Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
When and How Grid-Based Information Management for VTE Prevention: Boundary Conditions and Configurational Pathways from a Mixed-Methods Study
Authors Wang C, Li H, Chen S, Zhou M, Ding T
Received 11 December 2025
Accepted for publication 4 February 2026
Published 12 February 2026 Volume 2026:19 588156
DOI https://doi.org/10.2147/JMDH.S588156
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Chunyan Wang,1 Haiyan Li,2 Shiyuan Chen,1 Min Zhou,1 Tian Ding3
1Department of Vascular Surgery, Affiliated Hospital of North Sichuan Medical College, Nanchong, 637000, People’s Republic of China; 2Department of Vascular Surgery, First Affiliated Hospital of Naval Medical University, Shanghai, 200433, People’s Republic of China; 3Phase I Clinical Trial Center, Affiliated Hospital of North Sichuan Medical College, Nanchong, 637000, People’s Republic of China
Correspondence: Chunyan Wang, Department of Vascular Surgery, Affiliated Hospital of North Sichuan Medical College, Nanchong, 637000, People’s Republic of China, Email [email protected]
Background: Venous thromboembolism (VTE) is a significant cause of preventable morbidity and mortality among hospitalized patients. Although grid-based information management systems have shown effectiveness in VTE prevention, the boundary conditions and configurational pathways leading to optimal outcomes remain unclear.
Objective: To investigate the impact mechanism of grid-based information management on VTE prevention effectiveness, identify boundary conditions of moderating effects, and explore configurational pathways leading to high prevention outcomes.
Methods: A mixed-methods study design was employed. A total of 119 hospitalized patients from Affiliated Hospital of North Sichuan Medical college were enrolled between January and December 2024, with 58 patients in the control group (traditional management) and 61 in the intervention group (grid-based information management). The Johnson-Neyman (J-N) technique was used to identify the boundary conditions of nurses’ VTE knowledge and departmental collaboration on intervention effectiveness. Fuzzy-set qualitative comparative analysis (fsQCA) was employed to identify configurational pathways leading to high VTE prevention outcomes.
Results: The intervention group demonstrated significantly higher VTE risk assessment completion rates (86.9% vs 63.8%, absolute difference 23.1%, 95% CI 8.7– 37.5%, P< 0.01), prevention measure implementation rates (90.2% vs 58.6%, absolute difference 31.6%, 95% CI 17.2– 46.0%, P< 0.01), and lower VTE incidence (3.3% vs 8.6%, absolute risk reduction 5.3%, 95% CI 0.4– 10.2%, NNT=19, 95% CI 10– 250, P=0.032). J-N analysis revealed that the positive effect of grid-based information management on VTE risk assessment became significant when nurses’ VTE knowledge scores reached ≥ 42 points (P< 0.05), and the effect on prevention measure implementation became significant when departmental collaboration scores reached ≥ 3.4 points (P< 0.05). FsQCA identified three configurational pathways leading to high VTE prevention outcomes: technology-driven, collaboration-driven, and comprehensive support pathways, with an overall solution consistency of 0.892 and coverage of 0.684.
Conclusion: Grid-based information management effectively improves VTE prevention outcomes, but its effectiveness is contingent upon nurses’ knowledge levels and departmental collaboration. Multiple equifinal pathways exist to achieve high VTE prevention outcomes, providing evidence for tailored implementation strategies.
Keywords: venous thromboembolism, vte, grid-based information management, mixed-methods study, Johnson–Neyman technique, fuzzy-set qualitative comparative analysis, fsQCA
Introduction
Venous thromboembolism (VTE), encompassing deep vein thrombosis (DVT) and pulmonary embolism (PE), represents a major source of preventable morbidity and mortality in hospitalized patients.1,2 VTE is recognized as the third most common cardiovascular disorder following ischemic heart disease and stroke, characterized by high incidence, insidious symptoms, and frequent underdiagnosis.3,4 Despite the availability of effective prophylactic strategies, studies consistently demonstrate suboptimal adherence to VTE prevention guidelines, with prophylaxis rates among medical inpatients often falling below 50%.5,6
Clinical decision support systems (CDSS) integrated within electronic health records have emerged as promising tools to improve VTE prophylaxis rates.7,8 Kucher et al7 demonstrated that computerized alert systems significantly improved VTE prophylaxis prescription and reduced VTE incidence. Similarly, Galanter et al9 reported that mandatory VTE risk assessment within electronic medical records promoted improved rates of pharmacologic prophylaxis. However, the effectiveness of such systems varies considerably across healthcare settings, suggesting the presence of boundary conditions that moderate their impact.10–12
Grid-based information management represents an innovative approach that combines grid management philosophy with information technology, establishing multi-level management systems and leveraging information systems for precise intervention delivery.13 This approach has shown promising results in VTE prevention; however, existing studies predominantly employ simple pre-post comparison designs with several limitations. First, they lack in-depth exploration of impact mechanisms and fail to reveal the boundary conditions under which grid-based information management demonstrates effectiveness. Second, they overlook the synergistic effects of different condition combinations on prevention outcomes, making it difficult to provide evidence for differentiated implementation strategies.14,15
To address these gaps, the present study employs a mixed-methods design combining Johnson-Neyman (J-N) moderation analysis with fuzzy-set qualitative comparative analysis (fsQCA). The J-N technique, originally developed by Johnson and Neyman16 and recently gaining increased attention in health services research,17,18 allows precise identification of moderator values at which intervention effects transition between significance and non-significance, thereby revealing “when” conditions are effective. FsQCA, developed by Ragin,19,20 examines how combinations of conditions lead to outcomes, thereby revealing “how” conditions combine to be effective. This methodological combination enables comprehensive investigation of both boundary conditions and configurational pathways, providing robust evidence for precision implementation of VTE prevention strategies.
Methods
Study Design and Setting
This study employed a mixed-methods research design conducted at Affiliated Hospital of North Sichuan Medical college, China. The study protocol was approved by the Shanghai Changhai Hospital (First Affiliated Hospital of Naval Medical University) Ethics Committee (approval number: CHEC2023-109), and all participants provided written informed consent.
Participants
Patients were enrolled using convenience sampling between January and December 2024. Inclusion criteria were: (1) age ≥18 years; (2) admission to high VTE-risk departments including orthopedics, oncology, hematology, hepatobiliary surgery, obstetrics and gynecology, gastrointestinal surgery, neurosurgery, thoracic surgery, respiratory medicine, neurology, and cardiovascular medicine; and (3) hospital stay >24 hours. Exclusion criteria were: (1) history of DVT or PE; (2) psychiatric disorders or cognitive impairment; and (3) withdrawal from the study or incomplete data.
