Back to Journals » Vascular Health and Risk Management » Volume 19
Venous Thromboembolism in Pregnancy: Challenges and Solutions
Authors Varrias D, Spanos M ![]() , Kokkinidis DG, Zoumpourlis P, Kalaitzopoulos DR
, Kokkinidis DG, Zoumpourlis P, Kalaitzopoulos DR ![]()
Received 2 June 2023
Accepted for publication 13 July 2023
Published 20 July 2023 Volume 2023:19 Pages 469—484
DOI https://doi.org/10.2147/VHRM.S404537
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Dimitrios Varrias,1,2,* Michail Spanos,3,* Damianos G Kokkinidis,4 Panagiotis Zoumpourlis,1,2 Dimitrios Rafail Kalaitzopoulos5
1Department of Medicine, Jacobi Medical Center, Bronx, NY, 10461, USA; 2Albert Einstein College of Medicine, Bronx, NY, 10461, USA; 3Cardiovascular Research Center, Massachusetts General Hospital, Boston, MA, USA; 4Section of Cardiovascular Medicine, Yale University School of Medicine, Yale New Haven Hospital, New Haven, CT, USA; 5Department of Gynecology and Obstetrics, Cantonal Hospital Schaffhausen, Schaffhausen, Switzerland
*These authors contributed equally to this work
Correspondence: Dimitrios Varrias, Jacobi NYCHHC, 1400 Pelham Parkway South, 3N1, Bronx, NY, 10461, USA, Tel +1 7189185000, Email [email protected]
Abstract: Venous thromboembolism (VTE) is a serious medical condition that can lead to severe morbidity and mortality, making it a significant public health concern. VTE is a multifactorial condition that results from the interaction of genetic, acquired, and environmental factors. Physiological changes during pregnancy increase the risk of VTE as they express Virchow’s triad (increased coagulation factors, decreased fibrinolysis, trauma, and venous stasis). Moreover, pregnancy-related risk factors, such as advanced maternal age, obesity, multiple gestations, and cesarean delivery, further increase the risk of VTE. Managing VTE in pregnancy is challenging due to the complexity of balancing the risks and benefits of anticoagulant therapy for both the mother and the fetus. A multidisciplinary approach involving obstetricians, hematologists, and neonatologists, is necessary to ensure optimal outcomes for both the mother and baby. This review aims to discuss the current challenges associated with VTE in pregnancy and identify potential solutions for improving outcomes for pregnant women at risk for VTE.
Keywords: venous embolism, thrombosis, pregnancy, VTE, anticoagulation
Introduction
Venous thromboembolism (VTE) is a significant pregnancy complication, with an incidence of approximately 1 per 1000 pregnancies (reported incidence; 0.025% to 0.1%).1,2 Despite advances in diagnostic and therapeutic approaches, VTE remains a leading cause of maternal mortality in developed countries. In the United States, VTE is responsible for approximately 10% of maternal deaths, with pulmonary embolism (PE) being the most common cause. In the CDC’s pregnancy-related mortality surveillance, PE accounted for 20% of pregnancy-related deaths between 1991 and 1999, surpassing other complications associated with pregnancy, such as infection, hemorrhage, and pregnancy-induced hypertension.3 However, it is essential to note that when VTE is diagnosed exclusively based on a clinical evaluation, the incidence of the disease may be overestimated. Nonetheless, an analysis of 395,335 pregnant women in a retrospective case-control study at 24 weeks of gestation found the incidence of VTE to be 85 per 100,000 pregnancies,4 while in a community-based study over 30 years, 200 women per 100,000 person-years were diagnosed with VTE, and DVT was three times more common than PE.5 European countries have observed similar trends.5,6 Based on a retrospective study of more than 72,000 deliveries, the incidence of DVT was 0.71 per 1000 births (95% CI 0.5–0.9), of which 0.5 (95% CI 0.33–40.66) occurred antenatally and 0.21 (95% CI 0.11–31) following delivery.7 According to the same study, PE occurred 0.15 times per 1000 deliveries (95% CI 0.06–0.24), with 0.07 cases (95% CI 0.01–0.13) occurring before and 0.08 (95% CI 0.02–0.14) after the delivery.7 Regarding the antepartum period, data about VTE are somewhat conflicting, with some studies observing a higher incidence in the second and third trimesters.8–10 In contrast, others observe similar risk of VTE during all three trimesters of pregnancy.11–14 A consensus exists that the risk of VTE is highest in the postpartum period, with the incidence peaking in the first six weeks following delivery.9 The incidence of VTE varies according to different population groups and risk factors. For example, the incidence of VTE is higher in women with a history of VTE or thrombophilia, those undergoing assisted reproductive technology, and those with medical comorbidities such as diabetes or hypertension.9,15 Furthermore, racial and ethnic disparities have been reported in the incidence of VTE during pregnancy, with African American women being at a higher risk than White caucasian women.16
Given the relatively high incidence of VTE during pregnancy, the associated morbidity and mortality, and the difficulty in diagnosis, it is crucial to understand the risk factors and pathophysiology that form the current challenges of VTE in pregnancy. This knowledge can inform clinical practice and guide the development of evidence-based approaches to prevent and manage VTE in pregnant women. This review article provides a comprehensive overview of the current knowledge regarding VTE in pregnancy, emphasizing the clinical challenges of diagnosis and treatment and the most up-to-date clinical strategies to address them. By synthesizing current evidence-based knowledge and identifying gaps in understanding, this review aims to provide a valuable resource for healthcare providers and researchers working to improve outcomes for pregnant women at risk for VTE.
Pathophysiology
Physiological Hypercoagulable State During Pregnancy
Virchow’s triad is converged—endothelial trauma, venous stasis, and hypercoagulability—during pregnancy and postpartum (Figure 1). Normal pregnancy is accompanied by hypercoagulability and hypofibrinolysis. These changes in the coagulation and fibrinolytic systems aim to reduce intrapartum blood loss but, at the same time, inadvertently increase the risk of thromboembolism. The coagulation system during pregnancy is physiologically activated due to increased procoagulant factors and the decrease or inactivation of anticoagulant and fibrinolytic systems. Factors VII, VIII, X, XII, von Willebrand factor, and fibrinogen increase.17 Notably, factor VII reaches very high levels increasing as much as tenfold,18 while fibrinogen levels at term are 200% higher than before pregnancy.19 In addition, a significant decrease in the level of physiological anticoagulants is observed, manifested as diminished protein S activity and acquired resistance to activated protein C.17 Furthermore, there is a reduction in fibrinolytic activity due to an increase in both plasminogen activator inhibitor-1 (PAI-1) and plasminogen activator inhibitor type 2 (PAI-2).20
 |
Figure 1 Convergence of Virchow’s triad during pregnancy —endothelial trauma, venous stasis, and hypercoagulability—as well as postpartum. Coagulation is gradually activated to prepare the mother for delivery. The anticoagulant activity of protein S is reduced, and activated protein C resistance rises. A higher concentration of fibrinogen, factors V, IX, X, and VIII, enhances procoagulant activity, leading to increased thrombin production, as demonstrated by an increase in soluble fibrin and prothrombin levels. Reduced fibrinolysis results from increased plasminogen activator inhibitor type 1 and 2 and decreased tissue plasminogen activator (tPA) activity. Endothelial damage to the pelvic vessels results from mechanical stress during normal, induced, or operative vaginal delivery. Venous stasis occurs due to the combination of estrogen-induced venodilation, pelvic venous compression, and compression of the left iliac vein by the right iliac artery. |
Platelet function is also altered during pregnancy. Platelets decrease in number but are more responsive to agonists, such as adenosine diphosphate (ADP) and thrombin, leading to increased platelet aggregation.21 This may be in part due to changes in their surface receptors.22 Finally, placental trophoblastic cells release nanoparticles that have been shown, in vitro, to exert prothrombotic effects on platelets and the vascular endothelium.23 The enhanced platelet aggregation further increases the risk of thrombosis, which, combined with the reduction in fibrinolytic activity, results in the formation of fibrin clots more resistant to degradation. In addition to the changes in the coagulation system and platelet function, pregnancy is also associated with alterations in hormonal homeostasis and hemodynamics. Pregnancy hemodynamic changes are characterized by increased intravascular volume and reduced systemic vascular resistance.24 An increase in estrogen, progesterone, and relaxin during pregnancy causes systemic vasodilation and increased venous capacitance,25 which increases vessel diameter and decreases blood flow velocity as observed by real-time and duplex Doppler ultrasound.26 This hemodynamic state favors the stasis of blood in the venous circulation. Mechanical obstructions further aggravate the venous pooling due to the gravid uterus compressing the iliac veins and compromising the venous return.27 This, combined with prolonged immobility, such as bed rest or prolonged sitting or standing, commonly seen during pregnancy, further increase the thrombotic risk.28,29 The elevation in estrogen and progesterone levels can also decrease antithrombin activity and increase clotting factors synthesis,30 activate the hypoxia-inducible factor-1 pathway,31,32 and result in hypercoagulability and platelet activation and aggregation.30 Finally, the vessel wall structure is also altered during pregnancy, with an increase in the number of smooth muscle cells and a decrease in elastin content which render the vessel wall prone to injury and subsequent thrombosis.33
It is becoming apparent that in conjunction with the overall hypercoagulable state, increased vascular compliance, venous stasis, mechanical compression of the pelvic veins, and delivery-associated endothelial damage complete Virchow’s triad of hypercoagulability, stasis, and vascular damage creating a highly thrombogenic environment, even during normal, uncomplicated pregnancy.
