Back to Journals » Clinical Ophthalmology » Volume 20
Visual Outcomes and Reading Performance of a Non-Diffractive EDOF IOL in Chinese Eyes: A Prospective Comparison of Emmetropia and Mini-Monovision Targets
Authors Chao CC, Lin YY, Sung SY, Chang YL, Chang CK
Received 13 January 2026
Accepted for publication 15 April 2026
Published 21 April 2026 Volume 2026:20 590555
DOI https://doi.org/10.2147/OPTH.S590555
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Chen-Cheng Chao,1,2 Yu-Yi Lin,3 Shao-Yu Sung,1,4 Yu-Ling Chang,5 Chao-Kai Chang1,4,6
1Nobel Eye Institute, Taipei, Taiwan; 2Graduate Institute of Clinical Medicine, National Taiwan University, Taipei, Taiwan; 3Department of Optometry, MacKay Medical University, New Taipei City, Taiwan; 4Graduate Institute of Clinical Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan; 5Department of Pediatrics, Cathay General Hospital, Taipei, Taiwan; 6Department of Medicine, MacKay Medical University, New Taipei City, Taiwan
Correspondence: Chao-Kai Chang, Email [email protected]
Purpose: To evaluate the visual outcomes, reading performance, and patient satisfaction following bilateral implantation of a non-diffractive extended depth-of-focus (EDOF) intraocular lens (IOL) in Chinese eyes, and to compare the efficacy of emmetropia versus mini-monovision targets.
Patients and Methods: This prospective, multi-center, observational study included 72 patients (144 eyes) who underwent phacoemulsification with bilateral implantation of the AcrySof IQ Vivity IOL (or Toric model). Patients were divided into two groups based on the refractive target: emmetropia (n=29) and mini-monovision (n=43). At 3 months postoperatively, binocular uncorrected distance (UDVA), intermediate (UIVA), and near (UNVA) visual acuities were assessed. Functional outcomes were evaluated using the International Reading Speed Test (IReST), the Questionnaire for Visual Disturbances (QUVID), and the Intraocular Lens Satisfaction (IOLSAT) questionnaire.
Results: At 3 months, both groups achieved excellent binocular uncorrected distance visual acuity (emmetropia: 0.03 ± 0.06 logMAR; mini-monovision: 0.05 ± 0.06 logMAR) and uncorrected intermediate visual acuity (emmetropia: 0.12 ± 0.14 logMAR; mini-monovision: 0.13 ± 0.14 logMAR). No statistically significant differences were observed in binocular UIVA (p=0.317) or UNVA (p=0.684) between the emmetropia and mini-monovision groups, although the mini-monovision group demonstrated significantly higher rates of spectacle independence (89.2% vs. 70.4%, p = 0.049). The mean reading speed improved significantly from 172 ± 67 wpm preoperatively to 201 ± 58 wpm postoperatively (p< 0.05). Regarding visual disturbances, 100% of patients in both groups reported “none to a little” for starbursts, halos, and glare. Patient satisfaction was high in both cohorts (66.7% in the emmetropia group and 79.5% in the mini-monovision group).
Conclusion: The non-diffractive Vivity IOL provides excellent distance and intermediate vision with a favorable visual disturbance profile in Chinese eyes. While the mini-monovision strategy enhanced spectacle independence and patient satisfaction, the improvements in uncorrected near acuity were not statistically significant compared to emmetropia. These short-term findings suggest that a myopic target closer to − 0.75 D or − 1.00 D may need to be evaluated to maximize chart-based near vision benefits in this population.
Keywords: extended depth of focus, EDOF, intraocular lens, IOL, non-diffractive, mini-monovision, presbyopia, visual outcomes
Introduction
Cataract remains a primary cause of visual impairment and blindness worldwide.1 With the continuous advancement of surgical techniques and rising patient expectations, modern cataract surgery has transitioned into a refractive procedure where achieving spectacle independence is a major goal.2 While traditional monofocal intraocular lenses (IOLs) provide excellent distance vision, they lack the necessary depth of focus for intermediate and near tasks, often necessitating the use of corrective lenses.2,3
To address presbyopia, various lens designs have been developed, including multifocal and extended depth of focus (EDOF) IOLs.3,4 Diffractive EDOF and multifocal lenses, while effective, are often associated with photic phenomena such as halos and glare due to their light-splitting optics, which can be particularly bothersome for certain patients.4,5 The AcrySof IQ Vivity (Alcon, Fort Worth, TX, USA) represents a significant technological shift as a non-diffractive EDOF IOL. It utilizes proprietary wavefront-shaping X-WAVE™ technology on its anterior surface to stretch and shift the wavefront, thereby elongating the focus without splitting light.6 This design aims to provide a continuous range of vision while maintaining a visual disturbance profile comparable to a monofocal lens.5,7,8
Despite the growing global adoption of non-diffractive EDOF technology, a critical knowledge gap remains regarding its optimal application in Asian populations. Chinese eyes are known to exhibit distinct biometric characteristics, including differences in pupil dynamics, anterior chamber depth, and effective lens position compared to Western cohorts, which may influence the optical performance and neuroadaptation of specialized IOLs.9,10 Furthermore, while “mini-monovision”—the practice of targeting a slight myopic offset in the non-dominant eye—is a common strategy to enhance near vision, the ideal refractive target to maximize spectacle independence without compromising patient satisfaction in this specific demographic has not been clearly established.11–13
Most existing studies on the Vivity IOL have focused either on bilateral emmetropia or randomized controlled trials in Western or South Asian populations.13,14 To our knowledge, there is a lack of prospective, multi-center data directly comparing the efficacy and functional outcomes of emmetropia versus mini-monovision targets using this non-diffractive platform specifically in Chinese eyes. This study seeks to address this gap by evaluating visual outcomes, reading performance, and patient satisfaction, providing clinical guidelines for refractive targeting in this population.
