Back to Journals » Clinical Ophthalmology » Volume 17
Visual Field Progression After Glaucoma Surgery in Pseudoexfoliation versus Primary Glaucoma
Received 21 July 2023
Accepted for publication 25 September 2023
Published 12 October 2023 Volume 2023:17 Pages 3037—3045
DOI https://doi.org/10.2147/OPTH.S431723
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Aparna Rao, Rakhi P D’Cruz
Glaucoma Service, LV Prasad Eye Institute, MTC Campus, Bhubaneswar, India
Correspondence: Aparna Rao, LV Prasad Eye Institute, MTC Campus, Bhubaneswar, 751024, India, Tel +91 674 398 7999/7201, Fax +91 674 398 7130, Email [email protected]; [email protected]
Purpose: To compare visual field progression in severity-matched pseudoexfoliation glaucoma (XFG) and primary glaucoma after intraocular pressure (IOP) reduction by filtering surgery.
Methods: Patients with XFG (n=32), primary open-angle glaucoma (POAG, n=33) or primary angle closure glaucoma (PACG, n=28) that underwent routine cataract and glaucoma filtering surgery by the same surgeon (APR) between May 2017 and September 2021, were included for this prospective study. Rate of progression (ROP) was determined using guided progression analysis and compared between XFG and primary glaucoma. Multivariate regression was done to analyse the factors responsible for progression in each group.
Results: Visual field progression after surgery was noted in 48 eyes (n=11 XFG, 18 POAG and 19 PACG eyes) at a mean follow-up of 10± 5.6 months after surgery with RVI seen in 18 of 48 eyes. The final IOP (p=0.8) and mean ROP (p=0.09) were not significantly different between XFG and primary glaucoma. The XFG eyes had a greater number of eyes (36%) showing an ROP worse than − 5dB/yr, with 45% of eyes showing an IOP spike > 5mm Hg, and a higher mean IOP spike between visits. The ROP in eyes with RVO and > 5mm Hg IOP spikes was greater in XFG than in POAG or PACG. In the multivariate analysis, higher IOP fluctuations > 5mm Hg, and associated retinal vein occlusions (RVO) were significant factors for visual progression greater than − 5dB/year (R2=53.5%) in POAG and XFG eyes. Age, gender, baseline MD, and number of medications before surgery or at final follow-up did not influence visual progression rates in either group.
Conclusion: A higher IOP fluctuation > 5mm Hg and associated RVO were the significant factors predicting visual field progression after filtering surgery in XFG and POAG eyes. Control of both IOP-dependent and -independent mechanisms of VF progression is therefore essential in these eyes.
Keywords: pseudoexfoliation syndrome, pseudoexfoliation glaucoma, visual field, glaucoma progression, primary glaucoma
Introduction
Exfoliation syndrome /glaucoma has been recognized as a unique disease with distinctive identifiable clinical features that is refractory to conventional treatment.1,2 The presence of exfoliation is a known risk factor for faster rates of glaucoma progression, and this differentiates it from other forms of primary glaucoma.1–4 The untreated intraocular pressure (IOP) is reported to be higher in exfoliation glaucoma (XFG) than other primary glaucoma including primary open-angle glaucoma (POAG), angle closure glaucoma (PACG) and normal tension glaucoma (NTG).1,2,4–7 The medical and surgical treatment of XFG is more challenging, with more severe disease at presentation, higher rates of intraoperative complications, and frequent systemic and ocular co-morbid associations.1,8,9
Preservation of visual function remains the main goal of IOP reduction in glaucoma treatment and surgery. It is understood that IOP reduction by itself slows down or halts progressive disease, and therefore changes the rate of decline of visual field changes over time.4–6,8 Both IOP-dependent and -independent risk factors for glaucoma progression have been identified in primary glaucoma, including POAG, PACG, and NTG.4,5,8 While the goal of therapy for glaucoma remains IOP reduction, it is also known that a small proportion of eyes may still progress after achieving the target IOP. This paradox is often complicated by differences in the severity of the disease at presentation in most studies comparing different forms of glaucoma. Further, most studies do not consider the re-establishment of longitudinal visual field (VF) slopes or the overall course of the disease after surgical intervention.6,7 While it is recognized that XFS is unique from other forms of glaucoma, its presence by itself portends a worse prognosis in patients with the disease.4,5 While the Early Manifest Glaucoma Trial (EMGT) and Ocular hypertension study (OHTS) identified XFS as a risk factor for glaucoma progression, this holds true only for untreated cases.4,6 It is unclear if XFG eyes behave similarly or differently from high-tension primary glaucoma after adequate IOP reduction with medical or surgical therapy. Several independent studies have reported comparable IOP reduction in XFG eyes with medical or surgical therapy, challenging the conventional knowledge of XFS disease being an independent risk factor for glaucoma progression.9–12
Konstas et al has reported progression in >70% XFG eyes with an IOP of 20mm Hg or more.2 They did observe, however, that a small proportion of patients (28%) may still progress despite aggressive therapy in XFG. This may be attributed to other systemic and ocular associations in XFG that pose challenges to the preservation of visual function in XFG eyes. Ayala et al observed a 58% GPA progression rate in XFG compared to 13% in POAG eyes over 3 years.11 Yet, the authors have not mentioned if the slope in mean deviation (MD) or GPA was any different after surgery in POAG and XFG eyes. Very few studies focus on the long-term IOP and visual field changes with treatment in XFG and other forms of primary glaucoma. While some risk factors like uncontrolled IOP and worse visual field at presentation may be the cause for faster progression in XFG compared to POAG, long-term outcomes in severity matched XFG and primary glaucoma after similar IOP reduction after surgical treatment are lacking. This is crucial to answering if XFG eyes indeed are an independent risk for visual field progression despite similar IOP reductions by surgery.
