Back to Journals » Infection and Drug Resistance » Volume 19
Vibrio Vulnificus-Induced Septic Shock Complicated by Necrotizing Fasciitis: A Case Report and Review of Clinical Characteristics
Authors Wang B, Liu S, Zhang P ![]()
Received 3 September 2025
Accepted for publication 3 January 2026
Published 26 February 2026 Volume 2026:19 564956
DOI https://doi.org/10.2147/IDR.S564956
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemant Joshi
Bojiang Wang,1 Shuzheng Liu,2 Peixun Zhang2,3
1Qingdao Medical College, Qingdao University, Qingdao, Shandong, People’s Republic of China; 2Department of Trauma and Orthopedics, Peking University People’s Hospital, Qingdao; Women and Children’s Hospital, Qingdao University, Qingdao, Shandong, People’s Republic of China; 3Department of Trauma and Orthopedics, Peking University People’s Hospital, Beijing, People’s Republic of China
Correspondence: Peixun Zhang, Email [email protected]
Background: Vibrio vulnificus is a halophilic marine bacterium capable of causing rapidly progressive septic shock and necrotizing fasciitis, particularly in immunocompromised individuals. Mortality rates remain high due to the fulminant nature of the infection and diagnostic challenges.
Case Presentation: A 70-year-old female with poorly controlled type 2 diabetes presented with fever and septic shock 48 hours after ingesting raw seafood. The clinical course was characterized by rapid deterioration, severe coagulopathy, and the development of extensive necrotizing fasciitis in the right upper limb. Vibrio vulnificus infection was confirmed via next-generation sequencing (NGS) on hospital day 6. Despite broad-spectrum antibiotic therapy and fluid resuscitation, surgical intervention was delayed until day 9 following multidisciplinary consultation. Intraoperative findings revealed extensive “dishwater” necrosis. The patient suffered from recurrent sepsis, graft failure, and deep vein thrombosis. Due to the rapid progression and delayed source control, the outcome was unfavorable, leading to discharge against medical advice.
Conclusion: This case underscores the high mortality risk associated with Vibrio vulnificus infection in immunocompromised individuals, particularly those with diabetes mellitus. Observations from this patient highlight that antibiotic therapy alone is often insufficient for necrotizing soft tissue infections. It is emphasized that in these high-risk populations, early recognition must trigger immediate, aggressive surgical debridement alongside antimicrobial therapy. Delays in surgical source control, even while awaiting molecular confirmation, can irreversibly compromise patient survival.
Keywords: vibrio vulnificus, septic shock, necrotizing fasciitis, surgical debridement, case report
Background
Vibrio vulnificus is a Gram-negative, halophilic bacterium that predominantly inhabits temperate and tropical marine environments, thriving in estuarine and coastal waters with temperatures ranging from 20°C to 35°C.1,2 Human infections typically arise from direct contact of open wounds with contaminated seawater or the ingestion of raw or undercooked seafood, particularly shellfish such as oysters.
The clinical spectrum of Vibrio vulnificus infection ranges from self-limiting gastroenteritis to rapidly progressive wound infections and primary septicemia. Sepsis caused by this pathogen is notorious for its fulminant clinical course. It has been cited as having the highest case-fatality rate of any foodborne pathogen, comparable to biosafety level 3 or 4 agents.3 Epidemiological data indicate that mortality is time-dependent: survival rates drop precipitously with delayed intervention. Studies suggest that mortality can reach 33% if antibiotic treatment is delayed by 24 hours and may approach 100% if delayed beyond 72 hours.4 This extreme lethality underscores the unforgiving nature of the infection.
Susceptibility is significantly amplified in individuals with underlying comorbidities, including chronic liver disease, diabetes mellitus, hemochromatosis, and immunosuppression. In these hosts, mechanisms such as iron overload and immune dysfunction facilitate rapid bacterial proliferation and systemic inflammatory cascades, leading to multi-organ failure.