Thrombophilia in Pregnancy
Thrombophilia refers to inherited or acquired conditions that may increase the risk of thrombosis during pregnancy, leading to VTE. Thrombophilia, which occurs in 8–15% of Caucasians, is the second most common risk factor for pregnancy-related VTE (with a history of VTE being the first).34 There are two main types of thrombophilia – acquired and inherited thrombophilia (IT). The inherited forms are due to genetic mutations affecting genes implicated in the coagulation cascade. Several ITs have been associated with an increased risk of VTE during pregnancy, including factor V Leiden, prothrombin gene mutation, and deficiencies of Antithrombin, protein C, and Protein S.35 ITs are relatively rare in the general population. For instance, Factor V Leiden, the most common IT in the Caucasian population, has a prevalence of approximately 5%.36 The mutation resists the anticoagulant effects of activated protein C, leading to a prothrombotic state. Prothrombin G20210A gene mutation is another common IT, occurring in approximately 2% of the general population. It results in the overproduction of prothrombin, a precursor of thrombin, leading to thrombotic conditions, such as VTE and PE.37 Deficiencies of Antithrombin, protein C, and protein S are ITs that are relatively rare but associated with a high risk of VTE during pregnancy and recurrent pregnancy loss.35,38 Antithrombin is a natural anticoagulant that inhibits thrombin and other coagulation factors, while protein C and protein S are cofactors in the inactivation of coagulation factors. Deficiencies in any of these factors lead to a prothrombotic state, with the risk of VTE during pregnancy increased by up to 30-fold.39 According to their absolute risk for initial and recurrent venous thromboses, thrombophilias may be categorized into high, moderate, and low. Antithrombin III deficiency, protein C deficiency, and protein S deficiency are considered high-risk thrombophilias, moderately risk thrombophilias include factor V Leiden, prothrombin gene mutations, factor VIII deficiency, and low-risk thrombophilias encompass factor XI, factor IX, and hyperhomocysteinemia.40
Furthermore, additional criteria such as the zygosity of the mutation and prior personal or family history significantly influence the risk for VTE in pregnancy.35 As more of those criteria are met, the risk of thrombosis increases. For instance, the risk of VTE in pregnant women heterozygous for factor V Leiden without a personal history of VTE or an affected first-degree relative is estimated not to exceed 5–10 per 1000 deliveries. In contrast, the risk increases to up to 10% if a personal history of VTE is present,15,41,42 and up to 15/1000 deliveries with an affected first-degree relative.15,41 Finally, homozygous pregnant women without a personal history of VTE or a first-degree relative affected by VTE are at a 1–2% risk, whereas those with a history have a 17% risk.41
In addition to inherited thrombophilias, acquired thrombophilias can also increase the risk of VTE during pregnancy. Antiphospholipid syndrome (APS) is the most common cause of pregnancy-acquired thrombophilia.43 Recently, studies have provided further insight into the pathogenesis of APS. Vascular thrombosis is associated with antiphospholipid (APL) antibodies in this syndrome. Specifically, anticardiolipin and lupus anticoagulant antibodies were most commonly found to be associated with thromboembolic events.44,45 A 2:1 ratio of venous-to-arterial thrombosis characterizes APS, and thrombosis tends to be recurrent. VTE, specifically deep venous thrombosis of the legs, is the most common manifestation and recurrence of APS.46 It has been reported that 76% of recurrences will also be venous if the initial thrombotic event is venous.46 The hypercoagulable state of pregnancy compounds the risk of thrombosis to the extent that over half of the thrombotic episodes in patients with APS are related to pregnancy or combined oral contraceptives.47 Some studies have shown that many pregnant APS patients still experience thrombotic episodes despite receiving thromboprophylaxis.48,49 Diagnosing thrombophilias during pregnancy can be challenging, as many of the laboratory tests used to diagnose these conditions are affected by pregnancy-related changes in hemostasis.50 However, identifying women with thrombophilias is important, as it can inform decisions about prophylactic anticoagulation during pregnancy and postpartum. Women with a personal or family history of VTE or a strong family history of thrombophilia should be screened for inherited thrombophilias before or early in pregnancy. Women with a history of recurrent pregnancy loss or fetal death may also be candidates for screening for antiphospholipid syndrome.
Diagnosis and Management
Clinical Presentation and Diagnostic Workup of VTE in Pregnancy
VTE in pregnancy can present in various ways, ranging from asymptomatic to life-threatening events such as massive pulmonary embolism (PE) with hemodynamic instability. Several symptoms that raise suspicion for VTE in non-pregnant women, including mild tachycardia, tachypnea, dyspnea, and lower extremity edema and pain, are nonspecific and common during a routine, uncomplicated pregnancy. Consequently, physical examination is often insufficient for diagnosing VTE. In the case of DVT in pregnancy, the two most common presenting symptoms are pain and swelling. These symptoms may or may not be associated with erythema, warmth, and lower extremity tenderness. It is estimated that 80% of pregnant women who suffer from DVT experience these symptoms, but the diagnosis is frequently missed.14 While pregnancy-related DVTs are almost identical to those seen in non-pregnant women, there is a greater prevalence of left-sided DVTs (70% to 90%) involving the proximal and iliac veins during pregnancy.12,51 A possible explanation for this phenomenon may be the enhanced venous stasis due to compression of the left iliac vein by the right iliac artery and compression of the inferior vena cava by the gravid uterus.12,52 Symptoms of PE in pregnant women include palpitations, dyspnea, and movement-exacerbating chest pain and present a diagnostic challenge for clinicians since many of these symptoms are caused by benign conditions that are common during pregnancy, such as pregnancy-related physiological dyspnea, gastroesophageal reflux disease, or discomfort caused by the gravid uterus. A clinician’s threshold for conducting imaging in this population should be low, given the recognition that PE can also present with similar symptoms and is a significant cause of maternal mortality.
According to clinical guidelines, several diagnostic modalities are available for diagnosing VTE in pregnant women.53,54 When DVT is in the differential, whole leg ultrasound (US) (Compressing the femoral to the popliteal vein and visualization of the iliac veins) should be considered.54 If DVT is detected by compression maneuvers from the femoral to the popliteal vein or a thrombus is visualized in the iliac vein, DVT is diagnosed, and appropriate therapy should be initiated. If the whole leg US is negative, DVT is excluded, and patients can be followed clinically. In case of equivocal US results or if high suspicion remains despite non-visualization of thrombi in the iliac vein, Magnetic Resonance Imaging (MRI) can be considered.55,56 When a pregnant patient presents with symptoms suspicious of PE, a careful assessment of risk factors for PE should be obtained. Without risk factors and routine physical examination, other likely diagnoses should be considered. In a moderate-high PE suspicion case, the definite diagnosis of PE requires either one of two imaging modalities that involve radiation, a Ventilation-perfusion (VQ) scan, or Computed Tomography Pulmonary Angiography (CTPA).54 It is recommended to conduct bilateral leg ultrasounds with iliac visualization before either test, as the presence of DVT may make further testing unnecessary, avoiding ionizing radiation. If a VQ scan yields a typical result, PE would be excluded, whereas a PE diagnosis is made if it produces a high probability result. If the VQ scan is non-diagnostic, a CTPA should be performed. As with the VQ scan, a normal CTPA test would exclude disease, while a positive test would confirm the diagnosis. If the CTPA is ambiguous or non-diagnostic, a similar approach can be taken by performing a VQ scan or repeating the CTPA test.54 Finally, the place of D-dimer testing for diagnosing or excluding VTE in pregnancy is currently equivocal. Although “normal” D-dimer values have been well described for various assays in asymptomatic pregnant women, the cut-points below which PE can be safely excluded in symptomatic pregnant women have not been established. The current state of research does not allow us to determine whether PE can be safely excluded in patients with average D-dimer results and a non-high clinical probability. On the contrary, several case reports have established that D-dimer levels in pregnant women with radiologically confirmed PE have been below non-pregnant cut-points.57–59
Pharmacological and Non-Pharmacological Management of VTE in Pregnancy
The treatment of VTE in pregnancy is particularly challenging, as the safety of anticoagulant drugs and their potential adverse effects on the developing fetus must be carefully considered.60 Anticoagulant therapy is the mainstay of treatment for VTE in pregnancy. The choice of anticoagulant agent depends on several factors, including the location and severity of the thrombosis, the gestational age, and the potential for adverse effects on the fetus. Among the anticoagulation options are low-molecular-weight heparins (LMWHs), unfractionated heparins (UFHs), and Warfarin which should be used postpartum only. LMWHs are preferred over UFH as the first-line treatment for preventing and treating VTE in pregnancy.53,61,62 Randomized trials have shown that LMWHs are equally or more effective than UFH in non-pregnant women.63,64 LMWHs are excreted in breast milk at a minimal level, so they pose no risk to breastfeeding infants.65 Moreover, compared with UFH, LMWHs exhibit less risk of adverse effects, including hemorrhage, heparin-induced thrombocytopenia, osteoporosis, and allergic reactions.62 It is recommended that pregnant women avoid Warfarin. Warfarin crosses the placenta and increases the risk of severe complications, such as miscarriage, stillbirth, developmental abnormalities, neurological disorders, and excessive bleeding.66 However, Warfarin can be used while breastfeeding. UFH is administered by continuous intravenous or subcutaneous injection, while LMWH is administered by subcutaneous injection. The initial dose of UFH is calculated based on the patient’s weight and adjusted according to the activated partial thromboplastin time (aPTT). In contrast, the dose of LMWH is based on the patient’s weight and administered twice daily without monitoring. Currently, treatment durations for pregnancy range from three to six months, including six weeks after delivery66,67 The use of long-term (ie, extended period over 12 months) anticoagulation is advised for women with antiphospholipid antibody syndrome or two or more thrombophilias that also have VTE68 and for women with any thrombophilia and history of recurrent thromboses.69 In addition to anticoagulant therapy, non-pharmacological interventions can also manage VTE in pregnancy. Compression stockings can help reduce the risk of post-thrombotic syndrome and alleviate leg swelling and pain symptoms. They should be worn during the day and removed at night.70,71 Moreover, early and frequent ambulation is encouraged and can help prevent venous stasis and reduce the risk of VTE. Bed rest should be avoided unless necessary.70 IVC filters can be considered in patients with recurrent VTE despite anticoagulant therapy or in those with contraindications to anticoagulant therapy;70 however, their use should be carefully weighed against the potential risks and benefits.72 Finally, thrombolytic therapy involves administering drugs that dissolve blood clots (eg, tissue plasminogen activator and streptokinase) and restore blood flow, which is considered a last-resort treatment. A significant concern with thrombolytic therapy during pregnancy centers on the effects it has on the mother (ie, major hemorrhage) and on the placenta (ie, premature labor, placental abruption).73 It has been reported that thrombolysis can be successfully performed during pregnancy without causing harm to the fetus, but there are limited reports of these cases, and most involve streptokinase.74–76 Therefore, available guidelines recommend thrombolytic therapy in pregnancy only for life-threatening issues (eg, PE with refractory cardiorespiratory compromise).77
Pregnant women with VTE require close monitoring to assess treatment response, prevent recurrent VTE, and manage potential complications. The frequency and type of monitoring depend on several factors, including the severity of the VTE, the kind of anticoagulant used, and the fetus’s gestational age.10 In general, pregnant women on anticoagulation therapy should have regular monitoring of their coagulation parameters, as well as regular fetal monitoring to assess fetal growth and well-being. In addition, pregnant women with VTE should receive education on the signs and symptoms of recurrent VTE and be advised to seek prompt medical attention if they experience any new or worsening symptoms.78
Challenges
Challenges in History
Identifying High-Risk Pregnancies
It is well established that pregnancy is associated with an increased incidence of VTE due to various mechanisms, as mentioned above. Thus, identifying high-risk women is crucial for decreasing the incidence of VTE in pregnancy and reducing fetal and maternal mortality (Table 1).
