Back to Journals » Clinical Ophthalmology » Volume 20
Standard Automated Perimetry Before and After Extended Depth-of-Focus Intraocular Lens Implantation: Longitudinal Changes in Global Indices and Test Reliability
Authors Hida WT ![]() , da Silva MGB, Moscovici BK
, da Silva MGB, Moscovici BK ![]() , Vilar C, Campos PTS, Gouvea L, Chow M
, Vilar C, Campos PTS, Gouvea L, Chow M ![]() , Tzelikis PFDM
, Tzelikis PFDM ![]() , Chaves MAPD
, Chaves MAPD ![]() , Motta AFP, de Medeiros AL, Lake JC, Carricondo PC
, Motta AFP, de Medeiros AL, Lake JC, Carricondo PC ![]()
Received 18 January 2026
Accepted for publication 17 February 2026
Published 18 February 2026 Volume 2026:20 591132
DOI https://doi.org/10.2147/OPTH.S591132
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Wilson Takashi Hida,1 Maira Gomes Barbosa da Silva,2 Bernardo Kaplan Moscovici,2– 4 César Vilar,1,5 Paulo Tadeu Silva Campos,6 Larissa Gouvea,7 Michael Chow,8 Patrick Frensel de Moraes Tzelikis,1 Mario Augusto Pereira Dias Chaves,1 Antonio Francisco Pimenta Motta,1 Andre Lins de Medeiros,1 Jonathan Clive Lake,1 Pedro Carlos Carricondo9
1Department of Ophthalmology, Hospital Oftalmológico de Brasília, Brasília, DF, Brazil; 2Department of Ophthalmology, Federal University of São Paulo (UNIFESP), São Paulo, SP, Brazil; 3Department of Ophthalmology, Hospital Visão Laser, Santos, SP, Brazil; 4Postgraduate Program in Translational Medicine, Department of Medicine, Escola Paulista de Medicina, Federal University of São Paulo, São Paulo, SP, Brazil; 5Vilar Hospital de Olhos, Teresina, PI, Brazil; 6Renato Ambrosio Eye Research Center, Brasília, DF, Brazil; 7Storm Eye Institute, Medical University of South Carolina, Charleston, SC, USA; 8Department of Ophthalmology, Santa Casa de São Paulo, São Paulo, SP, Brazil; 9Department of Ophthalmology, University of São Paulo, São Paulo, SP, Brazil
Correspondence: Bernardo Kaplan Moscovici, Department of Ophthalmology, Federal University of São Paulo (UNIFESP), Rua Cayowaá, 854, ap 82, São Paulo, SP, 05018-001, Brazil, Tel +55 11 99614-0730, Email [email protected]
Purpose: To describe changes in standard automated perimetry (SAP) parameters before and after extended depth-of-focus (EDOF) intraocular lens implantation (Symfony) in a longitudinal before–and–after design.
Methods: Patients undergoing cataract surgery with EDOF IOL implantation were evaluated with SAP preoperatively (baseline) and postoperatively (6– 12 months after surgery). Thirteen patients (23 eyes) completed both examinations. The right and left eyes were analyzed separately. Outcomes included foveal threshold, mean deviation (MD), pattern standard deviation (PSD), visual field index (VFI), and reliability indices (false-positive and false-negative rates). Data were summarized as mean ± standard deviation (SD) and compared between time points using paired tests. SAP was performed with the Humphrey Field Analyzer II using the SITA Standard 24– 2 strategy.
Results: SAP outcomes showed small, non-significant changes from baseline to follow-up. MD improved slightly (right: − 1.1 ± 1.2 to − 0.8 ± 1.2 dB, p = 0.32; left: − 1.9 ± 0.9 to − 1.2 ± 1.1 dB, p = 0.12). VFI remained stable (right: 99.1% ± 1.1% to 98.8% ± 1.4%, p = 0.43; left: 98.0% ± 1.1% to 98.0% ± 2.1%, p = 1.00). Foveal threshold was unchanged (right: 35.1 ± 1.9 to 35.2 ± 0.9 dB, p = 0.86; left: 34.0 ± 1.0 to 34.5 ± 1.3 dB, p = 0.26). PSD showed no significant variation (right: 1.9 ± 0.9 to 1.7 ± 0.4 dB, p = 0.34; left: 1.8 ± 0.3 to 1.9 ± 1.2 dB, p = 0.73). Reliability indices were also stable: false positives (right: 1.9% ± 2.6% to 2.1% ± 1.4%, p = 0.75; left: 1.4% ± 2.5% to 0.5% ± 0.6%, p = 0.21) and false negatives (right: 1.6% ± 2.1% to 1.7% ± 3.1%, p = 0.91; left: 2.2% ± 2.9% to 1.1% ± 1.5%, p = 0.35).