Recent surveillance data suggest a rising global incidence of Vibrio vulnificus infections, driven partly by rising seawater temperatures associated with climate change which expand the pathogen’s geographical range. Beyond the human toll, this infection imposes a disproportionate economic burden on public health systems. Due to the requirement for prolonged intensive care, repeated surgical debridements, and potential amputations, Vibrio vulnificus is estimated to have the highest cost-per-case of any foodborne illness in the United States, with estimates exceeding $4 million per case in direct medical and quality-of-life costs.5
This case report describes a rapidly progressive Vibrio vulnificus infection complicated by septic shock and extensive necrotizing fasciitis in an elderly patient with poorly controlled diabetes. By detailing the diagnostic challenges and therapeutic timeline, we aim to enhance clinical awareness and emphasize the necessity of early multidisciplinary intervention to mitigate both the clinical mortality and the substantial public health burden associated with this pathogen.
Case Presentation
On September 26, 2024, a 70-year-old Chinese female presented to the emergency department of Peking University People’s Hospital (Qingdao), China, with a 24-hour history of fever and rapidly progressing gastrointestinal symptoms, including nausea, vomiting, and diarrhea.
Upon admission to the intensive care unit (ICU), the patient exhibited signs of septic shock. Vital signs were as follows: body temperature 36.8°C (after antipyretics), heart rate 93 bpm, respiratory rate 19 breaths/min, blood pressure 88/51 mmHg (maintained on norepinephrine), and oxygen saturation 95% on room air. Physical examination revealed generalized petechiae, notable cyanosis, edema, and marked tenderness localized to the right forearm and hand (Figure 1). Abdominal examination showed mild distention. Pulmonary auscultation revealed coarse breath sounds bilaterally.
 |
Figure 1 Clinical presentation on the day of admission showing extensive ecchymosis, cyanosis, and significant edema of the right forearm and hand. |
Her medical history included type 2 diabetes mellitus (HbA1c 9.3%) poorly controlled with metformin, and hypertension. Although initially denying seafood exposure, subsequent questioning revealed ingestion of raw seafood approximately 48 hours prior to symptom onset.