Materials and Methods
This was a prospective, multi-centered and multi-surgeons (Chen-Cheng Chao, Tsu-Te Hu, Yu-lun Luo, Yu-Ting Jeng, and Chao-Kai Chang) study. The protocol and study-specific informed consent was approved by the Joint Institutional Review Board by Medical Research Ethics Foundation, Taipei, Taiwan (permit number: IIT#70563941/22-S-016-1) and well explained to participants with written informed consent. The study adhered to the tenets of the Declaration of Helsinki and was registered at ClinicalTrials.gov (NCT# 06719882) before any patients were enrolled.
The inclusion criteria for this study were the presence of age-related cataracts in both eyes, age between 50 and 80 years, and CDVA of both eyes under logMAR 0.3, with bilateral Vivity or Vivity Toric IOLs implantation. The refractive target for the emmetropia group was plano in both eyes. For the mini-monovision group, one eye was targeted for plano, and the fellow eye was targeted for −0.50 D. Phacoemulsification cataract surgery was performed on all patients. The exclusion criteria were complicated cataract; corneal opacities or irregularities; severe dry eye (Schirmer’s test I ≤ 5 mm); amblyopia; anisometropia; coexisting ocular pathologies such as glaucoma, non-dilating pupil, history of intraocular surgery, laser therapy, or retinopathy; optic nerve or macular diseases; and refusal or inability to maintain follow-up.
Preoperative ocular dominance was not strictly utilized to determine the refractive target for the mini-monovision group. In patients with significant and often asymmetric cataracts, standard dominance tests can be confounded by varying media opacities, which may artificially skew preference toward the eye with better preoperative contrast sensitivity rather than reflecting true neurological dominance. Instead, the refractive target for each patient was determined based on comprehensive preoperative counseling, individual lifestyle requirements, and the patient’s refractive history.
Although the patient recruitment volume varied across the three centers, all participating surgeons adhered to a strictly standardized surgical protocol to minimize potential site-specific confounding factors. Clear corneal phacoemulsification and IOL implantation were performed using an identical technique to minimize differences. The surgical procedure involved topical anesthesia, a 3-step clear corneal incision (2.2 mm) at 180° (temporal in both eyes), a 5.0 mm continuous curvilinear capsulorhexis, phacoemulsification using the stop-and-chop technique, IOL implantation with an injector, IOL centration, and a sutureless incision. All surgical procedures were conducted smoothly, and all IOLs were placed in the capsular bag. Bilateral surgeries were performed as delayed sequential procedures for all patients, with an interval of one week to one month between the first and second eye surgery. The primary postoperative endpoint at 3 months was defined based on the surgery date of the second eye.
Preoperatively, all patients underwent optical biometry with the IOL Master (IOLMaster 700, Carl Zeiss); calculations were performed using the Berrett Universal II formula, and the postoperative refractive targets were set as follows: bilateral plano for the emmetropia group, and a −0.50 D offset in one eye for the mini-monovision group. Preoperative evaluation included binocular uncorrected distance visual acuity (UDVA), Questionnaire for Visual Disturbances (QUVID),15 Intraocular Lens Satisfaction questionnaire (IOLSAT)16 and Intermediate reading speed test using International Reading Speed Test (IReST).17 Preoperative refractive error was not systematically analyzed as a baseline parameter, as subjective and objective refractions are often confounded by cataract-induced myopic shifts and media opacities. Reading speed (words per minute, wpm) was calculated using the formula reading speed = number of words read correctly/time in seconds to read text x 60.
Postoperative follow up visits were at 1 week, one month and 3 months. Binocular visual acuity including UDVA, corrected distance visual acuity (CDVA), uncorrected intermediate (66cm) visual acuity (UIVA), distance corrected intermediate visual acuity (DCIVA), uncorrected near (40cm) visual acuity (UNVA), and distance corrected near visual acuity (DCNVA) were recorded. The QUVID, IOLSAT and IReST were also implemented at postoperative 3 months.