Methods
This study was approved by the institutional review board of LVPEI, MTC campus, Bhubaneswar, India, and followed the tenets of the Declaration of Helsinki. We included patients from a prospective study (2019–140-IM-28) evaluating long-term medical and surgical outcomes of pseudoexfoliation disease stages seen at a tertiary eye care setting between May 2017 and September 2021 after a written informed consent as per institutional protocol. Pseudoexfoliation glaucoma was diagnosed in the presence of flaky white material on the lens capsule with glaucomatous optic neuropathy, and corresponding visual field (VF) changes. Both patients with open and closed angles XFG were included. POAG and PACG were diagnosed using standard International Society Geographical & Epidemiological Ophthalmology (ISGEO) definitions, and these were matched for severity using visual field mean deviation (MD) with XFG eyes.13 Of these patients, patients who had undergone routine cataract and glaucoma filtering surgery by the same surgeon (APR) with a minimum of 2-year follow-up and 5 visual fields were included for the study. The major indications of trabeculectomy with or without cataract surgery were uncontrolled IOP on medications, visual field progression, or intolerance to medications.
All patients underwent routine slit-lamp examination and standard automated perimetry (24–2 SITA standard, Humphrey Field Analyzer, II, Carl Zeiss, Meditech, Inc) at the presentation. After the initial visit, they were reviewed every 3–6 months with regular IOP and fundus examination. The standard deviation (SD) of IOP during all visits before surgery was calculated to determine the IOP fluctuations from the electronic hospital database. The visual field testing was considered reliable if the fixation losses, false-positive, and false-negative responses were <20%. A glaucomatous VF was defined if a patient had a glaucoma hemifield test was outside the normal limits or if the pattern standard deviation was flagged at p<0.05 on at least 2 consecutive baseline VF tests. After excluding the first fields, visual field progression was determined using the rate of progression based on guided progression analysis (GPA) that defines significant consistent deterioration from a baseline pattern deviation at ≥3 of the same test points on three consecutive examinations. We also evaluated the rate of change in MD and analysed progression using fresh baseline visual fields obtained after surgery, which were then compared to subsequent fields.
We excluded cases with insufficient follow-ups, corneal opacities, retinal pathologies causing visual field abnormality at presentation (age related macular degeneration, diabetic retinopathy), inflammation or previous trauma, refractive errors > ± 6 D, coexisting uveitis, ischemic optic neuropathy, and eyes with neovascular glaucoma. Eyes with visual field progression eyes were excluded if the progression noted corresponded to the area of RVO rather than the area of glaucomatous damage. Since retinal vein occlusions (RVO) are common in XFS, we did not exclude those that developed them after surgery or on review visits, while excluding those eyes where RVO was present at baseline. Visual field progression was confirmed in eyes with RVO only if progression was noted away from the area of RVO (Example: inferior field progression in inferior quadrant RVO).
Data Analysis
Analyses were performed using STATA Inc (USA, version 11), with p<0.05 defined as statistically significance. The Student’s t-test and Fisher’s exact test were used for comparison of clinical/visual field parameters between types of glaucoma. The Kaplan–Meier analysis was used to analyse surgical and clinical outcomes in groups. Association of clinical parameters like age, gender, mean IOP, ocular associations, diagnosis, and IOP variations depicted by standard deviation (SD) between visits, with rate of progression was analysed using univariate and multivariate regression for variables that reached p<0.1 significance level in univariate analysis. We performed the multivariate regression separately for those that progressed </>−5dB/year to analysed independently to see specific factors explaining faster rates of progression.
Results
The preoperative characteristics of all patients (N=32 XFG, 33 POAG and 28 PACG) in the study according to glaucoma type are given in Table 1. The XFG eyes were older at the time of surgery, though clinically, the glaucoma severity was matched for XFG, POAG, and PACG eyes, Figure 1. The mean MD (p=0.1) at the time of surgery did not vary between groups, Table 1. The mean preoperative IOP was similar between groups, with a greater number of XFG eyes (36% versus 26% POAG and 12% PACG eyes) requiring >3 medications before surgery.
