Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 15
Venetoclax Plus Blinatumoma as First Line Therapy for Newly Diagnosed Ph-Negative B-Cell Acute Lymphoblastic Leukemia
Authors Lei Y, Zhao X ![]() , Huang H, Duan L, Xu J, Miao K, Zhao H, Qiao C, Hong M, Qian S, Fan L, Zhu Y
, Huang H, Duan L, Xu J, Miao K, Zhao H, Qiao C, Hong M, Qian S, Fan L, Zhu Y ![]()
Received 29 July 2025
Accepted for publication 30 October 2025
Published 5 November 2025 Volume 2025:15 Pages 193—202
DOI https://doi.org/10.2147/BLCTT.S556608
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Wilson Gonsalves
Yutian Lei,1 Xiaoli Zhao,1 Huijun Huang,1 Limin Duan,1 Ji Xu,1 Kourong Miao,1 Huihui Zhao,2 Chun Qiao,1 Ming Hong,1 Sixuan Qian,1 Lei Fan,1 Yu Zhu1
1Department of Hematology, Jiangsu Province Hospital, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 2Department of Oncology, Nanjing second Hospital, Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China
Correspondence: Yu Zhu, Department of Hematology, Jiangsu Province Hospital, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China, Email [email protected]
Purpose: This study evaluated the efficacy and safety of a 14-day blinatumomab-venetoclax (BV) regimen as induction therapy for newly diagnosed Ph-negative B-cell acute lymphoblastic leukemia (B-ALL), focusing on rapid remission and tolerability in unfit patients.
Patients and Methods: Thirteen patients received venetoclax (100 mg on day 1, 200 mg on day 2, 300 mg on day 3, and 400 mg from days 4 to 14) with blinatumomab (9 to 28 ug/day) for 14 days. Bone marrow assessments were performed at days 14– 21. Primary endpoints were complete remission (CR) rate, minimal residual disease (MRD) negativity by flow cytometry, and adverse events.
Results: The CR rate after one cycle of BV regimen was 92.3% (12/13), and all patients achieved MRD-negativity; 91.7% (11/12) achieved MRD clearance by day 21. Grade 1– 2 cytokine release syndrome occurred in 46.2% (6/13; 1 grade 3). Hematologic toxicity included grade 3– 4 neutropenia (92.3%) and thrombocytopenia (46.2%), with only 30.8% febrile neutropenia. All AEs resolved rapidly with supportive care, allowing therapy to continue without interruption. At median follow-up of 283 days, 1-year relapse-free survival rate and overall survival rate were 60.6% and 83.3%.
Conclusion: The 14-day BV regimen induced rapid deep remission (91.7% MRD-negative by day 21) with manageable toxicity in Ph-negative B-ALL. Synergistic T-cell activation by venetoclax may explain enhanced efficacy.
Keywords: venetoclax, blinatumomab, Ph-negative B-cell acute lymphoblastic leukemia
Introduction
Classic induction therapy for adult Philadelphia chromosome (Ph)-negative acute B-lymphoblastic leukemia (B-ALL) primarily involves multi-drug combination chemotherapy, with the aim of eliminating the majority of blasts and restoring normal hematopoiesis. However, due to the generally poor condition of patients at diagnosis, bone marrow suppression caused by cytotoxic agents and high-dose glucocorticoids administration, induction therapy sometimes leads to uncontrollable infection and early death. In recent years, the addition of immunotherapy agents has led to a trend of reducing the intensity of induction chemotherapy for adult Ph-negative B-ALL, especially in patients with weak physical fitness, baseline comorbidities, or organ dysfunction, which has significantly improved the efficacy and safety of induction therapy for these patients.