Patients admitted between January and June 2024 (n=58) constituted the control group receiving traditional VTE prevention management. Patients admitted between July and December 2024 (n=61) constituted the intervention group receiving grid-based information management.
Intervention
Control Group
The Caprini Risk Assessment Model is a validated weighted scoring system that assigns points (1–5) to approximately 40 risk factors (eg, age, surgery, medical conditions, mobility). Total scores categorize risk as low (0–1), moderate (2), high (3–4), or highest (≥5).21–24 The control group received traditional VTE prevention management. Responsible nurses assessed patients’ VTE risk using the Caprini Risk Assessment Model,21,22 physicians prescribed prophylactic measures based on assessment results, and nurses provided routine health education.
Intervention Group
The intervention group received grid-based information management in addition to traditional management, comprising three core components:
(1) Three-tier grid management system: The hospital was divided into 10 secondary grid units based on specialty characteristics, establishing a nursing department (primary)-sector (secondary)-clinical unit (tertiary) three-tier grid management system. Three teams (management, expert, and quality control) were established vertically, spanning hospital, department cluster, and unit levels horizontally.
(2) Information technology integration for VTE prevention workflow: The 2017 Caprini Risk Assessment Model was embedded within the hospital information system.23 Responsible nurses completed assessments within 4 hours of admission, with automatic notification to physician workstations for confirmation within 2 hours. The system automatically generated risk stratification and displayed prophylaxis recommendations. Anticoagulant contraindication alerts and bleeding risk assessment prompts were integrated into the order entry system. A patient education module was developed within the hospital OA system, delivering content on graduated compression stockings, intermittent pneumatic compression devices, and ankle pump exercises through videos and graphics.
(3) Quality control monitoring: Core indicators including VTE risk assessment rate, assessment timeliness, assessment accuracy, prevention measure implementation rate, and VTE incidence were established. A self-developed quality control database enabled automatic indicator extraction, longitudinal trend analysis, cross-departmental comparison, and visual alerts, with monthly feedback and supervision by the quality control team.
Instruments
VTE Prevention Knowledge Questionnaire
The VTE Prevention Knowledge Questionnaire was specifically developed for this study to assess nurses’ comprehensive understanding of VTE prevention. The questionnaire development followed a systematic process involving literature review of current VTE prevention guidelines, semi-structured interviews with 15 clinical experts, and two rounds of Delphi consultation. The final 75-item questionnaire comprises six dimensions: VTE concepts (13 items), risk factors (31 items), basic prevention methods (6 items), physical prevention methods (13 items), pharmacological prevention methods (5 items), and post-VTE nursing care (7 items). Each item is scored dichotomously (1 = correct, 0 = incorrect), yielding total scores ranging from 0 to 75, with higher scores indicating greater VTE prevention knowledge. The questionnaire demonstrated strong psychometric properties: Cronbach’s α coefficient was 0.907 with dimension-specific α values ranging from 0.812 to 0.889, and the scale-level content validity index (S-CVI) was 0.887. Exploratory factor analysis confirmed the six-factor structure, explaining 67.3% of the total variance (KMO = 0.836), and test-retest reliability demonstrated excellent temporal stability (ICC = 0.913, 95% CI: 0.821–0.958).
Departmental Collaboration Scale
The Departmental Collaboration Scale was specifically developed for this study to assess interprofessional collaboration and multi-departmental coordination in the context of VTE prevention within grid-based information management systems. The scale development followed a rigorous process involving literature review of existing collaboration instruments, semi-structured interviews with 12 clinical experts, and two rounds of Delphi consultation. The final scale comprises five items, each rated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree): (1) “Information regarding patients’ VTE risk levels is effectively shared and communicated among different departments involved in patient care”; (2) “When VTE prevention issues arise, relevant departments respond promptly and coordinate their efforts efficiently”; (3) “There are clear protocols and communication channels for interdepartmental consultation regarding VTE risk management”; (4) “Healthcare professionals from different disciplines collaborate effectively in developing and implementing VTE prevention plans”; and (5) “The grid-based management system facilitates seamless coordination between clinical departments and support services for VTE-related care.” The total score ranges from 5 to 25, with higher scores indicating better departmental collaboration. The scale demonstrated acceptable psychometric properties: Cronbach’s α coefficient was 0.856, item-total correlations ranged from 0.621 to 0.784, and exploratory factor analysis revealed a unidimensional structure explaining 64.7% of the total variance (KMO = 0.812, factor loadings: 0.68–0.85). Content validity was established through expert panel review with a scale-level content validity index (S-CVI/Ave) of 0.93, and criterion-related validity was confirmed by significant correlation with the Collaborative Practice Assessment Tool (r = 0.724, P < 0.001). Test-retest reliability in a subsample of 30 participants demonstrated excellent temporal stability (ICC = 0.891, 95% CI: 0.782–0.947).
System Usability Scale
The System Usability Scale (SUS)25 assessed information system usability. This 10-item instrument yields total scores from 0–100, with scores ≥68 indicating good usability.26
Outcome Measures
VTE events were defined as symptomatic, objectively confirmed deep vein thrombosis (DVT) or pulmonary embolism (PE). DVT was confirmed by compression ultrasonography or venography, and PE by computed tomography pulmonary angiography (CTPA) or ventilation-perfusion scanning. Routine screening imaging was not performed; imaging was clinically indicated only. Asymptomatic/incidental VTE was not included. Primary outcomes included: (1) VTE risk assessment indicators: completion rate, accuracy rate, and bleeding risk assessment completion rate; (2) Prevention measure implementation: basic prevention, physical prevention (graduated compression stockings, intermittent pneumatic compression device utilization), and pharmacological prevention implementation rates; (3) VTE incidence and VTE-related mortality; and (4) Process measures: ultrasound result waiting time and prevention measure implementation time.
Statistical Analysis
Descriptive and Comparative Analyses
Descriptive statistics and between-group comparisons were performed using SPSS 26.0. Continuous variables were expressed as mean ± standard deviation, with between-group comparisons using independent samples t-tests. Categorical variables were expressed as frequencies and percentages, with between-group comparisons using chi-square tests.
Johnson-Neyman Moderation Analysis
Moderation analysis was conducted using the PROCESS macro for SPSS (Model 1).27,28 The J-N technique was employed to identify regions of significance for the conditional effect of grid-based information management on VTE prevention outcomes across the range of moderator variables.29,30 The J-N technique solves for the values of the moderator at which the conditional effect of the focal predictor transitions between statistical significance and non-significance, providing a more comprehensive picture than traditional “pick-a-point” approaches.31 Statistical significance was set at α = 0.05.
