Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Visceral Fat Area, Not Subcutaneous Fat Area, is Associated with Cardiac Hemodynamics in Type 2 Diabetes
Authors Qiu Y ![]() , Deng X
, Deng X ![]() , Sha Y
, Sha Y ![]() , Wu X, Zhang P, Chen K, Zhao Z, Wei W, Yang L, Yuan G, Zhao L, Wang D
, Wu X, Zhang P, Chen K, Zhao Z, Wei W, Yang L, Yuan G, Zhao L, Wang D
Received 29 September 2020
Accepted for publication 30 October 2020
Published 17 November 2020 Volume 2020:13 Pages 4413—4422
DOI https://doi.org/10.2147/DMSO.S284420
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Yue Qiu, Xia Deng, Yujing Sha, Xunan Wu, Panpan Zhang, Ke Chen, Zhicong Zhao, Weiping Wei, Ling Yang, Guoyue Yuan, Li Zhao, Dong Wang
Department of Endocrinology, Affiliated Hospital of Jiangsu University, Zhenjiang, Jiangsu 212001, People’s Republic of China
Correspondence: Dong Wang; Li Zhao
Department of Endocrinology, Affiliated Hospital of Jiangsu University, 438 Jiefang Road, Zhenjiang, Jiangsu 212001, People’s Republic of China
Tel +86-13605282460
; +86-15800578209
Email [email protected]; [email protected]
Background: This study was conducted in patients with type 2 diabetes mellitus (T2DM) to assess the association between visceral fat area (VFA) and cardiac hemodynamics.
Methods: A total of 568 patients with type 2 diabetes (mean age 54± 12 years; 40.8% of women) were enrolled. Visceral fat area (VFA, m2) and subcutaneous fat area (SFA, m2) were evaluated by a bioelectrical impedance analyzer. Cardiac hemodynamics were measured by echocardiography, and other clinical and laboratory variables were also assessed and recorded. Patients were divided into those with VFA ≤ 100 (n=369) and those with VFA > 100 (n=199).
Results: VFA, SFA, LVMI (left ventricular mass index), left atrial diameter, left ventricular diastolic diameter (LvDd), interventricular septal thickness (IVST), left ventricular systolic diameter (LvSd), and posterior wall thickness (PWT) levels in high-V groups were significantly higher than those in low-V groups. Correlation analysis showed that VFA was positively correlated with LVMI (r=0.120, p=0.004), LVM (r=0.249, p< 0.0001), left atrial diameter (r=0.375, p< 0.0001), aortic root diameter (r=0.243, p< 0.0001), left ventricular systolic diameter (LvSd) (r=0.211, p< 0.0001) and negatively correlated with LVEF (r=− 0.107, p=0.011). In multivariate linear regression analysis, VFA was the strongest independent determinant of LVMI (β=0.04, p=0.016), LVEF (β=− 0.01, p=0.023), and left atrial diameter (β=0.035, p< 0.0001), Internal diameter of the aortic root (β=0.014, p< 0.0001) and LvSd (β=0.017, p< 0.0001). In addition, the VFA also better predicted cardiovascular disease risk with AUC of 0.609 (95% CI:0.563– 0.656), compared with SFA, waist–hip ratio (WHR), in a statistically significant manner.
Conclusion: We found a significant correlation between VFA (but not SFA) and cardiac hemodynamic parameters. The VFA has advantages as a predictor of visceral obesity and is significantly associated with the development of cardiovascular risk factors (CVD) in T2DM patients.
Keywords: cardiac hemodynamics, left ventricular mass index, type 2 diabetes mellitus, visceral fat area
Introduction
Nowadays, diabetes mellitus is seriously increasing in the majority of the populations all over the world. The latest epidemiological data on diabetes show the prevalence of diabetes in adults living in China increased from 0.67% using the WHO criteria in 1980 to 12.8% using the ADA criteria in 2017.1 It has become a major public health problem in developing countries and is associated with the development and progression of high-mortality diseases such as obesity and its subsequent complications. Cardiovascular disease (CVD) is the most common cause of morbidity and mortality in patients with diabetes.2 However, the mechanistic link between diabetes mellitus and CVD is still debated. Besides traditional risk factors including centripetal obesity, insulin resistance and hypertension, novel risk factors such as chronic inflammation, lipid metabolism disorder, atherosclerosis and myocardial steatosis have also been speculated to contribute to the development of abnormal function and structure for CVD in T2DM.3–7
Recently, visceral fat has gained attention as one of the possible mechanisms for the link. Visceral fat, mainly found in the abdominal cavity, acts as an extremely active organ that produces several bioactive adipokines and proinflammatory cytokines.8,9 Excessive visceral fat area is associated with adipocyte dysfunction, increased inflammatory cytokine secretion, and impaired insulin sensitivity, which can increase the risk of atherosclerosis and lead to cardiac and endothelial dysfunction.10 A few studies reported visceral fat was associated with cardiometabolic risk in the general population,11,12 in hypertensive patients,13 in psoriasis patients,14 in women after menopause15 and in patients with coronary atherosclerosis.16 However, the relationship between VFA and cardiac hemodynamics has not been adequately evaluated in comparison with other clinical factors such as blood pressure, age or waist/hip ratio in T2DM.