Statistical Methods
Continuous variables are presented as mean ± standard deviation (SD), and categorical variables are presented as percentages. The Chi-square test was used for categorical variables. The Mann–Whitney U-test was adopted to compare variations (postoperative sphere, cylinder, and visual acuities) between the emmetropia and mini-monovision groups. The Kruskal–Wallis test was employed to evaluate the presence of center effects.
Results
A total number of 144 eyes of 72 patients bilaterally implanted with the Alcon Vivity IOL and targeted for emmetropia (n=29) and mini-monovision (n=43) were included in this study; 24 eyes (16.7%) received a toric version. Patients were prospectively recruited across three study sites in Taiwan. The distribution of patients reflected the regional clinical volumes of the respective centers, with 44 patients (approximately 60%) recruited at the Taipei Nobel Eye Institute, 14 patients (20%) at the Taichung Nobel Eye Institute, and 14 patients (20%) at the Kaohsiung Nobel Eye Institute. The preoperative baseline characteristics are summarized in Table 1
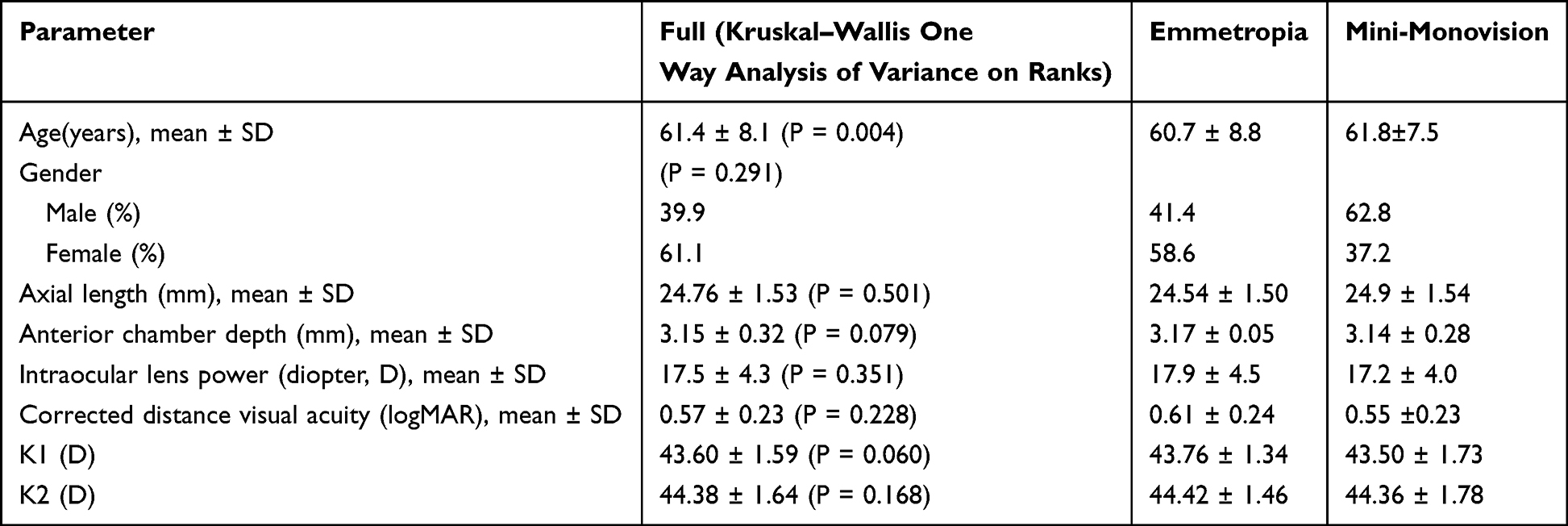 |
Table 1 Baseline Demographics |
In evaluating the refractive outcomes, postoperative mean spherical equivalent (MSE) was reported rather than mean absolute error (MAE). While MAE is the standard metric for assessing IOL formula predictability, reporting the actual postoperative MSE is crucial in this study to explicitly characterize the true refractive profile and the actual myopic offset achieved. This actual achieved refraction directly underpins the functional visual outcomes, reading performance, and spectacle independence observed in both the emmetropia and mini-monovision cohorts.
Table 2 summarizes the mean binocular postoperative visual and refractive outcomes at 3 months. To provide a more granular analysis, detailed monocular outcomes for each eye—including refractive error components and visual acuity at all tested distances—are provided as Supplementary Table S1. Statistical analysis indicated significant differences between the emmetropia and mini-monovision groups in terms of UDVA (p=0.044), DCIVA (p=0.003), and DCNVA (p=0.001). However, both groups demonstrated statistically comparable outcomes in UIVA (p=0.317), UNVA (p=0.684), and CDVA (p=0.756). Detailed logMAR values for each visual distance are presented in Table 2.
