Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Which Frailty Evaluation Method Can Better Improve the Predictive Ability of the SASA for Postoperative Complications of Patients Undergoing Elective Abdominal Surgery?
Authors Yin Y, Jiang L ![]() , Xue L
, Xue L
Received 7 January 2022
Accepted for publication 4 April 2022
Published 5 May 2022 Volume 2022:18 Pages 541—550
DOI https://doi.org/10.2147/TCRM.S357285
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Yanyan Yin,1 Li Jiang,2 Lixin Xue3
1Department of Neurological Rehabilitation, Beijing Rehabilitation Hospital, Capital Medical University, Beijing, 100144, People’s Republic of China; 2Department of Critical Care Medicine, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 3Department of General Surgery, Fuxing Hospital, Capital Medical University, Beijing, 100038, People’s Republic of China
Correspondence: Li Jiang, Department of Critical Care Medicine, Xuanwu Hospital, Capital Medical University, No. 45 Changchun Street, Xicheng District, Beijing, 100053, People’s Republic of China, Tel +8613601366055, Email [email protected]
Purpose: To determine which frailty method can better improve the predictive ability of the Surgical Apgar Score combined with American Society of Anesthesiologists physical status classification (SASA).
Patients and Methods: A prospective cohort study was conducted. A total of 194 elderly patients undergoing elective abdominal surgery were included. Preoperative frailty using FRAIL questionnaire, frailty index (FI), Clinical Frailty Scale (CFS) and SASA scores was assessed. Primary outcome was in-hospital Clavien-Dindo ≥grade II complications. Multiple logistic regression was used to examine the association between frailty and complications. Receiver operating characteristic curves were used to explore the predictive ability of frailty.
Results: According to the FRAIL, FI and CFS criteria, the prevalence of frailty in the study population was 43.8%, 32.5%, and 36.6%, respectively. After adjusting for all covariates, frailty was significantly associated with postoperative complications in hospital by FRAIL [odds ratio: 5.11, 95% CI: 1.41– 18.44, P = 0.013], by FI [OR: 4.25, 95% CI: 1.21– 14.90, P = 0.024] and by CFS [OR: 5.10, 95% CI: 1.52– 17.17, P = 0.008]. The area under the curve (AUC) for SASA was 0.768 (95% CI: 0.702– 0.826). Addition of frailty assessment (FRAIL, FI and CFS) increased the AUC to 0.787 (95% CI: 0.722– 0.842), 0.798 (95% CI: 0.734– 0.852), and 0.815 (95% CI: 0.753– 0.867), respectively. Compared to SASA, only addition of CFS had a significant difference (P = 0.0478).
Conclusion: Frailty is an effective predictor of postoperative complications in elderly Chinese patients undergoing elective abdominal surgery. Frailty assessment of CFS can better improve the predictive ability of SASA.
Keywords: frailty assessment, risk assessment tool, postoperative complication
Background
In 2017, 962 million people were aged 60 years or older worldwide, with nearly one in four of that population living in China.1 This number is projected to 1.4 billion by 2030 and reaching nearly 2.1 billion by 2050. As the population ages, the number of older adults undergoing surgery also increases. Postoperative complications were more common with increasing age.2–4 Postoperative complications in older adults remain a significant cause of increased costs, hospital length of stay (LOS), patient distress, and reported symptoms.5 Therefore, comprehensive preoperative risk assessment is imperative for older patients undergoing abdominal surgery. Effective assessment tools can help reduce length of hospital stay, adverse outcomes, and medical costs.6
Several surgical risk stratification scoring systems have been developed and validated, combining both pre- and intraoperative factors: The Physiological and Operative Severity Score for the enumeration of Mortality and morbidity (POSSUM),7 The Portsmouth POSSUM (P-POSSUM),8 The Estimation of Physiologic Ability and Stress (E-PASS)9 and The Surgical Apgar Score combined with American Society of Anesthesiologists physical status classification (SASA).10,11
Kenig et al found that the SASA was better than E-PASS, and P-POSSUM in predicting postoperative 30-day major morbidity in older patients undergoing abdominal elective cancer surgery.12 Several studies have shown that the inclusion of frailty assessment as part of risk assessment may improve the accuracy of surgical risk prediction in the elderly.13,14 Therefore, in our study, we chose SASA as the traditional method and introduced frailty score to improve the predictive ability of SASA. Although frailty as a medical syndrome and its application as a measure of decreased physiologic reserve are well recognized15,16 and numerous approaches to screen for grading frailty have been proposed, there is no consensus on which to use.17–19 In Suggestions from Chinese Experts on Preoperative Evaluation of Elderly Patients in 2015, the “FRAIL” scale was recommended, which is very concise but it is not widely used in China. Another commonly used frailty evaluation method is the FI model developed by Rockwood et al,20 which is conceptualized as a multidimensional risk state quantifiable by the number of deficit accumulation. Nevertheless, many ICU experts prefer the Clinical Frailty Scale (CFS).21,22 However, to the best of our knowledge, very few researches have been conducted on frailty in Asian settings, the differences of predictive ability within different combinations of frailty and traditional risk tools have not been investigated.
Aims
The purpose of this study was to explore the association between different frailty methods and postoperative complications after abdominal surgery and compare which frailty evaluation method can better improve the prediction ability of SASA for postoperative complications of patients undergoing elective abdominal surgery.
