Back to Journals » Journal of Inflammation Research » Volume 18
Viral Triggers Exposed: A Systematic Review of Virus-Induced Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis
Authors Fetriani U ![]() , Zakiawati D
, Zakiawati D
Received 11 June 2025
Accepted for publication 6 September 2025
Published 12 September 2025 Volume 2025:18 Pages 12575—12588
DOI https://doi.org/10.2147/JIR.S546186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Ulfa Fetriani,1 Dewi Zakiawati2
1Oral Medicine Residency Program, Department of Oral Medicine, Faculty of Dentistry, Padjadjaran University, Bandung, West Java, Indonesia; 2Department of Oral Medicine, Faculty of Dentistry, Padjadjaran University, Bandung, West Java, Indonesia
Correspondence: Ulfa Fetriani, Oral Medicine Residency Program, Department of Oral Medicine, Faculty of Dentistry, Padjadjaran University Jalan Sekeloa Selatan, Bandung, West Java, 40132, Indonesia, Tel +62 8971557962, Fax +62 22 7794121, Email [email protected]
Aim: Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are severe skin conditions characterized by widespread epidermal necrolysis and mucous membrane involvement. SJS affects less than 10% of the body surface area, while TEN involves over 30%, with cases between 10% and 30% classified as SJS/TEN overlap. Drug hypersensitivity reactions, especially to antibiotics, anticonvulsants, and non-steroidal anti-inflammatory medications, are the most common and well-established causes of SJS/TEN. In addition, infections, including viral ones like herpes simplex virus (HSV), influenza virus, varicella-zoster virus, and human immunodeficiency virus (HIV), have also been implicated as potential inducers, complicating management and requiring careful clinical vigilance.
Purpose: This review aims to investigate and compile information on reported cases of SJS/TEN potentially linked to virus infections.
Methods: Literature from PubMed, NCBI, ScienceDirect, and Cochrane Library databases was searched. The inclusion criteria were studies reporting details of patients diagnosed with SJS, TEN, or SJS/TEN overlap, potentially induced by viral infections. Cases were included if the viral infection occurred within one week before the rash onset, emphasizing the association between these infections and severe skin reactions.
Results: Ten studies were included in this systematic review, most of which demonstrated fair to good methodological quality. The review encompassed cases of virus-induced SJS/TEN, including herpes virus infection, influenza virus infection, varicella-zoster virus, HIV infection, COVID-19, and coxsackie infection, each with distinct manifestations.
Conclusion: The evidence strongly suggests that viral infections contribute to the development of SJS/TEN, yet the precise mechanisms remain unclear and warrant further research. Awareness of this risk is crucial, particularly in regions experiencing outbreaks of these viruses.
Keywords: viral infection, virus-induced, SJS, TEN
Introduction
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are severe adverse drug reactions characterized by widespread epidermal necrolysis. Both conditions present with skin blisters and affect mucous membranes in the mouth, nose, eyes, and genitals. SJS involves less than 10% of the body surface area and is marked by significant shedding of skin and mucosal epithelial cells, particularly in the oropharynx, eyes, urogenital, and anal mucosa.1 TEN is more severe, involving over 30% of the body surface area, while cases involving 10–30% are classified as SJS/TEN overlap. The mortality rates for SJS and TEN are 1–5% and 25–30%, respectively, with potential for long-term multi-organ damage following the acute phase. SJS/TEN is an immune-mediated hypersensitivity reaction, with over 200 drugs linked to its onset. Common triggers include nonsteroidal anti-inflammatory drugs (NSAIDs), sulpha-derived medications, lactam antibiotics, anticonvulsants, antiretroviral drugs, contrast agents, and allopurinol.2
The estimated annual incidence ranges from 1 to 2 cases per million population worldwide. Epidemiological studies reveal that medication hypersensitivity responses are the primary cause of 70–80% of reported cases. This is especially true for nonsteroidal anti-inflammatory medications, antibiotics, and anticonvulsants. A lesser but clinically important fraction of cases is induced by infections, including viral pathogens. The most prevalent infectious viruses include HIV, influenza, and herpes simplex virus.3