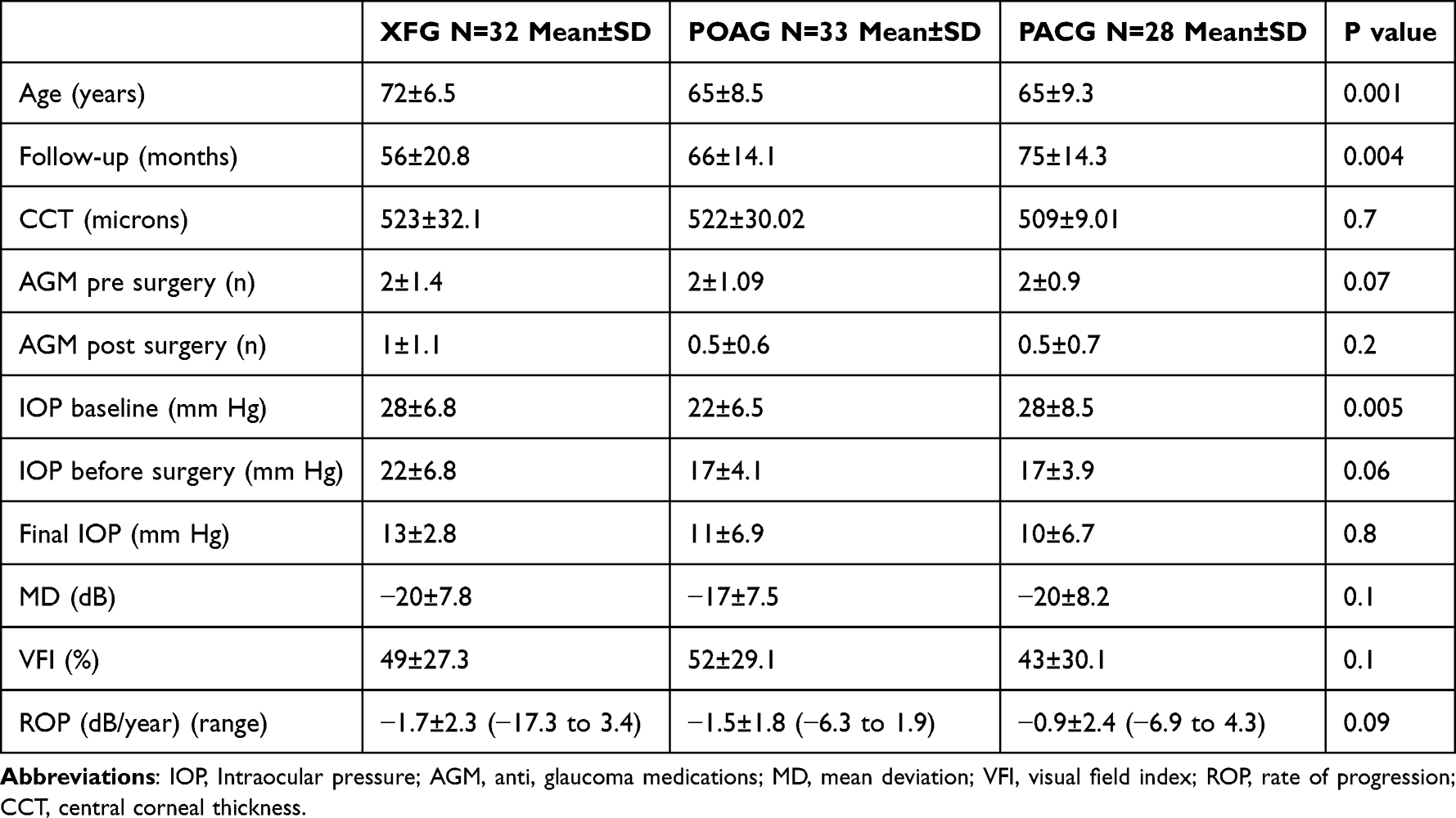 |
Table 1 Baseline Clinical Profile of Patients with Exfoliation and Primary Glaucoma That Underwent Glaucoma Surgery |
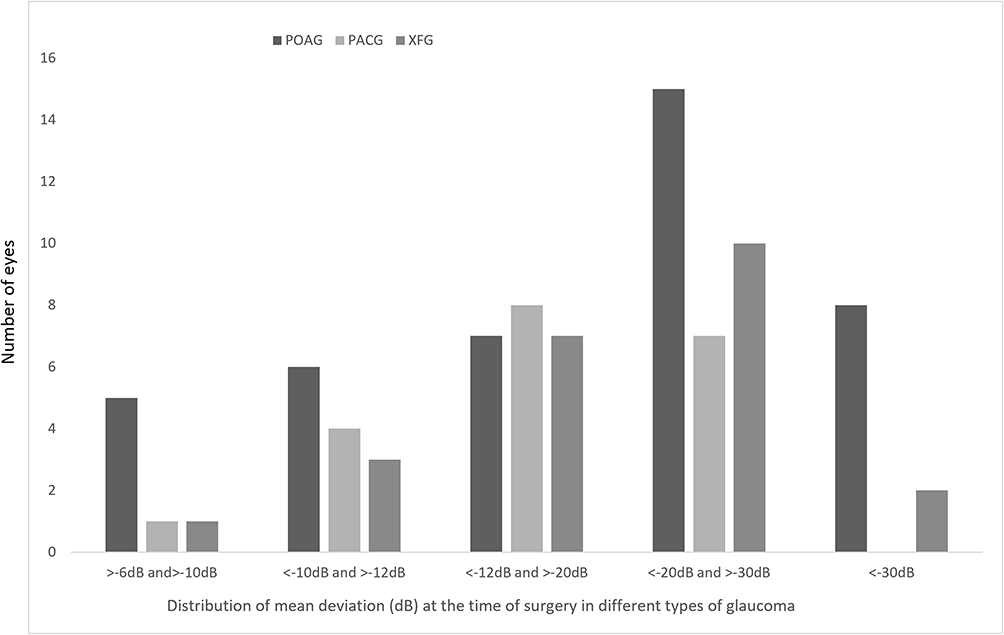 |
Figure 1 Distribution of visual field Mean deviation (MD) in eyes with exfoliation or primary glaucoma undergoing glaucoma filtering surgery-See text for details. |
The visual acuity improved by >2 lines in all the cases at 2 years, with 2 XFG eyes having diminished vision at 3 years post-surgery owing to retinal vascular occlusions. Two XFG patients and 3 POAG eyes underwent additional anti-VEGF injections for diabetic macular oedema (DME), with a rise in IOP mandating the addition of glaucoma drugs. Vitreous loss was noted intraoperatively in 2 XFG eye and 1 PACG eyes, both of which were managed with automated vitrectomy followed by intraocular lens (IOL) implantation in the sulcus (n=1) and bag (n=2). All three patients had transient inflammation in the anterior segment that resolved at 1 month after surgery, with 1 XFG eye requiring one AGM at the final follow-up. Complication rates were not significantly different between groups, Table 2.