Methods
Study Cohort
The present investigation was conducted as a prospective observational study. The study was approved by the Ethics Committee of Fuxing Hospital (affiliated with Capital Medical University) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants included in the study. All patients were older than 65 years and admitted to the General Surgery Department, Urological Surgery Department, or Gynecology Department of Fuxing Hospital affiliated with Capital Medical University between March 2017 and August 2019 for elective surgery. Patients suffering from hypothyroidism, Parkinson’s disease, or previous stroke and those with similar debilitating symptoms due to treatment with carbidopa/levodopa, donepezil, or antidepressants were excluded. Patients with severe cognitive impairment or mental illness and those who refused to participate, were bedridden for a long time, were completely incapable of participation, or were unable to undergo frailty assessment were also excluded.
Frailty Measures
- We selected three different methods to evaluate frailty. One is the FRAIL scale,23 a simple questionnaire containing 5 factors, which the presence of 3 or more factors is considered frail, the presence of 1–2 factors is considered pre-frail, and no factors present is considered robust. The second is the FI, which is derived from comprehensive geriatric assessment parameters. 24 According to the scale, the deficits were given some points; the total number in the denominator was 54. All the variables satisfied the 5 criteria in Searle SD’s study25 in our patient group. FI scores of the patients were generated after calculating the results by dividing total deficits points to total points of the evaluated deficits, where a score of ≤0.25 is considered robust, a score of 0.25–0.4 is considered pre-frail, and a score of >0.4 is considered frail. The third method is the CFS, 21 which has 9 levels separated into 3 three categories: 1–3 is considered robust, 4 is considered pre-frail, and 5–9 is considered frail. Forty-eight hours prior to surgery, FRAIL, FI, and CFS were assessed by two experienced doctors.
Risk Assessment Tools
SASA is a combination of the Surgical Apgar Score (SAS) with the American Society of Anesthesiologists performance score (ASA) classification using the following equation: SASA = SAS + (6 − ASA) × 2. SAS was calculated at the end of surgery from intraoperative data, such as estimated blood loss, lowest intraoperative heart rate, and lowest intraoperative mean arterial pressure, extracted from handwritten anesthesia records. As shown in Gawande, 11 the score is the sum of the points from each category. ASA Classification System described in Keats, 26 which were extracted from the anesthesiologist’s preoperative visit sheet.
Covariates
Data pertaining to the following potential confounding factors were obtained to determine whether frailty was an independent risk factor for postoperative complications: (1) demographics including age, gender, body mass index (BMI), education level; (2) preoperative physiological variables, such as Activities of Daily Living (ADL), and Charlson Comorbidity Index (CCI), presence of malignancy, ASA; (3) surgical variables, including type of surgery, duration of surgery, and total blood loss.
Outcomes
The outcome measure was in-hospital ≥ grade II postoperative complications, according to the Clavien-Dindo classification standard.27 This scoring system classifies complications into 5 classes based on the level of intervention required for treatment of complications. Patients with multiple-grade complications were classified according to the highest-grade complication. Explicitly, postoperative routine return to ICU was not counted as complication level 4, and staying in ICU for more than one day because of single or multiple-organ dysfunction was recorded as complication level 4. The complications were determined and recorded by a clinician who was not aware of the frailty status of the patients.
Statistical Analysis
Statistical analysis was carried out using SPSS version 26.0. The Kolmogorov-Smirnov test was used to determine the normality of the quantitative data distribution. Quantitative data were compared using a nonpaired t-test or Mann–Whitney U-test as appropriate, and χ2 test or Fisher’s exact test was used to assess differences in categorical data. Logistic regression analysis was performed to assess the association of FRAIL, FI, and CFS with postoperative complications after the operation. The Hosmer-Lemeshow goodness-of-fit chi-square test and R2 were used to assess the model fit. The discriminative ability of the criteria to correctly predict adverse outcomes was assessed by calculating the area under the curve (AUC) of the receiver operating characteristic (ROC) curve. A comparison of the ROC curves was performed using the method described by DeLong et al.28 A P value of less than 0.05 was considered significant. It should be noted that in the logistic regression, FRAIL, FI, and CFS were used as the categorical variables, while FRAIL, FI, and CFS were used as the continuous variables in the ROC.
Results
Baseline Characteristics
We assessed 223 Chinese older patients undergoing major abdominal surgery. Of these, 194 patients qualified the inclusion criteria and were enrolled in the study. The mean age of patients was 77.0 ± 7.7 years; males accounted for 46.4% of patients. According to FRAIL, FI, and CFS criteria, the prevalence of frailty in the study population was 43.8%, 32.5%, and 36.6%, respectively (Table 1).
