Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 12
When is dual bronchodilation indicated in COPD?
Authors Thomas M, Halpin DMG ![]() , Miravitlles M
, Miravitlles M ![]()
Received 1 April 2017
Accepted for publication 30 May 2017
Published 3 August 2017 Volume 2017:12 Pages 2291—2305
DOI https://doi.org/10.2147/COPD.S138554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Mike Thomas,1 David MG Halpin,2 Marc Miravitlles3
1Primary Care and Population Sciences, University of Southampton, Southampton, 2Department of Respiratory Medicine, Royal Devon and Exeter Hospital, Exeter, UK; 3Pneumology Department, Hospital Universitari Vall d’Hebron, Centro de Investigación Biomédica en Red de Enfermedades Respiratorias (CIBERES), Barcelona, Spain
Abstract: Inhaled bronchodilator medications are central to the management of COPD and are frequently given on a regular basis to prevent or reduce symptoms. While short-acting bronchodilators are a treatment option for people with relatively few COPD symptoms and at low risk of exacerbations, for the majority of patients with significant breathlessness at the time of diagnosis, long-acting bronchodilators may be required. Dual bronchodilation with a long-acting β2-agonist and long-acting muscarinic antagonist may be more effective treatment for some of these patients, with the aim of improving symptoms. This combination may also reduce the rate of exacerbations compared with a bronchodilator-inhaled corticosteroid combination in those with a history of exacerbations. However, there is currently a lack of guidance on clinical indicators suggesting which patients should step up from mono- to dual bronchodilation. In this article, we discuss a number of clinical indicators that could prompt a patient and physician to consider treatment escalation, while being mindful of the need to avoid unnecessary polypharmacy. These indicators include insufficient symptomatic response, a sustained increased requirement for rescue medication, suboptimal 24-hour symptom control, deteriorating symptoms, the occurrence of exacerbations, COPD-related hospitalization, and reductions in lung function. Future research is required to provide a better understanding of the optimal timing and benefits of treatment escalation and to identify the appropriate tools to inform this decision.
Keywords: COPD, dual bronchodilation, monobronchodilation, ICS, triple therapy
Introduction
Bronchodilators are a cornerstone of COPD treatment, commonly provided on a regular basis to reduce or prevent symptoms.1 While short-acting bronchodilators are an option for patients with occasional dyspnea at low risk of exacerbations, their use as regular treatment is not recommended.1 The majority of patients have breathlessness leading to exercise limitation at the time of diagnosis, and may require more intensive treatment than short-acting bronchodilators alone. For these patients, whether or not they are also at higher risk of exacerbations, long-acting bronchodilators (as monotherapy or in combination) are recommended as a preferred treatment choice in current guidelines and treatment-strategy reports.1,2 In some patients, particularly those at risk of exacerbation or with severe symptoms, dual bronchodilation can also be considered as initial therapy.1
Long-acting bronchodilator monotherapy has benefits across a range of parameters (airflow limitation,3–8 dyspnea,3,4,8 physical activity/exercise capacity,9–12 health status,3,4,6–8 and preventing exacerbations);4,8,13,14 however, many patients remain symptomatic despite treatment.15 When symptoms are uncontrolled or exacerbations occur, treatment should be adjusted with the aim of providing better symptom relief and reducing exacerbation risk. Identifying the need for treatment modification can be challenging, as patients with COPD often reduce physical activity levels in order to reduce symptom intensity, which complicates eliciting symptom burden.16
Dual bronchodilation improves lung function compared with a single bronchodilator; however, when comparing active treatments for other outcomes (eg, Transition Dyspnea Index, St George’s Respiratory Questionnaire) in clinical trials, the magnitude of effect is often not marked. For such outcomes, responder analyses (the proportion of patients achieving a specified treatment benefit) can indicate the likelihood of clinically important changes for an individual.17–26 Currently, there are no clear recommendations on which clinical indicators would prompt a patient and physician to consider stepping up treatment from mono- to dual bronchodilation or whether some patients should be started on dual therapy earlier in an attempt to maintain exercise capacity. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) has issued some general criteria of escalating or de-escalating treatment, based on persistent symptoms and further exacerbations.1 In this paper, we discuss what might trigger physicians to consider stepping up from mono- to dual therapy with long-acting bronchodilators and what further data are required to help physicians decide if step-up therapy is appropriate for their patient.
