Back to Journals » Clinical Optometry » Volume 17
Vision Performance of a 3-Zone Progressive™ Design Kalifilcon A Silicone Hydrogel Multifocal Contact Lens is Not Influenced by Pupil Size: Findings from a Multicenter Clinical Study
Authors Phatak NR ![]() , Reindel W, Rah MJ, Proskin H
, Reindel W, Rah MJ, Proskin H ![]() , Giedd K, Pucker AD
, Giedd K, Pucker AD
Received 10 January 2025
Accepted for publication 12 June 2025
Published 25 July 2025 Volume 2025:17 Pages 207—215
DOI https://doi.org/10.2147/OPTO.S513407
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Nitasha R Phatak,1 William Reindel,1 Marjorie J Rah,1 Howard Proskin,2 Kerry Giedd,3 Andrew D Pucker4
1Bausch + Lomb Incorporated, Rochester, NY, USA; 2Howard M. Proskin & Associates, Rochester, NY, USA; 3Eola Eyes, Orlando, FL, USA; 4Lexitas Pharma Services, Inc., Durham, NC, USA
Correspondence: Marjorie J Rah, Bausch + Lomb Incorporated, 1400 N. Goodman St, Rochester, NY, 14609, USA, Tel +1 585-413-6397, Email [email protected]
Purpose: Factors including age, refractive error, and luminance can affect pupil size and may influence the performance of multifocal contact lenses (MFCLs). This post-hoc analysis aimed to investigate correlations between pupil size and vision performance of a 3-Zone Progressive™ design, daily disposable silicone hydrogel (kalifilcon A) MFCL.
Methods: Habitual MFCL wearers aged ≥ 40 years were enrolled in a 3-week, single-arm, bilateral, open-label study to assess near, intermediate, and distant vision performance. Pupil sizes were recorded at dispensing, along with binocular high-contrast visual acuity (VA) by logMAR. VA was assessed at 1- and 3-weeks’ follow-up for distance, intermediate, and near vision, and participants rated vision performance using a 0– 100 scale (100=most favorable) at both these follow-ups. Responses with score ≥ 50 were considered favorable. Pearson correlation coefficient (r) was used to determine the correlation significance.
Results: Pupil size ranged from 2.0 mm to 7.0 mm. Mean logMAR VA was − 0.009, 0.046, and 0.114 (1 week), and − 0.012, 0.046, and 0.115 (3 weeks) for distance, intermediate, and near vision, respectively. Statistical analysis of the VA distribution found no significant correlation between VA and pupil size after 1 week of MFCL wear for distance or near vision (r2=0.003 and 0.006, respectively; both p≥ 0.05), and a weak but statistically significant correlation between intermediate VA and pupil size (r2=0.017; p< 0.05). No correlations were observed after 3 weeks for any distance (all p≥ 0.05). Participants rated subjective vision highly (84.0± 19.9, 89.2± 11.8, and 82.5± 18.5, respectively at 1 week, and 84.6± 18.0, 89.3± 12.6, and 84.2± 17.9, respectively at 3 weeks). Responses were favorable at both visits (p< 0.05). Correlations between vision rating and pupil size were not significant at either visit (p≥ 0.05).
Conclusion: The kalifilcon A daily disposable silicone hydrogel MFCL delivers stable VA and significantly favorable (p< 0.05) ratings at all distances for patients with a wide range of pupil sizes.
