Back to Journals » Risk Management and Healthcare Policy » Volume 15
What Kind of Interventions Were Perceived as Effective Against Coronavirus-19 in Nursing Homes in Italy? A Descriptive Qualitative Study
Authors Palese A ![]() , Chiappinotto S
, Chiappinotto S ![]() , Peghin M
, Peghin M ![]() , Marin M, Turello D, Caporale D, Tascini C
, Marin M, Turello D, Caporale D, Tascini C
Received 7 June 2022
Accepted for publication 15 August 2022
Published 21 September 2022 Volume 2022:15 Pages 1795—1808
DOI https://doi.org/10.2147/RMHP.S377249
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Alvisa Palese,1 Stefania Chiappinotto,1 Maddalena Peghin,2 Meri Marin,3 David Turello,3 Denis Caporale,3 Carlo Tascini2
1Department of Medical Science, University of Udine, Udine, Italy; 2Division of Infectious Diseases, Department of Medicine, University of Udine, Udine, Italy; 3Azienda Sanitaria Universitaria Friuli Centrale, Udine, Italy
Correspondence: Alvisa Palese, Department of Medical Sciences, University of Udine, Udine, 33100, Italy, Tel +39(0)432 590926, Fax +39(0)432 507715, Email [email protected]
Purpose: To identify interventions implemented during the first, second and third waves of the Coronavirus disease 2019 (COVID-19) among Italian Nursing Homes (NHs).
Patients and Methods: A descriptive qualitative design according to COnsolidated criteria for REporting Qualitative (COREQ) guideline. A purposeful sample of five public NHs, located in the north-east of Italy, equipped with from 60 to 151 beds, participated. Six nurse managers, four clinical nurses and one NH director were interviewed in depth at the end of 2021. These interviews were audio-recorded and then transcribed verbatim. A qualitative content analysis was performed to identify effective interventions as perceived by participants to protect facilities and residents from the pandemic.
Results: Three main sets of interventions have been applied, at the environmental, nurse staff and at the resident levels. Some have been enacted in all facilities, others in a few but in a homogeneous fashion, while other interventions have been implemented in some NHs also in contrast with available national or local recommendations.
Conclusion: Despite their documented frailty and precarious system, NHs implemented several interventions to protect their residents from the COVID-19. All interventions have been designed and implemented during the event, suggesting the need to increase the NHs’ preparedness to face future disasters. Regarding those interventions enacted in contrast to the recommendations or not homogeneously across NHs, future investigations are suggested to assess their actual effectiveness and accumulate evidence for the future.
Keywords: COVID-19, nursing homes, interventions, perceived effectiveness, qualitative study
Introduction
The older population has been documented as being at great vulnerability to Coronavirus disease 2019 (COVID-19)1 and at great risk of death,2 especially those living in long-term care facilities, such as Nursing Homes (NHs).3–5 Italy was the first western country to be hit by the pandemic and the most affected,6 with an enormous impact among NHs.7 In NHs, the limited space,4,8 the high concentration of frail older people, the multi-morbidity and dependence in daily living activities requiring multiple contacts by health care providers (HCPs) have been reported to increase the risk of COVID-19 infection. Moreover, the pre-existing shortages in nurses, the high turnover rates preventing the development of strong competences6 in infection prevention/control,9 exacerbated by delays in the availability of guidelines on addressing the pandemic,7 resulted in a greater diffusion of the virus. NH mortality rates have been documented to range from 0.5% (German) to 6.2% (Spain); however, in some Italian regions such as the Friuli Venezia Giulia (7.4%) and Lombardy (12.9%), the mortality rate was higher than in other European countries.7,10,11 At the national level, among the general population, since the beginning of the pandemic to the end of January 2022, a total mortality in excess of 178,000 deaths has been documented, compared to that reported in 2015–2019 years, mainly due to the increased deaths among the older people aged >80.11 Specifically, in the Friuli Venezia Giulia region, an excess of deaths of +9% during the first wave and of +45.6% during the second wave were recorded, as compared to the year before.12
Available literature has documented that NHs were unprepared to protect both residents and staff while providing adequate care due to insufficient resources and personal protective equipment (PPE), insufficient work training and to the inability to provide distancing or other adequate preventive measures.6,7 According to the increasing awareness of the NH issues, guidelines have been developed and disseminated across the country.13 Nevertheless, which concrete managerial actions have been implemented daily, translating the recommendations available and tailoring them to the NHs’ level, and deciding interventions according to the emerging needs in addition to or against the recommendations, has never been documented. In this context, the COVID-19 crisis has become an opportunity to broaden the knowledge of the NHs’ setting as they reacted to the pandemic during the successive waves.6 The implicit knowledge14 developed by NH managers undertaking several decisions with the intent to protect residents and staff might be an opportunity to gain insights and to expand our knowledge. Therefore, the aim of this study was to identify interventions implemented in Italian NHs during the first (March 2020), and up to the fourth wave (November 2021) of the COVID-19 pandemic and perceived as effective in preventing the spread of the virus among residents.
Materials and Methods
Study Design
A descriptive qualitative study design15 was performed in 2021 and reported here according to the COnsolidated criteria for REporting Qualitative research (COREQ) guideline.16
Setting and Participants
A purposeful sample17 of NHs in the Friuli Venezia Giulia region was chosen according to its capacity to identify key informants regarding the phenomenon of interest. Specifically, public NHs regulated by the Regional Health Service in the north-east of Italy were approached. To ensure a maximum sample variation,17 the five NHs were selected according to their ample diversity in the number of infected residents across the COVID-19 waves as well as in the different rates of mortality. All NHs contacted agreed to participate; their mission was homogeneous according to the regional rules, being devoted to older individuals with moderate-to-severe functional dependence in need of care and with different clinical conditions, mainly dementia.18 Moreover, these NHs ensured an average of 17 minutes of nursing care delivered by registered nurses (RNs) and 90 minutes by nursing aides (NAs)/day to each resident.
Given that, in Italy, the SARS-CoV-2 vaccination campaign started on 27th December 2020 and the priority was given to HCPs and older people, at the time of the interview, the second dose had been administered in all NHs, reaching a near-complete coverage.
In these settings, a purposeful sample17 of one director, six nurse managers, and four clinical nurses (hereinafter NMs) was identified with the support of the NH Directors and the Regional Health Service reference office. The following were eligible and included: (a) those occupying leadership and clinical positions and involved daily in translating the regional and national recommendations regarding the COVID-19 pandemic, tailoring them to the NH level, and who had the authority to introduce additional interventions according to the emerging needs; (b) those working in the same NH in all waves; and (c) those who were willing to participate. All NMs invited to participate agreed.
At the end of the data collection process, an additional NH was involved to perform the member checking19 aimed at assessing the saturation of the data collected. The mission of the additional facility, the rules followed as well as the amount of nursing care and residents’ profile was homogeneous with those NHs already involved.
The characteristics of the NH involved in the project are summarized in Table 1; the NM profile is reported in Table 2.