At present, the detection of visceral fat mainly includes CT, magnetic resonance imaging (MRI) and dual bioelectrical impedance.17 Although CT and MRI are the gold standard for quantitative estimation of adipose tissue distribution, these technologies are costly, have radiation issues, and cannot be routinely available. As a non-invasive and relatively accurate method of quantifying visceral fat, dual bioelectrical impedance has other advantages, such as operator independency, and lower costs, when compared to CT and MRI.18,19 It can be widely used in clinic with a high sensitivity and specificity (0.941 and 0.988, respectively).20 Besides, recent studies have found that dual bioelectrical impedance analysis can accurately measure the body’s various tissue components, including visceral fat and muscle.21
Hence, this study intends to measure VFA by dual bioelectrical impedance and investigate its relationship with cardiac hemodynamics in patients with type 2 diabetes.
Methods
Study Design and Patients
A total of 568 consecutive asymptomatic patients with T2DM, who were admitted to our institution (Affiliated Hospital of Jiangsu University, China) for diabetic educational program between June 2019 and February 2020, were enrolled in this study. The diagnosis of T2DM was performed according to the 1999 World Health Organization (WHO) diabetes diagnosis and classification criteria.22 43.1% of patients had a previous diagnosis of type 2 diabetes mellitus and hypertension and were in treatment for both conditions. These criteria were chosen to ensure the formation of a high cardiovascular risk cohort. The following conditions should be excluded for all included patients: (1) patients with incomplete clinical and biochemical data; (2) recent use of glucocorticoids or antipsychotics; (3) Patients with type 1 diabetes, special type diabetes and acute severe metabolic disorder of diabetes; (4) patients with coronary atherosclerotic heart disease, congestive heart failure, severe arrhythmia, post-cardiac valve replacement and cardiac pacemaker; (5) Patients with severe liver and kidney dysfunction and abnormal thyroid function; (6) Patients with tumors, autoimmune diseases or diseases of the blood system. This study was approved by the medical ethics committee of the Affiliated Hospital of Jiangsu University in Zhenjiang, China and obtained written informed consent of all subjects.
Physical Examination
All study subjects were examined in the morning after an overnight fast. Height, body weight, waist circumference (WC), hip circumference (HC), heart rate and blood pressure (BP) were measured by trained survey personnel according to standardized methods.
Laboratory Measurement
The participants were asked to collect elbow venous blood after an overnight fast of longer than 8 h. Fasting blood glucose (FBG) was detected by glucose oxidase method, fasting plasma insulin (FIns) and C-peptide (FC-P) were measured by chemiluminescence method, and HbA1c was determined by HPLC. An automatic biochemical analyzer was used to detect aspartate aminotransferase (AST), alanine transaminase (ALT), glutamyl transpeptidase (GT), TC, TG, HDL-C and LDL-C.
Measurement of VFA and Cardiac Hemodynamic Parameters
VFA, along with SFA, was measured at the umbilical level by a dual bioelectrical impedance (DUALSCAN; Omron Healthcare Co. Ltd, Kyoto, Japan). LVEF was calculated by the Teichholz formula. Left atrial diameter, left ventricular end diastolic, LvDd and LvSd were measured using 2-dimensional echocardiography, according to the guidelines of the American Society of Echocardiography.23 Left ventricular posterior wall thickness (PWT) and interventricular septal thickness (IVST) were measured at end-diastole.
Data Measurements
The homeostasis model assessment ratio (HOMA-R) index was calculated as fasting plasma glucose × fasting plasma insulin∕22.5 for assessing insulin resistance.24 Body mass index (BMI) was calculated from height and weight and the waist–hip ratio (WHR) was calculated from the waist and hip circumference.
LVMI was calculated by this formula:23
LV mass = 0.80 × 1.04 × {(IVST + LvDd + PWT)3 −LvDd3+ 0.6 (g)
LVMI = LV mass∕body surface area (body weight0.425 × height0.725 × 0.007184).
Statistical Analysis
All statistical analyses were performed using SPSS version 26.0 (SPSS Inc, Chicago, IL, USA). Data are expressed as mean ± standard deviation (SD) and percentages. Participants were divided into two groups according to the diagnostic criteria of abdominal obesity as follows: Q1 low-VFA (VFA≤100 cm2), Q2 high-VFA (VFA>100 cm2). The relationship between variables was assessed using Pearson or Spearman correlation analysis. Linear regression analyses on cardiac functional parameters were performed to identify clinical and laboratory variables that were associated with cardiac functional parameters. The factors related at the p < 0.05 level were selected as independent variables for multivariable analysis. The receiver operating characteristic (ROC) curves were generated to identify the optimal value for the prediction of the risk of cardiovascular disease in this population. Optimal cutoffs were derived from maximizing the Yoden index. All tests of significance were 2-tailed, and p < 0.05 was considered statistically significant.
Results
A total of patients with type 2 diabetes (mean age 54 ± 12 years; 40.8% female) were enrolled in the present study. Patients were 54.0 ± 12.0 years-old, systolic and diastolic blood pressure were 127.8 ± 17.6 mmHg and 74.9 ± 10.2 mmHg, and HbA1C was 9.5 ± 2.2%. Among 568 patients, 369 and 199 were classified as low-V and high-V patients. As shown in Table 1, high-V group was significantly younger, has significantly higher LVM and LVMI, higher prevalence of hypertension and hyperlipidemia, and lower LVEF than the low-V group. HbA1c, fasting C-peptide and HOMA-IR level in high-V group were significantly higher than in those with low-V. VFA, SFA, WHR, BMI, TG, LDL-C levels in high-V group were significantly higher than those in low-V group. LVMI, LVM, Left atrial diameter, aortic root diameter, LvDd, LvSd, IVST, PWT were increased, along with the increase of the VFA (p<0.05).
