Back to Journals » Clinical Ophthalmology » Volume 20
Vitrectomy with Subretinal Tissue Plasminogen Activator for Submacular Hemorrhage: A Multicenter Retrospective Analysis of Functional and Anatomical Outcomes Across Multiple Etiologies
Authors Chakraborty S ![]() , Sheth JU
, Sheth JU ![]() , Ganguly S, Reddy R
, Ganguly S, Reddy R
Received 3 January 2026
Accepted for publication 27 February 2026
Published 9 March 2026 Volume 2026:20 589150
DOI https://doi.org/10.2147/OPTH.S589150
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yousef Fouad
Somnath Chakraborty,1 Jay U Sheth,2 Santanu Ganguly,1 Rahul Reddy1
1Department of Retina Services, Retina Institute of Bengal, Siliguri, India; 2Department of Retina Services, Shantilal Shanghvi Eye Institute, Mumbai, India
Correspondence: Somnath Chakraborty, Department of Retina Services, Retina Institute of Bengal C/O Reddy Health Care 3 rd Floor Uttarapan Market Complex, Hill Cart Road, Pradhan Nagar, Siliguri, West Bengal, 734003, India, Tel +91-9002508334, Email [email protected]
Purpose: To evaluate visual and anatomical outcomes of pars plana vitrectomy (PPV) with subretinal tissue plasminogen activator (tPA) and gas or air tamponade for large submacular haemorrhage (SMH> 4 disc diameters) of varied etiologies and assess postoperative anti-vascular endothelial growth factor (anti-VEGF) requirements in a multicenter real-world cohort.
Patients and Methods: This retrospective, two-center study included 32 eyes undergoing PPV with subretinal tPA (25– 50 μg/0.1– 0.2 mL) and SF6 or air tamponade, followed for ≥ 6 months. The primary outcome was change in best-corrected visual acuity (BCVA). Secondary outcomes included central macular thickness (CMT), SMH dimensions, subretinal/intraretinal fluid (SRF/IRF) status, intraocular pressure (IOP), and anti-VEGF use.
Results: Mean patient age was 60.8 ± 19.1 years; etiologies included polypoidal choroidal vasculopathy (PCV; 53.1%), neovascular age-related macular degeneration (nAMD; 28.1%), trauma (12.5%), and retinal artery macroaneurysm (RAM; 6.3%). BCVA improved significantly from 1.13 ± 0.30 to 0.56 ± 0.26 logMAR (P< 0.001), with 55.2% gaining ≥ 3 lines. CMT reduced from 501 ± 219 to 276 ± 70 μm (P< 0.001), and SMH size decreased from 5 ± 2 to 0 disc diameters by 6 months. SRF resolved in 65.65% of eyes (P< 0.001), while IRF remained stable (P=0.51). IOP normalized after a transient 1-month rise. Mean anti-VEGF use was 1.2 injections/eye (bevacizumab 88.2%, brolucizumab 11.8%). No major complications occurred; one transient vitreous hemorrhage and three cataract progressions were noted.
Conclusion: PPV with subretinal tPA achieved rapid hemorrhage clearance, significant visual gain, and durable anatomical restoration with minimal complications and limited anti-VEGF need. It offers an effective, safe option for large SMH across etiologies, enabling timely foveal recovery and improved long-term functional outcomes.
Keywords: submacular hemorrhage, tissue plasminogen activator, anti-vascular endothelial growth factor, age-related macular degeneration, vitrectomy, polypoidal choroidal vasculopathy
Introduction
Submacular hemorrhage (SMH) represents one of the most devastating complications affecting macular vision, with potential for irreversible photoreceptor damage and permanent visual impairment.1–3 The spectrum of conditions predisposing to SMH encompasses various retinal and choroidal pathologies. Neovascular age-related macular degeneration (nAMD) remains the most common etiology in elderly populations, with hemorrhage typically arising from rupture of fragile choroidal neovascular membranes.1,2 Polypoidal choroidal vasculopathy (PCV), increasingly recognized as a distinct entity particularly prevalent in Asian populations, frequently presents with recurrent hemorrhagic episodes due to rupture of thin-walled polypoidal lesions.4–8 Retinal arterial macroaneurysms (RAM) represent another significant cause, especially in hypertensive patients, where acute rupture can lead to massive subretinal bleeding.1,2 Traumatic etiologies, while less common, can result in particularly challenging cases due to associated choroidal rupture and complex hemorrhage patterns.1,2
The natural history of untreated SMH is associated with poor structural and functional outcomes. Experimental models demonstrate photoreceptor injury within 24 hours of subretinal blood exposure, progressing to irreversible outer retinal atrophy within one week.1–3 Clinical series corroborate these findings: persistent subretinal blood induces sustained photoreceptor–RPE separation, iron-mediated oxidative injury, and subsequent subretinal fibrosis, producing permanent central scotomas.1–3 Visual prognosis correlates quantitatively with hemorrhage duration, thickness and en-face extent, emphasizing the time-sensitive nature of intervention.1–3
Current management algorithms span observation and anti-vascular endothelial growth factor (anti-VEGF) monotherapy for thin SMH associated with active macular neovascularization (MNV), to intravitreal tissue plasminogen activator (tPA) with pneumatic displacement for liquefiable clots, and pars plana vitrectomy (PPV) with direct subretinal tPA delivery for large or organized haemorrhages that resist pneumatic techniques.1,9,10 Photodynamic therapy (PDT) retains a role for selected PCV cases but has no applicability for clot displacement.1,6,9,10 Comparative evidence is limited: most series are retrospective, single-center and etiologically homogeneous, with variable SMH size/time thresholds and inconsistent reporting of OCT-based anatomic endpoints; meta-analyses report heterogeneous visual outcomes and a higher surgical complication burden in operative cohorts.2,11
No single modality is universally superior: small SMH (<1–2DD) may resolve with anti-VEGF alone, whereas large or thick haemorrhages (>4 DD) commonly require pneumatic displacement.1,9,10 The evidence base is limited, predominantly retrospective, single-center series often restricted to one etiology (usually nAMD), and studies vary in definitions of “large” (eg >2 DD vs >4 DD) and treatment windows (some ≤2 weeks). Reporting is heterogeneous, with few studies simultaneously assessing visual and OCT-anatomic endpoints and scarce head-to-head comparisons. A meta-analysis of 960 AMD-related SMH eyes found no significant VA difference between anti-VEGF alone and surgical intervention, although surgical cohorts had larger haemorrhages and higher complication rates (retinal detachment 10.6% vs 0.1% with injections).2 A retrospective series of 32 heterogeneous eyes reported a non-significant trend favoring pneumatic ± tPA over PPV + tPA for ≥3-line gain (46% vs 18%).11 Overall, existing cohorts are small, technique-heterogeneous, and of limited follow-up, constraining definitive recommendations.
