Back to Journals » Clinical Ophthalmology » Volume 20
Virtual Reality in Ophthalmic Surgical Education: Current Innovations and Future Perspectives
Authors Ahuja AS ![]() , Yang S, Paredes III AA, Tu DC
, Yang S, Paredes III AA, Tu DC
Received 3 January 2026
Accepted for publication 14 April 2026
Published 25 May 2026 Volume 2026:20 593471
DOI https://doi.org/10.2147/OPTH.S593471
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Abhimanyu S Ahuja,1 Sen Yang,1 Alfredo A Paredes III,2 Daniel C Tu1,3
1Department of Ophthalmology, Casey Eye Institute, Oregon Health and Science University, Portland, OR, USA; 2Charles E. Schmidt College of Medicine, Florida Atlantic University, Boca Raton, FL, USA; 3Operative Care Division, Veterans Affairs Portland Health Care System, Portland, OR, USA
Correspondence: Daniel C Tu, Department of Ophthalmology, Casey Eye Institute, Oregon Health and Science University, Portland, OR, USA, Tel +1-503-494-9255, Email [email protected]
Abstract: Virtual reality (VR) and augmented reality (AR) technologies have recently gained momentum in medical education and show particular promise for ophthalmic surgical training. VR creates immersive, computer-generated environments for simulated learning, whereas AR enhances the real-world by superimposing interactive digital elements. Traditional microsurgical training relies on wet-lab practice using model or cadaver eyes, as well as operative experience on live patients. The educational value of wet-lab training often depends on time-intensive direct supervision by a senior surgeon, while early surgical experience on live patients is associated with higher complication rates among novice surgeons. Virtual reality technologies offer a structured learning environment in which ophthalmology residents can practice independently without relying on senior supervision or live patients. By expanding opportunities for early skills practice while reducing patient risk, these tools may serve as a valuable adjunct to supervised operative training during the initial stages of surgical skill acquisition. New applications are emerging for commercially available VR headsets such as the Apple Vision Pro and Meta Quest, while standalone simulators like Haag-Streit Eyesi, HelpMeSee, and Alcon Fidelis have been developed specifically for ophthalmology. These platforms support immersive training environments, with tools such as RetinaVR for vitrectomy simulation and the AAO VR Education app for retinopathy of prematurity diagnosis. The Apple Vision Pro, paired with the ZEISS Surgery Optimizer application, enables three-dimensional surgical video recording, supports case storage and review by trainees, and facilitates learning from procedures performed by experienced surgeons. Compared to traditional simulators, these innovations reduce cost and hardware barriers, while enhancing scalability and customization. Standalone simulators such as HelpMeSee offer validated modules for manual small incision cataract surgery and phacoemulsification, while Alcon Fidelis introduces high-fidelity haptics and foot-pedal functionality to simulate intraocular procedures. Many established simulators such as HelpMeSee and Eyesi demonstrate stronger evidence of construct validity, whereas newer consumer-based platforms currently have more limited ophthalmic validation. Looking ahead, the integration of artificial intelligence with VR systems may further personalize surgical education by analyzing surgical recordings to estimate complication risk and skill progression. In this Perspective article, we synthesize findings from peer reviewed studies alongside recent reports describing emerging VR platforms to compare levels of validation across technologies, identify current evidence gaps, and assess the potential of these immersive platforms to make surgical training more affordable, efficient, and widely accessible.
Keywords: virtual reality, augmented reality, cataract, retina, surgical training, graduate medical education
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Lansingh has been published for this article.
Introduction
While both virtual reality (VR) and augmented reality (AR) technologies have existed since the 1990s, technological advancements within the past decade have significantly expanded their applications in medicine.1 Simulation-based learning is grounded in educational theories, including deliberate practice and experiential learning.2,3 Deliberate practice emphasizes structured repetition of tasks with immediate feedback to progressively refine performance, while experiential learning conceptualizes skill acquisition as a cyclical process involving concrete, real-world experience, reflective observation, abstract conceptualization, and active experimentation.2,3 Within this framework, immersive simulation provides a structured environment for active experimentation and skill rehearsal prior to real-world clinical exposure.3 Together, these models support the use of immersive simulation as a supplement to traditional surgical education with the potential to accelerate technical skill development in controlled environments.2,3 VR refers to the creation of a simulated environment, often experienced through a head-mounted display that delivers visual, auditory, and tactile information, allowing users to navigate digital scenarios as if they were physically present.4 Conversely, AR utilizes a headset capable of superimposing digital contents onto the real-world, thus displaying a real and simulated experience simultaneously.1 In ophthalmic training, junior residents have higher rates of surgical complications than senior trainees, and among all trainees, complication rates increase with case complexity, showcasing the challenges of acquiring surgical proficiency solely through conventional operative exposure.5,6 VR and AR technologies have been implemented to enable trainees to practice surgical techniques on virtual patients, enhancing their skills and reducing errors before operating on real patients, thereby serving as an adjunct to supervised operative training, particularly during the early stages of residency.7 Additionally, VR and AR allow trainees to practice simple tasks without continuous supervision by medical staff, reducing cost and increasing training efficiency.7 In ophthalmology, specific VR and AR tools have emerged for surgical training. These include applications for commercially available headsets and dedicated simulators developed for ophthalmic education (Figure 1). Standalone systems such as Eyesi and HelpMeSee generate virtual environments composed of surgical microscopes, artificial eyes, and surgical instruments for cataract surgical training.8,9 These simulators also concurrently record parameters such as instrument handling, efficiency, and complications.8,9 More recently, applications developed for devices like the Apple Vision Pro and Meta Quest have introduced a lower-cost, scalable approach to immersive surgical education.
