appropriate policies and guidelines.
Method
A qualitative research method was employed in this study to investigate the perspectives of healthcare professionals on the medical management of patients with COVID-19. This method was chosen as it allows us to understand a complex phenomenon from the perspective of the participants. The study was conducted at King Abdul-Aziz Medical City, which includes King Abdullah Specialized Hospital and King Abdullah International Medical Research Center (KAIMRC), in Riyadh, Saudi Arabia.21 To date, this tertiary medical facility has received more than 24,233 cases of COVID-19 since the outbreak.
Data Collection
Participants were selected using a purposive sampling strategy. In particular, frontline healthcare providers (physicians and nurses), researchers, and decision-makers involved in the management of COVID-19 cases were chosen. Participants were fluent in English, which is the official language of communication between employees. Data were collected using a semi-structured interview with each participant as this is a suitable method to learn their perspectives on the medical management of COVID-19 cases. Accordingly, interviews were conducted individually face to face. The duration of each interview, whose audio was recorded, was from approximately 45–60 minutes. The interview guide to help the interviewer address the aim of the study was composed of four open-ended questions revolving around ethical challenges related to the medical management of COVID-19 cases, scarcity of resources in this emergency situation, appropriateness of giving care, and discontinuing medical treatment.
Data Analysis
The data were analysed using the thematic analysis technique, which is an inductive approach to qualitative data analysis and refers to the process of identifying and interpreting patterned meaning within the collected data. The accuracy of the transcribed interviews were double checked by the research team, who read the transcripts multiple times to immerse themselves in the texts and to ensure complete comprehension. The analysis approach consist of several phases, including coding, searching, reviewing, defining, and naming themes.22 The study team highlighted important statements and labeled them with codes explaining the content. The statements were grouped based on the codes to gain a better understanding of the recurrent patterns and common meanings, as well as to give each topic a concise theme’s name. The analytic narrative is presented with the supporting quotes, and contextualized in current literature. The type of analysis is reiterative and recursive, meaning the analyst goes back and forth between the phases. The analysis was performed separately by the research team members, and the outcome compared to ensure the rigor of the study.
Ethical Concerns
Ethical approval was obtained from the Research Ethics Committee at KAIMRC with protocol number (RC20/223/R). Participants were provided with study information explaining various relevant aspects of the study, including its purpose and the nature of participation, which was voluntary. Participants accepted by signing the informed consent to participate and their response will be published. No personal information was collected, and participants’ responses were anonymous.
Results
Sample Profile
The study sample was composed of 24 clinical and non-clinical healthcare providers with different specialties and qualifications. The participants were experts in experimental medicine (n=5), staff in ICUs (n=2), medical laboratory workers involved in the analysis of COVID-19 samples (n=10), and IRB members who participated in the evaluation of research proposals related to COVID-19 (n=7). This blend of specialties enriched the data by ensuring there was a diverse mix of profound experiences and feelings. The majority of the participants were males (n=17). There were 14 Saudis. Table 1 provides more description of the participants’ characteristics.