Keywords: presbyopia, visual acuity, progressive multifocal design, contact lens
Introduction
As adults face middle age, most contend with presbyopia, as a progressively less flexible crystalline lens leads to near vision refractive error.1 This phenomenon is readily corrected with a variety of eyeglass lens options, both for those who are new to vision correction and for habitual glasses wearers.2
For individuals who are habitual wearers of corrective contact lenses (CLs), there are several options. These include continuing with their single-vision CLs and using reading glasses for near vision tasks, initiating monovision CL wear (one CL in the dominant eye for distance vision and a second CL in the nondominant eye for near vision), initiating multifocal CL (MFCL) wear (either in both eyes or in one eye, with a monovision CL in the other), or converting to glasses with multifocal or progressive lenses and discontinuing CL wear altogether.3,4
MFCLs accounted for 15% of soft CL fits worldwide in 2023, with over half of these CLs fitted to presumed presbyopes.5 The total number of MFCL wearers is expected to increase annually based on factors including demographics, increased popularity of this CL type, and the emergence of MFCL-based myopia management in younger patients.6
Modern MFCL designs incorporate simultaneous image refraction in zones of the CL, and include aspheric CLs that project near images through the CL center and distant images through the periphery, concentric designs that utilize alternating concentric rings to project near and far images to the retina simultaneously, and combinations of the two.7
Pupil size is an important consideration in MFCL design, as pupil size not only changes rapidly and acutely with variations in luminance, but also changes slowly with age-associated increases in refractive error, and with age itself.7,8 These factors may be considered when designing CLs to attempt to account for pupil variation over the range of refractive error as well as with age.7,9 Conversely, other findings have reported no correlation between either objective or subjective vision performance, with either refractive error or pupil size while wearing center-near aspheric MFCLs; a further study concluded that neither age nor refractive error are relevant to their MFCL optic zone designs.10,11 These contradicting positions call into question which patient biometric parameters are critical to optimizing MFCL design to achieve optimal vision performance.
Novel computer eye models accounting for patient-specific aberrations, changes in pupil diameter, and amplitude of accommodation have enabled development of a unique center-near, 3-Zone Progressive™ design (kalifilcon A, Bausch + Lomb INFUSE® One-Day Multifocal Silicone Hydrogel Contact Lens, Bausch & Lomb Incorporated, Rochester, NY, USA).7,12–16 This study aimed to evaluate the objective and subjective vision of participants while wearing the kalifilcon A MFCL; the objective of this post-hoc analysis was to determine any correlation between objective and subjective vision and participant pupil size.
Material and Methods
This clinical investigation was conducted in accordance with Federal Codes and Directives.17,18 The protocol was developed in alignment with the International Organization for Standardization (Geneva, Switzerland),19 appropriate medical device regulation,20 the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) Harmonised Guideline for Good Clinical Practice,21 the Declaration of Helsinki, and applicable local regulations.
A total of 20 investigative sites in the United States participated in this 3-week, single-arm, bilateral, open-label study, for which results have already been posted to ClinicalTrials.gov.22 The study protocol and amendments, informed consent form, and other study materials were reviewed and approved by a central institutional review board (Sterling IRB, Atlanta, GA, USA).
Participant Selection
At the screening/dispensing visit, all eligible enrolled participants provided informed consent and completed the Health Insurance Portability Accountability Act-compliant release form. Eligibility was confirmed before performing any study-specific procedures.
Eligible participants were presbyopic, at least 40 years of age, and adapted, habitual wearers of soft MFCLs, who agreed to wear dispensed study CLs on a daily disposable basis for approximately 3 weeks, and attend in-office follow-up visits at 1 and 3 weeks. The 3-week time period accounted for patients adapting, or starting to adapt, to the MFCLs, based on a typical initial adaptation period of about 2 weeks,23,24 and is reflective of real-world scheduling practice for patient follow-ups to assess patient progress and comfort, and daily wear experience.23 Full inclusion and exclusion criteria are in Supplementary Table 1.
Study Contact Lens
Participants were fitted with kalifilcon A MFCLs using the manufacturer-recommended fitting guide. CLs were dispensed and worn on a daily disposable basis for approximately 3 weeks. The test CL is summarized as follows: sphere power: −6.00 D to +3.00 D, in steps of 0.25 D; ADD: low and high; diameter: 14.2 mm; base curve: 8.6 mm. Each CL came packaged in a phosphate-buffered saline solution containing poloxamer 181, poloxamine 1107, glycerin, and erythritol to support ocular surface homeostasis.25
Study Assessments
Investigators measured binocular high-contrast logarithm of the minimum angle of resolution visual acuity (logMAR VA) for distance, intermediate, and near vision. Distance measurements were taken using Precision Vision (Woodstock, IL, USA), 90% high contrast, logMAR chart with Sloan letters (CAT. NO. 2103–2), and the Precision Vision Small Illuminator Cabinet (CAT. NO. 914). This chart is designed for use at 6.5 feet (2 meters) and was positioned in front of the participant at approximately eye level. Intermediate measurements were taken using the corresponding chart (CAT. NO. 2105, designed for use at 65 cm). Near measurements were taken using the corresponding chart (CAT. NO. 2107, designed for use at 40 cm). Additionally, investigators measured participant pupil size without CLs at the screening/dispensing visit.