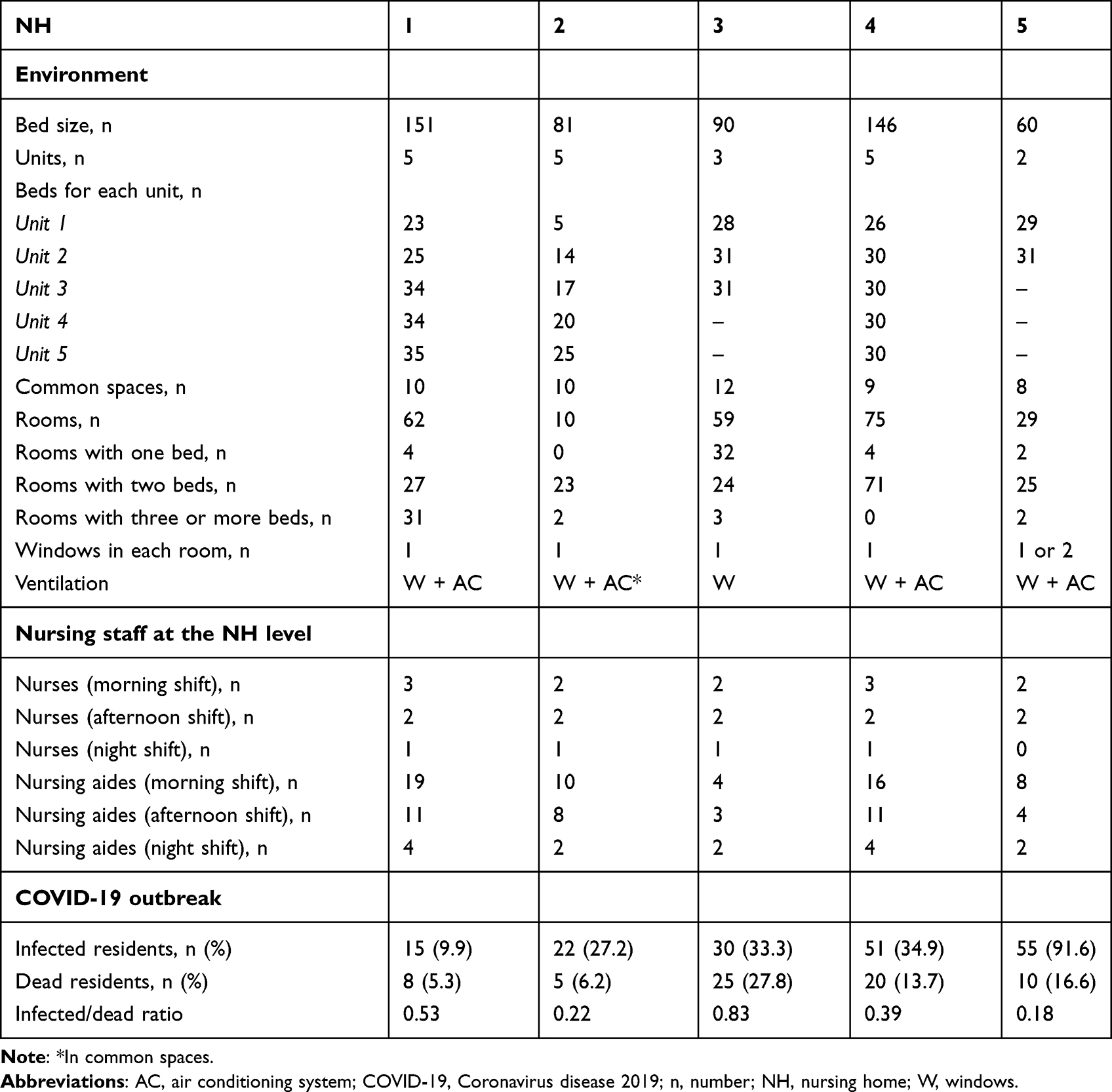 |
Table 1 Nursing Homes’ Profile |
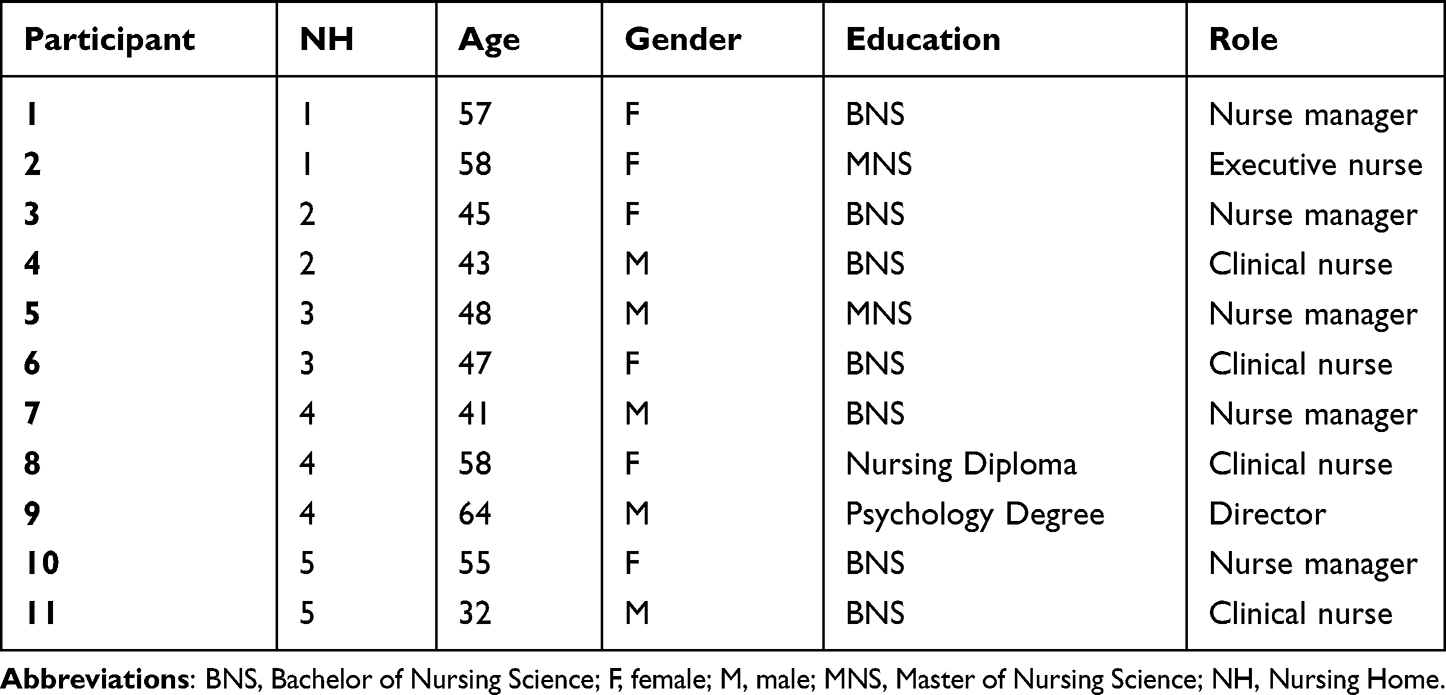 |
Table 2 Participants’ Profile |
Data Collection Process
An interview guide (Table 3) was developed in a preliminary fashion according to the evidence available.4,20–27 The data collection was performed in October–November 2021 by the same researcher (AP), educated at the advanced level, with experience in qualitative research and with no previous contacts with the NHs. The researcher contacted the NM(s) by sharing the main aims of the study and the questions by phone/email. The preliminarily contact was also the occasion to briefly present the profile of the researcher. Then, on the day and at the time preferred by the potential participants, in a calm environment facilitating interactions among participants without interruptions, the interviews were performed. During the interview, there were present only the researcher and the participants. The interviews lasted from 55 minutes to 115 minutes, and all were audio-recorded and then transcribed verbatim.