Conclusion: In this longitudinal before–and–after evaluation, EDOF IOL implantation was not associated with clinically meaningful changes in SAP outcomes, with stable global indices, foveal threshold, and reliability measures.
Keywords: intraocular lenses, extended depth of focus, perimetry, visual fields, cataract extraction
Introduction
Presbyopia-correcting intraocular lenses (IOLs) have evolved substantially, and extended depth-of-focus (EDOF) optics have been introduced to expand the range of functional vision while preserving optical quality. A longitudinal evaluation using standard automated perimetry (SAP) parameters after implantation of trifocal and EDOF lenses has been reported, supporting the relevance of perimetry as a functional outcome in this setting.1 Other studies have specifically investigated the influence of EDOF IOL implantation on SAP outcomes and visual field sensitivity, providing further evidence of postoperative perimetric behavior in eyes with EDOF optics.2,3 Earlier work also suggested that multifocal IOLs can influence SAP test results, reinforcing the importance of evaluating perimetry in eyes implanted with presbyopia-correcting lenses.4 Because SAP remains central to functional assessment in glaucoma and optic neuropathies, even small systematic shifts in global indices after IOL implantation may affect longitudinal interpretation in patients requiring future visual field monitoring.
Beyond perimetry-focused investigations, evidence syntheses comparing trifocal and EDOF IOLs have summarized postoperative visual performance and optical quality trade-offs across platforms, including systematic reviews and meta-analyses.5–11 Clinical comparative studies have reported visual acuity, quality of vision, contrast sensitivity, and patient-reported outcomes after bilateral implantation with trifocal or EDOF lenses, providing additional context for functional performance following presbyopia-correcting IOL implantation.12–18 Reviews of multifocal and EDOF IOL concepts and performance further discuss how design-related light distribution and contrast-related effects may influence threshold-based testing conditions.19–22
Interpretation of longitudinal SAP findings requires consideration of measurement variability. Test–retest variability is a known feature of automated perimetry, and practical recommendations exist for interpreting change over time in clinical settings.23,24 In addition, media opacity can affect automated perimetry, and cataract extraction has been associated with changes in visual field measurements, which should be considered when evaluating pre- and postoperative SAP results in cataract populations.25,26 Therefore, in a before–and–after cataract surgery design, it is important to interpret SAP changes in light of both expected test–retest behavior and the potential influence of cataract removal on perimetric sensitivity. Related work from our group has examined objective and subjective outcomes with contemporary presbyopia-correcting IOL strategies, supporting continued investigation of functional endpoints beyond visual acuity alone.27,28 Additional clinical reports have examined outcomes of combining EDOF and multifocal approaches, and optical analyses have characterized clinically relevant properties of bifocal, trifocal, and EDOF designs.29,30
Therefore, the purpose of the present study was to describe SAP parameters before and after EDOF IOL implantation using a longitudinal before–and–after design, focusing on global indices, foveal thresholds, and test-reliability measures.
Methods
Study Design and Ethical Approval
This was a single-center, longitudinal before–and–after observational study. The protocol was reviewed and approved by the Research Ethics Committee of Hospital Oftalmológico de Brasília (HOB), Brasília, DF, Brazil (CAAE: 36566520.3.0000.5667), and all participants provided written informed consent before enrollment. The study adhered to the tenets of the Declaration of Helsinki.
Participants and Eligibility Criteria
Adults aged 50–79 years scheduled for cataract surgery with implantation of an extended depth-of-focus (EDOF) intraocular lens (IOL) were consecutively recruited. Thirteen patients (23 eyes) completed both baseline and follow-up SAP examinations. Eyes were included if no ocular condition was present that could reasonably affect visual field testing. Exclusion criteria comprised known or suspected glaucoma, optic nerve disease, retinal pathology, prior intraocular surgery, uveitis, or neurologic disorders associated with visual field defects. Eyes were also excluded if postoperative complications occurred that could affect visual field testing.
Intraocular Lens and Surgery
All eyes received an EDOF IOL (Symfony) (Tecnis Symfony, Johnson & Johnson Vision, Santa Ana, CA, USA). Phacoemulsification with in-the-bag IOL implantation was performed by the attending surgeon using routine surgical technique. Postoperative topical therapy (antibiotic and anti-inflammatory drops) was administered in accordance with the institutional standard protocol.
Cataract Grading and Visual Acuity
Cataract severity was graded using the Lens Opacities Classification System III (LOCS III), and eyes with nuclear opalescence grades NO2–NO3 were included. Preoperative and postoperative visual acuity of 20/40 or better was required for SAP testing.
