")
Back to Journals » Patient Preference and Adherence » Volume 17
Views on Suspected Adverse Drug Events in Older Adults with Chronic Conditions: A Qualitative Study
Authors Wang D , Meng X , Liu L , Wang A
Received 13 June 2023
Accepted for publication 10 August 2023
Published 18 August 2023 Volume 2023:17 Pages 2051—2061
DOI https://doi.org/10.2147/PPA.S420620
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Daqiu Wang,1 Xin Meng,2 Lei Liu,1 Aiping Wang2
1Liaoning University of Traditional Chinese Medicine, Shenyang, People’s Republic of China; 2The First Affiliated Hospital of China Medical University, Shenyang, People’s Republic of China
Correspondence: Aiping Wang, Department of Public Service, the First Affiliated Hospital of China Medical University, No. 155, Nanjing North Street, Heping District, Shenyang, Liaoning Province, People’s Republic of China, Tel + (0086)02483282288, Fax + (0086)02483282288, Email [email protected]
Purpose: To explore how elderly patients with chronic conditions identify and cope with suspected adverse drug events (ADEs) in northern China with the aim of encouraging the elderly to participate in medication safety monitoring.
Patients and Methods: A purposive sampling method was adopted to select 15 elderly patients with chronic conditions from a medical center in northern China for semi-structured-interviews, and the data were collated and analyzed through thematic framework analysis.
Results: Five major themes and 12 subthemes were refined, namely (1) lack of knowledge: poor awareness of the medications and ambiguous knowledge of ADEs, (2) barriers to identifying suspected ADEs: unawareness and uncertainty, seeking alternative explanations, and limited access to information, (3) the basis for identifying suspected ADEs: time cues and actively seeking communication (4) coping with suspected ADEs: cope with it themselves, not talking to the health care provider on their own initiative and actively seeking communication, and (5) expectations: desire for more reliable information and hope to be safeguarded for medication safety.
Conclusion: Due to the lack of relevant knowledge and limited access to information, the elderly were limited in identifying suspected ADEs, but they were positive towards participating in medication safety monitoring and hoped to obtain reliable medication information and detailed medication assessment by enhancing communication with medical professionals in order to achieve medication safety.
Keywords: the elderly, adverse drug events, medication safety, qualitative study
Introduction
In order to enable patients worldwide to access to safer medical care and achieve universal health coverage, the World Health Organization (WHO) has issued the Global Patient Safety Action Plan 2021–2030.1 The need to ensure the safety of each clinical procedure, with particular reference to “medication without harm” is clearly stated in the plan. According to the Annual Report on National Adverse Drug Reaction Monitoring issued by the National Centre for ADR Monitoring in 2020,2 the incidence of adverse drug events (ADEs) in older adults was 30.3%, higher than that in previous years. Older adults are susceptible to pharmacokinetic and pharmacodynamic changes and are more sensitive to drugs, which will increase the risk of drug interactions and ADEs.3 An ADE is defined as “untoward occurrences following exposure to a drug but not necessarily caused by the drug”,4,5 and ADEs in older adults can lead to unplanned drug-related hospital admissions6 and increase the risk of geriatric syndrome and significantly decrease the quality of life,7 and even cause death.8 Therefore, it is necessary to pay more attention to the safety of medication use in elderly population.
In China, medical institutions and manufacturers are the main bodies for ADR reporting to the ADR monitoring system. According to data in 2020 China’s ADR monitoring system, reports by physicians, pharmacists, nurses from medical institutions accounted for 85.4%, reports from manufacturers accounted for 14.5% and reports from individuals accounted for only 0.1%.2 However, several studies have shown that health care professionals (HCP) tend to underestimate the incidence and severity of ADEs among their patients, especially symptomatic ADEs and unalarming ADEs, which can affect quality of life.9–11 Over the past 10 years, a number of EU countries have established spontaneous reporting systems that provide opportunities for the public to report suspected ADEs directly,12–14 which demonstrated that patients’ participation in pharmacovigilance was vital and beneficial for the post-marketing safety surveillance of medicines. A systematic review15 has suggested the value of patient reporting to the pharmacovigilance system. Patient reports can add new information and views on ADEs different from the HCP reports, which can reinforce safety signals and increase the knowledge about ADEs.
Although older adults are vulnerable to ADEs, especially those who are non-hospitalized and taking regular medications without safety monitoring from HCP, older patients often have difficulties in recognizing a symptom as an adverse effect of their drugs.16 Therefore, it is vital to understand how the older patients identify and cope with suspected ADEs, which can help to improve medical safety for older patients, as well as to enhance the satisfaction of elderly patients with their drug therapy. The aim of this study was to explore the perspectives and experiences of coping with suspected ADEs in elderly patients with chronic diseases in northern China, in order to encourage elderly patients to participate in medication safety monitoring.
Materials and Methods
This was a descriptive qualitative study which was reported following the Consolidated Criteria for Reporting Qualitative Research (COREQ).17 The study complied with Declaration of Helsinki and was approved by the Medical Science Research Ethics Committee of the First Affiliated Hospital of China Medical University (No.: 2018–266).