Initial laboratory investigations indicated severe infection, coagulopathy, and multiple organ dysfunction (Table 1). Immediate management involved aggressive fluid resuscitation and norepinephrine infusion (0.15–0.4 µg/kg/min) to stabilize hemodynamics. Due to progressive dyspnea and hypoxemia, the patient underwent endotracheal intubation and mechanical ventilation at 17:40 on the day of admission. Empiric broad-spectrum antimicrobial therapy was initiated with intravenous meropenem (1.0 g every 8 hours) and linezolid (0.6 g every 12 hours). Hydrocortisone sodium succinate (50 mg every 6 hours) was administered for septic shock management.
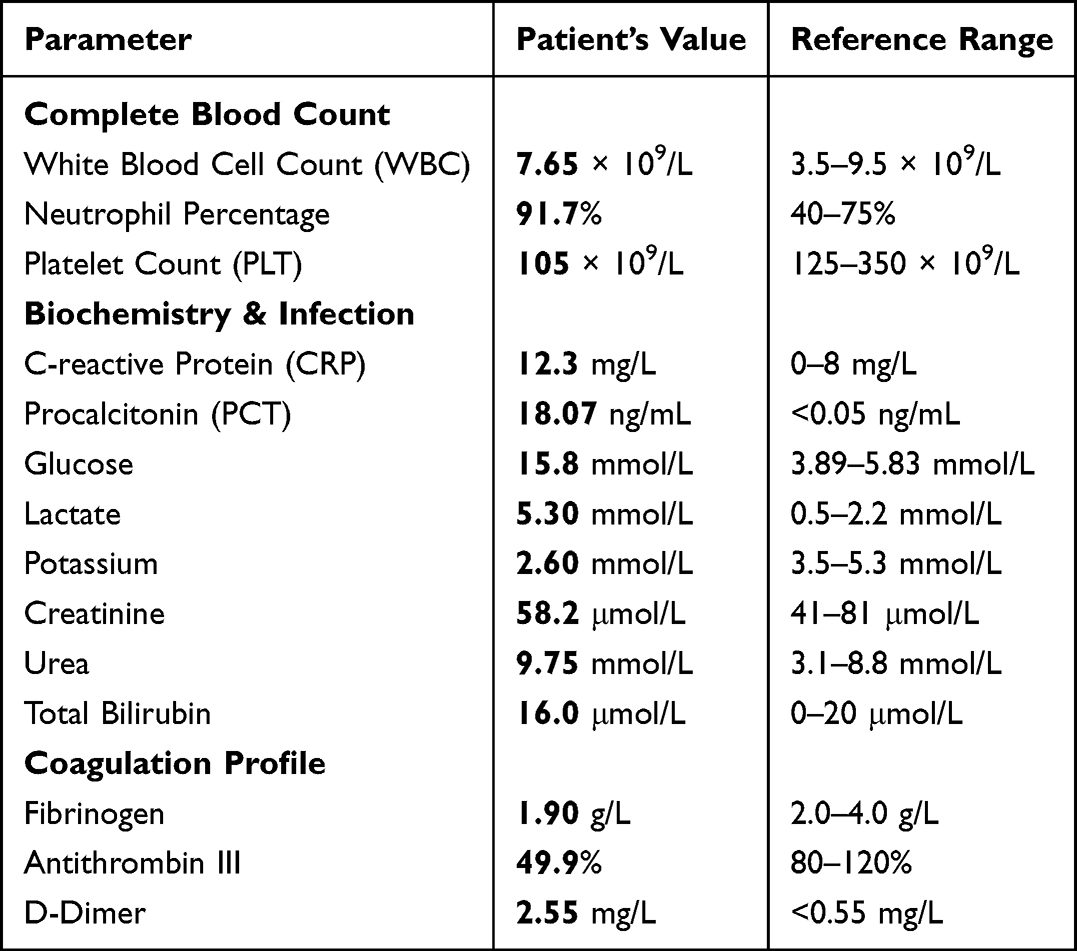 |
Table 1 Key Laboratory Parameters of the Patient Upon Admission (September 26–27, 2024) |
Despite initial hemodynamic stabilization, the local infection progressed. By day three, the right upper limb developed cyanotic necrosis and severe tension blisters. Surgical intervention was initially deferred due to the patient’s unstable hemodynamic status and severe coagulopathy, characterized by an Antithrombin III level of 49.9% and platelet count dropping to a nadir of 14 × 109/L, which posed a prohibitively high bleeding risk. On hospital day six (October 1), next-generation sequencing (NGS) confirmed Vibrio vulnificus infection (Figure 2).
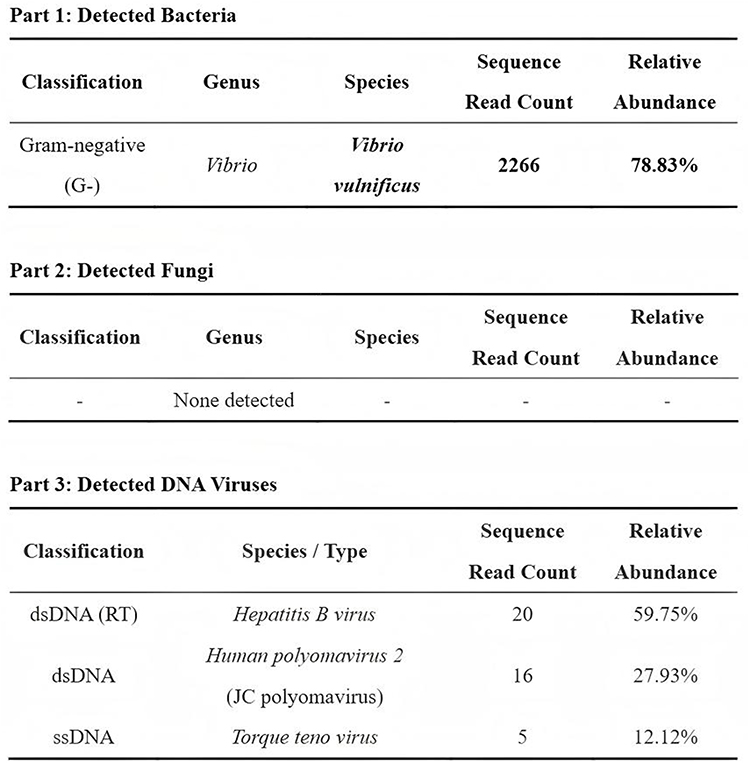 |
Figure 2 Next-generation sequencing (NGS) results from blood samples on hospital day 6 confirming the detection of Vibrio vulnificus (Sequence read count: 2266, Relative abundance: 78.83%). |
Following a Multidisciplinary Team (MDT) consultation on day nine (October 4), urgent surgical intervention was deemed critical despite the risks. The first surgical debridement was performed on day nine, involving extensive excision of necrotic skin and superficial fascia with characteristic “dishwater” pus drainage (Figure 3). Over the course of hospitalization, the infection proved difficult to control due to the patient’s underlying comorbidities. Progressive necrosis of the subcutaneous tissues and tendons was noted by day 26 (Figure 4), necessitating a second radical debridement combined with split-thickness skin grafting and vacuum-sealing drainage (VSD) (Figure 5). Antibiotic therapy was adjusted to tigecycline (50 mg q12h) and ciprofloxacin (0.2 g q12h) on October 8 (Day 13) based on clinical response.
