Back to Journals » Clinical Ophthalmology » Volume 20
Visual Field Stability After Trifocal Intraocular Lens Implantation: A Longitudinal Standard Automated Perimetry Study
Authors Hida WT ![]() , Da Silva MGB, Moscovici BK
, Da Silva MGB, Moscovici BK ![]() , Vilar C, Campos PTS, Gouvea L, Chow M
, Vilar C, Campos PTS, Gouvea L, Chow M ![]() , Tzelikis PFDM
, Tzelikis PFDM ![]() , Chaves MAPD
, Chaves MAPD ![]() , Motta AFP, Lake JC, Carricondo PC
, Motta AFP, Lake JC, Carricondo PC ![]()
Received 23 December 2025
Accepted for publication 7 March 2026
Published 19 March 2026 Volume 2026:20 591088
DOI https://doi.org/10.2147/OPTH.S591088
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Bharat Gurnani
Wilson Takashi Hida,1 Maira Gomes Barbosa Da Silva,2 Bernardo Kaplan Moscovici,2– 4 César Vilar,1,5 Paulo Tadeu Silva Campos,6 Larissa Gouvea,7 Michael Chow,8 Patrick Frensel de Moraes Tzelikis,1 Mario Augusto Pereira Dias Chaves,1 Antonio Francisco Pimenta Motta,1 Jonathan Clive Lake,1 Pedro Carlos Carricondo9
1Department of Ophthalmology, Hospital Oftalmológico de Brasília, Brasília, DF, Brazil; 2Department of Ophthalmology and Visual Sciences, Federal University of São Paulo (UNIFESP), São Paulo, SP, Brazil; 3Department of Ophthalmology, Hospital Visão Laser, Santos, SP, Brazil; 4Postgraduate Program in Translational Medicine, Department of Medicine, Escola Paulista de Medicina, Federal University of São Paulo, São Paulo, SP, Brazil; 5Vilar Hospital de Olhos, Teresina, PI, Brazil; 6Renato Ambrosio Eye Research Center, Brasília, DF, Brazil; 7Storm Eye Institute, Medical University of South Carolina, Charleston SC USA; 8Department of Ophthalmology, Santa Casa de São Paulo, São Paulo, SP, Brazil; 9Department of Ophthalmology, University of São Paulo, São Paulo, SP, Brazil
Correspondence: Bernardo Kaplan Moscovici, Department of Ophthalmology and Visual Sciences, Federal University of São Paulo (UNIFESP), R. Botucatu, 822 - Vila Clementino, São Paulo, SP, 04023-062, Brazil, Tel +55 11 5085 2082, Email [email protected]
Purpose: To investigate whether implantation of a diffractive trifocal intraocular lens (IOL) is followed by systematic changes in standard automated perimetry (SAP) global indices and test reliability in a paired pre–post design.
Methods: Patients who underwent uncomplicated cataract surgery with PanOptix trifocal IOL implantation and completed SAP before and after surgery under the same institutional protocol were analyzed. Baseline SAP was obtained within 6 months preoperatively, and follow-up SAP was obtained within 12 months postoperatively. Unreliable examinations were excluded, and right and left eyes were analyzed separately. Outcomes included mean deviation (MD), pattern standard deviation (PSD), visual field index (VFI), foveal threshold, and reliability indices. Pre- and postoperative values were compared using paired tests.
Results: Reliability remained comparable to baseline. False-positive rates were 1.7% ± 2.6% preoperatively versus 1.6% ± 1.6% postoperatively in right eyes (p = 0.88) and 1.5% ± 2.1% versus 1.3% ± 1.9% in left eyes (p = 0.73). False-negative rates were 0.9% ± 1.5% versus 1.7% ± 2.1% in right eyes (p = 0.24) and 1.5% ± 2.2% versus 1.9% ± 2.5% in left eyes (p = 0.62). Global indices showed no significant pre–post differences: MD was − 1.3 ± 1.2 dB versus − 1.2 ± 0.9 dB in right eyes (p = 0.54) and − 1.7 ± 1.6 dB versus − 1.5 ± 1.6 dB in left eyes (p = 0.65). VFI was 99.0% ± 0.4% versus 98.9% ± 0.9% in right eyes (p = 0.77) and 98.2% ± 0.8% versus 97.8% ± 1.8% in left eyes (p = 0.45). PSD was unchanged (right p = 0.34; left p = 0.08). Foveal threshold decreased slightly in right eyes (35.9 ± 1.3 to 35.0 ± 1.1 dB, p = 0.06).
Conclusion: Trifocal IOL implantation was not associated with clinically meaningful deterioration in SAP global indices or reliability measures during follow-up.