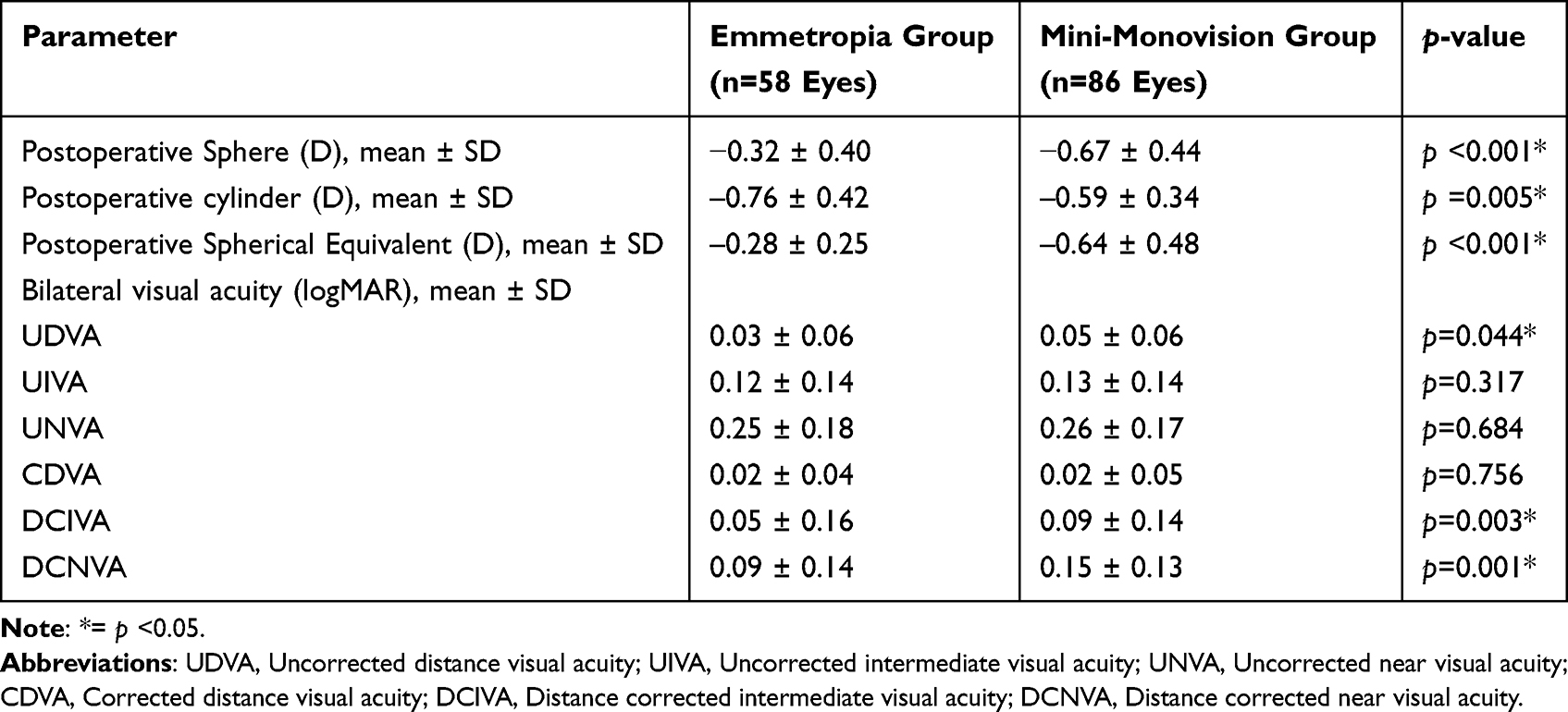 |
Table 2 Postop Refractive and Bilateral Visual Acuity Results at 3 Months |
Regarding binocular cumulative visual acuity in the emmetropia group, 62.07% of patients achieved a binocular UDVA of 20/20 or better. At intermediate distance, 65.52% achieved 20/25 or better, and at near distance, 79.31% achieved 20/40 or better. In the mini-monovision group, 65.52% achieved a binocular UDVA of 20/20 or better. At intermediate distance, 89.66% achieved 20/25 or better, and at near distance, 93.10% achieved 20/40 or better. Although the percentage of patients achieving specific thresholds appeared higher in the mini-monovision group, the mean logMAR visual acuity outcomes were statistically comparable between the two groups for uncorrected intermediate and near vision (Figures 1 and 2).