Blinatumomab, a bispecific monoclonal antibody targeting CD19 and redirecting CD3-positive T cells, has been increasingly employed in the consolidation treatment of CD19-positive B-ALL and in the salvage therapy for patients with relapsed or refractory disease, demonstrating encouraging therapeutic efficacy. For Ph-positive ALL, blinatumomab combined with potent tyrosine kinase inhibitors has been widely administered throughout the treatment course, improving the prognosis of patients remarkably.1,2 Nevertheless, single agent blinatumomab as frontline treatment remains suboptimal for newly diagnosed Ph-negative B-ALL. The unsatisfactory response for frontline administration of blinatumomab was considered mainly due to effector/target ratios caused by high leukemia burden and T cell exhaustion from immunosuppressive environment.3,4
Venetoclax, an oral BCL-2 inhibitor, has demonstrated efficacy and favorable tolerability in relapsed/refractory B-ALL according to retrospective small cohort studies.5,6 Promising remission rates are also shown in the frontline treatment of B-ALL when venetoclax is combined with chemotherapy or other targeted agents. Luskin et al reported a combination of venetoclax with mini-hyper-CVD in 19 patients with ALL, including 11 newly diagnosed cases aged ≥60 years (8 B-lineage cases). After two cycles, 10 patients achieved complete remission (CR) with minimal residual disease (MRD) negativity.7 A case report described long-term leukemia-free survival in an elderly Ph-negative B-ALL patient following sequential therapy with venetoclax, ruxolitinib, dexamethasone, and blinatumomab.8 Venetoclax was reported to be able to synergize with T-cell immunotherapy and enhance the cytotoxicity of T cell-based therapies against B-cell lines in vitro.9 We initially trialed venetoclax plus blinatumomab induction therapy in a cachectic elderly patient with newly diagnosed Ph-negative B-ALL and a history of gastrectomy for gastric cancer. This regimen led to a negative MRD status by flow cytometry rapidly, with no severe adverse event (AE) throughout the induction phase. The favorable outcome in this case led us to adopt and further evaluate this chemotherapy-free regimen in a subsequent series of eligible patients. Herein, we present the clinical outcomes and safety profile of this cohort.
Materials and Methods
Study Design and Patients
This single-center, retrospective case series included 13 consecutive adults with newly diagnosed Ph-negative B-ALL who received a chemotherapy-free induction regimen of venetoclax plus blinatumomab at Jiangsu Province Hospital between March 1, 2024, and March 31, 2025. The requirement for informed consent was waived by the Institutional Review Board for this retrospective analysis.
Patients were included in this analysis if they: (1) were aged 18 years or older; (2) had a confirmed diagnosis of newly diagnosed Ph-negative B-ALL with CD19 positivity confirmed by flow cytometry; and (3) initiated the venetoclax-blinatumomab induction regimen during the study period. Patients were excluded for a diagnosis of Burkitt leukemia or mixed-phenotype acute leukemia. Notably, the presence of active infection or abnormal liver function at baseline did not preclude inclusion, as the regimen was considered for patients ineligible for intensive chemotherapy. The patient identification and inclusion process are detailed in Figure 1.
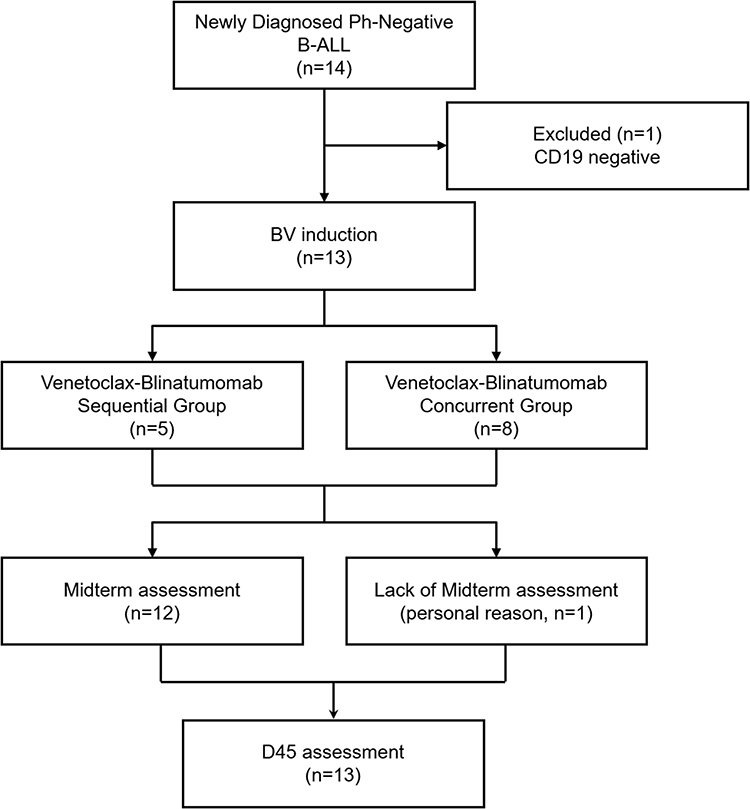 |
Figure 1 Patient Screen Flow Diagram. |
All patients received pre-phase treatment with dexamethasone (10 mg daily for 3–5 days) for cytoreduction. Prophylactic measures against tumor lysis syndrome, including hydration, urine alkalization, and antihyperuricemic therapy, were implemented based on individual risk. All patients received vigorous intravenous hydration approximately 2000 mL/m2/day. Antihyperuricemic therapy with either febuxostat or allopurinol was commenced 2–3 days prior to dexamethasone therapy and maintained for 10–14 days. Laboratory parameters, including levels of potassium, phosphorus, calcium, lactate dehydrogenase, and uric acid, were monitored frequently. Baseline cytogenetic and molecular profiling was performed for all patients, with risk stratification assessed according to National Comprehensive Cancer Network (NCCN) guidelines.10
Treatment
The protocol involved venetoclax and blinatumomab, with blinatumomab dosed at 9 µg for the first 7 days and escalated to 28 µg from day 8 to the end of treatment. Venetoclax was initiated at 100 mg on day 1, increased to 200 mg on day 2, 300 mg on day 3, and maintained at 400 mg from day 4 to the end of treatment up to14 days. For the first 5 cases, blinatumomab was initiated on day 8 after venetoclax administration considering the risk of tumor lysis syndrome (Venetoclax-Blinatumomab Sequential Group). Fortunately, we found that this sequential treatment did not show any signs of tumor dissolution. We subsequently initiated the treatment plan of starting the two agents simultaneously for 14 days overlapping (Venetoclax-Blinatumomab Concurrent Group), which showed an acceptable safety profile and has significantly shortened hospital stay (Figure 2).