Keywords: PanOptix, humphrey field analyzer, SITA standard, visual field index, cataract surgery
Introduction
Standard automated perimetry (SAP) is a cornerstone functional test for glaucoma and other optic neuropathies, and its interpretation depends on understanding both measurement variability and optical factors that can influence threshold detection. In cataract-age populations, SAP is frequently needed for diagnosis or surveillance, yet the optical status of the eye changes substantially after lens extraction and intraocular lens (IOL) implantation. As presbyopia-correcting IOLs are increasingly selected to reduce spectacle dependence, it becomes clinically relevant to clarify whether postoperative SAP results can be interpreted using the usual framework in patients implanted with these lenses.1–4
Diffractive trifocal IOLs are designed to provide functional vision across distance, intermediate, and near ranges by distributing incident light into multiple focal planes. While postoperative evaluation typically focuses on visual acuity at various distances and patient-reported visual quality, trifocal optics can, in principle, affect contrast under specific conditions, raising the question of whether threshold-based functional testing may be affected. In this context, prior perimetry-oriented work in eyes implanted with presbyopia-correcting lenses, as well as earlier observations with multifocal optics, support the rationale for evaluating SAP behavior after trifocal implantation.1–4
Beyond perimetry-specific studies, a large body of comparative clinical literature and evidence syntheses has examined outcomes with presbyopia-correcting IOLs, including visual performance across distances, contrast-related measures, dysphotopsia profiles, and patient satisfaction. Optical and conceptual reviews have further discussed how design features such as light allocation and image quality metrics may translate into real-world performance, particularly in tasks that depend on contrast and spatial resolution. These data provide important context for interpreting functional endpoints in trifocal pseudophakia.5–22
Longitudinal interpretation of SAP also requires attention to test–retest variability, learning effects, fatigue, and measurement noise, which can produce modest fluctuations even in stable eyes. Media opacity is an additional consideration: cataract can depress sensitivity measures, and cataract extraction may alter SAP indices as optical clarity improves. Therefore, in before–and–after cataract surgery designs, any observed SAP differences must be considered in light of both expected variability and the effect of cataract removal, rather than attributed to the IOL alone.23–26 Related work from our group and others has examined objective and subjective outcomes with contemporary presbyopia-correcting strategies, supporting continued investigation of functional endpoints beyond visual acuity.23–30
From a practical standpoint, many patients seeking presbyopia correction are within the age range at which glaucoma risk increases. If trifocal implantation were to systematically shift SAP global indices or compromise test reliability, postoperative fields could be more difficult to interpret and might confound longitudinal follow-up. Conversely, demonstrating stability of SAP indices and preserved reliability would support confidence in SAP interpretation in trifocal pseudophakia when perimetry becomes clinically indicated.1–4
Accordingly, the purpose of this study was to evaluate SAP parameters before and after diffractive trifocal IOL implantation using a longitudinal paired design, focusing on global indices, foveal thresholds, and test-reliability measures. By characterizing postoperative SAP behavior in eyes without ocular comorbidity expected to affect visual fields, we aim to inform clinical interpretation of perimetry in patients with trifocal IOLs.1–4
Methods
Study Design and Ethics
This single-center study used a longitudinal paired (pre–post) design. The protocol was approved by the Research Ethics Committee of Hospital Oftalmológico de Brasília (HOB), Brasília, DF, Brazil (CAAE: 36566520.3.0000.5667). Written informed consent was obtained from all participants. All procedures followed the principles of the Declaration of Helsinki.
Participants
Consecutive adults scheduled for bilateral cataract surgery with diffractive trifocal IOL implantation were screened. Eyes were eligible when no ocular, neurologic, or systemic condition was present that could reasonably affect visual field testing. Exclusion criteria included known or suspected glaucoma, other optic neuropathies, retinal disease, uveitis, prior intraocular surgery, and neurologic disorders associated with visual field defects. Cataract extraction (not clear lens exchange) was the surgical indication in included cases. Cataract grading (eg, LOCS III) and postoperative manifest refraction were not collected as standardized study variables.
Intraocular Lens and Surgery
All eyes received the AcrySof IQ PanOptix diffractive trifocal IOL (Alcon Inc, Fort Worth, TX, USA), non-toric model, implanted in the capsular bag. Phacoemulsification was performed by the same surgeon using a routine technique. Postoperative topical medications were prescribed according to standard practice (antibiotic and anti-inflammatory drops), with additional therapy when clinically indicated. No intraoperative complications were recorded.