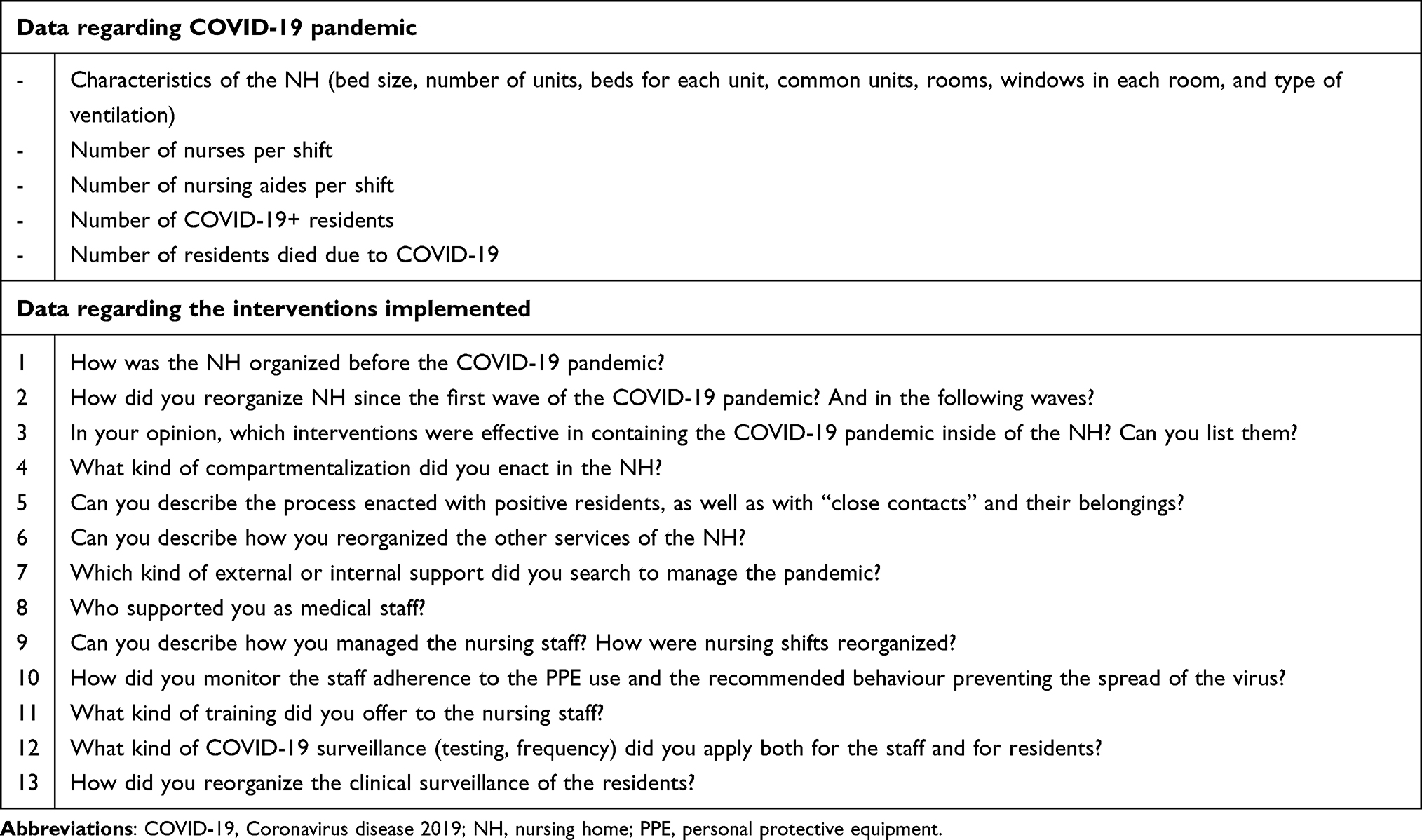 |
Table 3 Interview Guide |
Data Analysis
A content analysis17,28 was performed to identify the manifest interventions implemented and those implicit (as, for example, the decisions not immediately visible with actions). The data analysis process was performed by one researcher (AP) and then agreed by a second researcher (SC), who performed the same process in an independent fashion. Then, the research team (see authors) reached a consensus. Researchers put aside their preconceptions, and the interviews were anonymized to ensure the maximum flexibility needed to examine the phenomenon in its natural state and discover the tacit knowledge of NMs in dealing with the pandemic in NHs.14
The data analysis process conducted was the following:
- The verbatim transcriptions were read and reread carefully, and the first level of analysis was performed by identifying the meaning units (eg, sentences or words as expressed by participants with meaning).
- Then, each unit of meaning was coded, and a list of interventions started to emerge. The interventions were aggregated and categorised into themes according to their similarity and differences.
- The themes were organized according to the
(a) chronological order, according to when the interventions were implemented as narrated by participants, and
(b) the focus, from the broad context (environment) to the specific cases (the resident).
- After that, each intervention was checked in the guidelines available at the study time to assess their status (mandatory or recommended).13,29–31 Moreover, NHs providing the interventions were identified with a number in order to ensure anonymity (eg, “Avoiding common meals”, NH 1). Moreover, quotes were extracted to provide examples of the interventions implemented.
Strategies used to ensure rigour and trustworthiness have been summarized in Supplementary Table 1.
Results
Three main sets of interventions have been implemented by NHs over the waves to contrast the COVID-19 outbreak, at the environmental, nurse staff and resident levels (Table 4).
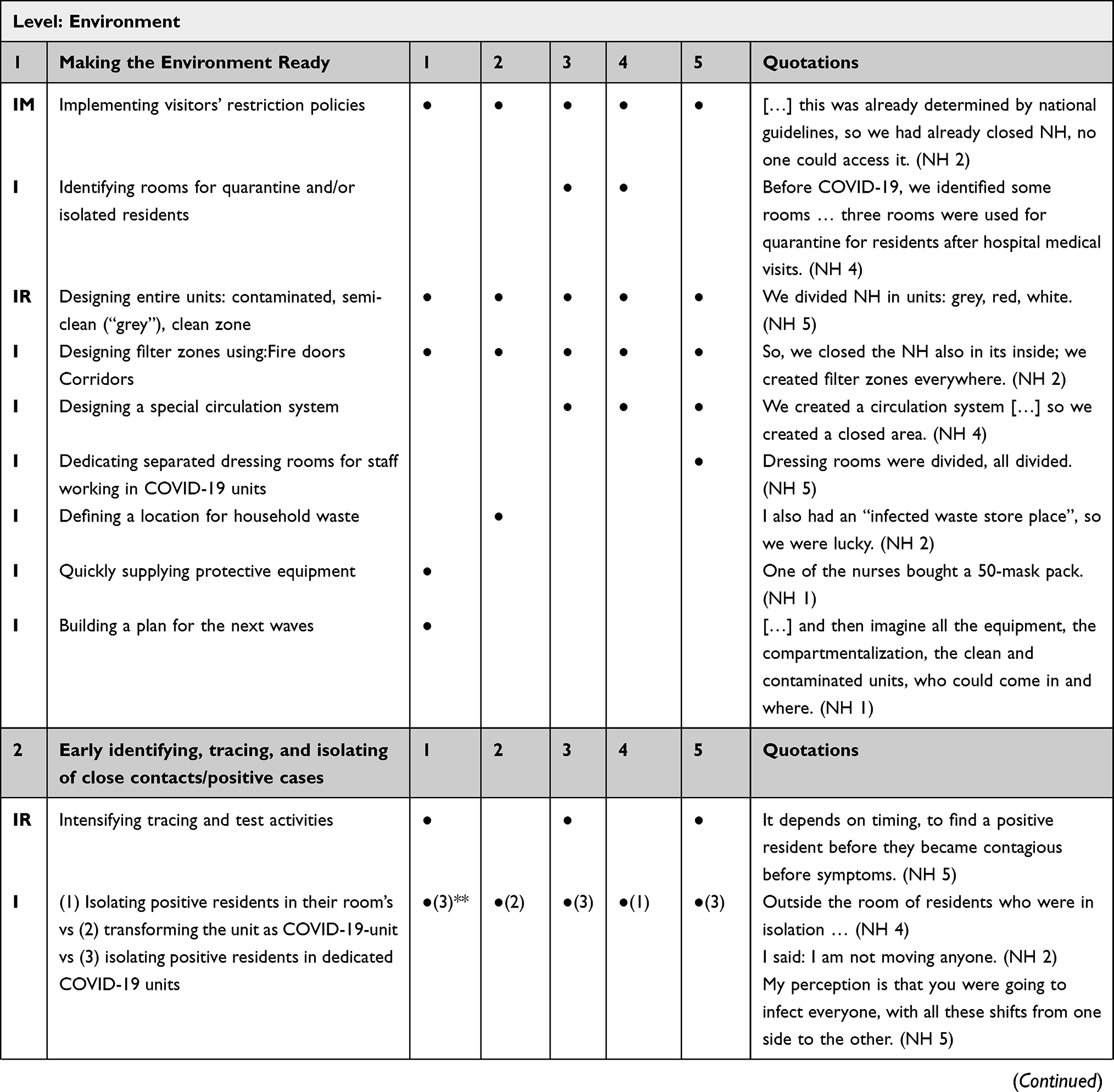 | 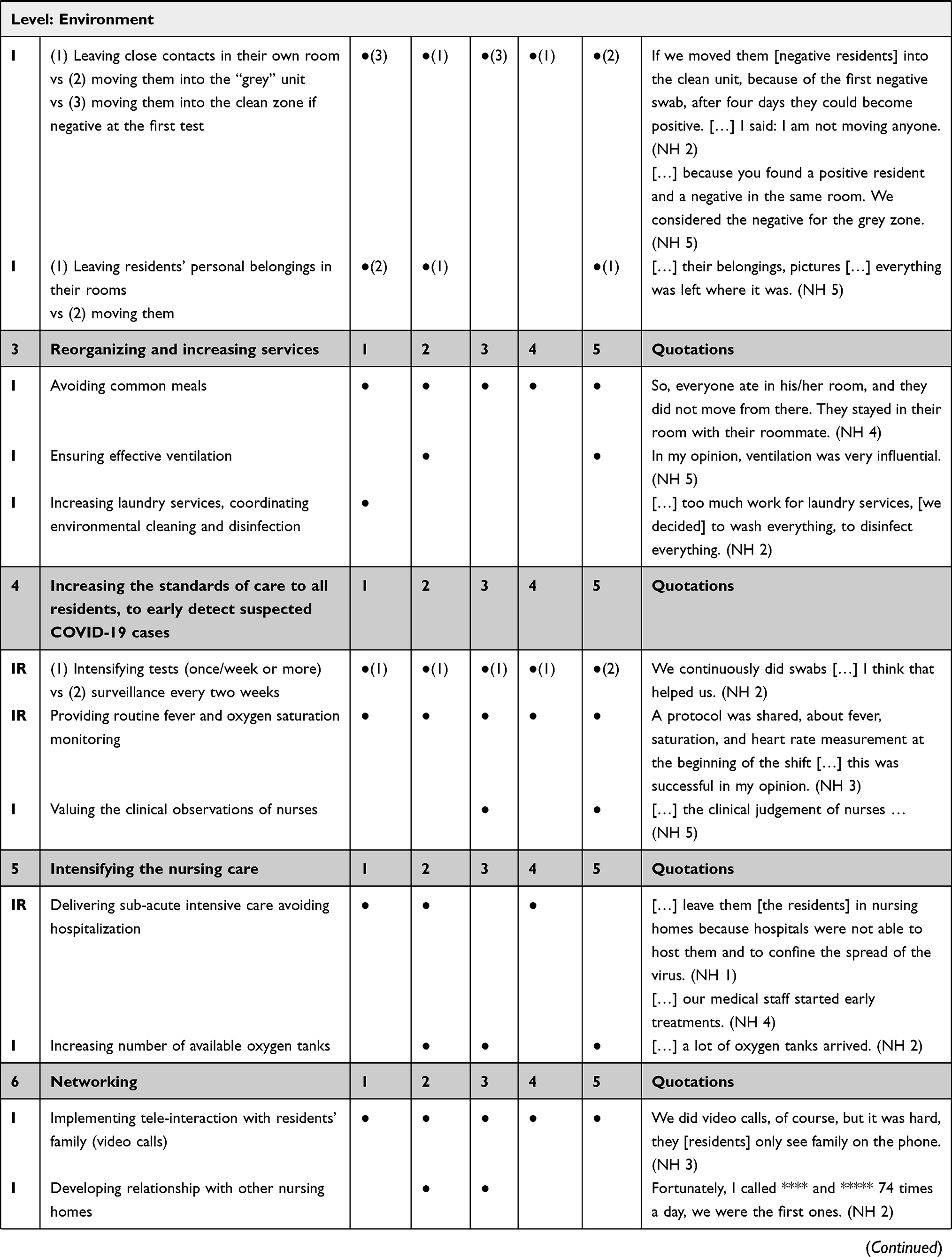 | 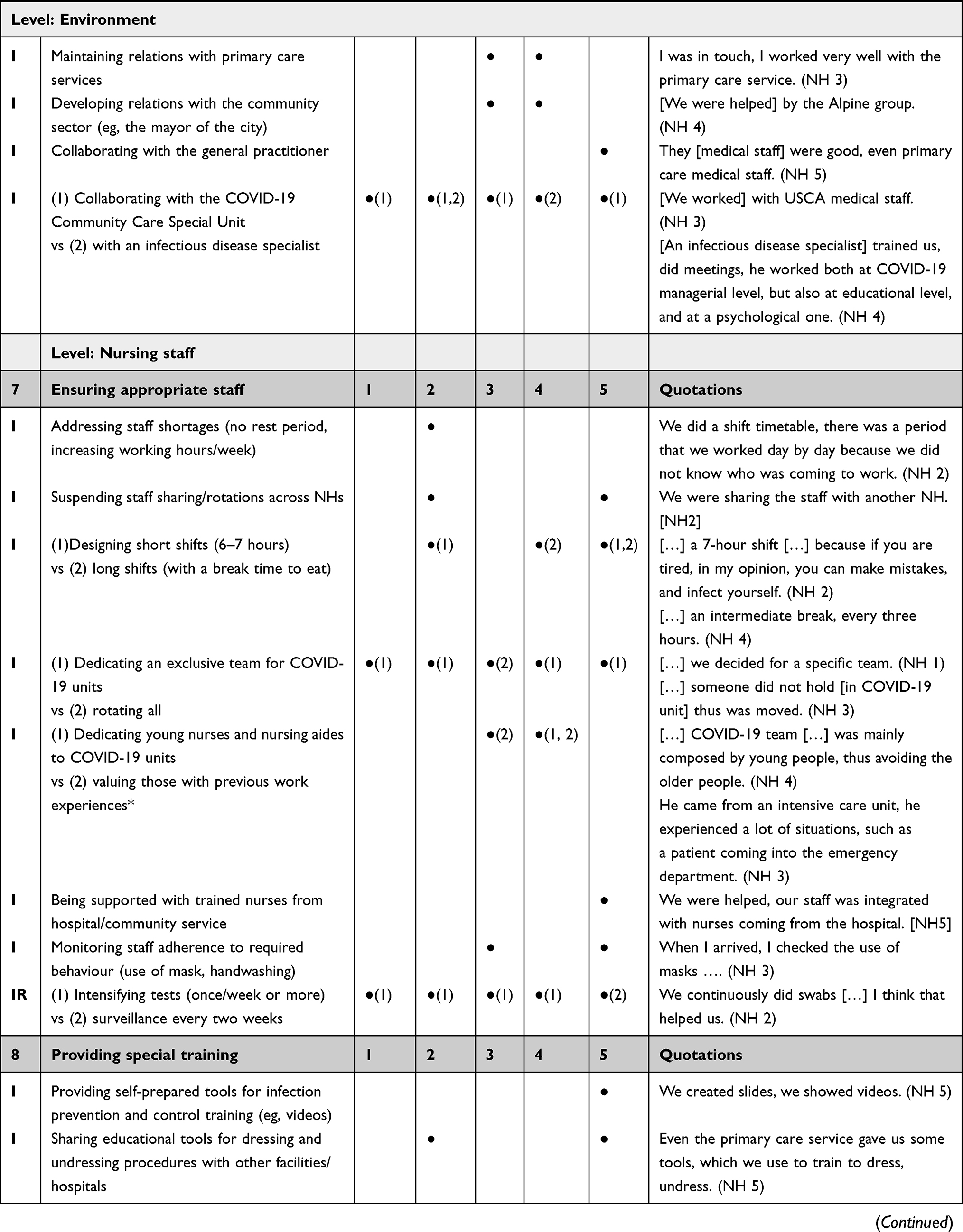 | 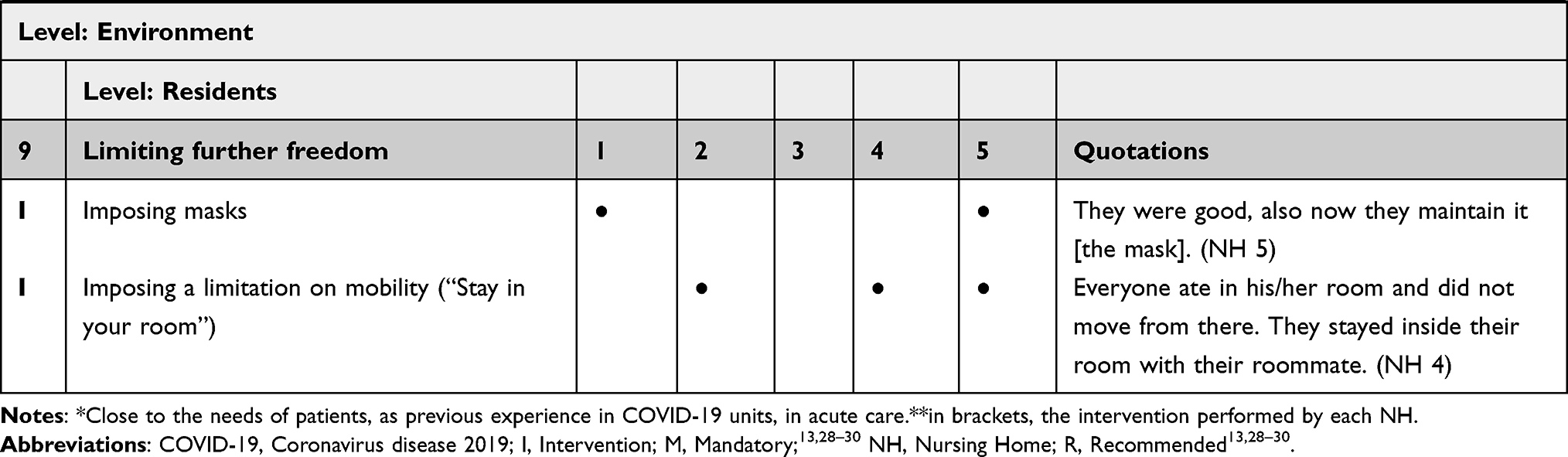 |
Table 4 Interventions Perceived as Effective |
Interventions at the Environment Level
Making the Environment Ready
The first interventions implemented were at environmental level, to prepare the facilities for the pandemic outbreak, to keep the virus out and to prevent its circulation inside. All NHs adopted severe visiting restriction policies, closing the environment to external access, according to the recommendations provided by authorities.13,29–31 This was felt to be a necessary decision to protect the NH and its residents from the virus circulating. Some NHs (3, 4) decided to dedicate some rooms for residents with suspected COVID-19 or to reserve these for preventive quarantine (NH 3) for those returning from hospital visits or discharges. However, at the outbreak of the pandemic