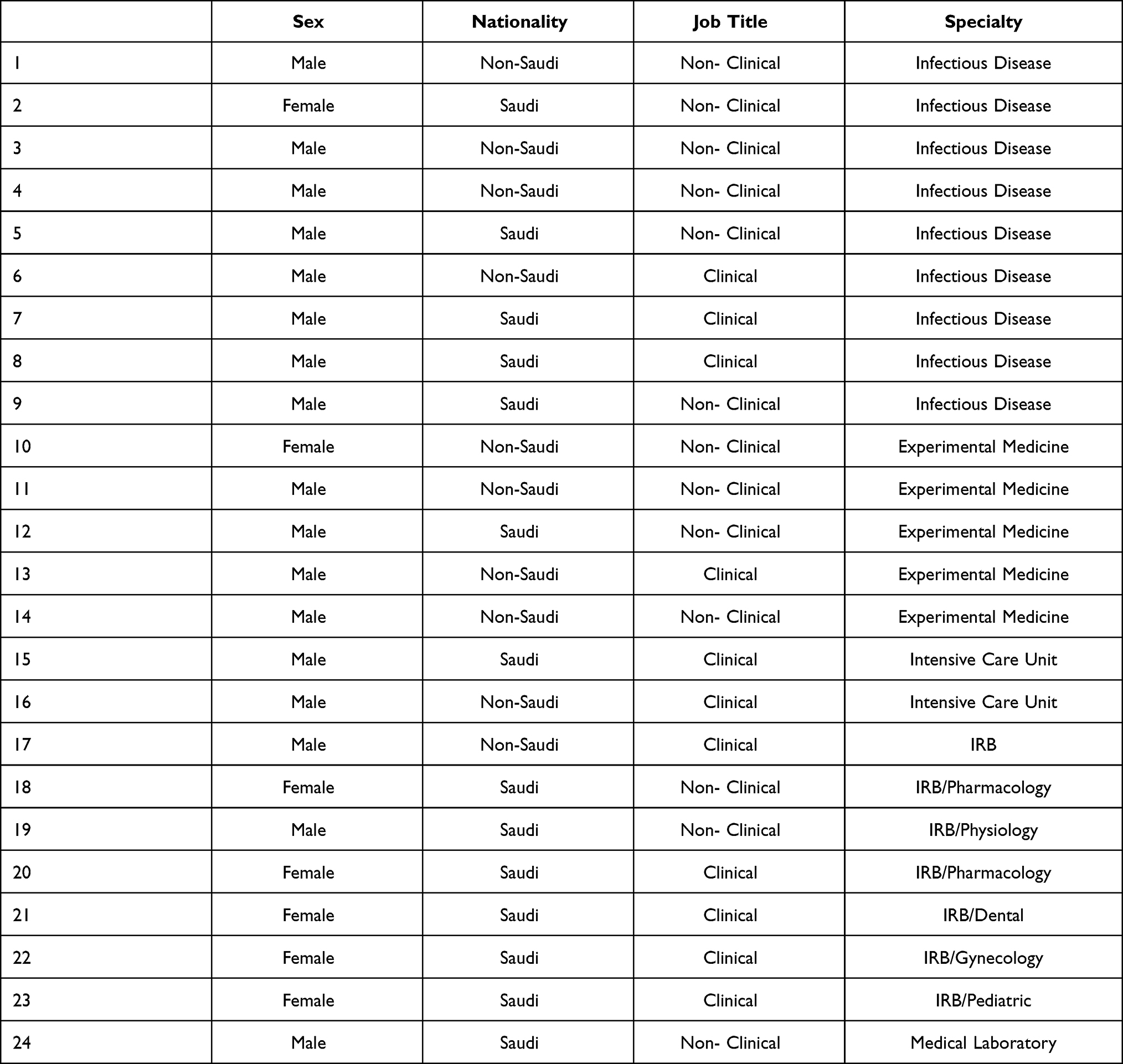 |
Table 1 Participants’ Characteristics |
Interview Findings
In this section, we present the findings of the interviews with the healthcare professionals, which were grouped around four main themes: a) Treatment challenges related to COVID-19 patients, b) uncertainty about the medical outcome, c) medical care discrimination, and d) decision about discontinuing medical treatment.
Treatment Challenges Related to COVID-19 Patients
Participants reported diverse emotions and feelings related to the practiced medical care for patients infected with COVID-19. However, negative emotions were dominant due to the lack of evidence-based treatment. Some participants expressed their resentment toward the use of certain medicines that had not been properly tested through the regular process of clinical trials. Authorizing these medications, even in emergency situations, was unethical in their view. Patients should not be exposed to unsafe medicines in the hopes they will be effective in treating patients’ conditions. Some participants believed that approving such medications was for political gain rather than a medical decision that should be made by physicians. For example, two participants stated the following:
Well the treatment! I think it’s a shame! I was against it. I was one of those people who opposed chloroquine at the beginning because we should not try anything [on patients] that did not go through RCTs [randomized clinical trials] Phase 3 … It should not be imposed by the Ministry of Health … this is what is happening in France, Algeria, Saudi Arabia … the therapeutic protocol imposed by higher up not by the doctors in the bedside. So, normally, the decision should be from the physician … not political decisions and we knew longer after that it’s disastrous …
I think there’s a lot of treatments that were tested without being tested in animals and human … I think it a source of backfire. It is not because there is no treatment that you should do nonsense … so this is what is happening in general in COVID-19 … I think the politician [is playing] a big part of it.