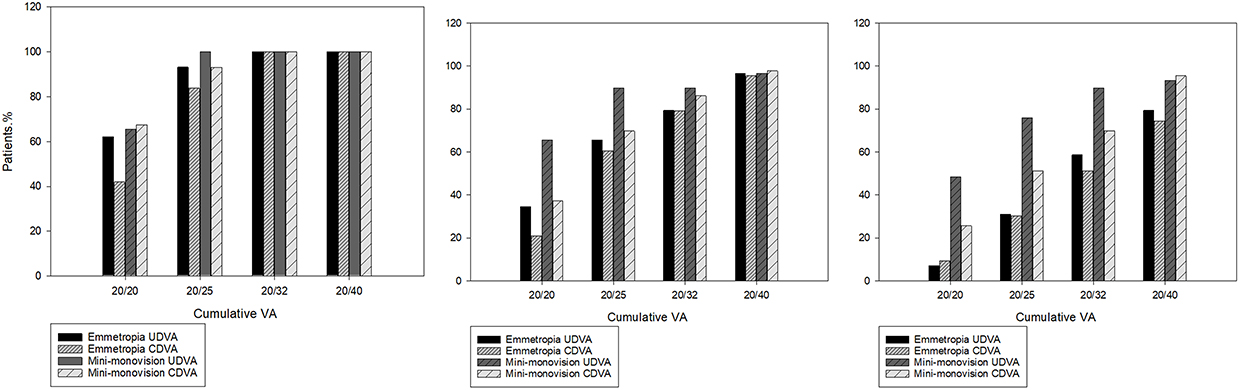 |
Figure 1 Cumulative distribution of binocular uncorrected and corrected distance, intermediate, and near visual acuity at 3 months postoperatively in the emmetropia and mini-monovision groups. |
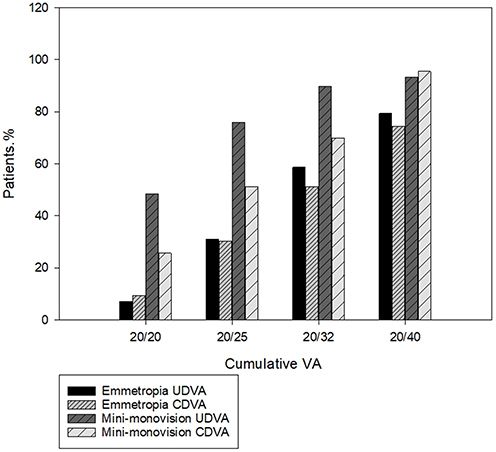 |
Figure 2 Cumulative distribution of binocular uncorrected and corrected near visual acuity at 3 months postoperatively. |
Regarding visual disturbances assessed by the QUVID questionnaire, 100% of patients in both groups reported “none to a little” for the severity and bothersomeness of starbursts, halos, and glare at 3 months postoperatively. No patients reported moderate to severe symptoms.
Patient satisfaction was high; the combined rate of patients who were “satisfied” or “very satisfied” was 66.7% in the emmetropia group and 79.5% in the mini-monovision group. (Figure 3) In terms of spectacle independence, 70.4% of patients in the emmetropia group reported “never” or “rarely” needing glasses, compared to 89.2% in the mini-monovision group, demonstrating higher satisfaction and spectacle independence in the mini-monovision cohort (Figure 4).
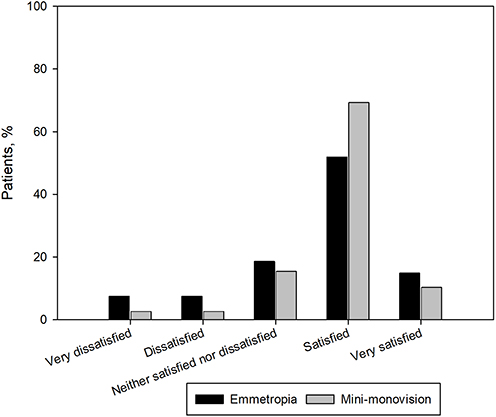 |
Figure 3 Postoperative patient satisfaction at 3 months comparing the emmetropia and mini-monovision groups. |
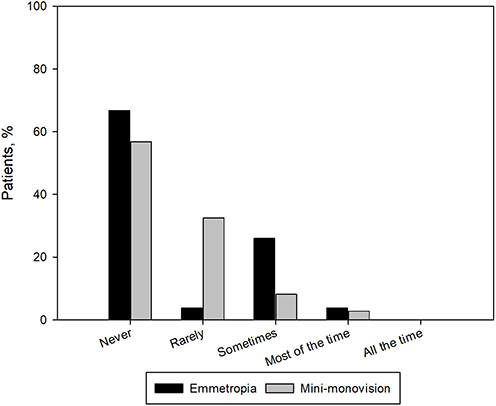 |
Figure 4 Postoperative spectacle Independence at 3 months comparing the emmetropia and mini-monovision groups. |
The overall binocular distance-corrected mean reading speed at 60 cm significantly improved from 172 ± 67 wpm preoperatively to 201 ± 58 wpm at 3 months postoperatively (p < 0.05).