inside the facility, all NHs compartmentalized the environment by dividing it into units to create clean, semi-clean and contaminated zones, according to guidelines.13,29–31 When possible, the same units of the NHs were used; when this was a challenge, the NHs transformed those units previously designed as closed, such as the areas devoted to patients with dementia. However, in one NH (1), based on a home-like approach, with several common places and open environments, the compartmentalization was a challenge.
NHs often use the fire doors (1, 2, 4, 5) or corridors (3) to ensure a compartmentalization of the units and the care processes. In the filter zones, the space was dedicated to staff to safely change into or out of their PPE (NHs 1, 2, 5). In an NH (3), where the nature of the environment prevented the creation of this space, an increased discomfort among the staff was reported.
After having redesigned the environment, a special circulation system pathway was created (NH 3, 4, 5), from clean to contaminated units, further decreasing the risk of spreading the infection, also including an exclusive staff dressing room for dedicated COVID-19 teams to protect HCPs at the end of the shift. In this context, an NH (2) even defined the location for infected wastes to prevent contamination of other areas.
Actions were taken to quickly supply PPE (NH 1) by collaborating with volunteers, mayors, and others to provide the equipment that was also promoted. The set of interventions designed in the first wave was then refined and refined again and implemented in the second, third and fourth waves as a sort of pandemic plan based on an inductive approach (NH 1).
Early Identifying, Tracing, and Isolating Close Contacts and/or Positive Cases
When the cases of positive and close contact residents appeared, some NHs (1, 3, 5) intensified the tracing activities, as recommended.13,29–31 On the other hand, NHs adopted opposite interventions that were also against the national rules. Three different interventions were adopted:
(a) one NH (4) isolated residents who tested in his/her room, without moving in the dedicated COVID-19 units; on the contrary
(b) one NH (2) transformed the entire unit into a COVID-19 unit, whereas
(c) the remaining NHs (1, 3, 5) transferred the resident to a dedicated COVID-19 unit.
Moreover, according to the underlying concept of “close contacts”, the interventions regarding the roommates were also different: specifically, when a resident was found positive at the swab, the roommate was identified as a “close contact” because they shared the same environment: consequently,
(a) some NHs (2, 4) decided to leave them in the same room with the positive roommate(s);
(b) other NHs (1, 3) moved them to clean units, if the swab was negative; lastly,
(c) a NH (5) used the “grey unit” for a few days after the first negative test, leaving them in as a sort of quarantine.
