Back to Journals » Risk Management and Healthcare Policy » Volume 16
Who is Facing Higher Increased Demand After the Online-Offline Channel Integration? Evidence from Public Hospitals in China
Received 17 July 2023
Accepted for publication 11 November 2023
Published 30 November 2023 Volume 2023:16 Pages 2635—2648
DOI https://doi.org/10.2147/RMHP.S431056
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Heng Zhao, Xuejing Cao
School of Economics and Management, Tongji University, Shanghai, 200092, People’s Republic of China
Correspondence: Xuejing Cao, School of Economics and Management, Tongji University, 1239 Siping Road, Yangpu District, Shanghai, 200092, People’s Republic of China, Tel +86 18116152181, Email [email protected]
Background: In recent years, the medical industry has been significantly impacted by internet technology, especially with the growing integration of online and offline channel within public hospitals.
Objective: Our study aims to explore the effects of hospitals’ online-offline channel integration on doctors’ offline visits and investigate how the effects of integration varied across doctors with different professional titles.
Methods: Our study employs a panel dataset from a large comprehensive hospital in China and conducts staggered difference-in-differences (DID) approach.
Results: We find that online-offline channel integration within public hospitals is associated with about 15.5% increase in offline visits, and the 1% growth of monthly number of online visits is associated with about 10.6% monthly offline visits increase. Furthermore, our results indicate that the effectiveness of online-offline channel integration is more pronounced for doctors with lower professional titles compared to those with higher professional titles.
Conclusion: Our study provides evidence for policymakers and hospital managers that integrating online and offline channels can optimize the distribution of medical personnel resources within public hospitals. We recommend that young or less-experienced doctors actively participate in hospital-operated online platforms to enhance their professional skills through practical experience.
Keywords: healthcare, operation management, online-offline channel integration, public hospitals, staggered difference-in-differences
Introduction
Before the widespread adoption of internet technology in the healthcare industry, patients have difficulty in finding suitable healthcare providers due to limited access to information about doctors and a lack of understanding of their individual medical conditions. Generally, doctors with higher professional titles are more likely to be regarded as well-trained ones who are able to provide higher-quality care1,2 and therefore their workload is commonly heavier than that of doctors with lower professional titles.3–5 The introduction of online consultation channels within hospitals alleviates the information asymmetry between doctors and patients to some extent. By reducing the cost for patients to communicate with doctors, it becomes easier for patients to gain knowledge about doctors’ professional competence and service attitude after the online-offline channel integration. As a result, the demand for patient visits among doctors may be affected.
Empirical evidence from the medical field has demonstrated that the introduction of online channels can stimulate additional demand for offline medical services.6–8 On the one hand, due to the limitations of virtual visits, doctors may ask patients to come in person for face-to-face conversation and the use of medical equipment for testing and treatment after initial online consultations. On the other hand, patients, especially health-anxious people,9 may be more proactive in seeking communication with doctors after the introduction of online channels due to the reduced travel cost of accessing medical services. According to the trust transfer theory,10 trust established by patients in their doctors through online channels can be extended to traditional offline channels,11 resulting in an increased demand for face-to-face consultations with doctors whom they have previously interacted with online. It is worth noting that the increase in demand for offline visits triggered by the introduction of online channels may potentially aggravate the problem of medical resource imbalance in China. This issue is particularly pressing in light of the scarcity of high-quality medical resources, including those for doctors with higher professional titles, that are already in short supply. Current research shows that the opening of online medical services has a greater impact on offline appointments for doctors with higher professional titles.8
However, the results from existing relevant literature may not be generalized to our research context, since these papers7,8 only discussed about doctors’ online activities on third-party online health platforms, such as haodf.com. It is worth mentioning that doctors who open online consultation at third-party online platforms actually use their off-hours to provide service. Besides, the potential for increased social influence and financial gain offered by third-party online platforms is able to motivate doctors to take a more proactive approach in engaging with them.2–12 It is predictable that opening online services on third-party online platforms could increase their offline appointments.
In our context, online services are operated by hospitals instead of e-commerce enterprises. In recent years, public hospitals in China have been progressively introducing online channel and integrating online-offline service. Hospitals view their online platforms as an additional channel for outpatient treatment delivery, and the fees for online consultations and duty rosters are determined by the hospital’s administrative department according to traditional norms. On the contrary, doctors have more agency in third-party healthcare platforms where they are able to negotiate their payment and work schedule. Given the differences in research contexts, it is crucial to employ appropriate data to examine the impact of online-offline channel integration on the offline visit demand of doctors with different professional titles in public hospital settings.
To clarify this issue, we employ a panel dataset from a large, comprehensive hospital in China that captured the online and offline visits of 725 doctors with various professional titles over a 27-month period. During this observation window, the hospital gradually introduced online medical services for some of the doctors. We conduct a staggered difference-in-differences (DID) analysis and find that the integration of online-offline service is associated with about 15.5% additional offline visits, and that the number of online visits has a positive impact on the number of offline visits, which contradicts the original intention of using the online channel as a substitute for the traditional channel. More importantly, our results indicate that the effectiveness of the online-offline channel integration is more pronounced for doctors with lower professional titles compared to those with higher professional titles. Furthermore, the results of split-sample analysis show that it has no significant effect on doctors with higher professional titles, who are already overloaded. According to the study,13 there exists an inverted U-shaped relationship between workload and performance, suggesting that the optimal level of employee performance is achieved when the workload is moderate. In the current Chinese medical system, doctors with lower (vs higher) professional titles often experience a lower visit demand.3–5 Therefore, it can be inferred that hospitals’ implementing a moderate online-offline service integration has the potential to optimize the utilization level and enhance the performance of doctors with lower professional titles, while maintaining the service quality delivered by doctors with higher professional titles.
Literature Review
There is growing attention from researchers towards the innovation of healthcare service delivery. This study is closely related to the stream of literature on the impact of e-visit adoption on physicians. Previous studies have provided substantial evidence that online consultation services can positively impact service providers in several ways. Firstly, online consultation can strengthen physician-patient communication and enhance the relationship and trust between them,14–16 especially during the pandemic.17 Secondly, physicians can gain popularity and broaden their service channel to more available patients.18 Thirdly, after the opening of online consultation, physicians’ monetary return and reputation may increase through online knowledge sharing.19,20 Lastly, some studies suggest that online consultation can help physicians save time and improve their operational efficiency.16,21 However, online consultation may create excess work burdens on healthcare providers, and they are concerned about safety.22 Online consultation may not be safe, effective, and convenient if patients and physicians do not know and trust each other enough.23 Physicians who use nontraditional consultations (telephone, text messaging, email, and other virtual online consultations) may miss rare but serious conditions and/or lead to face-to-face visits in subsequent days.24 They may experience worse work-life balance, working additional hours resulting from patients’ e-visits on evenings and weekends.25 Furthermore, acceptance of online consultation varies due to individual differences in physicians’ perceived usefulness, perceived ease of use, and perceived behavioral control. In other words, some physicians who are unfamiliar with internet technology are more likely to believe that online consultation complicates their daily work.26
The limited number of studies most relevant to this research have explored how the impact of physicians’ adoption of a new service channel on their offline service quantity. Prior studies indicate that physicians’ consultation service and article sharing at online platforms can lead to increases in offline service quantity,7 and find that opening online consultation services improve the interaction between physicians and their patients, which is based on the signaling theory, then increase physicians’ offline appointments.8 However, one study finds differently that physicians’ participation in online platforms experience decreases in offline service quantity, which indicates that physicians might substitute part of offline service with online consultations.27 Similarly to our study, some literature explore the heterogeneous effect across different healthcare service providers.7,27 They examine various moderating factors, including but not limited to the doctors’ professional titles, medical specialties, and “recommendation heat” on third-party online platforms.
