Back to Journals » Biologics: Targets and Therapy » Volume 20
Vunakizumab and Acitretin for Elderly Refractory Generalized Pustular Psoriasis: A Case Report and Comprehensive Literature Review
Authors Deng S, Jiang Y ![]() , Li W, Shu Z, Chen T, Liang J, Zhang X
, Li W, Shu Z, Chen T, Liang J, Zhang X ![]()
Received 27 December 2025
Accepted for publication 11 March 2026
Published 22 May 2026 Volume 2026:20 592069
DOI https://doi.org/10.2147/BTT.S592069
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shein-Chung Chow
Shilin Deng,1,2 Yu Jiang,1,2 Wei Li,1,2 Zhirong Shu,1,2 Tingnan Chen,1,2 Jingyao Liang,1,2 Xibao Zhang1,2
1Institute of Dermatology, Guangzhou Medical University, Guangzhou, 510095, People’s Republic of China; 2Department of Dermatology, Guangzhou Dermatology Hospital, Guangzhou, 510095, People’s Republic of China
Correspondence: Jingyao Liang, Institute of Dermatology, Guangzhou Medical University, Guangzhou, 510095, People’s Republic of China, Email [email protected] Xibao Zhang, Institute of Dermatology, Guangzhou Medical University, Guangzhou, 510095, People’s Republic of China, Email [email protected]
Abstract: Generalized pustular psoriasis (GPP) is a severe and potentially life-threatening form of psoriasis. Although spesolimab, an inhibitor of the interleukin (IL)-36 pathway, has been approved for the treatment of GPP, access to this agent remains limited. Vunakizumab, a humanized IgG1/κ monoclonal antibody that selectively neutralizes interleukin (IL)-17A inhibitors, is not yet approved for GPP. We herein report a 72-year-old male with a 40-year history of plaque psoriasis who developed GPP refractory to methotrexate combined with guselkumab and acitretin (20 mg/day). Following switching to vunakizumab (240 mg intravenously every 2 weeks) in combination with acitretin (40 mg/day), the patient achieved a GPPASI 75 response within 2 weeks and near-complete clearance (GPPASI ≈ 100) by week 12. Six induction doses of vunakizumab were administered, and acitretin was tapered to 20 mg/day for long-term maintenance. Throughout 36 weeks of follow-up, no disease relapse or drug-related adverse events were observed. This case, together with a review of the literature, provides support for IL-17A blockade combined with acitretin as a feasible and fast-acting regimen for refractory GPP in elderly patients.
Keywords: generalized pustular psoriasis, GPP, vunakizumab, acitretin, IL-17 inhibitors
Introduction
Generalized pustular psoriasis (GPP), also known as von Zumbusch psoriasis, is characterized by widespread pustules, systemic immune dysregulation and inflammation, and significant morbidity.1,2 As a rare subtype of psoriasis (accounting for 0.6–2.4%), it is marked by a high relapse rate and notable ethnic and geographical differences.3,4 A proportion of GPP cases harbors various genetic mutations, with IL36RN, CARD14, AP1S3, MPO, SERPINA3, BTN3A3, and MEFV identified as GPP-associated genes.5 Beyond these genetic predispositions, immunological dysregulation plays a pivotal role. For example, non-drug-induced GPP is characterized by upregulated expression of T helper 17 (TH17) cell-related genes.6
Treatment options for GPP can be classified into conventional therapies and biologic agents. Systemic treatment, particularly in severe cases, commonly employs acitretin as first-line monotherapy. For severe GPP, systemic therapy commonly utilizes acitretin as first-line monotherapy, given its proven efficacy in controlling pustular eruptions and systemic inflammation.7 Currently, interleukin-36 (IL-36) inhibitors (eg, spesolimab) are the only biologic agents approved globally for the management and prevention of GPP flares, offering targeted efficacy for acute exacerbations. Notably, Japan has approved a broad range of biological agents for the management of GPP, including interleukin-17 (IL-17) inhibitors (eg, secukinumab, brodalumab, ixekizumab, and bimekizumab),8 which thus provides more therapeutic options for local clinicians and patients. Additionally, with the continuous advancement of biological agents, vunakizumab, a novel-generation anti-IL-17A agent, has demonstrated consistent efficacy and favorable safety profiles in the treatment of moderate-to-severe chronic plaque psoriasis across various regions of China,9,10 which also serves as a potential key basis for its use in GPP treatment. However, high-quality evidence from randomized controlled trials (RCTs) to guide optimal treatment strategies remains scarce, particularly for refractory or complex cases. Thus, the management of GPP continues to pose a significant clinical challenge. In selected cases, combining biologic agents with a conventional systemic therapy (eg, acitretin) may represent a rational therapeutic strategy to enhance efficacy and reduce the risk of relapse.