 |
Table 1 Clinical Characteristics According to VFA Levels |
In Table 2, VFA was positively correlated with LVMI (r=0.120, p=0.004), LVM (r=0.249, p<0.0001), left atrial diameter (r=0.375, p<0.0001), aortic root diameter (r=0.243, p<0.0001), LvSd (r=0.211, p<0.0001), LvDd (r=0.185, p<0.0001), IVST (r=0.240, p<0.0001), PWT (r=0.237, p<0.0001) while negatively correlated with LVEF (r=−0.107, p=0.011). Among the clinical factors in Table 3, we determined which factors were associated with the cardiac hemodynamics. Besides VFA, these cardiac hemodynamics were mainly correlated with the prevalence of hypertension, SFA, WHR, Cr and SBP (p<0.05). Left atrial diameter, Internal diameter of aortic root and LvSd were also correlated with Fasting c-peptide, DBP (p<0.05). The LVMI had a significant correlation with VFA (r=0.120, p=0.004), SFA (r=0.132, p=0.02), heart rate (r=−0.106, p=0.011), SBP (r=0.181, p<0.0001), BMI (r=0.156, p<0.0001), TC (r=−0.099, p=0.018), HDL-C (r=−0.084, p=0.046) and WHR (r=0.092, p=0.028).
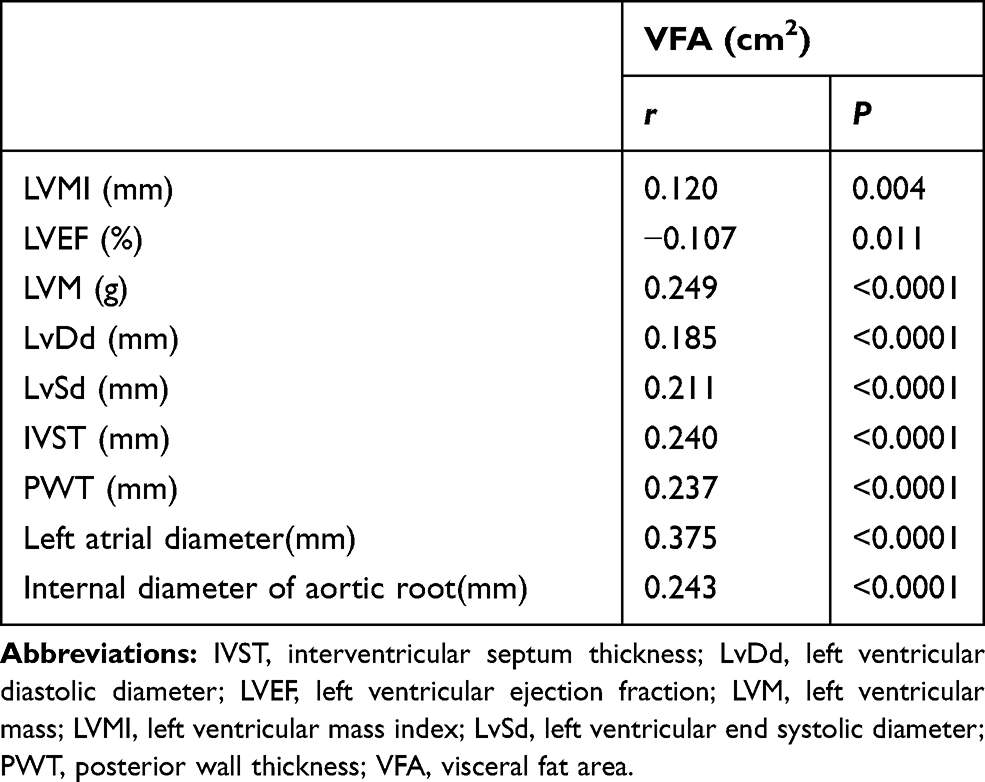 |
Table 2 Correlation Between VFA and Cardiac Hemodynamics |
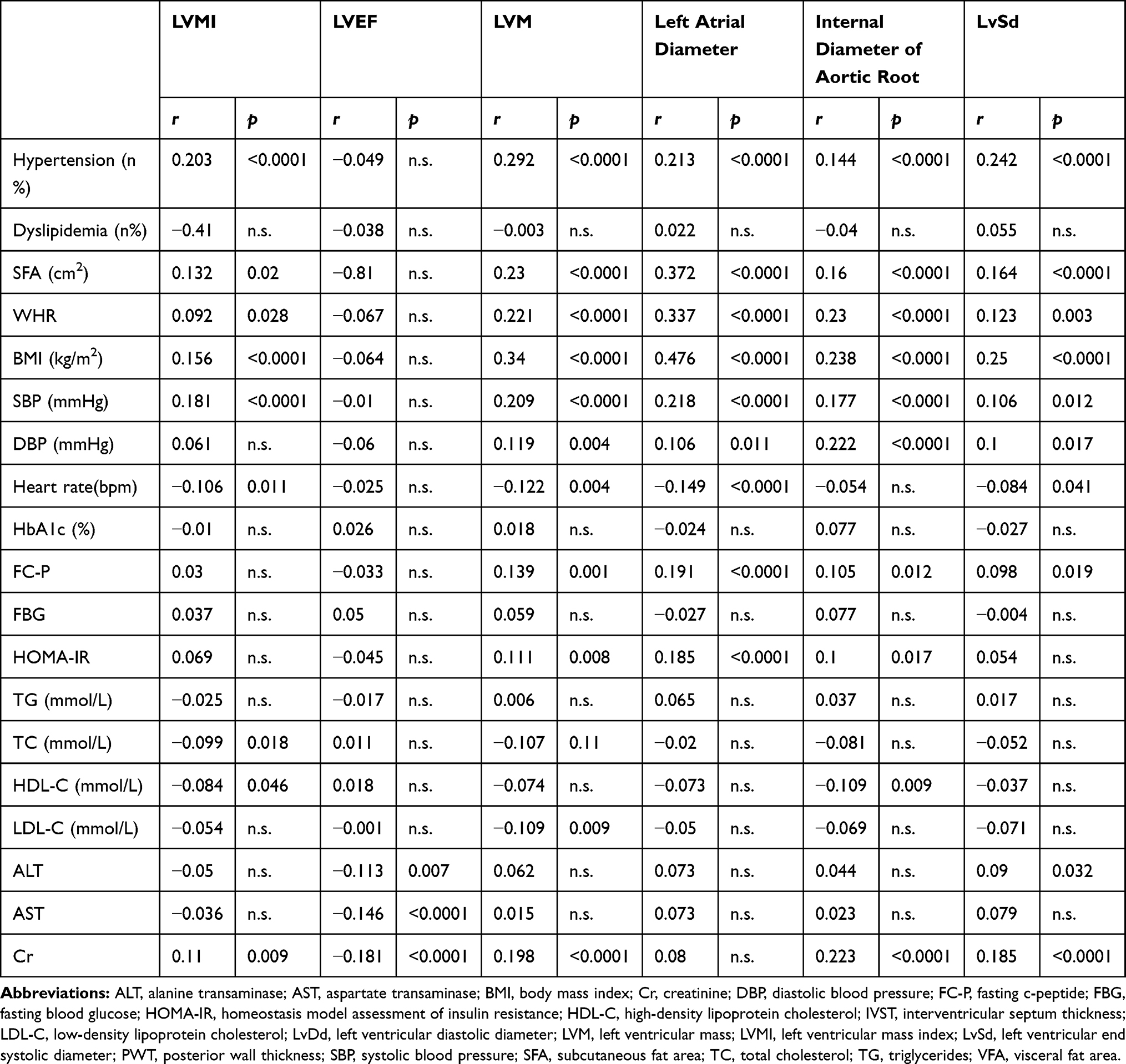 |
Table 3 Pearson’s Correlation Between Cardiac Hemodynamics and Clinical Data |