Discussion
This prospective, non-randomized observational study assesses the AcrySof IQ Vivity IOL in Chinese eyes. Unlike monofocal IOLs, EDOF technology extends the visual range to enhance intermediate vision.3 While various optical designs exist—including small aperture, diffractive, and non-diffractive technologies—the goal remains to achieve excellent distance acuity with functional intermediate and near vision.4 Our findings confirm that the wavefront-shaping technology of the Vivity IOL performs robustly in the Chinese population, whose distinct biometric characteristics, such as pupil dynamics and effective lens position, differ from Western cohorts—such as variations in pupil dynamics and effective lens position —the Vivity IOL’s non-diffractive design, which relies on a central 2.2 mm wavefront-shaping zone, appears to be relatively pupil-independent, allowing it to adapt well to these specific anatomical traits.9,10 Our binocular visual acuity outcomes were comparable to or exceeded those reported in previous global reviews, suggesting that the optical performance of this non-diffractive IOL is stable and reproducible across different ethnic groups.14
Monovision is a common strategy to reduce spectacle dependence, and “mini-monovision” utilizes a smaller refractive difference (typically −0.25 D to −1.0 D) to improve near vision while minimizing adverse effects. Studies on the Vivity IOL have generally demonstrated that a mini-monovision strategy provides good distance and intermediate visual acuity with functional near vision.11–13,18–20 However, a critical finding in our study was the lack of statistical difference in UNVA between the emmetropia and mini-monovision groups (p=0.684).
This outcome warrants a critical comparison with recent literature. In a randomized study conducted in a primarily South Asian population by Vasavada et al, UNVA was found to be significantly better in the mini-monovision group.13 The discrepancy between their findings and ours may be attributed to two main factors. First, our mini-monovision group had a conservative mean spherical equivalent difference of approximately −0.64 D. Second, our sample size of 72 patients may have constrained the statistical power necessary to detect subtle differences in near visual acuity, potentially resulting in a false negative regarding statistical significance.
Despite the lack of chart-based statistical superiority for UNVA, the mini-monovision group reported significantly higher spectacle independence (89.2% vs. 70.4%). This discrepancy implies that even a modest myopic shift of −0.64 D enhances “functional ease” in daily tasks, reducing the frequency of spectacle need even if standardized clinical measurements do not show a statistical leap. Consequently, while a myopic target closer to −0.75 D or −1.00 D might be considered to achieve a distinct advantage in chart-based near acuity, this must be approached cautiously and tailored to individual patient tolerance.
Regarding visual disturbances, studies evaluating EDOF IOLs generally report a favorable profile.5,7,21 Our results align with these findings, as 100% of our patients reported “none to a little” severity for starbursts, halos, and glare. This suggests that the non-diffractive optical design effectively minimizes light-splitting artifacts, a crucial factor for Asian patients who may have high expectations regarding visual quality in low-light conditions.5,7,8,21–24 This favorable disturbance profile strongly correlates with the high patient satisfaction rates observed (79.5% in the mini-monovision group).
Consistent with the IOLSAT results in previous studies, which frequently exceed 90% satisfaction.,5,7,8 our study showed high satisfaction rates (79.5% in the mini-monovision group). This satisfaction is strongly correlated with spectacle independence. Interestingly, although the mini-monovision group did not show superior UNVA on the logMAR chart, they reported significantly higher spectacle independence (89.2% vs. 70.4%). This discrepancy implies that even a modest myopic shift of −0.64 D enhances “functional ease” in daily tasks, reducing the frequency of spectacle need even if clinical measurements do not show a statistical leap.
Reading speed provides insight into functional vision beyond static visual acuity. Our study demonstrated an average intermediate reading speed of 201 ± 58 wpm with the Vivity IOL. This performance is comparable to or better than previously reported values for multifocal IOLs (which range from 136 to 166 wpm), suggesting that the wavefront-shaping technology preserves contrast sensitivity and reading fluency effectively.25–27 It is important to note that our reading speed tests were conducted in Traditional Chinese, and cultural differences in reading habits, character recognition, and linguistic structure should be taken into account when directly comparing these reading speeds to Western studies.
It is worth noting that while a statistically significant difference in residual cylinder was observed between the two groups, this variation is likely clinically insignificant. Previous studies have demonstrated that the Vivity IOL provides a high tolerance to residual astigmatism (up to 0.50 D to 1.00 D) without significantly degrading visual quality.28,29 Given that the mean residual cylinder in both groups remained well below these thresholds, the slight disparity in astigmatism likely did not negatively impact overall visual outcomes.
