")
Back to Journals » Journal of Asthma and Allergy » Volume 17
What is the Best Way to Diagnose Possible Asthma Patients with Negative Bronchodilator Reversibility Tests?
Authors Başa Akdoğan B , Koca Kalkan I, Köycü Buhari G, Özdedeoğlu Ö, Ateş H, Aksu K , Öner Erkekol F
Received 1 September 2023
Accepted for publication 8 February 2024
Published 22 February 2024 Volume 2024:17 Pages 113—122
DOI https://doi.org/10.2147/JAA.S437756
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Buket Başa Akdoğan, Ilkay Koca Kalkan, Gözde Köycü Buhari, Özlem Özdedeoğlu, Hale Ateş, Kurtuluş Aksu, Ferda Öner Erkekol
Department of Chest Diseases, Division of Immunology and Allergy, University of Health Sciences Ataturk Chest Diseases and Chest Surgery Education and Research Hospital, Ankara, Turkey
Correspondence: Buket Başa Akdoğan, Department of Chest Diseases, Division of Immunology and Allergy, University of Health Sciences Ataturk Chest Diseases and Chest Surgery Education and Research Hospital, Incirlist, No: 57 Floor:3, 34147 Bakirkoy/Istanbul, Ankara, Turkey, Tel +90 5053518861 ; +90 850 4339393, Email [email protected]
Objective: The best method and strategy for the diagnosis of asthma remains unclear, especially in patients with negative bronchodilator reversibility test (BDRT). In our study, we aimed to investigate the diagnostic yield of peak expiratory flow (PEF) variability for this patient group.
Methods: A total of 50 patients with suspected asthma, all with negative BDR test, were included in the study. Demographic information and symptoms were recorded and PEF variability was monitored for 2 weeks. Metacolinbronchial provocation test (mBPT) was performed. Asthma was diagnosed when PEF variability ≥ 20% and/or positive mBPT was observed.
Results: 30 of 50 patients were diagnosed with asthma. After 1 month, 17 patients were evaluated for treatment outcomes. The sensitivity and specificity of PEF variability for different cut-off values (≥ 20%, > 15% and > 10%) were 61.5– 83.3, 88.5– 62.5 and 100– 16.7, respectively. One of the most important findings of our study was the absence of variable airflow limitation or airway hyper reactivity in 39% patients with a previous diagnosis of asthma. Multiple logistic regression analysis revealed that a low baseline FEF25-75 value was an independent predictive factor for the diagnosis of asthma (p= 0.05).
Conclusion: The most efficient diagnostic test for asthma is still unclear due to many factors. Our study is one of the few studies on this subject. Although current diagnostic recommendations generally recommend a PEF variability of 10% for the diagnosis of asthma, this threshold may not be appropriate for the BDR-negative patient group. Our results suggest using a threshold value of < 15% for PEF variability when excluding asthma and ≥ 20% when confirming the diagnosis of asthma in patients with clinically suspected but unproven reversibility. Furthermore, FEF25-75 is considered to be an important diagnostic parameter that should be included in diagnostic recommendations for asthma.
Keywords: diagnosis of asthma, reversibility, peak expiratory flow (PEF) variability, bronchial challenge test, forced expiratory flow (25-75%)
Introduction
Asthma is the most common chronic disease worldwide. More than 339 million people live with asthma.1 It is estimated that 100 million people will be diagnosed with asthma by 2025.2 It is a heterogeneous disease, usually characterised by chronic airway inflammation. It is characterised by variable airflow obstruction as well as adaptive respiratory symptoms that vary in time and intensity. The need to address the variable airflow limitation that characterises asthma before initiating treatment is emphasised in updated asthma management guidelines.3,4
Population-based studies in children, adults and the elderly show that 20–70% of people with asthma go undiagnosed and ultimately untreated. These studies also show that 30–35% of children are frequently misdiagnosed with asthma and that asthma is overdiagnosed in the general population5 There are many studies investigating the use of testing methods such as spirometric reversibility, PEF monitoring and mBPT for the correct diagnosis of asthma.6,7 However, the most appropriate test and strategy for diagnosis remains unclear, especially in patients in whom early reversibility cannot be demonstrated by spirometry.6–8
In our study, we aimed to draw attention to personalised PEF devices, which we believe may be helpful in the diagnosis and follow-up of asthma even during unprecedented events such as pandemic restrictions.9 To increase the diagnostic efficiency and usability of PEF variability, we aimed to review the cut-off value of 10% recommended by GINA3 and the cut-off value of 20%10 recommended by other guidelines and to determine the most appropriate PEF variability cut-off value.
Materials-Methods
Patient Population
The people who applied to our outpatient clinic with complaints consistent with asthma between June 2016 and 2017 were evaluated. From this patient population, patients who had no problems in physical examination, whose early reversibility could not be demonstrated in simple spirometry, and who could not prove variable airway obstruction were targeted. Patients aged 18–65 years, with a smoking history <10 pack/year, who were not pregnant at the time of admission, who did not have respiratory tract infection in the last 6 weeks and who did not have any symptoms suggestive of other respiratory diseases (eg sarcoidosis, COPD, bronchiectasis) were included in the study. Patients who did not meet these criteria, who could not cooperate during spirometric evaluation, PEF monitoring and mBPT tests, or who had missing data were excluded from the study. A total of 58 patients were evaluated. All data of 50 patients were completed.
Study Design
Demographic information, history, symptoms, presence of atopy, eosinophil level, skin prick test and/or specific IgE results of all patients included in the study were recorded. The symptom severity score was calculated by scoring the number of daytime symptoms (<2 per month, 1–2 times per month, >2 per week) + activity restriction + nocturnal symptom (0–4).