Relevant medical literature on long-acting bronchodilator monotherapy, dual bronchodilation, and/or inhaled corticosteroids (ICSs) plus long-acting β2-agonists (LABAs) was identified by searching the PubMed (Medline) database for articles published in English since 2005. Search terms were “chronic obstructive pulmonary disease” OR “COPD” AND “long-acting β2-agonist”, “long-acting muscarinic antagonist” OR “anti-cholinergic”, “LABA/LAMA” OR “dual bronchodilation”, “tiotropium”, “salmeterol”, “salmeterol/fluticasone propionate”, “IND/GLY”, “indacaterol”, “glycopyrronium”, “olodaterol”, “umeclidinium”, “vilanterol”, “UMEC/VI”, “formoterol”, “aclidinium”, and “arformoterol”. Results were filtered manually to identify studies of long-acting bronchodilation monotherapy reporting effects on lung function and/or patient reported outcomes in comparison with placebo and dual bronchodilation or ICS/LABA combinations in patients with COPD (Table 1). The authors have additionally selected papers that are relevant to clinical practice at the time of publication, and provide their opinions on the evolving therapy area of COPD management.
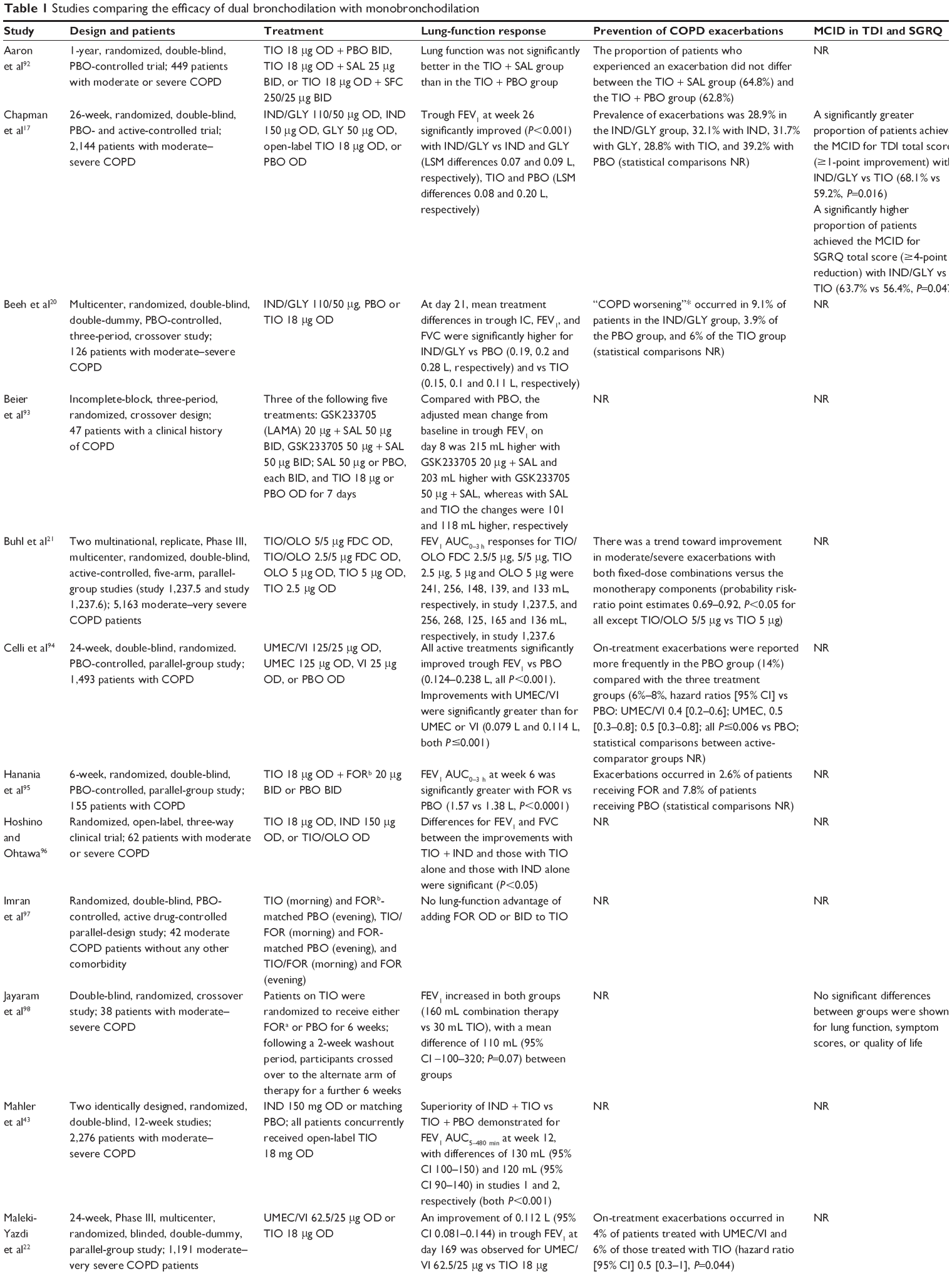 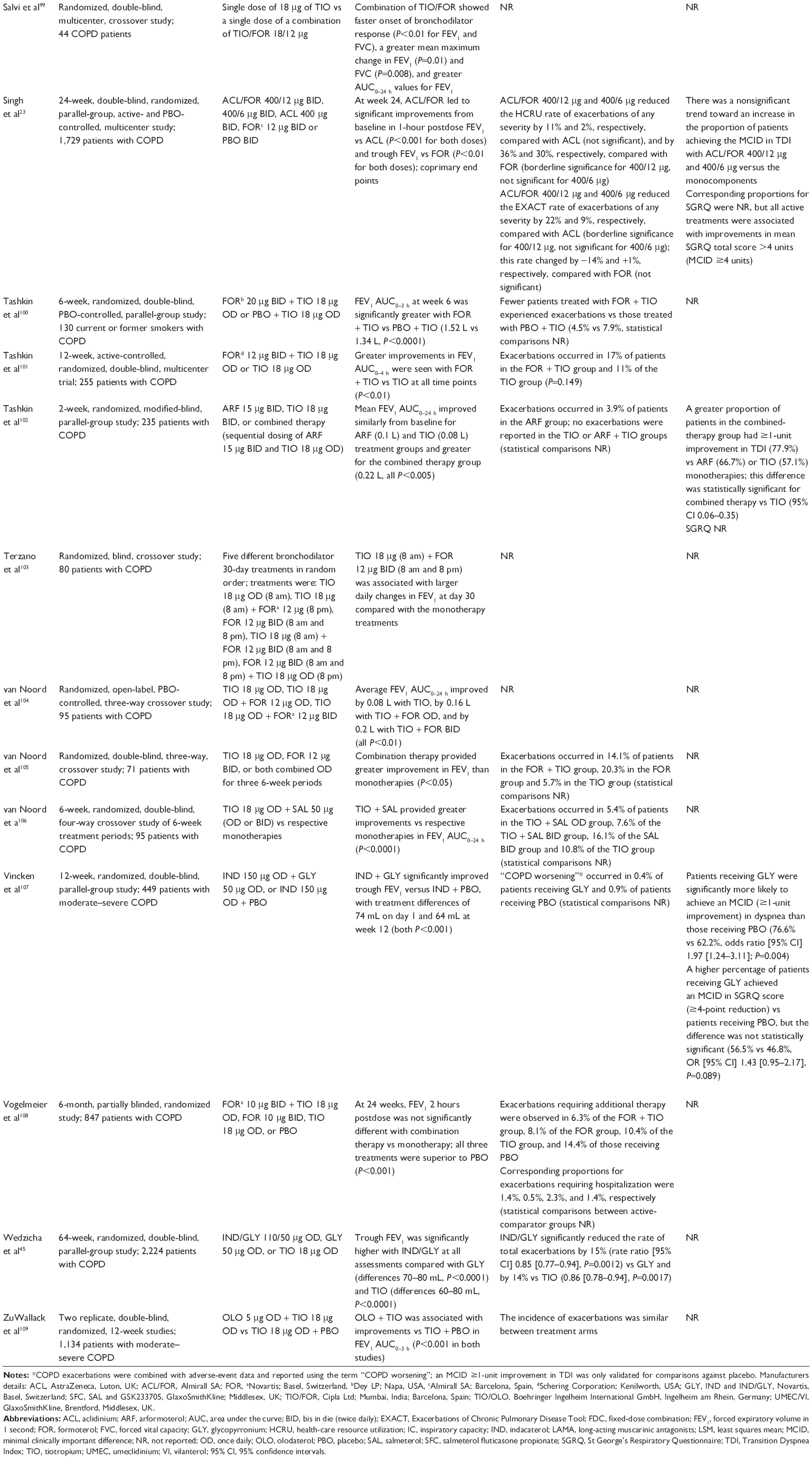 | Table 1 Studies comparing the efficacy of dual bronchodilation with monobronchodilation |
What is the rationale for switching from mono- to dual bronchodilation?
LABAs and long-acting muscarinic antagonists (LAMAs) act via different mechanisms; when used together in patients with COPD, they exert additional bronchodilating effects.27,28 Muscarinic receptors are expressed in the human lung, and are also localized in the smooth muscle of all airways, with a higher density of receptors in the larger airways. β2-adrenoceptors are abundantly expressed on human airway smooth muscle. The density of the receptors is the same throughout the different airway levels, which is particularly important in COPD, as the small airways are affected. Bronchodilation can thus be achieved through stimulation of the β2-adrenoceptors with BAs or by inhibiting the action of acetylcholine at muscarinic receptors with MAs, indirectly leading to smooth-muscle relaxation.29 Multiple studies have assessed whether LABA/LAMA dual bronchodilation results in additional improvements in lung function, exacerbation rates, achievement of minimal clinically important differences in Transition Dyspnea Index and St George’s Respiratory Questionnaire scores (Table 1), and other outcome measures when compared with monobronchodilation. In patients with moderate COPD who remained symptomatic despite LAMA monotherapy, the step-up to dual bronchodilation significantly improved lung function compared with continuation of previous treatment.30 Another study by Donohue et al measured the efficacy of dual bronchodilation (umeclidinium/vilanterol 62.5/25 μg; GlaxoSmithKline, Brentford, Middlesex, UK) in patients identified as responsive or unresponsive to monobronchodilation (umeclidinium 62.5 μg, vilanterol 25 μg).31 Umeclidinium/vilanterol significantly increased lung function versus umeclidinium in umeclidinium responders and versus vilanterol in vilanterol responders. Notably in umeclidinium and vilanterol nonresponders, lung function was still significantly increased, but by a smaller amount.31 The study did not assess the impact of mono- versus dual bronchodilation on exacerbations.32,33 The CRYSTAL study examined directly switching from various treatments to glycopyrronium (GLY; Novartis, Basel, Switzerland) (50 μg) or indacaterol (IND)/GLY (110/50 μg; Novartis) in terms of lung function and symptoms in symptomatic patients with moderate COPD. IND/GLY significantly improved lung function and dyspnea after direct switch from LAMA, LABA, or ICS/LABA.34
Activity limitation is an important feature of COPD, with dyspnea, deteriorating physical conditioning, and avoidance of activity contributing to a vicious circle of decline.16 Physical inactivity is associated with adverse clinical outcomes, including hospitalizations and mortality. Increasing activity is thus crucial for effective management strategies that could improve long-term outcomes in COPD.35 Improving physical activity and exercise capacity are closely related clinical outcomes in COPD; however, it is important to make a distinction between the two. Physical activity reflects what someone actually does that results in energy expenditure, whereas exercise capacity indicates what a person is physically capable of doing.36 Clinical trials are yet to find a clear association between physical activity and exercise capacity. This may be because physical activity is hard to assess, as it is measured by direct observation, such as questionnaires or patient diaries, which can be subjective and a time-consuming method to assess in large populations.35 This may explain why studies focus more on exercise capacity in clinical trials and a clear association is yet to be found.