At the 1- and 3-week follow-up visits, participants rated distance vision, intermediate vision, and near vision attributes of study CL performance, by eye, on scales of 0 (least favorable) to 100 (most favorable). The focus of this post-hoc analysis was to evaluate for any relationship between objective vision, as measured by logMAR VA, and pupil size, and subjective vision (numerical rating of test participants) and pupil size. Pupil size was assessed by each investigator, as per their routine practice.
Safety was recorded throughout the study and summarized by relationship to study CL, and included adverse events, symptoms/complaints, slit lamp examination, best spectacle-corrected VA, spherocylindrical refraction, and keratometry.
Statistical Analysis
The target number of participants was 300 to allow for ≤10% losses and achieve exact binomial test 93% power (nominal 5% one-sided significance level).
All analyses were reported on per-participant data. For variables originally reported on individual eyes, per-participant scores were obtained by taking the mean value across the reported scores on both eyes. These variables included: subjective performance ratings for near, intermediate, and distance vision; subjective overall vision performance rating; and pupil size. Per-participant performance ratings were categorized as favorable if the score was ≥50 and unfavorable if the score was <50.
Reported summaries of performance ratings at each visit included the mean and standard deviation of the ratings, the number and percentage of favorable responses, and the p-value from a two-sided binomial test comparing the percentage of favorable responses to 50%. Summaries of the binocular high-contrast logMAR VA scores at each visit included the number of participants, mean, standard deviation, and minimum and maximum values.
For the logMAR VA assessments and subjective overall vision performance ratings at each visit, the relationship with baseline pupil size was investigated through the calculation of Pearson correlation coefficients. The p-value from a two-sided z test performed to compare each correlation to zero was reported. All statistical hypothesis tests were two-sided and employed an α=0.05 level of significance.
Results
In total, 301 adapted MFCL wearers were enrolled in the study. Study CLs were dispensed to 294 eligible participants, 291 participants completed the first follow-up visit, and 290 participants completed both follow-up visits. Demographics of the study participants are presented in Table 1.
 |
Table 1 Demographics of Participants (n=294) |
Pupil size was measured for both eyes of each participant and ranged from 2.0 mm to 7.0 mm across all eyes. No significant correlation between average pupil size and participant age was observed (p=0.86).
Measured binocular logMAR VA while wearing the study CL appears in Figure 1. All data obtained from eligible participants were considered, which resulted in 294 observations at screening/dispensing, 291 at 1-week follow-up, and 290 at 3-week follow-up. The mean change from screening was larger for distance VA (mean ± SD: 0.008±0.0628 and 0.006±0.0678 increase at 1 week and 3 weeks, respectively) than for intermediate or near VA.
 |
Figure 1 Binocular High-Contrast logMAR Visual Acuity. n=294 at screening/dispensing visit; n=291 at 1-week follow-up; n=290 at 3-week follow-up. Abbreviation: logMAR, logarithm of the minimum angle of resolution. |
Subjective vision performance ratings for distance, intermediate, and near vision are shown in Figure 2. Ratings at each visit were consistent, with mean ratings at 1 week for distance, intermediate, and near vision of 84.0±19.9, 89.2±11.8, and 82.5±18.5, respectively, and 84.6±18.0, 89.3±12.6, 84.2±17.9, respectively, at 3 weeks (Figure 2A).
 |
Figure 2 (A) Kalifilcon A MFCL Subjective Vision Performance Rating. (B) Kalifilcon A Subjective Vision Performance Rating Favorability (Fraction of Responses ≥50/Favorable). Ratings were significantly favorable at all distances (p<0.05). Abbreviations: SD, standard deviation; MFCL, multifocal contact lens. |
Overall, responses were significantly favorable at distance, intermediate, and near vision, with mean ratings of 92.4%, 99.0%, and 92.8%, respectively, after 1 week of MFCL wear and 94.0%, 98.6%, and 95.7%, respectively, after 3 weeks (Figure 2B; all p<0.05).