Our study has several important limitations. First, this was a non-randomized observational study, which introduces inherent selection biases regarding which patients opted for mini-monovision versus emmetropia. Second, the sample size was relatively small, which limited our statistical power to detect significant differences in certain uncorrected near outcomes. Third, the follow-up period was limited to 3 months; while refractive stability is achieved early, long-term neuroadaptation requires further observation. Fourth, we did not perform defocus curve testing, which would have provided a more comprehensive understanding of the visual performance across all distances. Finally, we did not analyze the impact of angle alpha or kappa, which can be significant in refractive cataract surgery in Asian populations. Additionally, we did not explicitly evaluate the role of ocular dominance in our cohort. While identifying the dominant eye is traditional in monovision planning, the inherent unreliability of these tests in cataractous eyes and the very conservative myopic offset (≤ 0.50 D) utilized in our study suggest that dominance may have a less critical impact on visual satisfaction in a non-diffractive EDOF micro-monovision paradigm. However, the potential influence of dominance on long-term neuroadaptation to these specialized lenses remains a topic for future investigation.
Conclusion
In conclusion, the AcrySof IQ Vivity IOL serves as an effective solution for presbyopia correction in Chinese patients, delivering high patient satisfaction and minimal photic phenomena. While a conservative mini-monovision strategy enhances spectacle independence, the improvements in measured near vision were not statistically significant. These short-term, non-randomized findings suggest that while the current approach yields excellent functional outcomes, a slightly larger myopic offset may need to be carefully evaluated in future randomized trials to maximize chart-based near vision benefits.
Data Sharing Statement
The individual de-identified participant data that underlie the results reported in this article will be available. The specific data available includes the clinical outcomes (visual acuity, reading performance, and patient-reported outcomes) used for statistical analysis. The study protocol will also be made available upon request. These data and documents will be accessible to researchers who provide a methodologically sound proposal to achieve the goals of the approved proposal. Data will be available beginning 6 months and ending 5 years following article publication. Requests for data sharing should be directed to the corresponding author, Chao-Kai Chang, at [email protected].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990-2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–9. doi:10.1016/S2214-109X(17)30393-5
2. Sieburth R, Chen M. Intraocular lens correction of presbyopia. Taiwan J Ophthalmol. 2019;9(1):4–17. doi:10.4103/tjo.tjo_136_18
3. Kanclerz P, Toto F, Grzybowski A, et al. Extended depth-of-field intraocular lenses: an update. Asia Pac J Ophthalmol. 2020;9(3):194–202. doi:10.1097/APO.0000000000000296
4. Kohnen T, Suryakumar R. Extended depth-of-focus technology in intraocular lenses. J Cataract Refract Surg. 2020;46(2):298–304. doi:10.1097/j.jcrs.0000000000000109
5. Kandavel R, Colvard M, Dredge J, et al. Comparative study between non-diffractive extended depth of focus and monofocal intraocular lenses. Clin Ophthalmol. 2023;17:1161–1168. doi:10.2147/OPTH.S402069
6. Lago CM, de Castro A, Marcos S. Computational simulation of the optical performance of an EDOF intraocular lens in post-LASIK eyes. J Cataract Refract Surg. 2023;49(11):1153–1159. doi:10.1097/j.jcrs.0000000000001260
7. Carreras H, Reñones J, Carreras MDR, et al. Clinical performance of an extended range of vision intraocular lens after LASIK. J Refract Surg. 2024;40(10). doi:10.3928/1081597X-20240903-01
8. Pastor-Pascual F, Orts-Vila P, Tañá-Sanz P, et al. Non-diffractive, toric, extended depth-of-focus intraocular lenses in eyes with low corneal astigmatism. Eye and Vision. 2024;11(1):14. doi:10.1186/s40662-024-00380-7
9. Wang D, Amoozgar B, Porco T, et al. Ethnic differences in lens parameters measured by ocular biometry in a cataract surgery population. PLoS One. 2017;12(6):e0179836. doi:10.1371/journal.pone.0179836
10. Leung CK, Palmiero P-M, Weinreb RN, et al. Comparisons of anterior segment biometry between Chinese and Caucasians using anterior segment optical coherence tomography. Br J Ophthalmol. 2010;94(9):1184–1189. doi:10.1136/bjo.2009.167296
11. Solomon KD, Sandoval HP, Potvin R. Visual outcomes, satisfaction, and spectacle Independence with a nondiffractive extended vision intraocular lens targeted for slight monovision. J Cataract Refract Surg. 2023;49(7):686–690. doi:10.1097/j.jcrs.0000000000001191