Fuzzy-Set Qualitative Comparative Analysis
FsQCA was performed using fsQCA 3.0 software. Sample Size Justification for fsQCA: Although traditionally used with small-N cases, recent guidelines support larger-N applications.32,33 Our department-level analysis (n=10) meets minimum recommendations (10–15 cases), and the patient-level sample (n=119) provides sufficient diversity. Robustness checks with varying consistency thresholds (0.75–0.85) yielded stable results. Variables were calibrated into fuzzy-set membership scores (0–1) using the direct calibration method, with anchors set at the 95th percentile (full membership), 50th percentile (crossover point), and 5th percentile (full non-membership).34,35 Necessity analysis used a consistency threshold of ≥0.9.36 Sufficiency analysis employed frequency threshold of 1, raw consistency threshold of 0.80, and PRI consistency threshold of 0.70.37,38 The intermediate solution was reported following best practice guidelines.39,40
Results
Participant Characteristics
A total of 119 patients were enrolled, with 58 in the control group and 61 in the intervention group. No significant differences were observed between groups in demographic characteristics, clinical variables, or baseline VTE risk (Table 1).
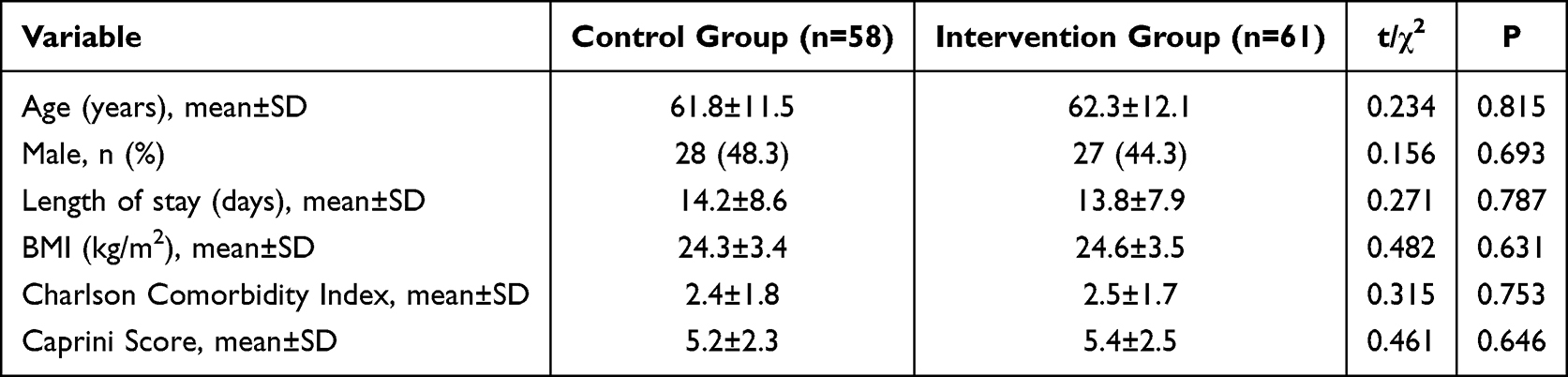 |
Table 1 Baseline Characteristics of Participants |
VTE Prevention Outcomes
The intervention group demonstrated significantly better VTE prevention outcomes across all indicators (Table 2). VTE risk assessment completion rate was significantly higher in the intervention group (86.9% vs 63.8%, χ2=8.462, P<0.01), as were assessment accuracy rate (83.6% vs 46.6%, χ2=18.234, P<0.01), bleeding risk assessment completion rate (91.8% vs 36.2%, χ2=40.125, P<0.01), and prevention measure implementation rate (90.2% vs 58.6%, χ2=15.623, P<0.01). VTE incidence was significantly lower in the intervention group (3.3% vs 8.6%, χ2=4.580, P=0.032). Absolute risk reduction: 5.3% (95% CI 0.4–10.2%), NNT=19 (95% CI 10–250). Process measures also improved significantly, with reduced ultrasound waiting time (87.1±24.3 vs 162.0±38.5 minutes, t=12.845, P<0.01) and prevention measure implementation time (52.0±18.6 vs 116.5±33.2 minutes, t=13.127, P<0.01).
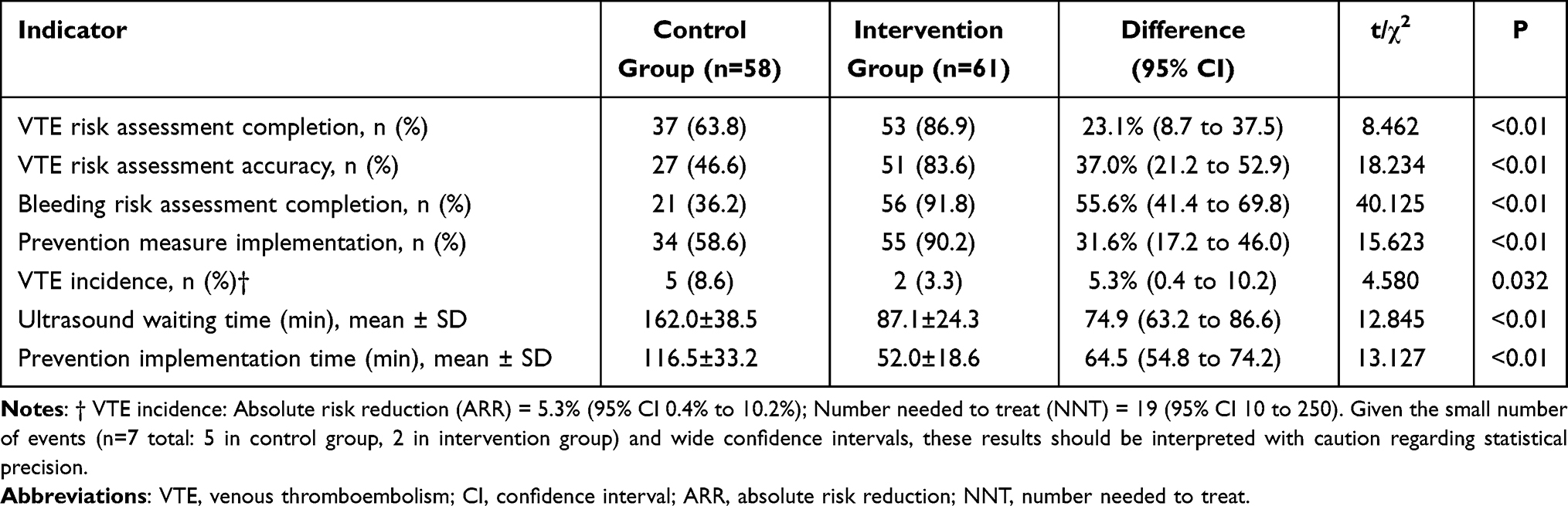 |
Table 2 Comparison of VTE Prevention Outcomes Between Groups |
Johnson-Neyman Moderation Analysis
Moderating Effect of Nurses’ VTE Knowledge
A moderation model was constructed with grid-based information management implementation as the independent variable (X), VTE risk assessment completion rate as the dependent variable (Y), and nurses’ VTE knowledge score as the moderator (M). The interaction term (X×M) significantly predicted Y (β=0.023, SE=0.008, t=2.875, P<0.01), indicating that nurses’ VTE knowledge moderated the relationship between grid-based information management and VTE risk assessment rate.