In the present study, we report the successful resolution of GPP with the combination of vunakizumab and acitretin in an elderly male patient refractory to multiple conventional therapies. Additionally, we summarize the current literature to evaluate this combination strategy for the treatment of GPP in elderly patients.
Case Report
A 72-year-old male was admitted to the Department of Dermatology, our hospital, due to extensive pustular eruptions on an erythematous base that had persisted for six months. He had a 40-year history of plaque psoriasis, with no family history of psoriasis or other autoimmune diseases. Laboratory tests for systemic inflammation showed leukocytosis (5.38×109cells/L) with an elevated neutrophil percentage (NEUT%) of 76.20%, an accelerated erythrocyte sedimentation rate (ESR) of 55 mm/h, and an increased C-reactive protein (CRP) level of 30.39 mg/dL; these findings were accompanied by persistent fever (body temperature > 38 °C). The patient was diagnosed with GPP based on clinical manifestations and histopathological examination (Figure 1A and B).11
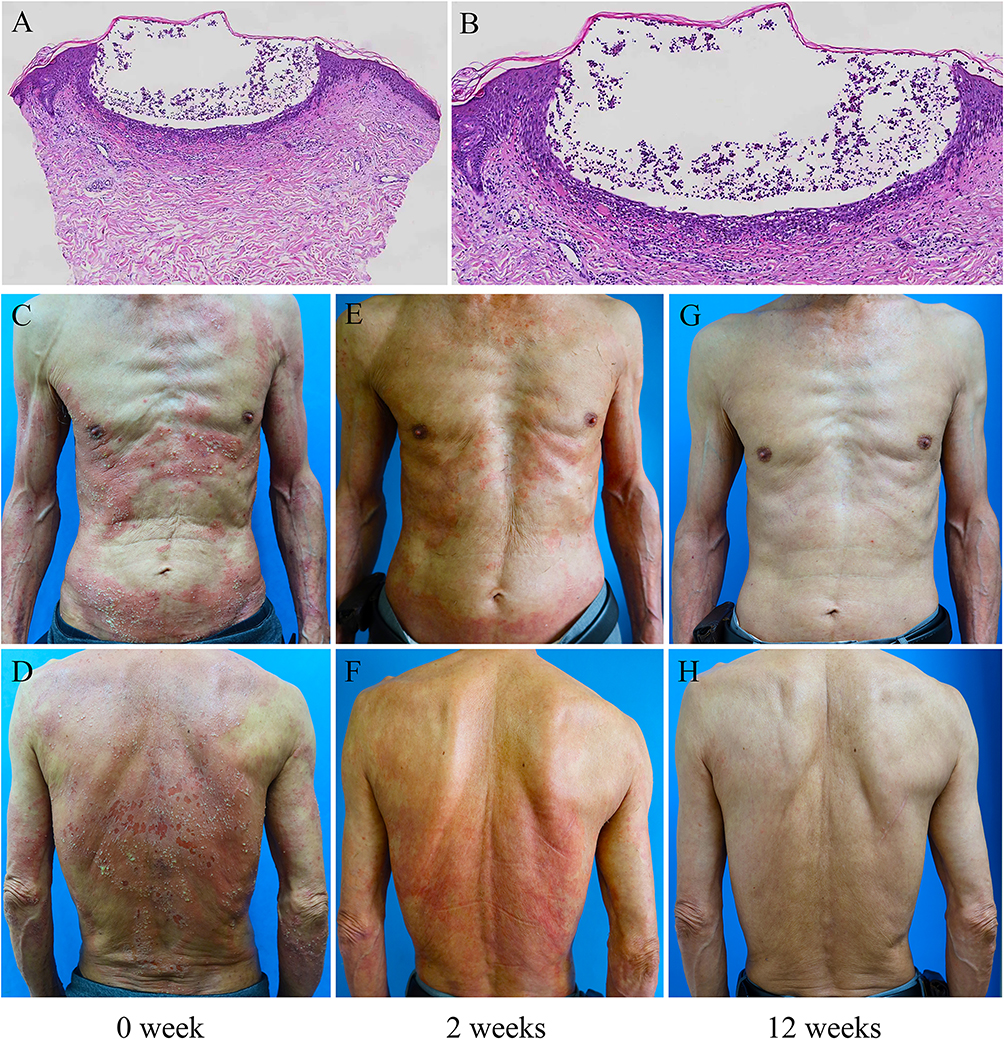 |
Figure 1 A biopsy of a pustular lesion revealed psoriasiform epidermal hyperplasia and intra-epidermal neutrophilic aggregates that formed pustules (H&E staining; (A) ×50; (B) ×100). A 72-year-old man presented with widespread erythematous plaques and coalescing pustules on the trunk, upper limbs, and back (C and D). Significant clinical improvement was observed at week 2 following the first vunakizumab infusion combined with Acitretin (E and F). Almost complete skin clearance was achieved at week 12 of treatment with vunakizumab combined with acitretin (G and H). |