 |
Table 1 Risk Factors Associated with Pregnancy-Associated VTE |
Pregnancy-related risk factors for VTE include preterm birth,81 preeclampsia,81 cesarean delivery,81 assisted reproductive technology,81 stillbirths,81,82 obstetric hemorrhages,81,82 and postpartum infection.81,83 Peripartum-associated comorbidities predisposing for VTE include diabetes mellitus,81 systemic lupus erythematosus,84 inflammatory bowel disease,81 and sickle cell disease.85,86 Obesity is not consistently associated with antepartum VTE, but postpartum thrombosis occurs at higher rates in patients with BMI above 35 who also present concurrent mobility problems and decreased functional capacity.79,81–83
One logical approach is to classify risk factors as weak or moderate based on the postpartum or peripartum period. Moderate risk factors (OR 2–9) include thrombophilia and previous venous thromboembolism, while weak risk factors include bed rest (> three days) and varicose veins (OR <2).87 In addition to those mentioned above, factors previously reported to increase the risk of postpartum VTE include age >35 years, cesarean section, blood group A, hypertension, and postpartum bleeding.4 In an extensive registry originating from Australia, stillbirth (aOR 5.97), lupus (aOR 8.83), and transfusion (aOR 8.84) were most strongly associated with PE in postpartum. In contrast, age ≥ 40 years (aOR 1.67), parity ≥ 3 (aOR 1.49), pregnancy hypertension (aOR 2.06), and preterm live birth (aOR 2.18) were associated to a lesser extent.1
Special Populations
Women with Prior History of VTE
According to existing literature, a prior history of thrombosis is one of the most significant risk factors,15 particularly when unprovoked. Pabinger et al found that 4 of 65 women (6.1%) without thromboprophylaxis experienced VTE compared with 5 of 73 women (6.9%) who had received prophylaxis.42 In a cohort of 88 women with a previous episode of VTE who became pregnant at least once without receiving antithrombotic prophylaxis, 120 peripartum periods without prophylaxis were recorded with a postpartum VTE recurrence rate of 8.3%.88
Cesarean Delivery
Many independent VTE risk factors previously confounded the association between cesarean delivery and VTE. In large cohorts, as the Australian registry and the study of Abe et al, cesarean section carried an increased risk regardless of whether it was conducted in the presence (aOR 3.7) or absence (aOR 3.11) of labor after adjusting for confounders.1,89 In the Norwegian study, however, uncomplicated cesarean delivery was not associated with an increased risk after complication adjustment.83 It remains unclear if a cesarean section is associated with a higher incidence of VTE or if this can be attributed to the reasons leading to a cesarean section or underlying complications, such as extensive blood loss or infection.
Assisted Reproduction
Ovarian stimulation results in a hyperestrogenic state. Similarly to the combined oral contraceptive pill or hormone replacement therapy, exogenous estrogens have been associated with hypercoagulability and VTE.90,91 Studies suggest that oestradiol levels correlate with fibrinogen, D-dimers, and activated protein C (APC) resistance.92 Furthermore, ovarian stimulation is associated with increases in several circulating coagulation factors; factor V, fibrinogen, von Willebrand factor, increased coagulation activation markers; prothrombin fragment 1 + 2 and D-dimers, and impairment of endogenous anticoagulants; decreased antithrombin and protein S levels.93,94 As a result, all patients should be individually assessed for their risk of thrombotic complications before having IVF, considering thrombophilias, previous VTE, family history of VTE, concurrent medical conditions, increased age (>40 yrs), or obesity.
Antiphospholipid Syndrome
Antiphospholipid syndrome is defined by venous or arterial thrombosis and specific pregnancy complications with persistently positive tests for antiphospholipid antibodies. It usually warrants long-term anticoagulation after a first thrombotic event because of an increased risk of recurrence. Women with APS receive antenatal therapeutic doses of low molecular weight heparin (LMWH) (those on Warfarin convert to LMWH before six weeks of pregnancy) until after delivery and then change back to oral anticoagulants. However, the optimal management of such women to prevent recurrent thrombosis is difficult due to the scarcity of relevant data. In the Bauersachs et al study of 28 women, two thrombotic events occurred postpartum despite treatment, highlighting the increased risk.95 These women require close management and collaboration between experts, including a hematologist. Women not on blood thinners should start LMWH promptly in the first trimester, which should be continued for at least six weeks after delivery. In the presence of antiphospholipid antibodies alone, without APS, RCOG suggests LMWH for seven days postpartum.96
Challenges in Physical Examination
Physiological lower extremity edema is expected during the second and third trimesters; consequently, women manifesting symptoms suggestive of deep vein thrombosis (DVT) during the first trimester exhibit a much higher likelihood (odds ratio, 53) of being diagnosed with DVT compared to those who presents symptoms later in pregnancy.97 It is important to note that pregnant patients may present with atypical symptoms, often involving pain in the thigh or buttock.79 This is because while the general population suffers from DVTs in smaller and more distally located veins, pregnant individuals demonstrate a slightly increased proportion of DVTs located in iliofemoral vessels (64% vs 54%) and a considerably higher proportion of DVTs isolated to the iliac vein (17% vs 3%), both correlated with increased embolization risks.