Although the prior studies have attempted to utilize the term “online-offline integration” as their research background or independent variable, the “integration” here is not clear-cut since physicians’ online activities in their studies are conducted on a third-party (e-commerce-operating) online platform. Consequently, physicians have to perform these activities during their off-duty time since the majority of their time is spent attending to patients in their affiliated healthcare institution.7 Thus, the mixed results from existing literature cannot be directly generalized to our research context. Our study aims to address the research gap by examining the online activities of physicians on a hospital-operated online platform, where their online professional activities are integrated with their offline work, taking place during their on-duty time and are supervised by the healthcare institution, ie, the public hospital. Examining the impact of physicians’ adoption of online consultation on hospital-operated platforms is of substantial practical value and research significance, particularly in China where a substantial number of physicians are affiliated with public hospitals. Moreover, compared to empirical studies conducted on third-party online platforms, investigating physicians’ adoption of online consultation on hospital-operated platforms presents a lower risk of self-selection bias.
Methods
Hypotheses Development
This study first explores the main effects of online-offline channel integration on doctors’ offline visits. Healthcare service could be termed a “reputation” good,28 accumulated reputation can help to reduce information asymmetry and build the trust between service providers and patients, significantly influence patients’ choice.29–33 Meanwhile, doctors’ online activities would enhance their professional reputation accumulation and strengthen doctor-patient relationship.27,34 According to the trust transfer theory,10 patients can transfer the trust in a specific doctor established online to the offline channel, in other words, when they seek traditional office visits, they prefer to visit the doctor with whom they have previously established a relationship online.11 Similarly, according to the signaling theory,35 opening and providing online consultation services could be interpreted as a signal of doctors’ willingness to communicate with patients and whether they care about patients, perhaps leading to additional offline visits.8 One study suggests that although patients’ e-visit adoption causes additional offline visits, there is no evidence showing that doctors’ e-visit adoption has a significant impact on the demand for office visits, however, they find the number of new patients significantly decrease post doctor e-visit adoption.6 Accordingly, it may be expected that if the doctor work capacity has the flexibility to increase adaptively, doctors’ e-visit adoption may incur more offline visits in total. Some relevant studies obtain the similar result that the doctors’ online activities have positive effects on their offline visit demand.7,8
Based on the theoretical considerations and empirical findings from previous research, we anticipate that the online platform operated by the hospitals provides a convenient approach for patients to seek communication with doctors and build long-lasting relationship and trust with the doctor and hospital. As a result, it may attract more visits through the traditional offline channel. Thus, we propose our first hypothesis.
Hypothesis 1. Online-offline channel integration within hospitals is associated with doctors’ higher offline visits.
We further consider that the number of online consultations conducted by doctors represents the intensity of their intervention in the hospital-operated online platform. If doctors conducted more online consultations, they conveyed a stronger message that they are more inclined to care about patients’ convenience and are more willing to communicate with them, which could strengthen the “signaling value” of doctors online adoption.8,35 We propose the following hypothesis.
Hypothesis 2. Doctors conducting more online consultation have higher offline visits.
Following the development of hypotheses on main effects, we next specifically focus on determining if the change in offline visits of doctors who are assigned to serve patients online varies by the professional titles. Previous research targeting third-party online healthcare platforms observed that doctors with higher (vs lower) professional titles will experience a larger increase in offline demand from the utilization of online consultation and proposed the following possible mechanisms. Doctors with lower professional titles may encounter “cold start” problem due to information asymmetry;2,27 Doctors with lower (vs higher) are sending weaker signals for medical service quality, thus they attracts lower patient visits.8 However, our research context is different from them, which means that previous research findings cannot be directly applicable to our research hypotheses. In our context, there are three main differences between doctors with higher professional titles and lower professional titles.
(1) The doctors with higher professional titles may prefer conducting online consultation more on third-party platforms rather than hospital-operated platforms. This is because that on third-party online platforms, the doctors are viewed as the primary subject of service providing, whether it is during online consultation or through publicity propaganda; However, on online platforms operated by hospitals, the hospital is the primary subject of online medical services. Furthermore, compared to hospital-operated online platforms, third-party online platforms are considered to be a broader stage for doctors (especially those with higher professional titles) to increase their financial gains, as well as their popularity and reputation.2,12,27
(2) The doctors with higher (vs lower) professional titles are facing larger outpatient visit demand, but they have more heavy complex daily workloads that include but not limited to surgery-related tasks and administrative work. So, even if the adoption of online channel boost doctors’ offline demand, doctors with higher (vs lower) professional titles may have more “rigid and saturated” service capacity, making them less adaptive to changing visit demand.
(3) The mitigating effect of online-offline channel integration on information asymmetry may be stronger for doctors with lower professional titles. It is because the doctors with higher (vs lower) professional titles already have a higher reputation and popularity among patients and the general public. Patients easily develop a certain level of trust with them due to their high professional titles and accumulated word of mouth over time, even before having any direct contact with them. In contrast to doctors with lower professional titles, their level of professional skills and service attitude are usually underestimated by the potential visitors. Hospital-operated online platform, which is targeted more on treating less-acute and less-serious patients, provides a new approach for those less-trained doctors to be noticed and visited, helping reduce the information asymmetry between them and patients. According to the trust transfer theory,10 the trust of service quality established during the initial online conversation could lead to the development of long-term relationships and subsequent offline visits. Thus, we propose the following hypothesis.
Hypothesis 3. The effects of online-offline integration and online visits will be stronger for doctors with lower (vs higher) professional titles.
Data and Measures
The data for this empirical study was collected from a China’s grade A tertiary hospital, the highest level in the nation’s three-tier hospital rating system.36,37 Our data set includes all monthly outpatient care counters of 810 doctors across both online and offline channels during a 27-month period, from January 2020 to March 2022. Doctor attendance in the outpatient department varies; some doctors have no outpatient visit record in some months due to “late entry” and “early exit” in study sample, which is commonly observed in related empirical study settings.6 Thus, we end up with an unbalanced panel data sample, including 17,090 physician-month observations. The only limitation we have on our sampling is that doctors who have served for less than six months during the study period are excluded. We impose this restriction since the focus of our research is active outpatient service providers in this healthcare system. This reduces our sample to 727 doctors with 16,704 doctor-months observations.
In order to enhance the understanding of the overall demand trends for both offline and online service channels of the hospital, we demonstrate the trends of offline and online visitors over time in Figure 1. In the figure, the abrupt surge in online visits and the sudden decline in offline visits in the 27th Month (March 2022) can be attributed to patients’ increased preference for online visits due to concerns over the pandemic, but at this time, the complete lockdown had not yet begun, and patients could still choose to visit offline.