Standard Automated Perimetry Protocol
Standard automated perimetry (SAP) was carried out at two time points: preoperatively (baseline) and postoperatively (follow-up), using the same device and test strategy at both visits. SAP was performed using the Humphrey Field Analyzer II (Carl Zeiss Meditec) with the SITA Standard 24–2 strategy (Goldmann size III). Trained technicians performed examinations under standardized instructions. Reliability parameters recorded by the perimeter were used to assess test quality. Tests were considered reliable if fixation losses were <20%, false-positive errors <15%, and false-negative errors <15%. Baseline SAP was obtained within 6 months before surgery, and follow-up SAP was performed 6–12 months after surgery. To minimize potential inter-eye correlation, right and left eyes were analyzed separately. Because SAP measurements show inherent variability across repeated tests and require careful interpretation of longitudinal change, SAP outcomes were considered within the framework of established test–retest behavior and recommendations for monitoring visual field change over time.23,24 In addition, given that cataract and cataract extraction can influence automated perimetry, baseline-to-follow-up comparisons were interpreted with awareness of cataract-related effects reported in the literature.25,26 No additional statistical adjustment for cataract-related effects was performed beyond the within-eye before–and–after comparison and the interpretation within published cataract/SAP evidence.
Outcomes
Primary outcomes were changes from baseline to follow-up in global SAP indices and foveal threshold, assessed separately for right and left eyes. Secondary outcomes included SAP reliability indices, specifically false-positive and false-negative rates.
Statistical Analysis
Data are presented as mean ± standard deviation (SD). Baseline and follow-up values were compared using paired statistical tests, with a two-sided significance threshold of p < 0.05. Analyses were performed separately for right and left eyes. Statistical analyses were conducted using standard statistical software. Analyses were performed in R (version 4.2, R Foundation for Statistical Computing, Vienna, Austria). Given