 |
Figure 3 Intraoperative findings on hospital day 9. Extensive necrosis of the skin and subcutaneous fascia was observed, accompanied by purulent discharge, following surgical incision and debridement. |
 |
Figure 4 Clinical appearance on hospital day 26 showing progressive necrosis of the peripheral subcutaneous tissues and darkening/necrosis of the extensor tendons on the dorsum of the hand. |
 |
Figure 5 Surgical management on hospital day 26 involving radical debridement followed by split-thickness skin grafting and application of vacuum-sealing drainage (VSD). |
The clinical course was complicated by acute kidney injury (AKI) with blood urea nitrogen elevating to 12.69 mmol/L, which was managed conservatively with fluid volume optimization and diuretics. Additionally, severe electrolyte disturbances (hypokalemia: 2.60 mmol/L) were corrected to prevent arrhythmias. Despite these intensive interventions, the patient suffered from recurrent sepsis and deep vein thrombosis (confirmed by ultrasound on October 16). By day 37, partial necrosis of the skin graft was observed (Figure 6). Magnetic resonance imaging (MRI) subsequently confirmed extensive infectious changes involving the soft tissues of the right arm extending proximally to the shoulder region (Figure 7). Ultimately, after 50 days of hospitalization, the patient and family declined limb amputation and requested discharge against medical advice.
 |
Figure 6 Clinical presentation on hospital day 37 revealing partial necrosis and darkening of the skin graft. |
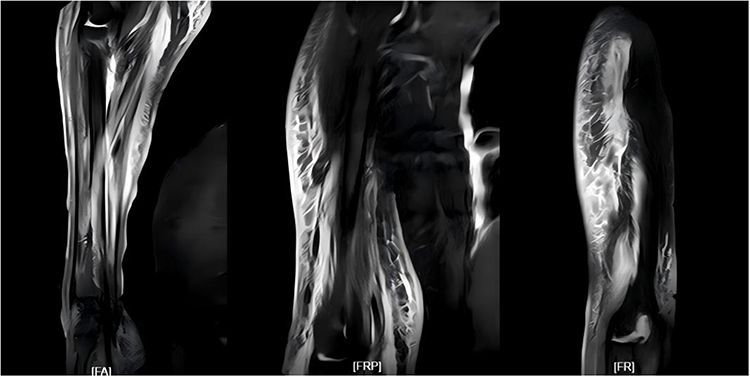 |
Figure 7 Magnetic resonance imaging (MRI) demonstrating the proximal extension of the necrotizing fasciitis and infectious changes involving the right arm and shoulder region. |
Discussion
Epidemiology
Vibrio vulnificus is a halophilic Gram-negative bacterium that exhibits strict dependence on marine environments. It predominantly inhabits estuarine and coastal waters in temperate and tropical zones, thriving in water temperatures between 20°C and 35°C. The pathogen bioaccumulates in filter-feeding shellfish, particularly oysters. Human transmission occurs primarily through two pathways: wound exposure to contaminated seawater (causing wound infection) or ingestion of raw/undercooked seafood (causing primary septicemia).