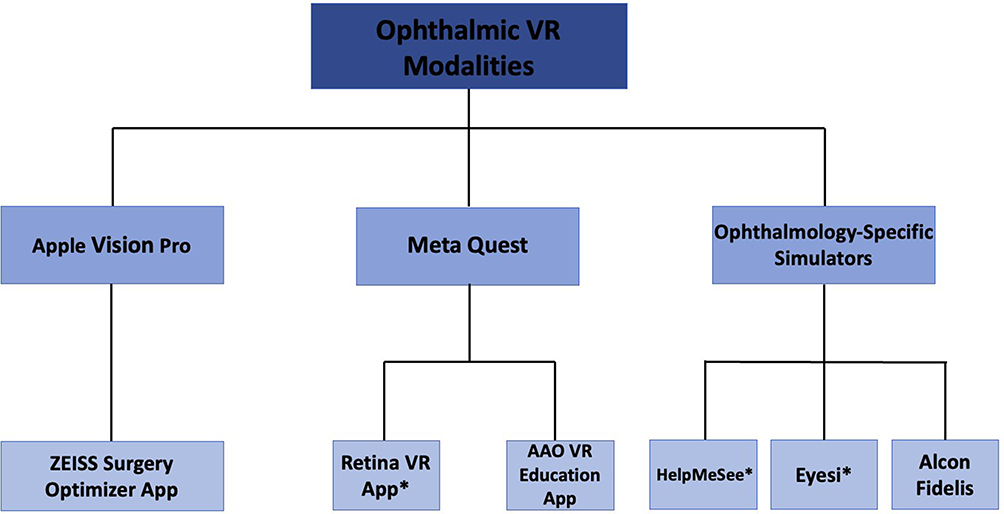 |
Figure 1 Overview of virtual reality (VR) platforms and applications used in ophthalmic surgical training. Abbreviations: AAO, American Academy of Ophthalmology; VR, Virtual Reality; App, Application. Notes: “*” indicates VR modalities with evidence of validation. |
Current Innovations
Platforms such as Apple Vision Pro primarily support immersive 3D surgical video review and case analysis, complementing rather than replacing interactive task-based simulation.10 Commercial headsets like the Apple Vision Pro and Meta Quest, along with standalone ophthalmology simulators such as Haag-Streit Eyesi, HelpMeSee, and Alcon Fidelis, have expanded opportunities for ophthalmic surgical training through recent technological advancements. To inform this Perspective, we reviewed peer reviewed studies identified through searches of PubMed and Google Scholar evaluating VR and AR applications in ophthalmic surgical education, alongside recent reports describing emerging immersive technologies. We utilized combinations of keywords including, “virtual reality,” “augmented reality,” “mixed reality,” “simulation,” “ophthalmology,” “surgical training,” “cataract surgery,” “phacoemulsification,” “manual small incision cataract surgery,” “vitrectomy,” “retinopathy of prematurity,” and the names of various platforms discussed in this manuscript including Apple Vision Pro, ZEISS Surgery Optimizer, Meta Quest, RetinaVR, AAO VR Education, Eyesi, HelpMeSee, and Alcon Fidelis. Studies were selected based on relevance to ophthalmic surgical education. Given the rapidly evolving nature of this field, we aimed to critically synthesize established validation data with emerging platforms in order to contextualize current evidence and identify areas for further investigation.
Apple Vision Pro
The Apple Vision Pro is a mixed reality headset that was released in the United States in February 2024.10 Unlike platforms such as Eyesi, HelpMeSee, and RetinaVR, which operate exclusively in VR environments, the Apple Vision Pro incorporates digital overlays into the physical world using inputs such as hand gestures, eye tracking, and voice commands.10 The device offers high-resolution visual display capabilities, potentially supporting clearer surgical video review.10 Preliminary research has suggested that extended reality systems like the Apple Vision Pro may offer future applications in ophthalmology, including support for diagnostic screening and visual rehabilitation in conditions such as strabismus.11 Additionally, access to the Apple App Store allows developers to design applications for ophthalmic microsurgical education, potentially expanding the device’s utility in surgical training.