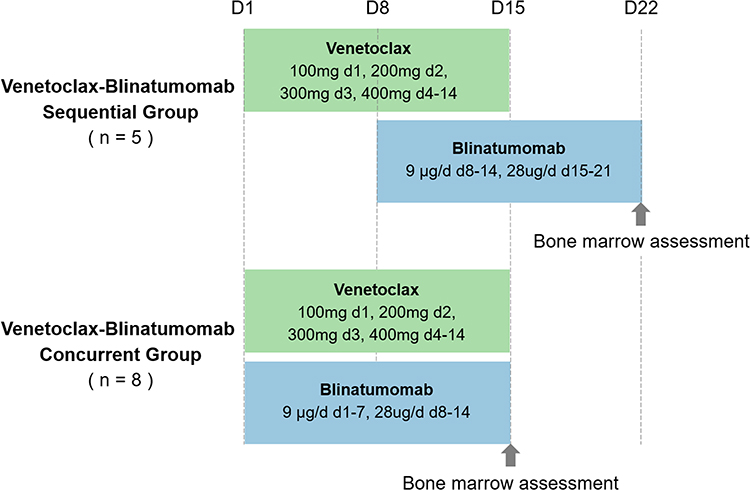 |
Figure 2 Timeline of venetoclax-blinatumomab administration and bone marrow assessments in concurrent and sequential groups. |
When venetoclax was co-administered with potent CYP3A4 inhibitors, the dose was adjusted to 100 mg or 75 mg in accordance with the manufacturer’s prescribing guidelines. All patients received prophylactic intrathecal injections as early as conditions permitted.
Response and Outcomes
Patients underwent midterm efficacy analysis between 14 and 21 days from initiation of regimen, usually at the end of blinatumomab administration. Bone marrow assessment was repeated before consolidation course initiation when the blood cell counts fully recovered. Efficacy assessments were based on the NCCN guideline 2024.10 CR was defined as no circulating lymphoblasts or extramedullary disease, trilineage hematopoiesis and <5% leukemic blasts, absolute neutrophil count ≥1×109/L, and platelets ≥100×109/L. The clearance of extramedullary disease was confirmed by imaging studies (CT or PET-CT) when clinically indicated. MRD was assessed by 10-color multiparameter flow cytometry at a sensitivity threshold of 1×10−4 (0.01%) bone marrow mononuclear cells. AEs were graded according to the Common Terminology Criteria for Adverse Events Version 5.0. Cytokine release syndrome (CRS) and neurologic toxicity were evaluated according to the American Society for Transplantation and Cellular Therapy Consensus Grading.11
Statistical Analysis
Descriptive statistics were used for the case series. Between-group comparisons for categorical variables were performed using the Fisher’s exact test. Given the limited sample size, 95% confidence intervals (CI) for key rates were calculated using the Agresti–Coull method.
Results
A total of 13 patients with Ph-negative B-ALL were enrolled from March 2024 to March 2025. The median age of the cohort was 52 years (range: 18–74 years), with 8 cases being male (61.5%; Table 1). The median white blood cell count prior to pretreatment was 2.61×109/L (range: 1.56–222.17×109/L). The median percentage of blasts identified by bone marrow morphology was 79.2% (range: 46–96%). According to the NCCN guideline 2024, 7 cases (53.8%) were classified as poor risk group, clinical characteristics was detailed in Table 2.