Dyspnea, tachycardia, and lower extremity swelling that mimic signs and symptoms of PE are routinely observed in pregnancy due to physiologic changes. Those findings can complicate the assessment of PE presence based solely on clinical factors. Specifically, Varrias et al showed that sinus tachycardia is mainly considered physiologic in pregnancy but is associated with unfavorable outcomes.98 In the Dipep study, pregnant and postpartum women were tested for PE. Those without PE exhibited similar rates of typical PE symptoms, including pleuritic chest pain (52%), shortness of breath (54%), palpitations (13%), cough (8%), and syncope (5%) relative to women with validated, proving that solely clinical diagnosis of PE in pregnant population is a diagnostic conundrum.99
Challenges in Laboratory Findings
D-dimer assays are commonly used in non-pregnant patients to rule out VTE, mainly PE, but the utility of D-dimer among pregnant patients is still debatable One of the concerns is that D-dimer levels increase with gestational age resulting in reduced specificity for VTE100 (Table 2). Despite previous negative studies advising against it,101 recent evidence has led the 2019 European Society of Cardiology (ESC) guidelines to recommend considering D-dimer measurement to rule out PE in pregnant or postpartum patients (class IIa, level B).82,102
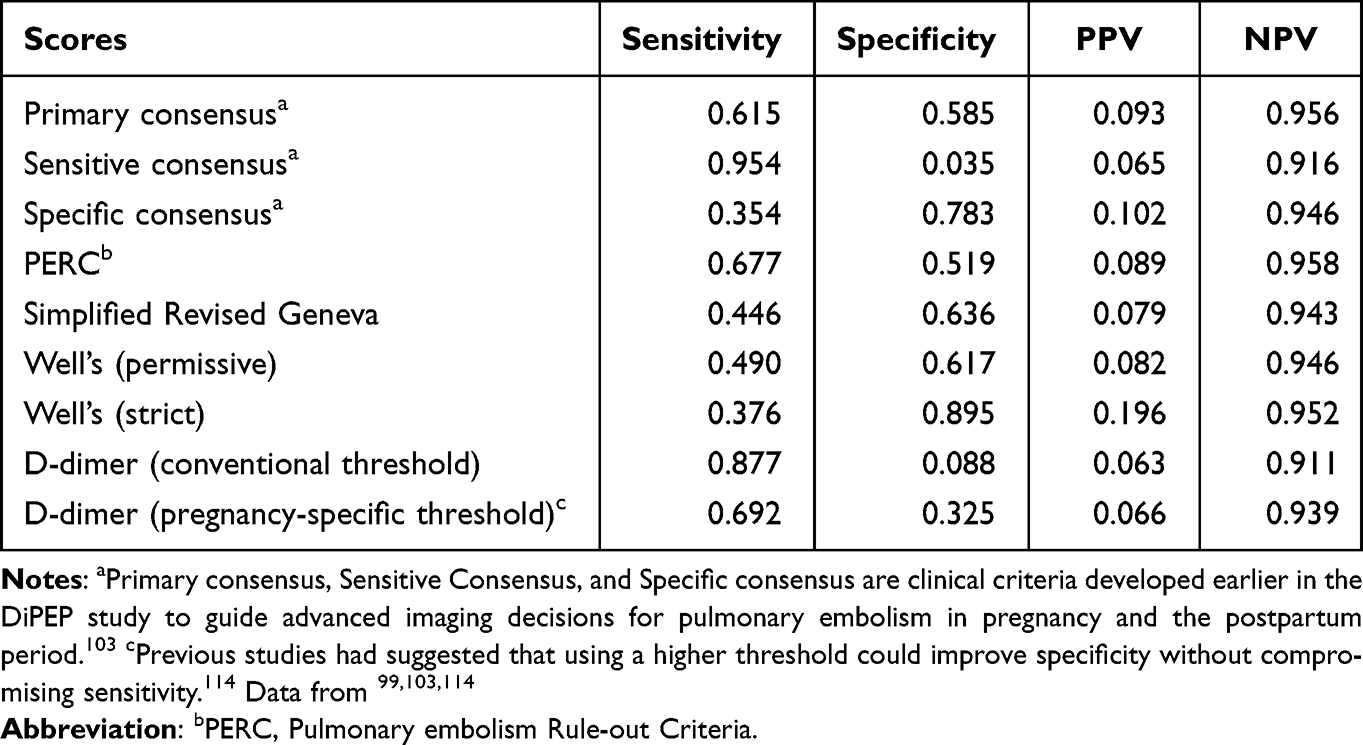 |
Table 2 The Table Shows How the Following Clinical Criteria Would Perform in 1000 Women, of Whom 65 Had PE as per the DiPEP study |
Challenges in Imaging
Computed Tomography Pulmonary Angiography (CTPA)
In the United States and the rest of the world, CTPA has become the diagnostic imaging standard in non-pregnant patients due to its widespread availability, rapid results provision, and superior sensitivity and specificity for PE compared to ventilation/perfusion (V/Q) scans.105 One of the contraindications of CTPA is a severe allergic reaction to iodine contrast. CTPA should be performed with caution in patients with severe kidney disease. Although excessive maternal iodine exposure poses a risk for fetal hypothyroidism,106 contemporary (ie, water-soluble, low-osmolar) iodinated contrast is rapidly cleared from the circulation. Despite initial concerns, it was not associated with severe fetal thyroid dysfunction.106 Regarding breastfeeding, iodinated contrast does not present a risk to breastfeeding infants, negating postpartum patients’ need to “pump and dump” after CTPA.107 Radiation from diagnostic imaging is an important consideration.
Regarding radiation, the estimated mean fetal doses from CTPA (0.05–0.3 mGy) may be slightly lower than those from V/Q scans (0.17–0.4 mGy). Nevertheless, both are far below the 50 to 100 mGy deterministic threshold for fetal radiation complications and present a minimal estimated risk of excess cancer-related death during childhood (approximately 1/100,000).108,109 Despite the low risk of ionizing radiation in the fetus, PE imaging may play a role in lifetime attributable maternal cancer risk, mainly because breast tissue is highly radiosensitive during pregnancy.
Although MRI could be considered for diagnosing PE in the general population, magnetic resonance angiography is discouraged due to low sensitivity in the general population. Enhanced MRI is contraindicated peripartum due to the fetal risks associated with gadolinium contrast.107,110
Solutions
Lab Testing
D Dimers: Previously, the use of D-dimer testing in pregnant women was limited due to concerns such as (1) limited and inconsistent data on sensitivity and NPV of D‐dimer for suspected VTE in pregnancy; (2) absence of pregnancy-specific clinical decision rules to stratify patients according to pretest probability (PTP); (3) unclear appropriate cutoff values for D-dimer tests due to physiological increase during pregnancy. Bellesini et al addressed these concerns, demonstrating high sensitivity and NPV of 99.5% (95% CI, 95.0–100.0; I², 0%) and 100% (95% CI, 99.1–100.0; I², 0%), respectively, for D-dimer testing. Of note, the single-study estimates for sensitivity and NPV were close to 100%, with low heterogeneity levels. These findings align with the sensitivity observed in the general population, supporting using the D‐dimer test to rule out VTE in non‐high‐risk pregnant women without imaging safely.111 In contrast, it is essential to mention that the DIPEP study showed very low specificity regardless of the cutoff; thus, D dimer testing could not discriminate between pregnant and postpartum women with or without a PE.99
Genetic Testing: Despite extensive efforts to identify high-risk pregnancies using comorbidities, established family risk factors cannot be detected in many families with VTE clustering. Individuals with a first-degree relative with a history of VTE are at increased risk of VTE, almost independent of known heritable risk factors, suggesting the existence of unknown genetic risk factors.112 Recently, genome-wide association studies on VTE have been published.113 This would cast some light on genetic causes of pregnancy-associated VTE. In a detailed review regarding the emerging field of non-coding RNAs by Spanos et al, EV-lncRNAs associated with thrombotic risks are identified, among others related to cardiovascular diseases.114 In the Norwegian hospital case-control study, Dahm et al found new associations between single nucleotide polymorphisms (SNPs): seventeen SNPs and one SNP belonging to the gene encoding P-selectin were associated with postpartum VTE.115
Physical Examination
Signs and symptoms of VTE in pregnancy are similar to those in non-pregnant individuals, and they vary between DVT and PE. These include shortness of breath, tachycardia, leg pain or swelling, pelvic discomfort, and chest pain. Shortness of breath is the most common presenting symptom (34.7%), followed by tachycardia (30.4%), leg pain or weakness (9.6%), and chest pain (13%).116 Thus, it is essential to understand how the accuracy of common symptoms or findings changes during the antepartum or peripartum period. Although there are few validating studies on this population, the DIPEP analysis provided some insight, as presented in the modified Table 3.
 |
Table 3 Diagnostic Accuracy of Presenting Features as Calculated in the Study Population of DiPEP |
Chan et al created a clinical prediction tool that promises to make the diagnosis of DVT in pregnant women in the first trimester more reliable. It includes three clinical parameters: (i) left lower extremity symptoms, (ii) difference in calf circumference of more than 2 cm, and (iii) presentation in the first trimester, collectively called the LEFt rule. The LEFt rule can be used in cases where the initial diagnostic workup with compressive ultrasound (CUS) is equivocal.97
Imaging
As discussed in detail in the existing literature, lung ventilation/perfusion scintigraphy (V/Q scan) and (CTPA) are widely used to evaluate PE in pregnancy.82,117 Ventilation/perfusion single photon emission computed tomography (V/Q SPECT) is a promising technique that offers higher sensitivity than planar V/Q and requires a lower radiation dose than CTPA. Despite rapid adoption in other advanced countries, V/Q SPECT remains relatively uncommon in the United States.118
Planar lung V/Q scan was a standard test for non-pregnant adults with suspected PE until the turn of the century, and it continues to be a routine test during pregnancy. Guidelines recommend perfusion-only scintigraphy (including half-dose perfusion scintigraphy) in pregnant patients with normal chest radiographs to reduce maternal and fetal radiation exposure.82,119 Ventilation/perfusion scans are a valuable alternative for patients with CKD or anaphylaxis where CTPA is generally contraindicated. However, they should be avoided in asthmatic patients or patients with severe lung disease. Disadvantages of V/Q scans include limited availability at some centers, longer test completion time, slightly higher fetal radiation dose, and inability to identify alternative diagnoses (ie, if the result is indeterminate or negative for PE).
When transport is an issue in hemodynamically unstable patients, echocardiographic evidence of RV pressure overload strongly suggests the presence of PE in patients with high pretest probability and no other likely causes of RV dysfunction (class I, level C).82 Both in the general population and in pregnant patients, echocardiographic evidence of RV dysfunction in stable patients contributes to PE severity assessment and assists in clinical decision-making.
Point of care ultrasound (POCUS) has brought a revolution in the diagnostic world, giving the opportunity to clinicians to diagnose dangerous urgent conditions without relying to a radiologist. POCUS may not have an established role in diagnosing PE, although there are signs with decent diagnostic accuracy.120 Unlike PE, POCUS has tremendous capabilities when it comes to the diagnosis of DVT. There have been numerous studies so far showing that, with the right training, internists, emergency and critical care physicians can match the accuracy of radiologists when it comes to the diagnosis of DVT.121,122 Serial compression Doppler ultrasonography has the same sensitivity and specificity to exclude deep vein thrombosis in pregnant women when compared to studies involving men and nonpregnant women, therefore providing a valuable weapon in our diagnostic arsenal.123
Advanced Therapies
Most VTE cases in pregnancy will resolve favorably with anticoagulation alone. However, cases of massive PE often times require escalation of care to advanced therapies.124 These therapies include systemic thrombolysis, catheter-directed thrombectomy/thrombolysis, surgical thrombectomy, or extracorporeal membrane oxygenation (ECMO).10 Although the existing literature is limited and it remains a conflicting topic, advanced treatment options can also be considered in cases with sub-massive PE (right ventricular dysfunction or myocardial necrosis without hypotension).125
Systemic thrombolysis can be used in pregnancy if indicated, as mentioned above. Based on a few cases of thrombolysis in pregnancy, a literature review reported 2.8% (4/141) deaths of pregnant women and 1.4% (2/141) neonatal deaths.126 Transplacental passage of tissue plasminogen activator and streptokinase is negligible and has not been linked with fetal coagulopathy or other malformations.127 Although there is no robust data comparing thrombolysis outcomes between pregnant women and the general population, a meta-analysis of studies on the use of systemic thrombolysis in antepartum and postpartum women reported a 28.4% risk for major bleeding (primarily vaginal hemorrhage or intra-abdominal bleeding depending on the mode of delivery).128
In the general population, IVC filters are considered when anticoagulation therapy is contraindicated, ineffective (recurrent VTE on full-dose anticoagulation therapy), or not well tolerated because of complications such as heparin-induced thrombocytopenia or heparin allergy.72 So far, there are no randomized clinical trials to assess the efficacy or risks of IVC filter placement in pregnancy, but in general, there is no mechanistic rationale for suggesting a different approach in pregnancy.