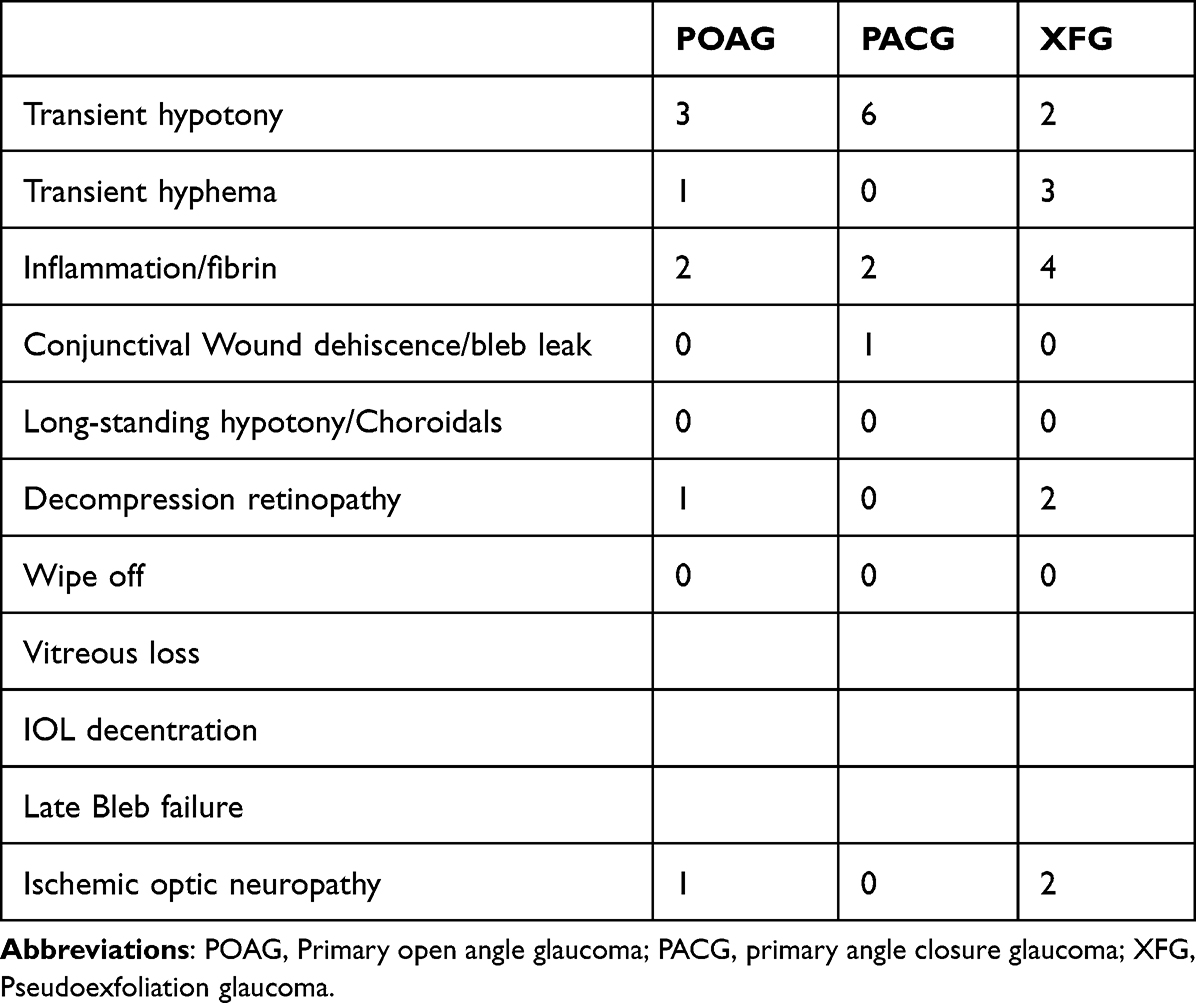 |
Table 2 Complication Rates of Combined Surgery in Pseudoexfoliation Glaucoma and Primary Glaucoma |
The IOP profile at the time of surgery, 1 year, and the last visit is depicted in Figure 2, showing no significant difference in final IOP between groups. All eyes achieved >30% reduction in IOP in all groups, with the mean IOP reduction rate (%) defined as the ratio of IOP reduction to the baseline IOP ((baseline IOP − follow-up IOP) / baseline IOP). All eyes with IOP fluctuations after surgery required medications for IOP control. The number of medications at final follow-up was similar between groups with a greater number of XFG eyes requiring ≥2 medicines for adequate IOP control after surgery.