PEF measuring devices were distributed to 50 patients at the first visit. Instructions for use of the device were explained to the participants. Electronic PEF meters were not used. The same type of PEF meters were used for each patient. They were asked to measure PEF 3 times a day, in the morning, in the evening and when there was a complaint, and to record their best values on the given chart. At the end of the second week, the patients were called for the 2nd visit. From the charts, thePEFvariability was calculated daily and the average was taken. Patients with PEF variability greater than 20% were considered as positive. The GINA asthma report was used to calculate the PEF variability. mBPT was administered using the two-minute tidal volume inhalation technique. BPT contraindications and preparation guidelines were followed. Individuals with PEF variability >20% and/or positive mBPT were diagnosed with asthma. PEF follow-up and mBPT tests were performed in all patients. 30 patients were diagnosed with asthma and treated according to GINA guidelines. The quality of life evaluations of the diagnosed patients were calculated based on the asthma control test (ACT), asthma quality of life scale (AQLQ) and short form 36 (SF-36). A total of 17 patients came for follow-up. 13 patients did not come for follow-up. Symptom scores, ACT, AQLQ, SF-36 quality of life questionnaires, and drug compliance status of the treated patients were checked at 1 month (Figure 1). The study was approved by the Medical Specialist Education Board and the Local Ethics Committee. (Approval number: 08–2018/1552). Informed consent forms were obtained from all patients before the tests.
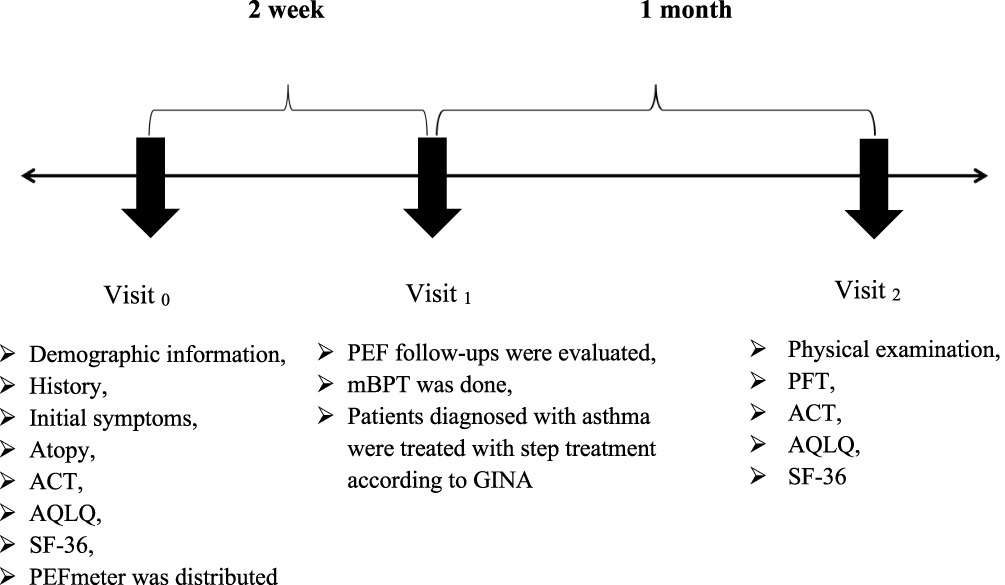 |
Figure 1 Material and method: Demographic characteristics, physical examinations, pulmonary function tests, asthma control tests, quality of life questionnaires were performed at the first application of the participants (Visit 0) who consented to participate in the study. PEF meters were provided to each of them, and their usage was explained. A chart was given to the participants for follow-up standardization. They were asked to perform PEF follow-up for 2 weeks. After 2 weeks, the participants were given mBPT appointments (Visit 1). According to the patients whose results were evaluated, treatment was started according to the recommendations of the GINA guideline. They were called for control after 1 month (Visit 2). Physical examination, pulmonary function tests, quality of life questionnaires, and asthma control tests were renewed and recorded. |