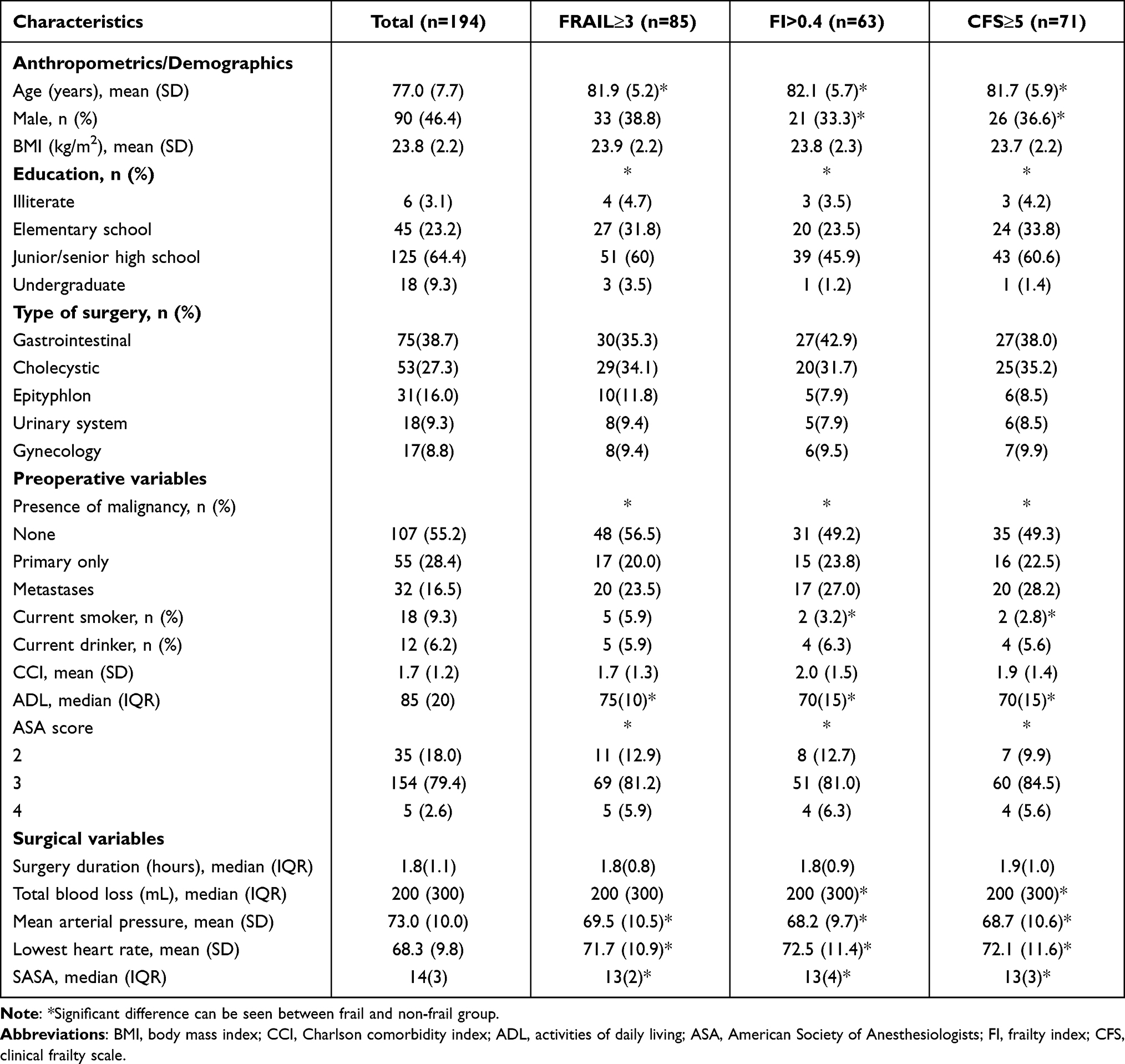 |
Table 1 Characteristics of the Patients at Baseline |
Frailty and In-Hospital Postoperative Complications
Among the 194 patients who were included in the final analysis, 29.90% (58/194) had postoperative complications. The number of patients with grade II, III, IV, and grade V complications was 13, 0, 26, and 19, respectively. According to the criteria of FRAIL, FI, and CFS, the incidence of complications in the non-frail and frail groups were 17.43% (19/109) and 45.89% (39/85), 17.56% (23/131) and 55.56% (35/63), and 16.26% (20/123) and 53.52% (38/71), respectively. The between-group differences in this respect were all statistically significant (P < 0.001) (Table 2).
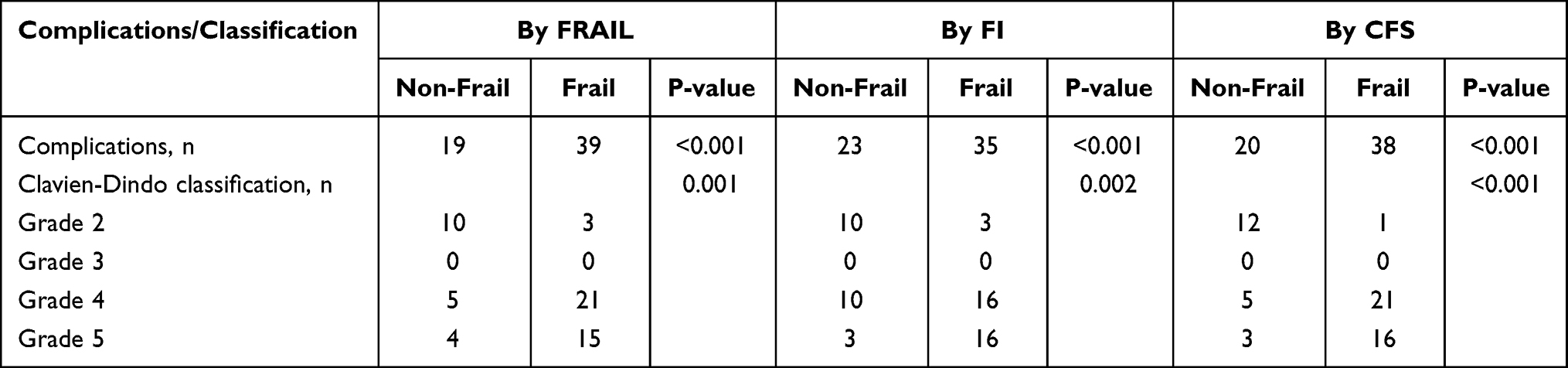 |
Table 2 Association Between Frailty Category and In-Hospital Postoperative Complications |
Univariate logistic analysis showed that the frailty was associated with postoperative complications regardless of which criteria were used: FRAIL (OR = 4.02, 95% CI: 2.09–7.72); FI (OR = 5.87, 95% CI: 3.00–11.48); or CFS (OR = 5.93, 95% CI: 3.04–11.57) (Table 3). Multiple logistic regression analysis was performed to adjust for potential confounding variables. Model I was adjusted for age and gender; Model II was adjusted for presence of malignancy, BMI, CCI, ADL, ASA, type of surgery, surgery duration and total blood loss, which was recognized as a significant predictor of prognosis in univariate analysis; Model III was adjusted for all covariates. On multiple regression analysis, frailty of each method was found to be a significant predictor of postoperative complications (Table 4).