As the Apple Vision Pro has just recently launched, its current use in educating ophthalmology trainees remains limited. However, ZEISS recently released the ZEISS Surgery Optimizer software for the Apple Vision Pro, offering an immersive platform for reviewing surgical cases that may support intraocular surgical skill development (Table 1).12 Video-based review has been shown to improve learning outcomes in various disciplines by enhancing cognitive skills such as decision-making.13 Currently, ophthalmology trainees often record their cataract surgeries while operating with a surgical microscope and later review two-dimensional footage on a computer to identify areas for improvement. However, the ZEISS Surgery Optimizer app allows residents to upload and archive surgical cases for later review, and also provides access to cases shared by other surgeons, facilitating exposure to a wider range of surgical techniques.12 Unlike traditional two-dimensional video review, the app enables three-dimensional visualization that simulates the view through a surgical microscope.12,14 In surgical education, video review has demonstrated greater efficacy than traditional teaching, and the incorporation of three-dimensional modalities into video review has been associated with faster acquisition of surgical skills and improved theoretical understanding of techniques.15 Specifically, the use of 3D video imaging technology in surgical visualization and training has demonstrated favorable educational outcomes in many surgical subspecialties including neurosurgery,16,17 general surgery,18 otolaryngology,19 and urology,20 suggesting that similar 3D technology in the Apple Vision Pro may offer educational benefit. Within ophthalmology, three-dimensional viewing systems have been deployed in vitreoretinal surgery, which have demonstrated the potential to bolster resident and fellow comprehension of intraocular anatomy.21–23 While formal validation studies are not yet available, the ZEISS Surgery Optimizer represents a novel attempt to integrate three-dimensional video review into ophthalmology training using a commercially available mixed reality headset. Future updates may include AI-assisted video parsing to enhance feedback and learning efficiency. As an emerging technology, the discussion of the Apple Vision Pro within this Perspective aims to identify areas requiring formal validation and to promote rigorous, evidence-based comparison with established simulation platforms through future studies.
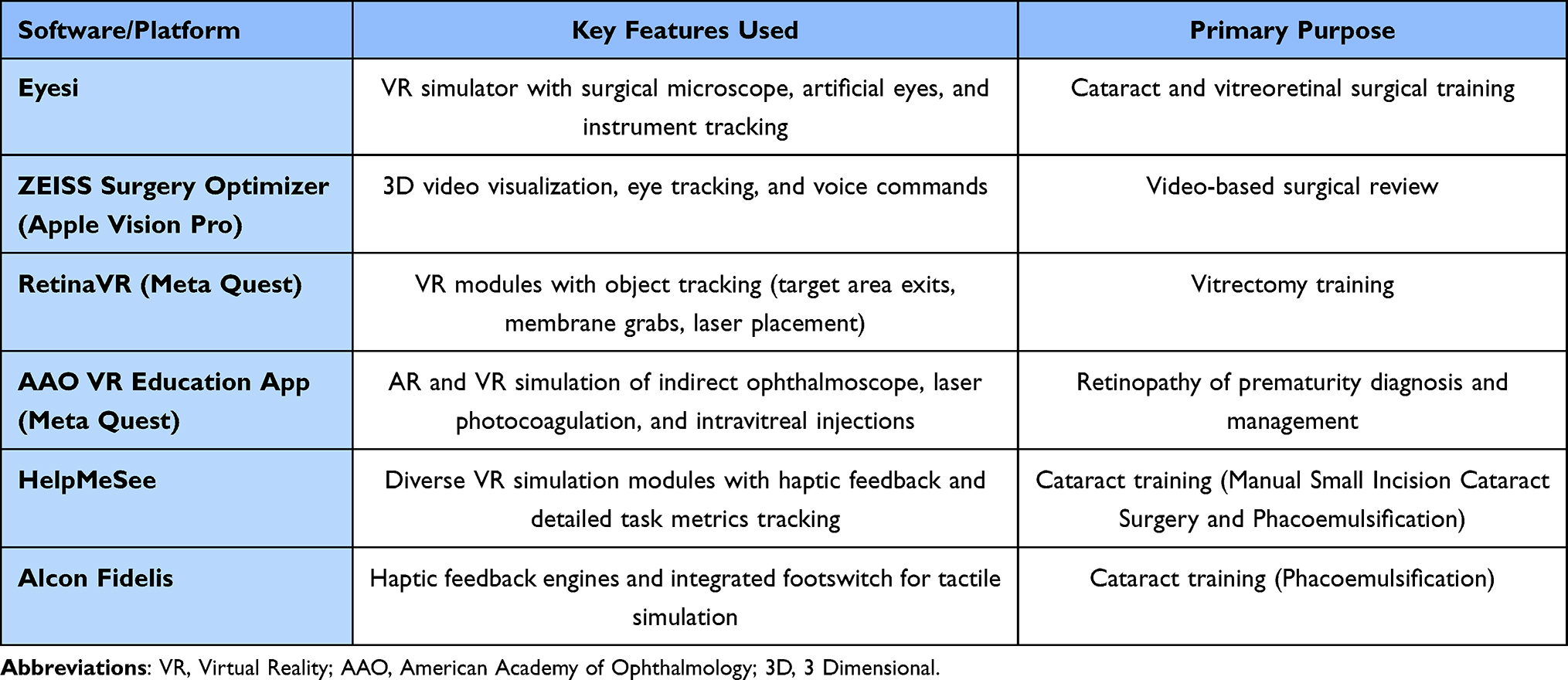 |
Table 1 Key Features and Purpose of VR Simulators |
Meta Quest
The Meta Quest 3 released in 2023 as the newest version of the Meta Quest headset and offers both VR and AR functionality.24 The device offers improved display resolution compared to earlier models, which may support enhanced visual clarity.24 Within Meta Quest, newly developed apps such as RetinaVR have provided immersive VR training modules for developing skills necessary for vitrectomy surgery.25 Antaki et al designed RetinaVR and compared novice ophthalmology residents with no surgical experience to fellowship-trained vitreoretinal surgeons with an average of approximately 16 years of surgical experience.25 Participants were assessed on efficiency, measured by module completion time, and