Correlations between logMAR VA and pupil size are shown in Figure 3, and between subjective vision performance rating and pupil size in Figure 4. Statistical testing of the logMAR VA distribution found weak but statistically significant correlations between intermediate VA and pupil size at screening/dispensing (r2=0.02; p=0.01) and 1-week follow-up (r2=0.017; p=0.02). No significant correlation was found between any distance VA, or vision performance rating, and pupil size at either follow-up visit (all p≥0.05).
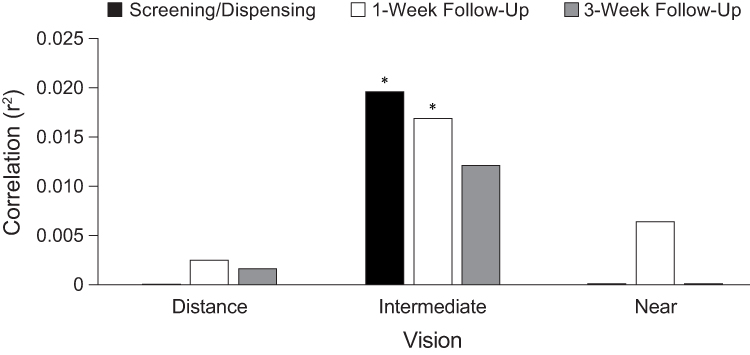 |
Figure 3 Pearson Correlations Between logMAR Visual Acuity and Pupil Size. *Indicates significant but weak correlation (p<0.05; r2=0.01–0.02). Abbreviation: logMAR, logarithm of the minimum angle of resolution. |
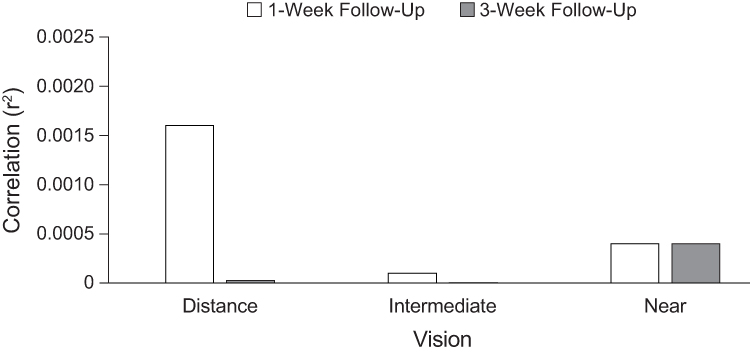 |
Figure 4 Pearson Correlations Between Subjective Vision Performance Rating and Pupil Size. No significant correlations (all p≥0.05). |
The single adverse event that was observed in the study was determined device related (vital dye staining of the cornea ≤2, present in both eyes). The event resolved without intervention, and the participant completed the study.