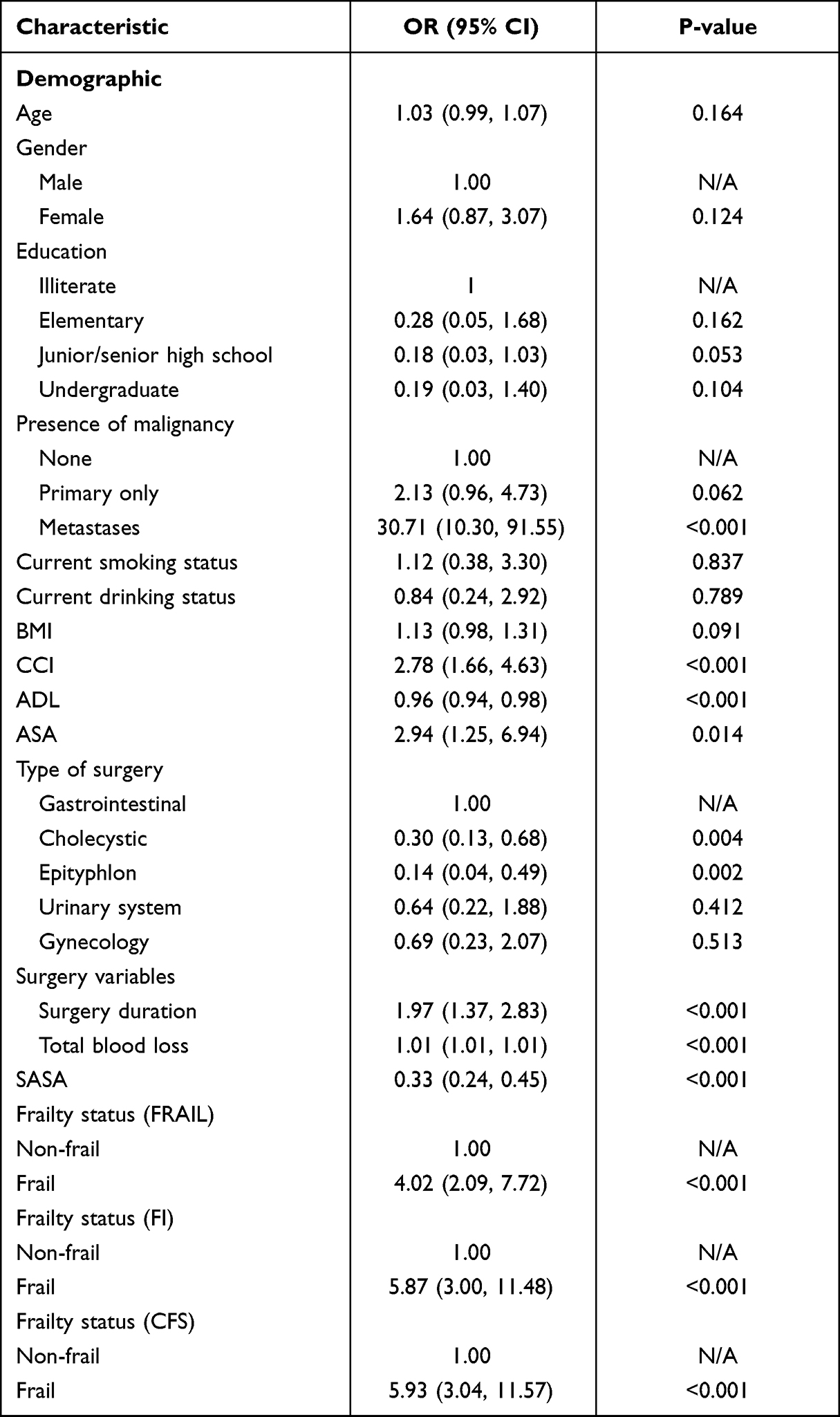 |
Table 3 Univariate Logistic Regression of Postoperative Complications in Hospital |
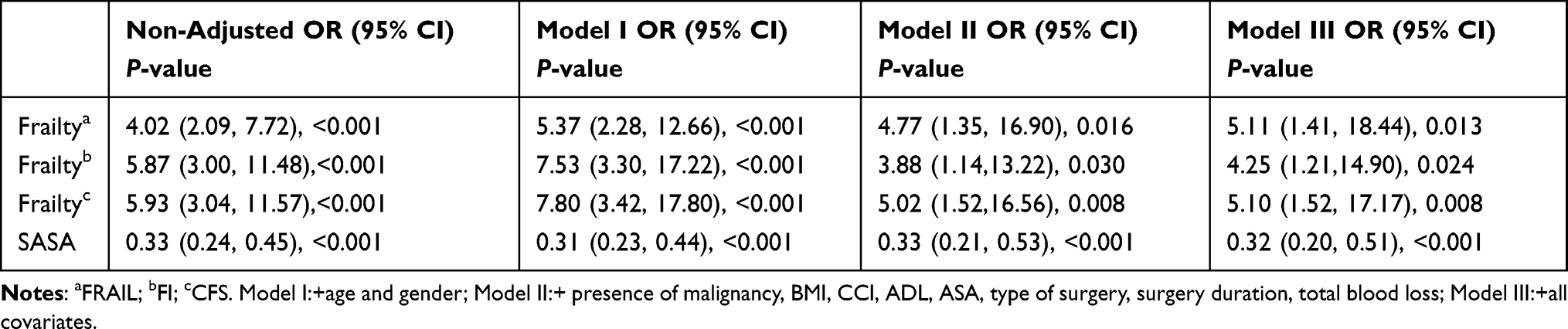 |
Table 4 Multiple Logistic Regression Analysis of In-Hospital Postoperative Complications |
Comparison of Predictive Ability of Different Frailty Method with SASA
The AUC for SASA was 0.768 (95% CI: 0.702–0.826). FRAIL, FI, and CFS scores effectively predicted the occurrence of postoperative complications [AUC: 0.684 (95% CI: 0.614–0.749), 0.728 (95% CI: 0.660–0.789), and 0.753 (95% CI: 0.686–0.812), respectively]. The predictive ability of SASA was similar to that of other frailty methods, SASA versus FRAIL and FI and CFS, for which the P values were 0.1034, 0.4586, and 0.7411, respectively (Figure 1). Irrespective of which definition was used, addition of the frailty assessment could improve the predictive ability of SASA for postoperative complications, where AUC increased to 0.787 (95% CI: 0.722–0.842), 0.798 (95% CI: 0.734–0.852), and 0.815 (95% CI: 0.753–0.867) as determined by FRAIL, FI, and CFS criteria, respectively (Figure 2). However, only addition of CFS could improve the AUC for predicting postoperative complications significantly (P = 0.0478). Simultaneously, the model fitting result after addition of CFS assessment to the SASA was better than other combinations (Table 5).
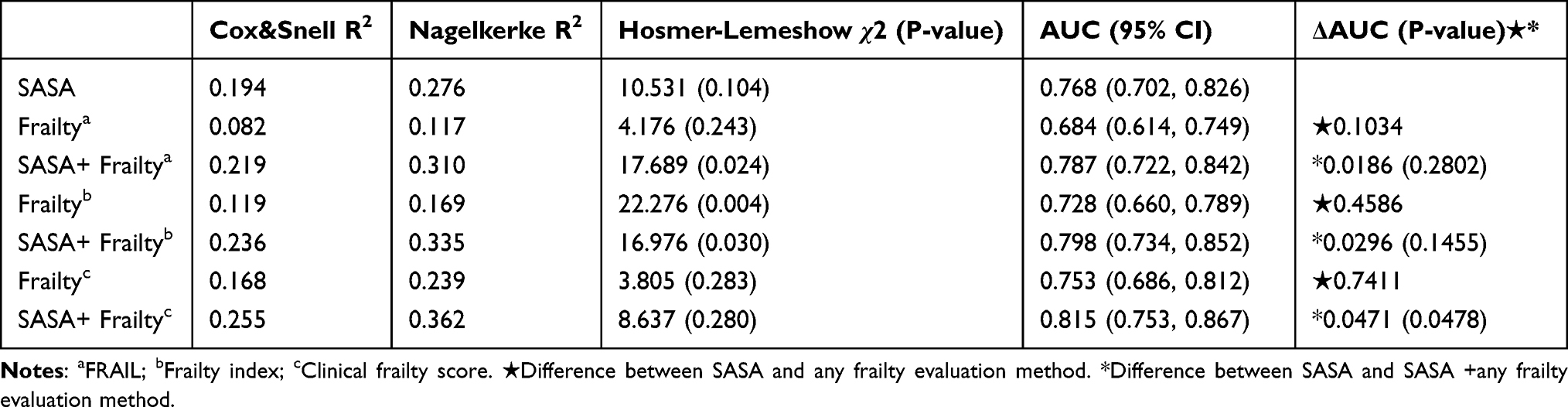 |
Table 5 Performance of Risk Assessment Tool and Frailty Assessment Methods in Predicting Postoperative Complications |
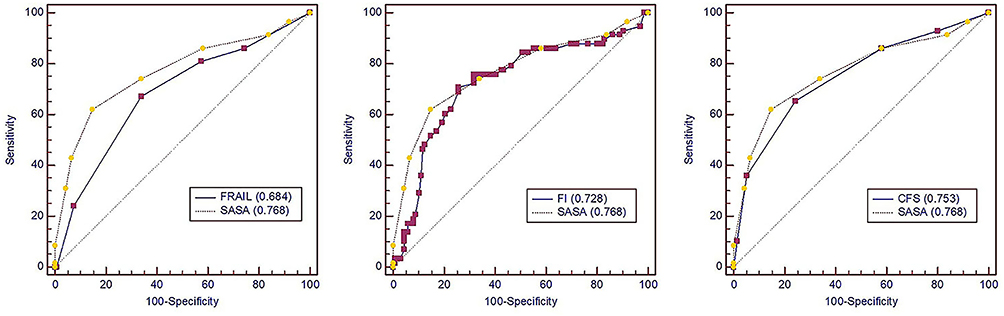 |
Figure 1 Receiver operating characteristic (ROC) curves showing the predictive ability of three different frailty method and SASA. |
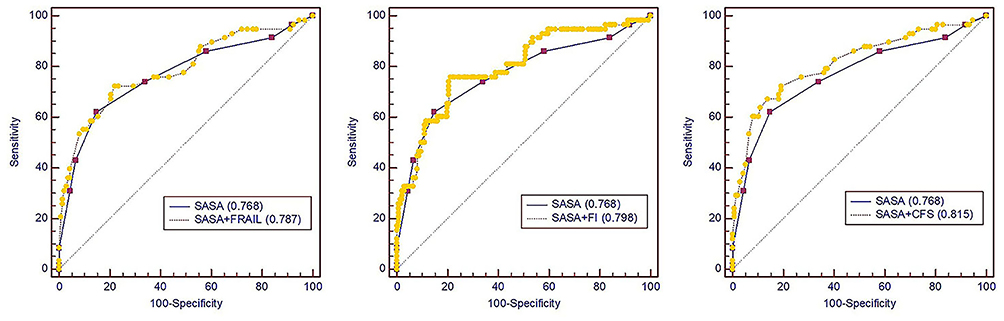 |
Figure 2 Receiver operating characteristic (ROC) curves showing the predictive ability of three different frailty method+SASA and SASA. |
Discussions
Within the literature, numerous studies have compared frailty and adverse outcomes in older surgical patients.29,30 Meanwhile, several surgical risk stratification scoring systems have been developed and validated, combining both pre- and intraoperative factors. However, limited researches have investigated frailty in Asian settings. In addition, no study has compared the ability of predictivity for postoperative complications between SASA and frailty or compared different frailty evaluation method to improve the predictivity of SASA.