Given these gaps, we conducted a pooled two-center retrospective analysis of PPV with subretinal tPA and tamponade for large SMH (>4 DD), across multiple indications. We aimed to assess functional outcomes (best corrected visual acuity [BCVA]) and anatomical outcomes (optical coherence tomography [OCT] metrics, fluid resolution) over 6 months, and describe the need for adjunctive anti-VEGF therapy.
Materials and Methods
This was a retrospective, consecutive case series conducted at two tertiary eye institutes in India between January 2021 and August 2025. Institutional Review Board approval was obtained at both sites, and the study adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all patients for the treatment, data collection, and publication, including the images.
Design
The study included all eyes presenting with SMH of ≤30 days total duration and >4 DD in largest linear dimension that underwent PPV with subretinal tPA injection and gas or air tamponade between the study period and with a minimum follow-up of 6 months. For descriptive analysis, SMH was categorized as acute (≤14 days) or subacute (>14 days). Eligible cases required foveal involvement, irrespective of underlying etiology. Exclusion criteria comprised prior vitreoretinal surgery, concurrent retinal detachment necessitating additional procedures, inability to comply with postoperative positioning, and insufficient follow-up data for outcome assessment.
Surgical Technique
Standard three-port 23- or 25-gauge PPV was performed under retrobulbar or general anaesthesia. Core vitrectomy and PVD induction were undertaken as needed. A small retinotomy adjacent to the haemorrhage permitted subretinal tPA delivery via a 39- or 41-g cannula with viscous-fluid control. tPA dose was 25–50 μg in 0.1–0.2 mL according to clot burden. Controlled subretinal lavage with small volumes of balanced salt solution was used to soften and mobilize the clot. In selected eyes, only when the clot appeared liquefied and freely mobile, a limited aspiration was performed through the same small-gauge subretinal cannula using very low vacuum and brief, controlled suction bursts. If the clot remained adherent or if there was risk of RPE/retinal contact, aspiration was not attempted. Complete intraocular tamponade was achieved using 20% SF6 or air per surgeon choice; an intravitreal anti-VEGF was administered at closure based on the indication (Video S1). Postoperative prone positioning (3–7 days) was advised. Anti-VEGF therapy was administered based on underlying pathology and clinical response, with bevacizumab representing the primary agent utilized, supplemented by brolucizumab in select cases requiring enhanced efficacy. Injection frequency followed pro-re-nata (PRN) protocols with monthly assessments during the initial three months followed by extended intervals based on disease activity. Reinjections were administered based on structural evidence of disease activity on follow-up imaging, including recurrence or persistence of SMH, new or increasing SRF or IRF.
Outcome Measures
Primary outcome measure consisted of BCVA change from baseline to final follow-up visit. Secondary outcome measures included intraocular pressure (IOP) measurements, central macular thickness (CMT) assessed via spectral-domain optical coherence tomography (SD-OCT), SMH size measurements in DD, hemorrhage height and width in microns, presence or absence of intraretinal and subretinal fluid (IRF and SRF), lens status changes, and frequency of repeat anti-VEGF injections.
Statistical Analysis
The statistical analysis was performed using SPSS 23.0 (SPSS Inc., Chicago, IL, USA). Normality was assessed using Shapiro–Wilk testing, with parametric or non-parametric methods selected accordingly. Paired t-tests or Wilcoxon signed-rank tests analyzed continuous variables comparing baseline to follow-up values. McNemar’s exact test evaluated paired proportional data for categorical variables such as fluid presence. Statistical significance was defined as two-tailed P-value <0.05.