safety, evaluated by the number of iatrogenic retinal touches.25 Additional module-specific metrics were recorded, including exits from the target area, deviations from the shaving path, number of membrane grabs, and number and location of laser applications.25 For efficiency metrics, there were no significant differences in module completion time between novices and experts.25 However, experts achieved significantly higher safety scores in the membrane peeling module and scored significantly higher on the core vitrectomy module-specific tasks.25 Finally, experts demonstrated significantly greater precision in laser placement within the endolaser application module.25 Because RetinaVR performance appears to correlate with surgical experience and proficiency across several modules, the platform demonstrates preliminary construct validity, indicating that it can distinguish between users of differing expertise based on their performance within the simulator.25 However, given the small sample size of 20 surgeons included in the study and the high variance observed within the novice cohort, larger studies should be performed to enable more robust statistical analysis and confirm construct validity.25
In late 2024, the American Academy of Ophthalmology collaborated with FundamentalVR to develop the AAO VR Education app for the Meta Quest platform, aimed at training users in the diagnosis of retinopathy of prematurity (ROP).26 The app allows ophthalmology trainees to simulate examinations of virtual infants using digital tools such as an indirect ophthalmoscope, scleral depressor, and BIO lens, and includes modules for familiarization with common treatment steps such as laser photocoagulation and intravitreal injections.26 This app may help expand exposure to ROP-related training, particularly in settings where opportunities for hands-on experience with pediatric patients are limited. However, while RetinaVR has demonstrated preliminary construct validity for surgical skill assessment, the AAO VR Education app has not yet undergone formal validation studies, and its educational impact remains to be determined.
Ophthalmic Surgical Simulators
Over the last few years, a variety of standalone VR simulators, such as Eyesi, HelpMeSee, and Alcon Fidelis, have been developed specifically for ophthalmic surgical training. The Eyesi surgical simulator, introduced in 2004,27 is among the earliest standalone virtual reality platforms and has since become the most extensively studied and widely adopted simulator in ophthalmic surgical training, with multiple studies demonstrating its construct validity.27–29 The simulator is primarily used for phacoemulsification and vitreoretinal training and consists of a microscope-based system with three-dimensional visualization, a mannequin head with a virtual eye, and foot pedal controls, providing a platform that has been shown to enhance surgical performance, reduce intraoperative complication rates, and improve trainee confidence.30 While Eyesi provides a well-established benchmark for simulation-based training, newer standalone simulators such as HelpMeSee and AlconVR have been developed to expand procedural training capabilities, improve accessibility across diverse training environments, and incorporate features such as haptic feedback.