Surgical thrombectomy, percutaneous catheter thrombectomy, and extracorporeal membrane oxygenation (ECMO) are other invasive treatment options for VTE in pregnancy. Out of 127 peripartum women with PE, 36 were treated with classic thrombectomy, 7 with percutaneous catheter thrombectomy, and three were treated with ECMO and anticoagulation. Patients treated with surgical thrombectomy had a survival rate of 86%, a significant bleeding rate of 20%, a fetal death rate of 20%, and a premature delivery rate of 8%. All patients who underwent percutaneous thrombectomy survived (rate of 100%), the major bleeding rate was 20%, and the fetal death rate was 25%. In 2/7 women, this method was insufficient and led to escalation with other treatments (ECMO or surgical thrombectomy). ECMO for 4–10 days was used in 3/127 cases. All patients survived without any significant bleeding, and there was one documented premature delivery.129 Although this data come from a small sample, it suggests that percutaneous and surgical thrombectomy are noteworthy alternatives to thrombolysis, especially early postpartum, to avoid the risk of massive postpartum hemorrhage as a complication of thrombolytics. Skilled medical professionals should conduct these procedures in specialized centers with available supportive measures (cardiopulmonary bypass).125
Multidisciplinary Approach
In the peripartum period, the decision for anticoagulation should be ideally taken with the help of an obstetrician with expertise in thrombosis, an MFM subspecialist, or a “thrombologists.” A multidisciplinary team approach is optimal due to the complexity of the condition and the need for sub-specialized care. Massive PE in pregnancy is life-threatening for the mother and the fetus. Therefore, life-saving therapies such as systemic thrombolysis, surgical thrombectomy, catheter-directed thrombectomy, or extracorporeal membrane oxygenation (ECMO) should not be withheld. In such cases, treatment must be provided by a multidisciplinary team, including but not limited to MFM (maternal-fetal medicine), VTE experts (including interventional radiology and vascular surgery as appropriate), and obstetric anesthesia. Lately, there has been a shift toward the creation of Pulmonary Embolism Response Teams (PERTs). Their role is to anticipate and facilitate coordination of care in cases of severe PE that necessitate the input of specialists from different fields. Those teams have been successfully utilized in cases of severe PE in pregnancy with great results.130 Furthermore, for those with conditions that warrant treatments other than anticoagulants (ie, antithrombin concentrate) and those at increased risk for both thrombosis and bleeding (ie, concomitant von Willebrand disease or significant thrombocytopenia), involvement of thrombologists and hematologists is recommended. As suggested by Bannow et al, postpartum patients should follow up with their primary care doctor in 1–2 weeks postpartum in order to discuss their postpartum anticoagulation plan. Nurse visits and telehealth are reasonable, but in settings where this approach is not feasible due to resource limitations, access to a reliable contact with 24-hour availability is essential.131
Conclusions
It is well established that the risk of VTE is higher in the peripartum period, primarily due to concomitant physiologic changes. The need to identify high-risk women, diagnose them and treat them effectively is evident, given that VTE significantly contributes to fetal and maternal mortality. VTE in pregnancy can be a diagnostic conundrum due to the physical and laboratory findings shared between normal pregnancy and systemic thrombosis. The knowledge of the accuracy of specific physical findings and symptoms and the risk each individual carries based on comorbidities and laboratory findings may help clinicians diagnose VTE promptly. As in the general population, diagnoses of DVT are made optimally by following diagnostic algorithms, including MR and CT venography, D-dimers, and serial CUS. When PE is suspected, X-ray, CTPA, V/Q scan, and possibly TTE can lead to a diagnosis or assist with decision-making. Preventing and treating PE in the obstetric population is a challenge not only because of the paucity of data regarding the safety and efficacy of anticoagulants in such patients but also because of the potential hazard that this may pose to the mother and the developing fetus. The primary anticoagulation choice in pregnancy is LMWH which should be administered for at least three months. Advanced treatments such as thrombolysis, IVC filters, and mechanical methods of thrombus removal can be associated with significant fetal morbidity and mortality but should be considered in challenging cases: failure of other treatments, massive or sub-massive PE, or acute limb-threatening DVT. Despite the radical advancements in diagnosing and treating VTE in the general population, a disproportionate amount of studies have investigated the accuracy, efficacy, and safety of the most commonly used tests and therapies in pregnant or postpartum women. A multidisciplinary approach is needed for such a high-risk and delicate population, especially for complicated cases requiring advanced treatments.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Morris JM, Algert CS, Roberts CL. Incidence and risk factors for pulmonary embolism in the postpartum period. J Thromb Haemost. 2010;8(5):998–1003. doi:10.1111/j.1538-7836.2010.03794.x
2. Bourjeily G, Paidas M, Khalil H, Rosene-Montella K, Rodger M. Pulmonary embolism in pregnancy. Lancet. 2010;375(9713):500–512. doi:10.1016/S0140-6736(09)60996-X
3. Chang J, Elam-Evans LD, Berg CJ, et al. Pregnancy-related mortality surveillance--United States, 1991--1999. MMWR Surveill Summ. 2003;52(2):1–8.
4. Simpson EL, Lawrenson RA, Nightingale AL, Farmer RD. Venous thromboembolism in pregnancy and the puerperium: incidence and additional risk factors from a London perinatal database. BJOG. 2001;108(1):56–60. doi:10.1111/j.1471-0528.2001.00004.x
5. Heit JA, Kobbervig CE, James AH, Petterson TM, Bailey KR, Melton LJ. Trends in the incidence of venous thromboembolism during pregnancy or postpartum: a 30-year population-based study. Ann Intern Med. 2005;143(10):697–706. doi:10.7326/0003-4819-143-10-200511150-00006
6. Greer IA. Thrombosis in pregnancy: maternal and fetal issues. Lancet. 1999;353(9160):1258–1265. doi:10.1016/S0140-6736(98)10265-9
7. McColl MD, Ramsay JE, Tait RC, et al. Risk factors for pregnancy-associated venous thromboembolism. Thromb Haemost. 1997;78(4):1183–1188.
8. Kourlaba G, Relakis J, Kontodimas S, Holm MV, Maniadakis N. A systematic review and meta-analysis of the epidemiology and burden of venous thromboembolism among pregnant women. Int J Gynaecol Obstet. 2016;132(1):4–10. doi:10.1016/j.ijgo.2015.06.054
9. Pomp ER, Lenselink AM, Rosendaal FR, Doggen CJM. Pregnancy, the postpartum period and prothrombotic defects: risk of venous thrombosis in the MEGA study. J Thromb Haemost. 2008;6(4):632–637. doi:10.1111/j.1538-7836.2008.02921.x
10. Bates SM, Rajasekhar A, Middeldorp S, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: venous thromboembolism in the context of pregnancy. Blood Adv. 2018;2(22):3317–3359. doi:10.1182/bloodadvances.2018024802
11. Martinelli I, De Stefano V, Taioli E, Paciaroni K, Rossi E, Mannucci PM. Inherited thrombophilia and first venous thromboembolism during pregnancy and puerperium. Thromb Haemost. 2002;87(5):791–795.
12. Ginsberg JS, Brill-Edwards P, Burrows RF, et al. Venous thrombosis during pregnancy: leg and trimester of presentation. Thromb Haemost. 1992;67(5):519–520.
13. James AH, Jamison MG, Brancazio LR, Myers ER. Venous thromboembolism during pregnancy and the postpartum period: incidence, risk factors, and mortality. Am J Obstet Gynecol. 2006;194(5):1311–1315. doi:10.1016/j.ajog.2005.11.008
14. James AH, Tapson VF, Goldhaber SZ. Thrombosis during pregnancy and the postpartum period. Am J Obstet Gynecol. 2005;193(1):216–219. doi:10.1016/j.ajog.2004.11.037
15. Bates SM, Greer IA, Middeldorp S, Veenstra DL, Prabulos AM, Vandvik PO. VTE, thrombophilia, antithrombotic therapy, and pregnancy: antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e691S–e736S. doi:10.1378/chest.11-2300
16. Blondon M, Harrington LB, Righini M, Boehlen F, Bounameaux H, Smith NL. Racial and ethnic differences in the risk of postpartum venous thromboembolism: a population-based, case-control study. J Thromb Haemost. 2014;12(12):2002–2009. doi:10.1111/jth.12747
17. Bremme KA. Haemostatic changes in pregnancy. Best Pract Res Clin Haematol. 2003;16(2):153–168. doi:10.1016/s1521-6926(03)00021-5
18. Dalaker K, Prydz H. The coagulation factor VII in pregnancy. Br J Haematol. 1984;56(2):233–241. doi:10.1111/j.1365-2141.1984.tb03951.x
19. Thornton P, Douglas J. Coagulation in pregnancy. Best Pract Res Clin Obstet Gynaecol. 2010;24(3):339–352. doi:10.1016/j.bpobgyn.2009.11.010
20. Estellés A, Gilabert J, Andrés C, España F, Aznar J. Plasminogen activator inhibitors type 1 and type 2 and plasminogen activators in amniotic fluid during pregnancy. Thromb Haemost. 1990;64(2):281–285.
