Back to Journals » Breast Cancer: Targets and Therapy » Volume 14
Weekly vs Every-3-Week Carboplatin with Weekly Paclitaxel in Neoadjuvant Chemotherapy for Triple-Negative Breast Cancer: A Retrospective Analysis
Authors Landry KK ![]() , Lyon JL, Victoria KE, Changizzadeh PN, Cole BF, Pulluri B
, Lyon JL, Victoria KE, Changizzadeh PN, Cole BF, Pulluri B ![]() , Sikov WM
, Sikov WM ![]() , Wood ME
, Wood ME
Received 9 November 2021
Accepted for publication 4 February 2022
Published 15 March 2022 Volume 2022:14 Pages 63—70
DOI https://doi.org/10.2147/BCTT.S342635
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Pranela Rameshwar
Kara K Landry,1 Jessica L Lyon,2 Kitty E Victoria,1 P Nick Changizzadeh,3 Bernard F Cole,4 Bhargavi Pulluri,5 William M Sikov,6 Marie E Wood1
1Division of Hematology and Oncology, Department of Medicine, University of Vermont Medical Center, Burlington, VT, USA; 2Larner College of Medicine at the University of Vermont, Burlington, VA, USA; 3Hematology and Oncology, Eastern Connecticut Hematology and Oncology, Norwich, CT, USA; 4College of Engineering and Mathematical Sciences, University of Vermont, Burlington, VA, USA; 5Division of Hematology and Oncology, Saint Agnes Hospital, Baltimore, MD, USA; 6Women and Infants Hospital of Rhode Island, Program in Women’s Oncology, and Warren Alpert Medical School of Brown University, Providence, RI, USA
Correspondence: Marie E Wood, Department of Medicine, Division of Hematology and Oncology, University of Vermont Medical Center, 111 Colchester Avenue, Burlington, VA, 05401, USA, Tel +1 802-847-8400, Email [email protected]
Background: Adding carboplatin to weekly paclitaxel as part of neoadjuvant chemotherapy (NACT) for stage II–III triple negative breast cancer (TNBC) has been shown to significantly increase the pathologic complete response (pCR) rate. Hematologic toxicities associated with every 3-week dosing of carboplatin have led some oncologists to explore weekly dosing as an alternative, but there are little published data comparing the two dosing schedules.
Methods: We performed a retrospective analysis of patients who received paclitaxel and carboplatin, usually followed by AC, as initial NACT for TNBC at two academic cancer centers between 2008 and 2018 for whom pathologic results and post-operative follow-up were available. We recorded pCR, defined as ypT0/isN0, treatment delivery and disease-free survival, censored as of the patient’s last follow-up visit.
Results: A total of 76 patients were identified (median age 49 years). A total of 47 received weekly carboplatin, of whom 83% received at least 11 of 12 planned doses, and 29 received every 3-week carboplatin, of whom 90% received all 4 planned doses. pCR rates were similar, 53% with weekly and 55% with every 3-week carboplatin dosing. At median follow-up of 18 months (range < 1– 118), 93% of patients who achieved pCR were alive and free from recurrence, compared to 74% of those who did not.
Conclusion: pCR rates were similar between patients receiving weekly or every 3-week carboplatin and were similar to those reported in prior trials with carboplatin. These data suggest that providers can choose either weekly or every 3-week carboplatin dosing without compromising the likelihood of achieving pCR.