The J-N technique identified the boundary of the region of significance. When nurses’ VTE knowledge score was below 42 points, the conditional effect of grid-based information management on VTE risk assessment rate was 0.089 (95% CI: −0.012 to 0.190), which was not statistically significant (P>0.05). When knowledge scores reached or exceeded 42 points, the conditional effect ranged from 0.156 to 0.312 and was statistically significant (P<0.05), with the effect strengthening as knowledge levels increased (Figure 1).
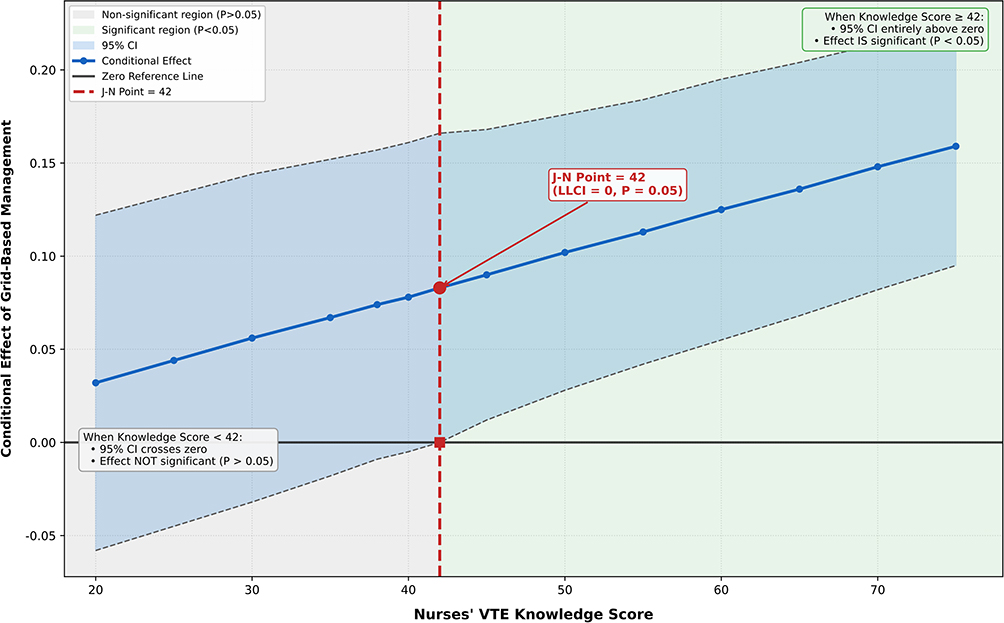 |
Figure 1 Johnson-Neyman Plot for the Moderating Effect of Nurses’ VTE Knowledge. |
Moderating Effect of Departmental Collaboration
A second moderation model was constructed with departmental collaboration score as the moderator, and prevention measure implementation rate as the dependent variable. The interaction term was significant (β=0.185, SE=0.056, t=3.304, P<0.01), indicating that departmental collaboration moderated the relationship between grid-based information management and prevention measure implementation.
J-N analysis revealed that when departmental collaboration score was below 3.4 points, the conditional effect of grid-based information management on prevention measure implementation was not statistically significant (P>0.05). When collaboration scores reached or exceeded 3.4 points, the effect was significant (P<0.05) (Figure 2).
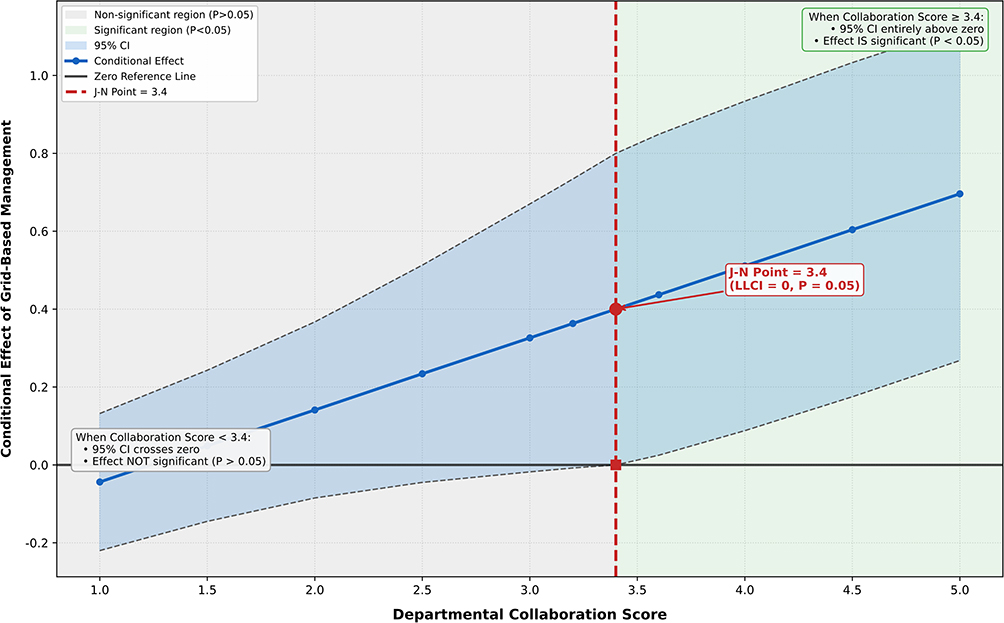 |
Figure 2 Johnson-Neyman Plot for the Moderating Effect of Departmental Collaboration. |
Fuzzy-Set Qualitative Comparative Analysis
Variable Calibration
Raw data were calibrated into fuzzy-set membership scores. The VTE prevention composite score (weighted combination of assessment rate, prevention rate, and inverse VTE incidence) served as the outcome variable. Six condition variables were included: grid system completeness, nurses’ knowledge level, departmental collaboration, information system usability, management support, and training investment. Calibration anchors are presented in Table 3.