Multivariate linear regression analysis (Table 4) found that with LVMI as the dependent variable, VFA and LVMI were independently correlated after adjusting for gender and age (p=0.016). After further correction of TC, HDL-C and LDL-C, VFA and LVMI still showed an independent correlation (p=0.044). After HbA1c correction, the correlation between VFA and LVMI remained independent (p=0.039). These cardiac hemodynamic parameters were also taken as dependent variables, respectively. Furthermore, VFA was also an independent determinant of these cardiac hemodynamic parameters (p<0.05), after correction according to the above model. This indicates that excessive VFA is independently associated with cardiac dysfunction in patients with type 2 diabetes.
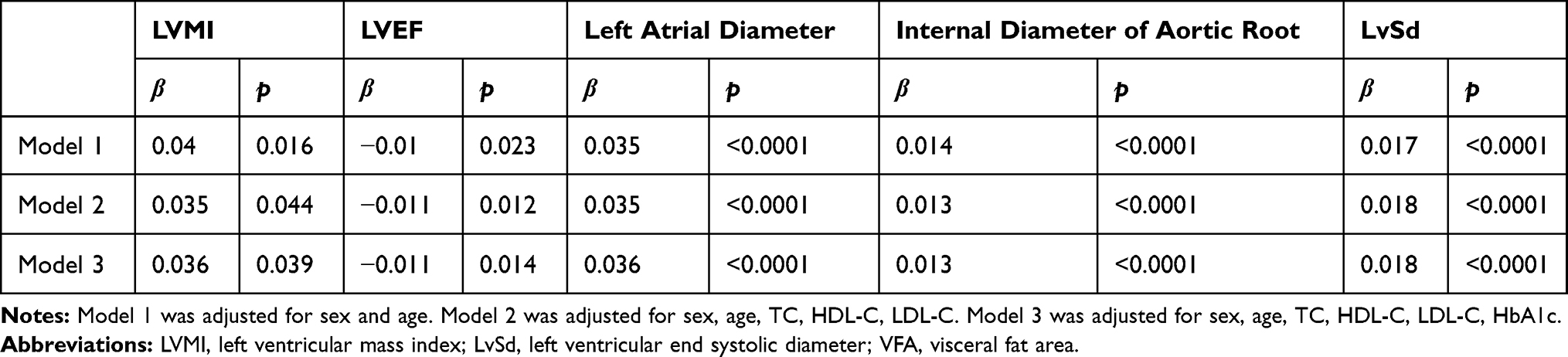 |
Table 4 Multivariate Linear Regression Analysis Between Cardiac Hemodynamics and VFA |
We further performed an analysis of the association of clinical characteristics and the risk of cardiovascular disease (Table 5). According to the prevalence of hypertension, the patients were divided into the hypertensive group and the non-hypertensive group. Compared with the non-hypertensive group, the levels of VFA, SFA, WHR, HOMA-IR in the hypertensive group were significantly increased (p<0.05 or p<0.01). Compared with patients without hypertension, all cardiac hemodynamic parameters were noticeably increased in patients with hypertension (p<0.001), except for LVEF.