Keywords: triple negative breast cancer, neoadjuvant treatment, carboplatin dosing, chemotherapy
Introduction
Breast cancers are typically categorized by their expression of estrogen and progesterone receptors (ER, PR) and the presence or absence of human epidermal growth factor receptor 2 (HER2) gene amplification.1 Those without any of these markers are referred to as triple-negative breast cancers (TNBC), which accounts for approximately 10–15% of all breast cancers. TNBC is more common in women who carry germline mutations in BRCA1, comprising 70–80% of breast cancers that develop in such patients, though BRCA mutations are detected in less than 20% of patients diagnosed with TNBC, and is seen more commonly in women of African or Hispanic descent. This subtype is associated with a worse prognosis and, when diagnosed without overt metastatic disease, a higher risk of early relapse. In the absence of molecular targets that guide treatment of other breast cancer subtypes, current optimal treatment for non-metastatic TNBC is cytotoxic chemotherapy, typically sequential or concurrent administration of an anthracycline-based regimen such as doxorubicin or epirubicin and cyclophosphamide (AC or EC) and a taxane [2, 3]. With regard to the choice of taxane and dosing schedule, the E1199 study demonstrated that weekly paclitaxel was more effective than either every 3-week paclitaxel or weekly or every 3-week docetaxel following AC as adjuvant therapy for node-positive TNBC.2
Gene expression analysis reveals heterogeneity within TNBC, with one group of investigators identifying at least six subtypes that appear to differ by response to treatment.3 However, one characteristic shared by a majority of TNBC, whether associated with an identifiable BRCA mutation or not, is impairment of DNA repair by homologous recombination, also referred to as homologous recombination deficiency (HRD).4 While this defect presumably plays a role in development of the malignancy, it also renders the cancer cells more vulnerable to DNA-damaging chemotherapeutic agents. While many of the agents used to treat TNBC target DNA (excluding the taxanes), employing platinum-based antineoplastic therapies, which create DNA crosslinks that can lead to double-stranded DNA breaks, has been of particular interest.
In patients with non-metastatic TNBC, achievement of a pathologic complete response (pCR) with neoadjuvant chemotherapy (NACT), usually defined as the absence of residual invasive disease in the breast and sampled axillary nodes (ypT0/isN0), is associated with large improvements in long-term outcomes compared to patients with residual invasive disease. In a recently updated meta-analysis, TNBC patients who attained pCR were found to have an 82% improvement in event-free survival (EFS) and an 80% improvement in overall survival (OS) compared to patients with residual invasive disease at surgery.5–10 However, in large, multicenter neoadjuvant trials, sequential administration of weekly paclitaxel and AC or EC typically yields pCRs in less than one-third of patients.11–15 As a result, clinical trials have investigated a variety of approaches to try to increase the pCR rate in TNBC, including several studies that focused on incorporation of platinum agents, more commonly carboplatin, into NACT for TNBC. These studies have demonstrated significantly improved pCR rates (~50–60%) with the addition of carboplatin, and one trial has reported significant improvement in disease-free survival among patients treated with carboplatin compared to those who did not receive this agent.11,12,16,17
Given the compelling evidence supporting the inclusion of carboplatin into NACT regimens, clinical trials have included both weekly or every 3-week carboplatin regimen, but a direct comparison between these two dosing schedules on achieving a pCR has not been studied in a randomized trial. Thus, our current study aims to evaluate pCR rates in TNBC associated with the neoadjuvant use of weekly carboplatin dosing (with an area-under-the-curve (AUC) of 2) versus every 3-week dosing (AUC of 6) at two institutions to compare their efficacy in real-world settings.
Patients and Methods
This is a retrospective review of women treated with neoadjuvant chemotherapy for TNBC at either the University of Vermont (UVM) or Women and Infants Hospital of Rhode Island (WIHRI), a teaching hospital for the Warren Alpert Medical School of Brown University. Women were eligible to be included if they were treated between 2008 and 2018, received neoadjuvant chemotherapy with carboplatin weekly or every 3 weeks in addition to weekly paclitaxel prior to any other chemotherapy and had pathology reports available from their definitive surgery. The study was IRB approved at both institutions.
Chart review was performed for all patients meeting eligibility criteria. Charts were reviewed for age, date at diagnosis, date of first treatment, clinical stage, tumor size and grade at diagnosis, nodal involvement, ER and PR receptor expression, HER2 status as determined by immunohistochemical stain or fluorescent-in-situ-hybridization, BRCA mutation status, and dosing and modifications for all chemotherapy administered. We also recorded date of surgery, whether or not a pCR was achieved, and pathologic stage at surgery.
Date of last follow-up and months since surgery were determined as well as disease status at follow-up, including any reported distant or local recurrences and whether the patient was alive or deceased. A patient was considered operable if her baseline clinical stage was Ia-IIIa and inoperable if her baseline clinical stage was IIIb-c. For the purposes of this study, pCR was defined as ypT0/isN0. Disease-free survival (DFS) was censored as of last oncologic follow-up visit. After both institutions completed chart reviews, their data was combined.
Statistical Analysis
Statistical analyses were conducted with particular attention aimed at the differences in outcomes between women receiving weekly (AUC2) versus every 3-week (AUC6) carboplatin dosing. pCR rates were defined as the ratio of the responders to the total evaluable patients in each group. 95% confidence intervals were based on exact methods using the binomial distribution. Comparison of pCR rates was performed using Fisher’s exact test. Analyses were performed using Stata version 16.1 (StataCorp LLC, College Station, TX).