Standard Automated Perimetry Protocol
SAP was carried out on a Humphrey Field Analyzer (Carl Zeiss Meditec, Dublin, CA, USA). The identical test algorithm and stimulus parameters were used for the preoperative and postoperative examinations, which were conducted by trained technicians following a uniform set of instructions. Test quality criteria were prespecified: fixation losses <20%, false-positive responses <15%, and false-negative responses <15%; any field not meeting these thresholds at either visit was excluded from analysis. Trial lenses were used to provide the appropriate test-distance refraction, and the same approach to refractive correction was applied at both time points. The baseline SAP examination was performed within 6 months prior to surgery, and follow-up testing was performed within 12 months after surgery, consistent with the institutional follow-up schedule. Given the known test–retest variability of SAP, longitudinal comparisons were interpreted in light of established recommendations for assessing visual field change.23,24 Because media opacity and cataract extraction can influence perimetric sensitivity, pre–post differences were also considered in that context.25,26 To reduce inter-eye dependence, right and left eyes were evaluated separately.
Outcomes
Primary outcomes were within-eye pre- to postoperative differences in SAP parameters, including global indices and foveal threshold, evaluated separately for right and left eyes. Secondary outcomes included reliability indices (fixation losses and false-positive/false-negative rates), acknowledging that cataract and cataract extraction can influence automated perimetry in cataract populations.25,26 The right and left eyes were analyzed separately to minimize inter-eye correlation.
Statistical Analysis
Continuous variables are reported as mean ± standard deviation. Baseline and postoperative measurements were compared using paired statistical tests (parametric or nonparametric, as appropriate). Analyses were performed separately for right and left eyes, using two-sided tests with p <0.05 considered statistically significant. Statistical analyses were performed in R (R Foundation for Statistical Computing, Vienna, Austria) or equivalent software. No a priori sample-size calculation was performed; therefore, the study may be underpowered to detect very small effects.
Results
Perimetry Reliability Indices
Test reliability was comparable at baseline and follow-up (Table 1). False-positive rates remained low and did not differ significantly after surgery (right eyes: 1.7% ± 2.6% vs 1.6% ± 1.6%, p = 0.88; left eyes: 1.5% ± 2.1% vs 1.3% ± 1.9%, p = 0.73). False-negative rates were also similar between visits (right eyes: 0.9% ± 1.5% vs 1.7% ± 2.1%, p = 0.24; left eyes: 1.5% ± 2.2% vs 1.9% ± 2.5%, p = 0.62) (Table 1).
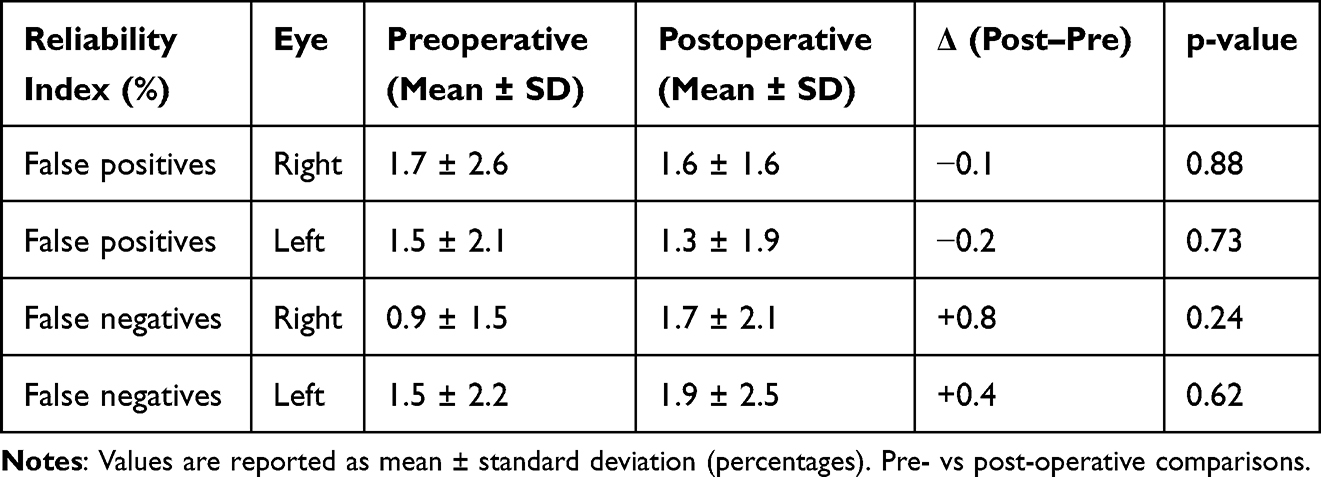 |
Table 1 Standard Automated Perimetry Reliability Indices Before and After Trifocal IOL Implantation (PanOptix) |
Global Indices (MD and VFI)
Global SAP indices showed no significant pre–post differences (Table 2). Mean deviation was stable in both eyes (right: −1.3 ± 1.2 dB vs −1.2 ± 0.9 dB, p = 0.54; left: −1.7 ± 1.6 dB vs −1.5 ± 1.6 dB, p = 0.65) (Figure 1A and Table 2). Visual field index values also remained essentially unchanged (right: 99.0% ± 0.4% vs 98.9% ± 0.9%, p = 0.77; left: 98.2% ± 0.8% vs 97.8% ± 1.8%, p = 0.45) (Figure 1B and Table 2).