Discussion
This study aimed to evaluate the objective and subjective vision performance of a center-near, 3-Zone Progressive kalificon A MFCL, and the objective of this post-hoc analysis was to determine any correlation with wearer pupil size. The findings presented here indicate favorable and consistent near, intermediate, and distance vision, and that pupil size did not correlate with measured or subjective vision performance of this MFCL. There were no clinically meaningful correlations between near, intermediate, or distance logMAR VA and pupil size, or between subjective near, intermediate, or distance vision performance and pupil size. While some weak statistical correlations for intermediate logMAR VA were significant at the screening/dispensing or 1-week visit, none were significant at the 3-week visit. The weak correlation related to intermediate logMAR VA was also not reflected in intermediate subjective vision performance. The 3-week time period in this study allows for initial adaptation and is reflective of real-world practice to assess patient progress and comfort with their MFCLs, as well as their wear experience in their day-to-day lives.23,24
The results of the present study were similar to those reported for 84 presbyopes refitted with one of three MFCLs of different materials (lotrafilcon B, nelfilcon A, and delefilcon A).10 Those participants had a slightly wider pupil size range than in the present study (2.0–8.0 mm vs 2.0–7.0 mm in our study), and, similar to the results presented here, no significant correlations were observed between visual quality or VA and pupil size for distance, intermediate, or near vision.10 Based on these findings, and in agreement with ours, the authors concluded that pupil size was not significantly related to subjective vision performance.10 Another study reported only small differences in MFCL center-near ADD power and through-focus performance with different pupil sizes, and concluded that pupil size plays a secondary role in MFCL performance.26
The lack of correlation between pupil size at any distance after 3 weeks of CL wear in this study might indicate participants starting to adapt to the study CL. In addition, the lack of clinically significant correlations between both logMAR VA and subjective vision rating may reflect the relatively small decrease in pupil diameter caused by aging, versus other factors, and the small variation in pupil size among presbyopes. Indeed, while luminance can significantly affect pupil diameter (increased diameter with decreased luminance), data indicate that decreased diameter caused by wearer age is significant only when comparing pre-presbyopes with presbyopes.8 This is consistent with the lack of significant correlation between pupil size and participant age in our study (p≥0.05).
The results presented here should be considered in the context of the limitations intrinsic to a post-hoc analysis of a single-arm, bilateral, open-label study. The lack of a standardized protocol guiding pupil size assessment is an additional consideration and reflects the real-world nature of the assessments. The unique nature of the 3-Zone Progressive design of the kalifilcon A MFCL prevents a like-for-like comparison with other lens designs, but the relatively large sample size and consistent values across the assessed outcomes add weight to the findings presented here. Future areas of investigation could also include subanalyses of results for myopes and hyperopes, findings according to pupil size ranges, area and shape, and any impact of the length of daily wear of the MFCL. In addition, a longer study duration may support analysis of the stability of the performance of the kalifilcon A MFCL over time, and indicate the impact of any further adaptation of wearers to the CL.
The 3-Zone Progressive design of the kalifilcon A MFCL tested in this study was developed using computer-based eye models built from ocular biometry data, including pupil size, higher-order aberrations, residual accommodation, corneal topography and diameter, anterior chamber depth, axial chamber length, and subjective refractions across nine distances.27 Accurate prediction of MFCL logMAR VA using these models allowed in silico evaluation of multiple designs,16 and the final optimum design that performed well across a range of pupil sizes was identified after thousands of iterations.27 The 3-Zone Progressive design of the kalifilcon A MFCL also benefits from only two ADD powers across the power range for this MFCL (low: +0.75D to +1.50D, and high: +1.75D to +2.50D) to enable simplified fitting,12,14,27 an attribute enhanced by the findings presented here, which show patient pupil size does not affect the vision performance of this lens.
Together with these most recent findings, available data demonstrate that the kalifilcon A MFCL delivers presbyopes high-performance near, intermediate, and distance vision, along with the benefits of the lens material and packaging solution reported previously, including high levels of comfort and an improved wearing experience, regardless of pupil size.25,28,29
Conclusion
Overall, the kalifilcon A MFCL 3-Zone Progressive design delivered favorable outcomes for distance, intermediate, and near vision for patients with a wide range of pupil sizes and was well-tolerated by participants in this study. There was no correlation between pupil size and subjective near and distance vision performance associated with wear of the kalifilcon A MFCL, and the statistically significant correlations between pupil size and intermediate logMAR VA were not reflected in subjective vision performance. These findings indicate that this MFCL design is an option for a broad range of patients requiring multifocal correction, and it offers a simplified MFCL fitting procedure for eyecare professionals.
Data Sharing Statement
All relevant data are within the manuscript. Clarification requests around the manuscript and its data can be made to the corresponding author.