Results
Seventy-six women met eligibility criteria and were included in the analysis (26 from UVM and 50 from WIHRI). The mean age for this cohort was 49 years (range 25–76), 69 women (91%) had operable disease (Stage IA-IIIA) prior to initiation of neoadjuvant chemotherapy, and 46% were lymph node positive at diagnosis. One patient with stage IV disease due to ipsilateral cervical lymph node involvement was included, as she was treated with curative intent. The majority (69/76, or 91%) of women had tumors with ER expression of <1%. Sixty-three women had undergone genetic testing of which 9 (14%) were found to have a pathogenic mutation in BRCA 1 or BRCA 2. Forty-seven (62%) of the women received weekly carboplatin dosing, of whom 83% received at least 11 of 12 planned doses, and 29 (38%) received every 3-week carboplatin dosing, of whom 90% received all 4 planned doses. Patients receiving weekly carboplatin were more likely to be clinically node negative (48% vs 62%), inoperable (29.8% vs 6.9%), BRCA negative (76.6% vs 62%) or weakly ER positive as defined as ER expression of 1–10% (12.8% vs 3.4%), though none of these differences reached statistical significance in this relatively small patient group (see Table 1). The average age of participants was similar between the two groups, at 47 years of age for the weekly carboplatin group and 48 years of age for the every 3-week group. Rates of completing >90% of planned doses of weekly paclitaxel were similar in the two groups (89% in the weekly carboplatin cohort vs 90% in the every 3-week carboplatin cohort). All patients subsequently received doxorubicin and cyclophosphamide (AC) prior to surgery, with the exception of 4 patients in the weekly carboplatin cohort. In the every 3-week carboplatin cohort, 13 patients also received bevacizumab on an open label study, two may have received bevacizumab (vs placebo) on a blinded clinical trial, and 3 may have received veliparib or atezolizumab (vs placebo) on blinded clinical trials. Median follow-up for this cohort was 18 months (range <1 – 118). Median follow-up was shorter (13 months) for the cohort receiving weekly carboplatin compared to the cohort receiving every 3-week carboplatin (53 months), reflecting the transition to greater use of the weekly dosing schedule in the latter portion of our timespan. See Table 1 for additional details of the characteristics of our patient group and the two cohorts.
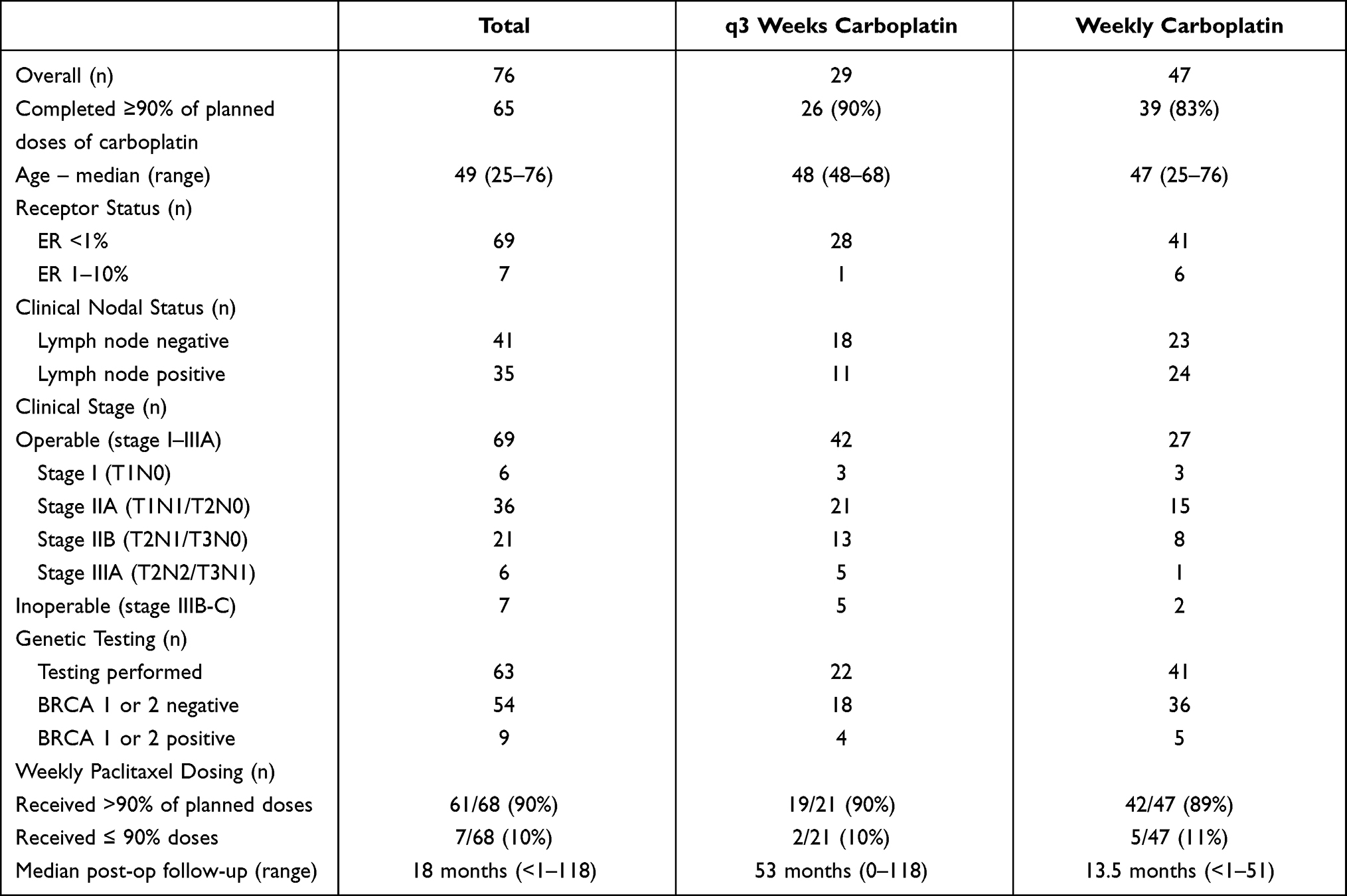 |
Table 1 Patient Characteristics |
The majority (41/76 or 54%) of all women in our review achieved pCR (see Table 2). Rates of achieving a pCR did not differ significantly between those receiving weekly carboplatin (53% [95% CI 38–68%]) and those who received every 3-week carboplatin (55% [95% CI 36–74%]) (p > 0.99). pCR rates were higher among women with operable disease (39/69, 57%) than in women with inoperable disease (2/7, 29%), and among women who were node negative at baseline (68%) versus node positive (37%). Eight of 9 (89%) women with a germline BRCA mutation achieved a pCR, compared to 67% (36/54) of women known to be negative for a BRCA mutation. Among 13 patients who definitely received bevacizumab along with every 3-week carboplatin, 9 (69%) achieved pCR; excluding these patients, and those who may have received bevacizumab on a blinded trial, the pCR rate for every 3-week carboplatin drops to 6/14 (43%).
 |
Table 2 Pathologic Complete Response (pCR)* Rates by Every 3-Weeks versus Weekly Dosing of Carboplatin |
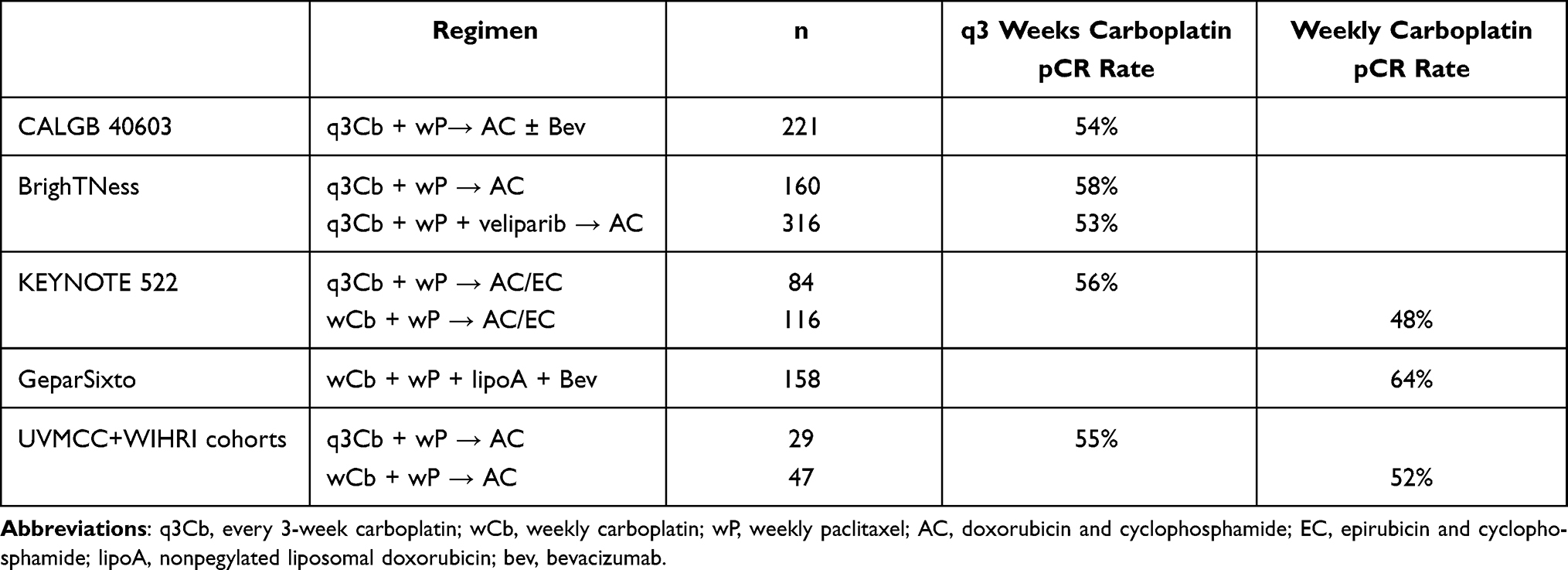 |
Table 3 Variations of Carboplatin Dosing in Neoadjuvant Treatment of Breast Cancer and Reported pCR Rates |