Initially, the patient received a combination therapy consisting of oral methotrexate (MTX) 10 mg/week, subcutaneous guselkumab 100 mg/month, and oral acitretin 20 mg/day. However, half a month after the second guselkumab infusion, he experienced a severe exacerbation of GPP. Dermatological examination revealed widespread pustular papules, plaques, and confluent erythema involving the trunk and upper limbs. These lesions were studded with numerous yellowish, sterile pustules; on the trunk, some pustules fused to form pustular lakes. Additionally, eroded areas were observed on the back due to pustule rupture (Figure 1C and D). The patient’s generalized pustular psoriasis area and severity index (GPPASI) score was 39 (range: 0–72), generalized pustular psoriasis physician global assessment (GPPGA) score was 4 (indicating severe disease), and dermatology life quality index (DLQI) score was 23 (indicating an extremely large impact on quality of life).12,13
Considering the severe disease status and refractory nature of the condition, the treatment regimen was adjusted to combination therapy with vunakizumab (240 mg intravenously every two weeks) and oral acitretin (40 mg/day). Significant clinical improvement was observed immediately after the first vunakizumab infusion. By week 2 (Figure 1E and F), the patient achieved a GPPASI 75 response (ie, a 75% reduction in GPPASI score from baseline). Subsequently, after complete clearance of pustules, the dose of acitretin was reduced to 20 mg/day. By week 12 (Figure 1G and H), the patient nearly achieved a GPPASI 100 response (near-complete clearance of lesions). A total of six doses of vunakizumab were administered, and maintenance therapy with oral acitretin (20 mg/day) was continued until week 36. No disease relapse or treatment-related adverse events were reported. This case report was approved by the Ethics Committee of Guangzhou Dermatology Hospital, and written informed consent was obtained from the patient for publication, including the publication of images (gzsp202508).