Results
Study Cohort
Thirty-two eyes from 32 patients were included (Table 1); mean age was 60.8 ± 19.1 years with equal sex distribution (16 males, 16 females). Right eyes numbered 14 (43.8%) and left 18 (56.2%); primary etiologies were PCV in 17 (53.1%), nAMD in 9 (28.1%), post-traumatic in 4 (12.5%), and RAM in 2 (6.3%). Half the cohort had systemic comorbidity (hypertension alone 25.0%; hypertension with diabetes 12.5%; diabetes alone 6.2%); mean symptom duration before surgery was 22.3 ± 21.1 days (median 16; IQR 12–24).
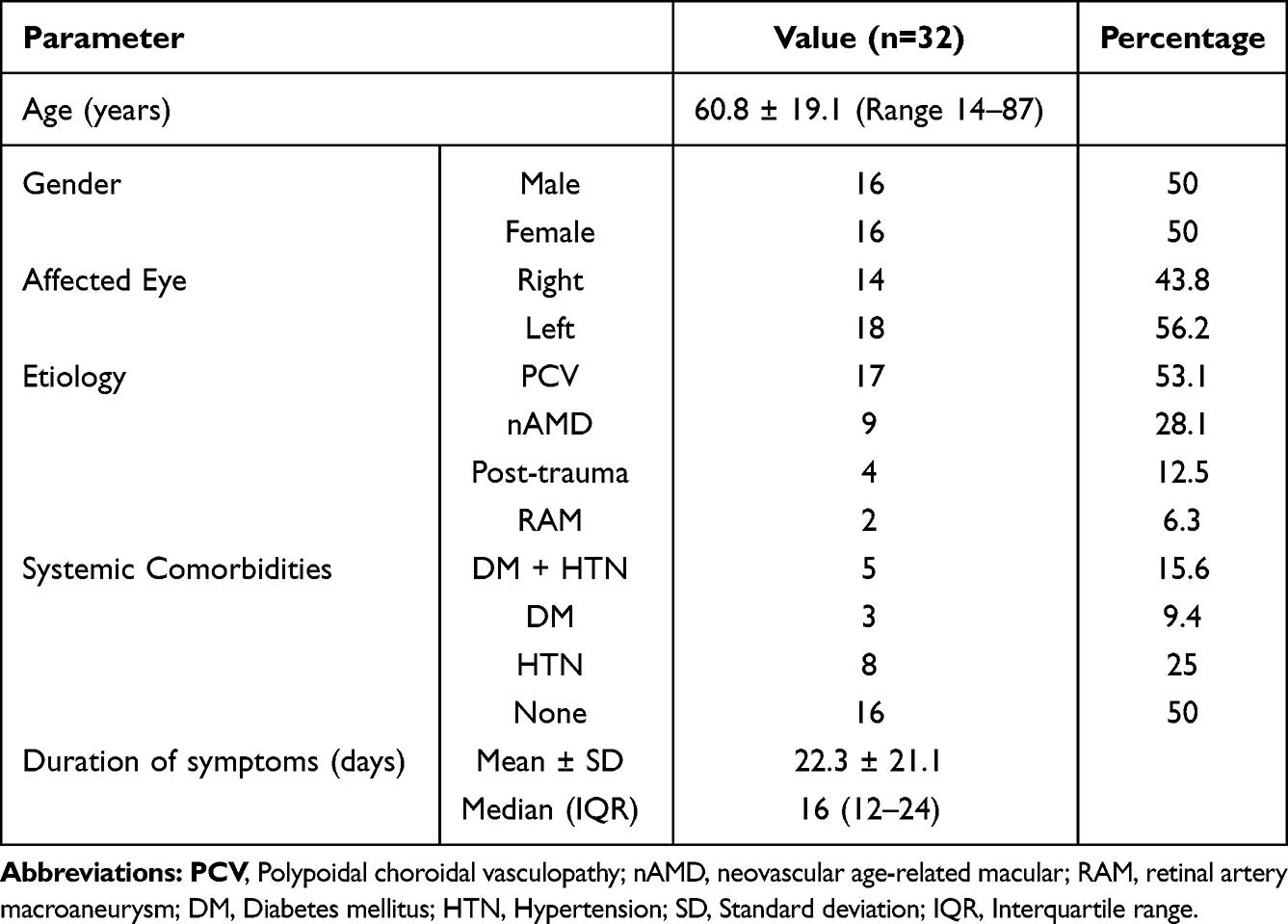 |
Table 1 Baseline Demographics and Clinical Characteristics of the Study Eyes |
Best-Corrected Visual Acuity
Visual acuity outcomes demonstrated significant improvement across all time points (Table 2). Mean BCVA improved from 1.13 ± 0.30 logMAR at baseline (≈20/270 Snellen) to 0.56 ± 0.26 logMAR at 6 months (≈20/72 Snellen), representing a gain of 0.58 ± 0.35 logMAR (P<0.001). Progressive improvement was observed at each visit: 0.76 ± 0.34 logMAR at 1 month, 0.60 ± 0.27 logMAR at 3 months, and 0.56 ± 0.26 logMAR at final follow-up (all P<0.001 versus baseline). By 6 months, 55.2% of eyes gained ≥3 lines of vision with no cases of significant vision loss.