Residents’ belongings (eg, clothes and personal items) were also managed differently, with one NH (1) moving them to where the resident was moved, in the attempt to recreate his/her routine, whereas others (NHs 2, 5) left the belongings in the original room through to the end of the pandemic wave.
Reorganizing and Increasing Services
All services were immediately reorganized: meals in common areas were avoided in all NHs, and each resident ate in his/her room; moreover, common areas (eg, for physiotherapy therapies) were also closed. In one NH (2), disposable cutlery was provided. Attention was also given to appropriate ventilation, opening the windows more often (NH 5) and increasing inspections in the air-conditioning systems when available (NH 2). In one NH (1), the laundry services were used, and more coordination of the environmental cleaning and disinfection services was ensured, increasing the time devoted to these services, and promoting their coordination with the nursing care.
Increasing the Standards of Care to Early Detect Suspected COVID-19 Cases
Nursing surveillance was increased in its frequency and tools: in some NHs (1, 2, 3, 4, 5), nurses focused on the early identification of those infected by frequently monitoring the residents’ temperature and oxygen saturation, as recommended13,29–31 and by valuing the clinical observation and judgement, especially of nurses who knew the residents, their personal history and clinical issues in depth because they had been caring for them for several years (NHs 3, 5).
Intensifying the Nursing Care
As residents manifested COVID-19-related health problems, NHs (1, 2, 4) increased the amount of nursing care, reaching levels similar to sub-acute settings, to avoid hospitalization, due to the limited bed capacity of the hospitals, the need to limit the spread of the virus and the willingness to ensure residents’ comfort in their place of life. Given that only one NH (1) was equipped with a centralized oxygen system, some of the remaining facilities (NHs 2, 3, 5) requested large supplies of additional tanks, while another (NH 4) started acute treatments, substantially changing its mission.
Networking
After the first difficulties in contacting family members, residents received and made video calls in all NHs on a regular basis. This intervention was perceived as important in preventing the residents’ sense of abandonment and to ensure increased involvement of the families. Moreover, some NHs developed networks to share approaches as well as to support each other in coping with difficulties never encountered before. Specifically, other NHs (2, 3), primary care services (NHs 3, 4), the community sector, such as the mayor of the city (NHs 3, 4), or the general practitioners who were already working in the NH before the pandemic were contacted (NH 5). Great support was provided by the COVID-19 Community Care Special Units, composed of medical staff identified as being trained in the specific care (NHs 1, 2, 3, 5). However, two NHs (2, 4) also hosted an infectious disease specialist, who helped them in undertaking locally the best strategies to deal with the pandemic, supporting the staff psychologically.