In this study, we explored the association between frailty and postoperative complications after elective abdominal surgery in older Chinese patients. To do so, we assessed the effect of the addition of different frailty assessments on the predictive ability of the SASA score. We found that frailty was a significant predictor of postoperative complications no matter which method was used, while the CFS assessment could better improve the ability of SASA for predicting postoperative complications and showed a better model fitting result. Comparatively, CFS is a more simple and effective method to help surgeons improve the ability of traditional scoring methods to predict prognosis.
Different methods to assess frailty, leading to prevalence rates ranging from 25% to 46%,31 have been reported, which are comparable to our study. In our research, the incidence rates of frailty assessed using FRAIL, FI, and CFS criteria were 43.8%, 32.5%, and 36.6%, respectively. These rates are at a higher level than those reported before. Specifically, the median age of the patients in our study was 79-years-old, which is older than those study,32 and in our study, the patients planning surgery were often accompanied by poor appetite and mood, who were more likely to be frail.
In this study, frailty was an independent predictor of postoperative complications in elderly Chinese patients undergoing elective abdominal surgery and remained an independent risk factor for postoperative complications even after adjusting for factors normally considered to influence prognosis, such as age, co-morbidity, ASA, ADL, and surgical site, no matter which method was used. This result may help explain the differences in postoperative recovery of elderly patients undergoing the same surgery at the same age. This result may also suggest that it is more important for surgeons to be aware of whether patients should be evaluated for frailty, rather than to agonize over which frailty evaluation method to use.