Statistical Analyses
Statistical analyses were made by using the SPSS software. The conformity of the variables to the normal distribution was examined using visual (histogram and probability graphs) and analytical methods (Kolmogorov-Smirnov/Shapiro–Wilk tests). In descriptive statistics, mean and standard deviation were used for normally distributed variables, as well as a median and interquartile range for non-normally distributed variables. The difference between the groups in terms of these frequencies, if any, was tested by comparing them using Chi-square or Fisher tests. The correlation coefficients and statistical significance of the variables were subjected to the Pearson test for normally distributed variables and the Spearman test for at least one of the variables that were not normally distributed or ordinal. P values equal to or less than 0.05 were considered statistically significant.(p ≤ 0.05) Sensitivity, specificity and predictive values of the tests were calculated.
Results
Of the 50 patients included in the study, 30 patients were diagnosed with asthma and 20 patients were followed up as patients with non-specific symptoms. There was no significant difference between the study groups in terms of demographic and clinical characteristics (Table 1).
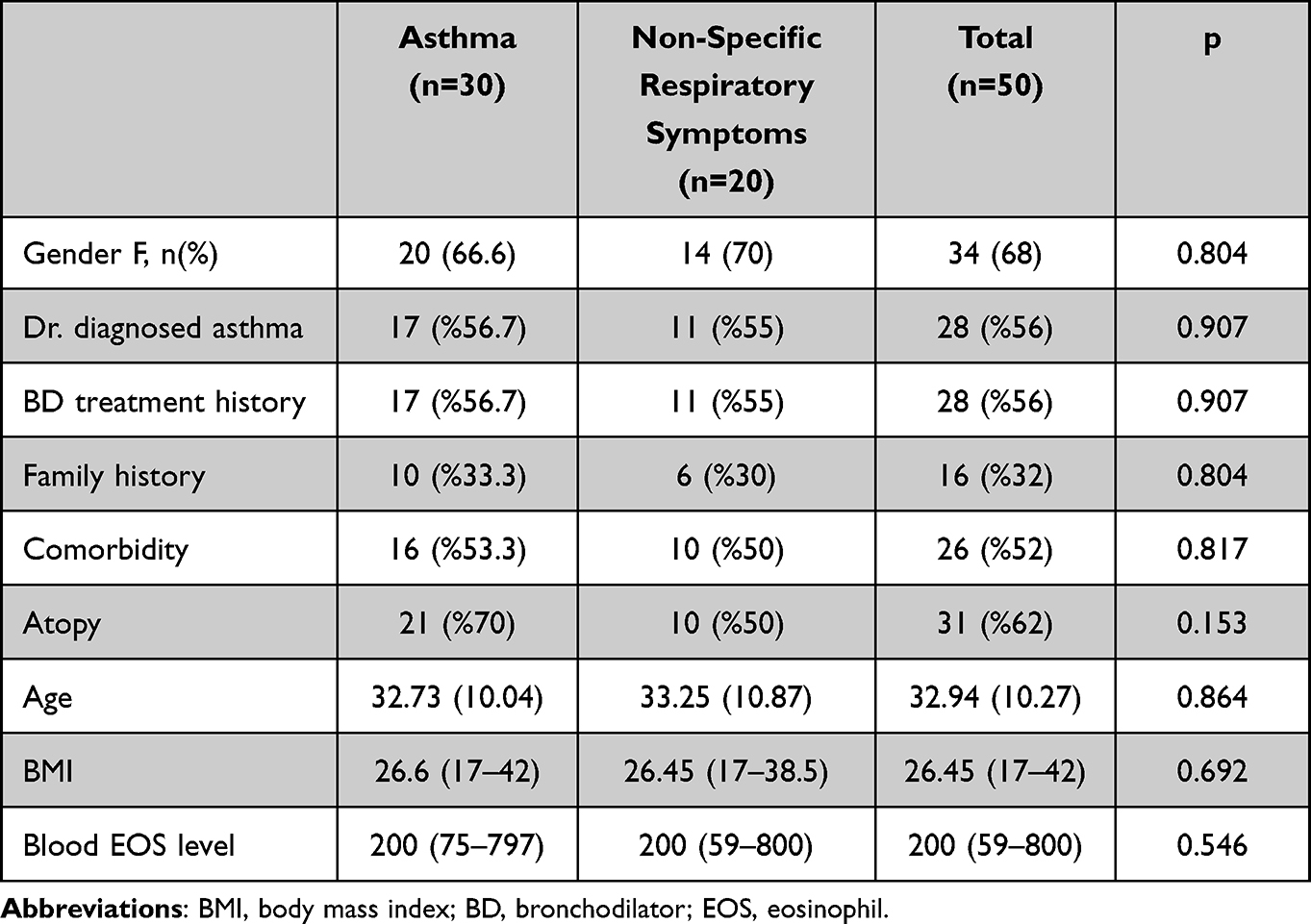 |
Table 1 Demographic and Clinical Features of the Study Group |
When the cardinal symptoms of asthma were questioned, wheezing was statistically significant in the group diagnosed with asthma compared to the group with non-specific symptoms (p = 0.021) (Table 2). No significant difference was found in terms of other symptoms. When we compared asthma patients with non-specific respiratory symptomatic cases, a statistically significant difference was found in favor of asthma in terms of activity limitation (p = 0.05) and total symptom score (p = 0.028).
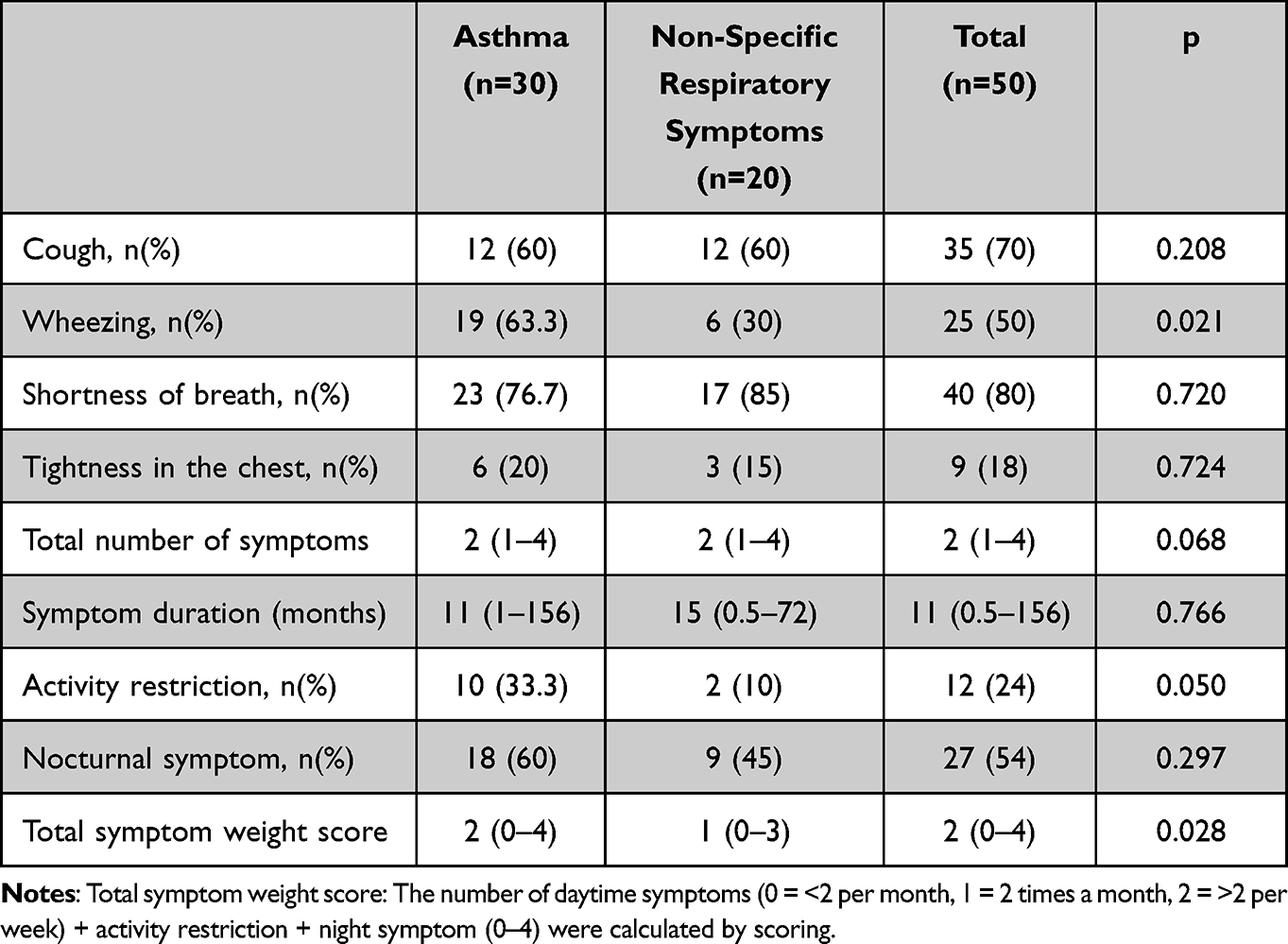 |
Table 2 Clinical Features of the Study Group |
When pulmonary function tests were evaluated, baseline FEF25-75 measurements were significantly lower in the asthma group compared to the other group. There was no statistically significant difference between the two groups in terms of other parameters (Table 3). When the ACT, AQLQ and SF-36 were evaluated, no significant difference was found between the two groups. Baseline FEF25-75 measurement abnormality was found to be an independent predictor of asthma diagnosis (p = 0.05) (Table 4).