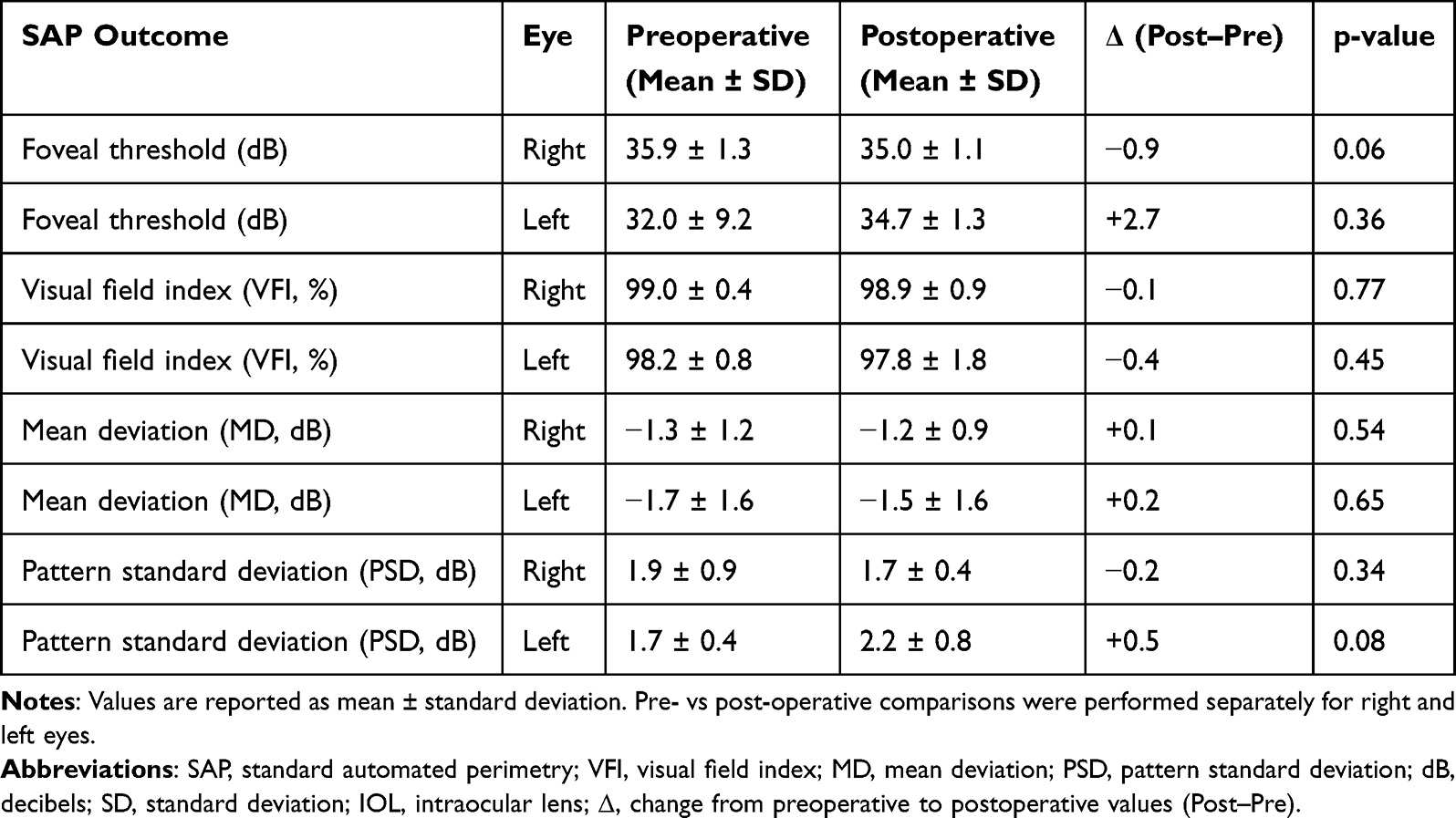 |
Table 2 Visual Field Outcomes Before and After Trifocal IOL Implantation (PanOptix) |
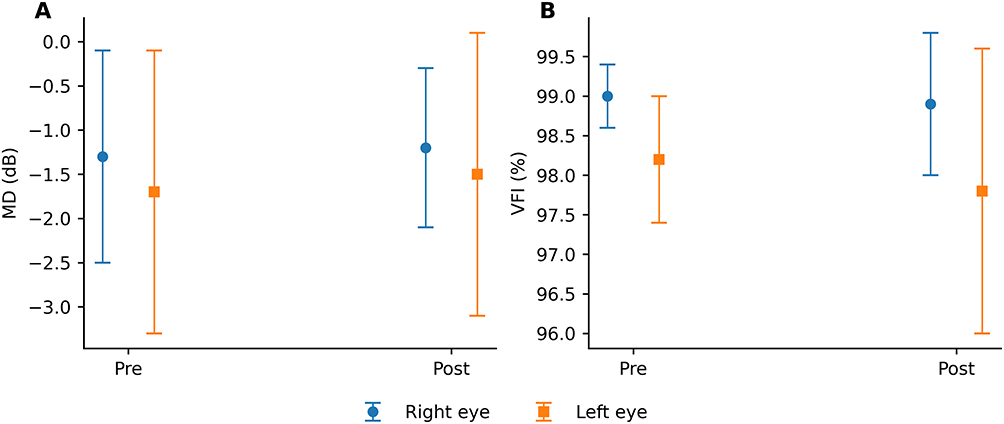 |
Figure 1 (A) Mean deviation (MD) measured by standard automated perimetry (SAP) before and after diffractive trifocal intraocular lens (IOL) implantation (PanOptix). The right and left eyes are shown separately; (B) Visual field index(VFI) measured by standard automated perimetry (SAP) before and after diffractive trifocal intraocular lens (IOL) implantation (PanOptix). The right and left eyes are shown separately. |
Pattern Standard Deviation (PSD)
Pattern standard deviation did not differ significantly between baseline and follow-up (Figure 2 and Table 2). In the right eyes, PSD decreased from 1.9 ± 0.9 dB to 1.7 ± 0.4 dB (p = 0.34). In