Another participant emphasized that it is the healthcare practitioners’ responsibility to provide treatments in relation to the severity of the patient’s disease. They should not attempt any new treatment regimen for the sake of trying it without proper indications.
If the medicine is there, it should be given to the patient after proper evaluation of the disease stage … but if the [patients’] diseases are mild and you give them medicines that are irrelevant to [their conditions] … then it would be unethical. So, you know the issue of ethics depends on the practitioners
Uncertainty About the Medical Outcome
Lack of evidence related to an effective treatment regimen for COVID-19 cases has generated some ethical challenges for healthcare providers. While they attempted to provide medical care to the best of their knowledge and ability, they were uncertain about its effectiveness for some cases due to the ambiguity in the virus’ behavior. This kind of uncertainty has put patients in a difficult situation in which they are unable to make informed decisions about the offered treatment as described in the following quote:
The biggest challenge [regarding treatment] is to know the outcome because most of it is not based on solid evidence … I mean there is constantly evolving evidence, but the patients are not in positions to deny anything at that stage; majority is to provide the best available information … based on care and treatment to the patients.
Some participants expressed feeling moral uncertainty due to the lack of clinical evidence to support the available treatment:
There is no effective treatment or proven one, so … the most ethical challenge for me is giving the antivirals without evidence.
We don’t have proven therapy [for COVID-19] so we should not give patients unapproved medication. So, including patients in the clinical trials is the best option.
Participants exhibited their disagreement with giving medications to COVID-19 patients without prior proof of the efficacy and safety of the drugs. In their opinions, these new treatment regimens (medications) should only be given to patients enrolled in clinical trials. Such uncertainty about the treatment outcome has generated psychological distress for healthcare providers. The uncertainty about the future and the consequences of medical management a psychological reaction known as moral uncertainty might be developed.
Medical Care Discrimination
With regards to the priority of providing medical care to COVID-19 patients in this emergency situation, most participants stated care should be provided based on need and who arrived for treatment first. They rejected any kind of discrimination as care should be provided equally to the population regardless of factors such as ethnicity, age, gender, and class:
If you open the door for discrimination [with regards to who will receive treatment], then it will be women versus men, black versus white, rich versus poor, obese versus slim … so that’s my answer is: first come first serve. I was shocked about what happened in Italy …
A major ethical concern like what happened in Italy that they have to choose between the young vs elderly people … has family or does not have a family. So, this is the biggest ethical challenge: on whom to provide care and whom to deny.
Other participants emphasized that priority of care should be based on whether it will be beneficial for the patients or not, meaning the patients’ outcome prognosis is the criteria:
First come first serve! … I have been working in ICU for 40 years … sometimes in the ICU when it’s full … you have to save four patients who crashed at the same time. Then, you have to make selections. So, what we do is to select based on the patients’ outcome prognosis.
We do not allow any kind of discrimination … The only criteria is would the patient benefit from the care or not …
One participant explained that patients on a respirator should continue receiving care, which should not be withdrawn until death, regardless of the prognosis:
If someone is in ventilator and he is not doing very well, I do not stop the ventilator until he die …
Interestingly, one participant believed that care should first be directed to the elderly as they had the greatest need compared to young people with stronger immune systems to resist the disease:
I think the priority of care should go to elders [with chronic diseases, such as] heart diseases, diabetes, etc., because they are the ones who are most affected by the virus. Young people usually have strong immunity. I don’t think the priority should go to them …
Decision to Discontinue Medical Treatment
Participants agreed that medical care should be provided in a fair manner to all patients whether they had COVID-19 or not. Unfortunately, in some cases, the hard decision of discontinuing medical treatment should be made, especially when resources are scarce and many patients need ICU care. From the participants’ perspectives, the criteria should be whether the patients will benefit from the given medical care or will it only prolong their suffering. Participants indicated that families are always engaged in the decision, but are usually in favor of prolonging the lives of their loved ones:
When there is no benefit from the medical care, it is better to terminate/stop the suffering and the agony of the patients. So, we talk to the family, but sometimes … the family would never agree with that … we tried to go around this situation by having three physicians to sign no code without the family, which I do not like personally.
The feeling of the family become really strange sometimes … when the patient is 86–90 years old and he is blind and he bedridden and the family want you to push further to do more and more. Sometimes, you deal with some people like this. Really crazy!