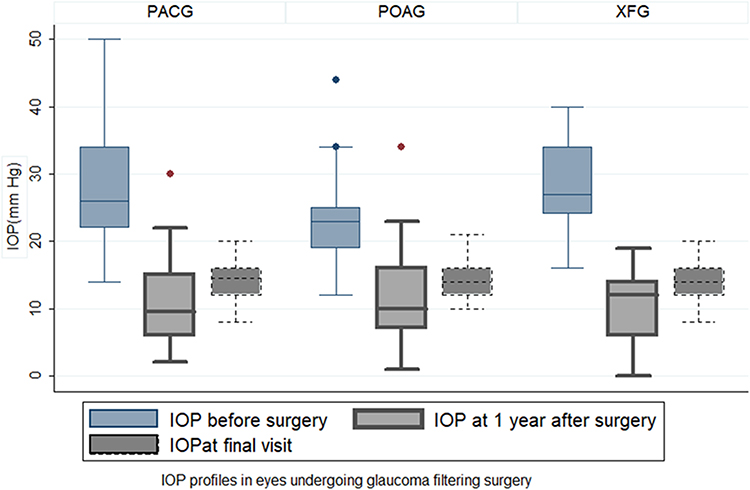 |
Figure 2 Intraocular pressure profiles before and after glaucoma filtering surgery in eyes with exfoliation or primary glaucoma. |
Seven eyes (2 XFG, 3 POAG, and 2 PACG eyes) showed a transient progression on visual fields which, however, was not reproduced on repeat examination. Visual field progression on GPA after surgery was noted in 48 of 93 eyes (n=11 XFG, 18 POAG, and 19 PACG eyes) at a mean follow-up of 10± 5.6 months after surgery. Disc haemorrhage was noted in 2 XFG eyes (at 25 and 31 months) and 1 POAG eye (at 7 months) after surgery. The XFG group had the maximum number of eyes (36%) showing ROP worse than −5dB/year compared to POAG (11.1%) and PACG (10.5%), p<0.01, Figure 3. The XFG eyes had a greater mean ROP (−5± 5.7, r=−17.3dB/yr to −1.3db/yr) than POAG (−2 ± 1.7db/yr, r=−6.3db/r to −1.2db/yr) or PACG eyes (−1.7±1.9db/yr, r=−6.8db/yr to −1.2db/yr), p=0.0001. The number of eyes with IOP fluctuations was greater in progressing POAG (50%) and XFG (45%) eyes (5.5%) than PACG eyes, Figure S1. The mean IOP fluctuation was more in progressing XFG eyes (5±5.8mm Hg) and POAG (5±8.3mm Hg) eyes than PACG (2±1.4mm Hg) eyes, p<0.0001, or eyes that were clinically stable, p<0.001.
 |
Figure 3 Rate of visual field progression (dB/year) in eyes undergoing glaucoma filtering surgery (>-5dB means a rate greater than −5db/year-see text for description). |
Of 48 eyes with progression, 18 eyes (6 XFG, 8 POAG, and 4 PACG) had RVO at follow-up after surgery needing additional interventions. Of 18 eyes with RVO, 12 eyes (5 XFG, 8 POAG and 1 PACG) had IOP fluctuations of >5mm Hg that mandated the addition of medications for IOP control. All eyes with IOP fluctuations were controlled medically and none required additional surgery for IOP control. The ROP of in these eyes with RVO (progression on visual field seen in quadrants away from RVO as specified earlier) and >5mm Hg IOP spikes was also greater in XFG (−12±5.59db/yr) and POAG (−6±1.3dB/yr) eyes than PACG eyes (−3±0.4dB/yr), p<0.0001.
On multivariate analysis, higher IOP fluctuations (SD) >5mm Hg and associated RVO were significant factors for visual progression (R2=53.5%), Table 3 and Figure 4. Analyzing the association between groups showed that this association held true for POAG and XFG eyes in eyes with VF progression. Age, gender, MD at surgery, and the number of medications before surgery or at final follow-up did not influence visual progression rates in either group.