Monobronchodilators have been shown to improve exercise tolerance in COPD patients,9,12 and while some early exercise studies of dual bronchodilators demonstrated benefit versus placebo, benefit versus monobronchodilators was not seen,37,38 perhaps due to the absence of a training or rehabilitation component within the older study designs.
The more recent PHYSACTO study was designed to evaluate the effects of bronchodilation alone or in combination with 8 weeks of additional exercise training on exercise capacity, and level of physical activity in patients with moderate–severe COPD. All patients were enrolled in a 12-week self-management behavior-modification program, focused on improving patient engagement in, and maintenance of, physical activity.39 PHYSACTO found that tiotropium (TIO)/olodaterol (Boehringer Ingelheim International GmbH, Ingelheim am Rhein, Germany), either alone or in combination with exercise training, did not significantly improve physical activity compared with placebo, although a significant reduction in symptom burden was observed. It is interesting to note that self-managed behavior modification alone significantly improved physical activity compared with baseline; this may have made any detectable differences in treatment benefit difficult. Furthermore, there was no correlation between exercise tolerance and change in physical activity.36
Recently, the dual bronchodilator IND/GLY was shown to reduce hyperinflation and improve daily physical activity levels compared with placebo, despite no patient education or lifestyle advice, suggesting a potential role in major clinical concerns in COPD.40 Therefore, a picture of the potential benefit of dual bronchodilation on activity is emerging; however, as lung-function decline in COPD is progressive, it is unknown whether earlier intervention with these treatments may be more beneficial in preserving physical ability. The impact of delaying step-up therapies on clinical parameters, such as activity levels, has yet to be established.
In symptomatic patients, the recently updated GOLD strategy document recommends that patients at lower risk of exacerbations (GOLD group B) should be treated with a long-acting bronchodilator, escalating to dual bronchodilation if symptoms persist.1 The LABA/LAMA IND/GLY has been shown to reduce dyspnea significantly compared with placebo and TIO monotherapy in dyspneic patients (modified Medical Research Council (mMRC) dyspnea scale score >2).41 This finding is supported by another post hoc analysis indicating that IND/GLY significantly reduced dyspnea compared with TIO in patients with a baseline dyspnea index score ≤7.42 Similarly, for the nonexacerbator phenotype, GesEPOC (Guía Española de la Enfermedad Pulmonar Obstructiva Crónica) recommends initial therapy with LAMA or LABA monotherapy escalating to second-line therapy with a LABA/LAMA combination.2 GesEPOC cites evidence from replicate studies demonstrating IND plus TIO to be superior to TIO alone,43 and another demonstrating IND/GLY to be superior to the ICS/LABA combination salmeterol/fluticasone (SFC; GlaxoSmithKline) on lung-function parameters in nonexacerbating patients to support the recommendation.2,44 In high-risk symptomatic patients (GOLD D), GOLD recommends LABA/LAMA as the preferred choice.1 If a single bronchodilator is chosen as initial treatment, LAMA is recommended, escalating to LABA/LAMA if exacerbations persist.1 SPARK and FLAME demonstrated that IND/GLY significantly reduced COPD exacerbations versus the LAMA GLY and SFC in patients with severe–very severe COPD.45,46 Additionally, both studies found a significant reduction in rescue-medication use versus the active comparators.45,46 Notably, the safety profile of dual bronchodilators is similar to that observed with placebo and individual monocomponents, with a comparable incidence of adverse events and serious adverse events.17,19,23 Furthermore, dual bronchodilators are associated with a lower incidence of pneumonia and oral candidiasis than ICS/LABA (SFC).46–49
Role of ICS
According to GOLD and GesEPOC, initial therapy with ICS/LABA may be first choice in those with suggestions of a steroid-responsive component to their airway disease, eg, those with a confirmed comorbid diagnosis of asthma, or those with a biomarker signature of TH2 disease.1,2,50 If exacerbations persist despite therapy with LABA/LAMA or ICS/LABA, treatment can be escalated to triple therapy (ICS/LABA/LAMA).1,2 Trial evidence showing a reduction in exacerbations with ICS/LABA compared with one or both components alone forms the basis for such recommendations; in the majority of these trials, patients had a history of one or more exacerbations in the year prior to the study.5,51–54 The addition of an ICS to a LABA/LAMA has not been studied specifically to date in any completed trials. Findings from the ongoing IMPACT and TRIBUTE are eagerly anticipated; both studies will investigate the efficacy of triple therapy vs LABA/LAMA in GOLD D patients.55,56 Post hoc analyses have suggested greater efficacy of ICS vs LABA monotherapy in patients with a blood eosinophil count ≥2% or ≥297.8 cells/μL.57,58 However, recently published data from FLAME demonstrated that a blood eosinophil count ≥2% was not a useful clinical biomarker in identifying patients who are likely to have a response to an ICS/LABA regimen when compared with a LABA/LAMA.46,59 Following ICS withdrawal, one analysis found an increased exacerbation rate in patients with higher eosinophil counts,60 and when stratified by exacerbation history, high eosinophils (≥400 cells/μL) were only associated with increased exacerbations in patients with two or more exacerbations in the previous year.61 Most studies showing an effect of an ICS have included participants with an FEV1 <50% predicted.62
Among patients at low risk of future exacerbation, a considerable proportion of patients inappropriately receive ICS/LABA, either alone or as part of triple therapy.63,64 Management of exacerbating patients has largely focused on maximizing bronchodilation, rather than prescribing an ICS-containing regimen.1,65 Due to the increased risk of pneumonia with an ICS,66 GOLD 2017 recommends that ICS withdrawal be considered if no benefit is seen.1 This recommendation is based on findings from WISDOM, which demonstrated that ICSs can be withdrawn in COPD patients without increased risk of exacerbation, provided adequate bronchodilator therapy is in place.67 If patients develop further exacerbations despite treatment with ICS/LABA/LAMA, the addition of a macrolide, roflumilast, carbocysteine, or theophylline should be considered, depending on patient phenotype.1,2,68
Which criteria might be most useful to guide treatment step-up from mono- to dual bronchodilation?
While different guidelines and strategy documents provide advice on the parameters to monitor routinely, namely lung-function measurements, symptoms, exacerbations, imaging, and smoking status,1,2 guidance related to the criteria that warrant step-up from mono- to dual bronchodilation are generally unclear, due to a lack of specific evidence.
The GesEPOC guidelines2 state that dual bronchodilation “should be tried” in symptomatic patients or those with evident exercise limitations following bronchodilator monotherapy. The National Institute for Health and Care Excellence guidelines provided more detailed recommendations compared with other guidance at the time of their publication; however, it is generally recognized that these have not been updated since 2010, and more evidence has become available since their publication.69 Recently, the GOLD recommendations have provided more specific guidance for stepping up from mono- to dual bronchodilation, ie, in group B patients with “persistent symptoms” and in group C patients with “persistent exacerbations”.1
Although a lack of evidence makes any particular recommendations speculative, several factors offer potential in aiding decisions on whether patients should change treatments, as shown in Table 2 and described in the following sections.