Settings and Participants
A purposive sampling method was adopted to select the elderly patients with chronic diseases who consulted at the geriatric outpatient department of the First Hospital of China Medical University which is one of the largest public hospitals in northern China from July 2018 to March 2020. The inclusion criteria were as follows: (1) those aged 60 years or above, (2) those with at least one chronic non-communicable disease, as diagnosed by physicians, and (3) those may experience suspected ADEs with personal experience of taking regular medications (for more than 4 weeks), including prescription, over-the-counter, and health products. The exclusion criteria were as follows: (1) those with serious physical illnesses that prevented them from participating in the study, and (2) those with mental or cognitive impairment and those who were unconscious and unable to communicate normally. To ensure the participants were representative and typical, the first researcher selected the sample based on the strategy of maximum variation in terms of gender, education, different ages and occupations before the interviews. This sampling strategy enables the researcher to obtain a broad perspective and experience from the patients. Recruitment of participants was continued until data saturation was achieved.
Data Collection
Based on Lazarus and Folkman’s stress and adaptation theory,18 a semi-structured interview outline was developed by means of literature review and group discussions which consisted of one academic professor and two Ph.D. candidates, all of whom had experience of qualitative studies. After interviewing two participants, the formal semi-structured interview outline was formed, as illustrated in Table 1. The interviews took place in a private room of the outpatient department to ensure a comfortable and quiet environment, to facilitate recording, and to protect the privacy of the interviewees. The required equipment was prepared before the interview, including project introduction, characteristics questionnaire used to collect demographics information (age, gender, education level, and occupation before retirement) and disease-related variables (diagnosed chronic diseases by physicians), medications that they are taking regularly, interview outline, notebook and pen, and a recorder with sufficient power. Interviewees were informed about the purpose prior to the interview, signed an informed consent (including consent to participate in this study and consent to publication of anonymized statements) and the recordings were started with their permission. After collecting demographic information about the interviewees, a face-to-face in-depth interview was conducted by the first author according to the interview outline, and non-verbal information such as expressions, body movements, sighs, or longer pauses was recorded in the notebook. During the interview, attention was paid to the interviewee’s situation. When the interviewee felt unwell or tired, the interview was suspended immediately. If the interviewer could not continue after the break, the interview was continued on another day. The interviews lasted 25–60 mins.
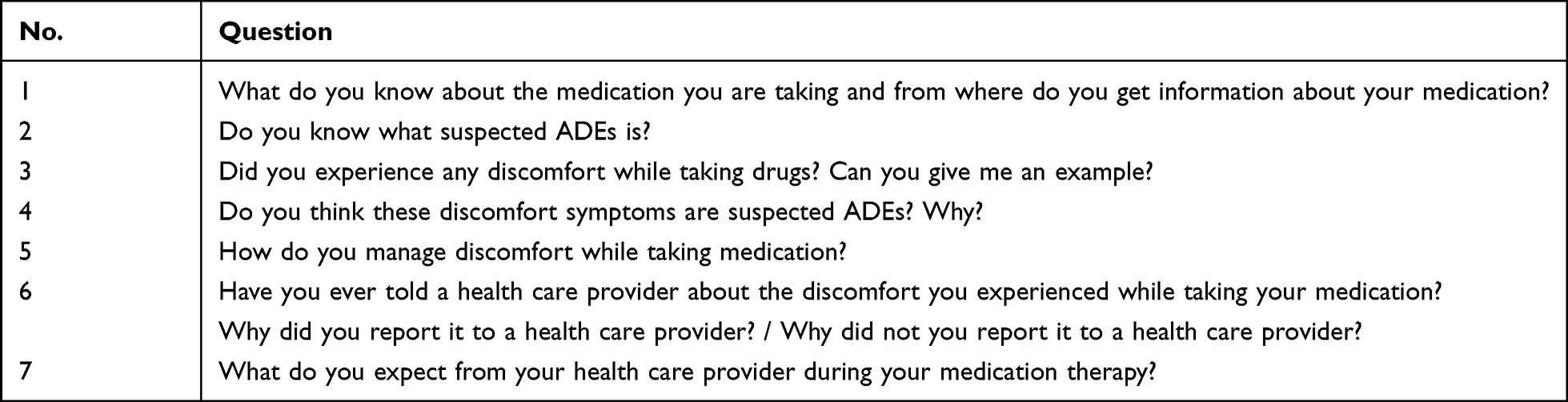 |
Table 1 Interview Outline |
Data Analysis
The thematic framework analysis was used to analyze the data.19–21 The specific steps were as follows: (1) familiarization: within 24 h of the interview, the audio recordings were transcribed verbatim into text and combined with the interviewers’ field notes to form an interview profile. The interview data were imported into Microsoft Word for management, named by the date of the interview and the interviewee number. The true names of the interviewees did not appear in the interview data and were replaced by numbers, such as P1 and P2. After the interview text was transcribed correctly, two researchers (Wang and Meng) analyzed the data separately by reading the data repeatedly in an immersive manner, and constructing a thematic framework which is based on “Lazarus and Folkman’s stress and adaptation theory”, that is, knowledge of ADE, identifying suspected ADEs, and coping with suspected ADEs. (2) Coding of data: duplicates were created in Microsoft Excel, corresponding themes were marked in different colors in the original data through reading and understanding of the original data, and memos were created, including key information provided by interviewees, ideas generated in the process of reading interviewees’ data and phrases or sentences in the interviewee’s original words. The two researchers independently extracted data to develop initial themes and sub-themes; and next, they discussed the findings and agree on the preliminary themes and sub-themes. (3) Indexing of the data according to the theme: After the original data were marked, data with similar content or the same nature were combined for further analysis of the theme. (4) Summarizing and synthesizing data: a theme table was created in Microsoft Word to present the theme, subthemes and supporting quotes, and the original words of the interviewees were quoted as much as possible for key words or expressions and a descriptive analysis was conducted. (5) Interpreting: After the data were collated and analyzed, the interviewees were quizzed about relevant opinions on the analysis and conclusion of the text data.