Discussion
GPP is an inflammatory skin disease mainly involving keratinocyte, neutrophils, and monocytes. Its core pathological process is driven by the IL-36, IL-1, or TNF-α/IL-17A pathways which are characterized by periodic cutaneous neutrophil infiltration and pustule formation.14 Notably, IL-17 and IL-36 cytokines can induce each other in GPP, triggering systemic dissemination of inflammatory mediators that may lead to multisystem damage or psychological disorders.15–17 Acitretin, a first-line agent for psoriasis, has been shown to significantly attenuate inflammatory responses in both GPP and psoriasis vulgaris (PV) patients, particularly by reducing IL-17 levels.18,19 In a psoriasis-like mouse model, acitretin markedly downregulated IL-17A-induced IL-36β and IL-36γ expression at both the gene and protein levels in keratinocyte.20 Previous studies have supported robust, safe, and durable therapeutic responses to monotherapy with IL-17 inhibitors or acitretin in psoriasis.9,10,21,22 Furthermore, a meta-analysis of GPP treatments confirmed that IL-36 and IL-17 inhibitors yielded higher responder rates compared to TNF-α and IL-23 inhibitors; IL-36 inhibitors achieved the highest response rates within 4 to 8 weeks, whereas IL-17, TNF-α, and IL-23 inhibitors showed progressively increasing response rates up to 12 weeks.23
To contextualize our treatment approach, we conducted a systematic search of three major medical databases (PubMed, Scopus, and Web of Science) using the following terms: TNF-ɑ inhibitors (adalimumab, infliximab, etanercept, certolizumab pegol), IL-17 inhibitors (secukinumab, brodalumab, ixekizumab, bimekizumab, vunakizumab), IL-23 inhibitors (risankizumab, guselkumab), and “generalized pustular psoriasis”. The search was limited to English-language studies and included records up to October 30, 2025. A total of 1706 published studies matching our predefined search strategy were identified. After removing duplicates and screening titles and abstracts, 97 potentially relevant full-text articles remained. These studies were subsequently assessed against the following inclusion criteria: (1) original research providing a detailed treatment course for patients diagnosed with GPP; (2) participants aged 65 years or older; and (3) concurrent administration of biologic therapy and oral acitretin. Ultimately, 5 eligible studies were selected for data extraction24–28(Table 1). Most reported cases adopted an initial treatment strategy combining conventional agents with biologics;24,25,27,28 however, acitretin was often the preferred long-term maintenance therapy. Clinical improvement with acitretin monotherapy was gradual, typically requiring 3 to 6 months to reach peak efficacy.29 Specifically, among these cases, one patient was switched to an IL-17 inhibitor due to inadequate response to an IL-23 inhibitor,24 and another transitioned from biologics to conventional therapy (oral MTX) due to financial constraints.25 Two additional patients experienced acitretin-related adverse events, leading to drug discontinuation and subsequent disease flare.24,28 In one case, acitretin (50 mg daily) was added to a TNF-α inhibitor regimen.27 Tang et al26 reported a severe GPP case where complete lesion resolution was achieved with initial combination therapy of infliximab and acitretin.