Global incidence is rising, with high-risk regions including the United States, Taiwan, Japan, and coastal China.6 Notably, climate change and warming seawaters are expanding the pathogen’s geographical and seasonal range.7 Susceptibility is markedly increased in individuals with chronic liver disease, diabetes mellitus, hemochromatosis, and immunosuppression. In these patients, mechanisms such as iron overload and immune dysfunction facilitate rapid bacterial proliferation, leading to fulminant sepsis with mortality rates exceeding 50%. In the presented case, the patient’s poorly controlled diabetes (HbA1c 9.3%) served as a critical predisposing factor. The onset in late September aligns with the peak seasonal incidence, highlighting the need for vigilance during warmer months.
Pathogenic Mechanism
The pathogenesis of Vibrio vulnificus infection involves a complex cascade of virulence factors.8 Upon invasion, the bacterium expresses capsular polysaccharides that resist phagocytosis. Virulence factors such as the hemolysin VvhA cause erythrocyte lysis and endothelial damage, leading to tissue ischemia and massive edema. Concurrently, metalloproteases (eg, VvpE) degrade the extracellular matrix, facilitating the rapid spread of infection along fascial planes, resulting in the characteristic “dishwater” pus and extensive necrosis.
Host factors play a critical role. In diabetic patients, hyperglycemia impairs neutrophil chemotaxis and phagocytosis. Furthermore, bacterial lipopolysaccharide (LPS) activates the Toll-like receptor 4 (TLR4) signaling pathway, which triggers nuclear factor kappa B (NF-κB) translocation. This results in a “cytokine storm,” characterized by the massive release of pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6). This systemic inflammatory response syndrome (SIRS) drives the refractory shock, lactic acidosis, and multi-organ dysfunction observed in this patient. Additionally, Vibrio cytolysins can induce apoptosis via mitochondrial pathways, exacerbating tissue death and thrombocytopenia.
Clinical Features
Clinical manifestations typically present as either primary septicemia or necrotizing wound infections. Primary septicemia, often following seafood ingestion, is characterized by the abrupt onset of fever, chills, and hypotension, frequently accompanied by secondary metastatic cutaneous lesions (bullae and ecchymosis). Wound infections present with rapid local swelling, erythema, and pain disproportionate to physical findings, which can evolve into necrotizing fasciitis within hours. Characteristic laboratory findings include severe thrombocytopenia, coagulopathy (prolonged prothrombin time, hypofibrinogenemia), metabolic acidosis, and elevated inflammatory markers (CRP, procalcitonin).
Treatment
Effective management of Vibrio vulnificus sepsis hinges on early recognition and immediate activation of MDT intervention.
Early Identification and Diagnosis
Early diagnosis is the strongest predictor of survival but remains challenging due to non-specific early symptoms. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score is a commonly used tool to screen for necrotizing soft tissue infections. However, its sensitivity in early Vibrio infections can be limited. Retrospectively, this patient’s LRINEC score at admission was only 3 points (CRP 12.3 mg/L, WBC 7.65×109/L, Hemoglobin 107 g/L, Sodium 138 mmol/L, Creatinine 58 μmol/L, Glucose 15.8 mmol/L), which falls into the “low risk” category. This highlights a critical pitfall: relying solely on scoring systems can lead to missed diagnoses in fulminant cases where physiological derangement (eg, shock) outpaces laboratory markers.