Despite challenges in identifying environmental risk factors, infections have also been associated with SJS/TEN. Viruses, bacteria, and other infections can trigger the condition, and vaccines for meningococcal B, yellow fever, and influenza have also been linked to cases. Viruses such as can potentially trigger SJS/TEN through various mechanisms.4–6 Following infections with human herpesviruses (HHV) 6 and 7, the immune response that should help to clear up the virus could put the body in a heightened state of sensitivity. This increases the risk of subsequent drug therapy to super-react. In addition, high levels of cytokines/chemokines, such as interferon γ (IFN-γ), produced after viral stimulation, can disrupt the immune balance by upregulating the major histocompatibility complex body (MHC II) molecules in antigen-presenting cells.4 This will promote the presentation of drug haptens. Another theory suggests that reactivation of latent viruses can cause drug eruptions, with delayed reactions occurring after the virus is reactivated and full antigens are formed.7
The role of viral infections in the pathogenesis of SJS/TEN remains incompletely understood. Current evidence suggests two possible pathways. First, some viral infections can cause SJS/TEN directly without drug exposure. Second, viruses can act as catalysts or triggers by altering the immune response or altering drug metabolism. In the literature, the terms “virus-induced” and “virus-triggered” SJS/TEN are often used interchangeably, making it difficult to distinguish between the two. For this review, we will always use the term “virus-induced” to describe and encompass both possible pathways.
Since management approaches vary based on the underlying cause, it is important to comprehend how these etiological elements are distributed. Infection-induced instances call for a distinct treatment strategy, occasionally necessitating targeted antiviral therapy and supportive care, whereas drug-induced cases frequently call for the offending agent to be removed right away. Thus, investigating how viral infections contribute to SJS/TEN is very important, particularly when outbreaks or endemic viral illnesses are involved.
This systematic review aims to investigate and compile information on reported cases of SJS/TEN potentially linked to virus infections, providing clinicians with valuable insights for better recognizing and managing these cases.
Materials and Methods
Eligibility Criteria
This systematic review and meta-analysis are reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.8 The review included case reports or case series that provided detailed clinical descriptions of patients diagnosed with SJS, TEN, or SJS/TEN overlap, where the condition was caused or suspected to be caused by viral infections (such as HSV, influenza virus, varicella-zoster virus, human immunodeficiency virus (HIV) and coxsackievirus), and where the full text was available. Cases were considered related to infectious agents if the infectious process was noted to have taken place within one week prior to the onset of the rash. The exclusion criteria for this review were studies involving patients where the exact cause of SJS, TEN, or SJS/TEN overlap could not be determined or where a viral infection was excluded as a possible cause, as well as case reports or case series describing other mucocutaneous side effects associated with viral infections.
Search Strategy and Study Selection
The literature search was conducted on July 4, 2024, and completed on the same day. We systematically searched and obtained papers from or case series. The search terms used were ((viral infection) OR (virus induced) OR (herpes simplex virus) OR (human herpes virus) OR (influenza virus) OR (coxsackievirus)) AND ((Stevens-Johnson Syndrome) OR (Stevens Johnson) OR (COVID-19) OR (toxic epidermal necrolysis) OR (Lyell’s syndrome) OR (Lyell Syndrome)). The details of the Medical Subject Headings (MeSH) terms are listed in Table 1. All records were then input into Rayyan software, which can detect duplicates and allow all authors to collaborate in selecting relevant studies. Selected authors conducted the initial search and imported all studies from various academic databases into the Rayyan software. Another author then cross-checked all the initial searches. All authors independently screened all available studies. All conflicts encountered during the screening process were resolved through group discussion until a conclusion was reached. If any missing or further data were needed, the corresponding authors were sent an inquiry email.