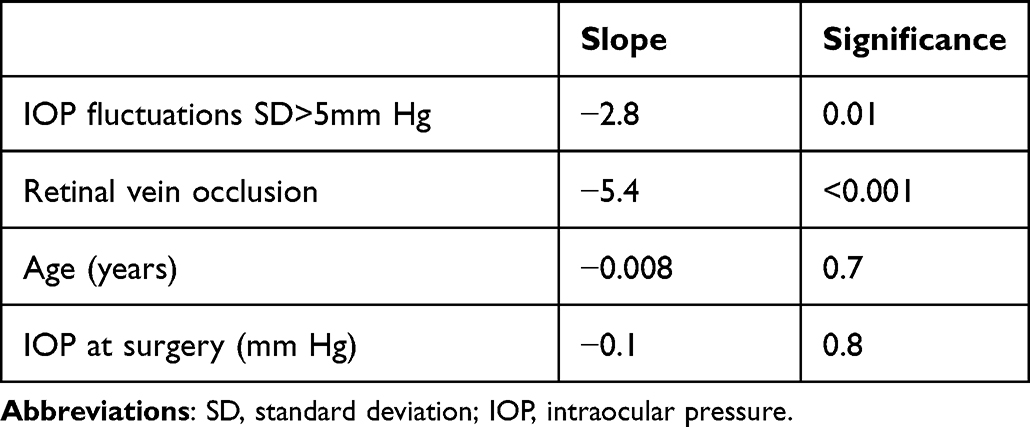 |
Table 3 Multivariate Regression of Factors Influencing Rate of Progression of Visual Field in Exfoliation Glaucoma and Primary Glaucoma |
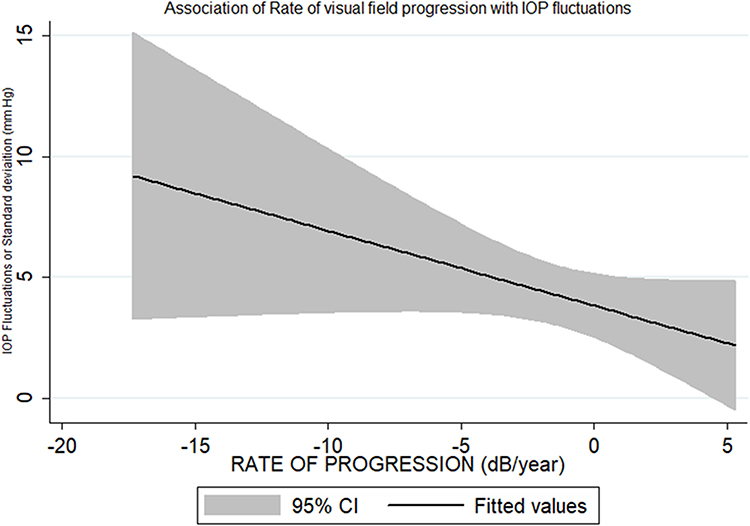 |
Figure 4 Multivariate linear regression of the IOP fluctuations (standard deviations of mm Hg). |
Discussion
This study found similar IOP after surgery in severity-matched XFG and POAG eyes, with XFG having a greater number of eyes (36%) showing an ROP worse than −5dB/yr, 45% of eyes showing an IOP spike and a higher mean IOP spike between visits. The ROP in eyes with RVO and >5mm Hg IOP spikes was greater in XFG than POAG or PACG. A higher IOP fluctuation >5mm Hg and associated RVO were the significant factors predicting visual field progression after surgery in POAG and XFG but not in PACG eyes. Age, gender, baseline MD, and the number of medications did not seem to influence visual progression rates in any group.
Exfoliation glaucoma has been recognized as a risk factor for visual field progression and visual impairment.2–5,9 It is known to progress faster than other forms of primary glaucoma, if untreated.4,6,10 Yet, the treated outcomes were no different between the groups in this study. This may be owing to the study being closer to clinical practice than most randomised clinical trials (RCT’s) that have strict inclusion/exclusion criteria or standardised treatment targets/outcomes. Exfoliation glaucoma is rarely included in clinical trials owing to the assumption that they behave differently compared to other types of primary glaucoma. The EMGT reported XFG as a risk factor associated with faster progression.6 This has been reported in other studies with XFG diagnosis being considered a risk factor for glaucoma progression.2,4,5,10 This may have been owing to missed diagnosis, delayed treatment, or ocular associations that were missed or not evaluated.7 The surgical outcomes in XFG are also reported to be worse owing to frequent complications, and association both intra and postoperatively.1,9,10,14–20 The eyes undergoing trabeculectomy have been reported to have faster rates of progression than the general glaucoma population, with one-third of these eyes predicted to become blind with those ROP if continued without surgical intervention.14,15 Previous studies have reported a rate of VF loss of −0.1–0.5dB/year in primary glaucoma after adequate treatment.14,16,17,19,20 Population demographics determining the ROP are demonstrated in high rates of VF loss in Swedish population with rate of 0.36dB/year.18 The EMGT trial demonstrated a median VF loss of <−0.5dB/year in untreated POAG eyes with early damage.6,20 It also reported that the presence of exfoliation increased the chances of progression by 200%. Though XFG is reported as a significant risk factor in univariate analysis, this does not hold true in multivariate analysis when other factors and IOP are included in the model in several studies.18,20 These inconsistencies in studies regarding the rate of progression and the higher rate of progression in eyes undergoing surgery reflect the different cohorts/types of glaucoma studied, higher severity in eyes undergoing surgery than those with early glaucoma, and the lack of reported IOP parameters, ocular/systemic associations like RVO as IOP independent factors, which do play an important role in determining the clinical course of any glaucoma as seen in this study. We believe, our results are therefore truer to the clinical scenarios and therefore offer a more pragmatic approach to the causes of VF progression in XFG compared to POAG or PACG. Such comparisons have not been made earlier in most studies, which have excluded eyes with RVO or excluded eyes with exfoliation when analysing VF progression versus IOP outcomes after surgery.6,14,18–20
RVO significantly influenced the ROP in XFG and POAG eyes in this study. Vascular factors are an important cause of visual field abnormalities in patients with glaucoma. Yet, this study included progression seen in quadrants away from the site of RVO removing potential bias of “progression” by RVO itself. RVO suggests an underlying vascular risk factor that is commonly known to be associated with glaucoma.21–23 One study has, however, identified exfoliation as an independent risk factor for RVO, with a higher incidence of ischemic RVO in these eyes. It is difficult to postulate if RVO suggests disturbed optic-nerve autoregulation in XFG, or POAG eyes, implying the need for aggressive treatment.24 Whether the RVO represents a cause or an effect of generalised vascular dysregulation is worth studying in XFG and POAG. Nevertheless, such associations would cause IOP fluctuations and rapid VF progression in multiple ways in both POAG and XFG, as seen in this study. This study suggests that such an underlying vascular factor may contribute to field progression after surgical IOP control in POAG and XFG eyes, though the mechanisms of such damage may only be presumed to be progressive ganglion cell damage by ischemia. It is difficult to estimate if any surgical intervention has indeed flattened the slope of progression owing to the variable time taken for stabilization after any IOP reduction. Nevertheless, associations like RVO reflect that IOP-independent mechanisms and IOP spikes >5mm Hg are significant causes for VF progression despite surgical IOP control in XFG and POAG.