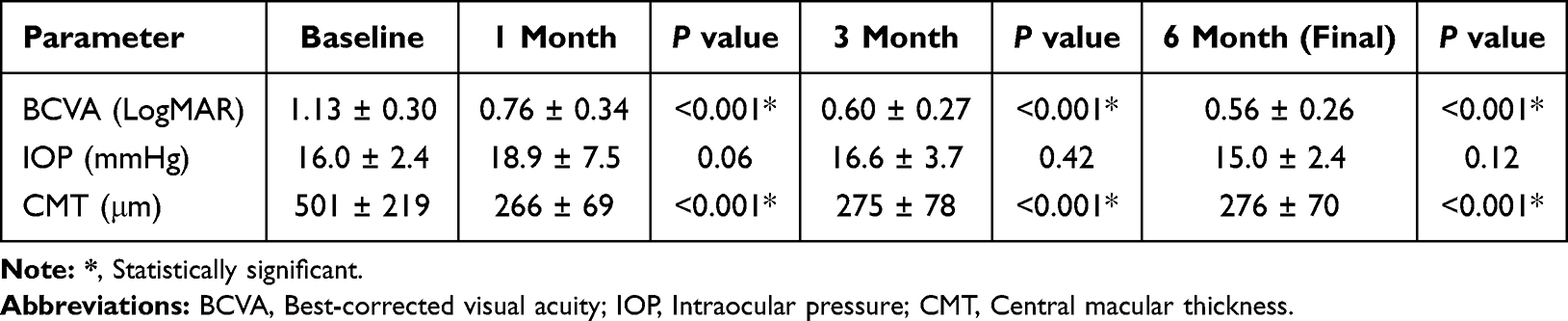 |
Table 2 Changes in the Best-Corrected Visual Acuity, Intraocular Pressure, and Central Macular Thickness in the Study Eyes |
Anatomical Outcomes
Hemorrhage displacement was highly effective, with significant reductions in CMT and SMH dimensions. Mean CMT decreased from 501 ± 219 µm at baseline to 266 ± 69 µm at 1 month (−235 ± 219 µm, P<0.001), remaining stable at 3 months (275 ± 77 µm) and 6 months (276 ± 70 µm, both P<0.001) (Table 2).
Baseline SMH averaged 5 ± 2 DD, reducing to 2 ± 1 DD at 1 month (P<0.001), 1 ± 0 DD at 3 months (P=0.018), and completely resolving in subfoveal location in all eyes by 6 months (P<0.001) (Table 3).
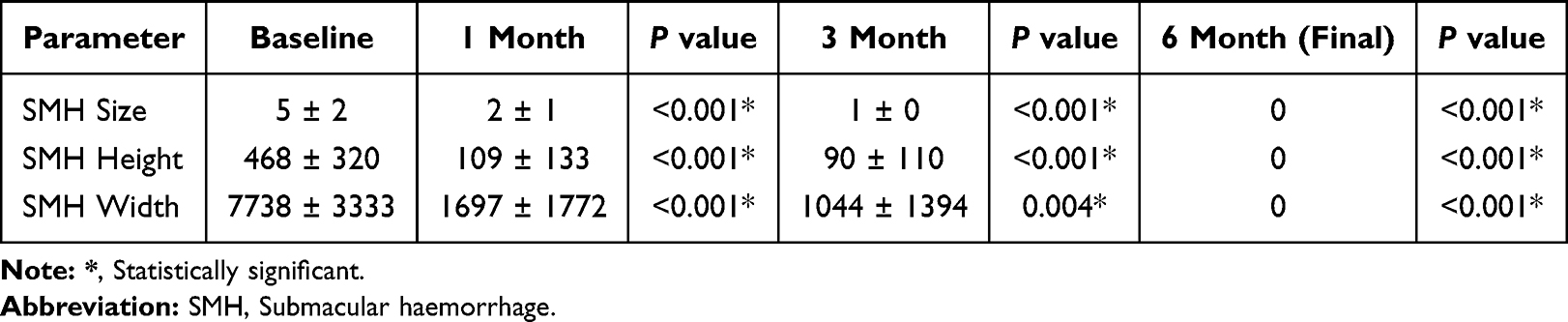 |
Table 3 Changes in the Anatomical Parameters in the Study Eyes |
SMH height declined from 468 ± 320 µm to 109 ± 133 µm at 1 month (P<0.001) and to 90 ± 110 µm by final follow-up. Width decreased from 7738 ± 3333 µm to 1697 ± 1772 µm at 1 month and 1044 ± 1394 µm finally (P<0.001) (Table 3).
SRF resolved in most eyes, reducing from 81.25% to 15.6% (P<0.001) (Table 4). IRF was infrequent (12.5% at baseline, 21.88% at 6 months) and showed no significant change (P>0.24 at all intervals) (Table 4). Cases 1 and 2 are representative cases.
 |
Table 4 Proportion of Eyes with Residual Subretinal Fluid and Intraretinal Fluid |
Intraocular Pressure
IOP remained stable without clinically significant elevation (Table 2). Baseline IOP was 16.0 ± 2.4 mmHg, rising transiently at 1 month to 18.9 ± 7.5 mmHg (+2.9 ± 8.0 mmHg; P=0.06), likely tamponade-related, before normalizing to 16.6 ± 3.7 mmHg at 3 months and 15.0 ± 2.4 mmHg at 6 months (P>0.1 vs baseline).