In a case when the patient requires a ventilator but there are not enough resources, one of the participants stated the decision of discontinuing care should be made by the physician if the patient is going to die, and the respiratory machine should be given to another patient who will benefit from it. He explained:
If the patient is going to die for sure, we’ll not continue using the ventilator for him. In the normal situation, they [healthcare practitioners] will inform the family first. But since there is an emergency situation, they should decide. Maybe they don’t have time to call the family. So, in this situation, if the patient is dying, they can do it.
Others believed that the decision to remove one patient from a respiratory machine who is less likely to recover for the benefit of another patient who is more likely to recover should not be the responsibility of the treating physician. The appropriate action should be determined by a medical committee, and then the decision should be discussed with the family.
Discussion
The ethical practices and challenging scenarios related to patients’ rights and healthcare have always been hotly debated.23 Today, COVID-19 has tested and led to ethical dilemmas for global healthcare systems in terms of medical management. This predicament has resulted in many countries racing toward developing an effective vaccine to combat the spread of the virus and also finding a proper treatment regimen for its manifestations. Therefore, lack of medical evidence for treating infected patients has contributed to many ethical challenges. Most healthcare practitioners have never dealt with a situation that pressures and challenges their ethics in this way. The uncertainty about what actions to take during the pandemic was obvious in the participants’ responses, including their opinions about the treatment of COVID-19 patients, medical outcomes, and who should receive care.
Participants in this study experienced many ethical challenges related to the treatment of COVID-19 patients. They felt pressured to follow certain treatment protocols, including administering drugs given for other types of diseases, such as chloroquine, that had not been rigorously tested for COVID-19. Similarly, healthcare organizations around the globe were pressured to try various existing medications, hoping to find an effective cure. Although the reason for using these medications is to benefit patients, unproven treatment protocols could expose patients to risk, which is ethically unacceptable given that patients in this situation are vulnerable and must completely trust their physicians. So, this practice challenges the ethical principles of beneficence and non-maleficence, in which healthcare providers have a duty to do no harm to patients.24 The COVID-19 pandemic has raised the following ethical questions: Do the pandemic situation and uncertainties about the disease justify breaking international regulatory guidelines to try new drugs directly on patients before going through the proper clinical trial phases? Does the urgency and necessity justify action?
The ethical dilemma the participants encountered and highlighted related to whether to give the patients medications known to treat other diseases, with side effects, led to feelings of frustration. This situation in which healthcare providers are unable to take the ethically appropriate action for their patients could lead to the development of a psychological reaction and being moral distressed.25,26 During emergency situations, healthcare providers might make decisions that conflict with their values, beliefs, and the fundamental role of their profession in providing competent and ethical care.
Participants raised another ethical issue during clinical trials: some healthcare practitioners/researchers were ready to try medications for the sake of trying them, regardless of patients’ proper health evaluation. The beneficence concept in ethics aims to ensure the well-being and welfare of patients/research participants during clinical trials and research.27 The accurate and proper diagnosis of an illness and its severity must be prioritized by practitioners/researchers to maximize benefits and minimize the harm to patients as much as possible.
Ensuring justice among patients who receive treatment was another ethical challenge. The participants in this study experienced ethical dilemmas during the COVID-19 pandemic, particularly related to what was happening in certain parts of the world, such as Italy, where emergency rooms and ICUs were overwhelmed by COVID-19 patients.28 Therefore, physicians and nurses had to decide to whom to provide urgent care and treatment. The ethical considerations related to this challenge, which have already been discussed for decades, are currently being faced in emergency rooms and intensive care units. Providing fair distribution of resources and ensuring patients’ rights and equality are respected are ethical obligations that must be met by healthcare providers to ensure justice in relation to patients’ treatment.29
Different approaches by healthcare providers/participants in this study were considered to justify their decisions related to the ethics of medical care discrimination during emergency situations. They reflected on the fact that some physicians and nurses have acted compassionately toward patients, meaning they have prioritized patients with family and dependents and given precedence to seniors over younger patients. This might be contrary to the ethical principles of justice when it comes to medical treatment as they are obligated to provide fair medical care to all. Another approach based on logic, rather than compassion, was suggested by the participants: the patient who is responding to the treatment/care should be served first and resources should be reallocated from unresponsive patients. To ensure justice in this situation, it is important to make certain that healthcare resources are used fairly.27
The COVID-19 pandemic has also led to the urgent question of whether to stop medical treatments, such as ventilators, for patients who are unresponsive/not benefiting from treatment. This action could be justified by the fact that if resources are limited, equity is still necessary for justice. To ensure ethical decision-making in this case, it is important to make certain no negligence exists, consent has been secured, and no progress has been made with treatment.30 However, all these scenarios and ethical considerations must be discussed and debated further to ease the burden on and confusion among healthcare providers.