Interventions at the Nursing Staff Level
Ensuring Appropriate Staff
Due to the large number of infected staff, one facility (NH 2) was forced to address important staff shortages by increasing the number of hours/week and limiting the rests between shifts. Another (NH 4) has empathised that many nurses and nursing aides were living together or shared transports (eg, car); therefore, each positivity meant that other staff members needed to quarantine as close contact(s). Moreover, some NHs (2, 5) shared the same staff, and they immediately suspended the rotations across the facilities when cross-contamination appeared.
In the attempt to manage all these difficulties and the dramatic shortage, NHs enacted different interventions. To increase the capacity to deal with the difficulties in wearing PPE for several hours, some (NHs 2, 5) introduced short shifts (6−7 hours in duration), while others (NHs 4, 5) maintained long shifts (8 or more hours), with breaks every 3–4 hours. Furthermore, other facilities (NHs 1, 2, 4, 5) created an exclusive team dedicated to COVID-19 units, believing that the degree of expertise both in the use of PPE and in managing the complex residents were easily increased due to the prolonged exposition; on the other hand, one NH (3) decided to rotate the staff to limit the risk and the heavy workloads due to the shortages of PPE. One NH (4) dedicated only young professionals to the COVID-19 unit, to preserve older ones or those with health issues. Other NHs (3, 4), valued previous experiences in critical care patients, devoting these professionals to the care of COVID-19 residents, or employed trained staff from hospitals/districts who had been moved to the NH (5).
Moreover, to prevent contagion, some NHs (3, 5) supervised staff behaviour closely about the use of PPE and other measures (eg, hand hygiene and distancing), also providing warnings or disciplinary interventions for those not adhering to the expected behaviour. Following regional and national rules,13,29–31 NHs (1, 2, 3, 4) intensified the surveillance by testing each staff member once a week or more. Only one facility (NH 5) maintained surveillance every two weeks.
Providing Special Training
Some NHs (2, 5) recognized the importance of specific training, preparing and sharing education tools with other facilities with regard to dressing and undressing procedures. Moreover, one NH (5) developed a special training, with the use of videos and self-preparing tools, adapting the information received to the facility’s needs.
Interventions at the Resident’s Level
Limiting Further Freedom
Despite their condition in terms of COVID-19 (eg, infected or not), in some NHs (1, 5) the residents’ freedom was further limited by asking them to wear masks, even those who had difficulty maintaining the mask (eg, with cognitive decline): moreover, they were requested to stay in their bedroom all day (NHs 2, 4, 5).
Discussion
We described the interventions enacted by NMs and perceived to be effective in fighting the outbreak in public NHs. The NHs differed in the number of beds, from small to large, organized into units with an average of 30 beds, from one to two residents in each room, and with only one with mainly three beds in a room. The main NH features, and the amount of nursing care delivered to residents, were similar to those already documented among Italian facilities.32 At the fourth wave, the NHs included reported from a few (9.9%) residents to almost all (91.6%) residents being infected, and in all, there was a higher mortality than that reported in other countries,33 although data available should be considered with prudence given that only at the end of the pandemic will it be possible to definite the precise mortality rates according to the causes.34,35
Our NHs were not prepared to cope with a pandemic, as reported in many facilities around the world.26 Their marginal role in the health-care sector, with a poor coordination with hospitals considered to be at the core of the health-care system,7 might have rendered more challenging the interventions’ identification6 and implementation, along with the pre-existing frailty of the NH system.35 Moreover, according to the Haddon Matrix structure,23 where interventions affecting public health challenges – such as the COVID-19 pandemic is – have been divided into “pre-event”, “event” and “post-event” time, our NHs enacted interventions during the “event”, targeting the environment, the nursing staff and the residents. The first attempt was to keep the COVID-19 virus out of the facility; once the virus penetrated, the NHs turned their forces to the internal reorganization as an initial awareness of the situation and a consequent response to it. The NHs implemented several interventions to progressively escalate the issues, and it is possible that their perceived effectiveness has also been influenced by the interactions of such actions with each other.35,36 In other words, NHs built and provided a pandemic plan during the event, suggesting that investing in the NHs disaster preparedness is a priority.
At the overall level, three main patterns of interventions have emerged: some have been applied by all facilities, also in line with available recommendations (eg, visiting restrictions); others have been implemented by some facilities (eg, providing special training); whereas other have been implemented in different directions, also contrary to recommendations (eg, resident and roommate isolation), suggesting an area of further investigation. In the first period of COVID-19 pandemic, interventions were not derived from evidence: only some of them were based on scientific literature, while others were based on the opinion of experts or on local initiatives.24 This has created heterogeneity across NHs, triggering also ethical dilemmas among HCPs, for example, regarding the implications on residents, or the need to make choices sometimes against the recommendations.38
At first, NHs focused on interventions at environmental levels, mainly implementing national and/or regional guidelines13,29–31 and available evidence.21,22,27,37 Visitors’ restrictions (including volunteers) were implemented immediately, and compartmentalization was applied in all NHs, whereas other interventions (eg, quarantine area for residents returning from hospital, dressing rooms for staff) were implemented in only some. In short, the entire NH environment has been revised by sacrificing some common areas devoted to residents with specific needs (eg, dementia) and by an in-depth altering of the home-like environment that has been considered as a key role in improving the quality of life of residents.32,39
In the attempt to make an early identification of positive cases and close contacts, only three NHs intensified their tracing activities and testing, while suspected or actual cases and their belongings have been managed differently: cases (and their roommate(s)) were isolated immediately in their room; other NHs immediately transformed the entire floor into a COVID-19 unit in the consideration that all were living together, thus were close contacts; others moved the residents into the designed COVID-19 units, whereas their negative roommates were transferred to a grey area. Substantially, the initial idea of compartmentalization was violated according to the pragmatic concept of close contacts, such as all those living (and working) in the same floor, and the attempt to prevent internal transfers potentially increased the spread of the virus. In this field, a clear conceptual and practical definition of “close contacts” according to specific features of the NH environment is required and evaluating the effectiveness of the different compartmentalization strategies enacted is recommended.40–42
To support the reshaped environment and mission, services have been reorganized and increased, but, probably due to the limited resources available, the increased ventilation and coordination between the environmental cleaning and disinfection was enacted only in a few NHs, despite their relevance.21,25,27 Nurses have been invited to also increase the standards of care by undertaking more checks/monitoring of the residents’, not only to measure their vital signs but also to detect early changes22,41,42 by using news tools and their clinical judgement and their deeper knowledge of the personal and clinical history of each resident. However, given the lack of nurses and the increased needs, ensuring higher standards of monitorization might have led to missed care in some fundamental needs (eg, help with eating and hygiene).43 The nursing care has also been intensified, changing the NHs’ mission to a sub-acute setting of care (eg, providing oxygen and treatments), considering the facility to be the right place to care for residents. In this context, the NH care was rethought both in the medical and in the nursing care, confirming the need to reimagine the care delivered in the facilities according to the increased complexity of needs.44,45