21. Sheu JR, Hsiao G, Lin WY, et al. Mechanisms involved in agonist-induced hyperaggregability of platelets from normal pregnancy. J Biomed Sci. 2002;9(1):17–25. doi:10.1007/BF02256574
22. Janes SL, Goodall AH. Flow cytometric detection of circulating activated platelets and platelet hyper-responsiveness in preeclampsia and pregnancy. Clin Sci. 1994;86(6):731–739. doi:10.1042/cs0860731
23. Aharon A, Katzenell S, Tamari T, Brenner B. Microparticles bearing tissue factor and tissue factor pathway inhibitor in gestational vascular complications. J Thromb Haemost. 2009;7(6):1047–1050. doi:10.1111/j.1538-7836.2009.03342.x
24. Soma-Pillay P, Nelson-Piercy C, Tolppanen H, Mebazaa A. Physiological changes in pregnancy. Cardiovasc J Afr. 2016;27(2):89–94. doi:10.5830/CVJA-2016-021
25. Sanghavi M, Rutherford JD. Cardiovascular physiology of pregnancy. Circulation. 2014;130(12):1003–1008. doi:10.1161/CIRCULATIONAHA.114.009029
26. Macklon NS, Greer IA, Bowman AW. An ultrasound study of gestational and postural changes in the deep venous system of the leg in pregnancy. Br J Obstet Gynaecol. 1997;104(2):191–197. doi:10.1111/j.1471-0528.1997.tb11043.x
27. James AH. Pregnancy-associated thrombosis. Hematology. 2009;2009(1):277–285. doi:10.1182/asheducation-2009.1.277
28. Carr MH, Towers CV, Eastenson AR, Pircon RA, Iriye BK, Adashek JA. Prolonged bedrest during pregnancy: does the risk of deep vein thrombosis warrant the use of routine heparin prophylaxis? J Matern Fetal Med. 1997;6(5):264–267. doi:10.1002/(SICI)1520-6661(199709/10)6:5<264::AID-MFM4>3.0.CO;2-E
29. Kovacevich GJ, Gaich SA, Lavin JP, et al. The prevalence of thromboembolic events among women with extended bed rest prescribed as part of the treatment for premature labor or preterm premature rupture of membranes. Am J Obstet Gynecol. 2000;182(5):1089–1092. doi:10.1067/mob.2000.105405
30. Abou-Ismail MY, Citla Sridhar D, Nayak L. Estrogen and thrombosis: a bench to bedside review. Thromb Res. 2020;192:40–51. doi:10.1016/j.thromres.2020.05.008
31. Daikoku T, Matsumoto H, Gupta RA, et al. Expression of hypoxia-inducible factors in the peri-implantation mouse uterus is regulated in a cell-specific and ovarian steroid hormone-dependent manner. Evidence for differential function of HIFs during early pregnancy. J Biol Chem. 2003;278(9):7683–7691. doi:10.1074/jbc.M211390200
32. Song G, Kim J, Bazer FW, Spencer TE. Progesterone and interferon tau regulate hypoxia-inducible factors in the endometrium of the ovine uterus. Endocrinology. 2008;149(4):1926–1934. doi:10.1210/en.2007-1530
33. Chen J, Khalil RA. Matrix metalloproteinases in normal pregnancy and preeclampsia. Prog Mol Biol Transl Sci. 2017;148:87–165. doi:10.1016/bs.pmbts.2017.04.001
34. James AH. Venous thromboembolism in pregnancy. Arterioscler Thromb Vasc Biol. 2009;29(3):326–331. doi:10.1161/ATVBAHA.109.184127
35. American College of Obstetricians and Gynecologists. ACOG practice bulletin No. 197: inherited Thrombophilias in Pregnancy. Obstet Gynecol. 2018;132(1):e18–e34. doi:10.1097/AOG.0000000000002703
36. Ridker PM. Ethnic distribution of factor V Leiden in 4047 men and women. JAMA. 1997;277(16):1305. doi:10.1001/jama.1997.03540400055031
37. Nikolaeva MG, Momot AP, Zainulina MS, Yasafova NN, Taranenko IA. Pregnancy complications in G20210A mutation carriers associated with high prothrombin activity. Thromb J. 2021;19(1):41. doi:10.1186/s12959-021-00289-4
38. Mekaj Y, Lulaj S, Daci F, et al. Prevalence and role of Antithrombin III, protein C and protein S deficiencies and activated protein C resistance in Kosovo women with recurrent pregnancy loss during the first trimester of pregnancy. J Hum Reprod Sci. 2015;8(4):224. doi:10.4103/0974-1208.170407
39. Pabinger I, Schneider B. Thrombotic risk in hereditary antithrombin III, Protein C, or Protein S deficiency. Arterioscler Thromb Vasc Biol. 1996;16(6):742–748. doi:10.1161/01.ATV.16.6.742
40. Makris M. Thrombophilia: grading the risk. Blood. 2009;113(21):5038–5039. doi:10.1182/blood-2009-02-203281
41. Zotz RB, Gerhardt A, Scharf RE. Inherited thrombophilia and gestational venous thromboembolism. Best Pract Res Clin Haematol. 2003;16(2):243–259. doi:10.1016/s1521-6926(03)00022-7
42. Pabinger I, Grafenhofer H, Kaider A, et al. Risk of pregnancy-associated recurrent venous thromboembolism in women with a history of venous thrombosis. J Thromb Haemost. 2005;3(5):949–954. doi:10.1111/j.1538-7836.2005.01307.x
43. Khare M, Nelson-Piercy C. Acquired thrombophilias and pregnancy. Best Pract Res Clin Obstet Gynaecol. 2003;17(3):491–507. doi:10.1016/S1521-6934(03)00013-0
44. Lechner K, Pabinger-Fasching I. Lupus anticoagulants and thrombosis. Pathophysiol Haemost Thromb. 1985;15(4):254–262. doi:10.1159/000215157
45. Gastineau DA, Kazmier FJ, Nichols WL, Bowie EJW. Lupus anticoagulant: an analysis of the clinical and laboratory features of 219 cases. Am J Hematol. 1985;19(3):265–275. doi:10.1002/ajh.2830190308
46. Khamashta MA, Cuadrado MJ, Mujic F, Taub NA, Hunt BJ, Hughes GRV. The management of thrombosis in the antiphospholipid-antibody syndrome. N Engl J Med. 1995;332(15):993–997. doi:10.1056/NEJM199504133321504
47. Branch DW. Antiphospholipid antibodies and pregnancy: maternal implications. Semin Perinatol. 1990;14(2):139–146.
48. Lima F, Khamashta MA, Buchanan NM, Kerslake S, Hunt BJ, Hughes GR. A study of sixty pregnancies in patients with the antiphospholipid syndrome. Clin Exp Rheumatol. 1996;14(2):131–136.
49. Ringrose DK. Anaesthesia and the antiphospholipid syndrome: a review of 20 obstetric patients. Int J Obstet Anesth. 1997;6(2):107–111. doi:10.1016/S0959-289X(97)80007-6
50. Bates SM. Management of pregnant women with thrombophilia or a history of venous thromboembolism. Hematology. 2007;2007(1):143–150. doi:10.1182/asheducation-2007.1.143
51. Chan WS, Spencer FA, Ginsberg JS. Anatomic distribution of deep vein thrombosis in pregnancy. CMAJ. 2010;182(7):657–660. doi:10.1503/cmaj.091692
52. Hull RD, Raskob GE, Carter CJ. Serial impedance plethysmography in pregnant patients with clinically suspected deep-vein thrombosis. Clinical validity of negative findings. Ann Intern Med. 1990;112(9):663–667. doi:10.7326/0003-4819-112-9-663