Among 35 patients who failed to achieve pCR, residual disease stage in the breast and nodes was as follows: Stage IB – 17; Stage IIA – 11; Stage IIB – 1; Stage IIIB – 3; Stage IIIC – 2; Stage IV – 1.
At median follow-up of 18 months (range <1–118), 93% (38/41) of patients who achieved a pCR were free from recurrence, compared to 74% (26/35) of women who did not achieve a pCR. As of last oncologic follow-up, 81% (38/37) of patients in the weekly carboplatin cohort and 90% (26/29) of patients in the every 3-week cohort were free from recurrence, but median follow-up for the latter group was much longer (53 months vs 13.5 months). Among patients with operable disease, 85% (28/33) of patients in the weekly carboplatin cohort and 92% (25/27) of patients in the every 3-week cohort were free from recurrence at follow-up. Nine of the 61 (15%) patients who received >90% of planned doses of weekly paclitaxel and 1 of the 7 (14%) patients who received ≤90% of planned doses of weekly paclitaxel had recurrence of their disease during follow-up.
Discussion
In this retrospective analysis of women receiving neoadjuvant treatment for TNBC we identified similar rates of pCR with weekly (AUC2) or every 3-week (AUC6) carboplatin combined with weekly paclitaxel and usually followed by AC. Patients in the every 3-week carboplatin cohort who received bevacizumab (in the setting of a clinical trial) were more likely to achieve pCR than those who did not, but since no patients in the weekly cohort received bevacizumab it is difficult to determine how this may have influenced our overall findings, and it is unlikely that further data will become available to clarify this issue as bevacizumab is no longer being evaluated in the neoadjuvant setting in TNBC. The pCR rate was higher for women with operable disease (stage I–IIIA), node negative disease and pathogenic BRCA mutations. Recurrence-free survival among the two cohorts was similar.