Intravitreal Injections
Mean injection frequency was 1.2 per eye with median of 1.0 injection. Total injections administered numbered 35, with bevacizumab comprising 30 injections (88.2%) and brolucizumab accounting for 4 injections (11.8%). Overall, 12 eyes (37.5%) received no anti-VEGF injections during the 6-month study period, 5 eyes (15.6%) received 1 injection, 12 eyes (37.5%) received 2 injections, and 3 eyes (9.4%) received 3 injections. When stratified by diagnosis, eyes with nAMD received the highest mean number of injections (2.00 ± 1.69 injections), followed by PCV (1.69 ± 1.30 injections) and post-traumatic eyes (0.25 ± 0.50 injections; n=4).
Safety Analysis
In this series, serious complications were uncommon. One eye had an early postoperative vitreous cavity hemorrhage requiring vitreous lavage. Three of seven phakic patients underwent cataract extraction during follow-up due to progression of lens opacities. No eye developed a full-thickness macular hole, and there were no cases of sustained IOP elevation or neovascular glaucoma. One eye had a small epiretinal membrane at final follow-up. Cases 1 and 2 which are shown as Figures 1 and 2 respectively, are representative cases.
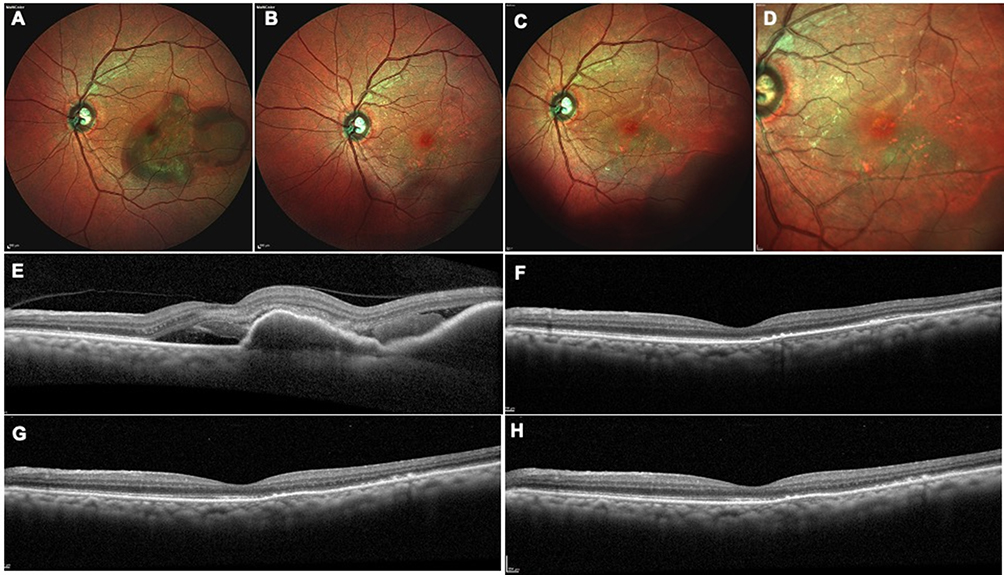 |
Figure 1 A 64-year-old female presented with a decrease of vision (DOV) in the left eye (OS) for 12 days. Best-corrected visual acuity (BCVA) was 20/200, and the eye was pseudophakic. Fundus examination revealed submacular hemorrhage (SMH) (A), which was confirmed on optical coherence tomography (OCT) (E), showing a large pigment epithelial detachment (PED) with associated subretinal fluid (SRF). A diagnosis of polypoidal choroidal vasculopathy (PCV) was made and the patient underwent pars plana vitrectomy with subretinal tissue plasminogen activator (tPA) injection and sulfur hexafluoride (SF6) gas tamponade. One month postoperatively, the SMH had resolved (B), with complete resolution of the PED and SRF on OCT (F), and BCVA improved to 20/80. At three and six months, the patient remained stable with further improvement in BCVA to 20/32, no recurrence of SMH on fundus examination ((C): 3 months; (D) 6 months), and a dry macula with complete absence of PED or SRF on OCT (G): 3 months; (H) 6 months). |
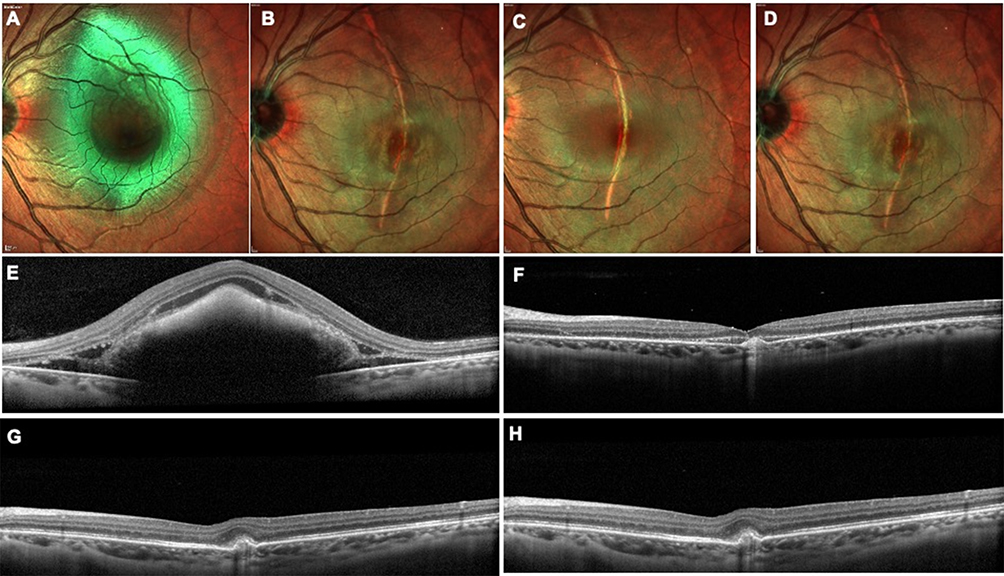 |
Figure 2 A 25-year-old female presented with diminution of vision (DOV) in the left eye (OS) for 10 days following blunt ocular trauma. Her best-corrected visual acuity (BCVA) was 20/200. The anterior segment examination was unremarkable with a clear crystalline lens. Fundus examination revealed a submacular hemorrhage (SMH) (A), which was confirmed on optical coherence tomography (OCT) (E). The patient underwent pars plana vitrectomy with subretinal injection of tissue plasminogen activator (tPA) and sulfur hexafluoride (SF6) gas tamponade. One month postoperatively, the SMH had resolved (B), and a subfoveal choroidal rupture was evident at this stage. The BCVA improved to 20/80. OCT showed trace subretinal fluid and a dense subfoveal hyperreflective band corresponding to the choroidal rupture (F). At three months (C) and six months (D) follow-up, the patient remained stable, with BCVA improving to 20/32, no recurrence of SMH, and fundus evidence of scarring along the choroidal rupture (C and D). Corresponding OCT images (G and H) showed a dry macula with persistent subretinal hyperreflectivity consistent with the healed rupture. |
Discussion