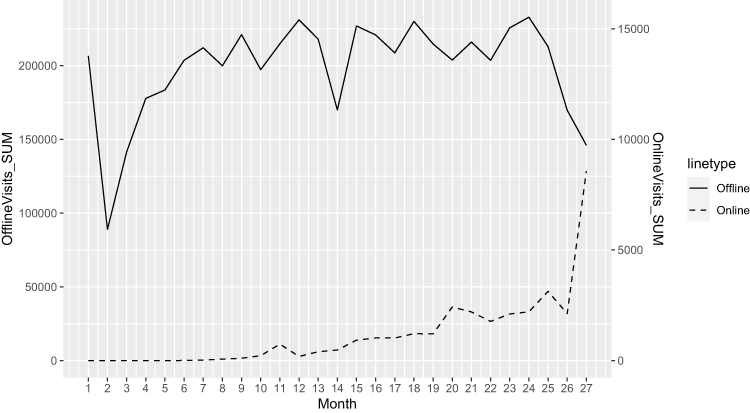 |
Figure 1 The Trends of Offline and Online Visitors Over Time. Notes: (i) Our observation window spans from January 2020 to March 2022, totaling 27 months. (ii) The downward trends in the 2nd, 14th, and 26th months are mainly due to the Chinese New Year holiday, which typically falls in February each year. |
It is worth noting that this study has largely minimized the influence of the COVID-19 pandemic on the results for several reasons. (a) The pandemic remained ongoing throughout the 27-month observation period. (b) Upon consulting city data, we found that although the COVID-19 pandemic started in 2020, the city’s only large-scale outbreak and complete lockdown measures began in April 2022. Our study excluded the period of complete lockdown, reducing the compulsory effects of the lockdown on patients’ offline visits. (c) All estimations in this study utilize fixed-effect models to control for time-specific effects at the monthly level.
In Table 1, we show the specific definitions and descriptive statistics of all variables. This study collects the monthly offline visits, monthly online visits, and attributes of doctors, including age, gender, professional title, department, whether they have adopted online channel and the time the adopter first adopted online channel. Note that not all doctors have adopted the online channel and not all adopters adopted the online channel simultaneously. Our outcome variable OfflineVisitsit refers to doctors’ monthly offline visits, measured by the number of offline outpatient visits that doctor i conducted in month t. Our main independent variables are Adoptionit and OnlineVisitit. The former is a dummy variable. The Adoptionit value equals one if the doctor i has adopted the hospital-operated online channel on or before the month t; otherwise, the value of Adoptionit equals zero. The latter is a numerical variable, OnlineVisitit, refers to the number of online visits that doctor i conducted in month t.
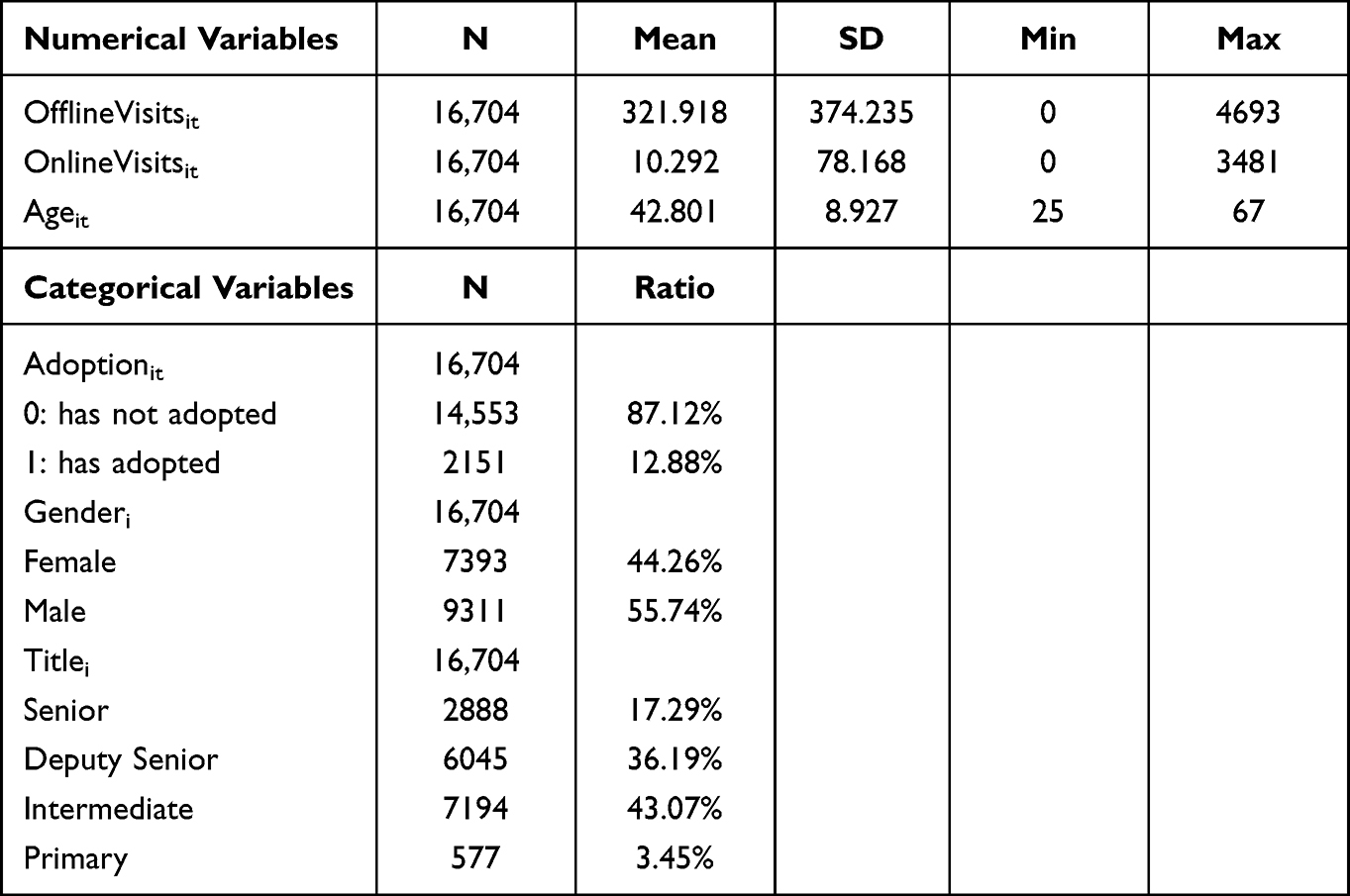 |
Table 1 Summary Statistics |
The occurrence of zero offline visits for a specific doctor in a given month indicates a significantly low demand for offline consultations. Such instances constitute a minor proportion within the dataset, as out of 16,704 doctor-month observations, only 12 observations recorded zero offline visits, involving seven distinct doctors. The occurrence of zero online visits for a specific doctor in a given month indicates not only a significantly low demand for online consultations but also the possibility that doctor i is a “non-adopter” or “not-yet-adopter” during month t.
Empirical Models
In accordance with government health ministries’ regulations, this healthcare institution launched the online-offline channel integration in June 2020 and scheduled doctors to take part in online consultations with outpatient patients. The introduction of online channels to doctors could be regarded as an exogenous shock that resulted in variances among doctors since it is determined by the administrative personnel in the executive office instead of the doctors themselves. To estimate the impact of online-offline channel integration on offline visits, we employ a staggered difference-in-differences econometric model to leverage our panel data structure while coping with variable timings of online adoption and controlling for doctor-specific and time-specific effects.6 The staggered DID regression model is given by:

We apply a logarithmic transformation for the outcome variable OfflineVisitsit because doctors’ monthly offline visits vary widely from ones digit to thousands digit in our study sample.8,38 The coefficient β1 captures the impact of online-offline channel integration on monthly offline visit. Our regression model also incorporates the individual (doctor) fixed effects and time (month) fixed effects, to control for unobserved time-invariant doctor characteristics and time-specific effect respectively. It is worth noting that we are including dummy variables for each month from January 2020 to March 2022 to control for time-specific effects (using “January 2001” instead of “January”), which have also accounted for seasonal and year fixed effects.