As a reaction of the well-documented fragmented relationship with the hospitals,7 with governments centered mainly on hospital issues, rendering these facilities as abandoned castles,45 our NHs attempted to develop networks with different potential partners, such as other nursing homes, primary care services, community care sectors and general practitioners. NHs have been documented as complex adaptive systems, each with their own history (eg, social and physical), capable of continuing internal adjustments in a dynamic way.46 According to the findings, our NHs have also demonstrated the capacity to search for external alliances, indicating the call for support,47 brought the facilities out of historical isolation6 and promoting new synergies, in order to provide common infection control measures, staff education and collaborative approaches.22,42
At the staff level, addressing the shortages exacerbated by the positive or quarantined cases among nurses and nurses’ aides was the main issue: in addition to increasing the working hours, there were contrasting interventions between those designing short and long shifts, between those who dedicated a team to COVID-19 patients and those who rotated the staff, or dedicated younger nurses/nursing aides or only those with experience. All these strategies seem to be supported by specific principles failing in the field of occupational health (eg, limiting work exposure, preventing tiredness, increasing the risk of inappropriate behaviours), patient safety (eg, dedicating a team to prevent rotations and ensuring nurses with competences), through to the ethical principles (eg, protecting aged professionals at increased risk). The debate regarding the best choice is still open given that no strong evidence is available to date,27,37 and also given the complexity of NHs where the nurse-to-patient ratio is higher, and nurses’ aides have limited training, suggesting an area for future investigation. In this turbulent context, surveilling the staff behavior in their adherence to established preventive principles was considered effective and compensated for the lack of specific training ensured before and during the outbreak, despite the evidence available on its efficacy.5,21,26
At resident level, they were invited to wear a mask and to stay in their room by implementing, in a certain way, what was required outside of the NHs, under the “stay at home” slogan. This should be considered a critical decision under the ethical point of view, considering that its implementation was not required and its capacity to dramatically limit the freedom of residents. An increased risk of depression, agitation, anxiety, negative emotions and a greater cognitive decline when residents in long-term facilities experience loneliness have been documented.48 However, the spirit underlining this intervention was to protect the residents, given the higher risk of direct transmission occurring in closed and crowded places and close-contact settings as NHs were.49
Limitations
The study has several limitations. First, we implemented a pragmatic approach, based on partnership as suggested by the available literature.50 There were included only five NHs with similar missions and located in an Italian rural region with the highest amount of older people and where the highest COVID-19 mortality rates have been documented. Second, we involved two participants/NH to deepen their experience: while the presence of two participants might have prevented inaccuracies, the time elapsed from the first wave to the interview may have introduced a recall bias. Moreover, having previously contacted the participants, explaining the main questions by telephone/email before the interview, may have generated socially desirable responses from them, although this was performed to allow an in-depth reflection of the actions undertaken. However, the questions were focused on events happened, without any intent to evaluate the interventions implemented. Third, we collected data regarding all interventions according to their perceived effectiveness, without taking into consideration their actual effectiveness: involved participants worked over the waves in the same NH environment, and this might have convinced them of the effectiveness of the interventions applied. Moreover, they might also have slightly changed the interventions over time: the several networks created might have allowed the opportunity to compare the interventions applied with those implemented in other settings and to assess their effectiveness. With this regard, developing concrete research alliances in this field might be important to assess the actual effectiveness of the interventions emerged. Fourth, interview transcripts were not returned to participants for comment and/or correction, as well as the findings were not shared with them to prevent additional burden during the fourth wave.
Conclusion
To the best of our knowledge, this is the first study describing the interventions enacted by NHs and perceived as effective by them from the first to the fourth wave of the COVID-19 pandemic in Italy. Despite their documented frailty and precarious system, the NHs implemented several interventions to protect their residents, at the environment, the nursing staff and at the residents’ levels. Three main patterns of interventions have emerged: some were enacted in all facilities, others in a few but in a homogeneous manner, while other interventions were implemented in opposing directions and also against the given recommendations. All the interventions were designed and implemented during the outbreak suggesting the need to increase the NHs’ preparedness to face possible disasters, such as a pandemic. Those applied in contrast to available guidelines or non-homogeneously across the NHs, such as how to compartmentalise the residents, how to manage the close contacts, and how to ensure the required amount of nursing care, should be subjected to quantitative investigation to discover their real effectiveness.
Ethical Approval
The study was approved by the Comitato Etico Unico Regionale Fvg (CEUR, Friuli Venezia Giulia, Italy) (September 15th, 2020; March 4th, 2022, Prot. ELDERLY COVID-19 FVG).
Consent
Written consent was obtained from all participants included in this study where there were specified study aims; the data collection procedures; the confidentiality of the data collected both at the individual and at the institutional level; and how the data analysis was performed rendering anonymous the extracted quotes.
Acknowledgments
We thank the participants for their time and their involvement in the research process.
Disclosure
This research did not receive any funding from agencies in the public, commercial, or not-for-profit sectors. No conflict of interest has been declared by the authors.
References
1. D’Adamo H, Yoshikawa T, Ouslander JG. Coronavirus disease 2019 in geriatrics and long-term care: the ABCDs of COVID-19. J Am Geriatr Soc. 2020;68(5):912–917. doi:10.1111/jgs.16445
2. Ciminelli G, Garcia-Mandicó S. COVID-19 in Italy: an analysis of death registry data. J Public Health. 2020;42(4):723–730. doi:10.1093/pubmed/fdaa165
3. Tan LF, Chua JW. Strategies to stop and prevent COVID-19 transmission in long-term care facilities (LTCFs). QJM. 2021;114(2):151–152. doi:10.1093/qjmed/hcaa265
4. Wang Z. Use the environment to prevent and control COVID-19 in senior-living facilities: an analysis of the guidelines used in China. Herd. 2021;14(1):130–140. doi:10.1177/1937586720953519
5. Hashan MR, Smoll N, King C, et al. Epidemiology and clinical features of COVID-19 outbreaks in aged care facilities: a systematic review and meta-analysis. E Clinical Med. 2021;33:100771. doi:10.1016/j.eclinm.2021.100771
6. Notarnicola E, Perobelli E, Rotolo A, Berloto S. Lessons learned from Italian nursing homes during the COVID-19 outbreak: a tale of long-term care fragility and policy failure. J Long Term Care. 2021;221–229. doi:10.31389/jltc.73
7. Arlotti M, Ranci C. The impact of COVID-19 on nursing homes in Italy: the case of Lombardy. J Aging Soc Policy. 2021;33(4–5):431–443. doi:10.1080/08959420.2021.1924344
8. Shallcross L, Burke D, Abbott O, et al. Factors associated with SARS-CoV-2 infection and outbreaks in long-term care facilities in England: a national cross-sectional survey. Lancet Healthy Longevity. 2021;2(3):e129–e142. doi:10.1016/S2666-7568(20)30065-9
9. Rubano MD, Kieffer EF, Larson EL. Infection prevention and control in nursing homes during COVID-19: an environmental scan. Geriatr Nurs (Minneap). 2022;43:51–57. doi:10.1016/j.gerinurse.2021.10.023
10. Istituto Superiore di Sanità (ISS). Caratteristiche dei pazienti deceduti positivi all’infezione da SARS-CoV-2 in Italia; 2022. Availlable from: https://www.epicentro.iss.it/coronavirus/bollettino/Report-COVID-2019_10_gennaio_2022.pdf.
11. Palmieri L, Andrianou X, Barbariol P, et al. Caratteristiche dei pazienti deceduti positivi all’infezione da SARS-CoV-2 in Italia. EpiCentro Istituto Superiore di Sanità. 2020;1:84.
12. Istituto nazionale di STATistica (ISTAT). Impatto dell’epidemia Covid-19 sulla mortalità totale della popolazione residente; 2022. Availlable from: https://www.iss.it/documents/20126/0/Report_ISS_Istat_2021_10_giugno+%281%29.pdf/3df35cd3-edd5-56e1-5867-d274f5032fb5?t=1623336923282.
13. Ministero della Salute. Misure urgenti in materia di contenimento e gestione dell’emergenza epidemiologica da COVID-19. Regione autonoma Friuli-Venezia Giulia; Availlable from: https://www.gazzettaufficiale.it/eli/id/2020/02/25/20A01276/sg.