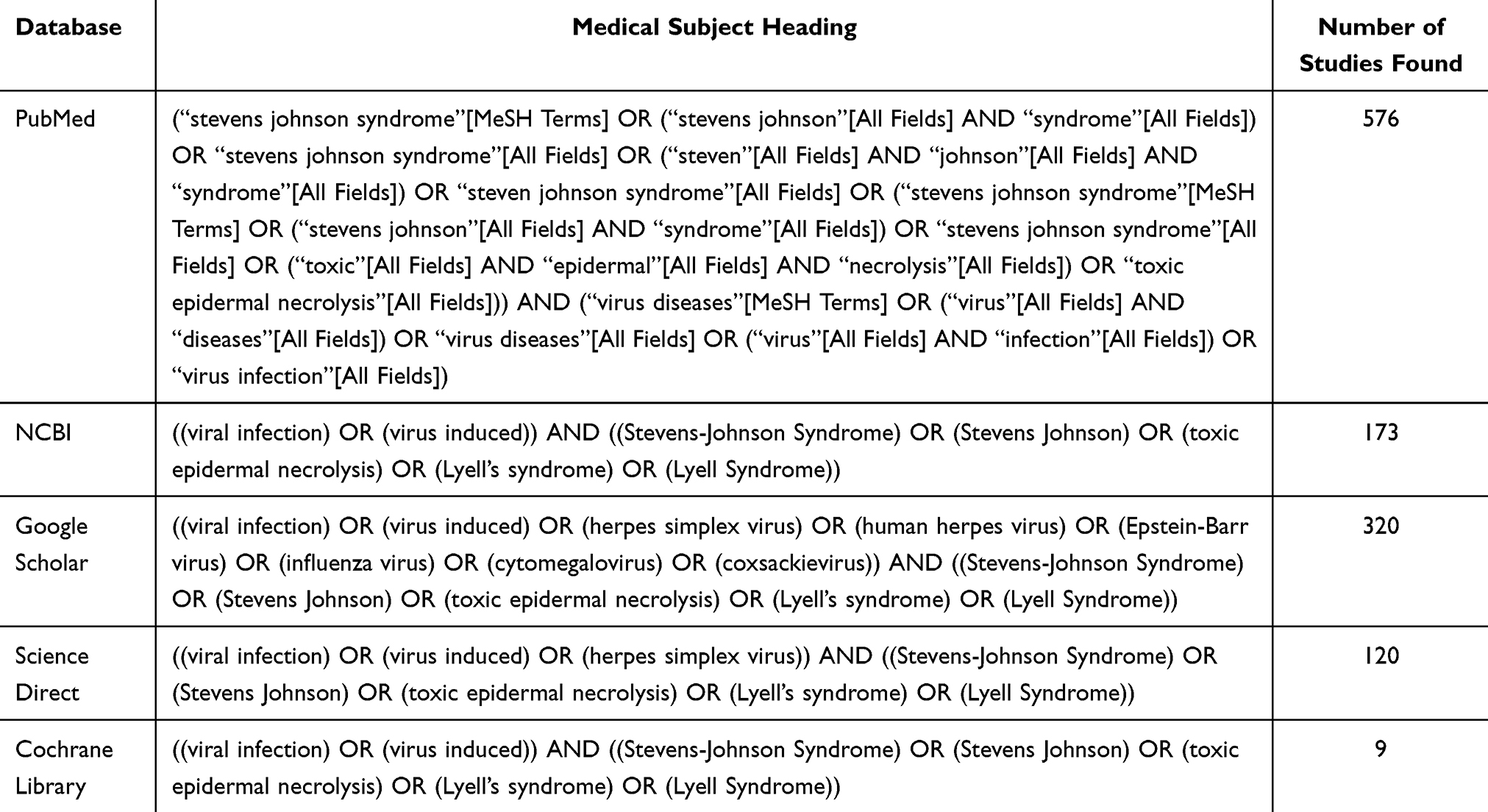 |
Table 1 Medical Subject Heading (MeSH) Terms Used in Each Database |
Data Extraction and Quality Assessment
The data extraction process was performed independently by the authors and then checked by another author. The authors recorded study characteristics (author, study year of publication, location, study design, and study period), demographic (age, gender), medical history, medications given, diagnosis of the reactions, diagnostic investigations (eg, physical examination, skin biopsy), time to onset of the reaction (from the onset of infection to the first symptoms of SJS/TEN), clinical manifestations, length of stay in hospital, outcome, as well as significant findings. All authors assessed the quality of each included study independently using the Joanna Briggs Institute (JBI) checklists for case reports and case series.9,10 The studies were scored either based on “Yes”, “No”, “Unclear or Not/Applicable” depending on the availability of information for every element. The assessment was conducted based on the reporting of 8 different elements namely, patient demographics, medical history, health status, physical examination and diagnosis, concomitant therapies, post-intervention health status, and drug administration reaction interface. Any discrepancies were resolved internally until an agreement was attained.