Ethics/Ethical Approval
This clinical investigation was conducted in accordance with Code of Federal Regulations (CFR) Title 21, Parts 11, 50, 54, 56, and 812,17 and with CFR Title 42, Part 11 – Clinical Trials Registration and Results Information Submission.18 The protocol was developed with consideration of International Organization for Standardization (Geneva, Switzerland) 14155-1:2020,19 European Parliament Medical Device Regulation 2017/745,20 ICH Harmonised Guideline for Good Clinical Practice E6(R3),21 the Declaration of Helsinki, and applicable local regulations. All eligible enrolled participants provided informed consent by completing an IRB-approved informed consent form.
Acknowledgments
Medical writing/editorial support was provided by Joseph Chinn (J Chinn LLC, Lafayette, CO, USA) and Vicky Reynolds (Illuminate Medical, UK), and was funded by the study sponsor. The abstract of this paper was presented at the 2024 Global Specialty Lens Symposium (GSLS), held January 17–30, 2024, Las Vegas, NV, USA.
Funding
This work was funded by Bausch & Lomb Incorporated.
Disclosure
Howard Proskin and Kerry Giedd are paid consultants for Bausch & Lomb Incorporated. Andrew D. Pucker is a paid consultant for Bausch & Lomb Incorporated, and also reports personal fees from HanAll Biopharma, grants from Alcon, and that he was an employee of Lexitas Pharma Services at the time this work was performed. Nitasha Phatak, William Reindel, and Marjorie Rah are employees of Bausch & Lomb Incorporated. The authors report no other conflicts of interest in this work.
References
1. Rich W, Reilly MA. A review of lens biomechanical contributions to presbyopia. Curr Eye Res. 2023;48(2):182–194. doi:10.1080/02713683.2022.2088797
2. Singh PT, Zeppieri M, Tripathy K. Presbyopia. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-.Available from: https://www.ncbi.nlm.nih.gov/books/NBK560568/.
3. Molina-Martin A, Pinero DP, Martinez-Plaza E, Rodriguez-Vallejo M, Fernandez J. Efficacy of presbyopia-correcting contact lenses: a systematic review. Eye Contact Lens. 2023;49(8):319–328. doi:10.1097/ICL.0000000000001013
4. Toshida H, Takahashi K, Sado K, Kanai A, Murakami A. Bifocal contact lenses: history, types, characteristics, and actual state and problems. Clin Ophthalmol. 2008;2(4):869–877. doi:10.2147/OPTH.S3176
5. Nichols JJ, Fisher D. Contact lenses 2023. Cont Lens Spectrum. 2024;39(1):14-16,18–19.
6. Walline JJ, Lindsley KB, Vedula SS, et al. Interventions to slow progression of myopia in children. Cochrane Database Syst Rev. 2020;1(1):CD004916. doi:10.1002/14651858.CD004916.pub4
7. Remon L, Perez-Merino P, Macedo-de-Araujo RJ, Amorim-de-Sousa AI, Gonzalez-Meijome JM. Bifocal and multifocal contact lenses for presbyopia and myopia control. J Ophthalmol. 2020;2020:8067657. doi:10.1155/2020/8067657
8. Guillon M, Dumbleton K, Theodoratos P, Gobbe M, Wooley CB, Moody K. The effects of age, refractive status, and luminance on pupil size. Optom Vis Sci. 2016;93(9):1093–1100. doi:10.1097/OPX.0000000000000893
9. Johnson & Johnson Vision Care. ACUVUE® pupil optimized design. Available from: https://www.jnjvisionpro.com/education-center/pupil-optimized-design.
10. Baker K, Merchea M.
11. Mathew J, Merchea M. Pupil size independence with multifocal contact lenses: fact or fiction? White paper. Available from: https://us.alconscience.com/sites/g/files/rbvwei1736/files/pdf/1905A202B-US-AOHM-19-E-0651a_Multifocal-Pupil-Size-White-Paper_Pitcher.pdf.
12. Bausch + Lomb INFUSE® ONE-DAY contact lens parameters. Available from: https://ecp.bauschcontactlenses.com/siteassets/pdf/infuse-oneday-contact-lens-parameters.pdf.
13. Bausch + Lomb INFUSE® ONE-DAY Multifocal. Available from: https://ecp.bauschcontactlenses.com/products/infuse-one-day/multifocal/.