the left eyes, PSD increased from 1.7 ± 0.4 dB to 2.2 ± 0.8 dB (p = 0.08). The direction of change was inconsistent across eyes and did not reach statistical significance.
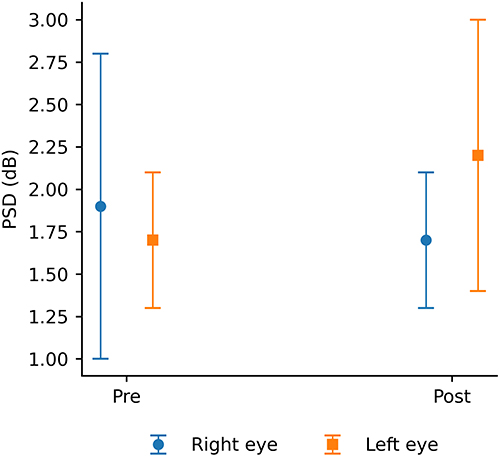 |
Figure 2 Pattern standard deviation (PSD) measured by standard automated perimetry (SAP) before and after diffractive trifocal intraocular lens (IOL) implantation (PanOptix). The right and left eyes are shown separately. |
Foveal Threshold
Foveal threshold measurements were largely preserved after surgery (Figure 3 and Table 2). In the right eyes, the mean foveal threshold decreased from 35.9 ± 1.3 dB to 35.0 ± 1.1 dB, approaching but not reaching statistical significance (p = 0.06). In the left eyes, there was no significant change (32.0 ± 9.2 dB to 34.7 ± 1.3 dB, p = 0.36) (Figure 3 and Table 2).