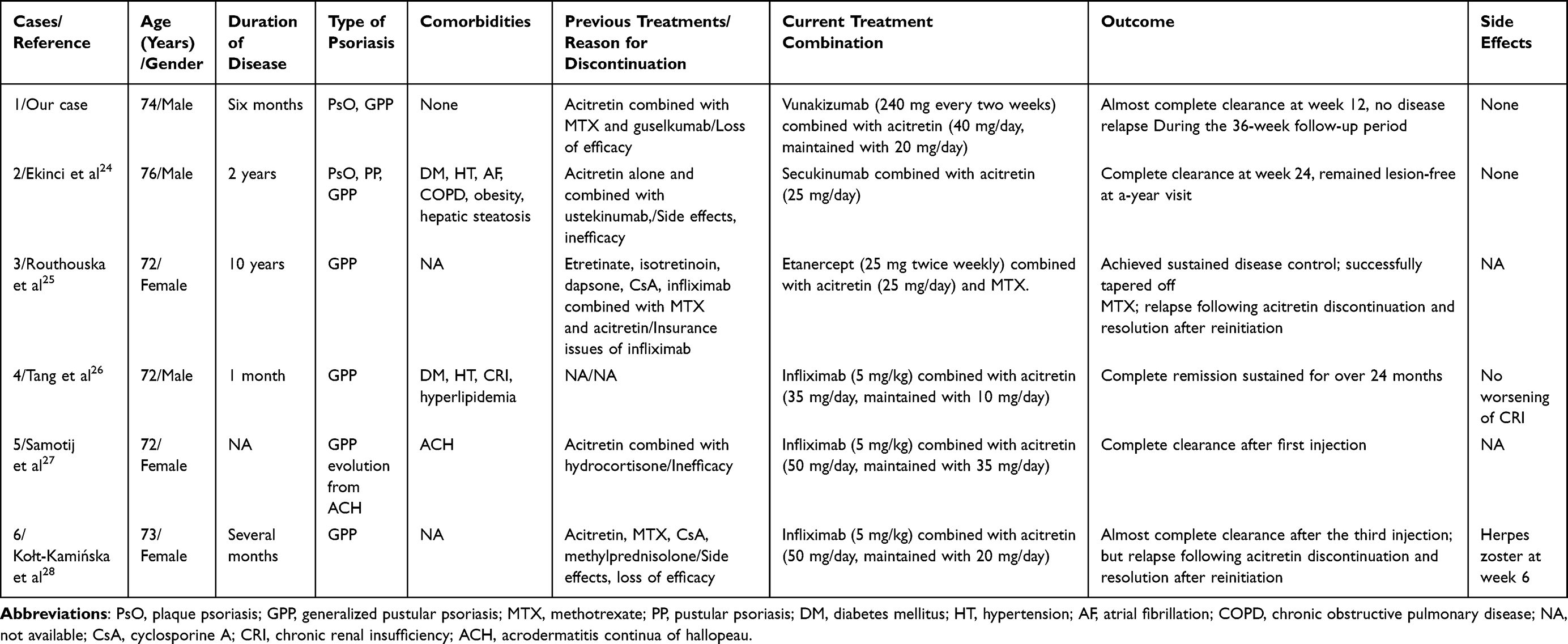 |
Table 1 Summary of Our Case and Reported Cases of Elderly Patients (≥ 65 years Old) Whose Treatment of Biological Agents and Acitretin |
Consistent with these findings, our elderly patient achieved favorable therapeutic outcomes with the combination of the IL-17A inhibitor vunakizumab and acitretin (40 mg/day). Although the current evidence base for GPP treatment is predominantly composed of case reports, it consistently demonstrates that this combination approach offers high efficacy and rapid clinical responses. However, several limitations of this study should be acknowledged. First, the absence of genetic testing limits our understanding of potential GPP-associated mutations. Second, the lack of long-term follow-up precludes assessment of the durability of treatment response and the potential for late-onset adverse effects. Most importantly, as a case report, this study is subject to the inherent limitations of anecdotal evidence, and its findings may not be generalizable to the broader GPP population.
Conclusion
Owing to impaired immune function and the presence of comorbidities, the management of GPP in elderly patients poses substantial challenges. Findings from this review indicate that acitretin is an effective and safe component of combination therapy, particularly when combined with IL-17 inhibitors. This study highlights the potential of acitretin-biologic combination therapy as an alternative strategy for GPP management. Further exploration of such combination regimens in RCTs is warranted. Ultimately, the overarching goal is to ensure that all GPP patients—regardless of age, geographical location, or comorbidities—have access to rapidly acting, safe, and durable therapeutic options.
Funding
This study was supported by Guangzhou Basic Research Plan Jointly Funded by the City, School (Hospital), and/or Enterprise (Grant No.2023A03J0942, 2023A03J0944 and 2023A03J0678); Scientific Research Project of Guangdong Provincial Bureau of Traditional Chinese Medicine (Grant No. 20261300); the Dongguan Social Science and Technology Development Program (20221800905522).