Results
Study Selection and Characteristics
The initial search yielded 1198 records, and 925 were screened after removing duplicates. A total of 813 studies were excluded after title and abstract screening, leaving 111 reports that were further assessed for eligibility. Studies with cases not confirmed as SJS/TEN, drug-induced SJS/TEN, and those written in a foreign language were excluded from leaving (Figure 1). We included 10 studies, consisting of seven case report studies, two case series studies, and one case control studies.
 |
Figure 1 PRISMA flowchart for selection of included studies. Notes: *If feasible, report the number of records identified from each database or register searched (rather than the total number across all databases/registers). **If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools. Adapted from Page M J, McKenzie J E, Bossuyt P M, Boutron I, Hoffmann T C, Mulrow C D et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372 :n71. Creative Commons. |
Quality of Study Assessment
The studies included in this review were assessed according to the JBI checklists. For case report studies, we used the JBI checklists for case reports. On the other hand, for case series studies, we used the JBI checklists for case series. All studies scored six or more based on the JBI critical appraisal tools, as seen in Tables 2 and 3. All included studies were rated as moderate to high quality based on the characteristics of the included studies in Table 4. In conclusion, all studies were deemed fit to be included in the review.
 |
Table 2 Quality Appraisal of Studies Included in the Systematic Review Using Joanna Briggs Institute (JBI) for Case reports9 |
 |
Table 3 Quality Appraisal of Studies Included in the Systematic Review Using Joanna Briggs Institute (JBI) for Case series10 |
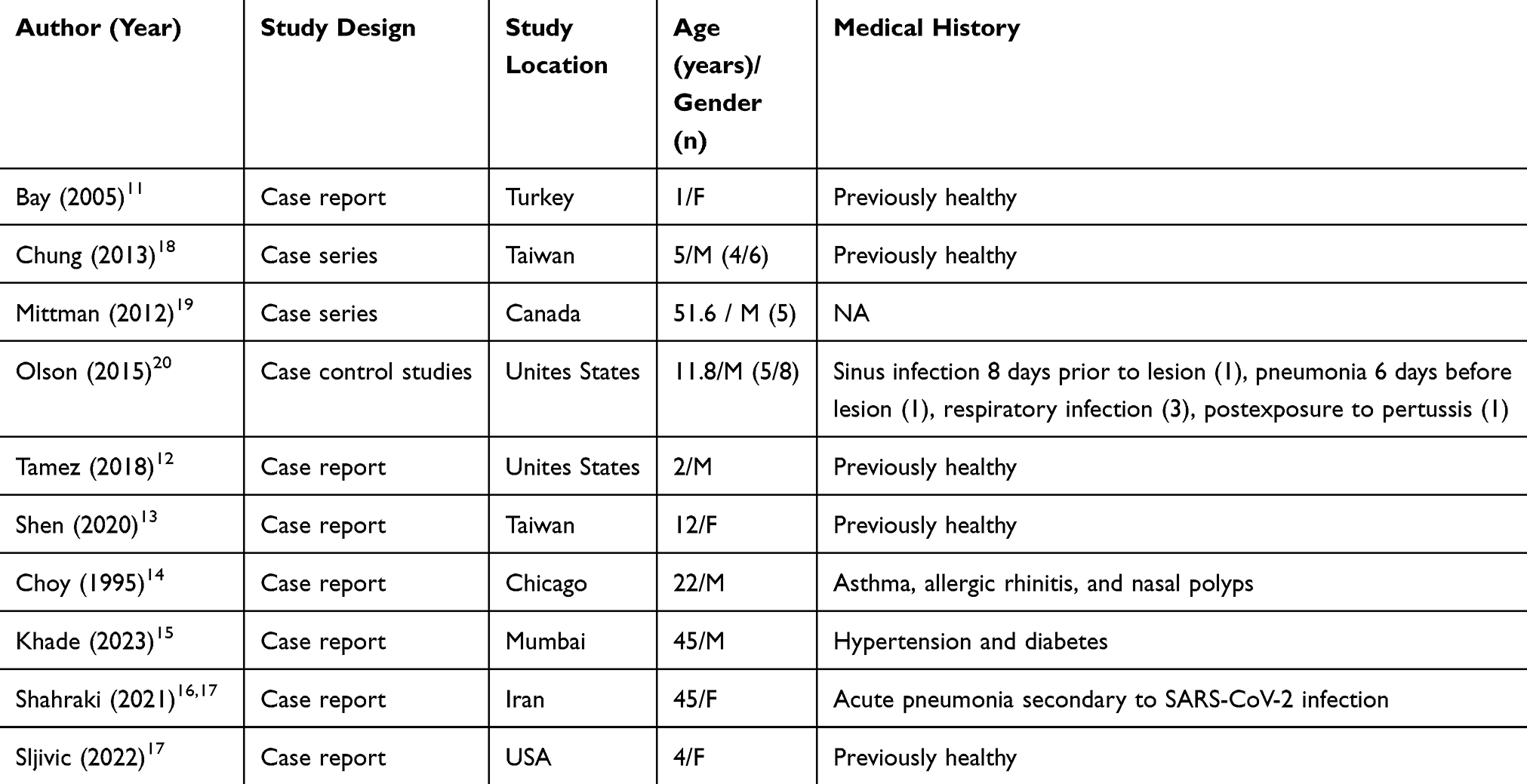 |
Table 4 Characteristics of the Included Studies |
Virus-Induced Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis
The results of the included studies were summarized in Table 5. This review found a case of varicella infection associated with SJS, as stated by Bay et al.11 The 12-month-old girl child present with disseminated symmetric, erythematous macules, papules, and vesicles on the head, trunk, extremities, and scalp of the patients. Moreover, blisters and crusted necrotic lesions had developed on the oral mucosa, trunk, and particularly on the flexural part of the extremities, typical of SJS that involves membrane and skin. The study by Chung et al12 provided insights into manifestations of coxsackie virus A6 (CVA6) infection-induced SJS diagnosed by real-time PCR. All the children presented with multiple to widespread central purpuric atypical target-like lesions on their limbs, faces, and trunks in the early stages, which then progressed to large blisters with purpuric bases at the maximal stage, along with mild to moderate lip erosions. All children also had systemic symptoms, including fever, sore throat, abdominal pain, vomiting, and diarrhea. All patients received only supportive treatments, and two patients received systemic corticosteroids. All six patients recovered within 1–3 weeks without complications, with the mean hospitalization duration being 14 ± 4.43 days.
 |
Table 5 Results of the Studies |
The study by Olson et al13 involved one case of a 16-year-old male with herpes simplex virus (HSV)-associated SJS, proven by PCR on an oral swab. The child was also positive for mycoplasma pneumonia, diagnosed by throat-swab PCR. He had mucositis in the ocular, oropharyngeal, and genital areas and presented with pneumonia and mild skin lesions. The child received amniotic membrane grafting to the eyes and recovered during hospitalization over 9 days. This review also found five reported cases of confirmed HIV-induced SJS/TEN as stated by Mittman et al.14 The patients had generalized pruritic maculopapular rash that became confluent with some desquamation, blistering in mouth, and conjunctivitis.
The study by Tamez et al15 revealed a case of SJS-associated influenza B virus infection in a 2-year-old boy who manifested prodromal symptoms such as fever, congestion, rhinorrhea, myalgia, and a progressive pruritic facial eruption. Over the next few days, he developed pink, annular, edematous papules and plaques on his face, trunk, buttocks, and extremities, many with dusky, violaceous centers, which became widespread. In this case, there was no genital or palmoplantar involvement. On the other hand, the study by Shen et al16 evaluated a case of a 12-year-old girl with toxic epidermal necrolysis (TEN) induced by human herpesvirus 7, diagnosed with PCR and lymphocyte transformation test. The girl presented with prodromal symptoms such as fever and generalized malaise. Over the next 5 days, she started to develop oral and ocular mucosal erosions, and violaceous macules with dusky red centres and blisters emerged on her face, trunk, and limbs, covering approximately 60% of her total body surface area. The patient was treated with tumor necrosis factor (TNF)-alpha inhibitors and steroids, and she recovered with sequelae of pterygium and post-inflammatory hyperpigmentation.