53. RCOG. Thromboembolic disease in pregnancy and the puerperium: acute management; green-top guideline No. 37b; 2001.
54. Chan WS, Rey E, Kent NE, et al. Venous thromboembolism and antithrombotic therapy in pregnancy. J Obstet Gynaecol Can. 2014;36(6):527–553. doi:10.1016/s1701-2163(15)30569-7
55. Dronkers CEA, Srámek A, Huisman MV, Klok FA. Accurate diagnosis of iliac vein thrombosis in pregnancy with magnetic resonance direct thrombus imaging (MRDTI). BMJ Case Rep. 2016;2016. doi:10.1136/bcr-2016-218091
56. Torkzad MR, Bremme K, Hellgren M, et al. Magnetic resonance imaging and ultrasonography in diagnosis of pelvic vein thrombosis during pregnancy. Thromb Res. 2010;126(2):107–112. doi:10.1016/j.thromres.2010.05.011
57. Damodaram M, Kaladindi M, Luckit J, Yoong W. D-dimers as a screening test for venous thromboembolism in pregnancy: is it of any use? J Obstet Gynaecol. 2009;29(2):101–103. doi:10.1080/01443610802649045
58. Levy MS, Spencer F, Ginsberg JS, Anderson JAM. Reading between the (guidelines). Management of submassive pulmonary embolism in the first trimester of pregnancy. Thromb Res. 2008;121(5):705–707. doi:10.1016/j.thromres.2007.07.001
59. To MS, Hunt BJ, Nelson-Piercy C. A negative D-dimer does not exclude venous thromboembolism (VTE) in pregnancy. J Obstet Gynaecol. 2008;28(2):222–223. doi:10.1080/01443610801915975
60. Gibson PS, Powrie R. Anticoagulants and pregnancy: when are they safe? Cleve Clin J Med. 2009;76(2):113–127. doi:10.3949/ccjm.75a.072272
61. Krivak TC, Zorn KK. Venous thromboembolism in obstetrics and gynecology. Obstet Gynecol. 2007;109(3):761–777. doi:10.1097/01.AOG.0000255819.10187.70
62. Greer IA, Nelson-Piercy C. Low-molecular-weight heparins for thromboprophylaxis and treatment of venous thromboembolism in pregnancy: a systematic review of safety and efficacy. Blood. 2005;106(2):401–407. doi:10.1182/blood-2005-02-0626
63. Segal JB, Streiff MB, Hofmann LV, Thornton K, Bass EB. Management of venous thromboembolism: a systematic review for a practice guideline. Ann Intern Med. 2007;146(3):211–222. doi:10.7326/0003-4819-146-3-200702060-00150
64. van Dongen CJJ, van den Belt AGM, Prins MH, Lensing AWA. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for venous thromboembolism. Cochrane Database Syst Rev. 2004;CD001100. doi:10.1002/14651858.CD001100.pub2
65. Richter C, Sitzmann J, Lang P, Weitzel H, Huch A, Huch R. Excretion of low molecular weight heparin in human milk. Br J Clin Pharmacol. 2001;52(6):708–710. doi:10.1046/j.0306-5251.2001.01517.x
66. Bates SM, Greer IA, Hirsh J, Ginsberg JS. Use of antithrombotic agents during pregnancy: the seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest. 2004;126(3 Suppl):627S–644S. doi:10.1378/chest.126.3_suppl.627S
67. American College of Obstetricians and Gynecologists. ACOG practice bulletin No. 196: thromboembolism in pregnancy. Obstet Gynecol. 2011;118(3):718–729. doi:10.1097/AOG.0b013e3182310c4c
68. Büller HR, Agnelli G, Hull RD, Hyers TM, Prins MH, Raskob GE. Antithrombotic therapy for venous thromboembolic disease: the seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest. 2004;126(3 Suppl):401S–428S. doi:10.1378/chest.126.3_suppl.401S
69. Schulman S, Granqvist S, Holmström M, et al. The duration of oral anticoagulant therapy after a second episode of venous thromboembolism. The duration of anticoagulation trial study group. N Engl J Med. 1997;336(6):393–398. doi:10.1056/NEJM199702063360601
70. Bagaria SJ, Bagaria VB. Strategies for diagnosis and prevention of venous thromboembolism during pregnancy. J Pregnancy. 2011;2011:206858. doi:10.1155/2011/206858
71. Middleton P, Shepherd E, Gomersall JC. Venous thromboembolism prophylaxis for women at risk during pregnancy and the early postnatal period. Cochrane Database Syst Rev. 2021;3(3):CD001689. doi:10.1002/14651858.CD001689.pub4
72. Harris SA, Velineni R, Davies AH. Inferior vena cava filters in pregnancy: a systematic review. J Vasc Interv Radiol. 2016;27(3):354–60.e8. doi:10.1016/j.jvir.2015.11.024
73. Pfeifer GW. Distribution and placental transfer of 131-I streptokinase. Australas Ann Med. 1970;19 Suppl 1:17–18. doi:10.1111/imj.1970.19.s1.17
74. Holden EL, Ranu H, Sheth A, Shannon MS, Madden BP. Thrombolysis for massive pulmonary embolism in pregnancy--a report of three cases and follow up over a two year period. Thromb Res. 2011;127(1):58–59. doi:10.1016/j.thromres.2010.06.003
75. te Raa GD, Ribbert LSM, Snijder RJ, Biesma DH. Treatment options in massive pulmonary embolism during pregnancy; a case-report and review of literature. Thromb Res. 2009;124(1):1–5. doi:10.1016/j.thromres.2009.03.001
76. Ahearn GS, Hadjiliadis D, Govert JA, Tapson VF. Massive pulmonary embolism during pregnancy successfully treated with recombinant tissue plasminogen activator: a case report and review of treatment options. Arch Intern Med. 2002;162(11):1221–1227. doi:10.1001/archinte.162.11.1221
77. Bates SM, Middeldorp S, Rodger M, James AH, Greer I. Guidance for the treatment and prevention of obstetric-associated venous thromboembolism. J Thromb Thrombolysis. 2016;41(1):92–128. doi:10.1007/s11239-015-1309-0
78. Dresang LT, Fontaine P, Leeman L, King VJ. Venous thromboembolism during pregnancy. Am Fam Physician. 2008;77(12):1709–1716.
79. Maughan BC, Marin M, Han J, et al. Venous thromboembolism during pregnancy and the postpartum period: risk factors, diagnostic testing, and treatment. Obstet Gynecol Surv. 2022;77(7):433–444. doi:10.1097/OGX.0000000000001043
80. Biron-Andreani C, Schved JF, Daures JP. Factor V Leiden mutation and pregnancy-related venous thromboembolism: what is the exact risk? Results from a meta-analysis. Thromb Haemost. 2006;96(1):14–18. doi:10.1160/TH06-02-0086
81. Sultan AA, Tata LJ, West J, et al. Risk factors for first venous thromboembolism around pregnancy: a population-based cohort study from the United Kingdom. Blood. 2013;121(19):3953–3961. doi:10.1182/blood-2012-11-469551
82. Konstantinides V, Meyer G, Becattini C, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41(4):543–603. doi:10.1093/eurheartj/ehz405
83. Jacobsen AF, Skjeldestad FE, Sandset PM. Ante- and postnatal risk factors of venous thrombosis: a hospital-based case-control study. J Thromb Haemost. 2008;6(6):905–912. doi:10.1111/j.1538-7836.2008.02961.x
84. Kim YH, Pfaller B, Marson A, Yim HW, Huang V, Ito S. The risk of venous thromboembolism in women with inflammatory bowel disease during pregnancy and the postpartum period: a systematic review and meta-analysis. Medicine. 2019;98(38):e17309. doi:10.1097/MD.0000000000017309
85. Sultan AA, West J, Tata LJ, Fleming KM, Nelson-Piercy C, Grainge MJ. Risk of first venous thromboembolism in and around pregnancy: a population-based cohort study. Br J Haematol. 2012;156(3):366–373. doi:10.1111/j.1365-2141.2011.08956.x
86. Clowse MEB, Jamison M, Myers E, James AH. A national study of the complications of lupus in pregnancy. Am J Obstet Gynecol. 2008;199(2):127.e1–6. doi:10.1016/j.ajog.2008.03.012
87. Duffett L, Castellucci LA, Forgie MA. Pulmonary embolism: update on management and controversies. BMJ. 2020;370:m2177. doi:10.1136/bmj.m2177
88. De Stefano V, Martinelli I, Rossi E, et al. The risk of recurrent venous thromboembolism in pregnancy and puerperium without antithrombotic prophylaxis. Br J Haematol. 2006;135(3):386–391. doi:10.1111/j.1365-2141.2006.06317.x
89. Abe K, Kuklina EV, Hooper WC, Callaghan WM. Venous thromboembolism as a cause of severe maternal morbidity and mortality in the United States. Semin Perinatol. 2019;43(4):200–204. doi:10.1053/j.semperi.2019.03.004
90. Sare GM, Gray LJ, Bath PMW. Association between hormone replacement therapy and subsequent arterial and venous vascular events: a meta-analysis. Eur Heart J. 2008;29(16):2031–2041. doi:10.1093/eurheartj/ehn299
91. Gomes V, Deitcher SR. Risk of venous thromboembolic disease associated with hormonal contraceptives and hormone replacement therapy: a clinical review. Arch Intern Med. 2004;164(18):1965–1976. doi:10.1001/archinte.164.18.1965
92. Rogolino A, Coccia ME, Fedi S, et al. Hypercoagulability, high tissue factor and low tissue factor pathway inhibitor levels in severe ovarian hyperstimulation syndrome: possible association with clinical outcome. Blood Coagul Fibrinolysis. 2003;14(3):277–282. doi:10.1097/01.mbc.0000061296.28953.d0
93. Biron C, Galtier-Dereure F, Rabesandratana H, et al. Hemostasis parameters during ovarian stimulation for in vitro fertilization: results of a prospective study. Fertil Steril. 1997;67(1):104–109. doi:10.1016/s0015-0282(97)81864-x
94. Phillips LL, Gladstone W, Vande Wiele R. Studies of the coagulation and fibrinolytic systems in hyperstimulation syndrome after administration of human gonadotropins. J Reprod Med. 1975;14(4):138–143.
95. Bauersachs RM, Dudenhausen J, Faridi A, et al. Risk stratification and heparin prophylaxis to prevent venous thromboembolism in pregnant women. Thromb Haemost. 2007;98(6):1237–1245. doi:10.1160/th07-05-0329
96. Alijotas-Reig J, Ferrer-Oliveras R; EUROAPS Study Group. The European Registry on Obstetric Antiphospholipid Syndrome (EUROAPS): a preliminary first year report. Lupus. 2012;21(7):766–768. doi:10.1177/0961203312440058
97. Chan WS, Lee A, Spencer FA, et al. Predicting deep venous thrombosis in pregnancy: out in “LEFt” field? Ann Intern Med. 2009;151(2):85–92. doi:10.7326/0003-4819-151-2-200907210-00004
98. Varrias D, Sharma N, Hentz R, et al. Clinical significance of unexplained persistent sinus tachycardia in women with structurally normal heart during the peripartum period. BMC Pregnancy Childbirth. 2022;22(1):677. doi:10.1186/s12884-022-05012-3
99. Goodacre S, Horspool K, Nelson-Piercy C, et al. The DiPEP study: an observational study of the diagnostic accuracy of clinical assessment, D-dimer and chest x-ray for suspected pulmonary embolism in pregnancy and postpartum. BJOG. 2019;126(3):383–392. doi:10.1111/1471-0528.15286
100. Gregory E. Nursing practice management: Karen, aged 15 years, has an above-the-knee amputation. The Journal of School Nursing. 1992;8(1):30, 32.