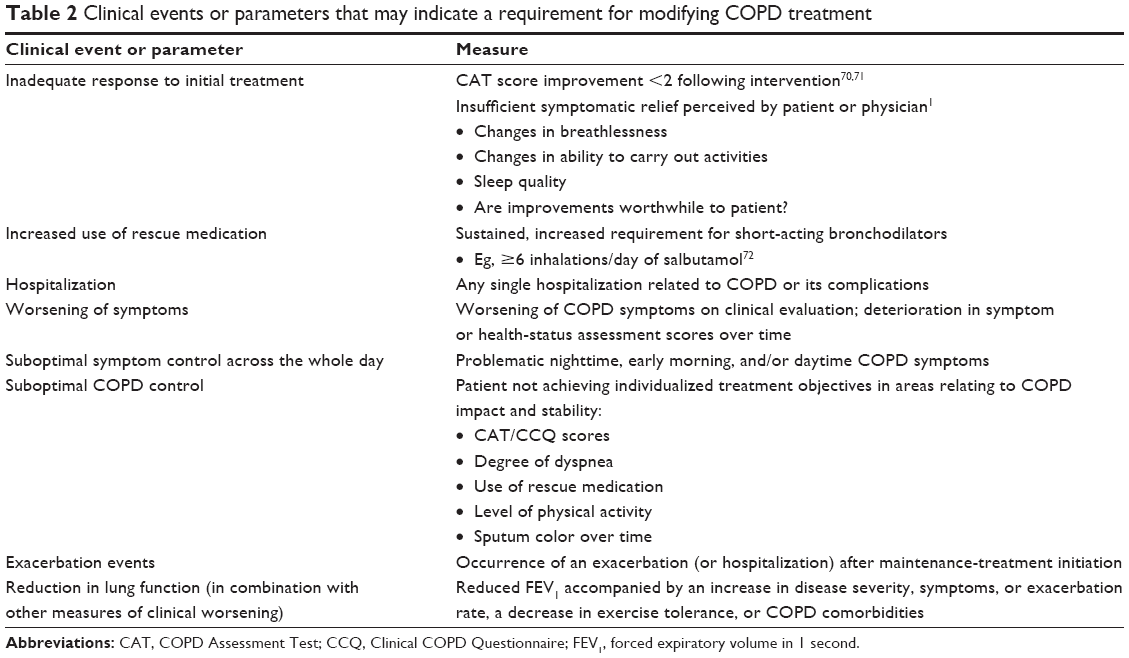 | Table 2 Clinical events or parameters that may indicate a requirement for modifying COPD treatment |
Inadequate response to initial treatment
In clinical practice, response to COPD pharmacotherapy and other medical treatment is often judged on the patient’s symptomatic response, eg, reduced breathlessness, increased exercise capacity, or reduced need for rescue medication.1 In the absence of other evidence, this may provide an indication to the physician as to whether a response is sufficient. This is inevitably subjective, as it is rare to abolish symptoms completely in COPD patients, and clinicians and patients must justify whether the treatment response is sufficiently large to make symptoms bearable and whether the change in functional capacity is adequate for the patient’s needs. An objective measure, such as the COPD Assessment Test (CAT), may be useful in assessing patient response to treatment and can be used routinely every 2–3 months.70 Research is ongoing to understand the minimal clinically relevant change in CAT score from one visit to the next, but a development steering group suggests a score difference of ≥2 suggests a clinically significant change in health status.70,71 Such a change or lack thereof could inform evaluation of treatment response after a suitable trial period. Adherence to treatment and inhalation technique should be assessed,1 and suboptimal adherence and inhalation technique should be addressed before concluding that current therapy is insufficient. If the patient or physician perceives inadequate symptomatic relief, assuming adherence to therapy and inhalation technique are acceptable, a change in treatment regimen should be considered.
Increased use of rescue medication
In our clinical experience, patients with a sustained daily requirement for short-acting bronchodilators may benefit from treatment intensification with long-acting bronchodilators. A retrospective analysis of clinical trial data (810 patients with moderate–very severe COPD) showed that short-acting BA reliever use is a predictor of short- and long-term (3-week and 10-month) exacerbation risk in patients with a history of exacerbations receiving budesonide/formoterol (AstraZeneca, Luton, UK) or formoterol.72 Exacerbation rate increased substantially with increasing reliever-medication use. Compared with patients who used a mean of fewer than two inhalations/day of reliever medication over a 2-month period, those who used a mean of 2–5, 6–9, and ≥10 inhalations/day (over the same time period) experienced 21% (P=0.22), 67% (P=0.0016), and 135% (P<0.001) higher exacerbation rates, respectively, over the following 10 months.72
Worsening of symptoms
Worsening of COPD symptoms on clinical evaluation may lead patients and physicians to consider stepping up treatment. Symptom or health-status assessment scores (eg, using the CAT or the Clinical COPD Questionnaire) may also inform patient–physician discussions on this topic, but trends and changes are more valuable than single measurements.1 As both questionnaires are short and easy to administer,71,73,74 these tools could be used at follow-up visits to provide additional confirmation of disease progression. The mMRC may not have sufficient sensitivity for this purpose.75
Suboptimal symptom control across the whole day
Although COPD symptoms can vary throughout the day, they are known to be problematic during both the day and night.76,77 An observational study of patients with stable COPD (n=727) reported a significant relationship between nighttime, early morning, and daytime symptoms.78 In each period, symptoms were associated with worse patient-reported outcomes (dyspnea, health status, sleep quality, and elevated anxiety and depression levels; all P<0.001 versus patients without symptoms in each corresponding period), suggesting that improving 24-hour symptom control should be an important consideration in the management of COPD. Most newer long-acting bronchodilators are effective for the full 24 hours after once-daily administration, and may be useful in improving overnight symptom control.79
Suboptimal COPD control
The concept of disease control considers the variable nature of the disease within the broader context of disease phenotype and severity. The two components of the “COPD control” concept are impact and stability.80 Impact refers to the clinical situation of a patient at a given moment in time, and can be measured by such instruments as the CAT, or by the degree of dyspnea, the use of rescue medication, the level of physical activity, and sputum color.80 Stability refers to the temporal evolution of impact over time (ie, by assessing impact at more than one time point and determining how this has changed or remained the same).80 The concept of COPD control has implications for treatment decisions, such that treatment may need to be stepped up if control is poor or maintained in the same way if there is disease stability. The ultimate goal of COPD treatment is optimal COPD control, as evidenced by the achievement of individualized treatment objectives. The proposal of the concept of control in COPD has yet to be validated.
Exacerbation events
The occurrence of exacerbations despite initial therapy may also be an indicator of the need for treatment escalation, such as switching to dual bronchodilation. Whether a single exacerbation is sufficient to merit escalation, or whether two exacerbations in a 12-month period or a single hospitalization should be the trigger, will be a matter of clinical judgment and depend to some extent on the severity of the COPD.
Reduction in lung function
Deterioration in lung function alone may not be an appropriate reason for switching therapy, as it does not capture the complexity of COPD: at a given level of airflow limitation, there is large variability in disease severity, symptoms, exercise tolerance, exacerbation rate, and the prevalence of comorbidities.81 However, a reduction in lung function considered alongside these factors may be a trigger for escalating COPD treatment.
Where are the evidence gaps?
Further work is needed to provide clear guidance for physicians regarding which tools and biomarkers can be used to assess patients and to guide decisions on which patients may need to progress from mono- to dual bronchodilation. Similarly, of all patients requiring an increase in medication from monotherapy with a long-acting bronchodilator, there is a need to clarify between those who would be more likely to benefit from a second long-acting bronchodilator and those more likely to benefit from an ICS and the effective dose.57,82,83 Investigations into the potential use of blood eosinophil counts as a predictive biomarker of ICS response are ongoing.