Rigor
Several strategies were applied to ensure trustworthiness of the research. To ensure the credibility of the data, the researchers used prolonged participation, member checking and peer debriefing. Prior to conducting the study, the first researcher (Wang) worked as a nurse in the geriatric outpatient department and had regular interactions with the participants. Afterwards, the interviews were transcribed verbatim and the transcribed text was sent back to the participants for verification. The researchers also analyzed and checked the true feelings of the participants through observations and field notes. Furthermore, the researchers asked a panel of experts to review the transcripts, extracted codes, and themes in order to check the dependability and conformability of the gathered data. Finally, all of the findings were taken from the participant data and supported with brief quotes in each theme.
Results
Participant Characteristics
A total of 15 elderly patients with chronic diseases, aged 61–81 years, eight males and seven females, were interviewed in this study. Two to nine chronic diseases were diagnosed by physicians in these interviewees, and 80% of the interviewees took five or more medications. Characteristics of the 15 interviewees is summarized in Table 2.
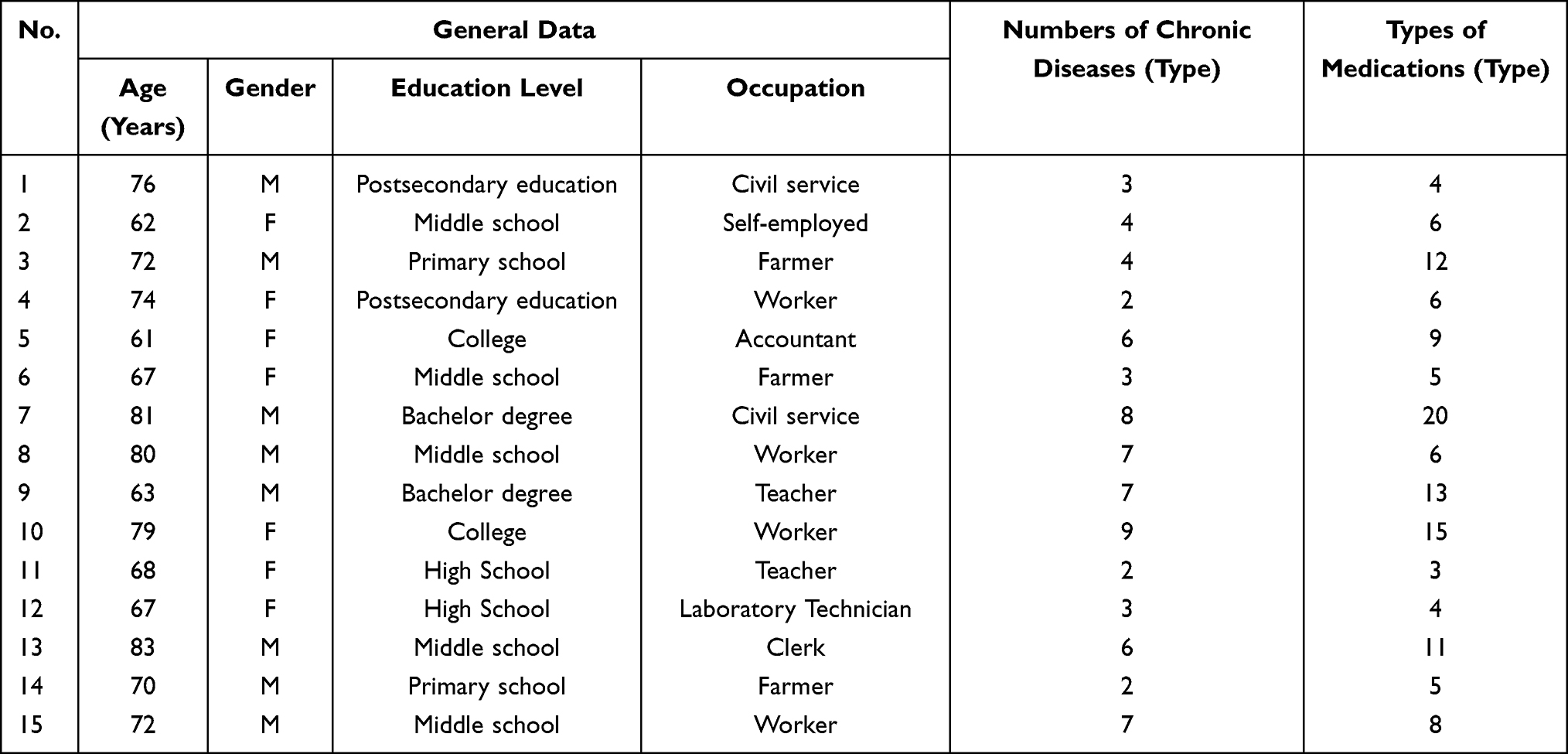 |
Table 2 Demographic Characteristics of the Participants |
Perspectives and Experiences of Coping with Suspected ADEs in Elderly Patients
The interview data for 15 elderly patients with chronic diseases were analyzed and grouped into five major themes. Figure 1 shows five major themes and 12 subthemes that arose from patient views on suspected ADEs.