To further estimate the effects of channel integration on the traditional channel, we add the logarithmic transformation for monthly online visits log(OnlineVisitsit) into model 1 as the other independent variable in our research. Referring to the previous study analyzing of treatment intensity,8 the sample of estimation model 2 only including the doctor-months form doctors who adopted the online channel in our 27 months observation window. We conduct two-way fixed effect regression model to estimate the effect of the treatment intensity:

Additionally, we use lagged online visits to mitigate endogeneity issue caused by potential reverse causality between monthly offline visits and monthly online visits.39–43 We choose a one-month lag here instead of a longer duration because it aligns with the usual practice observed among patients, especially those with chronic conditions. Typically, these individuals receive monthly medication prescriptions from hospitals. The model is as shown in regression model 3:

Next, we examine the moderation effect of doctors’ professional titles on the impact of online-offline channel integration on offline visits. According to the professional title evaluation system in the context of China,27,44 doctors are categorized into four tiers, from relatively lower to higher in status: “resident physician” (primary), “attending physician” (intermediate), “associate chief physician” (deputy senior), and “chief physician” (senior). Following the moderator settings from earlier studies,27 we use the dummy variable LowerProfessionalTitlei to measure the groups. “Resident physician” and “attending physician” are classified as lower professional titles whereas “associate chief physician” and “chief physician” are classified as higher professional titles. The LowerProfessionalTitlei value equals one if the doctor i has a lower professional title and otherwise it equals zero. The moderating effect of professional titles on the adoption of online-offline channel integration is examined in econometric model 4:

The moderating effect of professional titles on the intensity of online-offline channel integration is examined in econometric model 5:

Additionally, to guard against reverse causality,39–43 we use lagged independent variable and moderator variable in our econometric model 6, which is identical to the approach employed in model 3:

Note that the moderator LowerProfessionalTitlei itself is subsumed by Doctori. Therefore, it is omitted from the estimating model 4–6.
Results
Main Estimations
The results of models 1–3 are presented in columns (1), (3) and (5) in Table 2 respectively. Column (1) of Table 2 shows that the monthly offline visits would increase by about 15.5% (e0.144-1) after doctors adopted the online channel, which supports Hypothesis 1. Column (3) of Table 2 shows that the monthly online visits have a positive influence on the monthly offline visits, which supports Hypothesis 2. Specifically, the 1% growth of monthly number of online visits is associated to about 10.6% monthly offline visits increase. The result of model 3, shown by column (5) of Table 2, strengthens the robustness of the estimation result of model 2. It indicates that if the monthly number of online visits grew by 1%, the number of offline visits next month would increase by about 5.0%.
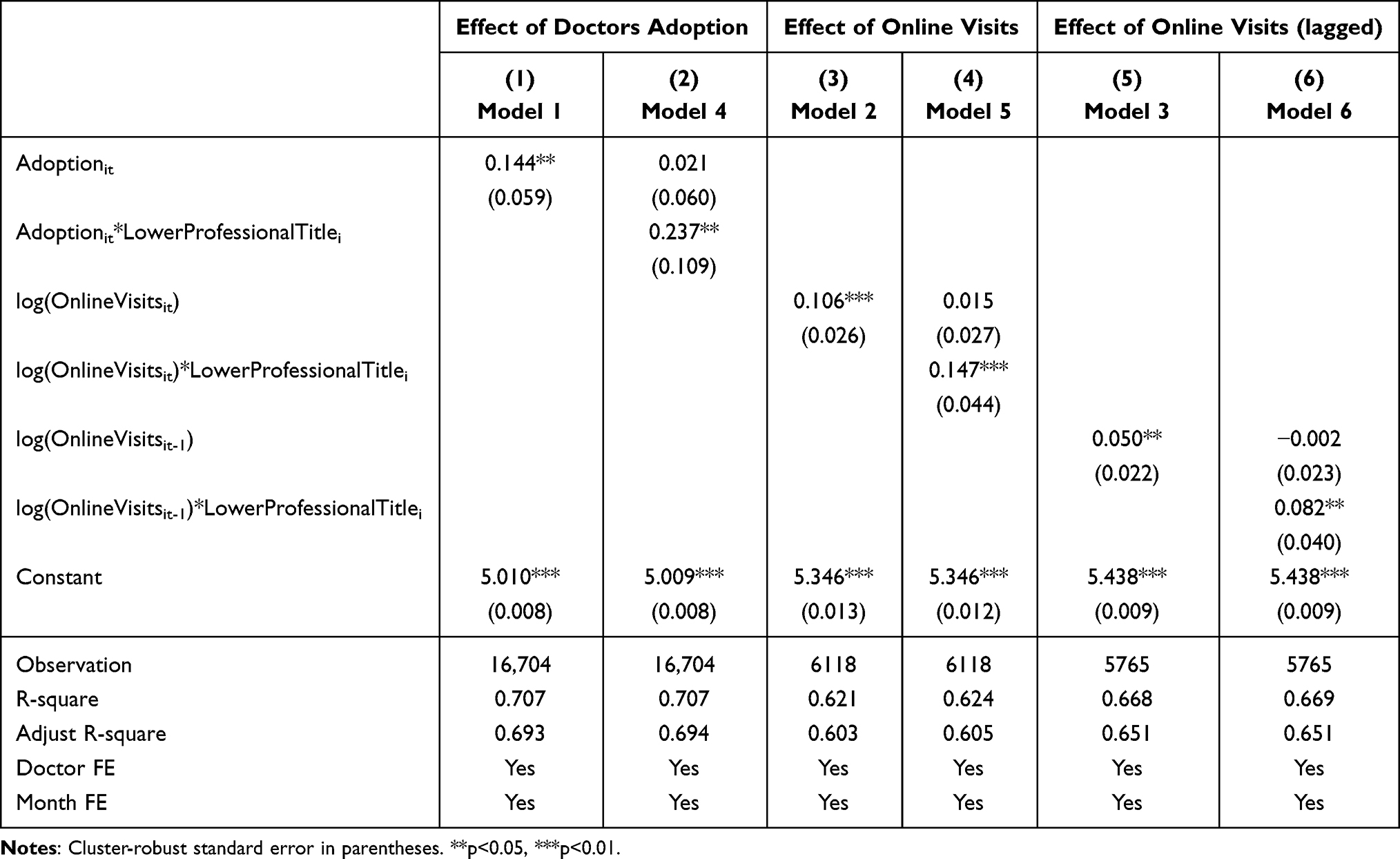 |
Table 2 Effects of Online-Offline Channel Integration on Offline Visits |
The results of model 4–6 are presented in the column (2), (4) and (6) in Table 2 respectively. In column (2) of Table 2, our result reveals that the coefficient of the interaction term Adoptionit*LowerProfessionalTitlei is significant and positive, Thus, compared to doctors with higher professional titles, those with lower professional titles gain more offline visits growth from online-offline channel integration. Moreover, column (4) and (6) of Table 2 present that the coefficient of the interaction term log(OnlineVisits)*LowerProfessionalTitlei is significant and positive, thereby indicating that with the same 1% increase in online visits, doctors with lower professional titles had a greater increase in offline visits than doctors with higher professional titles. These estimation results support Hypothesis 3.
Robustness Test
Parallel Trend Analysis
Following the literature,27,45 to test the parallel trend assumption of the difference-in-differences specification, we create a set of lead and lag indicators (month dummy variables) of each doctor-month observation, which are equal to 1 only in the corresponding month(s). Specifically, they are t_5 (five and more months before the adoption), t_4 (four months before the adoption), …, t0 (the adoption month), …, t4 (four months after the adoption) and t5 (five and more months after the adoption). We use five and more months before the adoption as the baseline (t_5), which is omitted in the parallel trend test. Figure 2 shows that there is no significant coefficient of the lead indicators (t_5 to t_1), indicating that the difference-in-differences (DID) approach is appropriate for this empirical study, which confirms the validity and robustness of our estimation results. Additionally, based on Figure 2, we observe a relatively rapid short-term growth effect of online-offline channel integration on doctors’ offline visits, and then the effect levels off after approximately one quarter. This suggests that the temporal impact of adopting an online platform tends to be short-term in nature.