HelpMeSee was initially designed to train surgeons in Manual Small Incision Cataract Surgery (MSICS), offering a modality particularly useful in low- and middle-income countries where access to phacoemulsification is limited.31 Hutter et al (2023) compared novice ophthalmologists with no cataract surgery experience or experience limited to phacoemulsification to a group of experienced surgeons proficient in both phacoemulsification and MSICS, using the HelpMeSee simulator.31 Participants completed a series of simulated MSICS tasks, such as creating a scleral groove, dissecting a tunnel, performing a capsulorrhexis, conducting hydrodissection and nuclear dislocation, delivering the nucleus, and inserting the intraocular lens.31 Each task was graded using specific performance metrics, such as achieving the correct groove length, maintaining an appropriate length of inner tunnel limit, forming a capsulorrhexis of ideal size, and avoiding endothelial touch.31 In total, 30 distinct metrics were assessed across the tasks, creating a maximum score of 30 points and a passing threshold defined as 20 points.31 Novices achieved a mean score of 15.5 (±3.0), while experienced surgeons achieved a mean score of 22.7 (±4.3), demonstrating a statistically significant difference.31 Only 6.7% of novice ophthalmologists achieved a passing score, compared to 70% of experienced surgeons.31 These findings support the construct validity of the HelpMeSee simulator, as it was able to differentiate between novice and experienced MSICS surgeons based on objective performance metrics.31 However, the study included only 25 participants, comprising 15 novices and 10 experts,31 highlighting the need for future studies with larger sample sizes to confirm construct validity. As a key component of MSICS, scleral tunnel construction has also been specifically studied using the HelpMeSee simulator.32 In another study, resident ophthalmologists were randomized into experimental and control groups.32 Residents in the experimental group were trained to perform scleral tunnel construction using learning modules on HelpMeSee.32 In contrast, residents in the control group received traditional training based on their institution’s curriculum, without the use of HelpMeSee.32 Subsequently, both groups performed live surgical training under the supervision of experienced surgeons.32 Residents were evaluated based on the number of errors during their first 20 procedures, including major errors such as uveal prolapse, buttonhole incision, Descemet membrane detachment, and tunnel laceration, as well as minor errors such as endothelial touch or contact with the iris or lens.32 Residents in the experimental group trained with HelpMeSee committed 52% fewer major errors than those in the control group, a statistically significant difference.32 Additionally, the experimental group committed 41% fewer minor errors, but this difference did not reach statistical significance.32 Together, these studies support the utility of HelpMeSee as a validated tool for MSICS training, demonstrating reductions in surgical error rates and the ability to distinguish between varying levels of surgical experience.
Starting in 2023, HelpMeSee introduced phacoemulsification training modules, and a subsequent study provided preliminary evidence supporting their construct validity.27 Participants were divided into expert and intermediate groups, based on whether they had performed more or fewer than 300 cataract surgeries, respectively.27 Participants were graded using a point-based system, with deductions applied for significant errors made during phacoemulsification modules.27 A variety of HelpMeSee modules were included, such as capsulorhexis, hydrodissection, irrigation and aspiration for cortex removal, and intraocular lens insertion and replacement, among others.27 Participants could achieve a maximum score of 46 points if no errors were committed across any modules.27 Expert surgeons achieved a mean score of 35.8 (±1.5), significantly higher than the 27.2 (±2.3) mean score of intermediate surgeons.27 By supporting both MSICS and phacoemulsification, HelpMeSee offers a unique advantage through its validated, simulation-based training platform, expanding cataract surgery training beyond phacoemulsification for residency programs that do not routinely include MSICS.27
Alcon Fidelis, introduced in 2024, is a standalone VR simulator that integrates a head-mounted display with a haptic feedback system to replicate both visual and tactile aspects of cataract surgery.33 Specifically, haptic engines simulate the tactile sensations of surgical instruments interacting with ocular structures, while an integrated footswitch replicates the foot-operated controls used in actual cataract surgery.33 Construct validity has not yet been demonstrated for Alcon Fidelis, but its integration of high-fidelity haptics suggests potential for future development as a realistic cataract surgery training tool.
Discussion
The Eyesi Ophthalmic Surgical Simulator remains the gold standard simulated surgical environment for ophthalmologic training and has been steadily adopted by residency programs worldwide as part of their core surgical curriculums.27 Previous systematic reviews on simulation-based ophthalmic training have shown that Eyesi is the most extensively studied VR surgical simulator, with dozens of validity studies demonstrating its utility.28,29 These reviews provide preliminary evidence that VR-based surgical modalities can improve operative performance when compared with traditional teaching approaches.29,34 Notably, extended reality (XR) platforms, encompassing both VR and AR, have been associated with significant reductions in cataract surgery complication rates, such as posterior capsular rupture, and with shorter operative times among trainees compared to control groups not exposed to XR-based training.34
The majority of current evidence is focused on cataract simulators, whereas fewer studies have examined vitreoretinal procedures.28,29 Among available platforms, Eyesi is the most extensively validated, with multiple studies confirming its construct validity and demonstrating measurable improvements in surgical skill acquisition.28,29 However, the benefits of Eyesi training appear to be greatest among novice residents, and its impact in more experienced trainees may be comparable to that of traditional wet-lab training using animal or cadaveric tissue.29 Combining wet-lab training with Eyesi simulation may provide the most robust improvements, with greater reductions in operative errors than either modality alone.29 Furthermore, cataract surgery simulators appear to confer skill enhancement only for the specific procedures being practiced.28 For example, proficiency gained through cataract surgery simulation on Eyesi may not readily translate to its vitreoretinal modules, highlighting the need for a broader range of modules and procedure-specific curricula.28,35,36 By expanding the breadth of available training modules, emerging platforms such as Apple Vision Pro and Meta Quest could address the current challenge of limited skill transferability across surgical domains.