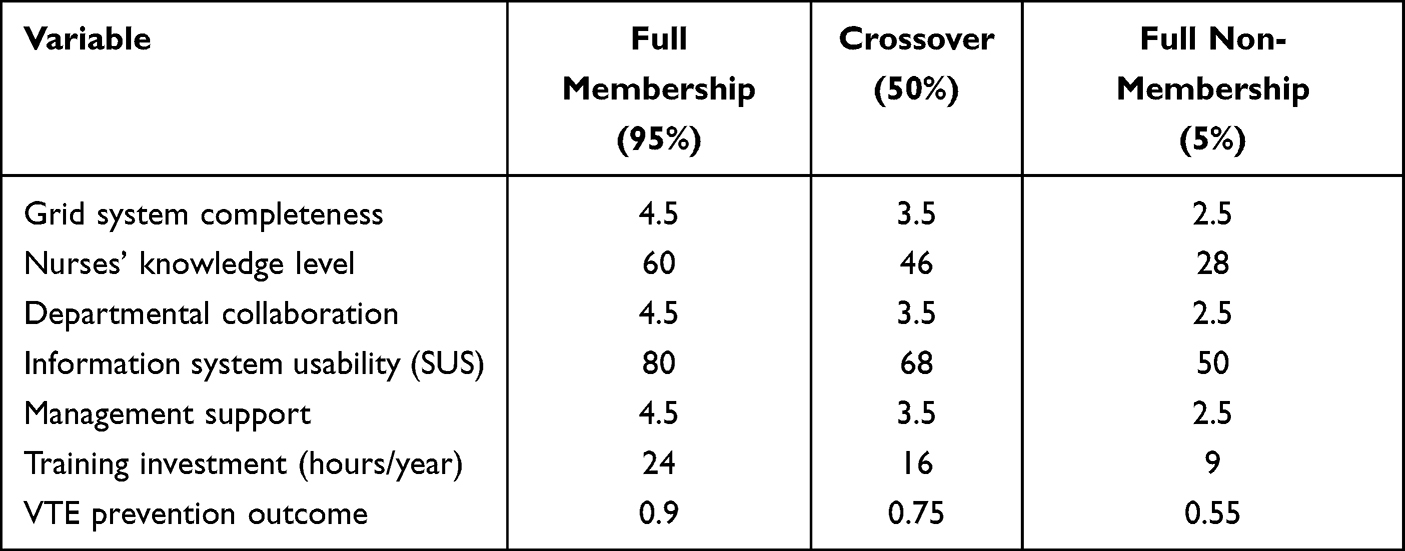 |
Table 3 Calibration Anchors for fsQCA Variables |
Necessity Analysis
Necessity analysis examined whether any single condition was necessary for high VTE prevention outcomes. Grid system completeness demonstrated a consistency of 0.924, exceeding the threshold of 0.9, indicating it constitutes a necessary condition for achieving high VTE prevention outcomes. All other conditions had consistency values below 0.9 and were not necessary conditions (Table 4).
 |
Table 4 Necessity Analysis Results |
Sufficiency Analysis
Truth table analysis identified three configurational pathways leading to high VTE prevention outcomes (Table 5).
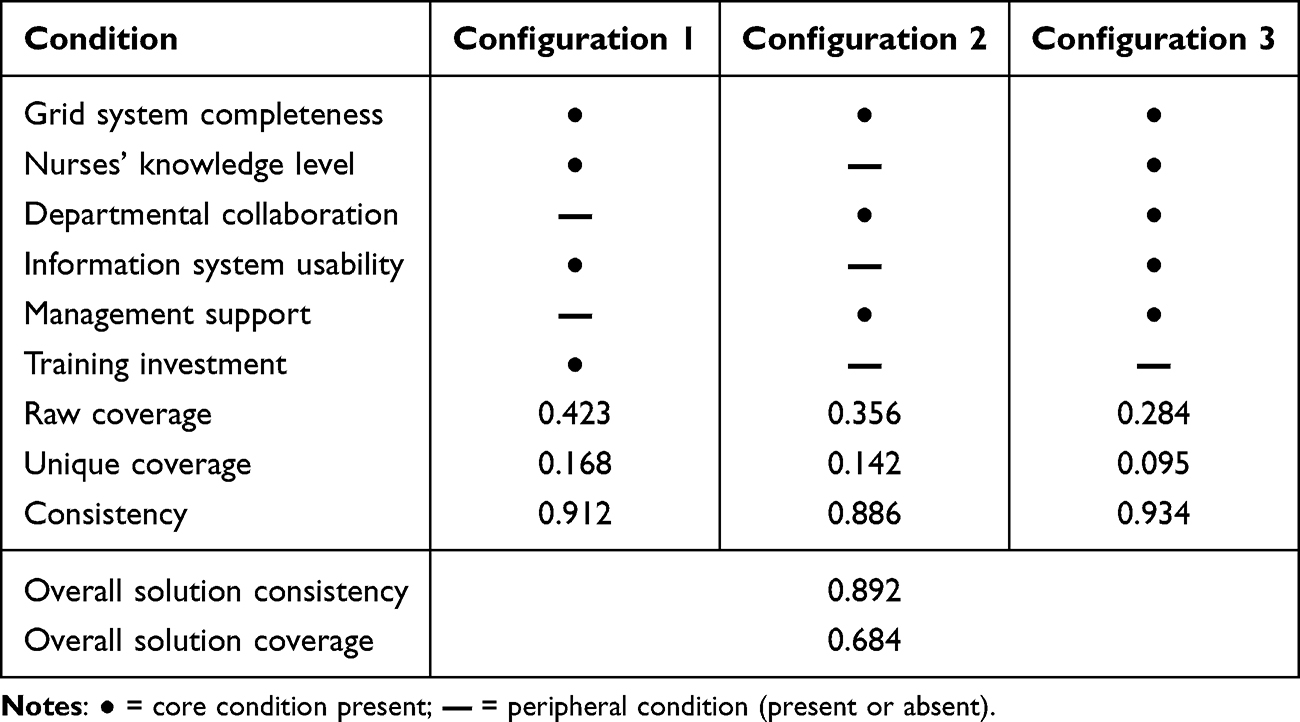 |
Table 5 Configurational Pathways for High VTE Prevention Outcomes |
Configuration 1 (Technology-driven pathway): Grid system completeness × High nurses’ knowledge × High system usability × High training investment. This pathway emphasizes achieving effective prevention through comprehensive technical support and personnel capacity building. It demonstrated the highest raw coverage (0.423), representing the most common pathway.