Traditional scoring methods have been widely utilized for predicting postoperative complications in older patients.12,33–35 However, it is known that the prognosis of patients depends on their usual general state, preoperative organ function assessment, and degree of surgical trauma interference. Therefore, in order to improve the predictive power of the traditional scoring method, we introduced the assessment of frailty of patients’ preoperative general state. We found that, irrespective of which definition was used, addition of the frailty assessment could improve the predictive ability of SASA for postoperative complications. Makary et al found that frailty assessment according to Fried criteria increased the area for three risk indices in predicting complications (American Society of Anesthesiologists (ASA) score, Lee’s revised cardiac risk index, and Eagle score).36 Kenig et al showed that the combination of the G8 frailty screening test and the SAS improved the discriminatory ability to identify patients at risk for complication in a population of older adult in emergency surgical setting.37 The results of these studies were similar but not identical to ours, our study found that CFS can better improve the prediction ability of SASA for postoperative complications of patients undergoing elective abdominal surgery. However, the ability of frailty assessment to improve the prognosis prediction of traditional scoring methods is not as high as that of other previous studies.14 The reason is that some indicators of SASA we adopted already have implications for cardiopulmonary storage function. At the same time, our patient population was older, and more patients were undergoing palliative surgery; thus, very little interventions could lead to adverse outcomes for patients. Yet, the addition of CFS could improve the AUC for predicting postoperative complications significantly (P = 0.0478), whereby the model fitting result after addition of CFS assessment to SASA was better than other combinations. It is reasonable to suggest that CFS can effectively improve the predictive ability of the traditional scoring method since it includes both activity ability and mental state, which can describe the overall state of the patient. In comparison, FRAIL does not consider mental state, while FI includes activity ability, mental state, comorbidities, and drugs. Although FI can accurately identify frail patients, it leads to poorer feasibility, as the patient’s impatience resulted in inaccurate evaluation. So in our study, we found that frailty assessment of CFS effectively improved the predictive ability of the traditional scoring method, it may improve clinical decision-making and the treatment plans optimization.