Despite its popularity and established evidence base, Eyesi is not without limitations. The Eyesi simulator has high upfront ($169,000+) and maintenance costs ($26,000+/year).37 HelpMeSee and AlconVR likely have similarly high costs, though specific pricing data remain limited. In contrast, commercial headsets like the Apple Vision Pro and Meta Quest 3 offer a more affordable entry point for institutions.38,39 Lower cost platforms may contribute to the democratization of surgical training by reducing barriers to access, particularly in low- and middle-income regions where cost-prohibitive systems such as Eyesi are less feasible. However, even low-cost headsets require software licenses, compatible devices, and ongoing support that may contribute to recurring expenses.39 As technology improves, hybrid models using both standalone systems and consumer hardware may become viable for comprehensive training.39 Alongside financial considerations, practical challenges to VR implementation should also be considered, including integration into residency curricula, faculty time requirements, and data storage and privacy considerations for surgical video recording.
Evidence supporting VR platforms in ophthalmology spans several domains, including construct validity, educational outcomes within simulated environments, and clinical outcomes in live surgical settings. Established systems such as Eyesi and HelpMeSee demonstrate construct validity and, in some studies, reduced surgical error rates among trainees.27–29,34 In contrast, emerging consumer-based platforms, including Apple Vision Pro and Meta Quest applications, currently demonstrate limited validation, with few data on downstream clinical outcomes. For example, platforms such as the AAO VR Education app and Alcon Fidelis lack evidence of construct validity. Additionally, although the use of 3D video has been associated with faster learning,15 tools like the ZEISS Surgery Optimizer app currently lack direct evidence demonstrating superiority over traditional teaching methods. While RetinaVR and HelpMeSee have demonstrated construct validity in preliminary studies,25,31 larger investigations are still needed to better quantify performance differences between novice and experienced surgeons.
Another limitation of current commercial headsets such as the Apple Vision Pro and Meta Quest 3 is the lack of haptic feedback, which reduces their ability to replicate surgical instrument handling. In contrast, Alcon Fidelis incorporates high-fidelity haptics,33 though likely at a higher overall cost, underscoring a trade-off between affordability and fidelity that residency programs will need to weigh when considering integration of these platforms into training curricula.
Artificial intelligence may advance these platforms by enabling automated skill assessment and tailored feedback. For example, AI tools now detect surgical instruments, identify phases of cataract surgery, and assess complications from operative videos.40 In a systematic review, Müller et al (2024) examined 12 AI models developed for surgical instrument detection and compared their reported area under the receiver operating characteristic curve (ROC AUC) values.40 Reported ROC AUC values for these models ranged from 0.976 to 0.998.40 An additional 17 models focused on surgical phase recognition, with ROC AUC values ranging from 0.772 to 0.990 and accuracy values ranging from 0.645 to 0.978.40 Finally, nine models aimed to estimate surgical skill or recognize complications, such as lens instability, and reported ROC AUC values ranged from 0.570 to 0.970.40,41 A key limitation, however, is the lack of standardization in reporting metrics; studies variably report outcomes such as accuracy, sensitivity, specificity, or ROC AUC, making comparisons across models difficult.40 While ROC AUC values for instrument detection approach 1.0, performance remains more variable for tasks such as phase recognition, skill assessment, and complication detection, highlighting the need for further refinement and validation.40 With further development, AI-based complication prediction and surgical efficiency assessment tools may eventually integrate with VR-based platforms, such as those incorporating 3D surgical video capture, to support personalized, data-driven surgical training. Standardized benchmarks will be needed to meaningfully evaluate AI-based tools in VR education.
Conclusion
VR platforms are expanding ophthalmic education, with some, but not all, technologies already demonstrating promising validity. Rigorous comparative studies evaluating VR alongside traditional surgical training models are still needed. Further, many existing investigations are limited by small cohorts, heterogeneity among novice trainees, and inconsistent performance metrics, underscoring the importance of larger, standardized studies with long-term follow-up.