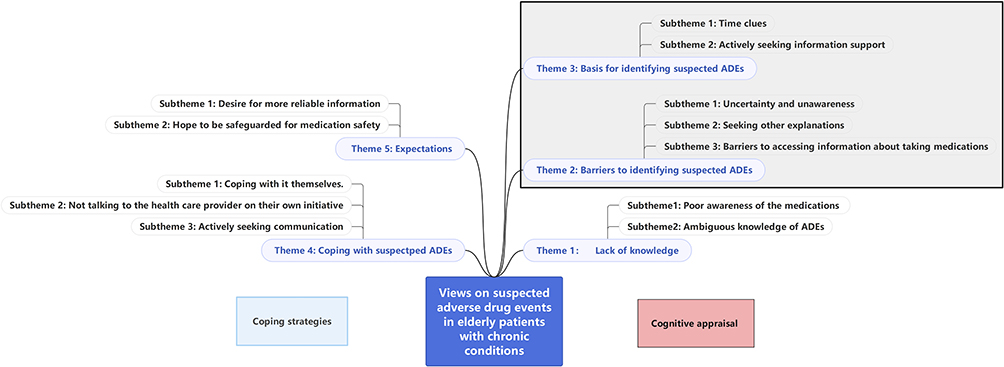 |
Figure 1 Older adults’ views on suspected ADEs. |
Theme 1: Lack of Knowledge
Subtheme 1: Poor Awareness of the Medications They Have Taken
Most of the interviewees did not have a clear idea of the medications they were taking (including usage, dosage and side effects), some of which were purchased by themselves or recommended by salesman in pharmacy.
I didn’t know what medicine I should take, so I just went to the pharmacy and told the clerk that I have discomfort in which part and then bought the medicine she recommended to me. (P6)
Some interviewees entirely relied on their caregivers for daily medication management and were neither aware of the type of medications they were taking nor the side effects of the drugs. Some interviewees fully trusted the doctor’s diagnosis and treatment and had no doubt about the medication prescribed by the doctor, as P9 argued that
I take medications as the physician prescribed, including the dosage and the manner instructed by the physician. I don’t enquire the details, because it doesn’t make sense. I can’t stop taking the medication, so I have to take them anyway.
The interviewees mentioned the heavy burden due to taking medications because they did not understand the purpose and significance of their medication; they felt hopeless as for their lives need to be sustained by medication forever. “It’s annoying to take medication every day and there is no hope for the future” (P9).
Subtheme 2: Ambiguous Knowledge of ADEs
In addition to lack of clarity about the drugs they were taking, the interviewees also had some limitations in their knowledge of ADEs. Most of the participants quoted the Chinese proverb “medicine is poisonous in three parts” to explain the adverse drug events, and agreed that there are certain side effects of drugs. Some participants described suspected ADEs as uncomfortable symptoms they perceived when taking medications. However, the respondents still had a certain lack of knowledge about ADEs. On the one hand, some interviewees thought that the side effects of drugs only exist in chemical drugs, and that Chinese medicine or proprietary Chinese medicine are safe and no adverse drug events would occur in the process of taking Chinese medicine; on the other hand, some interviewees thought that the side effects of drugs only occur when they started taking the drugs, and no adverse drug events would occur in long-term drugs, as P9 said: “I have been taking this medicine for years, what side effects can I experience now? If there are side effects, I have already suffered from them!”
Theme 2: Barriers to Identifying Suspected ADEs
Owing to “uncertainty and unawareness”, “seeking alternative explanations”, and “limited access to information”, it was difficult for interviewees to determine whether the discomforts they experienced while taking medication were suspected ADEs.