There is limited but increasing evidence directly assessing the proportion of patients who respond to dual bronchodilation who were uncontrolled with monotherapy. The benefits of directly switching from previous COPD treatment to dual bronchodilation on lung function and symptoms have been demonstrated in both CRYSTAL and a study by Kerwin et al.30,34 Donohue et al showed that nonresponders to LAMA or LABA monotherapy can experience significant and clinically meaningful improvements in lung function when treated with a LABA/LAMA combination,31 although other clinical outcomes were not evaluated.31 Nonetheless, this study supports the findings from many of the studies outlined in Table 1 in showing greater improvements in lung function with dual bronchodilation versus monotherapy. A subgroup analysis of data from SHINE and ILLUMINATE (n=2,667), showed that IND/GLY improved lung function in patients with moderate–severe COPD who had been previously treated with LAMA or LABA monotherapy. Improvements in dyspnea and health status with IND/GLY were also observed in participants previously receiving LAMA.84 However, several of the subgroups analyzed in this study were small, notably the prior-LABA-treatment group. Furthermore, all patients receiving medications during the prescreening of SHINE underwent extensive drug washout, except for those receiving short-acting BAs.84
As well as studies examining the magnitude of benefits of switching from mono- to dual-bronchodilator therapy, studies are required to look at the optimal timing of this escalation. It is not known whether greater benefits can be achieved if treatment is intensified early in the course of the disease or whether delaying the introduction of maximal bronchodilator therapy has any impact on overall disease progression.
Various applications of telemedicine and smartphone interventions are being investigated in COPD, and reports indicate some benefit in terms of reducing exacerbations, hospitalizations, and emergency-room visits.85,86 The use of smartphones requires effective synergistic strategies to improve outcomes,85,87 and a well-designed application could facilitate patient monitoring and alert physicians to the need to review treatment. With estimates of 2.6 billion smartphone owners by the end of 2017,88 the potential benefit of this direct interface with the patient should be assessed.
Avoiding unnecessary polypharmacy
In addition to the potential requirement for increasing treatment, physicians should be aware of the need to avoid unnecessary polypharmacy,1 eg, in patients in whom triple therapy, dual-, or monobronchodilation plus ICS therapy has been initiated, but who have not responded with perceived benefit (eg, symptom improvement) compared with previous dual therapy or monotherapy, respectively. “Perceived benefit” can be challenging to evaluate in clinical practice, particularly where the aim of therapy is to reduce exacerbations. For example, it can be difficult to discern whether an individual who continues to experience exacerbations following the addition of an ICS would have experienced a similar number or more of these events without this addition.
There is very little evidence to guide the stepping down of treatment between dual and monobronchodilation. There is evidence to support the withdrawal of ICSs in some patients receiving triple therapy. In addition to WISDOM67 (as mentioned earlier), OPTIMO also assessed the withdrawal of ICS therapy in patients at low risk of exacerbation receiving maintenance therapy with long-acting bronchodilators and ICSs. OPTIMO did not find any deterioration in lung function or exacerbation rate when ICS was withdrawn compared with continued ICS therapy, providing regular treatment with long-acting bronchodilators was maintained.89
Despite limited evidence related to stepping down from triple or dual therapy, there is general consensus that a large number of COPD patients are overtreated, particularly at the milder end of the spectrum.64,90,91 Ultimately, the decision to continue or withdraw stepped up therapy must be made on a patient-to-patient basis and must balance the risk of adverse events with any potential impact on lung function, symptoms, and exacerbation risk.
Summary
Bronchodilators are central to COPD treatment. Long-acting bronchodilators are recommended as initial therapy in symptomatic patients, whether or not the patient has a high risk of exacerbations. Dual bronchodilation may be suitable as a step-up approach in those with persistent symptoms or exacerbations. Initial therapy with dual bronchodilation could be appropriate for some patients, particularly those at risk of exacerbation or with severe symptoms at diagnosis. New evidence shows that LABA/LAMA combinations may reduce the rate of exacerbations compared with ICS/LABA, even in patients with a history of exacerbations. However, COPD is a heterogeneous condition, and an individualized treatment approach is required. Currently, it is not clear at which stage patients should progress from mono- to dual bronchodilation. We have identified and discussed a number of factors that may help physicians to identify the point at which patients should change treatment, although further work is required to clarify specific thresholds (Table 2). This may encompass the use of indicators such as symptomatic response, use of rescue medication, hospitalizations, disease control, and the occurrence of exacerbations. Future research should aim to provide a better understanding of when a patient should progress treatment, and identify the appropriate tools to inform this decision.
Acknowledgments
The authors were assisted in the preparation of the manuscript by Rebecca Douglas, a professional medical writer contracted to CircleScience, an Ashfield company, part of UDG Healthcare PLC. Medical writing support was funded by Novartis Pharma AG (Basel, Switzerland).
Disclosure
MT has received speaker’s fees from Aerocrine, AstraZeneca, Boehringer Ingelheim, Novartis, GlaxoSmithKline, and Teva, and received consulting fees from Aerocrine, Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, MSD, and Novartis. MM has received speaker’s fees from Almirall, AstraZeneca, Boehringer Ingelheim, Novartis, Pfizer, Grifols, Menarini, Gebro Pharma, and Zambon, and consulting fees from Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, Pfizer, Cipla, and Grifols. DMGH has received speaker’s fees from AstraZeneca, Boehringer Ingelheim, Novartis, and Pfizer, and consulting fees from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, and Pfizer. The authors report no other conflicts of interest in this work.
References
Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 report: GOLD executive summary. Eur Respir J. 2017;49(3):1700214. | ||
Miravitlles M, Soler-Cataluña JJ, Calle M, et al. Spanish COPD guidelines (GesEPOC) 2017: pharmacological treatment of stable chronic obstructive pulmonary disease. Arch Bronconeumol. 2017;53:324–335. | ||
Donohue JF, van Noord JA, Bateman ED, et al. A 6-month, placebo-controlled study comparing lung function and health status changes in COPD patients treated with tiotropium or salmeterol. Chest. 2002;122(1):47–55. | ||
D’Urzo A, Ferguson GT, van Noord JA, et al. Efficacy and safety of once-daily NVA237 in patients with moderate-to-severe COPD: the GLOW1 trial. Respir Res. 2011;12:156. | ||