Therefore, clinical suspicion must take precedence over scores. The RiCH scoring system (Rapid limb deterioration, Systemic inflammation, Chronic comorbidities) offers more specific guidance for Vibrio sepsis.9 This patient met all three criteria. We emphasize that for high-risk patients with seawater/seafood exposure presenting with sepsis and limb pain, Vibrio infection should be presumed until proven otherwise. While traditional cultures remain the gold standard, they can be slow. In this case, next-generation sequencing (NGS) provided definitive pathogen identification, demonstrating its value in culture-negative or ambiguous cases.
Selection of Antibiotics
Given the rapid progression of the disease, immediate empiric antibiotic therapy is crucial. Initial therapy with meropenem and linezolid was chosen to cover broad-spectrum pathogens pending culture results. The implementation of NGS was delayed until day 6 primarily due to the initial diagnostic uncertainty and the logistical time required to send samples to an external genomic laboratory. Once Vibrio vulnificus was confirmed, therapy was optimized.
Current guidelines recommend a combination of a third-generation cephalosporin (eg, ceftazidime or cefoperazone) plus a tetracycline (eg, doxycycline) or a fluoroquinolone (eg, ciprofloxacin).9,10 In this case, the regimen was adjusted to tigecycline and ciprofloxacin, and later ceftazidime, based on clinical response and the need for tissue penetration. The prolonged course of antibiotics was necessitated by the extensive necrosis and secondary complications, underscoring the difficulty of eradicating the pathogen once deep tissue invasion occurs.
Surgical Treatment
Urgent surgical debridement is the cornerstone of managing necrotizing fasciitis.11 Guidelines suggest that survival decreases significantly if surgery is delayed beyond 24 hours. In this case, the initial surgical debridement was performed on hospital day 9. This delay was multifactorial: primarily, the patient presented with profound septic shock and severe coagulopathy (Antithrombin III 49.9%, thrombocytopenia) upon admission, presenting an impermissibly high risk for immediate major surgery. Initial efforts focused on hemodynamic resuscitation and correcting coagulopathy. Once the patient’s condition stabilized sufficiently and the diagnosis of necrotizing fasciitis was confirmed by MDT, aggressive debridement was undertaken. This case reinforces that while hemodynamic stabilization is necessary, “damage control” surgery should be considered as early as possible.
Prognosis and Risk Analysis
Prevention strategies must target high-risk populations. Patients with liver disease or diabetes should be educated to avoid raw seafood and contact with seawater if they have open wounds. Furthermore, combatting neglected zoonotic diseases like Vibrio vulnificus requires a “One Health” approach, recognizing the interconnectedness of human, animal, and environmental health. Rising ocean temperatures are increasing the abundance of Vibrio species, directly impacting food safety and human infection rates. As highlighted by Meurer, an integrated surveillance system monitoring marine bacterial loads and notifying healthcare providers during peak risk periods is essential for timely diagnosis and treatment.12 Collaborative efforts between environmental scientists, veterinarians, and clinicians are vital to mitigate the impact of this evolving pathogen.
Limitations
This report has limitations. First, it is a single case study, which limits generalizability. Second, the LRINEC score at admission was deceptively low, which serves as a cautionary example rather than a standard presentation. Finally, the delay in surgical intervention, while clinically justified by the patient’s instability, contributed to the poor local outcome, highlighting the clinical dilemma between resuscitation and source control.
Conclusions
Through a case report and literature review, this paper elaborates on the severity and complexity of Vibrio vulnificus infection. The patient presented with septic shock complicated by necrotizing fasciitis, and the condition progressed rapidly. After multidisciplinary treatment, including anti-infection, surgical debridement, and supportive therapy, the prognosis was poor due to recurrent infections and the expansion of the necrotic tissue area. This paper emphasizes the importance of early recognition, timely diagnosis, and multidisciplinary collaboration. Clinicians should be highly vigilant about patients with a history of seafood contact and high-risk underlying diseases, and conduct etiological testing and targeted treatment in a timely manner to reduce the mortality rate.