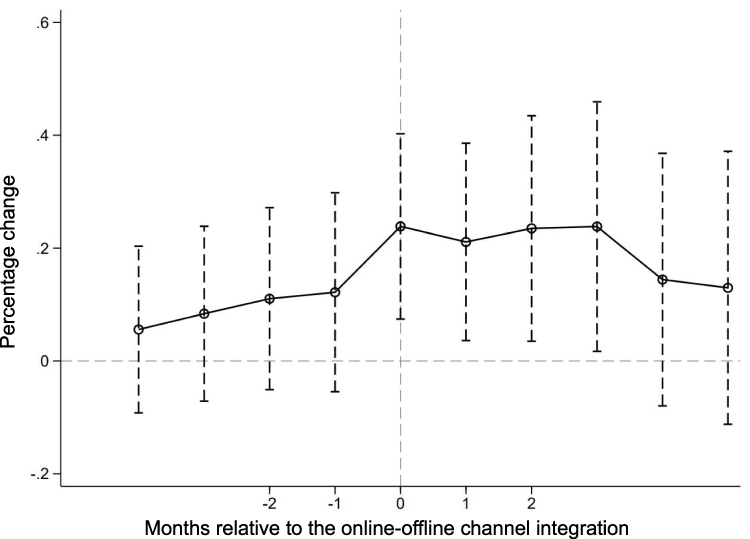 |
Figure 2 Parallel Trend Test Results. |
Propensity Score Matching - DID
One limitation of our empirical setting is that it cannot be fully guaranteed that the treatment group (online channel adopters) was selected randomly since administrative personnel in hospitals (policy makers) may have coordinated and communicated with doctors. To mitigate potential self-selection bias in our estimation due to systematic differences in characteristics between adopter and non-adopter doctors, we conduct propensity score matching to create a more balanced research sample.6,8,27 The matching characteristics are based on doctors’ attributes, including their age (average age during the observation period), gender, department, and professional title. Table 3 presents the summary statistics comparisons before and after using one-to-one nearest neighbor matching with a caliper of 0.25. The two groups of doctors are not found to differ significantly on any of the observed attributes after propensity score matching. Then, Table 4 shows the estimation results of model 1–4 based on the newly matched sample including 200 online channel adopters and 200 online channel non-adopters who generating 8986 doctor-month observations. The re-estimation results in Table 4 are consistent with our main results in Table 2, which corroborates our proposed findings.
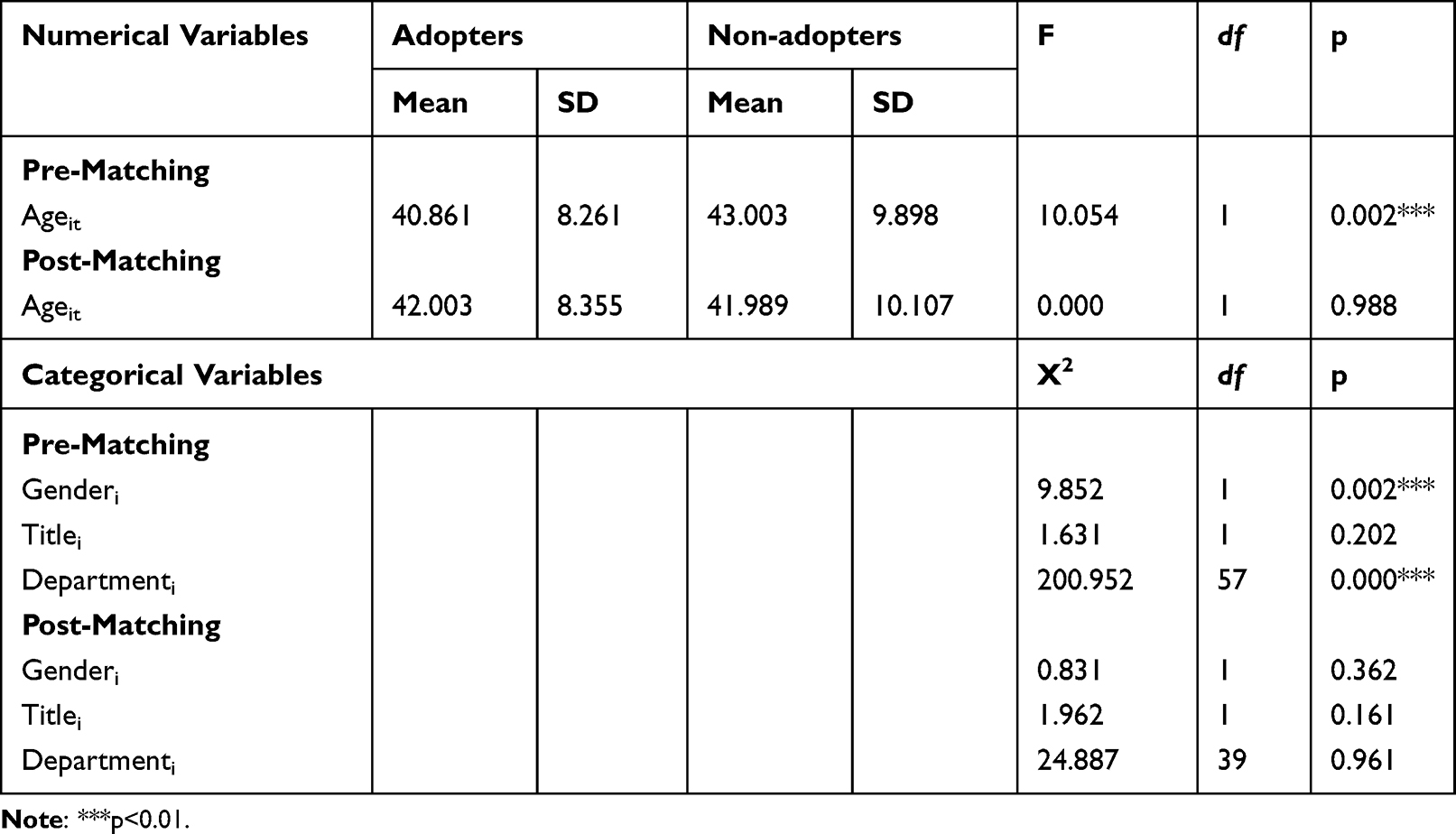 |
Table 3 Covariate Balance Pre- and Post- Matching on Covariates |
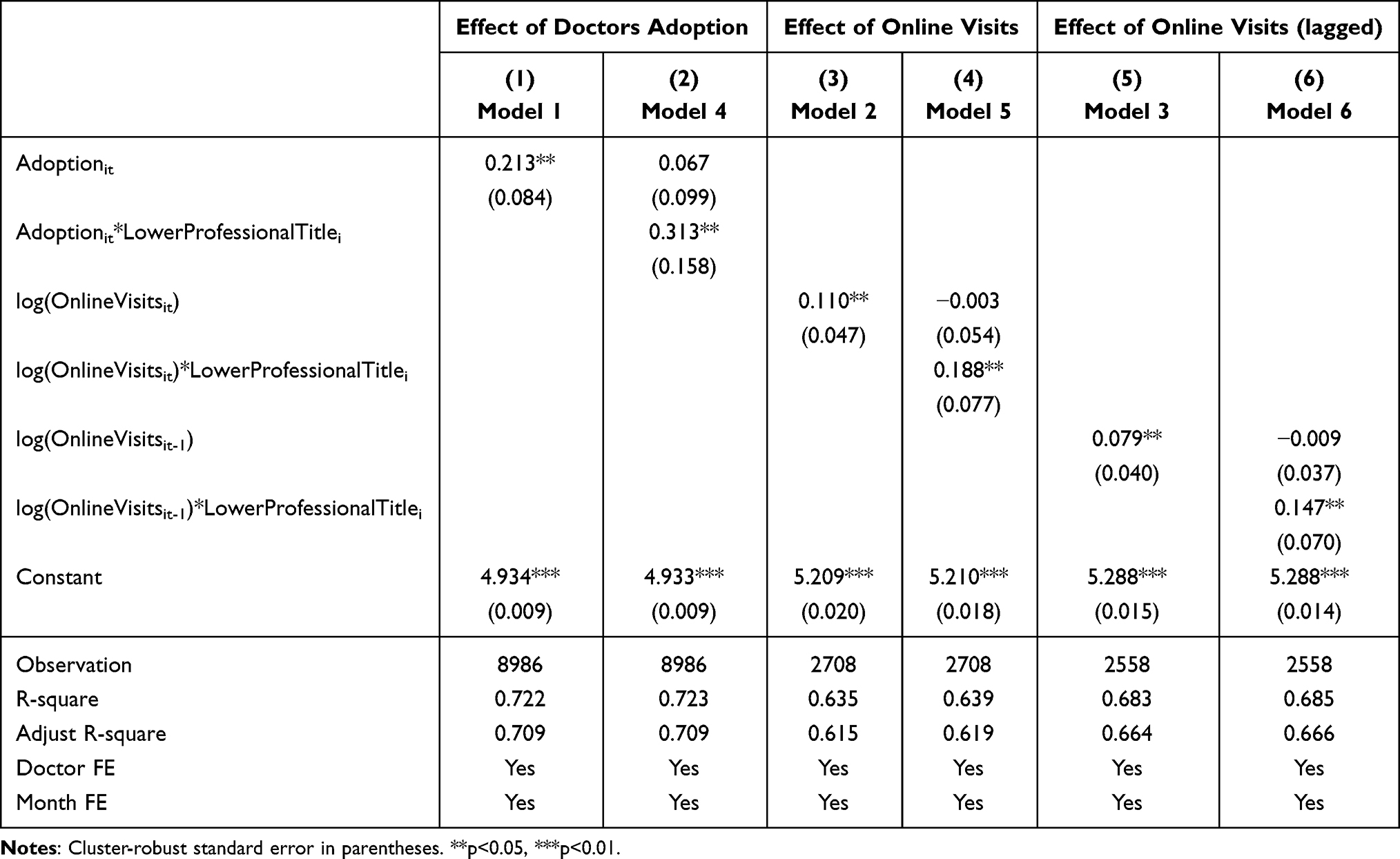 |
Table 4 Effects of Online-Offline Channel Integration on Offline Visits - PSM |
