Back to Journals » Neuropsychiatric Disease and Treatment » Volume 12
Vertebral artery dissection with compelling evidence on duplex ultrasound presenting only with neck pain
Authors Siepmann T, Borchert M, Barlinn K
Received 7 August 2016
Accepted for publication 20 September 2016
Published 1 November 2016 Volume 2016:12 Pages 2839—2841
DOI https://doi.org/10.2147/NDT.S119247
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Timo Siepmann, Monique Borchert, Kristian Barlinn
Department of Neurology, Carl Gustav Carus University Hospital, Technische Universität Dresden, Dresden, Germany
Abstract: Vertebral artery dissection (VAD) is among the most common identifiable etiologies of stroke in young adults and poses a diagnostic challenge due to nonspecific symptoms and substantial variability of imaging results. Here, we present a case of unspecific neck pain as isolated symptom of VAD with unusually compelling evidence on duplex ultrasound. This observation has clinical relevance as the absence of any neurological symptoms in our patient highlights the necessity of considering cervical artery dissection in patients presenting with unspecific symptoms such as neck pain, even if isolated. Furthermore, our image of intramural hematoma on duplex ultrasound has been captured in an unusual, clear and distinct fashion and might therefore be a useful reference image in the clinical assessment of patients with a suspicion of cervical artery dissection.
Keywords: vertebrobasilar, cervical, duplex sonography, magnetic resonance imaging
Introduction
Vertebral artery dissection (VAD) is among the most common identifiable etiologies of stroke in young adults aged 18–45 years, with an estimated annual incidence between 1 and 1.5 per 100,000.1 Compared to carotid dissection, detection of VAD is challenging due to nonspecific symptoms and substantial variability of imaging results. Intramural pathology can be captured by noninvasive techniques such as fat-saturated magnetic resonance imaging (MRI) and duplex ultrasound. Although duplex ultrasound provides hemodynamic information in real-time, the technique is limited by the low rate of clear findings suggestive of intramural hematoma in patients with VAD.2 Here, we present a case of unspecific neck pain as isolated symptom of bilateral VAD with unusually compelling evidence on duplex ultrasound.
Case description
A 28-year-old woman with a history of amyotrophic neuralgia one year ago with electroneurographic evidence of neurogenic paresis of the right serratus anterior muscle experienced acute neck pain radiating in both shoulders. She presented to her local neurologist. Physical and neurological examinations were normal. She was treated with oral prednisolone for five days for probable recurrent amyotrophic neuralgia. Pain ceased after seven days. An elective cervical MRI was performed 21 days later which showed no radiculopathy but suspicion of left VAD. Consequently, she was referred to our neurology department. Neurological examination was normal. Neither physical examination nor medical and family history revealed any indications of connective tissue disease or trauma. Routine laboratory results were normal. Duplex ultrasound showed luminal narrowing of the left vertebral artery (VA) along its extracranial course and hypoechoic thickening of the vessel wall suggestive of intramural hematoma (Figures 1 and 2) Fat-saturated T1 MRI confirmed dissection of the left VA and additionally showed dissection of the right extracranial VA (Figures 3 and 4). No infarction was seen on brain MRI. Antiplatelet therapy with oral aspirin (100 mg/day) was initiated and the patient was discharged. At follow-up visit six months later, she reported having experienced no neck pain since discharge. Neurological examination was normal. Duplex ultrasound showed a patent left VA with only slight residual luminal narrowing and decreased blood flow velocity of its intracranial segment compared to the contralateral VA. Duplex ultrasound of the right VA was unremarkable. Aspirin was prescribed for another six months after which another follow-up visit was scheduled. The patient gave informed consent to publish this report and accompanying images.