14. Bausch + Lomb INFUSE® ONE-DAY packaging insert. Available from: https://ecp.bauschcontactlenses.com/globalassets/pdf/packageinserts/vision-care/lenses/bausch-lomb-infuse-package-insert-fitting-guide.pdf.
15. US Food and Drug Administration. FDA 510(k) summary K220613. Bausch + Lomb (kalifilcon A) Soft (hydrophilic) Contact Lens, Bausch + Lomb. (kalifilcon A) Soft (hydrophilic) contact lens for astigmatism, Bausch + Lomb. (kalifilcon A) Soft (hydrophilic) contact lens for presbyopia. 2023. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf22/K220613.pdf.
16. Kingston A, Cox I. Predicting through-focus visual acuity with the eye’s natural aberrations. Optom Vis Sci. 2013;90(10):1111–1118. doi:10.1097/OPX.0000000000000031
17. Code of Federal Regulations. Title 21, food and drugs (last amended June 13, 2025). Available from: https://www.ecfr.gov/current/title-21.
18. Code of Federal Regulations. Title 42, public health. Part 11—clinical trials registration and results information submission (last amended June 3, 2025). Available from: https://www.ecfr.gov/current/title-42/chapter-I/subchapter-A/part-11.
19. International Organization for Standardization. ISO 14155:2020: Clinical investigation of medical devices for human subjects–Good clinical practice. Available from: https://www.iso.org/standard/71690.html.
20. European Parliament. Regulation (EU) 2017/745 of the European Parliament and of the Council of 5 April 2017 on medical devices, amending Directive 2001/83/EC, Regulation (EC) No 178/2002 and Regulation (EC) No 1223/2009 and repealing council directives 90/385/EEC and 93/42/EEC. 2017. Available from: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32017R0745.
21. International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. ICH Harmonized Guideline Good Clinical Practice (GCP) E6(R3). 2025. Available from: https://database.ich.org/sites/default/files/ICH_E6%28R3%29_Step4_FinalGuideline_2025_0106.pdf.
22. Bausch & Lomb Incorporated (Rochester NY). Evaluation of product performance of a new silicone hydrogel multifocal contact lens. Available from: https://clinicaltrials.gov/study/NCT05660577.
23. Lazon de la Jara P, Sulley A, Pepe P, Walsh K, Guillon M. Multifocal contact lens success predictability. Contact Lens Anterior Eye. 2024;47(2):102105. doi:10.1016/j.clae.2023.102105
24. Fernandes PR, Neves HI, Lopes-Ferreira DP, Jorge JM, Gonzalez-Meijome JM. Adaptation to multifocal and monovision contact lens correction. Optom Vis Sci. 2013;90(3):228–235. doi:10.1097/OPX.0b013e318282951b
25. Reindel W, Steffen R, Mosehauer G, et al. Performance of a silicone hydrogel daily disposable contact lens among wearers with lens-related dryness. Open Ophthalmol J. 2023;17:e187436412303021. doi:10.2174/18743641-v17-230316-2022-57
26. Vedhakrishnan S, Vinas M, Benedi-Garcia C, Casado P, Marcos S. Visual performance with multifocal lenses in young adults and presbyopes. PLoS One. 2022;17(3):e0263659. doi:10.1371/journal.pone.0263659
27. Bausch + Lomb Proven 3-Zone Progressive™ Design. Available from: https://ecp.bauschcontactlenses.com/lens-technologies/multifocal-technology/.
28. Rah M, Schafer J, Reindel W, Steffen R. Presbyopic patient assessment of a new daily disposable silicone hydrogel multifocal contact lens. Presented at the American Academy of Optometry. New Orleans, LA. October 11-14, 2023. Available from: https://aaopt.org/past-meeting-abstract-archives/?SortBy=&ArticleType=&ArticleYear=&Title=&Abstract=&Authors=&Affiliation=&PROGRAMNUMBER=235114.
29. Reindel W, Rah M, Proskin HM. Impact of pupil size on vision performance of a new multifocal daily disposable contact lens. Invest Ophthalmol Visual Sci. 2024;65(7):2689.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.