14. McAdam R, Mason B, McCrory J. Exploring the dichotomies within the tacit knowledge literature: towards a process of tacit knowing in organizations. J Knowledge Management. 2007;11(2):43–59. doi:10.1108/13673270710738906
15. Sandelowski M. What’s in a name? Qualitative description revisited. Res Nurs Health. 2010;33(1):77–84. doi:10.1002/nur.20362
16. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
17. Patton MQ. Qualitative Research & Evaluation Methods: Integrating Theory and Practice. Sage publications; 2014.
18. Palese A, Grassetti L, Bandera D, et al. High feeding dependence prevalence in residents living in Italian nursing homes requires new policies: findings from a regionally based cross-sectional study. Health Policy (New York). 2018;122(3):301–308. doi:10.1016/j.healthpol.2018.01.011
19. Morse JM. Critical analysis of strategies for determining rigor in qualitative inquiry. Qual Health Res. 2015;25(9):1212–1222. doi:10.1177/1049732315588501
20. Santana RF, Silva M, Marcos DA, Rosa C, Wetzel Junior W, Delvalle R. Nursing recommendations for facing dissemination of COVID-19 in Brazilian Nursing Homes. Rev Bras Enferm. 2020;73.
21. Wang J, Yang W, Pan L, et al. Prevention and control of COVID-19 in nursing homes, orphanages, and prisons. Environ Pollut. 2020;266:115161. doi:10.1016/j.envpol.2020.115161
22. Dykgraaf SH, Matenge S, Desborough J, et al. Protecting nursing homes and long-term care facilities from COVID-19: a rapid review of international evidence. J Am Med Dir Assoc. 2021;22(10):1969–1988. doi:10.1016/j.jamda.2021.07.027
23. Fritch WM, Agnew J, Rosman L, Cadorette MA, Barnett DJ. Application of the Haddon matrix to COVID‐19 prevention and containment in nursing homes. J Am Geriatr Soc. 2021;69(10):2708–2715. doi:10.1111/jgs.17358
24. Giri S, Chenn LM, Romero-Ortuno R. Nursing homes during the COVID-19 pandemic: a scoping review of challenges and responses. Eur Geriatr Med. 2021;12(6):1127–1136. doi:10.1007/s41999-021-00531-2
25. Huang C-Y, Kuo Y-H, Chuang S-T, Yen H-R, Tou S-I. The experience of executing preventive measures to protect a nursing home in Taiwan from a COVID-19 outbreak. Eur Geriatr Med. 2021;12(3):609–617. doi:10.1007/s41999-021-00459-7
26. Ochi S, Murakami M, Hasegawa T, Komagata Y. Prevention and Control of COVID-19 in Imperfect Condition: practical Guidelines for Nursing Homes by Japan Environment and Health Safety Organization (JEHSO). Int J Environ Res Public Health. 2021;18(19):10188. doi:10.3390/ijerph181910188
27. Shi M, Zhang F, He X, Huang S, Zhang M, Hu X. Are preventive measures adequate? An evaluation of the implementation of COVID-19 prevention and control measures in nursing homes in China. BMC Health Serv Res. 2021;21(1):1–14. doi:10.1186/s12913-021-06690-z
28. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
29. Ministero della Salute. Misure urgenti in materia di contenimento e gestione dell’emergenza epidemiologica da COVID-19. Availlable from: Ihttps://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2020&codLeg=73314&parte=1%20&serie=null.
30. Ministero della Salute. Circolare del Ministero della salute. COVID-2019, nuove indicazioni e chiarimenti. Availlable from: https://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2020&codLeg=73195&parte=1%20&serie=null.
31. Ministero della Salute. Precisazioni in ordine all’ordinanza del Ministero della Salute del 21 febbraio 2020 recante “Ulteriori misure profilattiche contro la diffusione della malattia infettiva COVID-19. Availlable from: https://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2020&codLeg=73442&parte=1%20&serie=null.
32. Palese A, Gonella S, Grassetti L, et al. What nursing home environment can maximise eating Independence among residents with cognitive impairment? Findings from a secondary analysis. Geriatr Nurs (Minneap). 2020;41(6):709–716. doi:10.1016/j.gerinurse.2020.03.020
33. World Helath Orgnization (WHO). Situation reports. Availlable from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports.
34. Veronese N, Koyanagi A, Stangherlin V, et al. Mortality attributable to COVID-19 in nursing home residents: a retrospective study. Aging Clin Exp Res. 2021;33(6):1745–1751. doi:10.1007/s40520-021-01855-6
35. Cepparulo A, Giuriato L. The residential healthcare for the elderly in Italy: some considerations for post-COVID-19 policies. Eur J Health Economics. 2021;24:1–15.
36. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. 2008;337:337. doi:10.1136/bmj.a1655
37. Ingram C, Downey V, Roe M, et al. COVID-19 prevention and control measures in workplace settings: a rapid review and meta-analysis. Int J Environ Res Public Health. 2021;18(15):7847. doi:10.3390/ijerph18157847
38. McLean E, Onarheim KH, Schanche E, Schaufel MA, Miljeteig I. Ethical dilemmas for nursing home doctors during the COVID-19 pandemic. Tidsskr nor Laegeforen. 2022;142:10.
39. Palese A, Decaro A, Bressan V, et al. Measuring the therapeutic properties of nursing home environments in the Italian context: findings from a validation and cross-sectional study design. Ann. Ig. 2020;32:117–131.
40. Alawi MMS. Successful management of COVID-19 outbreak in a long-term care facility in Jeddah, Saudi Arabia: epidemiology, challenges for prevention and adaptive management strategies. J Infect Public Health. 2021;14(4):521–526. doi:10.1016/j.jiph.2020.12.036
41. Tobolowsky FA, Bardossy AC, Currie DW, et al. Signs, symptoms, and comorbidities associated with onset and prognosis of COVID-19 in a nursing home. J Am Med Dir Assoc. 2021;22(3):498–503. doi:10.1016/j.jamda.2021.01.070
42. Gugliotta C, Gentili D, Marras S, et al. SARS-CoV-2 Epidemics in Retirement and Nursing Homes in Italy: a New Preparedness Assessment Model after the First Epidemic Wave. Int J Environ Res Public Health. 2021;18(11):5712. doi:10.3390/ijerph18115712
43. Sist L, Palese A. Le decisioni infermieristiche e le missed nursing care: risultati di una scoping review. [Decision Making process and missed nursing care: findings from a scoping review]. Assist Inferm Ric. 2020;39(4):188–200. doi:10.1702/3508.34952
44. Benvenuti E, Rivasi G, Bulgaresi M, et al. Caring for nursing home residents with COVID-19: a “hospital-at-nursing home” intermediate care intervention. Aging Clin Exp Res. 2021;33(10):2917–2924. doi:10.1007/s40520-021-01959-z
45. Trabucchi M, de Leo D. Nursing homes or abandoned castles: COVID-19 in Italy. Lancet Psychiatry. 2021;8(2):e6. doi:10.1016/S2215-0366(20)30541-1
46. Simpson KM, Porter K, McConnell ES, et al. Tool for evaluating research implementation challenges: a sense-making protocol for addressing implementation challenges in complex research settings. Implementation Sci. 2013;8(1):1–12. doi:10.1186/1748-5908-8-2
47. Coulongeat M, Aïdoud A, Poupin P, Dubnitskiy-Robin S, Fougère B. A local COVID-19 support platform for nursing homes: feedback and perspectives. J Am Med Dir Assoc. 2021;22(8):1599–1601. doi:10.1016/j.jamda.2021.06.001
48. Bethell J, Aelick K, Babineau J, et al. Social Connection in Long-Term Care Homes: a Scoping Review of Published Research on the Mental Health Impacts and Potential Strategies During COVID-19. J Am Med Dir Assoc. 2021;22(2):228–237.e25. doi:10.1016/j.jamda.2020.11.025
49. Nishiura H, Oshitani H, Kobayashi T, et al. Closed environments facilitate secondary transmission of coronavirus disease 2019 (COVID-19). MedRxiv. 2020;2:84.
50. Baier RR, McCreedy E, Uth R, Gifford DR, Wetle T. Nursing home leaders’ perceptions of a research partnership. Aging Clin Exp Res. 2021;33(12):3371–3377. doi:10.1007/s40520-021-01847-6
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.