Configuration 2 (Collaboration-driven pathway): Grid system completeness × Strong departmental collaboration × High management support. This pathway emphasizes the importance of organizational collaboration and management commitment. Even when nurses’ knowledge and information system conditions are not optimal, effective prevention can be achieved through strong collaborative mechanisms and management support.
Configuration 3 (Comprehensive support pathway): All core conditions present. This pathway demonstrated the highest consistency (0.934), representing the ideal state where all conditions are optimally present. However, its unique coverage was lowest, indicating substantial overlap with other configurations.
Discussion
Effectiveness of Grid-Based Information Management in VTE Prevention
The present study demonstrated that grid-based information management significantly improved VTE risk assessment completion rates, prevention measure implementation rates, and reduced VTE incidence, consistent with previous research on clinical decision support systems for VTE prevention.41,42 Several mechanisms may explain these findings. First, the three-tier grid management system breaks down traditional departmental silos, enabling hospital-wide coordination and resource integration for VTE prevention.43 Second, the information technology integration embeds assessment, alerting, intervention, and feedback processes into routine workflows, reducing human error and omissions.44,45 Third, the visual quality monitoring and early warning mechanisms facilitate continuous quality improvement.46 These findings align with the substantial body of evidence supporting electronic decision support for VTE prophylaxis. Streiff et al reported that mandatory computerized VTE risk assessment significantly improved prophylaxis rates and reduced preventable VTE.44 Similarly, systematic reviews have demonstrated that clinical decision support systems effectively improve VTE prophylaxis adherence, particularly when integrated into electronic health records with mandatory completion requirements.47–49
Nurses’ VTE Knowledge as a Boundary Condition
The J-N analysis revealed that a nurses’ VTE knowledge score of 42 points represents a critical boundary condition. When knowledge scores fall below this threshold, the positive effect of grid-based information management on VTE risk assessment is not statistically significant. This finding carries important practical implications: the effectiveness of information technology tools depends on users’ professional competence. Nurses with insufficient knowledge may be unable to effectively utilize the assessment tools and warning information provided by the system.50,51
This finding resonates with broader literature on the implementation of clinical decision support systems. Kawamoto et al identified that CDSS effectiveness is contingent upon integration with clinical workflow and the provision of recommendations rather than mere assessments.50 Our study extends this understanding by identifying specific knowledge thresholds below which technological interventions fail to demonstrate effectiveness. Healthcare organizations implementing grid-based information management should therefore prioritize systematic VTE knowledge training to ensure nurses’ competence reaches or exceeds this critical threshold before system implementation.52,53
The fsQCA results corroborate this finding, with nurses’ knowledge level appearing as a core condition in both the technology-driven and comprehensive support pathways. This convergence of findings from two distinct analytical approaches strengthens the evidence for the central role of nurses’ knowledge in VTE prevention effectiveness.
Achieving a nurses’ VTE knowledge score of ≥42 points is feasible through targeted educational initiatives. Structured training programs lasting 8–12 hours, incorporating both didactic instruction and case-based discussions on VTE pathophysiology, risk assessment, and prevention strategies, can effectively bridge knowledge gaps. Regular use of the validated VTE Prevention Knowledge Questionnaire for pre- and post-training evaluation, combined with quarterly competency assessments and remedial sessions for lower-scoring nurses, provides a sustainable approach to maintaining this threshold. Notably, in the present study, 68% of nurses attained this level following routine training, suggesting that the required competency is attainable with reasonable institutional investment in professional development.
Multiple Equifinal Pathways to High VTE Prevention Outcomes
The fsQCA identified three configurational pathways leading to high VTE prevention outcomes, demonstrating the complexity of causal relationships and the diversity of effective implementation approaches. Notably, grid system completeness appeared as a core condition in all configurations, validating its status as a necessary condition. The identification of multiple equifinal pathways provides important practical guidance. The collaboration-driven pathway suggests that for healthcare organizations with limited nurses’ knowledge reserves or suboptimal information system conditions, strengthening departmental collaboration and securing management support can compensate for these limitations while still achieving good prevention outcomes. The existence of multiple pathways provides healthcare organizations with flexibility in implementation strategy selection based on their specific resource endowments: organizations with strong technical infrastructure may pursue the technology-driven pathway, while those with strong organizational coordination capabilities may pursue the collaboration-driven pathway. Reaching a departmental collaboration score of ≥3.4 points can be supported by establishing structured interdisciplinary mechanisms. Forming dedicated VTE prevention committees with representatives from nursing, medicine, pharmacy, and quality improvement teams, alongside the adoption of standardized communication tools such as SBAR for VTE-related consultations, fosters more effective teamwork. Regular interdisciplinary case reviews and audits, monitored through the validated Departmental Collaboration Scale, further reinforce these efforts. In our intervention group, 60% of departments achieved this threshold through such measures, indicating that meaningful collaboration is realistic without requiring extraordinary organizational resources.
Complementary Value of J-N Analysis and fsQCA
This study combined J-N moderation analysis with fsQCA, achieving methodological complementarity and triangulation. J-N analysis, from a “net effects” perspective, precisely identified moderator thresholds, addressing the question of “when” conditions are effective. FsQCA, from a “configurational effects” perspective, revealed the synergistic effects of condition combinations, addressing the question of “how” conditions combine to be effective.
The conclusions from both methods mutually reinforce each other: J-N analysis identified nurses’ knowledge level as a key boundary condition, while fsQCA showed it as a core condition in most high-effectiveness configurations. J-N analysis identified the threshold for departmental collaboration, while fsQCA demonstrated its core role in the collaboration-driven pathway. This methodological combination provides a new approach for investigating the impact mechanisms of complex interventions.
Temporal Bias and Study Design Considerations
The quasi-experimental before-after design is susceptible to temporal confounding, including seasonal variations, changes in clinical practice, or system maturation effects. We conducted sensitivity checks: (1) no significant seasonal VTE variation (P=0.89 across quarters); (2) stable performance after initial implementation month; and (3) no significant baseline differences (Table 1). Nevertheless, unmeasured time-varying factors cannot be fully excluded, and improvements may partly reflect cumulative experience. Results should be interpreted cautiously, with confirmatory RCTs warranted.
Limitations
Several limitations should be acknowledged. First, the convenience sampling approach and single-center design may limit generalizability; multi-center validation studies are warranted. Second, while fsQCA requires a minimum number of cases, the department-level case count in this study was relatively limited; future research should expand the sample size. Third, this study did not assess cost-effectiveness, resource utilization, or nursing workload changes associated with implementation. Future studies should include health economic analyses.