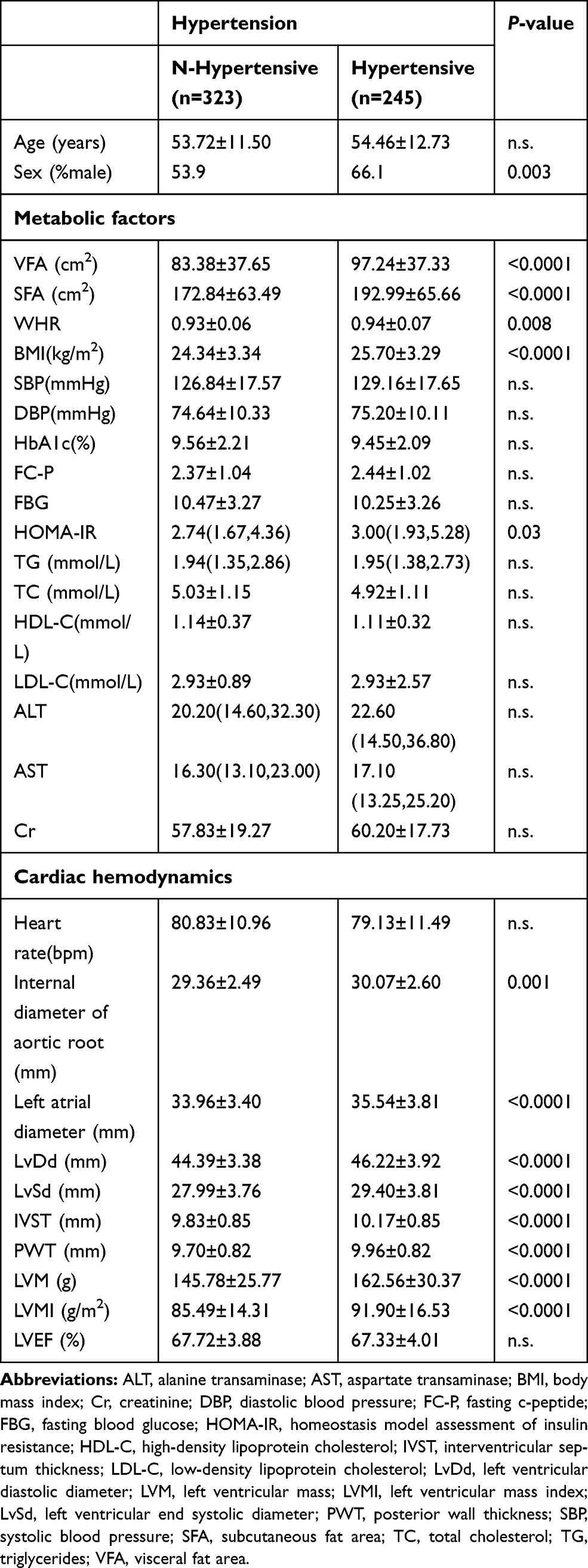 |
Table 5 Clinical Characteristics According to the Prevalence of Hypertension |
Figure 1 shows the performance for predicting the end-point among the markers for cardiovascular disease risk. The AUC of the markers were as follows: VFA 0.61 (95% CI: 0.56–0.66), SFA 0.60 (95% CI: 0.55–0.64) and WHR 0.57 (95% CI: 0.52–0.62). The results showed that the area under ROC curve predicted by VFA was larger than that of SFA and WHR, and the difference was considered statistically significant (p<0.01). When the VFA was 89.6 cm2, the maximum Youden index was 0.174, so 89.6 was the best cut-off value, with a sensitivity of 58% and a specificity of 59.4% (Table 6).
 |
Table 6 ROC Curve Analysis of VFA in Predicting Cardiovascular Disease Risk |
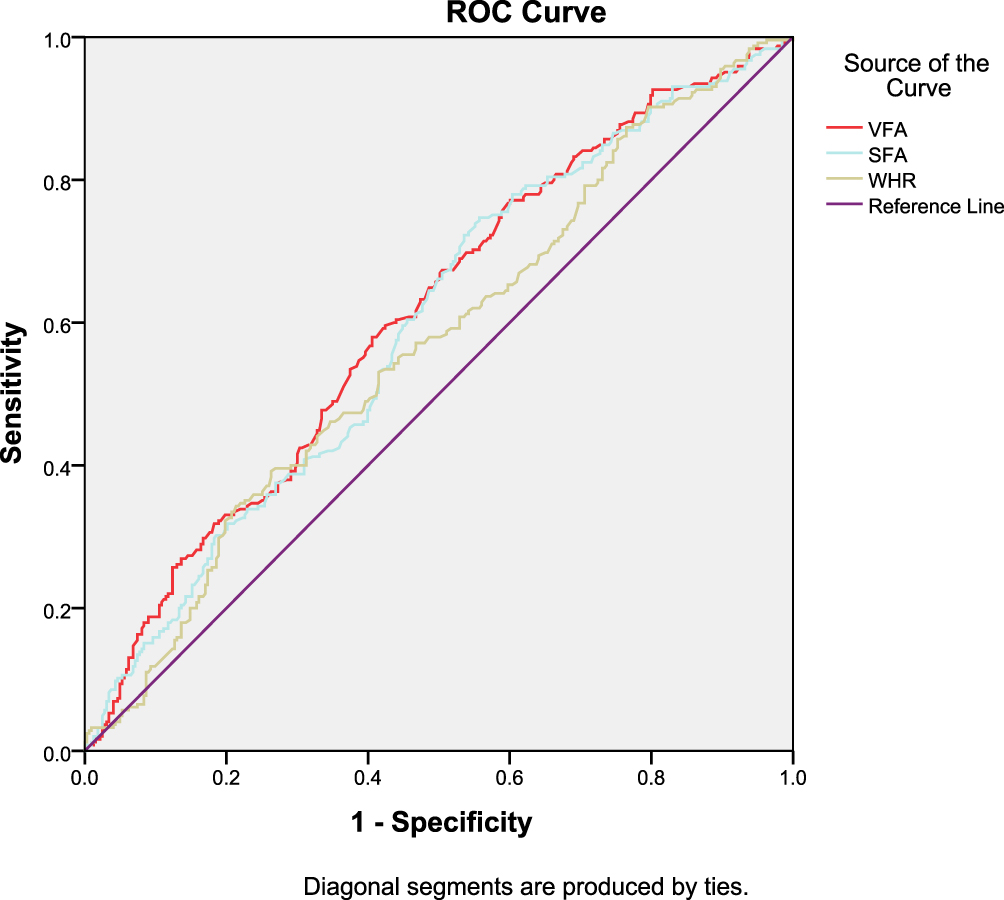 |
Figure 1 ROC curve analysis of VFA, SFA and WHR prediction of cardiovascular disease risk. Red, VFA; blue, SFA; brown, WHR. |
Discussion
Obesity is a major risk factor for type 2 diabetes. Long-term and persistent obesity significantly increases the incidence of diabetes, compared to the general population.1 What is more, people with abdominal obesity have a much greater risk of diabetes than those with buttock obesity.25 After the occurrence of diabetes, the glucose and lipid metabolism of the human body is further disturbed, resulting in the increase of blood glucose, blood lipid and fat redistribution, which will to a certain extent aggravate the degree of obesity. Thus, obesity and diabetes form a vicious circle of mutual cause and effect. The risk of cardiovascular disease is increased in diabetics, who account for 65% of all deaths in diabetics.26 Compared with non-diabetics, T2DM patients have earlier onset, more severe and more extensive cardiovascular disease. The risk of cardiovascular disease in diabetic patients is related to obesity, dyslipidemia, abnormal distribution of fat, IR, etc.27
VFA is a commonly used index to evaluate abdominal obesity. Visceral fat, as an important functional organ, is important for cardiometabolic complications. Visceral adipose tissue secretes many bioactive adipocytokines, such as leptin, adiponectin, leptin, tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), IL-8, and MCP-1.8 These adipocytokines are thought to contribute to changes in heart structure and function.28–30 This study was grouped according to the classification criteria of abdominal obesity, and the analysis showed that SFA, LVMI, LVEF, left atrial diameter, LvDd, IVST, LvSd, PWT levels in high-V groups were higher than those in low-V groups. These findings are similar to those studied in the general population study.11 For further study, with multiple linear regression analysis of LVMI as a dependent variable, the correlation between VFA and LVMI was significant (p<0.05). After adjusting for many factors, the correlation remained. Furthermore, VFA was also an independent determinant of LVEF, left atrial diameter, Internal diameter of aortic root, LvSd (p<0.05), after correction according to the above model. The ROC curve also shows that the predictive value of VFA for cardiovascular disease risk is 0.609. Thus, we had observed a significant association between visceral fat and cardiac hemodynamic parameters in all participants.