As in all research, this study had strengths and limitations. Its main strength was the fact that the sample was composed of frontline ICU consultants, infectious disease consultants, nurses, scientists, and decision-makers who had rich and illuminating experiences to share. One notable limitation was that the participants were from a single hospital where a coronavirus outbreak occurred in 2014. Thus, their experiences might be different from those working in other settings who had not previously dealt with a similar outbreak. Further studies are recommended at national and international levels to explore the experiences of frontline professionals, including nurses and physicians, working in different hospitals.
Conclusion
Due to several factors, including the nature of the pandemic, the large number of infected individuals, shortage of resources, and ambiguity regarding treatment procedures, the health crisis produced by the COVID-19 pandemic created significant ethical challenges for healthcare professionals. The ethical dilemmas that the study participants highlighted is related to using treatment without medical evidence, the uncertainty of the outcome, the patient’s right to treatment, justice, and situations necessitating difficult decisions related to who should receive care. Such ethical dilemmas could lead to the development of psychological reactions. Establishing centralized and responsive ethical committees may assist, comfort and advice practitioners through addressing their concerns when no dependable and definite therapy is known or scientifically proven.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Research Ethics Committee at KAIMRC. No personal information was collected, and participants’ confidentiality and privacy were respected.
Consent for Publication
We declare that the manuscript has been read and approved by all authors.
Acknowledgments
We would like to thank King Abdullah International Research Center KAIMRC for approving this study. We also would like to express our gratitude to the healthcare professionals who participated in this study.
Funding
This study received funding from King Abdullah International Medical Research Center.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Novel CP. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2020;41(2):145.
2. Cai J, Xu J, Lin D, et al. Series of children with 2019 novel coronavirus infection: clinical and epidemiological features. Clin Infect Dis. 2020;71:1547.
3. Zambrano LD, Ellington S, Strid P. Update: characteristics of symptomatic women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status — United States, January 22–October 3, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(44):1641–1647. doi:10.15585/mmwr.mm6944e3
4. Xia W, Shao J, Guo Y, Peng X, Li Z, Hu D. Clinical and CT features in pediatric patients with COVID‐19 infection: different points from adults. Pediatr Pulmonol. 2020;55(5):1169–1174. doi:10.1002/ppul.24718
5. World Health Organization. Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease is Suspected: Interim Guidance, 13 March 2020. World Health Organization; 2020.
6. Adly HM, AlJahdali IA, Garout MA, Khafagy AA, Saati AA, Saleh SA. Correlation of COVID-19 pandemic with healthcare system response and prevention measures in Saudi Arabia. Int J Environ Res Public Health. 2020;17(18):6666. doi:10.3390/ijerph17186666
7. Ministry of health. MOH stresses importance of taking 2 doses of COVID-19 vaccine to prevent mutations; 2021. Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2021-08-03-007.aspx.
8. Barry M, AlMohaya A, AlHijji A, et al. Clinical characteristics and outcome of hospitalized COVID-19 patients in a MERS-CoV endemic area. J Epidemiol Glob Health. 2020;10(3):214. doi:10.2991/jegh.k.200806.002
9. Alrashed S, Min-Allah N, Saxena A, Ali I, Mehmood R. Impact of lockdowns on the spread of COVID-19 in Saudi Arabia. Inform Med Unlocked. 2020;20:100420. doi:10.1016/j.imu.2020.100420
10. Goumenou M, Sarigiannis D, Tsatsakis A, et al. COVID-19 in Northern Italy: an integrative overview of factors possibly influencing the sharp increase of the outbreak. Mol Med Rep. 2020;22(1):20–32.