Disclosure
All authors declare no competing interests in this work.
References
1. Navarini AA, Burden AD, Capon F, et al. European consensus statement on phenotypes of pustular psoriasis. J Eur Acad Dermatol Venereol. 2017;31(11): 1792–6.
2. Chen HH, Abed SR. Update aetiopathogenesis and treatment of psoriasis: a literature review. J Dermatol Res. 2023;4:1–13.
3. Choon SE, van de Kerkhof P, Gudjonsson JE, et al. International consensus definition and diagnostic criteria for generalized pustular psoriasis from the international psoriasis council. JAMA Dermatol. 2024;160(7):758. doi:10.1001/jamadermatol.2024.0915
4. Prinz JC, Choon SE, Griffiths CEM, et al. Prevalence, comorbidities and mortality of generalized pustular psoriasis: a literature review. J Eur Acad Dermatol Venereol. 2023;37(2): 256–273.
5. Kodali N, Blanchard I, Kunamneni S, et al. Current management of generalized pustular psoriasis. Exp Dermatol. 2023;32(8):1204–1218. doi:10.1111/exd.14765
6. Benezeder T, Bordag N, Woltsche J, et al. IL-36-driven pustulosis: transcriptomic signatures match between generalized pustular psoriasis (GPP) and acute generalized exanthematous pustulosis (AGEP). J Allergy Clin Immunol. 2025;155(6):1913–1927. doi:10.1016/j.jaci.2025.01.046
7. Zhou LL, Georgakopoulos JR, Ighani A, et al. Systemic monotherapy treatments for generalized pustular psoriasis: a systematic review. J Cutaneous Med Surg. 2018;22(6):591–601. doi:10.1177/1203475418773358
8. Hsu FL, Tsai T. Epidemiological, genetic, clinical, and treatment differences of generalized pustular psoriasis and acrodermatitis continua of hallopeau across ethnicities: a systematic review. Am J Clin Dermatol. 2025;26(3):395–409. doi:10.1007/s40257-025-00937-9
9. Yan KX, Li FQ, Bi XD, et al. Efficacy and safety of vunakizumab in moderate-to-severe chronic plaque psoriasis: a randomized, double-blind, placebo-controlled Phase 3 trial. J Am Acad Dermatol. 2025;92(1):92–99. doi:10.1016/j.jaad.2024.09.031
10. Zhu KJ, Zheng QL, Zhu YJ, et al. Efficacy and safety of vunakizumab in patients with moderate-to-severe plaque psoriasis across different regions of China: a post-hoc exploratory analysis of a Phase III, randomized controlled trial. J Dermatolog Treatment. 2025;36(1). doi:10.1080/09546634.2025.2560505.
11. Rivera-Díaz R, Daudén E, Carrascosa JM, et al. Generalized pustular psoriasis: a review on clinical characteristics, diagnosis, and treatment. Dermatol Ther. 2023;13(3):673–688. doi:10.1007/s13555-022-00881-0
12. Choon SE, Lebwohl GM, Marrakchi S, et al. Study protocol of the global Effisayil 1 Phase II, multicentre, randomised, double-blind, placebo-controlled trial of spesolimab in patients with generalized pustular psoriasis presenting with an acute flare. BMJ Open. 2021;11(3):e043666. doi:10.1136/bmjopen-2020-043666
13. Burden AD, Choon SE, Gottlieb AB, et al. Clinical disease measures in generalized pustular psoriasis. Am J Clin Dermatol. 2022;23(Suppl 1):39. doi:10.1007/s40257-021-00653-0
14. Johnston A, Xing XY, Wolterink L, et al. IL-1 and IL-36 are dominant cytokines in generalized pustular psoriasis. J Allergy Clin Immunol. 2017;140(1):109–120. doi:10.1016/j.jaci.2016.08.056
15. Miura S, Garcet S, Salud-Gnilo C, et al. IL-36 and IL-17A cooperatively induce a psoriasis-like gene expression response in human keratinocytes. J Investig Dermatol. 2021;141(8):2086–2090. doi:10.1016/j.jid.2021.01.019
16. Pfaff CM, Marquardt Y, Fietkau K, et al. The psoriasis-associated IL-17A induces and cooperates with IL-36 cytokines to control keratinocyte differentiation and function. Sci Rep. 2017;7(1). doi:10.1038/s41598-017-15892-7.