This multicenter retrospective analysis demonstrates that PPV with subretinal tPA injection represents a highly effective and safe treatment for SMH across diverse etiologies. Our results show significant functional improvement with mean visual acuity gains of 5.8 lines, substantial anatomical improvement evidenced by CMT reduction of 225 μm, and excellent SRF resolution from 81.25% to 15.6% of cases. The modest anti-VEGF injection requirement of 1.2 injections per patient over 6 months and absence of serious complications support the favorable risk-benefit profile of this surgical approach.
Our findings align with other reports of surgical displacement of SMH. For example, Patikulsila et al12 reported on 9 eyes with large AMD-related SMH treated similarly; mean VA improved from logMAR 1.9 to 0.9 over ~21 months. In that study, 89% achieved complete blood displacement by 1 month.12 Our patients started with marginally better baseline VA (mean 1.13 vs 1.9) and ended with better mean VA (0.56 vs 0.9), possibly reflecting differences in hemorrhage chronicity (their mean duration 15 days vs our mean 22 days) or sample. The magnitude of VA gain in our series (~5.7 lines) is comparable or greater than in many published series, suggesting effective photoreceptor salvage. We also report detailed OCT data (CMT, SMH dimensions), highlighting quantitative clot clearance, which few prior studies have systematically done.
Less invasive alternatives include intravitreal tPA injection and expansile gas without vitrectomy. Several retrospective studies suggest this can benefit eyes with fresh SMH.1,2 Recently, Barzelay et al13 compared pneumatic ± intravitreal tPA to PPV + subretinal tPA in 150 eyes; they found that vitrectomy and tPA had a clear advantage for small and medium sized SMH. In contrast, Bell et al11 demonstrated higher rates of ≥3-line VA improvement with pneumatic displacement with intravitreal tPA compared to PPV with subretinal tPA (46% vs 18%), though the difference was not statistically significant. Their one-year VA outcomes did not differ significantly between groups.11 The authors suggested that for moderate-sized SMH, the less invasive pneumatic approach may yield similar visual outcomes. However, pneumatic methods often struggle with very thick or longstanding hemorrhages, where subretinal tPA may not adequately liquefy dense clot. In our series of very large SMH (mean 5 DD), pneumatic displacement alone might not have been sufficient, and indeed our final outcomes appear somewhat better than many pneumatic reports (mean VA ~20/72 vs ~20/100 in some series).
Intravitreal anti-VEGF injections alone have been used, especially when SMH is small (<1–2 DD) or in early AMD.1,2 Some case series show modest improvement with anti-VEGF alone, presumably by reducing associated fluid and allowing slow blood absorption.1,2 The meta-analysis by Shaheen et al2 found that anti-VEGF–treated SMH eyes (n=960) gained about –0.16 logMAR (improvement) on average, similar to the –0.36 logMAR gain with surgical cases, with no significant difference. However, anti-VEGF without clot displacement usually leaves the blood over the fovea for weeks to months, risking photoreceptor damage. In cases of massive SMH, many clinicians feel that active displacement is needed. In our cohort, which included large hemorrhages and chronic cases (some >3 weeks old), anti-VEGF alone would likely have resulted in poorer outcomes. Our relatively low injection rate (mean 1.2 in 6 months) suggests that the surgical removal of blood reduced the ongoing stimulus for aggressive VEGF therapy.