Abbreviations
CRP, C-reactive protein; PCT, Procalcitonin; NGS, Next-generation sequencing; APTT, Activated partial thromboplastin time; MDT, Multidisciplinary treatment; VSD, Vacuum-sealed drainage; LPS, Lipopolysaccharide; DIC, Disseminated intravascular coagulation; ATIII, Antithrombin III; AKI, Acute kidney injury.
Ethics Approval and Consent to Participate
Institutional approval was not required to publish the case details. The requirement for ethical approval was waived by the Ethics Committee of Peking University People’s Hospital (Qingdao), as this study represents a retrospective case report of a single patient and does not involve experimental clinical trials. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Natural Science Foundation of Shandong Province (ZR2024MH037), the National Natural Science Foundation of China (22278003), the Beijing Science and Technology Planning Project (Z241100009024027), the Shandong Provincial Clinical Specialty Department, and the Qingdao Municipal Health Care Key Discipline Construction Project-Climbing Peak Discipline.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Baker-Austin C, Oliver JD. Vibrio vulnificus. Trends Microbiol. 2018;26(1):81–10.
2. Heng SP, Letchumanan V, Deng CY, et al. Vibrio vulnificus: an environmental and clinical burden. Front Microbiol. 2017;8:997. doi:10.3389/fmicb.2017.00997
3. Baker-Austin C, Oliver JD, Alam M, et al. Vibrio spp. infections. Nat Rev Dis Primers. 2018;4(1):1–19. doi:10.1038/s41572-018-0005-8
4. Coerdt KM, Khachemoune A, Patsinakidis N. Vibrio vulnificus: review of mild to life-threatening skin infections. Dermatol Ther. 2021;34(2):e14792. doi:10.1111/dth.14792
5. USDA Economic Research Service. Cost Estimates of Foodborne Illnesses. U.S. Department of Agriculture. 2024. Available from: https://www.ers.usda.gov/data-products/cost-estimates-of-foodborne-illnesses.
6. Leng F, Lin S, Wu W, et al. Epidemiology, pathogenetic mechanism, clinical characteristics, and treatment of Vibrio vulnificus infection: a case report and literature review. Eur J Clin Microbiol Infect Dis. 2019;38(11):1999–2004. doi:10.1007/s10096-019-03629-5
7. Di W, Cui J, Yu H, et al. Vibrio vulnificus necrotizing fasciitis with sepsis presenting with pain in the lower legs in winter: a case report. BMC Infect Dis. 2022;22(1):478. doi:10.1186/s12879-022-07655-1
8. Lu K, Li Y, Chen R, et al. Pathogenic mechanism of Vibrio vulnificus infection. Future Microbiol. 2023;18(2):123–136. doi:10.2217/fmb-2022-0243
9. Hong GL, Lu CJ, Zhao GJ, et al. Diagnosis and treatment protocol for Vibrio vulnificus sepsis. Chin J Emerg Med. 2018;27(6):635–641.
10. Trinh SA, Gavin HE, Satchell KJF. Efficacy of ceftriaxone, cefepime, doxycycline, ciprofloxacin, and combination therapy for Vibrio vulnificus foodborne septicemia. Antimicrob Agents Chemother. 2017;61(11):e01113. doi:10.1128/AAC.01106-17
11. Chinese Association of Emergency Physicians. Chinese society of emergency medicine, committee of first aid resuscitation and disaster medicine of Chinese Medical Doctor Association, et al. Expert consensus on clinical diagnosis and treatment of necrotizing soft tissue infection in emergency [in Chinese]. Chin J Emerg Med. 2023;32(1):31–41.
12. Meurer IR. The importance of medical knowledge about q fever in the context of timely diagnosis and treatment and the use of the one health approach in combating this and other neglected zoonotic diseases [Letter]. Infect Drug Resist. 2025;18:5007–5008. doi:10.2147/IDR.S567142
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.