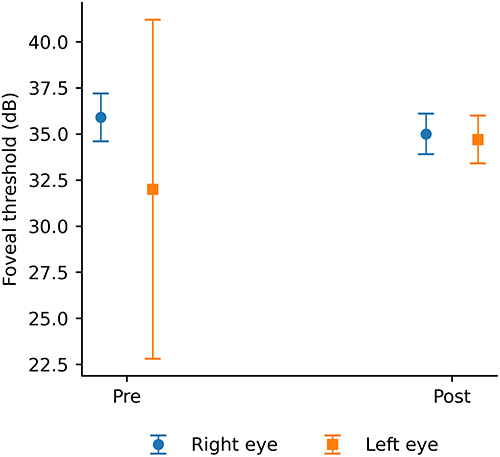 |
Figure 3 Foveal threshold (dB) measured by standard automated perimetry (SAP) before and after diffractive trifocal intraocular lens (IOL) implantation (PanOptix). The right and left eyes are shown separately. |
Discussion
In this longitudinal paired analysis, SAP outcomes after diffractive trifocal IOL implantation showed no evidence of a consistent postoperative shift in global indices or test reliability. Across both eyes, MD and VFI remained essentially stable, PSD did not change significantly, and reliability indices (false positives/false negatives) were comparable between baseline and follow-up. Taken together, these findings support the clinical interpretation that SAP can remain usable after trifocal implantation in eyes without comorbidities expected to affect the visual field.1–4
Prior work evaluating perimetry in presbyopia-correcting IOL recipients and earlier observations involving multifocal optics provide a rationale for examining SAP behavior in this setting. Our results fit the general message of this perimetry-focused literature: when test quality criteria are met and patients are appropriately selected, SAP indices do not necessarily show systematic postoperative deterioration attributable to the lens.1–4
The broader evidence base on presbyopia-correcting IOLs helps contextualize these findings. Comparative clinical studies and evidence syntheses have emphasized postoperative visual performance, quality-of-vision outcomes, and contrast-related measures, while acknowledging that optical trade-offs and dysphotopsias can occur depending on design and patient factors. Conceptual and optical reviews likewise stress that functional performance reflects interactions among residual refractive error, pupil characteristics, aberrations, and lens design rather than a single variable. In that framework, the absence of a consistent change in SAP indices in our cohort suggests that any optical effects of trifocality did not translate into a measurable group-level decrement in standard SAP metrics over the follow-up window used here.5–22
Any pre–post perimetry comparison must also be interpreted with the intrinsic variability of SAP in mind. Learning effects, attention, fatigue, and measurement noise can lead to small fluctuations in threshold testing even when reliability criteria are satisfied. Practical recommendations for assessing longitudinal change emphasize that modest differences in indices may reflect expected test–retest behavior rather than true functional change. The lack of a uniform direction of change across eyes and parameters in our dataset is most compatible with this expected variability.23,24
In addition, baseline testing is performed in the presence of cataract, whereas follow-up testing occurs after cataract extraction and IOL implantation. Because media opacity can influence perimetric sensitivity and cataract surgery can modify SAP measurements, pre–post differences may reflect changes in optical clarity in addition to any effects related to the implanted lens. In our cohort, the overall pattern was one of stability rather than a consistent increase or decrease in SAP indices, suggesting that the combined influence of cataract removal and trifocal optics did not produce a clinically meaningful shift in standard SAP outputs at the group level.25,26
Our findings can be compared with those of our recently published longitudinal SAP study in an EDOF-IOL cohort, using the same institutional perimetry approach. In that report, global indices and reliability measures likewise did not show a consistent shift from baseline to follow-up. Although the lens platform and study cohort differ, the similar overall pattern—stable global indices alongside preserved reliability—supports the practical point that SAP results can be interpreted longitudinally in pseudophakic eyes implanted with contemporary presbyopia-correcting optics when test quality is acceptable.30
Clinically, these results are relevant because patients receiving presbyopia-correcting IOLs may later require SAP for evaluation or monitoring as glaucoma risk increases with age. Demonstrating that SAP indices and reliability measures remain interpretable after trifocal implantation can help clinicians avoid over-interpreting minor fluctuations and can support routine application of established interpretive frameworks in this population, provided ocular comorbidities are absent and reliability thresholds are met.27,28 Optical discussions describing trifocal design characteristics further reinforce the value of integrating multiple functional endpoints when evaluating postoperative performance.29
This study has limitations. Postoperative SAP was obtained within a clinical follow-up window rather than at a single fixed interval, and we did not systematically capture cataract grading or postoperative manifest refraction, limiting our ability to assess how cataract severity and residual refractive error might relate to SAP metrics. Contrast sensitivity was not measured, so potential contrast-related effects could not be correlated directly with perimetric outcomes. As a paired before–after analysis, the design cannot completely separate effects related to cataract removal from those related to IOL optics. Finally, because eyes with glaucoma or other comorbidities were excluded, these findings should not be extrapolated to populations with established visual field loss, where variability and confounding may be greater.23–26
In summary, diffractive trifocal IOL implantation was not associated with clinically meaningful changes in SAP global indices or test reliability in this longitudinal paired assessment. These findings support clinical interpretation of SAP in trifocal pseudophakia using standard reliability criteria and usual interpretive principles.1–4
Acknowledgments
The authors thank the technicians and staff of the Department of Ophthalmology at the Hospital Oftalmológico de Brasília (HOB), Brasília, DF, Brazil, for their assistance with standard automated perimetry testing and study logistics.