In the treatment of TNBC, anthracycline and taxane-based regimens have been the mainstay of treatment. As shown in Table 3, recent studies have shown that the addition of carboplatin in the neoadjuvant setting improves pCR rates.11,12,17 However, the dosing of carboplatin used in these studies varies. In the GeparSixto trial, 315 patients with TNBC were randomly assigned to receive weekly carboplatin (AUC 2.0, subsequently reduced to 1.5 due to excessive hematologic toxicity at the original dose) versus no carboplatin in addition to weekly paclitaxel and nonpegylated liposomal doxorubicin and every 3-week bevacizumab. pCR rates were higher in patients assigned to receive carboplatin, but the rate of hematologic toxicities was also significantly higher. Additionally, early treatment discontinuation because of toxicity was more common (49% in carboplatin arm vs 36% in control arm). Similarly, in the Phase II CALGB 40603 (Alliance) trial, patients (n = 443) with stage II–III TNBC were randomized to the addition of carboplatin and/or bevacizumab to standard neoadjuvant chemotherapy. This trial utilized an every 3-week schedule at AUC 6. Again, the addition of carboplatin increased the pCR rate, from 41% to 54%, but patients assigned to receive carboplatin were also more likely to miss chemotherapy doses and to require dose reductions because of hematologic toxicity. The impact of hematologic toxicities on treatment delivery in a subset of patients treated on CALGB 40603 was magnified by the study’s requirement that missed doses not be made up; as a result, approximately one-third patients on the carboplatin arms received <11 of the 12 planned doses of weekly paclitaxel; compared to patients who received treatment as planned, these patients had an inferior pCR rate (44% vs 61%) and far inferior event-free survival.18 The BrighTNess trial was designed to assess the addition of a PARP inhibitor and carboplatin or carboplatin alone to standard neoadjuvant chemotherapy in TNBC.12 Similar to the CALGB 40603 trial, carboplatin dosing was every 3-weeks at AUC 6. The addition of carboplatin improved the pCR rate from 31% to 58%, while the addition of the PARP inhibitor failed to further improve the pCR rate. In contrast to CALGB 40603, on BrighTNess treatment delays were permitted during weekly paclitaxel ± carboplatin and, as a result, a much higher proportion of patients received all planned treatment, which may explain the higher overall pCR rate in patients assigned to carboplatin. Given the high rates of treatment delivery in our retrospective analysis, it is highly likely that the oncologists treating TNBC at our centers followed the BrighTNess example of allowing treatment delays in an effort to administer all planned treatments.
Few studies have directly compared weekly to every 3-week carboplatin in the treatment of neoadjuvant TNBC. The recently published Phase III KEYNOTE 522 trial,19 which examined the effect of adding neoadjuvant pembrolizumab on pCR rates and event-free survival in TNBC, allowed treating physician to choose to treat their patients with either every 3-week carboplatin (42%) or weekly carboplatin (58%). While the study was not designed to compare carboplatin dosing, it is interesting to note that on the placebo arm (not receiving pembrolizumab), the pCR rate was slightly higher among patients receiving every 3-week versus weekly carboplatin (56.0% vs 48.3%), while among patients who also received pembrolizumab pCR rates were similar between every 3-week (64%) and weekly (67%) carboplatin. As in CALGB 40603, KEYNOTE-522 did not permit treatment delays for toxicity. As a result, 22% of their patients received <10 of the planned 12 doses of weekly paclitaxel; in these patients pCR rates were lower (36% with placebo, 51% with pembrolizumab) than in patients who received at least 10 doses of weekly paclitaxel (55% with placebo, 70% with pembrolizumab). Unfortunately, a comparison of missed doses between the two carboplatin dosing schedules has not been reported. These results highlight the need for a formal comparison of weekly versus every 3-week administration. While our present study found similar overall pCR rates to those reported in prior studies, we did not find a difference in pCR rates between those receiving weekly vs every 3-week carboplatin. To our knowledge, this is the first study to focus on outcomes associated with differing carboplatin doses in the treatment of TNBC, and our findings support the use of either a weekly or every 3-week regimen. However, given that our study is a small retrospective analysis, and the KEYNOTE 522 trial does not plan to do a comparison of outcomes between physician-selected carboplatin dosing schedules, a larger study would be necessary to determine the optimal dosing schedule for carboplatin in this setting.