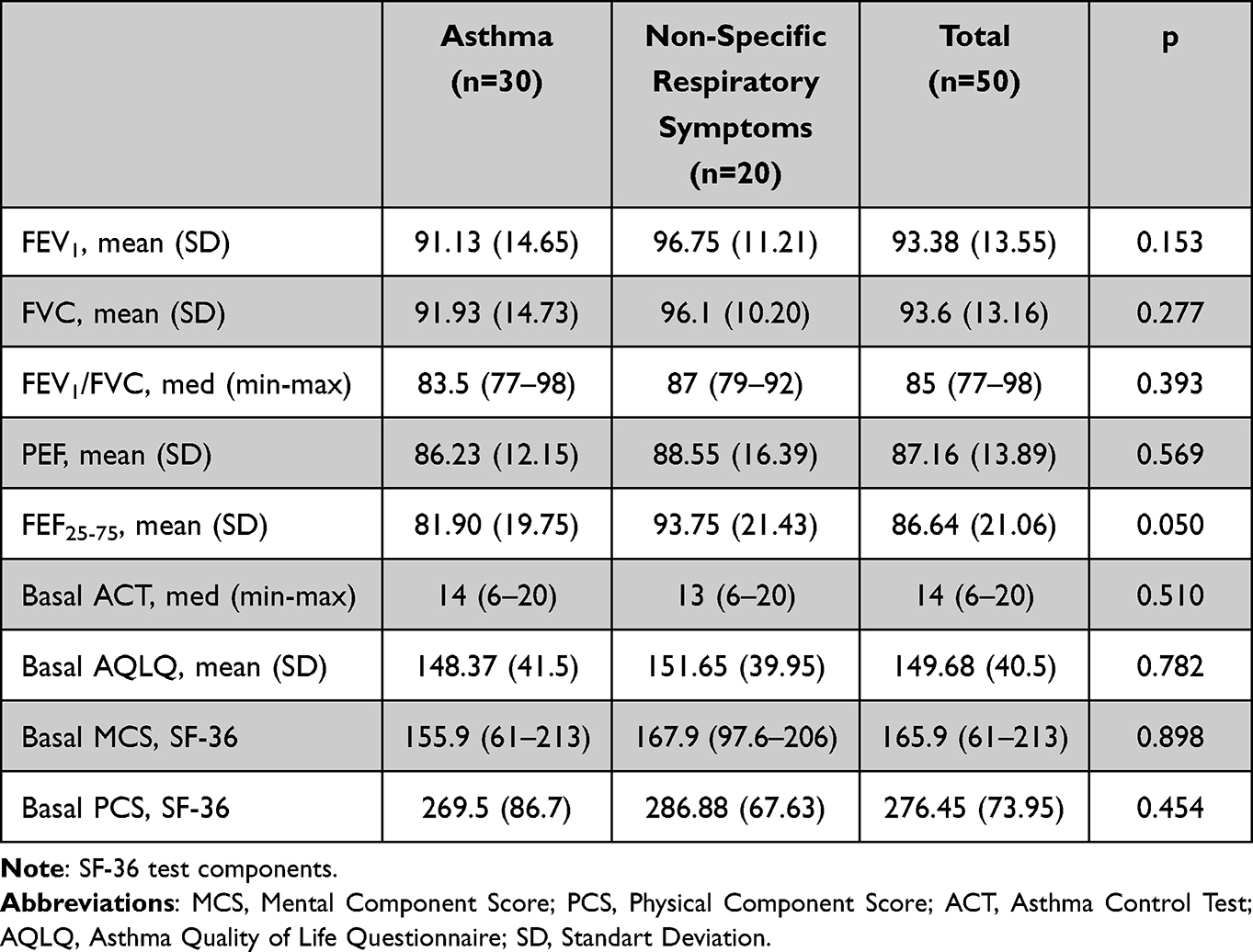 |
Table 3 Basal Spirometry and Survey Data of the Study Group (Visit 0) |
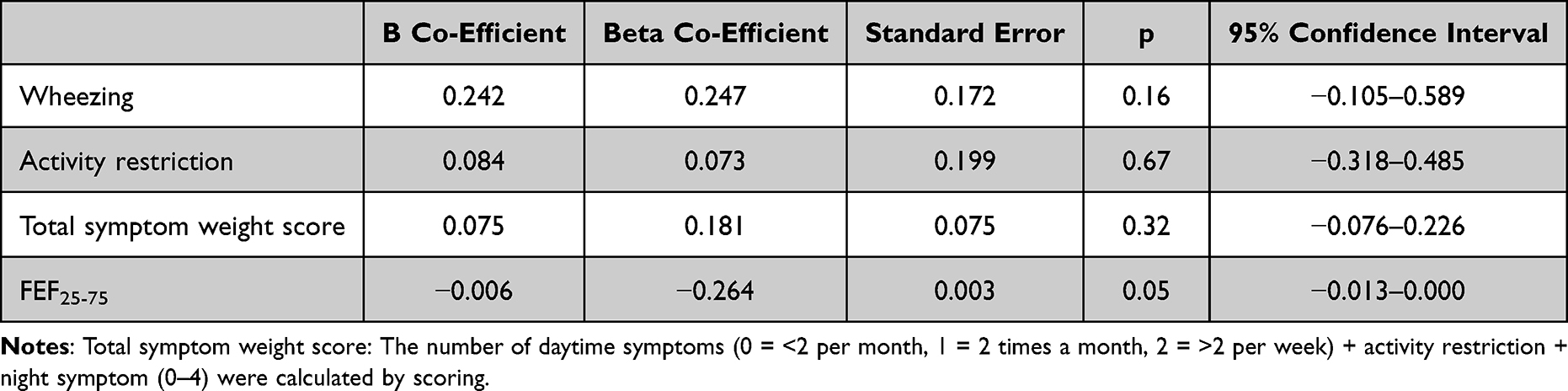 |
Table 4 Multivariate Linear Regression Analysis That Examines Various Parameters to Predict Asthma Diagnosis |
BPT alone was positive in 10 of 30 asthma cases. Both mBPT positivity and PEF variability were positive in 16 cases. Four of the 30 patients were diagnosed with asthma based on positive PEF variability. (Figure 2) When the sensitivity and specificity were evaluated for three different cut-off values of PEF variability, considering mBPT positivity as the baseline diagnostic test for the diagnosis of asthma, the sensitivity and specificity of PEF variability for different cut-off values (≥20%, >15% and >10%) were 61.5–83.3%, 88.5–62.5% and 100–16.7%, respectively (Table 5).