Subtheme 1: Uncertainty and Unawareness
Most participants reported that they experienced some discomfort while taking medications, but were unsure whether their perceived discomfort was an adverse drug event. Firstly, the lack of drug-related knowledge decreased the participants’ confidence in identifying suspected ADEs, as P6 mentioned “I do have fatigue while taking medication, but I am not really sure about whether it is drug-related.” Secondly, doctors usually paid too much attention on the usage of drugs and disease control in the process of drug treatment without mentioning drug-related side effects and safety monitoring, which lead to patients not paying much attention to the occurrence of adverse drug events in their daily life,
every time the doctor asked me about blood pressure, blood lipid, how the drugs have been taken, but never asked me whether I had any adverse event. I didn’t pay attention and I really don’t know. (P2)
The third reason is that the participants did not pay much attention to the discomfort during the medication process because the discomfort was relieved on its own, or was relieved by self-medication, such as: “I use cloisonne when I am constipated, so I don’t think about whether my constipation is caused by the medication or not” (P7); the fourth reason is that the patients were taking multiple medications at the same time and it was difficult to determine which medication caused the adverse event, as P7 argued that “I took so many kinds of medications, and I don’t know which drug is related to the AE.”
Subtheme 2: Seeking Other Explanations
When determining adverse drug events, interviewees usually did not directly associate the perceived discomfort to the side effects of the drug, but first sought other explanations, such as attributing the discomfort to their old age, thinking that the discomfort was due to the physical deterioration that occurred with age. Some interviewees also believed that their discomfort was related to mental health or personal lifestyle. In addition, participants attributed the discomfort to their suffered diseases or the status of a specific period, such as P1 mentioned “I started to forget after the last stroke, my memory has been declining”, and P5 argued that “I have insomnia. I can’t sleep and I wake up easily. I always thought it was because of menopause, and it is normal to have poor sleep during menopause. I never considered insomnia was caused by the side effects of the medication I was taking” and “I have diabetes, sometimes when I eat less or exercise more, my blood sugar becomes unstable.” (P8)
Subtheme 3: Barriers to Accessing Information About Taking Medications
Interviewees mentioned that limited access to information resulted in a lack of drug-related knowledge and difficulties in the identification of suspected ADEs. Half of the interviewees said that they never read the drug instructions and had difficulty in reading and understanding them. One reason is that due to the poor vision of the elderly and too small font on the usage instructions, the elderly felt inconvenienced and did not read the accompanying consumer medication leaflets, “the words are too small to read and I have to take the glasses. Laborious” (P9). Another reason is that the contents covered in the leaflets were too complex, with many technical terms which they have difficulties in understanding, so that “I stopped reading them if I couldn’t understand them” (P6). A number of interviewees argued that physicians and patients paid more attention to the usage and dosage of the drugs for either the drugs purchased by themselves in pharmacies or prescribed by doctors, but did not discuss much about the side effects and the possible ADEs that might occur while taking the medications. Furthermore, due to insufficient time to communicate with physicians, the relevant information was not sufficiently obtained. “The physician didn’t tell me, and I didn’t ask either” (P8).
Theme 3: Basis for Identifying Suspected ADEs
Interviewees who experienced symptoms of discomfort during medication would determine whether they were drug-related through two ways: “time clues” and “actively seeking information support.”
Subtheme 1: Time Clues
Interviewees determined the suspected ADEs based on “time cues”, such as the AEs occurred after taking the drug or the symptoms disappeared after stopping the drug. What’s more, the “time cues” made them more confident about their judgment. Interviewee P4 mentioned that “I develop the discomfort after taking this drug.” And interviewee P6 argued that “I did not have this feeling anymore after stopping the drug.”
Subtheme 2: Actively Seeking Information Support
Interviewees said they would seek to obtain information to support their judgment when discomfort symptoms appeared. If a suspected ADE occurred, some interviewee would directly tell the physician about the experience of discomfort to have a definite determination from the physician. Interviewees would identify by reading the package insert or checking the relevant information with the help of the Internet.
I felt weak, and I had hypokalemia indicated by this physical examination. I browsed Baidu and learned that the drug I was taking would lead to decreased serum potassium, what’s why I feel weak…. (P5)
Interviewees actively communicated with others, especially patients and referred to others’ experiences of medication and discomfort symptoms when experiencing discomfort symptoms, “I knew a patient who used to take this medication and had this symptom, and we once discussed about it” (P2)
Theme 4: Coping with Suspected ADEs
Subtheme 1: Coping with It Themselves
Interviewees would first seek non-pharmacological remedies on their own to solve their perceived symptoms and if non-pharmacological measures were ineffective, some interviewees would self-medicate without consulting a physician to relieve their symptoms. P7 expressed that:
Sometimes my joints hurt badly, so I take some painkillers on my own, but taking too many painkillers resulted in stomach pain and my stomach hurt, so I take some yeast tablets. What else can I do? ….