 | Figure 1 Duplex ultrasound (B-mode) shows narrowing of left intervertebral VA. The asterisk indicates the false lumen caused by intramural hematoma. |
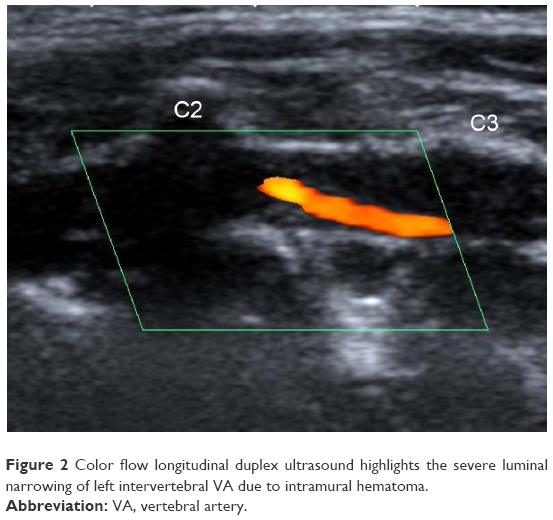 | Figure 2 Color flow longitudinal duplex ultrasound highlights the severe luminal narrowing of left intervertebral VA due to intramural hematoma. |
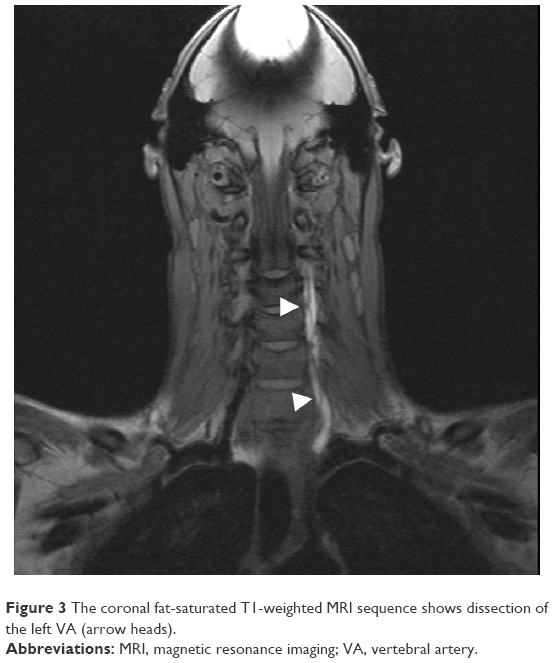 | Figure 3 The coronal fat-saturated T1-weighted MRI sequence shows dissection of the left VA (arrow heads). |
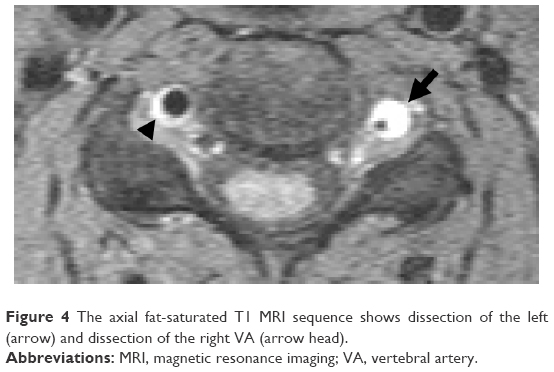 | Figure 4 The axial fat-saturated T1 MRI sequence shows dissection of the left (arrow) and dissection of the right VA (arrow head). |
Discussion
Our report of isolated pain in the neck as the sole symptom of spontaneous bilateral VA dissection has two clinically relevant implications. First, the absence of any neurological symptoms in our patient highlights the necessity of considering cervical artery dissection in patients presenting with unspecific symptoms such as neck pain, even if isolated.3 Second, our image of intramural hematoma on duplex ultrasound has educational value, as pathology is captured in an unusual, clear and distinct fashion and can be a useful supplement to other neurovascular reference images in the clinical assessment of patients with a suspicion of cervical artery dissection.