Conclusions
This study employed a mixed-methods approach combining J-N moderation analysis and fsQCA to investigate the impact mechanism of grid-based information management on VTE prevention outcomes. The findings indicate that: (1) Grid-based information management significantly improves VTE risk assessment and prevention measure implementation rates while reducing VTE incidence; (2) Nurses’ VTE knowledge level and departmental collaboration are critical boundary conditions for intervention effectiveness, with thresholds at 42 points and 3.4 points, respectively; (3) Three equifinal pathways exist for achieving high VTE prevention outcomes—technology-driven, collaboration-driven, and comprehensive support pathways—enabling healthcare organizations to select appropriate strategies based on their specific conditions. However, given the quasi-experimental design and single-center setting, multicenter randomized controlled trials are needed to confirm these boundary conditions and configurational pathways across diverse settings.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This study was approved by the Shanghai Changhai Hospital (First Affiliated Hospital of Naval Medical University) Ethics Committee (approval number: CHEC2023-109). The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent for Publication
All participants signed informed consent regarding publishing their data.
Funding
This work was supported by the 2023 Scientific Research Development Program of North Sichuan Medical College, Key Cultivation Project in Philosophy and Social Sciences (Project No. CBY23-ZDB04), entitled “Construction of an Information-Based Grid Management Model for Thrombosis Prevention and Control”.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Heit JA. Epidemiology of venous thromboembolism. Nat Rev Cardiol. 2015;12(8):464–12. doi:10.1038/nrcardio.2015.83
2. Wendelboe AM, Raskob GE. Global Burden of Thrombosis: epidemiologic Aspects. Circ Res. 2016;118(9):1340–1347. doi:10.1161/CIRCRESAHA.115.306841
3. Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41(4):543–603. doi:10.1093/eurheartj/ehz405
4. Nicholson M, Chan N, Bhagirath V, Ginsberg J. Prevention of Venous Thromboembolism in 2020 and Beyond. J Clin Med. 2020;9(8):2467. doi:10.3390/jcm9082467
5. Kahn SR, Panju A, Geerts W, et al. Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada. Thromb Res. 2007;119(2):145–155. doi:10.1016/j.thromres.2006.01.011
6. Cohen AT, Tapson VF, Bergmann JF, et al. Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross-sectional study. Lancet. 2008;371(9610):387–394. doi:10.1016/S0140-6736(08)60202-0
7. Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352(10):969–977. doi:10.1056/NEJMoa041533
8. Durieux P, Nizard R, Ravaud P, Mounier N, Lepage E. A clinical decision support system for prevention of venous thromboembolism: effect on physician behavior. JAMA. 2000;283(21):2816–2821. doi:10.1001/jama.283.21.2816
9. Galanter WL, Thambi M, Rosencranz H, et al. Effects of clinical decision support on venous thromboembolism risk assessment, prophylaxis, and prevention at a university teaching hospital. Am J Health Syst Pharm. 2010;67(15):1265–1273. doi:10.2146/ajhp090575
10. Maynard G, Stein J. Designing and implementing effective venous thromboembolism prevention protocols: lessons from collaborative efforts. J Thromb Thrombolysis. 2010;29(2):159–166. doi:10.1007/s11239-009-0405-4
11. Borab ZM, Lanni MA, Tecce MG, et al. Use of computerized clinical decision support systems to prevent venous thromboembolism in surgical patients: a systematic review and meta-analysis. JAMA Surg. 2017;152(7):638–645. doi:10.1001/jamasurg.2017.0131
12. Karajizadeh M, Hassanipour S, Sharifian R, et al. The effect of information technology intervention on using appropriate VTE prophylaxis in non-surgical patients: a systematic review and meta-analysis. Digit Health. 2022;8:20552076221118828. doi:10.1177/20552076221118828
13. Liao L. Grid information management innovation of government in the era of big data.
14. Flanders SA, Greene MT, Grant P, et al. Hospital performance for pharmacologic venous thromboembolism prophylaxis and rate of venous thromboembolism: a cohort study. JAMA Intern Med. 2014;174(10):1577–1584. doi:10.1001/jamainternmed.2014.3384
15. Tsaftaridis N, Goldin M, Spyropoulos AC. System-wide thromboprophylaxis interventions for hospitalized patients at risk of venous thromboembolism: focus on cross-platform clinical decision support. J Clin Med. 2024;13(7):2133. doi:10.3390/jcm13072133
16. Johnson PO, Neyman J. Tests of certain linear hypotheses and their applications to some educational problems. Stat Res Mem. 1936;1:57–93.
17. Bauer DJ, Curran PJ. Probing Interactions in Fixed and Multilevel Regression: inferential and Graphical Techniques. Multivariate Behav Res. 2005;40(3):373–400. doi:10.1207/s15327906mbr4003_5
18. Carden SW, Holtzman NS, Strube MJ. CAHOST: an Excel Workbook for Facilitating the Johnson-Neyman Technique for Two-Way Interactions in Multiple Regression. Front Psychol. 2017;8:1293. doi:10.3389/fpsyg.2017.01293
19. Ragin CC. Redesigning Social Inquiry: Fuzzy Sets and Beyond. University of Chicago Press; 2008; doi:10.7208/chicago/9780226702797.001.0001
20. Ragin CC. The Comparative Method: Moving Beyond Qualitative and Quantitative Strategies. University of California Press; 1987.
21. Caprini JA. Thrombosis risk assessment as a guide to quality patient care. Dis Mon. 2005;51(2–3):70–78. doi:10.1016/j.disamonth.2005.02.003
22. Pannucci CJ, Bailey SH, Dreszer G, et al. Validation of the Caprini risk assessment model in plastic and reconstructive surgery patients. J Am Coll Surg. 2011;212(1):105–112. doi:10.1016/j.jamcollsurg.2010.08.018
23. Lobastov K, Urbanek T, Stepanov E, et al. The Thresholds of Caprini Score Associated With Increased Risk of Venous Thromboembolism Across Different Specialties: a Systematic Review. Ann Surg. 2023;277(6):929–937. doi:10.1097/SLA.0000000000005843
24. Le Sage S, McGee M, Emed JD. Knowledge of venous thromboembolism (VTE) prevention among hospitalized patients. J Vasc Nurs. 2008;26(4):109–117. doi:10.1016/j.jvn.2008.09.005
25. Brooke J. SUS: a quick and dirty usability scale. In: Jordan PW, Thomas B, Weerdmeester BA, McClelland IL, editors. Usability Evaluation in Industry. Taylor & Francis; 1996:189–194.