Interviewees often chose to accept and tolerate their perceived discomfort when balancing drug efficacy with side effects. For instance, P3 argued that
the medicine has to be taken, I dare not think much about it, I think I will slowly be adapting to these symptoms; when the symptoms are severe, I take some else medicine to control them until they are relieved….
Subtheme 2: Not Talking to the Health Care Provider on Their Own Initiative
Most of the interviewees stated that they would not talk to their physicians on their own initiative about the presence of uncomfortable symptoms or information about self-medication. Because, on one hand, they were afraid of disturbing the physicians and increasing their burden, considering the busy work schedule of health care providers. P10 believed that “He is quite busy, so it’s unnecessary to tell him.” P7 argued that “The physician is too busy and has limited communication time, I understand, and I am unwilling to disturb him.” On the other hand, some interviewees mentioned that the reason they would not actively talk to physicians was the lack of opportunities and paths to facilitate communication with medical staff. For example, “Every month when I come to prescribe drugs, the physicians briefly communicate with me. Since the time is also limited, we just communicate briefly” (P7). In addition, some interviewees felt that it was not necessary to tell their physicians about the drugs that they had purchased on their own without consulting their physicians. Two interviewees stated that they would not take the initiative to tell the physician if the suspected ADE was not serious; they would actively communicate with the medical staff when the symptoms reached an intolerable level or cannot be handled by themselves. “Because it’s not necessary and it’s not serious, I can manage it myself and I will tell my physician when it is serious” (P9).
Subtheme 3: Actively Seeking Communication
There are three main motivations for patients to actively communicate with their physicians about medication information and discomfort during medication administration. Interviewees would talk to their doctor and seek help when the discomfort had become “intolerable” and seriously affected their daily life. Three interviewees mentioned that they actively communicated with their physicians about their medication and discomfort because they “hoped to be known”, and they hoped to seek the attention and help of physicians by strengthening their communication with them to find the cause of their discomfort symptom. Also, they hoped that physicians would pay more attention to their health status to give them feedback. “I do have this symptom, but I don’t know if it is drug-related, I think if I reported it, and then the physician can tell me whether it is or not”, (P2). The interviewees had the sense of relief when the physician determined that there was a correlation between the symptoms and the medication.
After taking this drug, I felt heartburn, very serious. I felt very bad all day. I was afraid that I was suffering from some other condition, and then I decided to talk to the physician. The physician told me it might be related to the medicine and asked me to stop the medicine. I was relieved to hear that the symptoms were caused by medication, and although I used to have stomach ulcers before, but now I’m obviously feeling better after I stopped the drug. (P7)
Another interviewee mentioned that he would actively communicate with physicians when he was unable to judge whether the discomfort symptoms experienced were suspected ADEs, expecting that active reporting could draw the attention of physicians and other patients, to raise public awareness of suspected ADEs.
I found it difficult to distinguish which were the side effects. I did have symptoms, but I don’t know whether they were symptoms or side effects. I think I should tell my physician, maybe someone else is also concerned about it. (P5)
Theme 5: Expectations
Subtheme 1: Desire for More Reliable Information
During the interviews, the interviewees mentioned that they would like to participate in the decision-making of the treatment regime and medication safety monitoring, although they obtained relevant information about the drug through reading the package insert, the Internet and their relatives and friends. Besides, they needed professional and reliable guidance from their physicians in the process of taking medications. “I wish the physician can tell me in detail, so I could observe myself at home”, (P2). “I still want to communicate more with the physician and I want the physician to tell me about my medication precautions rather than reading the instructions, which I think should be part of their work. But they are too busy to attend to, I understand, “(P7).
Subtheme 2: Hope to Be Safeguarded for Medication Safety
Interviewees would like to get more attention from their health care providers during medication, such as receiving regular and detailed medication assessments to ensure their medication safety.
If you ask me directly whether I have experienced any adverse drug events, indeed I cannot figure it out, but if you list several symptoms for me to choose, I can choose as I have adverse reactions indeed; this form (list of symptoms) is preferable to the question that if you have any adverse reactions. (P8)
P5 mentioned in the interview, “It’s good to be instructed in the details (by medical staff), it would be nice to be inquired every visit.”
Discussion
In this study, from the perspective of elderly patients with chronic diseases, the ADEs they experienced during medication, as well as their views and coping with suspected ADEs were explored. It was learned from the study that patients were positive and willing to participate in medication safety monitoring. However, due to lack of medication knowledge, the elderly patients with chronic diseases had poor awareness of ADEs. In addition, due to untimely communication and obstructed channels with healthcare professionals, non-hospitalized elders are not informed about how to participate in medication safety monitoring, and when they experience uncomfortable symptoms, they often cope with suspected ADEs on their own, increasing the potential for medication risk.