Split Sample Analysis
To further strengthen the heterogeneity analysis related to doctors’ professional titles, we conduct split sample analysis in the robustness check. The results of the split sample analysis, as shown in Table 5, are mostly consistent with the moderation effect analysis. Specifically, we observe that the regression coefficients for the group of doctors with lower professional titles are positive and significant, indicating that the adoption of online channel by doctors with lower professional titles would increase their offline visits, and more online service provided by doctors with lower professional titles bring more offline visits for themselves. However, the regression coefficients for the group of doctors with higher professional titles are positive but not significant. The split sample analysis provides further evidence that doctors’ adoption of online channels and provision of more online services have a positive impact on their offline visits, with a particularly noticeable effect among doctors with lower professional titles.
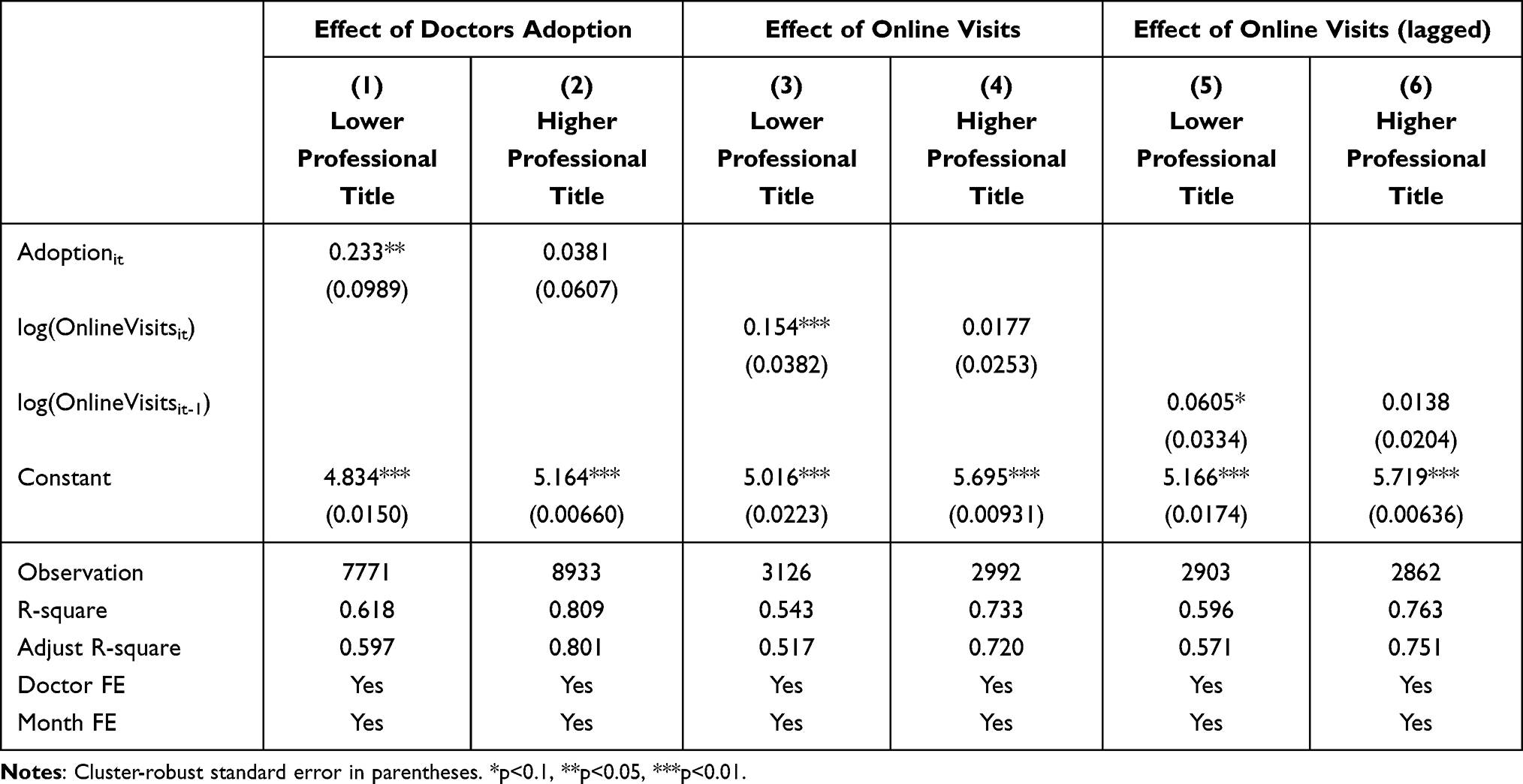 |
Table 5 Effects of Online-Offline Channel Integration on Offline Visits - Split Sample Analysis |
Discussion
Implications for Research
The current study analyzes a panel dataset from a comprehensive hospital that integrates online and offline medical services among its doctors to investigate the impact of this integration on the number of doctors’ offline visits, with an analysis of the heterogeneous effect across different professional titles.