Calverley PM, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356(8):775–789. | ||
Rossi A, Kristufek P, Levine BE, et al. Comparison of the efficacy, tolerability, and safety of formoterol dry powder and oral, slow-release theophylline in the treatment of COPD. Chest. 2002;121(4):1058–1069. | ||
Chapman KR, Rennard SI, Dogra A, et al. Long-term safety and efficacy of indacaterol, a long-acting β2-agonist, in subjects with COPD: a randomized, placebo-controlled study. Chest. 2011;140(1):68–75. | ||
Kerwin EM, D’Urzo AD, Gelb AF, Lakkis H, Garcia GE, Caracta CF. Efficacy and safety of a 12-week treatment with twice-daily aclidinium bromide in COPD patients (ACCORD COPD I). COPD. 2012;9(2):90–101. | ||
Beeh KM, Singh D, Di Scala L, Drollmann A. Once-daily NVA237 improves exercise tolerance from the first dose in patients with COPD: the GLOW3 trial. Int J Chron Obstruct Pulmon Dis. 2012;7:503–513. | ||
Maltais F, Celli B, Casaburi R, et al. Aclidinium bromide improves exercise endurance and lung hyperinflation in patients with moderate to severe COPD. Respir Med. 2011;105(4):580–587. | ||
O’Donnell DE, Flüge T, Gerken F, et al. Effects of tiotropium on lung hyperinflation, dyspnoea and exercise tolerance in COPD. Eur Respir J. 2004;23(6):832–840. | ||
O’Donnell DE, Casaburi R, Vincken W, et al. Effect of indacaterol on exercise endurance and lung hyperinflation in COPD. Respir Med. 2011;105(7):1030–1036. | ||
Halpin DM, Vogelmeier C, Pieper MP, Metzdorf N, Richard F, Anzueto A. Effect of tiotropium on COPD exacerbations: a systematic review. Respir Med. 2016;114:1–8. | ||
Jones PW, Singh D, Bateman ED, et al. Efficacy and safety of twice-daily aclidinium bromide in COPD patients: the ATTAIN study. Eur Respir J. 2012;40(4):830–836. | ||
Price D, West D, Brusselle G, et al. Management of COPD in the UK primary-care setting: an analysis of real-life prescribing patterns. Int J Chron Obstruct Pulmon Dis. 2014;9:889–905. | ||
Zuwallack R. How are you doing? What are you doing? Differing perspectives in the assessment of individuals with COPD. COPD. 2007;4(3):293–297. | ||
Chapman K, Bateman E, Gallagher N, Hu H, Banerji D. QVA149 once daily improves lung function, dyspnoea and health status independent of prior medications and disease severity: the SHINE study. Thorax. 2013;68 (Suppl 3):A182–A183 (Abstract P234). | ||
D’Urzo AD, Rennard SI, Kerwin EM, Mergel V, Leslbaum AR, Caracta CF. Efficacy and safety of fixed-dose combinations of aclidinium bromide/formoterol fumarate: the 24-week, randomized, placebo-controlled AUGMENT COPD study. Respir Res. 2014;15:123. | ||
Donohue JF, Maleki-Yazdi MR, Kilbride S, Mehta R, Kalberg C, Church A. Efficacy and safety of once-daily umeclidinium/vilanterol 62.5/25 mg in COPD. Respir Med. 2013;107(10):1538–1546. | ||
Beeh KM, Korn S, Beier J, et al. Effect of QVA149 on lung volumes and exercise tolerance in COPD patients: the BRIGHT study. Respir Med. 2014;108(4):584–592. | ||
Buhl R, Maltais F, Abrahams R, et al. Tiotropium and olodaterol fixed-dose combination versus mono-components in COPD (GOLD 2–4). Eur Respir J. 2015;45(4):969–979. | ||
Maleki-Yazdi MR, Kaelin T, Richard N, Zvarich M, Church A. Efficacy and safety of umeclidinium/vilanterol 62.5/25 mcg and tiotropium 18 mcg in chronic obstructive pulmonary disease: results of a 24-week, randomized, controlled trial. Respir Med. 2014;108(12):1752–1760. | ||
Singh D, Jones PW, Bateman ED, et al. Efficacy and safety of aclidinium bromide/formoterol fumarate fixed-dose combinations compared with individual components and placebo in patients with COPD (ACLIFORM-COPD): a multicentre, randomised study. BMC Pulm Med. 2014;14:178. | ||
Decramer M, Anzueto A, Kerwin E, et al. Efficacy and safety of umeclidinium plus vilanterol versus tiotropium, vilanterol, or umeclidinium monotherapies over 24 weeks in patients with chronic obstructive pulmonary disease: results from two multicentre, blinded, randomised controlled trials. Lancet Respir Med. 2014;2(6):472–486. | ||
Jones PW, Beeh KM, Chapman KR, Decramer M, Mahler DA, Wedzicha JA. Minimal clinically important differences in pharmacological trials. Am J Respir Crit Care Med. 2014;189(3):250–255. | ||
Jones PW, Rennard S, Tabberer M, Riley JH, Vahdati-Bolouri M, Barnes NC. Interpreting patient-reported outcomes from clinical trials in COPD: a discussion. Int J Chron Obstruct Pulmon Dis. 2016;11:3069–3078. | ||
Singh D. New combination bronchodilators for chronic obstructive pulmonary disease: current evidence and future perspectives. Br J Clin Pharmacol. 2015;79(5):695–708. | ||
Tashkin DP, Ferguson GT. Combination bronchodilator therapy in the management of chronic obstructive pulmonary disease. Respir Res. 2013;14:49. | ||
Cazzola M, Molimard M. The scientific rationale for combining long-acting β2-agonists and muscarinic antagonists in COPD. Pulm Pharmacol Ther. 2010;23(4):257–267. | ||
Kerwin EM, Kalberg CJ, Galkin DV, et al. Umeclidinium/vilanterol as step-up therapy from tiotropium in patients with moderate COPD: a randomized, parallel-group, 12-week study. Int J Chron Obstruct Pulmon Dis. 2017;12:745–755. | ||
Donohue JF, Singh D, Munzu C, Kilbride S, Church A. Magnitude of umeclidinium/vilanterol lung function effect depends on monotherapy responses: results from two randomised controlled trials. Respir Med. 2016;112:65–74. | ||
Donohue JF. Response to letter to the editor: improvements in lung function with umeclidinium/vilanterol versus fluticasone propionate/salmeterol in patients with moderate-to-severe COPD and infrequent exacerbations. Respir Med. 2016;110:81. | ||
Banerji D, Patalano F. Improvements in lung function with umeclidinium/vilanterol versus fluticasone propionate/salmeterol in patients with moderate-to-severe COPD and infrequent exacerbations. Respir Med. 2016;110:79–80. | ||
Vogelmeier C, Alamian-Mattheis M, Greulich T, et al. Efficacy and safety of the direct switch from various previous treatments to glycopyrronium or indacaterol/glycopyrronium in patients with moderate COPD: the CRYSTAL study. Presented at the British Thoracic Society, London, UK, 7–9 December 2016. 2016. | ||
Troosters T, van der Molen T, Polkey M, et al. Improving physical activity in COPD: towards a new paradigm. Respir Res. 2013;14:115. | ||
Troosters T, Lavoie K, Leidy N, et al. Effects of bronchodilator therapy and exercise training, added to a self-management behaviour-modification programme, on physical activity in COPD. Presented at the European Respiratory Society (ERS) International Congress, London, United Kingdom, 3–7 September 2016 (Poster PA713). 2016. | ||
Maltais F, Singh S, Donald AC, et al. Effects of a combination of umeclidinium/vilanterol on exercise endurance in patients with chronic obstructive pulmonary disease: two randomized, double-blind clinical trials. Ther Adv Respir Dis. 2014;8(6):169–181. | ||
Beeh KM, Korn S, Beier J, et al. QVA149 once daily improves exercise tolerance and lung function in patients with moderate to severe COPD: the BRIGHT study. Thorax. 2012;67 (Suppl 2):A147 (Abstract P191). | ||
Troosters T, Bourbeau J, Maltais F, et al. Enhancing exercise tolerance and physical activity in COPD with combined pharmacological and non-pharmacological interventions: PHYSACTO randomised, placebo-controlled study design. BMJ Open. 2016;6(4):e010106. | ||