Several ocular systemic associations have been reported in XFG eyes.1,2,7 These associations make it a unique form of glaucoma with its added risks and considerations. While the association of ischemic conditions like RVO is similar to that seen in NTG eyes, predominant IOP-dependent risk factors in XFG make it clinically similar to POAG eyes.1,21–23,25,26 Essentially, XFG eyes have a combination of vascular and IOP-dependant factors that make treatment of these eyes challenging.22,24,26,27 Surgical complications in this study were not significantly different between different groups. While it is known that XFG eyes are associated with higher rates of intraoperative and postoperative complications, these can be minimised to a large extent by evaluating cases by a single experienced surgeon, as in this study.
Studies have reported adequate short- and long-term IOP control with combined surgery in XFG and POAG eyes.9,14,20 Multiple IOP-related parameters have been reported to be associated with VF progression in many studies. While several parameters like higher baseline IOP, absolute IOP cut-offs, fluctuations (or SD), percentage reduction, and peak IOP have all been reported to be associated with VF progression, the SD of IOP between visits represents the true long-term control of IOP in glaucoma.6,18–20 This by far is clinically the most important factor for VF progression. This study also did not find any association of age or the number of medications with the rate of progression, which concurs with previous studies. This again highlights that though XFG eyes may be older at presentation or at the time of surgery, severity-matched XFG and POAG eyes behave similarly after IOP reduction by surgery. This is unlike other studies where this has been overlooked or excluded eyes with RVO, compared high-tension XFG eyes to NTG, or included a mixed cohort of those that did/did not undergo surgery.
Our study had several limitations. Though our cohort represented a more “life-like” scenario, we still had to exclude eyes with some ocular associations as detailed previously at baseline, some of which could be associations with XFG eyes as well. This may have caused a “selection bias” in this study. Those with insufficient follow-up were excluded, which could represent both clinical extremes of cases with best or worst outcomes as a cause for loss to follow-up. We only sought to identify eyes that underwent combined surgery to obviate bias due to the presence or development of cataracts on the visual field after glaucoma surgery alone. We also studied patients after adequate IOP control by surgery to allow for re-establishing a comparable baseline in both types of glaucoma despite differences in pathogenesis. This removes the bias/differences induced by the assumption of XFG eyes portending worse outcomes compared to primary glaucoma. Our study in effect reports XFG and POAG eyes with greater IOP spikes and RVO to have faster progression necessitating control of IOP-dependent and -independent mechanisms after surgery.
Acknowledgment
Hyderabad Eye Research Foundation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vesti E, Kivela T. Exfoliation syndrome and exfoliation glaucoma. Prog Retin Eye Res. 2000;19:345–368.
2. Konstas AG, Stewart WC, Stroman GA, et al. Clinical presentation and initial treatment patterns in patients with exfoliation glaucoma versus primary open angle glaucoma. Ophthalmic Surg Lasers. 1997;28:111–117. doi:10.3928/1542-8877-19970201-05
3. You QS, Xu L, Wang YX, et al. Pseudoexfoliation: normative data and associations: the Beijing eye study 2011. Ophthalmology. 2013;120:1551–1558. doi:10.1016/j.ophtha.2013.01.020
4. Heijl A, Buchholz P, Norrgren G, et al. Rates of visual field progression in clinical glaucoma care. Acta Ophthalmol. 2013;91:406–412. doi:10.1111/j.1755-3768.2012.02492.x
5. Kirwan JF, Hustler A, Bobat H, et al. Portsmouth visual field database: an audit of glaucoma progression. Eye. 2014;28:974–979. doi:10.1038/eye.2013.294
6. Leske MC, Heijl A, Hyman L, et al.; EMGT Group. Predictors of long-term progression in the early manifest glaucoma trial. Ophthalmology. 2007;114:1965–1972. doi:10.1016/j.ophtha.2007.03.016
7. Rao A, Raj N, Pradhan A, et al. Visual impairment in pseudoexfoliation from four tertiary centres in India. PLoS One. 2020;15(5):e0233268.