101. McLintock C, Brighton T, Chunilal S, et al. Recommendations for the diagnosis and treatment of deep venous thrombosis and pulmonary embolism in pregnancy and the postpartum period. Aust N Z J Obstet Gynaecol. 2012;52(1):14–22. doi:10.1111/j.1479-828X.2011.01361.x
102. van der Pol LM, Tromeur C, Bistervels IM, et al. Pregnancy-adapted years algorithm for diagnosis of suspected pulmonary embolism. N Engl J Med. 2019;380(12):1139–1149. doi:10.1056/NEJMoa1813865
103. Fuller GW, Nelson-Piercy C, Hunt BJ, et al. Consensus-derived clinical decision rules to guide advanced imaging decisions for pulmonary embolism in pregnancy and the postpartum period. Eur J Emerg Med. 2018;25(3):221–222. doi:10.1097/MEJ.0000000000000477
104. Chan WS, Lee A, Spencer FA, et al. D-dimer testing in pregnant patients: towards determining the next “level” in diagnosing deep vein thrombosis. J Thromb Haemost. 2010;8(5):1004–1011. doi:10.1111/j.1538-7836.2010.03783.x
105. Phillips JJ, Straiton J, Staff RT. Planar and SPECT ventilation/perfusion imaging and computed tomography for the diagnosis of pulmonary embolism: a systematic review and meta-analysis of the literature, and cost and dose comparison. Eur J Radiol. 2015;84(7):1392–1400. doi:10.1016/j.ejrad.2015.03.013
106. Lee SY, Rhee CM, Leung AM, Braverman LE, Brent GA, Pearce EN. A review: radiographic iodinated contrast media-induced thyroid dysfunction. J Clin Endocrinol Metab. 2015;100(2):376–383. doi:10.1210/jc.2014-3292
107. ACOG Committee on Obstetric Practice. ACOG committee opinion No. 723: guidelines for diagnostic imaging during pregnancy and lactation. Obstet Gynecol. 2017;130(4):e210–e216. doi:10.1111/j.1479-828X.2011.01361.x
108. Astani SA, Davis LC, Harkness BA, Supanich MP, Dalal I. Detection of pulmonary embolism during pregnancy: comparing radiation doses of CTPA and pulmonary scintigraphy. Nucl Med Commun. 2014;35(7):704–711. doi:10.1097/MNM.0000000000000114
109. Perisinakis K, Seimenis I, Tzedakis A, Damilakis J. Perfusion scintigraphy versus 256-slice CT angiography in pregnant patients suspected of pulmonary embolism: comparison of radiation risks. J Nucl Med. 2014;55(8):1273–1280. doi:10.2967/jnumed.114.137968
110. Nguyen ET, Hague C, Manos D, et al. Canadian Society of Thoracic Radiology/Canadian association of radiologists best practice guidance for investigation of acute pulmonary embolism, part 1: acquisition and safety considerations. Can Assoc Radiol J. 2022;73(1):203–213. doi:10.1177/08465371211000737
111. Bellesini M, Robert-Ebadi H, Combescure C, Dedionigi C, Le Gal G, Righini M. D-dimer to rule out venous thromboembolism during pregnancy: a systematic review and meta-analysis. J Thromb Haemost. 2021;19(10):2454–2467. doi:10.1111/jth.15432
112. Bezemer ID, van der Meer FJM, Eikenboom JCJ, Rosendaal FR, Doggen CJM. The value of family history as a risk indicator for venous thrombosis. Arch Intern Med. 2009;169(6):610–615. doi:10.1001/archinternmed.2008.589
113. Trégouët DA, Heath S, Saut N, et al. Common susceptibility alleles are unlikely to contribute as strongly as the FV and ABO loci to VTE risk: results from a GWAS approach. Blood. 2009;113(21):5298–5303. doi:10.1182/blood-2008-11-190389
114. Spanos M, Gokulnath P, Chatterjee E, Guoping L, Varrias D, Saumya D. Expanding the horizon of EV-RNAs: lncRNAs in EVs as biomarkers for disease pathways. Extracell Vesicle. 2023;2:100025. doi:10.1016/j.vesic.2023.100025
115. Dahm AEA, Bezemer ID, Bergrem A, et al. Candidate gene polymorphisms and the risk for pregnancy-related venous thrombosis. Br J Haematol. 2012;157(6):753–761. doi:10.1111/j.1365-2141.2012.09121.x
116. Heyl PS, Sappenfield WM, Burch D, Hernandez LE, Kavanaugh VM, Hill WC. Pregnancy-related deaths due to pulmonary embolism: findings from two state-based mortality reviews. Matern Child Health J. 2013;17(7):1230–1235. doi:10.1007/s10995-012-1117-5
117. American College of Obstetricians and Gynecologists Committee on Practice Bulletins—Obstetrics. ACOG practice bulletin No. 196: thromboembolism in pregnancy. Obstet Gynecol. 2018;132(1):e1–e17. doi:10.1097/AOG.0000000000002706
118. Le Roux PY, Pelletier-Galarneau M, De Laroche R, et al. Pulmonary scintigraphy for the diagnosis of acute pulmonary embolism: a survey of current practices in Australia, Canada, and France. J Nucl Med. 2015;56(8):1212–1217. doi:10.2967/jnumed.115.157743
119. Linnemann B, Bauersachs R, Rott H, et al. Diagnosis of pregnancy-associated venous thromboembolism - position paper of the working group in women’s health of the society of thrombosis and haemostasis (GTH). Vasa. 2016;45(2):87–101. doi:10.1024/0301-1526/a000503
120. Lieveld A, Heldeweg MLA, Smit JM, et al. Multi-organ point-of-care ultrasound for detection of pulmonary embolism in critically ill COVID-19 patients – a diagnostic accuracy study. J Crit Care. 2022;69:153992. doi:10.1016/j.jcrc.2022.153992
121. Barrosse-Antle ME, Patel KH, Kramer JA, Baston CM. Point-of-care ultrasound for bedside diagnosis of lower extremity DVT. Chest. 2021;160(5):1853–1863. doi:10.1016/j.chest.2021.07.010
122. Varrias D, Palaiodimos L, Balasubramanian P, et al. The use of point-of-care ultrasound (POCUS) in the diagnosis of deep vein thrombosis. J Clin Med. 2021;10:3903. doi:10.3390/jcm10173903
123. Chan WS, Spencer FA, Lee AY, et al. Safety of withholding anticoagulation in pregnant women with suspected deep vein thrombosis following negative serial compression ultrasound and iliac vein imaging. CMAJ. 2013;185(4):E194–200. PMID: 23318405; PMCID: PMC3589327. doi:10.1503/cmaj.120895
124. Jaff MR, McMurtry MS, Archer SL, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123(16):1788–1830. doi:10.1161/CIR.0b013e318214914f
125. Kalaitzopoulos DR, Panagopoulos A, Samant S, et al. Management of venous thromboembolism in pregnancy. Thromb Res. 2022;211:106–113. doi:10.1016/j.thromres.2022.02.002
126. Sousa Gomes M, Guimarães M, Montenegro N. Thrombolysis in pregnancy: a literature review. J Matern Fetal Neonatal Med. 2019;32(14):2418–2428. doi:10.1080/14767058.2018.1434141
127. Capstick T, Henry MT. Efficacy of thrombolytic agents in the treatment of pulmonary embolism. Eur Respir J. 2005;26(5):864–874. doi:10.1183/09031936.05.00002505
128. Marti C, John G, Konstantinides S, et al. Systemic thrombolytic therapy for acute pulmonary embolism: a systematic review and meta-analysis. Eur Heart J. 2015;36(10):605–614. doi:10.1093/eurheartj/ehu218
129. Martillotti G, Boehlen F, Robert-Ebadi H, Jastrow N, Righini M, Blondon M. Treatment options for severe pulmonary embolism during pregnancy and the postpartum period: a systematic review. J Thromb Haemost. 2017;15(10):1942–1950. doi:10.1111/jth.13802
130. Monteleone PP, Rosenfield K, Rosovsky RP. Multidisciplinary pulmonary embolism response teams and systems. Cardiovasc Diagn Ther. 2016;6(6):662–667. doi:10.21037/cdt.2016.11.05
131. Samuelson Bannow B, Federspiel JJ, Abel DE, Mauney L, Rosovsky RP, Bates SM. Multidisciplinary care of the pregnant patient with or at risk for venous thromboembolism: a recommended toolkit from the foundation for women and girls with blood disorders thrombosis subcommittee. J Thromb Haemost. 2023. doi:10.1016/j.jtha.2023.03.015
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Antithrombin Deficiency and Thrombosis: A Wide Clinical Scenario Reported in a Single Institution
Marco-Rico A, Marco-Vera P
Journal of Blood Medicine 2023, 14:499-506
Published Date: 1 September 2023
A Multicenter Study Assessing the Optimal Anticoagulation Strategies in COVID-19 Critically Ill Patients with New-Onset Atrial Fibrillation: Balancing Effectiveness and Safety
Al Sulaiman K, Aljuhani O, Korayem GB, Altebainawi AF, Alharbi A, Alalawi M, Joharji H, Almohsen RA, Faden RM, Alotaibi N, Alshalawi BS, Alkhushaym N, Alanazi FF, Alharbi A, Alqarni A, Samkari S, Alharbi B, Alshehab N, Alshehri RA, Vishwakarma R
International Journal of General Medicine 2024, 17:5611-5622
Published Date: 28 November 2024
Coexistence of Congenital Dysfibrinogenemia and Antiphospholipid Syndrome in Pregnancy: A Case Report
Wang Z, Mao S, Wang S, Zhang W, Jia C, Zhu T
International Journal of Women's Health 2025, 17:2885-2890
Published Date: 4 September 2025
Safety of Fondaparinux After Low-Molecular-Weight Heparin in Bleeding-Complicated High-Risk Pregnancies: A PSM Cohort Study
Yang H, Gao Y, Song X
International Journal of Women's Health 2026, 18:572932
Published Date: 8 April 2026