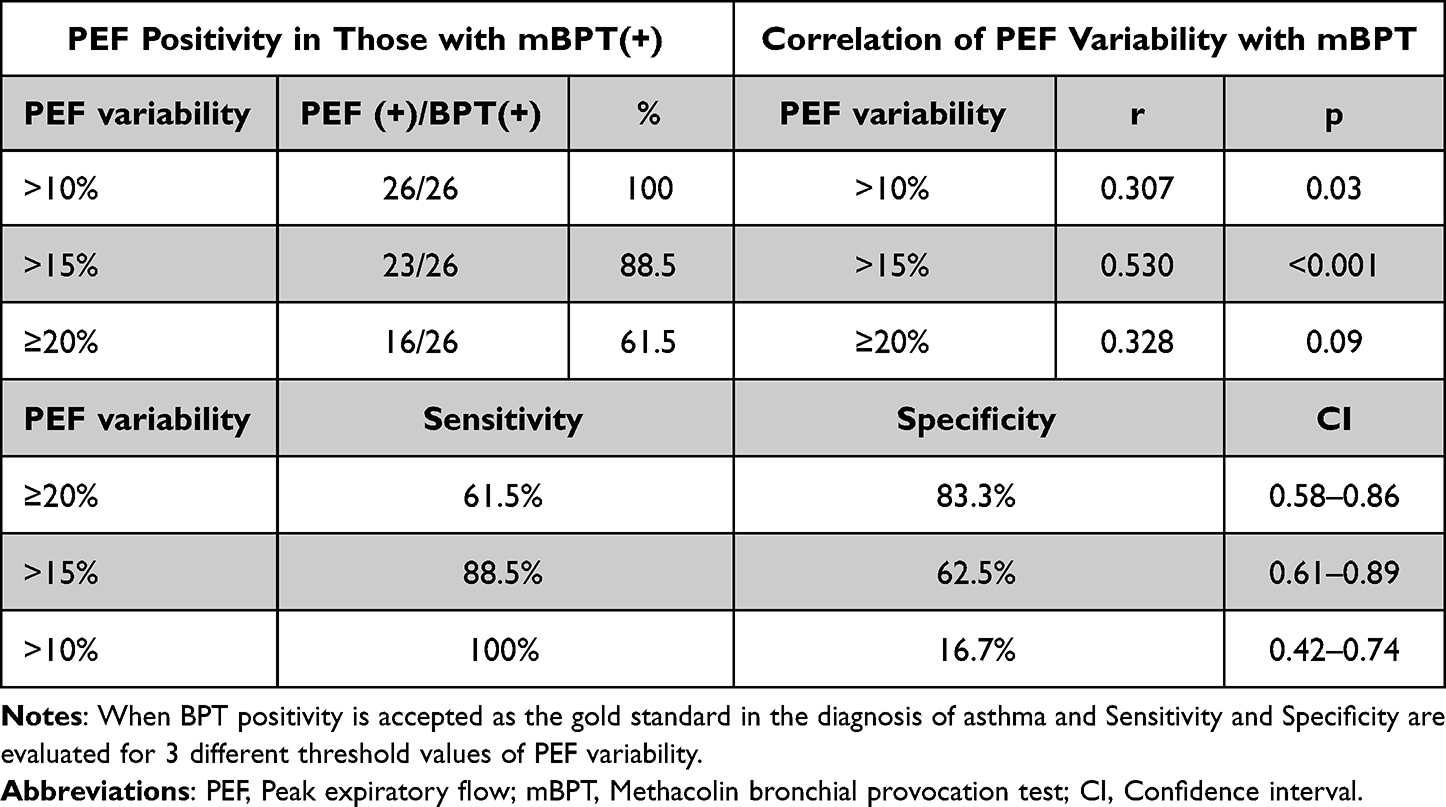 |
Table 5 Correlation Rates Between Patients with BPT Positivity and Different Cut-off Values of PEF Variability |
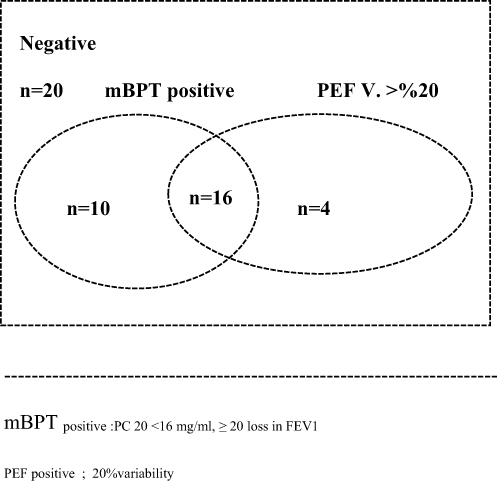 |
Figure 2 Results; BPT alone was positive in 10 of 30 asthma cases. Both mBPT positivity and PEF variability were positive in 16 cases. Only four out of 30 patients were diagnosed with asthma based on positive PEF variability. 20 patients were evaluated as non-specific respiratory symptoms. No treatment was given. At the end of the 1st month, 17 of the 30 treated patients attended visit 2. 13 patients did not attend visit 2. Treatment response of 17 patients was evaluated. |
One of the important results of our study was the absence of variable airflow limitation or airway hyperreactivity in 39.28% of patients with a history of asthma diagnosed by a physician and previously treated for asthma.