8. Henson DB, Shambhu S. Relative risk of progressive glaucomatous visual field loss in patients enrolled and not enrolled in a prospective longitudinal study. Arch Ophthalmol. 2006;124:1405–1408. doi:10.1001/archopht.124.10.1405
9. Ramyashri S, Rao A, Padhy D, et al. Small incision cataract surgery with trabeculectomy versus phacoemulsification trabeculectomy in pseudoexfoliation glaucoma. Indian J Ophthalmol. 2020;68:1090–1094.
10. Hollo G, Quaranta L, Cvenkel B, et al. Risk factors associated with progression in exfoliative glaucoma patients. Ophthalmic Res. 2012;47:208–213.
11. Ayala M. Risk factors for visual field progression in newly diagnosed exfoliation glaucoma patients in Sweden. Sci Rep. 2022;12:10763. doi:10.1038/s41598-022-14962-9
12. Ayala M. Comparison of visual field progression in new-diagnosed primary open-angle and exfoliation glaucoma patients in Sweden. BMC Ophthalmol. 2020;20:322. doi:10.1186/s12886-020-01592-w
13. Foster PJ, Buhrmann R, Quigley HA, et al. The definition and classification of glaucoma in prevalence surveys. Br J Ophthalmol. 2002;86:238–242. doi:10.1136/bjo.86.2.238
14. Bertrand V, Fieuws S, Stalmans I, Zeyen T. Rates of visual field loss before and after trabeculectomy. Acta Ophthalmol. 2014;92:116–120. doi:10.1111/aos.12073
15. Foulsham WS, Fu L, Tatham AJ. Prior rates of visual field loss and lifetime risk of blindness in glaucomatous patients undergoing trabeculectomy. Eye. 2015;29:1353–1359. doi:10.1038/eye.2015.156
16. Musch DC, Gillespie BW, Lichter PR, et al. CIGTS study investigators. Visual field progression in the collaborative initial glaucoma treatment study: the impact of treatment and other baseline factors. Ophthalmology. 2009;116:200–207. doi:10.1016/j.ophtha.2008.08.051
17. Chauhan BC, Mikelberg FS, Artes PH, et al. Canadian Glaucoma Study: 3. Impact of risk factors and intraocular pressure reduction on the rates of visual field change. Arch Ophthalmol. 2010;128:1249–1255.
18. De Moraes CG, Liebmann JM, Liebmann CA, et al. Visual field progression outcomes in glaucoma subtypes. Acta Ophthalmol. 2013;91:288–293.
19. Nouri-Mahdavi K, Hoffman D, Coleman AL, et al. Advanced glaucoma intervention study. predictive factors for glaucomatous visual field progression in the advanced glaucoma intervention study. Ophthalmology. 2004;111:1627–1635. doi:10.1016/j.ophtha.2004.02.017
20. Bengtsson B, Leske MC, Hyman L, et al.; Early Manifest Glaucoma Trial Group. Fluctuation of intraocular pressure and glaucoma progression in the early manifest glaucoma trial. Ophthalmology. 2007;114:205–209.
21. Cursiefen C, Hammer T, Kuchle M, et al. Pseudoexfoliation syndrome in eyes with ischemic central retinal vein occlusion. A histopathologic and electron microscopic study. Acta Ophthalmol Scand. 2001;79:476–478.
22. Mitchell P, Wang JJ, Smith W. Association of pseudoexfoliation syndrome with increased vascular risk. Am J Ophthalmol. 1997;124:685–687. doi:10.1016/S0002-9394(14)70908-0
23. David R, Zangwill L, Bardarna M, et al. Epidemiology of retinal vein occlusion and its association with glaucoma and increased intraocular pressure. Ophthalmologica. 1988;197:69–74. doi:10.1159/000309923
24. Burgoyne CF, Downs JC. Premise and prediction-how optic nerve head biomechanics underlies the susceptibility and clinical behavior of the aged optic nerve head. J Glaucoma. 2008;17:318–328. doi:10.1097/IJG.0b013e31815a343b
25. Andrikopoulos GK, Mela EK, Georgakopoulos CD, et al. Pseudoexfoliation syndrome prevalence in Greek patients with cataract and its association to glaucoma and coronary artery disease. Eye. 2009;23:442–447. doi:10.1038/sj.eye.6702992
26. Yüksel N, Karabaş VL, Arslan A, et al. Ocular hemodynamics in pseudoexfoliation syndrome and pseudoexfoliation glaucoma. Ophthalmology. 2001;108:1043–1049. doi:10.1016/S0161-6420(01)00572-3
27. Chakraborty M, Rao A. Alternate causes for pathogenesis of exfoliation glaucoma, a multifactorial elastotic disorder: a literature review. Curr Issues Mol Biol. 2022;44:1191–1202. doi:10.3390/cimb44030078
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.