While in our patient, dissection of the left VA was clearly detected on both duplex ultrasound and MRI, contralateral VAD was missed by duplex ultrasound most likely due to its distal manifestation. Direct B-mode imaging of the V3-VA is challenging, and stenotic lesions caused by intramural hematoma are commonly suspected on the basis of upstream flow disturbances (eg, high-resistance pulsatile flow). Thus, we may speculate that luminal narrowing of the right V3 segment was too slight to produce corresponding pre-stenotic flow changes.
In concordance with best available evidence, our patient was prescribed antiplatelet treatment.4 Improving accuracy in detection of VAD is important, since patients have an increased risk of acute ischemic stroke and early recurrent stroke due to embolism from thrombus formation at the dissection site.5–7 Data from observational and nonrandomized studies indicated efficacy of oral anticoagulation therapy applied for three or six months after dissection to prevent recurrent stroke, an observation which has been widely translated into clinical practice.8 Although this treatment regimen has been recommended by the American Heart Association (AHA) guidelines, similar evidence was found for antiplatelet therapy, which is why these guidelines also acknowledged that the relative efficacy of anticoagulation versus antiplatelet therapy remained unknown at the time of publication.9 A recent multicenter trial compared the two treatment forms in a randomized fashion but was stopped prematurely due to failure of recruitment. However, subsequent analysis showed no difference between the antiplatelet and anticoagulant treatment arms in preventing stroke and death in patients with symptomatic cervical artery dissection.4 Although the rate of strokes was slightly lower in the group of patients receiving anticoagulant therapy than in the antiplatelet group, this difference was counterpoised by one severe subarachnoid hemorrhage in the anticoagulant group.
Our clinical case of VAD with unusually clear evidence on duplex ultrasound, confirmed by fat-saturated MRI, and presenting with neck pain as the only symptom does not only highlight the diagnostic value of ultrasound as supplement to fat-saturated MRI but also emphasizes the importance of thorough clinical assessment in patients with nonspecific symptoms such as neck pain.
Acknowledgment
The authors extend their sincere appreciation to Professor Heinz Reichmann for his general support.
Disclosure
The authors report no conflicts of interest in this work.
References
Gottesman RF, Sharma P, Robinson KA, et al. Imaging characteristics of symptomatic vertebral artery dissection: a systematic review. Neurologist. 2012;18(5):255–260. | ||
Caplan LR. Dissections of brain-supplying arteries. Nat Clin Pract Neurol. 2008;4(1):34–42. | ||
Arnold M, Cumurciuc R, Stapf C, Favrole P, Berthet K, Bousser MG. Pain as the only symptom of cervical artery dissection. J Neurol Neurosurg Psychiatry. 2006;77(9):1021–1024. | ||
CADISS trial investigators, Markus HS, Hayter E, et al. Antiplatelet treatment compared with anticoagulation treatment for cervical artery dissection (CADISS): a randomised trial. Lancet Neurol. 2015;14(4):361–367. | ||
Debette S, Leys D. Cervical artery dissections: predisposing factors, diagnosis, and outcome. Lancet Neurol. 2009;8(7):668–678. | ||
Molina CA, Alvarez-Sabin J, Schonewille W, et al. Cerebral microembolism in acute spontaneous internal artery dissection. Neurology. 2000;55(11):1738–1740. | ||
Lucas C, Moulin T, Deplanque D, Tatu L, Chavot D. Stroke patterns of internal carotid artery dissection in 40 patients. Stroke. 1998;29(12):2646–2648. | ||
Menon RK, Markus HS, Norris JW. Results of a UK questionnaire of diagnosis and treatment in cervical artery dissection. J Neurol Neurosurg Psychiatry. 2008;79(5):612. | ||
Furie KL, Kasner SE, Adams RJ, Albers GW, et al; American Heart Association Stroke Council, Council on Cardiovascular Nursing, Council on Clinical Cardiology, and Interdisciplinary Council on Quality of Care and Outcomes Research. Guidelines for the prevention of stroke in patients with stroke or transient ischemic attack: a guideline for healthcare professionals from the American heart association/American stroke association. Stroke. 2011;42(1):227–276. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.