We have found that the release effect of patients’ online medical demand spills over to the traditional channel. Specifically, when online channels are introduced within hospitals, it leads to additional offline visits. Moreover, the number of online visits has a positive effect on the number of offline visits. These findings may be attributed to the facts that (1) online patients are more likely to seek the same doctor offline for follow-up diagnosis and treatment due to the continuity of diagnosis and treatment activities. (2) the online healthcare platform facilitates more convenient communication opportunities between patients and doctors, enhances patients’ understanding of doctors, and therefore helps alleviate the issue of information asymmetry and establish stronger connections between doctors and patients.
Furthermore, this study provides crucial evidence for the moderating effect of doctor professional titles on the impact of online-offline channel integration on offline visits. Combined with the results of the split sample analysis, we propose that the introduction of online channels has a greater impact on doctors with lower professional titles, while having no significant effect on doctors with higher professional titles. According to the previous study,13 there is an inverted U-shaped relationship between workload and performance, which implies that employee performance is highest when workload is moderate. As mentioned earlier, doctors with lower (vs higher) professional titles have relative fewer patients in the current Chinese medical system.3–5 Hence, we infer that a moderate level of online-offline service integration has the potential to enhance the performance and utilization of doctors with lower professional titles, without compromising the service quality provided by doctors with higher professional titles.
Implications for Practice
Our research provides practical insights for policymakers and hospital managers seeking to promote the integration of online-offline medical service within hospitals. First, the implementation of online channels by hospitals enables patients to communicate more effectively with their doctors while still being able to receive offline treatment from the same doctor if necessary. The transformation in medical service and doctor-patient communication brought by the introduction of online channels induces a spillover effect on the traditional service channel. The government can effectively leverage the spillover effect from online to offline to encourage doctors to make better use of innovative online service modes. This will foster positive interactions between doctors and patients in offline settings, and promote orderly medical treatment.
Second, this study highlights the differences in the impact of channels integration among the group of doctors, demonstrating its positive effect on physician training and optimizing the allocation of medical personnel resources. Our findings suggest that the young or less-trained doctors should actively engage in hospital-operated online platform to improve their professional skills through more practical experience. Additionally, hospital managers could consider integrating service channel innovation with physician training to effectively enhance the overall team’s work efficiency and service capabilities.
Last but not least, this study also indicates that the implementation of online medical services may lead to an increased workload for doctors. As a result, hospital managers need to pay attention to changes in the quality of service provided by doctors. To address this issue, we recommend providing doctors with adequate training and support to help them adapt to the new service channel. Additionally, hospitals should consider implementing measures such as increasing the number of doctors or adjusting their work schedules to ensure that care quality is not compromised.
In general, online-offline channel integration plays an important role in enhancing the operational efficiency, effectiveness, and user satisfaction of healthcare delivery. It enriches the avenues for patient inquiries and choices for seeking medical treatment, and improves hospitals’ ability to match patients’ heterogeneous needs in terms of health conditions and travel costs. This has the potential to address the limited availability of traditional consultations and improve the allocation of medical resources. Besides, hospitals and doctors can benefit from increased reputational and financial outcomes, while patients can save on travel expenses (including both time and financial cost) associated with medical consultations. In light of these findings, it is strongly recommended to introduce online medical services in hospitals, and our study contributes to the theoretical basis for this service innovation.
Limitations and Future Research
Several directions are available for extending our work. First, to fully untangle the effects of online-offline channel integration on healthcare service supply efficiency, granular data on doctors’ work hours is required. For instance, if one study clearly demonstrates that doctors’ offline visits increase without any change in their work hours, it could be inferred that the introduction of online channels enhances doctors’ efficiency.
Second, we did not test the impact of online-offline channel integration on healthcare service quality due to data limitations, this presents a potential avenue for future scholarly investigation and requires the collection of empirical information relevant to healthcare quality measurements, including but not limited to patient satisfaction and changes in health indices.
Third, our dataset only focuses on the conduct of physicians within a specific hospital across both online and offline channels. It is crucial to recognize that our results could potentially be influenced by the distinct attributes of this particular hospital. Future investigations could strive to broaden the scope of our conclusions, encompassing a wider range of scenarios, in turn enhancing the relevance of our research findings.
Conclusion
In this study, we examine the impact of integrating online and offline medical services on offline visits using a panel dataset from an online-offline integrated comprehensive hospital. Specifically, we investigate how the effects of integration varied across doctors with different professional titles. Our findings indicate that online-offline channel integration within public hospitals leads to an increase in additional offline visits, with the number of online visits having a positive impact on the number of offline visits. This goes against the original intention of using e-healthcare platforms as a substitute for offline services. Moreover, we observe that the introduction of online channels has a stronger effect on doctors with lower professional titles, while the integration has no significant impact on doctors with higher professional titles, who typically have heavier workloads.
Ethics
We declare that this research does not involve any biological experiments, personal interviews, or surveys. It is important to note that we did not collect any information pertaining to patients. No patient medical records were accessed. Besides, there is no inclusion of directly identifiable data about the doctors. The hospital has anonymized the doctors’ data provided to us by assigning each doctor a random number as fake employee IDs for differentiation. No doctor identifiers were used.
As the data in this study were compiled using the available information in the Medical Administration Office of the hospital, the proposed activity is not a study on human participants in accordance with local legislation and institutional requirements. The collected data does not cause harm to humans, does not involve sensitive personal information or commercial interests, and is anonymized.
We declare that the data accessed strictly adhered to relevant data protection and privacy regulations. All procedures followed were in accordance with the ethical standards of the Institutional Review Board of Tongji University and the Declaration of Helsinki. The specific name of the hospital is not publicly disclosed due to privacy and ethical reasons. It can be provided from the corresponding author, upon reasonable request.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Liu X, Guo X, Wu H, Wu T. The impact of individual and organizational reputation on physicians’ appointments online. Int J Electron Commer. 2016;20(4):551–577. doi:10.1080/10864415.2016.1171977
2. Guo S, Guo X, Fang Y, Vogel D. How doctors gain social and economic returns in online health-care communities: a professional capital perspective. J Manag Inf Syst. 2017;34(2):487–519. doi:10.1080/07421222.2017.1334480
3. Ma Y, Yin P, Yang X, Mei W. Correspondence analysis on clinic waiting time for outpatients. Chin J Health Stat. 2013;30:2–4+8. in Chinese.