Due to insufficient ability and limited access to information, the elderly lacked knowledge about taking medication, both the medication they were taking and the goals and significance of treatment, which led to many problems in taking medication, such as bad medication experience and unsatisfactory medication compliance. These findings are consistent with previous studies,22,23 which indicated insufficient knowledge about medications and medication-related problems in the public, especially the elderly. Moreover, lack of reliable medication knowledge can lead to poor awareness of medication safety monitoring in the elderly, which will decrease confidence in recognizing and identifying ADEs, as demonstrated in a prospective study involving 310 elderly veterans.24 Therefore, a variety of health education methods should be integrated into the clinical practice to provide more reliable and specialized information about medication safety monitoring for the elderly, to improve the medication literacy of patients and then to encourage them to participate in ADE monitoring, so as to ensure the medication safety.
Our results showed that patients actively sought referable information support to help them identify suspected ADEs and they also had the willingness to actively participate in medication safety monitoring. Furthermore, the value of patient involvement in pharmacovigilance was confirmed in the previous systematic review.15 Direct reporting of suspected ADRs by patients has been incorporated in the pharmacovigilance system in many countries, where patients provide first-hand information on the experience of drugs taking and additional information about the impact of ADEs on the daily life of patients, which can optimize the current pharmacovigilance system.15 However, elderly patients with chronic diseases have difficulties in identifying ADEs, which is one of the factors that prevent patients from reporting ADEs and is mentioned in a systematic review of factors affecting patient reporting of adverse drug reactions.25 Thus, it is essential to provide appropriate professional support to encourage patients to participate in medication safety monitoring.
In this study, it was revealed that when the interviewees were asked whether they have experienced any ADEs when they were taking medication, they preferred a symptom checklist than an open-ended question. Previous studies also demonstrated that a structured list was favorable for collecting detailed information about the patient’s medication and the ADEs experienced,26 and also made it easier to identify suspected ADEs, especially for older adults.16 Patients expected to obtain more specialized information about ADEs and other medication information from their physicians, and even needed the assistance of physicians in identifying ADEs. However, it was noted that insufficient communication between patients and healthcare providers was one of the barriers for patients to recognize and cope with ADEs. Patients’ coping with suspected ADEs increased the risk of medication due to inadequate communication time25 and poor communication between patients and healthcare professionals,22,23,27 such as passive listening27 and pessimistic attitude.22 Therefore, our findings suggested that it is necessary to make it easier for patients to report ADEs and enhance communication between patients and healthcare professionals so as to improve public awareness of ADEs and promote patient self-monitoring and spontaneous reporting of ADEs.
There were several limitations in this study. First, all interviewees were outpatients from one tertiary hospital, and the possibility of expanding the sample size and sample source to obtain more information could not be ruled out; second, this study explored the experiences of suspected ADEs in older people with chronic conditions from the patient’s perspective, however, during medication safety monitoring, the participation of doctors, nurses and pharmacists was also very important; further study is required to explore the perspectives of healthcare professionals to validate the findings of this study, and to provide information that can be used to adjust treatment regimes, to promote the participation of elderly patients with chronic diseases in safe medication monitoring.
Conclusion
Due to lack of relevant knowledge, elderly patients with chronic diseases have limited information about the drugs they are taking and as well as the adverse effects. Furthermore, the elderly had poor awareness about participating in medication safety monitoring due to limited access to information and problems in communication with healthcare professionals. However, the elderly had a positive attitude towards participating in medication safety monitoring and expected to obtain professional medication information and detailed medication assessment to ensure their medication safety. Therefore, for better medication safety in elderly patients, it is necessary to raise awareness of medications and their potential adverse drug events, as well as to encourage the elderly to participate in medication safety monitoring and reporting. Future research will focus more on projects to improve awareness of medications and common adverse drug events in the elderly, and to guide the elderly in monitoring and reporting of adverse drug events during their daily medicine taking.
Acknowledgments
We would like to express our gratitude to all the participants in the study for their useful input, and medical staffs in the geriatric department.
Funding
This study is supported by Basic Scientific Research Projects of Educational Department in Liaoning Province [grant numbers: LJKQR2021020].
Disclosure
The authors report no actual or potential conflicts of interest in this work.
References
1. World Health Organization. The Global Patient Safety Action Plan 2021-2030; 2021. Available from: https://www.who.int/publications/m/item/the-final-draft-of-The-global-patient-safety-action-plan.
2. National Centre for ADR Monitoring. National Adverse Drug Reaction Monitoring Annual Report (2020); 2021. Available from: http://www.cdr-adr.org.cn/center_news/202103/t20210326_48413.html.