Treatment was initiated in 30 patients diagnosed with asthma according to the GINA strategy report. Treatment was not given to 20 patients with non-specific respiratory symptoms. First month controls were planned after treatment.17 patients out of 30 patients came to the first month controls. 13 patients did not come to the controls. Medication compliance was questioned. Significant improvement was found in symptom scores, pulmonary function tests and quality of life of the patients compared to baseline (Table 6).
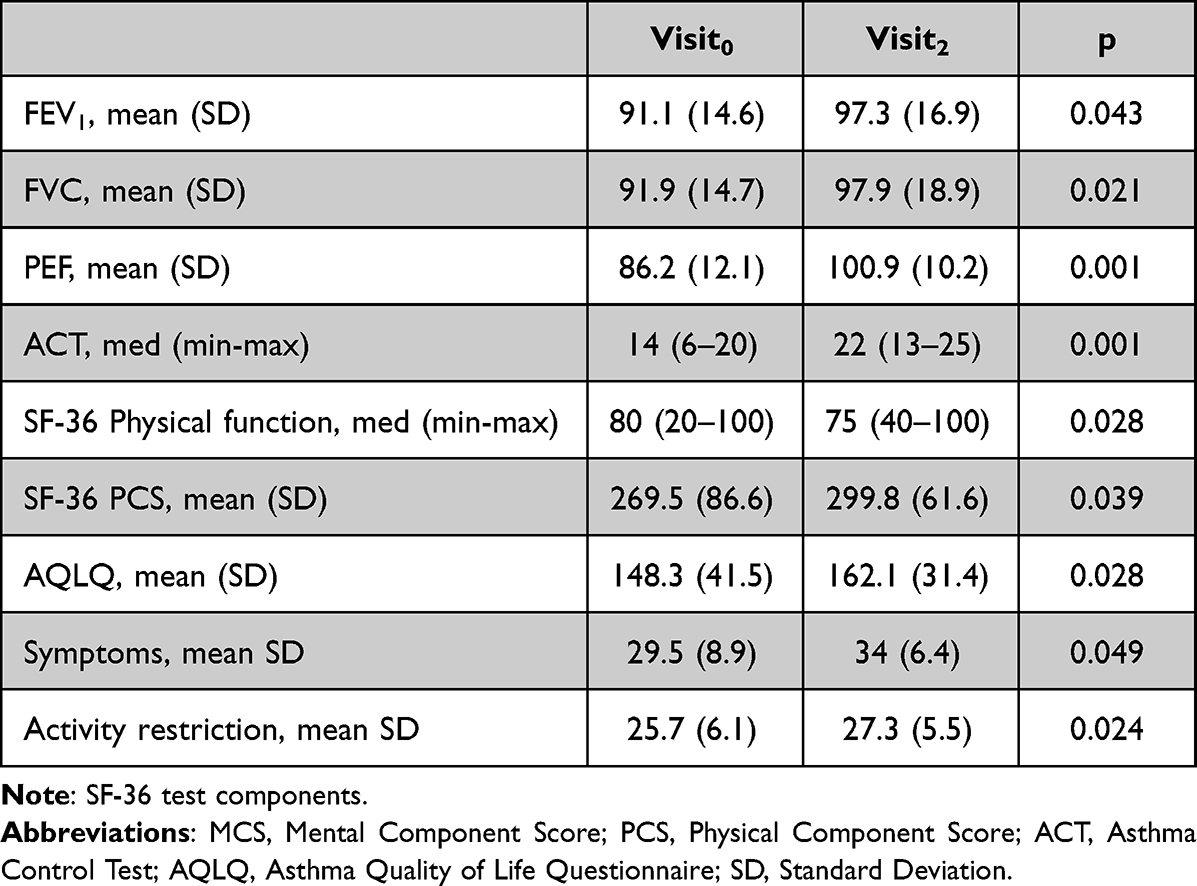 |
Table 6 1st Month Control Results of Those Who Started Treatment with Asthma Diagnosis (n=17) |
Discussion
Unfortunately, misdiagnosis of asthma is not uncommon.5,8 In the patient group participating in the study, over diagnosis was found to be 39%, supporting the literature. In our study, it was aimed to provide diagnostic guidance, to draw attention to PEF follow-up, and to determine the diagnostic efficacy of PEF variability measurement, especially in the patient group whose early reversibility could not be proven. We think that this study conducted before the pandemic will add value to PEF follow-up in cases where pulmonary function tests cannot be performed, such as pandemics. We think that wheezing is the most distinctive symptom for the diagnosis of asthma and FEF25-75 measurement is an important spirometric marker in the diagnosis of asthma in patients with symptoms compatible with asthma. As an ideal predictive value recommendation, we think that using a cut-off value of <15% PEF variability to exclude the diagnosis of asthma or ≥20% PEF variability to confirm the diagnosis would increase the diagnostic value.
A high prevalence of under and over diagnosis of asthma has been reported in the literature, with important consequences for patients and healthcare systems.8 José et al11 showed that 54% of patients were underdiagnosed and 34% were overdiagnosed with asthma in primary care. Gershon et al12 found that only 43% of patients diagnosed with asthma in Canada received a pre-diagnostic spirometric examination. Eguiluz-Gracia et al13 conducted a survey with 339 participants to assess asthma management during the pandemic. During this period, 62%, 76%, 66%, 76%, 76% and 87% of healthcare workers, respectively, reported that they did not use spirometry, impulse oscillometry, bronchodilator testing, FeNO or methacholine to diagnose asthma in adults. Furthermore, 73% of respondents reported that when they were first diagnosed with asthma, inhalation therapy was prescribed based on clinical parameters alone. Ambulatory peak expiratory flow (PEF) measurements were recommended for only 56% of asthma patients.10 In our study, similar to the literature, 39.2% of patients were diagnosed with over diagnosis of asthma despite a previous diagnosis of asthma.
Clinical use of standardised diagnostic algorithms and the development of new predictive biomarkers may help to reduce the prevalence of under diagnosis and over diagnosis of asthma.8 Both traditional methods and innovative alternative pulmonary function tests should be investigated for use during these periods.14 New digital health tools and mobile health technologies such as peak expiratory flow devices, electronic portable spirometers, portable exhaled nitric oxide meters, airwave oscillometry devices, and smart phone microphone spirometers have been proposed in the literature.14
In our study, no difference was found between the patient group with non-specific symptoms and the patient group with asthma in terms of symptom scores and quality of life questionnaires. Although the value of anamnesis in diagnosiswaswell recognised, it is important to assess patients’ perceptions of their symptoms. Accordingly, symptoms should be confirmed by objective tests and asthma diagnosis based on clinical parameters alone should be a thing of the past.