There are several limitations in our study. Firstly, this study mainly explored the association between frailty and short-term adverse postoperative outcomes, long-term outcomes were not assessed; Secondly, the sample size was not large enough; Thirdly, the study involved a single center, since the patients in our hospital were older and sicker, the general population of elderly patients was not appropriately represented. Multicenter research should be conducted to study the causal mechanisms and improvement strategy of frailty in the future.
Conclusions
In our study, frailty was a significant predictor of postoperative complications in elderly Chinese patients undergoing elective abdominal surgery. Incorporation of frailty assessment, CFS can improve the ability of SASA to predict postoperative complications.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was approved by the ethics committee of Fuxing Hospital (affiliated to the Capital Medical University) and conducted in accordance with the Declaration of Helsinki. The Approval Notice Number:2017FXHEC—KY021.
Consent for Publication
All patients/parents or guardians gave their written informed consent for participation in the study.
Acknowledgments
We thank all the staff of General surgery department, Intensive Care Medicine department, Anesthesiology department, Urinary surgery department, Gynecology department of Fuxing Hospital, Capital Medical University, for their cooperation and the anonymous reviewers. We would like to thank Dr Xiuming Xi for his suggestions on research design, Dr Huihui Sun and Bo Zhu for their help in data acquisition, and Meiping Wang for her help in data analysis.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was supported by The National Science and Technology Support Program (2012BAI11B05).
Disclosure
The authors report no conflicts of interest in this work.
References
1. United Nations. World Population Aging. New York: United Nations; 2017.
2. Kim S, Brooks A, Groban L. Preoperative assessment of the older surgical patient: honing in on geriatric syndromes. Clin Interv Aging. 2015;10:13–27. doi:10.2147/CIA.S75285
3. Hamel MB, Henderson WG, Khuri SF, Daley J. Surgical outcomes for patients aged 80 and older: morbidity and mortality from major noncardiac surgery. J Am Geriatr Soc. 2005;53(3):424–429. doi:10.1111/j.1532-5415.2005.53159.x
4. Pofahl WE, Pories WJ. Current status and future directions of geriatric general surgery. J Am Geriatr Soc. 2003;51(7 Suppl):S351–S354. doi:10.1046/j.1365-2389.2003.51347.x
5. Partridge JS, Harari D, Dhesi JK. Frailty in the older surgical patient: a review. Age Ageing. 2012;41(2):142–147. doi:10.1093/ageing/afr182
6. Kappen TH, Peelen LM. Prediction models: the right tool for the right problem. Curr Opin Anaesthesiol. 2016;29(6):717–726. doi:10.1097/ACO.0000000000000386
7. Copeland GP, Jones D, Walters M. POSSUM: a scoring system for surgical audit. Br J Surg. 1991;78:355–360. doi:10.1002/bjs.1800780327
8. Whiteley MS, Prytherch DR, Higgins B, Weaver PC, Prout WG. An evaluation of the POSSUM surgical scoring system. Br J Surg. 1996;83(6):812–815. doi:10.1002/bjs.1800830628
9. Haga Y, Ikei S, Ogawa M. Estimation of Physiologic Ability and Surgical Stress (E-PASS) as a new prediction scoring system for postoperative morbidity and mortality following elective gastrointestinal surgery. Surg Today. 1999;29(3):219–225. doi:10.1007/BF02483010
10. Kinoshita M, Morioka N, Yabuuchi M, Ozaki M. New surgical scoring system to predict postoperative mortality. J Anesth. 2017;31(2):198–205. doi:10.1007/s00540-016-2290-2
11. Gawande AA, Kwaan MR, Regenbogen SE, Lipsitz SA, Zinner MJ. An Apgar score for surgery. J Am Coll Surg. 2007;204(2):201–208. doi:10.1016/j.jamcollsurg.2006.11.011
12. Kenig J, Mitus JW, Rapacz K, Skorus U, Pietrzyk P, Sega A. Usefulness of scoring systems in outcome prediction for older cancer patients undergoing abdominal surgery. Acta Chir Belg. 2019;1–7. doi:10.1080/00015458.2019.1642577
13. Gleason LJ, Benton EA, Alvarez-Nebreda ML, Weaver MJ, Harris MB, Javedan H. FRAIL questionnaire screening tool and short-term outcomes in geriatric fracture patients. J Am Med Dir Assoc. 2017;18(12):1082–1086. doi:10.1016/j.jamda.2017.07.005
14. Han BR, Li QP, Chen X. Frailty and postoperative complications in older Chinese adults undergoing major thoracic and abdominal surgery. Clin Interv Aging. 2019;14:947–957. doi:10.2147/CIA.S201062
15. Feng MA, McMillan DT, Crowell K, Muss H, Nielsen ME, Smith AB. Geriatric assessment in surgical oncology: a systematic review. J Surg Res. 2015;193(1):265–272. doi:10.1016/j.jss.2014.07.004
16. Robinson TN, Walston JD, Brummel NE, et al. Frailty for surgeons: review of a national institute on aging conference on frailty for specialists. J Am Coll Surg. 2015;221(6):1083–1092. doi:10.1016/j.jamcollsurg.2015.08.428
17. Hogan DB, MacKnight C, Bergman H. Models, definitions, and criteria of frailty. Aging Clin Exp Res. 2003;15(3 Suppl):3–29.