As obesity, hypertension is also a common cardiovascular risk factor with high prevalence in the world.31,32 Chronic hypertension causes endothelial dysfunction and inflammation, accelerates lipid deposition, and leads to the occurrence and progression of atherosclerosis and ventricular hypertrophy.3,33 In this study, 43% of patients had hypertension. Patients were divided into two groups according to the prevalence of hypertension. The level of cardiac hemodynamic parameters was generally higher in patients with hypertension than in those without hypertension, the difference between the groups was statistically significant (P≤0.001). Patients in the hypertension group had higher VFA than SFA, and both levels were higher than those in the non-hypertension group, consistent with previous studies.34,35 Although the activation of renin-angiotensin system in diabetic patients is itself associated with oxidative damage and increased apoptotic necrosis of myocardial cells in diabetic heart, the dysfunction of adipose tissue is caused by visceral fat accumulation also produces angiotensin, thus inducing systemic hypertension.36 The pathogenesis of obesity and hypertension is complex and sometimes interdependent. The main role, other than endothelium and adipokines, is attributed to the genetic, to the environmental factors, to the sympathetic nervous system, to renal and adrenal function, and to the insulin resistance.37
WHR is also a common indicator of abdominal obesity. WHR was more efficient than WC and BMI to identify cardiometabolic risk factors in non-obese Chinese.31 On this basis, we found that VFA has a better predictive value than SFA and WHR. In line with other findings,38,39 our data showed that HbA1c, HOMA-IR, fasting C-peptide and Hb in the High-VFA group were higher than those in the Low-VFA group. Sogabe40 suggested that there was a correlation between VFA and liver enzyme spectrum, inconsistent with the results of this study. Nevertheless, data resulting from human studies are conflicting, these inconsistencies most likely result from variations in studied subjects: genetic background, sex and age, sample size and assay methods used.
Several limitations of the present study should be considered. First, our study population is only limited to primarily Han Chinese, the conclusions drawn from the data are not generally representative. Second, due to the cross-sectional nature of the study, we cannot draw a causal relationship between VFA and cardiac hemodynamics. Further longitudinal follow-up studies are needed to verify if visceral fat could be a therapeutic target for preventing the progression of CVD in T2DM.