According to a study by Khade et al,17 a 45-year-old man with several fluid-filled lesions on his upper and lower extremities and rough spots in his mouth for three days had a case of COVID-19 infection linked to SJS. Before lesions appear, patients report fever, lethargy, and burning eyes. Before the lesions appeared, the patient denied using any over-the-counter oral or topical medications. On the other hand, the study by Shahrakhi18 et al, A 45-year-old lady who had been prescribed azithromycin and naproxen for acute pneumonia caused by SARS-CoV-2 infection. She looked sick three days after taking the drug; she experienced photophobia, dysuria, ocular irritation, and macular rashes on her trunk and limbs. An ophthalmological examination revealed that both eyes had a complete epithelial defect. After the evaluation revealed that the patient had Stevens-Johnson syndrome, they were admitted to the hospital for systemic, ocular, and medical support. Over three weeks, the patient’s health improved and she recovered from life-threatening problems caused by COVID-19 and SJS. However, she still had ocular complications, such as corneal scarring, irregularity in the margin of her eyelid, and destruction of her meibomian glands.
The 4-year-old girl in the Sljivic et al19 study had a papular rash on her legs that got worse over time and expanded to her face, trunk, and genitalia. The patient’s COVID-19 test result was positive. She eventually recovered completely after receiving therapy with intravenous immunoglobulin (IVIG) and IV methylprednisolone. The importance to recognize the vast range of dermatologic manifestations in COVID-19 patients is highlighted by this instance.
Discussion
Stevens-Johnson Syndrome (SJS) and its more severe form, Toxic Epidermal Necrolysis (TEN), are rare yet serious mucocutaneous reactions characterized by widespread skin detachment and mucosal erosions. There were some reported cases of SJS/TEN that were induced by bacterial infections, such as Streptococcus, meningococcus, and Mycoplasma pneumoniae.5,6,13 While primarily attributed to adverse drug reactions, emerging evidence also suggests viral infections, including HIV, HSV, influenza virus, varicella virus, COVID-19, and coxsackievirus, may also significantly contribute to their development.11–16
This review identified six young patients with SJS affected by Coxsackievirus A6 infection, as reported by Chung et al.16 These patients exhibited blistering skin lesions typical of SJS, predominantly with mild erosions on the external lips. However, these patients lacked severe bleeding erosions on the inner lips or oral cavity mucosa involvement, typical in SJS.16 This can be an important clue for suspecting coxsackievirus-induced SJS/TEN. Histopathological findings of the patients also confirmed the SJS diagnosis. The findings were consistent with other studies showing granulysin, produced by CTLs or NK cells, as a key mediator of keratinocyte death in SJS/TEN.20,21 These findings suggest that coxsackievirus antigens provoke a robust immune reaction in the epidermis, leading to widespread mucocutaneous bullous reactions, often identified as apoptosis due to dysregulation in specific transmembrane protein pathways.4
Earlier studies noted a significantly higher incidence of drug-induced SJS/TEN in HIV-infected individuals compared to non-infected populations. In this review, Mittman et al reported cases of HIV-induced SJS/TEN.22,23 However, it was important to note that the patients also used drugs like nevirapine, trimethoprim/sulfamethoxazole, stavudine, and clarithromycin, which also might be associated with SJS/TEN. However, the study did not provide specific medication rates per SJS/TEN due to the small study size, preventing a conclusive causality assessment. In HIV patients, the incidence of Cutaneous Adverse Drug Reactions (CADR), including SJS, correlates with declining CD4 T-cell counts, highlighting immune system weakening. Research indicates elevated IgE levels in HIV patients can exacerbate CADR progression, including SJS, alongside further reductions in CD4 counts. HIV patients often exhibit a decline in interferon-γ producing (Th1 type) CD4 cells over time, with a concurrent increase in IL-4-producing (Th2 type) CD4 cells, consistent with SJS/TEN pathophysiology. Biopsies from HIV patients with CADR reveal infiltration of activated CD8 lymphocytes and cytokine production in the epidermis, increasing SJS-TEN risk.4,22,24