26. Bangor A, Kortum PT, Miller JT. An empirical evaluation of the System Usability Scale. Int J Hum Comput Interact. 2008;24(6):574–594. doi:10.1080/10447310802205776
27. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach.
28. Hayes AF, Montoya AK, Rockwood NJ. The analysis of mechanisms and their contingencies: PROCESS versus structural equation modeling. Australas Mark J. 2017;25(1):76–81. doi:10.1016/j.ausmj.2017.02.001
29. Preacher KJ, Curran PJ, Bauer DJ. Computational tools for probing interactions in multiple linear regression, multilevel modeling, and latent curve analysis. J Educ Behav Stat. 2006;31(4):437–448. doi:10.3102/10769986031004437
30. Spiller SA, Fitzsimons GJ, Jg L Jr, McClelland GH. Spotlights, floodlights, and the magic number zero: simple effects tests in moderated regression. J Mark Res. 2013;50(2):277–288. doi:10.1509/jmr.12.0420
31. Hayes AF. Moderation analysis in two-instance repeated measures designs: probing methods and multiple moderator models. Behav Res Methods. 2019;51(1):61–82. doi:10.3758/s13428-018-1088-6
32. Fiss PC. Building better causal theories: a fuzzy set approach to typologies in organization research. Acad Manage J. 2011;54(2):393–420. doi:10.5465/amj.2011.60263120
33. Schneider CQ, Wagemann C. Set-Theoretic Methods for the Social Sciences: A Guide to Qualitative Comparative Analysis. Cambridge University Press; 2012.
34. Greckhamer T, Misangyi VF, Fiss PC. The two QCAs: from a small-N to a large-N set theoretic approach. In: Configurational Theory and Methods in Organizational Research. Emerald Group Publishing; 2013:49–75. doi:10.1108/S0733-558X(2013)0000038007
35. Misangyi VF, Greckhamer T, Furnari S, et al. Embracing causal complexity: the emergence of a neo-configurational perspective. J Manage. 2017;43(1):255–282. doi:10.1177/0149206316679252
36. Ragin CC. Set relations in social research: evaluating their consistency and coverage. Polit Anal. 2006;14(3):291–310. doi:10.1093/pan/mpj019
37. Pappas IO, Woodside AG. Fuzzy-set qualitative comparative analysis (fsQCA): guidelines for research practice in information systems and marketing. Int J Inf Manage. 2021;58:102310. doi:10.1016/j.ijinfomgt.2021.102310
38. Greckhamer T, Furnari S, Fiss PC, Aguilera RV. Studying configurations with qualitative comparative analysis: best practices in strategy and organization research. Strateg Organ. 2018;16(4):482–495. doi:10.1177/1476127018786487
39. Thomann E, Maggetti M. Designing research with qualitative comparative analysis (QCA): approaches, challenges, and tools. Sociol Methods Res. 2020;49(2):356–386. doi:10.1177/0049124117729700
40. Bauernschmidt D, Wittmann J, Hirt J, Meyer G, Bieber A. Applying qualitative comparative analysis in a systematic review: lessons learned. Z Evid Fortbild Qual Gesundhwes. 2025;196:82–86. doi:10.1016/j.zefq.2025.03.013
41. Haut ER, Lau BD, Kraenzlin FS, et al. Improved prophylaxis and decreased rates of preventable harm with the use of a mandatory computerized clinical decision support tool for prophylaxis for venous thromboembolism in trauma. Arch Surg. 2012;147(10):901–907. doi:10.1001/archsurg.2012.2024
42. Titi MA, Alotair HA, Fayed A, et al. Effects of computerised clinical decision support on adherence to VTE prophylaxis clinical practice guidelines among hospitalised patients. Int J Qual Health Care. 2021;33(1):mzab034. doi:10.1093/intqhc/mzab034
43. Maynard GA, Morris TA, Jenkins IH, et al. Optimizing prevention of hospital-acquired venous thromboembolism (VTE): prospective validation of a VTE risk assessment model. J Hosp Med. 2010;5(1):10–18. doi:10.1002/jhm.562
44. Streiff MB, Lau BD, Hobson DB, et al. The Johns Hopkins Venous Thromboembolism Collaborative: multidisciplinary team approach to achieve perfect prophylaxis. J Hosp Med. 2016;11(2):S8–S14. doi:10.1002/jhm.2657
45. Lau BD, Streiff MB, Pronovost PJ, Haut ER. Venous Thromboembolism Quality Measures Fail to Accurately Measure Quality. Circulation. 2018;137(12):1278–1284. doi:10.1161/CIRCULATIONAHA.116.026897
46. Michtalik HJ, Carolan HT, Haut ER, et al. Use of provider-level dashboards and pay-for-performance in venous thromboembolism prophylaxis. J Hosp Med. 2015;10(3):172–178. doi:10.1002/jhm.2303
47. Grant PJ, Greene MT, Chopra V, Bernstein SJ, Hofer TP, Flanders SA. Assessing the Caprini Score for Risk Assessment of Venous Thromboembolism in Hospitalized Medical Patients. Am J Med. 2016;129(5):528–535. doi:10.1016/j.amjmed.2015.10.027
48. Kahn SR, Lim W, Dunn AS, et al. Prevention of VTE in nonsurgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e195S–e226S. doi:10.1378/chest.11-2296
49. Lester W, Freemantle N, Begaj I, et al. Fatal venous thromboembolism associated with hospital admission: a cohort study to assess the impact of a national risk assessment target. Heart. 2013;99(23):1734–1739. doi:10.1136/heartjnl-2013-304479
50. Kawamoto K, Houlihan CA, Balas EA, Lobach DF. Improving clinical practice using clinical decision support systems: a systematic review of trials to identify features critical to success. BMJ. 2005;330(7494):765. doi:10.1136/bmj.38398.500764.8F
51. Jaspers MW, Smeulers M, Vermeulen H, Peute LW. Effects of clinical decision-support systems on practitioner performance and patient outcomes: a synthesis of high-quality systematic review findings. J Am Med Inform Assoc. 2011;18(3):327–334. doi:10.1136/amiajnl-2011-000094
52. Barbar S, Noventa F, Rossetto V, et al. A risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism: the Padua Prediction Score. J Thromb Haemost. 2010;8(11):2450–2457. doi:10.1111/j.1538-7836.2010.04044.x
53. Sachdeva A, Dalton M, Lees T. Graduated compression stockings for prevention of deep vein thrombosis. Cochrane Database Syst Rev. 2018;11(11):CD001484. doi:10.1002/14651858.CD001484.pub4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.