The future may involve integration of AI-driven analytics and 3D surgical environments capable of simulating complex intraoperative scenarios ranging from shallow chambers to zonular dialysis. With continued validation, VR-based platforms could significantly elevate the scope and effectiveness of ophthalmic surgical training.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xiong J, Hsiang EL, He Z, Zhan T, Wu ST. Augmented reality and virtual reality displays: emerging technologies and future perspectives. Light Sci Appl. 2021;10(1):216. doi:10.1038/s41377-021-00658-8
2. Ericsson KA. Deliberate practice and acquisition of expert performance: a general overview. Acad Emerg Med. 2008;15(11):988–8. doi:10.1111/j.1553-2712.2008.00227.x
3. Wijnen-Meijer M, Brandhuber T, Schneider A, Berberat PO. Implementing Kolb´s Experiential Learning Cycle by Linking Real Experience, Case-Based Discussion and Simulation. J Med Educ Curric Dev. 2022;9:23821205221091510. doi:10.1177/23821205221091511
4. Girondini M, Montanaro M, Gallace A. Exploring virtual reality object perception following sensory-motor interactions with different visuo-haptic collider properties. Sci Rep. 2024;14(1):10011. doi:10.1038/s41598-024-59570-x
5. Melega MV, Pessoa Cavalcanti Lira R, da Silva IC, et al. Comparing Resident Outcomes in Cataract Surgery at Different Levels of Experience. Clin Ophthalmol. 2020;14:4523–4531. doi:10.2147/OPTH.S285967
6. Shakarchi FF, Karimaghaei S, Azhari J, et al. Posterior capsule rupture as a performance indicator in resident cataract surgery: an eight-year audit. AJO Int. 2025;2(4):100181. doi:10.1016/j.ajoint.2025.100181
7. Yeung AWK, Tosevska A, Klager E, et al. Virtual and Augmented Reality Applications in Medicine: analysis of the Scientific Literature. J Med Internet Res. 2021;23(2):e25499. doi:10.2196/25499
8. Wisse RP, Coster T, Van der Schaaf M, Ten Cate O. The Eyesi simulator in training ophthalmology residents: results of a pilot study on self-efficacy, motivation and performance. BMJ Simul Technol Enhanc Learn. 2017;3(3):111–115. doi:10.1136/bmjstel-2016-000137
9. Nair AG, Ahiwalay C, Bacchav AE, Sheth T, Lansingh VC. Assessment of a high-fidelity, virtual reality-based, manual small-incision cataract surgery simulator: a face and content validity study. Indian J Ophthalmol. 2022;70(11):4010–4015. doi:10.4103/ijo.IJO_1593_22
10. Apple Inc. Apple Vision Pro available in the US on February 2. 2024. Available from: https://www.apple.com/newsroom/2024/01/apple-vision-pro-available-in-the-us-on-february-2/.
11. Waisberg E, Ong J, Masalkhi M, et al. The future of ophthalmology and vision science with the Apple Vision Pro. Eye. 2024;38(2):242–243. doi:10.1038/s41433-023-02688-5
12. ZEISS. ZEISS Surgery Optimizer. Available from: https://www.zeiss.com/meditec/en/products/surgery-optimizer.html#apple-vision-pro.
13. Zhao J, Gu Q, Zhao S, Mao J. Effects of video-based training on anticipation and decision-making in football players: a systematic review. Front Hum Neurosci. 2022;16:945067. doi:10.3389/fnhum.2022.945067
14. ZEISS. ZEISS ARTEVO 800. Available from: https://www.zeiss.com/meditec/en/products/surgical-microscopes/ophthalmic-microscopes/artevo-800.html.
15. Ahmet A, Gamze K, Rustem M, Sezen KA. Is Video-Based Education an Effective Method in Surgical Education? A Systematic Review. J Surg Educ. 2018;75(5):1150–1158. doi:10.1016/j.jsurg.2018.01.014
16. Heath MD, Cohen-Gadol AA. Intraoperative stereoscopic 3D video imaging: pushing the boundaries of surgical visualisation and applications for neurosurgical education. Br J Neurosurg. 2012;26(5):662–667. doi:10.3109/02688697.2012.672057
17. Bruening DM, Truckenmueller P, Stein C, et al. 360° 3D virtual reality operative video for the training of residents in neurosurgery. Neurosurg Focus. 2022;53(2):E4. doi:10.3171/2022.5.FOCUS2261
18. Larkins K, Khan M, Mohan H, Warrier S, Heriot A. A systematic review of video-based educational interventions in robotic surgical training. J Robot Surg. 2023;17(4):1329–1339. doi:10.1007/s11701-023-01605-y
19. Niederhauser L, Fink RD, Mast FW, Caversaccio M, Anschuetz L. Video Learning of Surgical Procedures: a Randomized Comparison of Microscopic, 2- and 3-Dimensional Endoscopic Ear Surgery Techniques. Otol Neurotol. 2022;43(7):e746–e752. doi:10.1097/MAO.0000000000003550
20. Gribaudo M, Piazzolla P, Porpiglia F, Vezzetti E, Violante MG. 3D augmentation of the surgical video stream: toward a modular approach. Comput Methods Programs Biomed. 2020;191:105505. doi:10.1016/j.cmpb.2020.105505
21. Chhaya N, Helmy O, Piri N, Palacio A, Schaal S. COMPARISON OF 2D AND 3D VIDEO DISPLAYS FOR TEACHING VITREORETINAL SURGERY. Retina. 2018;38(8):1556–1561. doi:10.1097/IAE.0000000000001743
22. Shoshany TN, Agranat JS, Armstrong G, Miller JB. The User Experience on a 3-Dimensional Heads-Up Display for Vitreoretinal Surgery Across All Members of the Health Care Team: a Survey of Medical Students, Residents, Fellows, Attending Surgeons, Nurses, and Anesthesiologists. J Vitreoretin Dis. 2020;4(6):459–466. doi:10.1177/2474126420929614
23. Razavi P, Cakir B, Baldwin G, D’Amico DJ, Miller JB. Heads-Up Three-Dimensional Viewing Systems in Vitreoretinal Surgery: an Updated Perspective. Clin Ophthalmol. 2023;17:2539–2552. doi:10.2147/OPTH.S424229
24. Meta. Meta Quest 3. Available from: https://www.meta.com/quest/quest-3/?srsltid=AfmBOopx5jfR9W1uDqJ-xlqDALWJ3UUnLjoyj8jLGGbpHWeKOUZkR-B.