Additionally in this review, herpes simplex and herpesvirus 7 infections were identified as etiological factors for SJS/TEN, confirmed by PCR and lymphocyte transformation tests.13,16 Immune responses following these infections can sensitize the body, increasing susceptibility to severe drug reactions like SJS/TEN. This is due to cytokine/chemokine production, such as interferon γ (IFN-γ) that disrupts immune balance, facilitating drug-hapten presentation. Other factors include a conserved etiologic agent that interacts with drugs to form a virus-drug-host complex, potentially triggering SJS/TEN. Pathogen epitopes and drugs can induce T cell cross-reactivity, influencing immune balance and activating memory CD8+ T cells, implicated in SJS/TEN development.4
Furthermore, this review found cases of SJS/TEN associated with influenza B and varicella zoster virus (VZV) infections. This is due to presenting rapid progression and toxic appearances with facial-truncal eruptions of the patients that led to the diagnosis of SJS/TEN. Although rare as etiological agents of SJS/TEN, these viruses exact mechanisms in SJS/TEN development remain poorly understood.11,15
Although the terms “virus-triggered” and “virus-induced” SJS/TEN are often used interchangeably in the literature, our observations suggest that they may represent distinct pathogenic pathways. For example, drug exposure is frequently associated with HIV and herpes viruses, supporting the theory that viruses increase susceptibility to drug-induced reactions. Conversely, case reports of SJS/TEN associated with Coxsackievirus or influenza without concomitant drug administration suggest a direct viral cause. This overlap highlights the importance of using the correct terminology and further research to clarify whether specific viruses may serve as a cause per se or primarily trigger immune reactions to drugs. The limitations of this systematic review include the challenge of distinguishing infectious versus medication-induced SJS, particularly with concurrent medication treatments during viral infections. Additionally, the review’s limited number of studies restricts its generalizability and comprehensive understanding of virus-induced SJS/TEN. Further research is crucial to elucidate these complex interactions and clarify viruses’ roles in SJS/TEN pathogenesis. Nonetheless, this systematic review provides valuable insights into different manifestations of virus-induced SJS/TEN, contributing to current knowledge in the field.
Conclusion
Based on the available evidence, it is undeniable that virus infection plays a role in SJS/TEN formation. However, the interaction between viral infection and SJS/ TEN is not fully understood and the underlying mechanism needs further investigation. An awareness of the risk of this virus induced SJS is needed especially in epidemic areas.
Acknowledgments
The author would like to express our thanks to Professor Stephen J Challacombe, Professor W M Tilakaratne, and Dr. Adi Idris, who have guided and provided direction regarding this systematic review.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Edmonson KG, Davis KJ. Fitzpatrick’s Dermatology.
2. Roujeau JC, Ghislain PD, Valleyrie-Allanore L. Stevens-Johnson Syndrome. In: Williams H, Bigby M, Diepgen T, Herxheimer A, Naldi L Rzany B, editors. Evidence-Based Dermatol.
3. Wasuwanich P, So JM, Chakrala TS, Chen J, Motaparthi K. Epidemiology of stevens-johnson syndrome and toxic epidermal necrolysis in the United States and factors predictive of outcome. JAAD Int. 2023;13:17–25. doi:10.1016/j.jdin.2023.06.014
4. Cheng L. Current pharmacogenetic perspective on stevens-johnson syndrome and toxic epidermal necrolysis. Front Pharmacol. 2021;12:588063. doi:10.3389/fphar.2021.588063
5. Imatoh T, Saito Y. Associations between stevens–johnson syndrome and infection: overview of pharmacoepidemiological studies. Front Med. 2021;8:644871. doi:10.3389/fmed.2021.644871
6. Léauté-Labrèze C, Lamireau T, Chawki D, Maleville J, Taïeb A. Diagnosis, classification, and management of erythema multiforme and Stevens-Johnson syndrome. Arch Dis Child. 2000;83(4):347–352. doi:10.1136/adc.83.4.347
7. Mj T, M C, B M. Nonimmediate allergic reactions induced by drugs: pathogenesis and diagnostic tests. J Investig Allergol Clin Immunol. 2009;1(1).
8. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;332–336.
9. Institute JB. The Joanna Briggs Institute critical appraisal tools for use in jbi systematic reviews: checklists for case reports: The Joanna Briggs Institute. 2019.
10. The Joanna Briggs Institute. The Joanna Briggs Institute critical appraisal tools checklist for case series. Joanna Briggs Research. 2018.
11. Bay A, Akdeniz N, Ö Ç, Kösem M, Öner AF, Doǧan M. Primary varicella infection associated with stevens-johnson syndrome in a Turkish child. J Dermatol. 2005;32(9):745–750. doi:10.1111/j.1346-8138.2005.tb00836.x
12. Chung WH, Shih SR, Chang CF, et al. Clinicopathologic analysis of coxsackievirus a6 new variant induced widespread mucocutaneous bullous reactions mimicking severe cutaneous adverse reactions. J Infect Dis. 2013;208(12):1968–1978. doi:10.1093/infdis/jit383
13. Olson D, Watkins LKF, Demirjian A, et al. Outbreak of Mycoplasma pneumoniae –associated stevens-johnson syndrome. Pediatrics. 2015;136(2):e386. doi:10.1542/peds.2015-0278
14. Mittmann N, Knowles SR, Koo M, Shear NH, Rachlis A, Rourke SB. Incidence of toxic epidermal necrolysis and stevens-johnson syndrome in an HIV cohort: an observational, retrospective case series study. Am J Clin Dermatol. 2012;13(1):49–54. doi:10.2165/11593240-000000000-00000
15. Tamez RL, Tan WV, O’Malley JT, et al. Influenza B virus infection and Stevens-Johnson syndrome. Pediatr Dermatol. 2018;35(1):e45–8. doi:10.1111/pde.13370
16. Shen MH, Liu MT, Chung WH, Lu CW. Toxic epidermal necrolysis induced by human herpesvirus 7 treated with a tumor necrosis factor-α inhibitor. J Dermatol. 2020;47(10):1179–1181. doi:10.1111/1346-8138.15493
17. Khade P, Shah A, Kharkar V. Stevens-johnson syndrome in adult patient secondary to COVID-19 infection: case report. JMIR Dermatol. 2023;6.
18. Shahraki T, Hassanpour K, Arabi A, Ansari I, Sadoughi MM. Corona virus disease 2019-associated Stevens-Johnson syndrome: a case report. BMC Ophthalmol. 2021;21(1). doi:10.1186/s12886-021-02033-y
19. Sljivic S, Pogson K, Williams FN, Nizamani R, King BT. Case Report COVID-induced toxic epidermal necrolysis in a 4-year-old female: a case report and literature review [Internet]. Int J Burn Trauma. 2022.
20. Chung WH, Hung SI, Yang JY, et al. Granulysin is a key mediator for disseminated keratinocyte death in Stevens-Johnson syndrome and toxic epidermal necrolysis. Nat Med. 2008;14(12):1343–1350. doi:10.1038/nm.1884
21. Stock AT, Jones CM, Heath WR, Carbone FR. Rapid recruitment and activation of CD8+ T cells after herpes simplex virus type 1 skin infection. Immunol Cell Biol. 2011;89(1):143–148. doi:10.1038/icb.2010.66
22. Spcec O. Drug-induced toxic epidermal necrolysis (Lyell syndrome) in patients infected with the human immunodeficiency virus. J Am Acad Dermatol. 2010;1(1).
23. Berthold R, Maja M, Ulrich S. Incidence of stevens-johnson syndrome and toxic epidermal necrolysis in patients with the acquired immunodeficiency syndrome in Germany. JAMA Dermatol. 2010;1(1).
24. Yunihastuti E, Alvina W, Teguh K. Drug hypersensitivity in human immunodeficiency virus-infected patient: challenging diagnosis and management. Asian Pacific Allergy. 2014;4(1).
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.