Conclusion
The above results together confirm that excess visceral fat was significantly correlated with cardiac hemodynamic parameters and hypertension in T2DM. The VFA has advantages as a predictor of visceral obesity and is significantly associated with the development of CVD in T2DM.
Compliance with Ethical Standards
The study was approved by the Biomedical Research Ethics Committee of the Affiliated Hospital of Jiangsu University, Zhenjiang, China, and performed in accordance with the Declaration of Helsinki. All participants had informed consent to the purpose of the study.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was supported in part by grants from the National Natural Science Foundation of China (81870548, 81570721, 82000809), the Social Development Project of Jiangsu Province (BE2018692), the Natural Science Foundation of Jiangsu Province, China (BK20191222), the Fifth “169 project” Scientific Research Project of Zhenjiang City, Jiangsu Province, and the Social Development Project of Zhenjiang City(SH2019041), Jiangsu Province. The Scientific Research Projects of Jiangsu Health and Family Planning Commission (Y2018109).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ. 2020;369:m997. doi:10.1136/bmj.m997
2. Association AD, Association AD. 1. Improving Care and Promoting Health in Populations: standards of Medical Care in 2020. Diabetes Care. 2020;43(Suppl Supplement 1):S7–s13. doi:10.2337/dc20-S001
3. Petrie JR, Guzik TJ, Touyz RM, Petrie JR, Guzik TJ, Touyz RM. Diabetes, Hypertension, and. Cardiovascular Disease: clinical Insights and Vascular Mechanisms. Can J Cardiol. 2018;34(5):575–584. doi:10.1016/j.cjca.2017.12.005
4. Domingueti CP, Dusse LMS, Carvalho MDG, de Sousa LP, Gomes KB, Fernandes AP. Diabetes mellitus: the linkage between oxidative stress, inflammation, hypercoagulability and vascular complications. J Diabetes Complications. 2016;30(4):738–745. doi:10.1016/j.jdiacomp.2015.12.018
5. Kaneto H, Katakami N, Matsuhisa M, Matsuoka T-A. Matsuoka T-a. Role of reactive oxygen species in the progression of type 2 diabetes and atherosclerosis. Mediators Inflamm. 2010;2010:453892. doi:10.1155/2010/453892
6. DeFronzo RA. Insulin resistance: a multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidaemia and atherosclerosis. Neth J Med. 1997;50(5):191–197. doi:10.1016/s0300-2977(97)00012-0
7. Janochova K, Haluzik M, Buzga M. Visceral fat and insulin resistance - what we know? Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2019;163(1):19–27. doi:10.5507/bp.2018.062
8. Jensen MD. Visceral Fat. Endocrinol Metab Clin North Am. 2020;49(2):229–237. doi:10.1016/j.ecl.2020.02.002
9. Tsao Y-C, Lee -Y-Y, Chen J-Y, et al. Gender- and Age-Specific Associations Between Body Fat Composition and C-Reactive Protein with Lung Function: A Cross-Sectional Study. Sci Rep. 2019;9(1):384. doi:10.1038/s41598-018-36860-9
10. Csige I, Ujvárosy D, Szabó Z, et al. The Impact of Obesity on the Cardiovascular System. J Diabetes Res. 2018;2018:3407306. doi:10.1155/2018/3407306
11. Sawada N, Daimon M, Kawata T, et al. The Significance of the Effect of Visceral Adiposity on Left Ventricular Diastolic Function in the General Population. Sci Rep. 2019;9(1):4435. doi:10.1038/s41598-018-37137-x
12. Rawshani A, Rawshani A, Franzén S, et al. Mortality and Cardiovascular Disease in Type 1 and Type 2 Diabetes. New Engl J Med. 2017;376(15):1407–1418. doi:10.1056/NEJMoa1608664
13. Haberka M, Stolarz-Skrzypek K, Biedroń M, et al. Obesity, Visceral Fat, and Hypertension-Related Complications. Metab Syndr Relat Disord. 2018;16(10):521–529. doi:10.1089/met.2018.0062
14. Goolam Mahyoodeen N, Crowther NJ, Pillay L, et al. Relationship of Visceral Fat and Adipokines with Cardiometabolic Diseases in Psoriasis. Acta Derm Venereol. 2019;99(13):1218–1223. doi:10.2340/00015555-3327
15. Soto Rodríguez A, García Soidán JL, Arias Gómez MJ, Leirós Rodríguez R, Del Álamo Alonso A, Pérez Fernández MR. Metabolic syndrome and visceral fat in women with cardiovascular risk factor. Nutr Hosp. 2017;34(4):863–868. doi:10.20960/nh.1085
16. Sato F, Maeda N, Yamada T, et al. Association of Epicardial, Visceral, and Subcutaneous Fat With Cardiometabolic Diseases. Circ J. 2018;82(2):502–508. doi:10.1253/circj.CJ-17-0820
17. Dai Z-J, Wang X-J, Kang A-J, et al. Association between APE1 Single Nucleotide Polymorphism (rs1760944) and Cancer Risk: a Meta-Analysis Based on 6419 Cancer Cases and 6781 Case-free Controls. J Cancer. 2014;5(3):253–259. doi:10.7150/jca.8085
18. Omura-Ohata Y, Son C, Makino H, et al. Efficacy of visceral fat estimation by dual bioelectrical impedance analysis in detecting cardiovascular risk factors in patients with type 2 diabetes. Cardiovasc Diabetol. 2019;18(1):137. doi:10.1186/s12933-019-0941-y