12. Fernandes MC, Nunomura CY, Messias A. Visual performance and photic disturbances with diffractive and nondiffractive EDOF intraocular lenses using mini-monovision: randomized trial. J Cataract Refract Surg. 2024;50(2):153–159. doi:10.1097/j.jcrs.0000000000001330
13. Vasavada V, Vasavada SA, Shastri L, et al. Visual outcomes comparing emmetropia vs mini-monovision after bilateral implantation of a nondiffractive extended vision intraocular lens: randomized trial. J Cataract Refract Surg. 2024;50(8):799–804. doi:10.1097/j.jcrs.0000000000001458
14. Schallhorn JM. Multifocal and extended depth of focus intraocular lenses: a comparison of data from the United States food and drug administration premarket approval trials. J Refract Surg. 2021;37(2):98–104. doi:10.3928/1081597X-20201111-02
15. Lasch K, Marcus JC, Seo C, et al. Development and validation of a visual symptom-specific patient-reported outcomes instrument for adults with cataract intraocular lens implants. Am J Ophthalmol. 2022;237:91–103. doi:10.1016/j.ajo.2021.10.023
16. Urcola A, Lauzirika G, Illarramendi I, et al. Evaluation of visual, refractive, and functional outcomes after implantation of an extended depth of focus intraocular lens in patients with stable and mild glaucoma. Ophthalmol Ther. 2025;14(5):1039–1051. doi:10.1007/s40123-025-01124-z
17. Trauzettel-Klosinski S, Dietz K. Standardized assessment of reading performance: the new international reading speed texts IReST. Invest Ophthalmol Vis Sci. 2012;53(9):5452–5461. doi:10.1167/iovs.11-8284
18. Labiris G, Panagis C, Ntonti P, et al. Mix-and-match vs bilateral trifocal and bilateral EDOF intraocular lens implantation: the spline curve battle. J Cataract Refract Surg. 2024;50(2):167–173. doi:10.1097/j.jcrs.0000000000001336
19. Teus MA, Kohnen T, Ball J, et al. Visual and subject-reported outcomes of a wavefront shaping extended depth of focus intraocular lens implanted bilaterally with monovision. J Cataract Refract Surg. 2025;51(7):549–556. doi:10.1097/j.jcrs.0000000000001636
20. Zeilinger J, Kronschläger M, Schlatter A, et al. Comparing an advanced monofocal with a non-diffractive extended depth of focus intraocular lens using a mini-monovision approach. Am J Ophthalmol. 2025;271:86–95. doi:10.1016/j.ajo.2024.10.014
21. Lee MW. Visual outcomes following bilateral implantation of a non-diffractive extended depth of focus toric intraocular lens using a mini-monovision approach. Intl Ophthalmol. 2024;44(1):334. doi:10.1007/s10792-024-03247-x
22. Nguyen MTD, Yuan PH, Bachour K, et al. Visual outcomes and rotational stability of a new non-diffractive extended-vision toric intraocular lens. Can J Ophthalmol. 2024;59(4):234–240. doi:10.1016/j.jcjo.2023.05.010
23. Liu J-R, Szigiato A-A, Harasymowycz P. Outcomes of a non-diffractive extended depth of focus intraocular lens in patients with well-controlled glaucoma and ocular hypertension. Int J Ophthalmol. 2025;18(1):79–85. doi:10.18240/ijo.2025.01.09
24. Wiens J, Hall B. Visual outcomes of an extended depth of focus intraocular lens in patients with high ocular axial length. Can J Ophthalmol. 2025;60(4):e536–e540. doi:10.1016/j.jcjo.2025.01.019
25. Hienert J, Stjepanek K, Hirnschall N, et al. Visual performance of two diffractive trifocal intraocular lenses: a randomized trial. J Refract Surg. 2021;37(7):460–465. doi:10.3928/1081597X-20210420-01
26. Wendelstein JA, Casazza M, Reifeltshammer S, et al. Unilateral intraindividual comparison and bilateral performance of a monofocal spherical and diffractive extended depth of field intraocular lens mix-and-match approach. Clin Exp Ophthalmol. 2024;52(1):31–41. doi:10.1111/ceo.14315
27. Maurino V, Allan BD, Rubin GS, et al. Quality of vision after bilateral multifocal intraocular lens implantation: a randomized trial--AT LISA 809M versus AcrySof ReSTOR SN6AD1. Ophthalmology. 2015;122(4):700–710. doi:10.1016/j.ophtha.2014.10.002
28. Pedrotti E, Bonacci E, Alió Del Barrio JL, et al. Astigmatism tolerance and visual outcomes after bilateral implantation of a hybrid continuous transitional focus IOL. J Refract Surg. 2023;39(1):33–39. doi:10.3928/1081597X-20221130-02
29. Rementería-Capelo LA, Contreras I, Morán A, et al. Visual performance of eyes with residual refractive errors after implantation of an extended vision intraocular lens. J Ophthalmol. 2023;2023(1):7701390. doi:10.1155/2023/7701390
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Outcomes of a New Non-Diffractive Extended Depth-of-Focus Intraocular Lens Targeted for Mini-Monovision
Tomagova N, Elahi S, Vandekerckhove K
Clinical Ophthalmology 2023, 17:981-990
Published Date: 25 March 2023