18. Sternberg SA, Wershof SA, Karunananthan S, Bergman H, Mark Clarfield A. The identification of frailty: a systematic literature review. J Am Geriatr Soc. 2011;59(11):2129–2138. doi:10.1111/j.1532-5415.2011.03597.x
19. Bouillon K, Kivimaki M, Hamer M, et al. Measures of frailty in population-based studies: an overview. BMC Geriatr. 2013;13:64. doi:10.1186/1471-2318-13-64
20. Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173(5):489–495. doi:10.1503/cmaj.050051
21. Juma S, Taabazuing MM, Montero-Odasso M. Clinical frailty scale in an acute medicine unit: a simple tool that predicts length of stay. Can Geriatr J. 2016;19(2):34–39. doi:10.5770/cgj.19.196
22. Muessing JM, Nia AM, Masyuk M, et al. Clinical Frailty Scale (CFS) reliably stratifies octogenarians in German ICUs: a multicenter prospective cohort study. BMC Geriatr. 2018;18(1):162. doi:10.1186/s12877-018-0847-7
23. Morley JE, Malmstrom TK, Miller DK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J Nutr Health Aging. 2012;16(7):601–608. doi:10.1007/s12603-012-0084-2
24. Krishnan M, Beck S, Havelock W, Eeles E, Hubbard RE, Johansen A. Predicting outcome after hip fracture: using a frailty index to integrate comprehensive geriatric assessment results. Age Ageing. 2014;43(1):122–126. doi:10.1093/ageing/aft084
25. Searle SD, Mitnitski A, Gahbauer EA, Gill TM, Rockwood K. A standard procedure for creating a frailty index. BMC Geriatr. 2008;8(1):24. doi:10.1186/1471-2318-8-24
26. Keats AS. The ASA classification of physical status–a recapitulation. Anesthesiology. 1978;49(4):233–236. doi:10.1097/00000542-197810000-00001
27. Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–196. doi:10.1097/SLA.0b013e3181b13ca2
28. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44(3):837–845. doi:10.2307/2531595
29. Keenan LG, O’Brien M, Ryan T, Dunne M, McArdle O. Assessment of older patients with cancer: Edmonton Frail Scale (EFS) as a predictor of adverse outcomes in older patients undergoing radiotherapy. J Geriatr Oncol. 2017;8(3):206–210. doi:10.1016/j.jgo.2016.12.006
30. Lin HS, Watts JN, Peel NM, Hubbard RE. Frailty and post-operative outcomes in older surgical patients: a systematic review. BMC Geriatr. 2016;16(1):157. doi:10.1186/s12877-016-0329-8
31. Handforth C, Clegg A, Young C, et al. The prevalence and outcomes of frailty in older cancer patients: a systematic review. Ann Oncol. 2015;26(6):1091–1101. doi:10.1093/annonc/mdu540
32. Li JL, Henderson MA, Revenig LM, et al. Frailty and one-year mortality in major intra-abdominal operations. J Surg Res. 2016;203(2):507–512.e1. doi:10.1016/j.jss.2016.03.007
33. Jering MZ, Marolen KN, Shotwell MS, Denton JN, Sandberg WS, Ehrenfeld JM. Combining the ASA physical classification system and continuous intraoperative surgical apgar score measurement in predicting postoperative risk. J Med Syst. 2015;39(11):147. doi:10.1007/s10916-015-0332-1
34. Gonzalez-Martinez S, Martin-Baranera M, Marti-Sauri I, BorrellGrau N, Pueyo-Zurdo JM. Comparison of the risk prediction systems POSSUM and P-POSSUM with the surgical risk scale: a prospective cohort study of 721 patients. Int J Surg. 2016;29:19–24. doi:10.1016/j.ijsu.2016.03.005
35. Tominaga T, Takeshita H, Takagi K, et al. E-PASS score as a useful predictor of postoperative complications and mortality after colorectal surgery in elderly patients. Int J Colorectal Dis. 2016;31(2):217–225. doi:10.1007/s00384-015-2456-7
36. Makary MA, Segey DL, Pronovost PJ, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg. 2010;210(6):901–908. doi:10.1016/j.jamcollsurg.2010.01.028
37. Kenig J, Mastalerz K, Lukasiewicz K, Mitus-Kenig M, Skorus U. The Surgical Apgar Score predicts outcomes of emergency abdominal surgeries both in fit and frail older patients. Arch Gerontol Geriatr. 2018;76:54–59. doi:10.1016/j.archger.2018.02.001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.