19. Yamakage H, Ito R, Tochiya M, et al. The utility of dual bioelectrical impedance analysis in detecting intra-abdominal fat area in obese patients during weight reduction therapy in comparison with waist circumference and abdominal CT. Endocr J. 2014;61(8):807–819. doi:10.1507/endocrj.ej14-0092
20. Nagai M, Komiya H, Mori Y, Ohta T, Kasahara Y, Ikeda Y. Estimating visceral fat area by multifrequency bioelectrical impedance. Diabetes Care. 2010;33(5):1077–1079. doi:10.2337/dc09-1099
21. Mattar M-AM, Zekri A-RN, Hussein N, Morsy H, Esmat G, Amin MA. Polymorphisms of base-excision repair genes and the hepatocarcinogenesis. Gene. 2018;675:62–68. doi:10.1016/j.gene.2018.06.056
22. Lorenzo C, Haffner SM. Performance characteristics of the new definition of diabetes: the insulin resistance atherosclerosis study. Diabetes Care. 2010;33(2):335–337. doi:10.2337/dc09-1357
23. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1–39 e14. doi:10.1016/j.echo.2014.10.003
24. Kumashiro N, Erion DM, Zhang D, et al. Cellular mechanism of insulin resistance in nonalcoholic fatty liver disease. Proc Natl Acad Sci U S A. 2011;108(39):16381–16385. doi:10.1073/pnas.1113359108
25. Kim S, Cho B, Lee H, et al. Distribution of abdominal visceral and subcutaneous adipose tissue and metabolic syndrome in a Korean population. Diabetes Care. 2011;34(2):504–506. doi:10.2337/dc10-1364
26. Arakawa M, Mita T, Azuma K, et al. Inhibition of monocyte adhesion to endothelial cells and attenuation of atherosclerotic lesion by a glucagon-like peptide-1 receptor agonist, exendin-4. Diabetes. 2010;59(4):1030–1037. doi:10.2337/db09-1694
27. Halter JB, Musi N, McFarland Horne F, et al. Diabetes and cardiovascular disease in older adults: current status and future directions. Diabetes. 2014;63(8):2578–2589. doi:10.2337/db14-0020
28. Laurikka A, Vuolteenaho K, Toikkanen V, et al. Adipocytokine resistin correlates with oxidative stress and myocardial injury in patients undergoing cardiac surgery. Eur J Cardiothorac Surg. 2014;46(4):729–736. doi:10.1093/ejcts/ezt634
29. Shimabukuro M, Hirata Y, Tabata M, et al. Epicardial adipose tissue volume and adipocytokine imbalance are strongly linked to human coronary atherosclerosis. Arterioscler Thromb Vasc Biol. 2013;33(5):1077–1084. doi:10.1161/atvbaha.112.300829
30. Malavazos AE, Ermetici F, Coman C, Corsi MM, Morricone L, Ambrosi B. Influence of epicardial adipose tissue and adipocytokine levels on cardiac abnormalities in visceral obesity. Int J Cardiol. 2007;121(1):132–134. doi:10.1016/j.ijcard.2006.08.061
31. Lehrke M, Marx N. Diabetes Mellitus and Heart Failure. Am J Med. 2017;130(6s):S40–s50. doi:10.1016/j.amjmed.2017.04.010
32. Kokubo Y, Hypertension MC. Is a Risk Factor for Several Types of Heart Disease: review of Prospective Studies. Adv Exp Med Biol. 2017;956:419–426. doi:10.1007/5584_2016_99
33. Liu JE, Palmieri V, Roman MJ, et al. The impact of diabetes on left ventricular filling pattern in normotensive and hypertensive adults: the Strong Heart Study. J Am Coll Cardiol. 2001;37(7):1943–1949. doi:10.1016/s0735-1097(01)01230-x
34. Miazgowski T, Taszarek A, Miazgowski B. Visceral fat, cardiometabolic risk factors, and nocturnal blood pressure fall in young adults with primary hypertension. The Journal of Clinical Hypertension. 2019;21(9):1406–1414. doi:10.1111/jch.13639
35. Wang Z, Zeng X, Chen Z, et al. Association of visceral and total body fat with hypertension and prehypertension in a middle-aged Chinese population. J Hypertens. 2015;33(8):1555–1562. doi:10.1097/hjh.0000000000000602
36. Dhalla NS. Subcellular remodeling and heart dysfunction in chronic diabetes. Cardiovasc Res. 1998;40(2):239–247. doi:10.1016/s0008-6363(98)00186-2
37. Seravalle G, Grassi G. Obesity and hypertension. Pharmacol Res. 2017;122:1–7. doi:10.1016/j.phrs.2017.05.013
38. Sandeep S, Gokulakrishnan K, Velmurugan K, Deepa M. Visceral & subcutaneous abdominal fat in relation to insulin resistance & metabolic syndrome in non-diabetic south Indians. Indian J Med Res. 2010;131:629–635.
39. Miazgowski T, Krzyżanowska-Świniarska B, Dziwura-Ogonowska J, Widecka K. The associations between cardiometabolic risk factors and visceral fat measured by a new dual-energy X-ray absorptiometry-derived method in lean healthy Caucasian women. Endocrine. 2014;47(2):500–505. doi:10.1007/s12020-014-0180-7
40. Sogabe M, Okahisa T, Hibino S, Yamanoi A. Usefulness of differentiating metabolic syndrome into visceral fat type and subcutaneous fat type using ultrasonography in Japanese males. J Gastroenterol. 2012;47(3):293–299. doi:10.1007/s00535-011-0489-4
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.