the descriptive nature of this longitudinal study, no formal a priori sample size calculation was performed. A post-hoc sensitivity analysis indicated that the current sample size (23 eyes) had limited ability to detect very small changes in mean deviation (eg, approximately 0.3 dB would require n≈97 eyes, assuming SD of paired differences ≈1.3 dB, α = 0.05, two-sided).
Results
Study Population
Thirteen patients (23 eyes) completed both baseline and follow-up SAP examinations. The mean age of the patients was 64.1 years (SD ± 6.2), with 70% male and 30% female.
Standard Automated Perimetry Outcomes
Standard automated perimetry outcomes showed small, non-significant pre-to-postoperative changes in both eyes (Table 1 and Figure 1). Mean deviation (MD) demonstrated mild improvement without statistical significance (right: −1.1 ± 1.2 dB preoperatively vs −0.8 ± 1.2 dB postoperatively, p = 0.32; left: −1.9 ± 0.9 dB vs −1.2 ± 1.1 dB, p = 0.12) (Table 1 and Figure 1). Visual field index (VFI) remained essentially unchanged (right: 99.1% ± 1.1% vs 98.8% ± 1.4%, p = 0.43; left: 98.0% ± 1.1% vs 98.0% ± 2.1%, p = 1.00) (Table 1 and Figure 1).
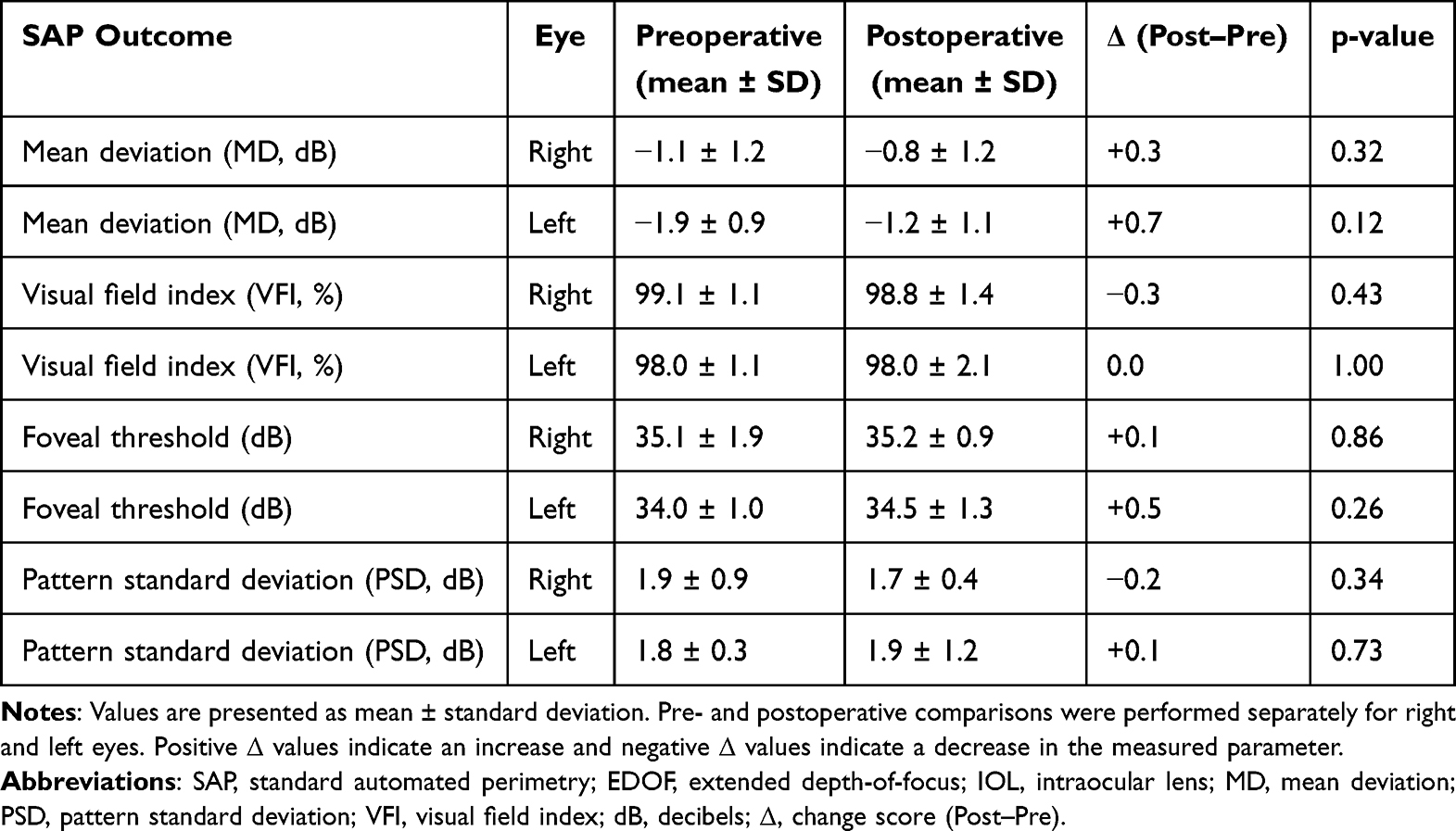 |
Table 1 Standard Automated Perimetry Outcomes Before and After EDOF IOL Implantation (Symfony), with Change Scores |
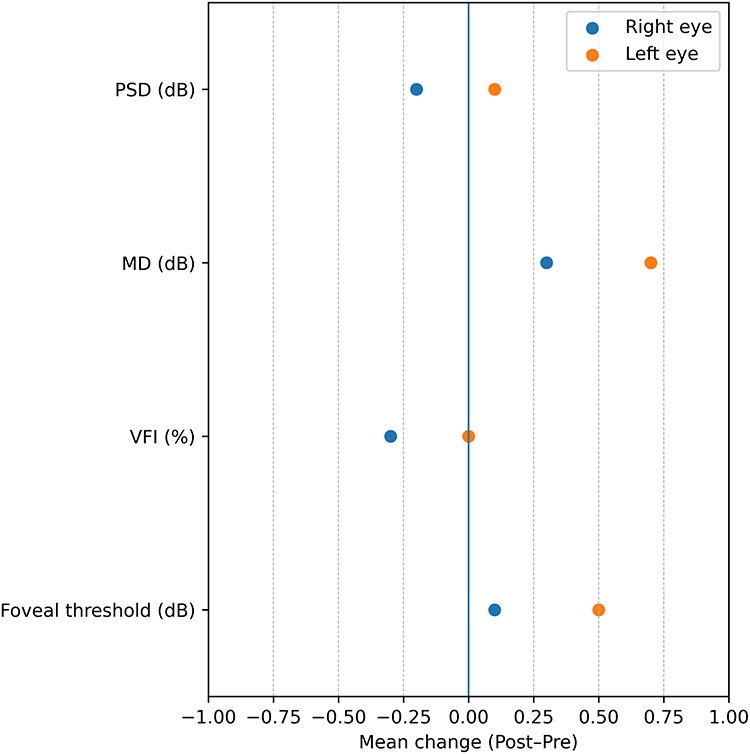 |
Figure 1 Mean change (Post–Pre) in standard automated perimetry (SAP) outcomes before and after extended depth-of-focus intraocular lens (EDOF IOL) implantation (Symfony). The vertical line at 0 indicates no change. The right and left eyes were analyzed separately. |
Foveal threshold values were stable over time. Right eyes showed no meaningful change (35.1 ± 1.9 dB vs 35.2 ± 0.9 dB, p = 0.86), while left eyes demonstrated a small, non-significant increase (34.0 ± 1.0 dB vs 34.5 ± 1.3 dB, p = 0.26) (Table 1 and Figure 1). Pattern standard deviation (PSD) also showed no statistically significant change (right: 1.9 ± 0.9 dB vs 1.7 ± 0.4 dB, p = 0.34; left: 1.8 ± 0.3 dB vs 1.9 ± 1.2 dB, p = 0.73) (Table 1 and Figure 1). The change-score visualization shows that outcome deltas were centered near zero for most parameters, with no consistent direction of change across eyes (Figure 1).