11. Dixon T. What impacts are emerging from Covid-19 for urban futures? Oxford COVID-19 Evidence Service; 2020.
12. Worldometers.info. Saudi Arabia population. Worldometer; 2020. Available from: https://www.worldometers.info/world-population/saudi-arabia-population/#:~:text=The%20population%20density%20in%20Saudi,42%20people%20per%20mi2).&text=The%20median%20age%20in%20Saudi%20Arabia%20is%2031.8%20years.
13. NeJhaddadgar N, Ziapour A, Zakkipour G, Abbas J, Abolfathi M, Shabani M. Effectiveness of telephone-based screening and triage during COVID-19 outbreak in the promoted primary healthcare system: a case study in Ardabil province, Iran. Z Gesundh Wiss. 2020;1–6. doi:10.1007/s10389-020-01407-8
14. Mohideen MR, Yiwey FM. Ethical dilemmas in pandemics-lessons from COVID-19. Galle Med J. 2020;25(2). doi:10.4038/gmj.v25i2.8019
15. McGuire AL, Aulisio MP, Davis FD, et al. Ethical challenges arising in the COVID-19 pandemic: an overview from the Association of Bioethics Program Directors (ABPD) task force. Am J Bioeth. 2020;20(7):15–27.
16. Deschepper M, Eeckloo K, Malfait S, Benoit D, Callens S, Vansteelandt S. Prediction of hospital bed capacity during the COVID-19 pandemic. BMC Health Serv Res. 2021;21(1):1. doi:10.1186/s12913-021-06492-3
17. Qureshi MN, AlRajhi A. Challenge of COVID-19 crisis managed by emergency department of a big tertiary centre in Saudi Arabia. Int J Pediatr Adolesc Med. 2020;7(3):147–152. doi:10.1016/j.ijpam.2020.08.001
18. Chamsi-Pasha H, Chamsi-Pasha M, Albar MA. Ethical dilemmas in the era of COVID-19. Avicenna J Med. 2020;10(3):102. doi:10.4103/AJM.AJM_119_20
19. Su Z, McDonnell D, Wen J, et al. Mental health consequences of COVID-19 media coverage: the need for effective crisis communication practices. Global Health. 2021;17(1):1–8. doi:10.1186/s12992-020-00654-4
20. da Silva ML, Rocha RS, Buheji M, Jahrami H, Cunha KD. A systematic review of the prevalence of anxiety symptoms during coronavirus epidemics. J Health Psychol. 2021;26(1):115–125. doi:10.1177/1359105320951620
21. King Abdullah International Medical Research Center [homepage]. Available from: https://kaimrc.med.sa/.
22. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;16(1):1609406917733847. doi:10.1177/1609406917733847
23. World Health Organization. Patients’ rights. WHO; 2020. Available from: https://www.who.int/genomics/public/patientrights/en/.
24. Jahn WT. The 4 basic ethical principles that apply to forensic activities are respect for autonomy, beneficence, nonmaleficence, and justice. J Chiropr Med. 2011;10(3):225. doi:10.1016/j.jcm.2011.08.004
25. Almutairi AF, Salam M, Adlan AA, Alturki AS. Prevalence of severe moral distress among healthcare providers in Saudi Arabia. Psychol Res Behav Manag. 2019;12:107. doi:10.2147/PRBM.S191037
26. Nathaniel A. Moral distress among nurses. Ethics and Human Rights Issue Update. 2002;1(3):3–8.
27. Alzheimer-europe.org. Alzheimer Europe - ethics - definitions and approaches - the four common bioethical principles – justice; 2020. Available from: https://www.alzheimer-europe.org/Ethics/Definitions-and-approaches/The-four-common-bioethical-principles/Justice.
28. Jachetti A, Colombo G, Brignolo-Ottolini B, et al. Emergency department reorganisation to cope with COVID-19 outbreak in Milan university hospital: a time-sensitive challenge. BMC Emerg Med. 2021;21(1):1–8. doi:10.1186/s12873-021-00464-w
29. Mawere M. Critical reflections on the principle of beneficence in biomedicine. Pan Afr Med J. 2012;11(1):29.
30. Welie JV, Ten Have HA. The ethics of forgoing life-sustaining treatment: theoretical considerations and clinical decision making. Multidiscip Respir Med. 2014;9(1):14. doi:10.1186/2049-6958-9-14
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.