In our series, over half the eyes had PCV. PCV is known to cause more severe hemorrhages due to aneurysmal lesions, and requires additional considerations like PDT.6,7 We did not routinely use PDT due to its unavailability in India since 2020; 55.6% of PCV eyes eventually received additional anti-VEGF at follow-up. The literature suggests PCV-related SMH carries a guarded prognosis, especially for very large bleeds.14 However, our visual results (final mean ~20/72) compare favorably to some PCV series, possibly because surgical evacuation neutralizes the hemorrhagic insult early.
Traumatic SMH (n=4) and RAM-related SMH often occur in younger patients and may have better photoreceptor resilience.1,2 We had 4 trauma cases; though we did not analyze them separately, these eyes generally regained good vision (in the mid-20/60 range) after displacement. Ruptured RAM has historically had poor natural outcome, but displacement (either pneumatic or vitrectomy) plus tPA has improved results in published series. We included all etiologies to reflect real-world practice; our positive outcomes suggest this technique is broadly applicable across causes.
PPV with subretinal tPA facilitates two key actions: enzymatic clot liquefaction and mechanical displacement.1–3 tPA converts plasminogen to plasmin, breaking down fibrin within the clot.1–3 The intraocular tamponade (gas/air) and face-down positioning then help the now-liquefied blood float out of the foveal zone.1–3 This minimizes the time that toxic iron and pressure effects remain on the foveal photoreceptors.1–3 In animal models, subretinal tPA alone (without surgery) limits photoreceptor loss if given promptly.3 In our patients, earlier surgery tended to correlate with better outcomes (although our sample size limited formal subgroup analysis). The median symptom duration was 16 days, many were treated within 2 weeks, which is consistent with literature suggesting that intervention within 1–2 weeks yields best results [5,10]. Delayed treatment (beyond 3–4 weeks) may allow irreversible damage, so we generally offered surgery as soon as feasible.
All eyes received intraocular gas or air. SF6 were used in our series, but one could also use C3F8 also. Expansile gases provide a longer tamponade, potentially giving more time for clot displacement, but carry risk of pressure rise and delayed visual recovery. Some surgeons prefer shorter-acting SF6 or even air for faster vision return. There is no consensus data; in our practice, tamponade was chosen by surgeon based on clot size and patient factors. We did not observe significant long-term IOP elevation, suggesting the gas strategy was safe when monitored.
In our protocol, some surgeons gave a bevacizumab injection at the end of surgery (5 of 32 eyes). Postoperatively, further injections were guided by OCT and angiographic findings. Overall, 63.3% of eyes did require at least one anti-VEGF over 6 months, reflecting the need to suppress underlying MNV. The mean of 1.2 injections (1.0 median) over 6 months is relatively low; in comparison, typical treat-and-extend AMD regimens give 3–6 injections in 6 months. This suggests that once the hemorrhage is evacuated, many eyes stabilize on minimal therapy. Our injection rate is also lower than that reported in non-surgical SMH series (some of which use monthly injections initially). Only 2 eyes needed 3 injections by 6 months. Notably, 37.5% of eyes needed no injections at all during follow-up; these included some traumatic cases and others where no active CNV was found post-op. The predominance of bevacizumab in our injection data (88.2%) simply reflects local practice (cost-effectiveness) rather than a biological effect.
This series has several strengths. It is one of the largest dedicated reports of PPV+tPA for SMH that includes multiple indications. The two-center design reduces single-surgeon bias and enhances generalizability. All surgeries were done by experienced retinal surgeons, using a consistent technique. We have comprehensive data: both functional and detailed anatomical outcomes at multiple timepoints. We also report ancillary outcomes (IOP, fluid status, injection frequency) and follow a structured follow-up schedule. This allows comparison with a range of published studies and registries.
Limitations include the retrospective and uncontrolled nature of the study. We cannot directly compare our approach to alternative therapies (eg pneumatic displacement alone or anti-VEGF monotherapy) within this dataset. Follow-up was limited to 6 months; longer-term results (eg 1–2 years) would be valuable, especially to assess final visual acuity and late complications (eg chorioretinal atrophy). The sample size (32 eyes) is modest, and subgroup analysis (by cause or tamponade type) is underpowered. The cohort is heterogeneous, with trauma and RAM cases included alongside neovascular AMD and PCV, which may confound pooled visual outcomes because baseline RPE health and visual potential differ by diagnosis. Some surgical choices (type of gas, use of concurrent intravitreal anti-VEGF) were left to surgeon discretion, and there was no standardized retreatment protocol (anti-VEGF was given PRN at the treating physician’s judgment). We did not systematically grade hemorrhage displacement (complete vs partial) and OCT measurements of SMH size/height were not obtainable in all eyes at every visit (eg when hemorrhage density or resolution precluded measurement), which may bias anatomical assessments. Taken together, these factors limit generalizability; the present results should be viewed as hypothesis-generating and warrant validation in larger, prospective, protocolized studies.
Future research directions should include prospective multicenter registry development with standardized surgical protocols, randomized controlled trials comparing subretinal tPA injection with pneumatic displacement for specific hemorrhage size ranges, longer-term follow-up examining visual stability and anti-VEGF treatment burden, correlation between OCT-measured hemorrhage characteristics and surgical outcomes, investigation of optimal tPA dosing regimens balancing efficacy and safety, and development of machine learning algorithms predicting treatment success based on baseline imaging features.