Perimetry Reliability Indices
Reliability indices remained stable from baseline to follow-up (Table 2 and Figure 2). False-positive rates were low at both time points and did not change significantly (right: 1.9% ± 2.6% vs 2.1% ± 1.4%, p = 0.75; left: 1.4% ± 2.5% vs 0.5% ± 0.6%, p = 0.21) (Table 2 and Figure 2). False-negative rates were likewise unchanged (right: 1.6% ± 2.1% vs 1.7% ± 3.1%, p = 0.91; left: 2.2% ± 2.9% vs 1.1% ± 1.5%, p = 0.35) (Table 2 and Figure 2). Consistent with these findings, change scores for reliability indices clustered near zero in both eyes, indicating comparable test quality at baseline and follow-up (Figure 2).
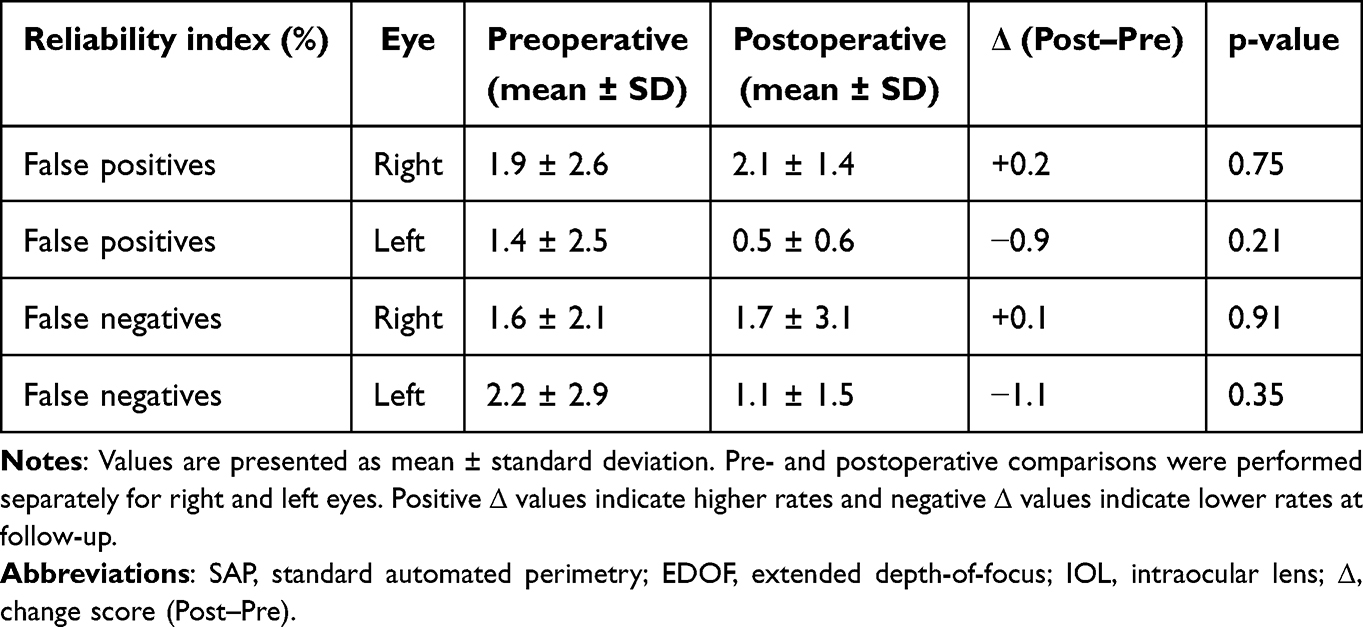 |
Table 2 Standard Automated Perimetry Reliability Indices Before and After EDOF IOL Implantation (Symfony), with Change Scores |
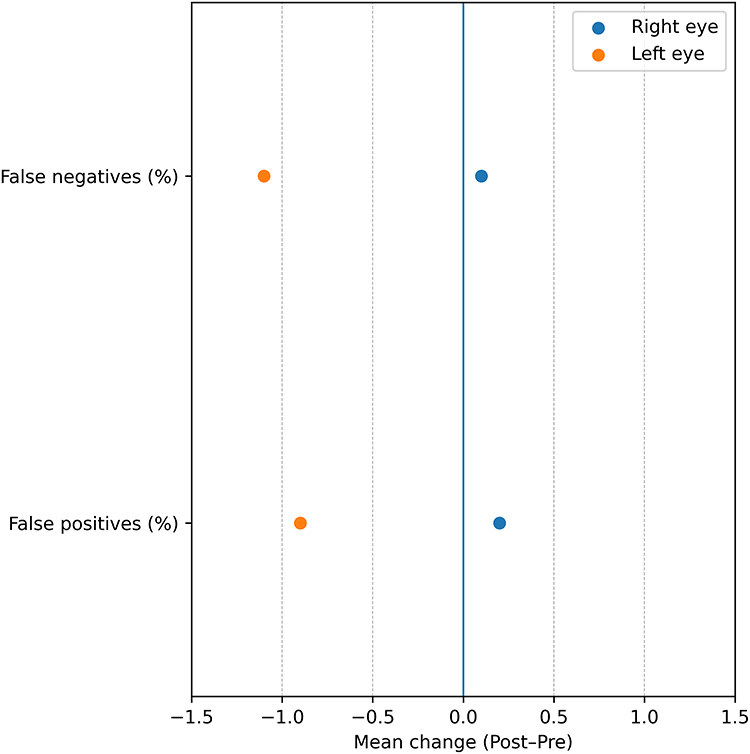 |
Figure 2 Mean change (Post–Pre) in standard automated perimetry (SAP) reliability indices before and after extended depth-of-focus intraocular lens (EDOF IOL) implantation (Symfony). The vertical line at 0 indicates no change. The right and left eyes were analyzed separately. |
Discussion
In this longitudinal before–and–after assessment, SAP outcomes following EDOF IOL implantation showed minimal change from baseline to follow-up, with small differences across global indices, foveal thresholds, and reliability measures. The overall pattern was one of stability rather than a directional shift in sensitivity. This result is consistent with the EDOF-focused perimetry literature, in which postoperative SAP indices and visual field sensitivity have generally remained unchanged after implantation, even when specific parameters show small fluctuations.2,3 Our findings also align with the longitudinal report evaluating SAP parameters after both trifocal and EDOF implantation, which found no clinically meaningful postoperative deterioration overall.1 The absence of significant changes in reliability indices further supports that the observed outcome differences are unlikely to be driven by systematic changes in test quality.