The addition of carboplatin to conventional neoadjuvant therapy does increase hematologic toxicities, leading to dose reductions and delays in treatment. Data comparing toxicities associated with weekly versus every 3-week dosing of carboplatin are limited. A randomized multicenter phase III study comparing weekly versus every 3-week carboplatin plus paclitaxel in patients with advanced ovarian cancer demonstrated less severe cytopenias, febrile neutropenia, renal toxicity and neuropathy in the cohort receiving weekly treatments. However, in this study, paclitaxel dosing was also every week versus every 3-week, confounding our ability to directly compare the effects of carboplatin dosing.20 Prior studies have also demonstrated a relationship between carboplatin dosing and toxicity,21 although these studies typically used higher doses than are used in the treatment of TNBC. As noted previously, many oncologists appear to prefer weekly dosing as demonstrated by choices made in the KEYNOTE-522 trial, with 58% of patients receiving weekly carboplatin.19
In our cohort, pCR was associated with having operable disease or a pathogenic mutation in BRCA. In both GeparSixto and BrighTNess, patients with a BRCA mutation had higher overall pCR rates than BRCA-negative patients, but the increase in the pCR rates with the addition of carboplatin was smaller in BRCA-mutated versus BRCA-wild type. For example, in BrighTNess, the pCR rate in BRCA-mutated patients was 41% without carboplatin and rose to 50% with carboplatin, while it increased from 29% to 59% with the addition of carboplatin in BRCA-wild type. In contrast, a recent meta-analysis that included seven studies comprising over 800 TNBC patients showed that the addition of platinum to chemotherapy regimens in the neoadjuvant setting increased the pCR rate in BRCA mutated by more than that seen in BRCA-wild-type TNBC patients, though this did not achieve statistical significance.22 Given the increased toxicities associated with the addition of carboplatin, regardless of dosing, identifying patients that are most likely to benefit from its addition may help minimize unnecessary toxicities to patients who are less likely to do so.
There are limitations to our study that should be acknowledged. As stated above, our study is relatively small and retrospective. It is important to note, however, that our study comprised data from two large academic institutions in New England, thus potentially making our results representative of practice patterns in this region. Moreover, the addition of carboplatin to standard breast cancer regimens is associated with increased, mainly hematologic, toxicities that can lead to treatment delays, dose reductions and even early treatment discontinuation.11,12,17 Toxicities may guide the selection of treatment regimens; however, our study did not assess the provider’s reasoning for choice of dosing regimen or toxicity data. Such studies would provide additional information for oncologists making treatment decisions in this setting. Lastly, our follow-up interval was short (median follow-up 18 months), so our ability to assess the impact of the alternative carboplatin dosing schedules on DFS is limited.
Conclusion
We have shown that pCR rates are similar for weekly and every 3-week carboplatin when given with weekly paclitaxel in the neoadjuvant treatment of TNBC. Higher rates of pCR were seen for women with operable disease and BRCA mutation carriers. Our findings support the assertion that providers can choose either weekly or every 3-week carboplatin dosing without compromising the likelihood of achieving pCR. Further research is needed, however, to confirm these findings, assess the impact on longer-term outcomes and explore differences in toxicity and tolerability of these two regimens.
Ethics Approval
This research study was conducted retrospectively from data obtained for clinical purposes and was approved at both institutions by the Women and Infants Hospital of Rhode Island IRB and the University of Vermont Medical Center IRB. All data accessed complied with relevant data protection and privacy regulations.
Consent
For this type of study, formal consent is not required.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Dr Bernard F Cole reports personal fees from Frontier Science and Technology Research Foundation and Epizyme, Inc., outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Fan C, Oh DS, Wessels L, et al. Concordance among gene-expression-based predictors for breast cancer. N Engl J Med. 2006;355(6):560–569. doi:10.1056/NEJMoa052933
2. Sparano JA, Zhao F, Martino S, et al. Long-term follow-up of the E1199 Phase III trial evaluating the role of taxane and schedule in operable breast cancer. J Clin Oncol. 2015;33(21):2353–2360. doi:10.1200/JCO.2015.60.9271