Spirometry-based reversibility testing and detection of peak expiratory flow (PEF) variability by PEF metre monitoring can be used to reveal variable airway restriction. However, it is often not possible to demonstrate variable airway restriction by early spirometry-based reversibility testing, especially in patients with mild asthma in whom asthma symptoms are not prominent or are intermittent.3 Diagnosis in this group is difficult and important due to studies on the rate of severe asthma attacks and mortality in patients with mild asthma.3,15,16
As emphasised in the guidelines, normal simple spirometric tests do not exclude the diagnosis of asthma.3,17 In this situation, the most objective measurement, its applicability and cut-off value remain unclear.6 Studies have showed that simple spirometry has a positive predictive value of 29% with a sensitivity of 53% and a negative predictive value of 77%.18 In a similar study, the sensitivity, positive predictive value and negative predictive value of pre- and post-bronchodilator spirometry for the diagnosis of asthma were reported to be 49%, 85% and 29%, respectively.9,17 In our study, there was no difference between the spirometrically diagnosed group and the non-specific symptomatic group in terms of baseline FEV₁, FVC, FEV₁/FVC, PEF ratios.
False negatives and false positives in the diagnosis of asthma can be reduced by performing direct and/or indirect mBPTs in individuals with asthma symptoms and normal respiratory examinations and spirometric tests.19–22 Direct mBPT is a more useful test to exclude rather than diagnose asthma. Its value is higher than its positive predictive value. However, mBPTis mostly performed in specialised centres and is not easily accessible as it requires expertise and equipment and can only be performed by trained professional health assistants. This test, which has a preliminary preparation and confirmation phase, is impractical and cannot be used in pandemic-like situations.9,20
PEF measurement using a portable handheld device is an inexpensive option recommended by guidelines for the diagnosis of asthma and occupational asthma.17 However, the optimal threshold for PEF variability remains unclear.8 Several studies have also showed that serial measurements in asymptomatic children can be useful for early diagnosis, especially in those with a family history.23 We believe that PEF measurements are valuable, reliable and more feasible in this and future life. With PEF measurements performed twice a day, daily PEF variability in healthy individuals was found to be 9% in adults and 12.3% in children with a 95% confidence limit.3
In our study, we found 100% sensitivity and 16.7% specificity when the threshold value of PEF variability in the diagnosis of asthma was a) >10%, b) 88.5% sensitivity and 62.5% specificity when it was >15%, and c) 61.5% sensitivity and 83.3% specificity when it was ≥20%. According to studies on the predictive value of PEF variability, after PEF monitoring with 5 measurements per day for 3 days in 100 stable asthmatic patients, a sensitivity of 64% and 51% and a specificity of 94.1% and 98.7% were found when the PEF variability threshold for the diagnosis of asthma was taken as 12.5% and 16.5%, respectively.24 Similarly, in a study involving 122 asthma patients in Denmark, the sensitivity and specificity of >20% PEF variability for the diagnosis of asthma were found to be 39% and 58%, respectively.25
We believe that the diagnostic yield for PEF variability increases with a cut-off value of <15% to exclude the diagnosis of asthma and ≥20% to confirm the diagnosis of asthma.
We believe that baseline FEF25-75 measurement abnormality is an independent predictive factor that may be a predictor of asthma diagnosis when simple spirometry is available. Despite similar results presented by many studies, we think that it has not yet been included in the guidelines because it does not have a specific predictive value. FVC values, FEF25-75 and mBPT PD20 were associated with FEV₁ (p < 0.001). It was found that those with lower FEF25-75 values (p < 0.001) were more likely to have a positive mBPT test and that FEF25-75 may be a predictive marker in newly diagnosed asthma. When the demographic data and SFTs of 829 asthmatic patients over 18 years of age included in the SARP study26 were analysed, low FEF25-75 was found to be an independent predictive factor for ICU admission, persistent symptoms, nocturnal symptoms, blood eosinophilia and AHR.26,27 The limitation of our study may be that the FeNO test was not included because a similar study comparing peripheral eosinophilia and the combination of FeNO and mBPT in BDR-negative patients was performed in our clinic. We recommend using this combination as an exclusion test.28
The limitation of our study is the small sample size. This leads to a small number of subgroups. Our goal is to increase this number of patients. This was not possible due to the pandemic. The need for optimal testing for the diagnosis of asthma continues. Improvement of studies should be our goal.
Conclusions
The best method for diagnosing asthma and its predictive value are still uncertain. This leads to the problem of over- and under-diagnosis, which can be misleading when the diagnosis is based on symptoms and the patient’s medical history. It is therefore important that variable airway obstruction is documented by objective diagnostic methods. Wheezing is a differential symptom for the diagnosis of asthma. In addition, FEF25-75 is an important predictive spirometric marker for the diagnosis of asthma in patients with symptoms compatible with asthma. The use of PEF meters should be promoted among specialists. We believe that the use of PEF variability with a threshold value of <15% to exclude the diagnosis of asthma or ≥20% to confirm the diagnosis will increase diagnostic yield.
Abbreviations
PEF, Peak Expiratory Flow; ACT, Asthma Control Test; PFT, Pulmonary Function Test; AQLQ, Asthma Quality of Life Questionnaires; SF36, Short Form 36; mBPT, Methacholin Bronchial Provocation Test; PC, Provocative Concentration; SAD, Small Airway Dysfunction.
Ethics Approval
We declare that our work is in conformity with the Declaration of Helsinki. Our study was approved by the ethics committee of Health Sciences University Kecioren Training and Research Hospital.
Funding
The authors did not receive support from any organization for the submitted work.
Disclosure
The authors have no relevant financial or non-financial interests to disclose for this work.
References
1. 2022 WHO Asthma Fact Sheet; 2022. Available from: http://www.who.int/mediacentre/factsheets/fs307/en.