A useful way to interpret the present results is through the lens of change-score magnitude. The change values for MD, VFI, PSD, and foveal threshold were close to zero. They did not show a consistent pattern across eyes, suggesting that the observed differences are more consistent with expected variability than with a true lens-related effect. Automated perimetry exhibits test–retest variability, and practical guidance emphasizes caution when attributing small pre–post differences to meaningful functional change.23,24 This is particularly relevant when global indices remain stable, and reliability metrics do not worsen, as in the present dataset.
Unlike diffractive multifocal designs that split light into distinct foci, EDOF optics are intended to extend the range of focus while preserving optical quality. Reviews and meta-analyses have generally reported favorable outcomes with EDOF lenses, including optical quality and patient-reported measures, while acknowledging design- and patient-related trade-offs.5–11,19–22 In threshold-based testing, such as SAP, contrast-related effects are expected to manifest as small differences in sensitivity rather than dramatic changes in global indices. The stability observed here supports the clinical impression that routine SAP remains interpretable after EDOF implantation in eyes without ocular comorbidity.
An additional consideration in a before–and–after cataract surgery design is the influence of media opacity and its removal. Cataract can depress perimetric sensitivity, and cataract extraction has been associated with changes in automated perimetry in different settings.25,26 In principle, improved media clarity after surgery could enhance measured sensitivity, whereas the optical characteristics of presbyopia-correcting lenses could exert opposing effects under certain conditions. The net result observed in this cohort was essentially neutral, with no consistent shift in either direction, suggesting that these factors did not translate into measurable changes in standard SAP indices at the group level. One plausible explanation for the absence of a statistically significant improvement in MD is that baseline SAP indices were already near normal (high VFI and mildly negative MD), limiting the potential for measurable postoperative gains (ceiling effect). In addition, because cataract severity was limited to NO2–NO3, any baseline cataract-related depression in SAP may have been modest, resulting in only small postoperative gains after media clarity improved. Finally, subtle contrast-related effects of EDOF optics in threshold-based testing could offset small improvements from cataract removal, leading to an overall neutral group-level change.