3. Scondotto G, Pojero F, Pollina Addario S, et al. The impact of polypharmacy and drug interactions among the elderly population in Western Sicily, Italy. Aging Clin Exp Res. 2018;30(1):81–87. doi:10.1007/s40520-017-0755-2
4. Edwards IR, Aronson JK. Adverse drug reactions: definitions, diagnosis, and management. Lancet. 2000;356(9237):1255–1259. doi:10.1016/s0140-6736(00)02799-9
5. Asscher AW, Parr GD, Whitmarsh VB. Towards the safer use of medicines. BMJ. 1995;311(7011):1003–1006. doi:10.1136/bmj.311.7011.1003
6. Oscanoa TJ, Lizaraso F, Carvajal A. Hospital admissions due to adverse drug reactions in the elderly. A meta-analysis. Eur J Clin Pharmacol. 2017;73(6):759–770. doi:10.1007/s00228-017-2225-3
7. Rolfes L, van Hunsel F, Taxis K, van Puijenbroek E. The Impact of Experiencing Adverse Drug Reactions on the Patient’s Quality of Life: a Retrospective Cross-Sectional Study in the Netherlands. Drug Saf. 2016;39(8):769–776. doi:10.1007/s40264-016-0422-0
8. Cahir C, Bennett K, Teljeur C, Fahey T. Potentially inappropriate prescribing and adverse health outcomes in community dwelling older patients. Br J Clin Pharmacol. 2014;77(1):201–210. doi:10.1111/bcp.12161
9. Hakobyan L, Haaijer-Ruskamp FM, de Zeeuw D, Dobre D, Denig P. Comparing adverse event rates of oral blood glucose-lowering drugs reported by patients and healthcare providers: a post-hoc analysis of observational studies published between 1999 and 2011. Drug Saf. 2011;34(12):1191–1202. doi:10.2165/11593810-000000000-00000
10. Gurwitz JHFT, Harrold LR, Rothschild J, Debellis K. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA. 2003;289(9):1107–1116. doi:10.1001/jama.289.9.1107
11. Pedros C, Formiga F, Corbella X, Arnau JM. Adverse drug reactions leading to urgent hospital admission in an elderly population: prevalence and main features. Eur J Clin Pharmacol. 2016;72(2):219–226. doi:10.1007/s00228-015-1974-0
12. Inch J, Watson MC, Anakwe-Umeh S. Patient versus healthcare professional spontaneous adverse drug reaction reporting: a systematic review. Drug Saf. 2012;35(10):807–818. doi:10.1007/BF03261977
13. Avery AJ, Anderson C, Bond CM, et al. Evaluation of patient reporting of adverse drug reactions to the UK ‘Yellow Card Scheme’: literature review, descriptive and qualitative analyses, and questionnaire surveys. Health Technol Assess. 2011;15(20):1–234, iii–iv. doi:10.3310/hta15200
14. Florence van Hunse LH, Pal S, Olsson S. Experiences with adverse drug reaction reporting by patients: an 11-country survey. Drug Saf. 2012;35(1):46–50. doi:10.2165/11594320-000000000-00000
15. Inacio P, Cavaco A, Airaksinen M. The value of patient reporting to the pharmacovigilance system: a systematic review. Br J Clin Pharmacol. 2017;83(2):227–246. doi:10.1111/bcp.13098
16. Cahir C, Wallace E, Cummins A, et al. Identifying Adverse Drug Events in Older Community-Dwelling Patients. Ann Family Med. 2019;17(2):133–140. doi:10.1370/afm.2359
17. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int j Quality Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
18. Lazarus RS, Folkman S. Stress, Appraisal and Coping. New York: Springer; 1984.
19. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13:117. doi:10.1186/1471-2288-13-117
20. Liao X, Liu JP, Robison N, Xie YM. Framework analysis method in qualitative research. Chine j Integrated Traditional Western Med. 2014;34(5):622–626.
21. Ward DJ, Furber C, Tierney S, Swallow V. Using Framework Analysis in nursing research: a worked example. J Adv Nursing. 2013;69(11):2423–2431. doi:10.1111/jan.12127
22. Valinciute-Jankauskiene A, Loreta K. Qualitative Study of General Public Views towards Adverse Drug Reactions in Lithuania. Healthcare. 2021;9(3):303. doi:10.3390/healthcare9030303
23. Nicosia FM, Spar MJ, Stebbins M, et al. What Is a Medication-Related Problem? A Qualitative Study of Older Adults and Primary Care Clinicians. J Gen Intern Med. 2020;35(3):724–731. doi:10.1007/s11606-019-05463-z
24. Mosher HJ, Lund BC, Kripalani S, Kaboli PJ. Association of health literacy with medication knowledge, adherence, and adverse drug events among elderly veterans. J Health Commun. 2012;17(Suppl 3):241–251. doi:10.1080/10810730.2012.712611
25. Al Dweik R, Stacey D, Kohen D, Yaya S. Factors affecting patient reporting of adverse drug reactions: a systematic review. Br J Clin Pharmacol. 2017;83(4):875–883. doi:10.1111/bcp.13159
26. Foster JM, van der Molen T, Caeser M, Hannaford P. The use of questionnaires for measuring patient-reported side effects of drugs: its importance and methodological challenges. Pharmacoepidemiol Drug Safety. 2008;17(3):278–296. doi:10.1002/pds.1533
27. Parekh N, Gahagan B, Ward L, Ali K. ‘They must help if the doctor gives them to you’: a qualitative study of the older person’s lived experience of medication-related problems. Age Ageing. 2019;48(1):147–151. doi:10.1093/ageing/afy142
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.