Watz H, Mailander C, Baier M, Kirsten A. Effects of indacaterol/glycopyrronium (QVA149) on lung hyperinflation and physical activity in patients with moderate to severe COPD: a randomised, placebo-controlled, crossover study (the MOVE study). BMC Pulm Med. 2016;16:95. | ||
Bateman ED, Mahler DA, Vogelmeier CF, Wedzicha JA, Patalano F, Banerji D. Recent advances in COPD disease management with fixed-dose long-acting combination therapies. Expert Rev Respir Med. 2014;8(3):357–379. | ||
Mahler DA, Keininger DL, Mezzi K, Fogel R, Banerji D. Efficacy of indacaterol/glycopyrronium in patients with COPD who have increased dyspnea with daily activities. Chronic Obstr Pulm Dis (Miami). 2016;3(4):758–768. | ||
Mahler DA, D’Urzo A, Bateman ED, et al. Concurrent use of indacaterol plus tiotropium in patients with COPD provides superior bronchodilation compared with tiotropium alone: a randomised, double-blind comparison. Thorax. 2012;67(9):781–788. | ||
Vogelmeier C, Bateman ED, D’Andrea P, et al. Once-daily QVA149 is more effective than twice-daily salmeterol/fluticasone in improving lung function, in patients with severe chronic obstructive pulmonary disease (COPD): the ILLUMINATE study. Am J Respir Crit Care Med. 2014;189(1):A3763. | ||
Wedzicha JA, Decramer M, Ficker JH, et al. Analysis of chronic obstructive pulmonary disease exacerbations with the dual bronchodilator QVA149 compared with glycopyrronium and tiotropium (SPARK): a randomised, double-blind, parallel-group study. Lancet Respir Med. 2013;1(3):199–209. | ||
Wedzicha JA, Banerji D, Chapman KR, et al. Indacaterol-glycopyrronium versus salmeterol-fluticasone for COPD. N Engl J Med. 2016;374(23):2222–2234. | ||
Donohue JF, Worsley S, Zhu CQ, Hardaker L, Church A. Improvements in lung function with umeclidinium/vilanterol versus fluticasone propionate/salmeterol in patients with moderate-to-severe COPD and infrequent exacerbations. Respir Med. 2015;109(7):870–881. | ||
Vogelmeier CF, Bateman ED, Pallante J, et al. Efficacy and safety of once-daily QVA149 compared with twice-daily salmeterol-fluticasone in patients with chronic obstructive pulmonary disease (ILLUMINATE): a randomised, double-blind, parallel group study. Lancet Respir Med. 2013;1(1):51–60. | ||
Vogelmeier C, Paggiaro PL, Dorca J, et al. Efficacy and safety of aclidinium/formoterol versus salmeterol/fluticasone: a phase 3 COPD study. Eur Respir J. 2016;48(4):1030–1039. | ||
Kostikas K, Clemens A, Patalano F. The asthma-COPD overlap syndrome: do we really need another syndrome in the already complex matrix of airway disease? Int J Chron Obstruct Pulmon Dis. 2016;11:1297–1306. | ||
Calverley PM, Boonsawat W, Cseke Z, Zhong N, Peterson S, Olsson H. Maintenance therapy with budesonide and formoterol in chronic obstructive pulmonary disease. Eur Respir J. 2003;22(6):912–919. | ||
Anzueto A, Ferguson GT, Feldman G, et al. Effect of fluticasone propionate/salmeterol (250/50) on COPD exacerbations and impact on patient outcomes. COPD. 2009;6(5):320–329. | ||
Dransfield MT, Bourbeau J, Jones PW, et al. Once-daily inhaled fluticasone furoate and vilanterol versus vilanterol only for prevention of exacerbations of COPD: two replicate double-blind, parallel-group, randomised controlled trials. Lancet Respir Med. 2013;1(3):210–223. | ||
Vestbo J, Anderson JA, Brook RD, et al. Fluticasone furoate and vilanterol and survival in chronic obstructive pulmonary disease with heightened cardiovascular risk (SUMMIT): a double-blind randomised controlled trial. Lancet. 2016;387(10030):1817–1826. | ||
Pascoe SJ, Lipson DA, Locantore N, et al. A phase III randomised controlled trial of single-dose triple therapy in COPD: the IMPACT protocol. Eur Respir J. 2016;48(2):320–330. | ||
Chiesi Farmaceutici. 2-Arm Parallel Group Study of Fixed Combination of CHF 5993 vs Ultibro® in COPD Patients (TRIBUTE). Available from: https://clinicaltrials.gov/ct2/show/NCT02579850. NLM identifier: NCT02579850. Accessed February 9, 2017. | ||
Pascoe S, Locantore N, Dransfield MT, Barnes NC, Pavord ID. Blood eosinophil counts, exacerbations, and response to the addition of inhaled fluticasone furoate to vilanterol in patients with chronic obstructive pulmonary disease: a secondary analysis of data from two parallel randomised controlled trials. Lancet Respir Med. 2015;3(6):435–442. | ||
Siddiqui SH, Guasconi A, Vestbo J, et al. Blood eosinophils: a biomarker of response to extrafine beclomethasone/formoterol in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192(4):523–525. | ||
Donohue JF. Another choice for prevention of COPD exacerbations. N Engl J Med. 2016;374(23):2284–2286. | ||
Watz H, Tetzlaff K, Wouters EF, et al. Blood eosinophil count and exacerbations in severe chronic obstructive pulmonary disease after withdrawal of inhaled corticosteroids: a post-hoc analysis of the WISDOM trial. Lancet Respir Med. 2016;4(5):390–398. | ||
Calverley P, Tetzlaff K, Vogelmeier C, et al. Evaluating blood eosinophils and exacerbation history to predict ICS response in COPD. Poster presented at: European Respiratory (ERS) Society International Congress; September 3–7, 2016; London (Poster OA1973). | ||
Vestbo J, Lange P. Prevention of COPD exacerbations: medications and other controversies. ERJ Open Research. 2015;1(1): pii:00011–02015. | ||
Vestbo J, Vogelmeier C, Small M, Higgins V. Understanding the GOLD 2011 strategy as applied to a real-world COPD population. Respir Med. 2014;108(5):729–736. | ||
Brusselle G, Price D, Gruffydd-Jones K, et al. The inevitable drift to triple therapy in COPD: an analysis of prescribing pathways in the UK. Int J Chron Obstruct Pulmon Dis. 2015;10:2207–2217. | ||
Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of COPD. Bethesda, MD: GOLD; 2016. Available from: http://goldcopd.org/global-strategy-diagnosis-management-prevention-copd-2016/. Accessed February 05, 2016. | ||
Festic E, Bansal V, Gupta E, Scanlon PD. Association of inhaled corticosteroids with incident pneumonia and mortality in COPD patients: systematic review and meta-analysis. COPD. 2015;13(3):312–326. | ||
Magnussen H, Disse B, Rodriguez-Roisin R, et al. Withdrawal of inhaled glucocorticoids and exacerbations of COPD. N Engl J Med. 2014;371(14):1285–1294. | ||
Miravitlles M, D’Urzo A, Singh D, Koblizek V. Pharmacological strategies to reduce exacerbation risk in COPD: a narrative review. Respir Res. 2016;17(1):112. | ||
Chronic obstructive pulmonary disease. Management of chronic obstructive pulmonary disease in adults in primary and secondary care. NICE clinical guideline 101 (partial update). Updated June 2010. Available from: https://www.nice.org.uk/guidance/cg101. Accessed June 5, 2017. | ||
GlaxoSmithKline. COPD Assessment Test: Expert Guidance on Frequently Asked Questions. Brentford, UK: GSK; 2012. Available from: http://www.catestonline.org/images/UserGuides/CATHCPUser%20guideEn.pdf. | ||
Jones PW, Brusselle G, Dal Negro RW, et al. Properties of the COPD assessment test in a cross-sectional European study. Eur Respir J. 2011;38(1):29–35. | ||
Jenkins CR, Postma DS, Anzueto AR, et al. Reliever salbutamol use as a measure of exacerbation risk in chronic obstructive pulmonary disease. BMC Pulm Med. 2015;15:97. | ||