This study has limitations. The analysis is based on summarized group-level results and on separate evaluations of the right and left eyes, which limits patient-level modeling and precludes assessment of the distribution of individual changes. Sample size and follow-up duration may also reduce sensitivity to detect very small effects. Finally, SAP outcomes may be influenced by learning effects, attention, and intrinsic variability despite acceptable reliability indices.23,24 Sample size and follow-up duration may reduce sensitivity to detect very small effects. However, the observed changes were small, non-directional, and compatible with expected test–retest variability. Future studies, using individual-level data, could quantify inter-eye correlation, explore predictors of change, and incorporate additional measures of optical quality to elucidate mechanisms.
In conclusion, EDOF IOL implantation was associated with stable SAP outcomes in this longitudinal before–and–after evaluation, with small changes in global indices, foveal thresholds, and reliability measures. These findings support the interpretability of SAP following EDOF implantation and are consistent with prior reports on perimetry in eyes with EDOF optics.1–3
Disclosure
The authors declare that they have no financial or proprietary interests in any material discussed in this article.
References
1. Abe RY, da Silva MGB, Alves TN, Tzelikis PFM, Hida WT. Longitudinal evaluation of trifocal and extended depth of focus lenses implantation using standard automated perimetry parameters. Int Ophthalmol. 2023;43(4):1285–8. doi:10.1007/s10792-022-02526-9
2. Lee J, Mori Y, Nejima R, Minami K, Miyata K. Influence of implantations of extended depth-of-focus on standard automated perimetry. Sci Rep. 2020;10(1):20153. doi:10.1038/s41598-020-77214-8
3. Takahashi M, Yamashiro C, Yoshimoto T, et al. Influence of extended depth of focus intraocular lenses on visual field sensitivity. PLoS One. 2020;15(9):e0237728. doi:10.1371/journal.pone.0237728
4. Aychoua N, Junoy Montolio FG, Jansonius NM. Influence of multifocal intraocular lenses on standard automated perimetry test results. JAMA Ophthalmol. 2013;131(4):481–485. doi:10.1001/jamaophthalmol.2013.2368
5. Tavassoli S, Ziaei H, Yadegarfar ME, et al. Trifocal versus extended depth of focus (EDOF) intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2024:
6. Karam M, Alkhowaiter N, Alkhabbaz A, et al. Extended depth of focus versus trifocal for intraocular lens implantation: an updated systematic review and meta-analysis. Am J Ophthalmol. 2023;251:52–70. doi:10.1016/j.ajo.2023.01.024
7. Zhong Y, Wang K, Yu X, Liu X, Yao K. Comparison of trifocal or hybrid multifocal–extended depth of focus intraocular lenses: a systematic review and meta-analysis. Sci Rep. 2021;11(1):6699. doi:10.1038/s41598-021-86222-1
8. Cho JY, Won YK, Park J, et al. Visual outcomes and optical quality of accommodative, multifocal, extended depth-of-focus, and monofocal intraocular lenses in presbyopia-correcting cataract surgery: a systematic review and Bayesian network meta-analysis. JAMA Ophthalmol. 2022;140(11):1045–1053. doi:10.1001/jamaophthalmol.2022.3667
9. Daka Q, Henein C, Fang CEH, et al. Effectiveness of intraocular lenses designed to correct presbyopia after cataract surgery: an overview of systematic reviews. Br J Ophthalmol. 2025;109(12):1323–1329. doi:10.1136/bjo-2025-327363
10. La Paz M D, Tsai LM. Outcomes and predictive factors in multifocal and extended-depth-of-focus intraocular lens implantation. Curr Opin Ophthalmol. 2024;35(1):28–33. doi:10.1097/ICU.0000000000001013
11. Artal P, Arvaniti M, Dimou P, et al. Peripheral vision in patients following intraocular lens implantation: a systematic review and meta-analysis. Am J Ophthalmol. 2024;264:120–134. doi:10.1016/j.ajo.2024.03.016
12. Tran DB, Owyang A, Hwang J, Potvin R. Visual acuity, quality of vision, and patient-reported outcomes after bilateral implantation with a trifocal or extended depth of focus intraocular lens. Clin Ophthalmol. 2021;15:403–412. doi:10.2147/OPTH.S295503