4. Zhang X. A comparative study on occupational stress of doctors. China Hospital CEO. 2014;222:47–49. in Chinese.
5. Wen J, Hao T, Hu X. Doctors’ workload in China: a status-quo study. Chin J Evid-Based Med. 2015;15:133–136. in Chinese. doi:10.7507/1672-2531.20150024
6. Bavafa H, Hitt LM, Terwiesch C. The impact of e-visits on visit frequencies and patient health: evidence from primary care. Manage Sci. 2018;64(12):5461–5480. doi:10.1287/mnsc.2017.2900
7. Wang L, Yan L, Zhou T, Guo X, Heim GR. Understanding physicians’ online-offline behavior dynamics: an empirical study. Inf Syst Res. 2020;31(2):537–555. doi:10.1287/isre.2019.0901
8. Fan W, Zhou Q, Qiu L, Kumar S. Should doctors open online consultation services? An empirical investigation of their impact on offline appointments. Inf Syst Res. 2023;34(2):629–651. doi:10.1287/isre.2022.1145
9. Tanis M, Hartmann T, Te Poel F. Online health anxiety and consultation satisfaction: a quantitative exploratory study on their relations. Patient Educ Couns. 2016;99(7):1227–1232. doi:10.1016/j.pec.2016.01.021
10. Stewart KJ. Trust transfer on the world wide web. Organ Sci. 2003;14(1):5–17. doi:10.1287/orsc.14.1.5.12810
11. Ma C. Will online medical community participation affect physicians’ offline service volume and their diagnosis and treatment revenue: an empirical study based on the PSM-DID model. Chin J Health Policy. 2021;14:47–53. in Chinese. doi:10.3969/j.issn.1674-2982.2021.09.008
12. Wang JN, Chiu YL, Yu H, Hsu YT. Understanding a nonlinear causal relationship between rewards and physicians’ contributions in online health care communities: longitudinal study. J Med Internet Res. 2017;19(12):e427. doi:10.2196/jmir.9082
13. Bruggen A. An empirical investigation of the relationship between workload and performance. Manag Decis. 2015;53(10):2377–2389. doi:10.1108/MD-02-2015-0063
14. Ball MJ, Lillis J. E-health: transforming the physician/patient relationship. Int J Med Inform. 2001;61(1):1–10. doi:10.1016/S1386-5056(00)00130-1
15. Sabesan S, Kelly J. Doctor patient communication in telehealth. Asia Pac J Clin Oncol. 2014;10:45.
16. Wu H, Deng Z, Wang B, Wang H. How online health community participation affects physicians’ performance in hospitals: empirical evidence from China. Inf Manag. 2021;58(6):103443. doi:10.1016/j.im.2021.103443
17. Narayane MM. Benefits of online doctor consultation during the pandemic. Biosci Biotechnol Res Commun. 2021;14(6):53–56. doi:10.21786/bbrc/14.6.13
18. Iacobucci G. NHS long term plan: all patients to have access to online GP consultations by 2023–24. BMJ. 2019. doi:10.1136/bmj.l87
19. Chen L, Rai A, Guo X Physicians’ online popularity and price premiums for online health consultations: a combined signaling theory and online feedback mechanisms explanation.
20. Li J, Tang J, Jiang L, Yen DC, Liu X. Economic success of physicians in the online consultation market: a signaling theory perspective. Int J Electron Commer. 2019;23(2):244–271. doi:10.1080/10864415.2018.1564552
21. Edwards HB, Marques E, Hollingworth W, et al. Use of a primary care online consultation system, by whom, when and why: evaluation of a pilot observational study in 36 general practices in South West England. BMJ open. 2017;7(11):e016901. doi:10.1136/bmjopen-2017-016901
22. Atherton H, Pappas Y, Heneghan C, Murray E. Experiences of using email for general practice consultations: a qualitative study. Br J Gen Pract. 2013;63(616):e760–e767. doi:10.3399/bjgp13X674440
23. Shaw S, Wherton J, Vijayaraghavan S, et al. Advantages and limitations of virtual online consultations in a NHS acute trust: the VOCAL mixed-methods study. Health Serv Deliv Res. 2018;6(21):1–136. doi:10.3310/hsdr06210
24. Greenhalgh T, Vijayaraghavan S, Wherton J, et al. Virtual online consultations: advantages and limitations (VOCAL) study. BMJ open. 2016;6(1):e009388. doi:10.1136/bmjopen-2015-009388
25. Bavafa H, Terwiesch C. Work after work: the impact of new service delivery models on work hours. J Oper Manag. 2019;65(7):636–658. doi:10.1002/joom.1052
26. Garavand A, Aslani N, Nadri H, Abedini S, Dehghan S. Acceptance of telemedicine technology among physicians: a systematic review. Inform Med Unlocked. 2022;30:100943. doi:10.1016/j.imu.2022.100943
27. Huang N, Yan Z, Yin H. Effects of online–offline service integration on e‐healthcare providers: a quasi‐natural experiment. Prod Oper Manag. 2021;30(8):2359–2378. doi:10.1111/poms.13381
28. Pauly MV, Satterthwaite MA. The pricing of primary care physicians services: a test of the role of consumer information. Bell J Econ Manage Sci. 1981;12(2):488–506. doi:10.2307/3003568
29. Orr D, Sidiki SS, McGhee CN. Factors that influence patient choice of an excimer laser treatment center. J Cataract Refract Surg. 1998;24(3):335–340. doi:10.1016/S0886-3350(98)80321-0
30. Resnick P, Kuwabara K, Zeckhauser R, Friedman E. Reputation systems. Commun ACM. 2000;43(12):45–48. doi:10.1145/355112.355122
31. McGlone TA, Butler ES, McGlone VL. Factors influencing consumers’ selection of a primary care physician. Health Mark Q. 2002;19(3):21–37. doi:10.1300/J026v19n03_03
32. Merle V, Germain JM, Tavolacci MP, et al. Influence of infection control report cards on patients’ choice of hospital: pilot survey. J Hosp Infect. 2009;71(3):263–268. doi:10.1016/j.jhin.2008.11.025
33. Shah J, Dickinson CL. Establishing which factors patients value when selecting urology outpatient care. Br J Med Surg Urol. 2010;3(1):25–29. doi:10.1016/j.bjmsu.2009.10.003
34. Peng Y, Yin P, Deng Z, Wang R. Patient–physician interaction and trust in online health community: the role of perceived usefulness of health information and services. Int J Environ Res Public Health. 2020;17(1):139. doi:10.3390/ijerph17010139
35. Spence M. Job Market Signaling. Q J Econ. 1973;87(3):355–374. doi:10.2307/1882010
36. Chen Y, Cai M, Li Z, Lin X, Wang L. Impacts of the COVID-19 pandemic on public hospitals of different levels: six-month evidence from Shanghai, China. Risk Manag Healthc Policy. 2021;14:3635–3651. doi:10.2147/RMHP.S314604
37. Li Z, Ma Z. Construction and scale development of willingness to utilize primary care services: a study from China. Risk Manag Healthc Policy. 2023;16:2171–2185. doi:10.2147/RMHP.S428369
38. Ayer T, Ayvaci MU, Karaca Z, Vlachy J. The impact of health information exchanges on emergency department length of stay. Prod Oper Manag. 2019;28(3):740–758. doi:10.1111/poms.12953
39. Boulding W, Staelin R. Identifying generalizable effects of strategic actions on firm performance: the case of demand-side returns to R&D spending. Mark Sci. 1995;14(3_supplement):G222–G236. doi:10.1287/mksc.14.3.G222
40. McAlister L, Srinivasan R, Kim M. Advertising, research and development, and systematic risk of the firm. J Mark. 2007;71(1):35–48. doi:10.1509/jmkg.71.1.035
41. Carnahan S, Somaya D. Alumni effects and relational advantage: the impact on outsourcing when a buyer hires employees from a supplier’s competitors. Acad Manage J. 2013;56(6):1578–1600. doi:10.5465/amj.2011.0089
42. Kong D, Yang J, Duan H, Yang S. Helpfulness and economic impact of multidimensional rating systems: perspective of functional and hedonic characteristics. J Consum Behav. 2020;19(1):80–95. doi:10.1002/cb.1796
43. Li Y, Lu LX, Lu SF. Does social media dominate government report cards in influencing nursing home demand? Manuf Serv Oper Manag. 2023;25(6):2085–2105. doi:10.1287/msom.2021.0303
44. Lu Y, Wang Q. Doctors’ preferences in the selection of patients in online medical consultations: an empirical study with doctor–patient consultation data. Healthcare. 2022;10(8):1435. doi:10.3390/healthcare10081435
45. Sun S, Lu SF, Rui H. Does telemedicine reduce emergency room congestion? Evidence from New York State. Inf Syst Res. 2020;31. doi:10.1287/isre.2020.0926
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.