Funding
There is nothing to disclose.
Disclosure
The authors declare that they have no financial or proprietary interests in any material discussed in this article.
References
1. Abe RY, da Silva MGB, Alves TN, Tzelikis PFM, Hida WT. Longitudinal evaluation of trifocal and extended depth of focus lenses implantation using standard automated perimetry parameters. Int Ophthalmol. 2023;43(4):1285–8. doi:10.1007/s10792-022-02526-9
2. Lee J, Mori Y, Minami K, et al. Influence of implantation of diffractive trifocal intraocular lenses on standard automated perimetry. BMC Ophthalmol. 2022;22:151. doi:10.1186/s12886-022-02372-4
3. Farid M, Chak G, Garg S, Steinert RF. Reduction in mean deviation values in automated perimetry in eyes with multifocal compared to monofocal intraocular lens implants. Am J Ophthalmol. 2014;158:227–231. doi:10.1016/j.ajo.2014.04.017
4. Aychoua N, Junoy Montolio FG, Jansonius NM. Influence of multifocal intraocular lenses on standard automated perimetry test results. JAMA Ophthalmol. 2013;131(4):481–485. doi:10.1001/jamaophthalmol.2013.2368
5. Zamora-de La Cruz D, Zúñiga-Posselt K, Bartlett J, Gutierrez M, Abariga SA. Trifocal intraocular lenses versus bifocal intraocular lenses after cataract extraction among participants with presbyopia. Cochrane Database Syst Rev. 2020;6:CD012648. doi:10.1002/14651858.CD012648.pub3
6. Shen Z, Lin Y, Zhu Y, Liu X, Yan J, Yao K. Clinical comparison of patient outcomes following implantation of trifocal or bifocal intraocular lenses: a systematic review and meta-analysis. Sci Rep. 2017;7:45337. doi:10.1038/srep45337
7. Zhu D, Karki S, Dhariwal M, Soini E, Asseburg C. Patient-reported outcomes of visual disturbances with a trifocal intraocular lens: a meta-analysis. Ophthalmol Ther. 2024. doi:10.1007/s40123-024-01085-9
8. Artal P, Arvaniti M, Dimou P, et al. Peripheral vision in patients following intraocular lens implantation: a systematic review and meta-analysis. Am J Ophthalmol. 2024;264:120–134. doi:10.1016/j.ajo.2024.03.016
9. Mencucci R, Favuzza E, Caporossi O, et al. Comparative analysis of visual outcomes, reading skills, contrast sensitivity, and patient satisfaction with two models of trifocal diffractive intraocular lenses and an extended range of vision intraocular lens. Graefes Arch Clin Exp Ophthalmol. 2018;256(10):1913–1922. doi:10.1007/s00417-018-4052-3
10. Escaf LJ, Escaf LC, Polo S, Rodríguez-Vallejo M, Fernández J. Standard results and contrast sensitivity reestablishment after implantation of a trifocal intraocular lens. Curr Eye Res. 2021;46(5):672–677. doi:10.1080/02713683.2020.1828486
11. Palomino-Bautista C, Sánchez-Jean R, Carmona-Gonzalez D, Piñero DP, Molina-Martín A. Depth of field measures in pseudophakic eyes implanted with different type of presbyopia-correcting IOLs. Sci Rep. 2021;11(1):12081. doi:10.1038/s41598-021-91654-w
12. Gundersen KG, Potvin R. Trifocal intraocular lenses: a comparison of the visual performance and quality of vision provided by two different lens designs. Clin Ophthalmol. 2017;11:1081–1087. doi:10.2147/OPTH.S136164
13. Donmez O, Asena BS, Kaskaloglu M, Akova YA. Patients satisfaction and clinical outcomes of binocular implantation of a new trifocal intraocular lens. Int Ophthalmol. 2020;40:1069–1075. doi:10.1007/s10792-020-01390-9
14. Modi S, Lehmann R, Maxwell A, et al. Visual and patient-reported outcomes of a diffractive trifocal intraocular lens compared with those of a monofocal intraocular lens. Ophthalmology. 2021;128(2):197–207. doi:10.1016/j.ophtha.2020.07.015
15. Martínez de Carneros-Llorente A, Martínez de Carneros A, Martínez de Carneros-Llorente P, Jiménez-Alfaro I. Comparison of visual quality and subjective outcomes among 3 trifocal intraocular lenses and 1 bifocal intraocular lens. J Cataract Refract Surg. 2019;45(5):587–594. doi:10.1016/j.jcrs.2018.12.005