13. Singh B, Sharma S, Dadia S, Bharti N, Bharti S. Comparative evaluation of visual outcomes after bilateral implantation of a diffractive trifocal intraocular lens and an extended depth of focus intraocular lens. Eye Contact Lens. 2020;46(5):314–318. doi:10.1097/ICL.0000000000000637
14. Savini G, Balducci N, Carbonara C, et al. Functional assessment of a new extended depth-of-focus intraocular lens. Eye. 2019;33(3):404–410. doi:10.1038/s41433-018-0221-1
15. Palomino-Bautista C, Sánchez-Jean R, Carmona-Gonzalez D, Piñero DP, Molina-Martín A. Depth of field measures in pseudophakic eyes implanted with different types of presbyopia-correcting IOLs. Sci Rep. 2021;11(1):12081. doi:10.1038/s41598-021-91654-w
16. Escaf LJ, Escaf LC, Polo S, Rodríguez-Vallejo M, Fernández J. Standard results and contrast sensitivity reestablishment after implantation of a trifocal intraocular lens. Curr Eye Res. 2021;46(5):672–677. doi:10.1080/02713683.2020.1828486
17. Asena L, Kırcı Doğan İ, Oto S, Dursun Altınörs D. Comparison of visual performance and quality of life with a new nondiffractive EDOF intraocular lens and a trifocal intraocular lens. J Cataract Refract Surg. 2023;49(5):504–511. doi:10.1097/j.jcrs.0000000000001142
18. Mencucci R, Favuzza E, Caporossi O, et al. Comparative analysis of visual outcomes, reading skills, contrast sensitivity, and patient satisfaction with two models of trifocal diffractive intraocular lenses and an extended range of vision intraocular lens. Graefes Arch Clin Exp Ophthalmol. 2018;256(10):1913–1922. doi:10.1007/s00417-018-4052-3
19. Breyer DRH, Kaymak H, Ax T, et al. Multifocal intraocular lenses and extended depth of focus intraocular lenses. Asia Pac J Ophthalmol. 2017;6(4):339–349.
20. Rampat R, Gatinel D. Multifocal and extended depth-of-focus intraocular lenses: current concepts, outcomes and future perspectives. Ophthalmology. 2021;128(11):e164–e185. doi:10.1016/j.ophtha.2020.09.026
21. Schallhorn JM. Multifocal and extended depth of focus intraocular lenses: a comparison of data from the United States Food and Drug Administration premarket approval trials. J Refract Surg. 2021;37(2):98–104. doi:10.3928/1081597X-20201111-02
22. de Vries NE, RMMA N, González-García MJ, Coco-Martín MB, Sobrado-Calvo P, Maldonado MJ. Multifocal intraocular lenses and contrast sensitivity. J Cataract Refract Surg. 2013;39(2):242–252. doi:10.1016/j.jcrs.2012.08.061
23. Heijl A, Lindgren G, Olsson J. Test–retest variability in glaucomatous visual fields. Am J Ophthalmol. 1989;108(2):130–135. doi:10.1016/0002-9394(89)90006-8
24. Chauhan BC, Garway-Heath DF, Goñi FJ, et al. Practical recommendations for measuring rates of visual field change in glaucoma. Br J Ophthalmol. 2008;92(4):569–573. doi:10.1136/bjo.2007.135012
25. Lam BL, Alward WLM, Kolder HE. Effect of cataract on automated perimetry. Ophthalmology. 1991;98(7):1066–1070. doi:10.1016/S0161-6420(91)32175-4
26. Koucheki B, Nouri-Mahdavi K, Patel G, et al. Visual field changes after cataract extraction: the AGIS experience. Am J Ophthalmol. 2004;138(6):1022–1028. doi:10.1016/j.ajo.2004.08.006
27. Hida WT, Moscovici BK, Cortez CM, et al. Comparison of visual outcomes of bilateral dual-technology diffractive intraocular lens vs blended enhanced monofocal with dual-technology intraocular lens. J Cataract Refract Surg. 2024;50(4):401–406. doi:10.1097/j.jcrs.0000000000001374
28. Zanata MC, Vilar C, Moscovici BK, et al. Objective and subjective visual outcome comparison analysis of two diffractive presbyopic correcting intraocular lenses. Rev Bras Oftalmol. 2025;84:1–8. doi:10.37039/1982.8551.20250091
29. Black S. Visual outcomes after combining extended depth-of-focus and multifocal intraocular lenses. Clin Ophthalmol. 2018;12:2129–2136. doi:10.2147/OPTH.S175901
30. Gatinel D, Loicq J. Clinically relevant optical properties of bifocal, trifocal, and extended-depth-of-focus intraocular lenses. J Refract Surg. 2016;32(4):273–280. doi:10.3928/1081597X-20160121-07
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.