Jones PW. COPD assessment test: rationale, development, validation and performance. COPD. 2013;10(2):269–271. | ||
Tsiligianni IG, van der Molen T, Moraitaki D, et al. Assessing health status in COPD: a head-to-head comparison between the COPD assessment test (CAT) and the clinical COPD questionnaire (CCQ). BMC Pulm Med. 2012;12:20. | ||
Stenton C. The MRC breathlessness scale. Occup Med (Lond). 2008;58(3):226–227. | ||
Price D, Small M, Milligan G, Higgins V, Gil EG, Estruch J. Impact of night-time symptoms in COPD: a real-world study in five European countries. Int J Chron Obstruct Pulmon Dis. 2013;8:595–603. | ||
Agusti A, Hedner J, Marin JM, Barbé F, Cazzola M, Rennard S. Night-time symptoms: a forgotten dimension of COPD. Eur Respir Rev. 2011;20(121):183–194. | ||
Miravitlles M, Worth H, Soler-Cataluña JJ, et al. Observational study to characterise 24-hour COPD symptoms and their relationship with patient-reported outcomes: results from the ASSESS study. Respir Res. 2014;15:122. | ||
Lôtvall J, Cosio BG, Iqbal A, et al. Indacaterol once-daily improves day-and night-time symptom control in COPD patients: a 26-week study versus placebo and tiotropium. Eur Respir J. 2009;34 (Suppl 53):346S (Abstract P2029). | ||
Soler-Cataluña JJ, Alcazar-Navarrete B, Miravitlles M. The concept of control of COPD in clinical practice. Int J Chron Obstruct Pulmon Dis. 2014;9:1397–1405. | ||
Agusti A, Calverley PM, Celli B, et al. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res. 2010;11:122. | ||
Pavord ID, Lettis S, Locantore N, et al. Blood eosinophils and inhaled corticosteroid/long-acting β-2 agonist efficacy in COPD. Thorax. 2016;71(2):118–125. | ||
Martinez FJ, Rabe KF, Sethi S, et al. Effect of roflumilast and inhaled corticosteroid/long-acting β2-agonist on chronic obstructive pulmonary disease exacerbations (RE2SPOND): a randomized clinical trial. Am J Respir Crit Care Med. 2016;194(5):559–567. | ||
Chapman KR, Bateman ED, Chen HT, Hu HL, Fogel R, Banerji D. QVA149 improves lung function, dyspnea, and health status independent of previously prescribed medications and COPD severity: a subgroup analysis from the SHINE and ILLUMINATE studies. J COPD Foundation. 2015;2(1):48–60. | ||
Alwashmi M, Hawboldt J, Davis E, Marra C, Gamble JM, Ashour WA. The effect of smartphone interventions on patients with chronic obstructive pulmonary disease exacerbations: a systematic review and meta-analysis. JMIR Mhealth Uhealth. 2016;4(3):e105. | ||
Esteban C, Moraza J, Iriberri M, et al. Outcomes of a telemonitoring-based program (telEPOC) in frequently hospitalized COPD patients. Int J Chron Obstruct Pulmon Dis. 2016;11:2919–2930. | ||
Halpin D, Banks L, Martello A. Working together to go ‘beyond the pill’: building a virtuous network of collaborators. BMJ Innovations. 2016;2:1–3. | ||
Statista. Smartphones: statistics and facts. Available from: https://www.statista.com/topics/840/smartphones. Accessed May 17, 2017. | ||
Rossi A, Guerriero M, Corrado A. Real-life study on the appropriateness of treatment in moderate COPD patients (OPTIMO). Eur Respir J. 2013;42 Suppl 57:143S–144S (Abstract P4144). | ||
Magnoni MS, Rizzi A, Visconti A, Donner CF. AIMAR survey on COPD phenotypes. Multidiscip Respir Med. 2014;9(1):16. | ||
Cazzola M, Rogliani P, Matera MG. Escalation and de-escalation of therapy in COPD: myths, realities and perspectives. Drugs. 2015;75(14):1575–1585. | ||
Aaron SD, Vandemheen KL, Fergusson D, et al. Tiotropium in combination with placebo, salmeterol, or fluticasone-salmeterol for treatment of chronic obstructive pulmonary disease: a randomized trial. Ann Intern Med. 2007;146(8):545–555. | ||
Beier J, van Noord J, Deans A, et al. Safety and efficacy of dual therapy with GSK233705 and salmeterol versus monotherapy with salmeterol, tiotropium, or placebo in a crossover pilot study in partially reversible COPD patients. Int J Chron Obstruct Pulmon Dis. 2012;7:153–164. | ||
Celli B, Crater G, Kilbride S, et al. Once-daily umeclidinium/vilanterol 125/25 mcg in COPD: a randomized, controlled study. Chest. 2014;145(5):981–991. | ||
Hanania NA, Boota A, Kerwin E, Tomlinson L, Denis-Mize K. Efficacy and safety of nebulized formoterol as add-on therapy in COPD patients receiving maintenance tiotropium bromide: results from a 6-week, randomized, placebo-controlled, clinical trial. Drugs. 2009;69(9):1205–1216. | ||
Hoshino M, Ohtawa J. Computed tomography assessment of airway dimensions with combined tiotropium and indacaterol therapy in COPD patients. Respirology. 2014;19(3):403–410. | ||
Imran M, Chhabra S, Kotwani A. Combinations of long acting β2 agonists to tiotropium: a randomized, double-blind, placebo-controlled, active-drug controlled, parallel design academic clinical trial in moderate COPD male patients. Arch Pharm Pract. 2015;6(2):19–23. | ||
Jayaram L, Wong C, McAuley S, Rea H, Zeng I, O’Dochartaigh C. Combined therapy with tiotropium and formoterol in chronic obstructive pulmonary disease: effect on the 6-minute walk test. COPD. 2013;10(4):466–472. | ||
Salvi S, Brashier B, Gothi D, et al. Bronchodilator efficacy of tiotropium-formoterol via single pressurized meter dose inhaler (pMDI) versus tiotropium alone in COPD. Pulm Pharmacol Ther. 2014;27(1):90–95. | ||
Tashkin DP, Littner M, Andrews CP, Tomlinson L, Rinehart M, Denis-Mize K. Concomitant treatment with nebulized formoterol and tiotropium in subjects with COPD: a placebo-controlled trial. Respir Med. 2008;102(4):479–487. | ||
Tashkin DP, Pearle J, Iezzoni D, Varghese ST. Formoterol and tiotropium compared with tiotropium alone for treatment of COPD. COPD. 2009;6(1):17–25. | ||
Tashkin DP, Donohue JF, Mahler DA, et al. Effects of arformoterol twice daily, tiotropium once daily, and their combination in patients with COPD. Respir Med. 2009;103(4):516–524. | ||
Terzano C, Petroianni A, Conti V, et al. Rational timing of combination therapy with tiotropium and formoterol in moderate and severe COPD. Respir Med. 2008;102(12):1701–1707. | ||
van Noord JA, Aumann JL, Janssens E, et al. Effects of tiotropium with and without formoterol on airflow obstruction and resting hyperinflation in patients with COPD. Chest. 2006;129(3):509–517. | ||
van Noord JA, Aumann JL, Janssens E, et al. Comparison of tiotropium once daily, formoterol twice daily and both combined once daily in patients with COPD. Eur Respir J. 2005;26(2):214–222. | ||
van Noord JA, Aumann JL, Janssens E, et al. Combining tiotropium and salmeterol in COPD: effects on airflow obstruction and symptoms. Respir Med. 2010;104(7):995–1004. | ||
Vincken W, Aumann J, Chen H, Henley M, McBryan D, Goyal P. Efficacy and safety of coadministration of once-daily indacaterol and glycopyrronium versus indacaterol alone in COPD patients: the GLOW6 study. Int J Chron Obstruct Pulmon Dis. 2014;9:215–218. | ||
Vogelmeier C, Kardos P, Harari S, Gans SJ, Stenglein S, Thirlwell J. Formoterol mono- and combination therapy with tiotropium in patients with COPD: a 6-month study. Respir Med. 2008;102(11):1511–1520. | ||
ZuWallack R, Allen L, Hernandez G, Ting N, Abrahams R. Efficacy and safety of combining olodaterol Respimat and tiotropium HandiHaler in patients with COPD: results of two randomized, double-blind, active-controlled studies. Int J Chron Obstruct Pulmon Dis. 2014;9:1133–1144. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.