25. Antaki F, Doucet C, Milad D, Giguère CÉ, Ozell B, Hammamji K. Democratizing Vitreoretinal Surgery Training With a Portable and Affordable Virtual Reality Simulator in the Metaverse. Transl Vis Sci Technol. 2024;13(4):5. doi:10.1167/tvst.13.4.5
26. American Academy of Ophthalmology. AAO VR Education. 2024. Available from: https://www.aao.org/education/interactive-tool/aao-vr-education.
27. Yaïci R, Poirot J, Dormegny L, et al. Validity evidence of a new virtual reality simulator for phacoemulsification training in cataract surgery. Sci Rep. 2024;14(1):25524. doi:10.1038/s41598-024-76405-x
28. Ong CW, Tan MCJ, Lam M, Koh VTC. Applications of Extended Reality in Ophthalmology: systematic Review. J Med Internet Res. 2021;23(8):e24152. doi:10.2196/24152
29. Lee R, Raison N, Lau WY, et al. A systematic review of simulation-based training tools for technical and non-technical skills in ophthalmology. Eye. 2020;34(10):1737–1759. doi:10.1038/s41433-020-0832-1
30. Wei JW, Zhang Q, Wang XY, et al. Advances in the application of virtual reality technology in ophthalmic surgical skills training. Int J Ophthalmol. 2026;19(2):393–404. doi:10.18240/ijo.2026.02.23
31. Hutter DE, Wingsted L, Cejvanovic S, et al. A validated test has been developed for assessment of manual small incision cataract surgery skills using virtual reality simulation. Sci Rep. 2023;13(1):10655. doi:10.1038/s41598-023-32845-5
32. Nair AG, Ahiwalay C, Bacchav AE, et al. Effectiveness of simulation-based training for manual small incision cataract surgery among novice surgeons: a randomized controlled trial. Sci Rep. 2021;11(1):10945. doi:10.1038/s41598-021-90410-4
33. Alcon. Alcon Introduces State-of-the-Art Virtual Reality Surgical Training Technology. 2022. Available from: https://www.alcon.com/media-release/alcon-introduces-state-art-virtual-reality-surgical-training-technology/.
34. Yang L, Al-Ani A, Bondok MS, Gooi P, Chung H. The impact of extended reality simulators on ophthalmic surgical training and performance: a systematic review and meta-analysis of 17,623 eyes. Eye. 2025;39(9):1700–1709. doi:10.1038/s41433-025-03722-4
35. La Cour M, Thomsen ASS, Alberti M, Konge L. Simulators in the training of surgeons: is it worth the investment in money and time? 2018 Jules Gonin lecture of the Retina Research Foundation. Graefes Arch Clin Exp Ophthalmol. 2019;257(5):877–881. doi:10.1007/s00417-019-04244-y
36. Thomsen ASS, Kiilgaard JF, la Cour M, Brydges R, Konge L. Is there inter-procedural transfer of skills in intraocular surgery? A randomized controlled trial. Acta Ophthalmol. 2017;95(8):845–851. doi:10.1111/aos.13434
37. Nandigam K, Soh J, Gensheimer WG, Ghazi A, Khalifa YM. Cost analysis of objective resident cataract surgery assessments. J Cataract Refract Surg. 2015;41(5):997–1003. doi:10.1016/j.jcrs.2014.08.041
38. Pottle J. Virtual reality and the transformation of medical education. Future Healthc J. 2019;6(3):181–185. doi:10.7861/fhj.2019-0036
39. Farra SL, Gneuhs M, Hodgson E, et al. Comparative Cost of Virtual Reality Training and Live Exercises for Training Hospital Workers for Evacuation. Comput Inform Nurs. 2019;37(9):446–454. doi:10.1097/CIN.0000000000000540
40. Müller S, Jain M, Sachdeva B, et al. Artificial Intelligence in Cataract Surgery: a Systematic Review. Transl Vis Sci Technol. 2024;13(4):20. doi:10.1167/tvst.13.4.20
41. Ghamsarian N, Taschwer M, Putzgruber-Adamitsch D, Sarny S, El-Shabrawi Y, Schoeffmann K. LensID: a CNN-RNN-Based Framework Towards Lens Irregularity Detection in Cataract Surgery Videos. In: International Conference on Medical Image Computing and Computer-Assisted Intervention. Cham: Springer International Publishing. 2021.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.