2. Thorat Y, Sundeep SS, Rahul RK. Peak flow meter with a questionnaire and mini-spirometer to help detect asthma and COPD in real-life clinical practice: a cross-sectional study npj primary care respiratory. Medicine. 2017;27:32. doi:10.1038/s41533-017-0036-8
3. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention; 2023 Available from: http://www.ginasthma.org/.Gına2023.
4. Çelik G. Türk Toraks derneği, Astım Tanı ve Tedavi Rehberi 2020 Güncellemesi; 2020.
5. Aaron SD, Boulet LP, Reddel HL, et al. Underdiagnosis and over diagnosis of asthma. Am J RespirCrit Care Med. 2018;198(8):1012–1020. doi:10.1164/rccm.201804-0682CI
6. Ulrik CS, Postma DS, Backer V. Recognition of asthma in adolescents and young adults: which objective measure is best? J Asthma. 2005;42:549–554. doi:10.1080/02770900500215715
7. Goldstein MF, Veza BA, Dunsky EH, et al. Comparisons of peak diurnal expiratory flow variation, postbronchodilator FEV1 responses, and methacholine inhalation challenges in the evaluation of suspected asthma. Chest. 2001;119(4):1001–1010. doi:10.1378/chest.119.4.1001
8. Renaud L, Imran S, Inigo O, et al. European Respiratory Society Guidelines for the Diagnosis of Asthma in Adults. Eur Respir J. 2022;15:2101585. doi:10.1183/13993003.01585-2021
9. Virant FS, Randolph C, Nanda A, et al. Pulmonary procedures during the COVD-19 pandemic: a Workgroup Report of the American Academy of Allergy, Asthma, and Immunology (AAAAI) Asthma Diagnosis and Treatment (ADT) Interest Section. J Allergy Clin Immunol Pract. 2022;10(6):1474–1484. doi:10.1016/j.jaip.2022.02.044
10. National Institute for Health and Care Excellence. Asthma: diagnosis, monitoring and chronic asthma management. NICE Guideline NG80. Available from: www.nice.org.uk/guidance/ng80/2021.
11. Jose BP, Camargos PA, Cruz Filho AA, Correa RA. Diagnostic accuracy of respiratory diseases in primary health units. Rev Assoc Med Bras. 2014;60(6):599–612. doi:10.1590/1806-9282.60.06.021
12. Gershon A, Victor C, Guan J, et al. Pulmonary function testing in the diagnosis of asthma: a population studyChest. Chest. 2012;141(5):1190–1196. doi:10.1378/chest.11-0831
13. Eguiluz-Gracia I, Berge M, Boccabella C, et al. Real-life impact of COVID-19 pandemic lockdown on the management of pediatric and adult asthma: a survey by the EAACI Asthma Section. Allergy. 2021;76:2776–2784.
14. Kouri A, Gupta S, Yadollahi A, et al. Addressing reduced laboratory-based pulmonary function testing during a pandemic. Chest. 2020;158(6):2502–2510. doi:10.1016/j.chest.2020.06.065
15. Helen R, FitzGerald M, Bateman E. GINA 2019: a fundamental change in asthma management: treatment of asthma with short-acting bronchodilators alone is no longer recommended for adults and adolescents EurRespir. Euro Respir J. 2019;53(6):1901046. doi:10.1183/13993003.01046-2019
16. Bateman E, O’Byrne P, FitzGerald JM. Positioning as-needed budesonide-formoterol for mild asthma: effect of prestudy treatment in pooled analysis of SYGMA 1 and 2. Ann Am Thorac Soc. 2021;18(12):2007–2017. doi:10.1513/AnnalsATS.202011-1386OC
17. Hunter CJ, Brightling CE, Woltmann G, et al. A comparison of the validity of different diagnostic tests in adults with asthma. Chest. 2002;121(4):1051–1057. doi:10.1378/chest.121.4.1051
18. Schneider A, Gindner L, Tilemann L, et al. Diagnostic accuracy of spirometry in primary care. BMC Pulm Med. 2009;9(1):31. doi:10.1186/1471-2466-9-31
19. Coates AL, Wanger J, Cockcroft DW, et al. ERS technical standard on bronchial challenge testing: general considerations and performance of methacholine challenge tests. Euro Respir J. 2018;52:1801033. doi:10.1183/13993003.01033
20. Drake S, Wang R, Healy L, et al. Diagnosing asthma with and without aerosol-generating procedures. J Allergy Clin Immunol Pract. 2021;9(12):4243–4251. doi:10.1016/j.jaip.2021.07.006
21. Cockcroft DW. Direct challenge tests: airway hyperresponsiveness in asthma: its measurement and clinical significance. Chest. 2010;138(2):18–24. doi:10.1378/chest.10-0088
22. Anderson SD. İndirect challenge tests: airway hyperresponsiveness in asthma: its measurement and clinical significance. Chest. 2010;138(2):25–30. doi:10.1378/chest.10-0116
23. Mehta B, Bhandari B, Singhal A, et al. Screening asymptomatic school children for early asthma by determining airway narrowing through peak expiratory flow rate measurement. J Edu Health Promot. 2020;9:72.
24. Aggarwal Augusta ND, Kumar V, Kumar V, et al. Assessment of diurnal variability of peak expiratory flow in stable asthmatics. Journal of Asthma. 2002;39(6):487–491. doi:10.1081/JAS-120004911
25. Backer V, Sverrild A, Ulrik CS, et al. Diagnostic work-up in patients with possible asthma referred to a university hospital. European Clinical Respiratory Journal. 2015;2(1):27768. doi:10.3402/ecrj.v2.27768
26. Riley CM, Wenzel SE, Castro M, et al. Clinical implications of having reduced mid forced expiratory flow rates (FEF25-75), Independently of FEV₁, in adult patients with asthma. PLoS One. 2015;10(12):e0145476. doi:10.1371/journal.pone.0145476
27. Postma DS, Brightling C, Baldi S, et al. Exploring the relevance and extent of small airways dysfunction in asthma (ATLANTIS): baseline data from a prospective cohort study. Lancet Respir Med. 2019;7(5):402–416. doi:10.1016/S2213-2600(19)30049-9
28. Koca Kalkan İ, Köycü Buhari G, Ateş H. Can fractional exhaled nitric oxide with blood eosinophil count have a place in the diagnostic algorithm for asthma? Asthma Allergy Immunology. 2021;19(2):100–109. doi:10.21911/aai.643
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.