16. Campos PTS, Hida WT, Moscovici BK, et al. Comparison of tolerance to induced astigmatism in pseudophakic eyes implanted with dual-technology diffractive IOL and enhanced monofocal IOL. Indian J Ophthalmol. 2025;73(9):1302–1306. doi:10.4103/IJO.IJO_2224_24
17. Souza LFF, Carricondo PC, Moscovici BK, Vilar CMC, Gouvea L, Hida WT. Refractive changes induced by ophthalmic viscosurgical devices in cataract surgery. Curr Eye Res. 2025;1–5. doi:10.1080/02713683.2025.2574886
18. Jonker SM, Bauer NJ, Makhotkina NY, Berendschot TT, van den Biggelaar FJ, Nuijts RM. Comparison of a trifocal intraocular lens with a +3.0 D bifocal IOL: results of a prospective randomized clinical trial. J Cataract Refract Surg. 2015;41(8):1631–1640. doi:10.1016/j.jcrs.2015.08.011
19. Bilbao-Calabuig R, Llovet-Rausell A, Ortega-Usobiaga J, et al. Visual outcomes following bilateral implantation of two diffractive trifocal intraocular lenses in 10,084 eyes. Am J Ophthalmol. 2017;179:55–66. doi:10.1016/j.ajo.2017.04.013
20. Poyales F, Pérez R, López-Brea I, Zhou Y, Rico L, Garzón N. Comparison of visual performance and patient satisfaction outcomes with two trifocal IOLs with similar optical design but different materials. Clin Ophthalmol. 2020;14:3237–3247. doi:10.2147/OPTH.S273641
21. Bissen-Miyajima H, Ota Y, Hayashi K, Igarashi C, Sasaki N. Results of a clinical evaluation of a trifocal intraocular lens in Japan. Jpn J Ophthalmol. 2020;64(2):140–149. doi:10.1007/s10384-019-00712-4
22. Alió JL, Plaza-Puche AB, Alió Del Barrio JL, et al. Clinical outcomes with a diffractive trifocal intraocular lens. Eur J Ophthalmol. 2018;28(4):419–424. doi:10.1177/1120672118762231
23. Heijl A, Lindgren G, Olsson J. Test–retest variability in glaucomatous visual fields. Am J Ophthalmol. 1989;108(2):130–135. doi:10.1016/0002-9394(89)90006-8
24. Chauhan BC, Garway-Heath DF, Goñi FJ, et al. Practical recommendations for measuring rates of visual field change in glaucoma. Br J Ophthalmol. 2008;92(4):569–573. doi:10.1136/bjo.2007.135012
25. Lam BL, Alward WLM, Kolder HE. Effect of cataract on automated perimetry. Ophthalmology. 1991;98(7):1066–1070. doi:10.1016/S0161-6420(91)32175-4
26. Smith SD, Katz J, Quigley HA. Effect of cataract extraction on the results of automated perimetry in glaucoma. Arch Ophthalmol. 1997;115(12):1515–1519. doi:10.1001/archopht.1997.01100160685004
27. Hida WT, Moscovici BK, Cortez CM, et al. Comparison of visual outcomes of bilateral dual-technology diffractive intraocular lens vs blended enhanced monofocal with dual-technology intraocular lens. J Cataract Refract Surg. 2024;50(4):401–406. doi:10.1097/j.jcrs.0000000000001374
28. Zanata MC, Vilar C, Moscovici BK, et al. Objective and subjective visual outcome comparison analysis of two diffractive presbyopic correcting intraocular lenses. Rev Bras Oftalmol. 2025;84:1–8. doi:10.37039/1982.8551.20250091
29. van den Berg AB, van den Berg RM, Moscovici BK, et al. Wavefront automated refraction comparison of three different IOLs: aspheric monofocal and two enhanced monofocal IOLs. Vision. 2026;10(1):6. doi:10.3390/vision10010006
30. Hida WT, da Silva MGB, Moscovici BK, et al. Standard automated perimetry before and after extended depth-of-focus intraocular lens implantation: longitudinal changes in global indices and test reliability. Clin Ophthalmol. 2026;20:1–8. doi:10.2147/OPTH.S591132
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Standard Automated Perimetry Before and After Extended Depth-of-Focus Intraocular Lens Implantation: Longitudinal Changes in Global Indices and Test Reliability
Hida WT, da Silva MGB, Moscovici BK, Vilar C, Campos PTS, Gouvea L, Chow M, Tzelikis PFDM, Chaves MAPD, Motta AFP, de Medeiros AL, Lake JC, Carricondo PC
Clinical Ophthalmology 2026, 20:591132
Published Date: 18 February 2026