3. Lehmann BD, Bauer JA, Chen X, et al. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J Clin Invest. 2011;121(7):2750–2767. doi:10.1172/JCI45014
4. Badve S, Dabbs DJ, Schnitt SJ, et al. Basal-like and triple-negative breast cancers: a critical review with an emphasis on the implications for pathologists and oncologists. Mod Pathol. 2011;24(2):157–167. doi:10.1038/modpathol.2010.200
5. Liedtke C, Mazouni C, Hess KR, et al. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J Clin Oncol. 2008;26(8):1275–1281. doi:10.1200/JCO.2007.14.4147
6. Guarneri V, Broglio K, Kau SW, et al. Prognostic value of pathologic complete response after primary chemotherapy in relation to hormone receptor status and other factors. J Clin Oncol. 2006;24(7):1037–1044. doi:10.1200/JCO.2005.02.6914
7. Ring AE, Smith IE, Ashley S, Fulford LG, Lakhani SR. Oestrogen receptor status, pathological complete response and prognosis in patients receiving neoadjuvant chemotherapy for early breast cancer. Br J Cancer. 2004;91(12):2012–2017. doi:10.1038/sj.bjc.6602235
8. Colleoni M, Viale G, Zahrieh D, et al. Chemotherapy is more effective in patients with breast cancer not expressing steroid hormone receptors: a study of preoperative treatment. Clin Cancer Res. 2004;10(19):6622–6628. doi:10.1158/1078-0432.CCR-04-0380
9. Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164–172. doi:10.1016/S0140-6736(13)62422-8
10. Spring LM, Fell G, Arfe A, et al. Pathologic complete response after neoadjuvant chemotherapy and impact on breast cancer recurrence and survival: a comprehensive meta-analysis. Clin Cancer Res. 2020;26(12):2838–2848. doi:10.1158/1078-0432.CCR-19-3492
11. Sikov WM, Berry DA, Perou CM, et al. Impact of the addition of carboplatin and/or bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense doxorubicin and cyclophosphamide on pathologic complete response rates in stage II to III triple-negative breast cancer: CALGB 40603 (Alliance). J Clin Oncol. 2015;33(1):13–21. doi:10.1200/JCO.2014.57.0572
12. Loibl S, O’Shaughnessy J, Untch M, et al. Addition of the PARP inhibitor veliparib plus carboplatin or carboplatin alone to standard neoadjuvant chemotherapy in triple-negative breast cancer (BrighTNess): a randomised, Phase 3 trial. Lancet Oncol. 2018;19(4):497–509. doi:10.1016/S1470-2045(18)30111-6
13. Rugo HS, Olopade OI, DeMichele A, et al. Adaptive randomization of veliparib-carboplatin treatment in breast cancer. N Engl J Med. 2016;375(1):23–34. doi:10.1056/NEJMoa1513749
14. Nanda R, Liu MC, Yau C, et al. Effect of pembrolizumab plus neoadjuvant chemotherapy on pathologic complete response in women with early-stage breast cancer: an analysis of the ongoing Phase 2 adaptively randomized I-SPY2 trial. JAMA Oncol. 2020;6(5):676–684. doi:10.1001/jamaoncol.2019.6650
15. Untch M, Jackisch C, Schneeweiss A, et al. Nab-paclitaxel versus solvent-based paclitaxel in neoadjuvant chemotherapy for early breast cancer (GeparSepto-GBG 69): a randomised, phase 3 trial. Lancet Oncol. 2016;17(3):345–356. doi:10.1016/S1470-2045(15)00542-2
16. Sirohi B, Arnedos M, Popat S, et al. Platinum-based chemotherapy in triple-negative breast cancer. Ann Oncol. 2008;19(11):1847–1852. doi:10.1093/annonc/mdn395
17. von Minckwitz G, Schneeweiss A, Loibl S, et al. Neoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG 66): a randomised phase 2 trial. Lancet Oncol. 2014;15(7):747–756. doi:10.1016/S1470-2045(14)70160-3
18. Sikov WM, Polley MY, Twohy E, et al. CALGB (Alliance) 40603: long-term outcomes (LTOs) after neoadjuvant chemotherapy (NACT) ± carboplatin (Cb) and bevacizumab (Bev) in triple-negative breast cancer (TNBC). J Clin Oncol. 2019;37:591. doi:10.1200/JCO.2019.37.15_suppl.591
19. Schmid P, Cortes J, Pusztai L, et al. Pembrolizumab for early triple-negative breast cancer. N Engl J Med. 2020;382(9):810–821. doi:10.1056/NEJMoa1910549
20. Pignata S, Scambia G, Katsaros D, et al. Carboplatin plus paclitaxel once a week versus every 3 weeks in patients with advanced ovarian cancer (MITO-7): a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2014;15(4):396–405. doi:10.1016/S1470-2045(14)70049-X
21. Colby C, Koziol S, McAfee SL, Yeap B, Spitzer TR. High-dose carboplatin and regimen-related toxicity following autologous bone marrow transplant. Bone Marrow Transplant. 2002;29(6):467–472. doi:10.1038/sj.bmt.1703417
22. Caramelo O, Silva C, Caramelo F, Frutuoso C, Almeida-Santos T. The effect of neoadjuvant platinum-based chemotherapy in BRCA mutated triple negative breast cancers -systematic review and meta-analysis. Hered Cancer Clin Pract. 2019;17:11. doi:10.1186/s13053-019-0111-y
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.