Conclusion
In conclusion, this multicenter analysis demonstrates that PPV with subretinal tPA injection achieves excellent functional and anatomical outcomes for SMH management across diverse etiologies. With mean visual improvement of 5.8 lines, significant macular thickness reduction, excellent fluid resolution, and favorable safety profile, this surgical approach represents an effective treatment option for thick and large submacular hemorrhages. While heterogeneity and sample size limit definitive subgroup conclusions, these findings provide supportive multicenter evidence for incorporating this technique into contemporary treatment algorithms for this challenging condition.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Confalonieri F, Ferraro V, Barone G, et al. Outcomes in the treatment of subretinal macular hemorrhage secondary to age-related macular degeneration: a systematic review. J Clin Med. 2024;13(2):367. doi:10.3390/jcm13020367
2. Shaheen A, Mehra D, Ghalibafan S, et al. Efficacy and safety of anti-VEGF injections and surgery for age-related macular degeneration-related submacular hemorrhage: a systematic review and meta-analysis. Ophthalmol Retina. 2025;9(1):4–9. doi:10.1016/j.oret.2024.07.024
3. Hochman MA, Seery CM, Zarbin MA. Pathophysiology and management of subretinal hemorrhage. Surv Ophthalmol. 1997;42(3):195–213. doi:10.1016/S0039-6257(97)00089-1
4. Chakraborty S, Sheth JU. Management of submacular hemorrhage using intravitreal brolucizumab with pneumatic displacement: a case series. Case Rep Ophthalmol. 2022;13(3):956–962. doi:10.1159/000527073
5. Sethia A, Sheth J, Gopalakrishnan M, Anantharaman G. Spontaneous formation and closure of full thickness macular hole after treatment with anti-vascular endothelial growth factor therapy in polypoidal choroidal vasculopathy. Indian J Ophthalmol. 2019;67(10):1756–1758. doi:10.4103/ijo.IJO_1597_18
6. Anantharaman G, Sheth J, Bhende M, et al. Polypoidal choroidal vasculopathy: pearls in diagnosis and management. Indian J Ophthalmol. 2018;66(7):896–908. doi:10.4103/ijo.IJO_1136_17
7. Sheth JU, Narayanan R, Anantharaman G, et al. Updated guidelines for the management of polypoidal choroidal vasculopathy: recommendations from the Indian Polypoidal Choroidal Vasculopathy Panel and the Vitreoretinal Society of India. Indian J Ophthalmol. 2022;70(8):3102–3111. doi:10.4103/ijo.IJO_2985_21
8. Sheth JU, Stewart MW, Narayanan R, et al. Macular neovascularization. Surv Ophthalmol. 2025;70(4):653–675.
9. Gabrielle PH, Delyfer MN, Glacet-Bernard A, et al. Surgery, tissue plasminogen activator, antiangiogenic agents, and age-related macular degeneration study: a randomized controlled trial for submacular hemorrhage secondary to age-related macular degeneration. Ophthalmology. 2023;130(9):947–957. doi:10.1016/j.ophtha.2023.04.014
10. Iglicki M, Zur D. New approaches in the management of submacular hemorrhages. Ophthalmologica. 2024;247(5–6):275–276.
11. Bell JE, Shulman JP, Swan RJ, Teske MP, Bernstein PS. Intravitreal versus subretinal tissue plasminogen activator injection for submacular hemorrhage. Ophthalmic Surg Lasers Imaging Retina. 2017;48(1):26–32. doi:10.3928/23258160-20161219-04
12. Patikulsila D, Winaikosol P, Choovuthayakorn J, Watanachai N, Chaikitmongkol V, Kunavisarut P. Pars plana vitrectomy and subretinal tissue plasminogen activator for large exudative submacular hemorrhage: a case series. BMC Ophthalmol. 2022;22(1):411. doi:10.1186/s12886-022-02639-w
13. Barzelay A, Daniels A, Cohen GY, Barak A, Schwartz S, Katz G. Pneumatic displacement with intravitreal tPA injection versus vitrectomy with sub retinal tPA injection in small and medium sub macular hemorrhages- a multicenter comparative study. BMC Ophthalmol. 2024;24(1):218. doi:10.1186/s12886-024-03468-9
14. Matsuo Y, Haruta M, Ishibashi Y, et al. Visual outcomes and prognostic factors of large submacular hemorrhages secondary to polypoidal choroidal vasculopathy. Clin Ophthalmol. 2021;15:3557–3562. doi:10.2147/OPTH.S327138
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of COVID-19 on Intravitreal Injection Clinic After Lockdown
Hsieh T, Gundlach BS, Ashrafzadeh S, Sarraf D, Tsui I
Clinical Ophthalmology 2022, 16:3089-3096
Published Date: 19 September 2022
Effectiveness and Safety of Intravitreal Brolucizumab for Diabetic Macular Edema After Vitrectomy: A Before-and-After Study at a Specialized Center in Japan
Saito K, Akiyama H
Clinical Ophthalmology 2025, 19:1957-1964
Published Date: 23 June 2025
Patient Experiences of Intravitreal Anti-Vascular Endothelial Growth Factor Injections for Age-Related Macular Degeneration: A Meta-Synthesis of Qualitative Studies
Liu D, Bi H, Sun Y, Gao Z, Lu P
Patient Preference and Adherence 2026, 20:610930
Published Date: 19 June 2026