17. Teshima R, Saito-Sasaki N, Sawada Y. Generalized pustular psoriasis and systemic organ dysfunctions. Int J Mol Sci. 2024;25(11):6270. doi:10.3390/ijms25116270
18. Shen SK, Tang XF, Wang WJ, et al. Transcriptomic landscape of generalized pustular psoriasis before and after Acitretin/glucocorticoids treatment. Clin Exp Med. 2025;26(1). doi:10.1007/s10238-025-01931-5.
19. Niu XW, Cao W, Ma HQ, et al. Acitretin exerted a greater influence on T -helper (T h)1 and T h17 than on T h2 cells in treatment of psoriasis vulgaris. J Dermatol. 2012;39(11):916–921. doi:10.1111/j.1346-8138.2012.01637.x
20. Tu J, Yin Z, Guo J, et al. Acitretin inhibits IL-17A-induced IL-36 expression in keratinocytes by down-regulating IκBζ. Int Immunopharmacol. 2020;79: 106045.
21. Torres T, Chiricozzi A, Puig L, et al. Treatment of psoriasis patients with latent tuberculosis using IL-17 and IL-23 inhibitors: a retrospective, multinational, multicentre study. Am J Clin Dermatol. 2024;25(2):333–342. doi:10.1007/s40257-024-00845-4
22. Piaserico S, Conti A, Console FL, et al. Efficacy and safety of systemic treatments for psoriasis in elderly patients. Acta Dermato-Venereolog. 2014;94(3):293–297. doi:10.2340/00015555-1719
23. Chen BL, Liu QW, Dong XW, et al. Biologics for generalized pustular psoriasis: a systematic review and single-arm meta-analysis. Front Immunol. 2024;15:1462158. doi:10.3389/fimmu.2024.1462158
24. Ekinci AP, Bölük KN, Kobaner GB. Secukinumab and Acitretin as a combination therapy for three clinical forms of severe psoriasis in multi-drug refractory patients: a case series of high efficacy and safety profile. Dermatolog Ther. 2021;34(1): e14704.
25. Routhouska SB, Sheth PB, Korman NJ. Long-term management of generalized pustular psoriasis with infliximab: case series. J Cutaneous Med Surg. 2008;12(4):184–188. doi:10.2310/7750.2008.07036
26. Tang MM, Spanou Z, Tang H, et al. Rapid downregulation of innate immune cells, interleukin-12 and interleukin-23 in generalized pustular psoriasis with infliximab in combination with Acitretin. Dermatology. 2012;225(4):338–343. doi:10.1159/000346243
27. Samotij D, Gawron E, Szczęch J, et al. Acrodermatitis continua of hallopeau evolving into generalized pustular psoriasis following COVID-19: a case report of a successful treatment with infliximab in combination with acitretin. Biologics. 2021;15:107–113.
28. Kołt-Kamińska M, Żychowska M, Reich A. Infliximab in combination with low-dose acitretin in generalized pustular psoriasis: a report of two cases and review of the literature. Biologics. 2021;15: 317–327.
29. Dogra S, Jain A, J KA. Efficacy and safety of Acitretin in three fixed doses of 25, 35 and 50 mg in adult patients with severe plaque type psoriasis: a randomized, double blind, parallel group, dose ranging study. J Eur Acad Dermatol Venereol. 2013;27(3): e305–e311.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.