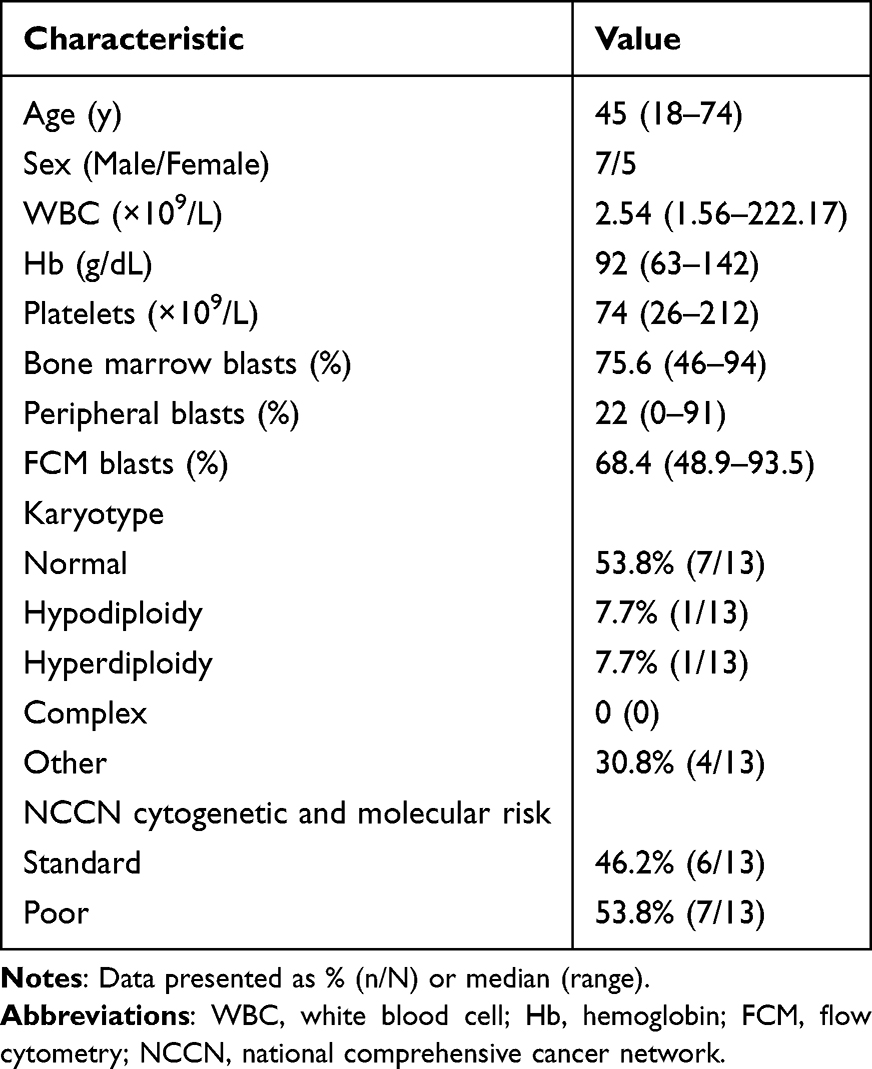 |
Table 1 Patient Demographic Data and Clinical Characteristics (n = 13) |
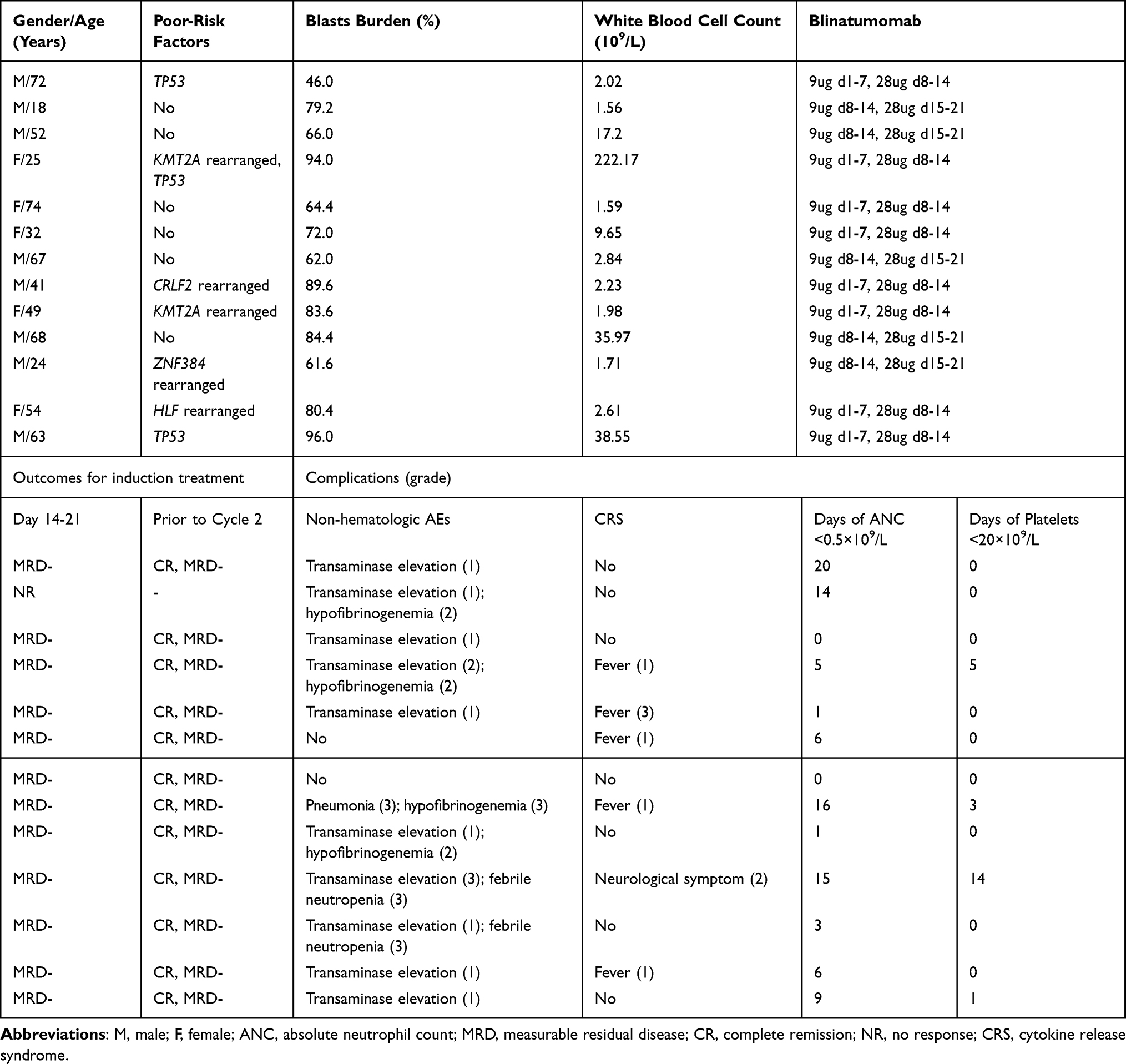 |
Table 2 Baseline Characteristics and Induction Therapy Data at Patient Level |
Bone marrow assessments were performed in 12 of 13 patients (92.3%) between days 14–21 after initiating induction therapy, coinciding with completion of the blinatumomab treatment course. Bone marrow morphological assessment revealed that 7 patients remained in marrow active hyperplasia and that other cases were found in reduced hyperplasia. Surprisingly, flow cytometric analysis demonstrated MRD negativity in 11 patients (91.7%; 95% CI, 64.6% to 99.6%) at this midterm assessment point. Only one patient showed primary resistance but subsequently attained CR following two cycles of dose modified Hyper-CVAD (300mg/m2 of cyclophosphamide administered intravenously over 2–3 hours every 12 hours for 6 doses on Days 1–3, 2 mg of vincristine administered intravenously on Days 4 and 11; 50mg/m2 of doxorubicin administered intravenously over 2 hours on Day 4; and 40 mg of dexamethasone daily on Days1-4 and on Days 11–1412). Twelve out of the 13 patients (92.3%; 95% CI, 66.7% to 99.6%) achieved CR with MRD negativity by flow cytometry after the first induction cycle.
During induction therapy, hematologic toxicities were predominant, with 11 patients (84.6%) developing grade 3–4 neutropenia. Febrile neutropenia occurred in 3 cases (23.1%), including one pulmonary fungal infection and two cases with unidentified infectious foci. Grade 3–4 thrombocytopenia was observed in 7 patients (53.8%). However, none of them experienced severe bleeding episodes. Hematologic toxicities were managed with comprehensive supportive care, including the use of granulocyte colony-stimulating factor, erythropoietin, and interleukin-11, alongside transfusions of red blood cells and platelets as needed. In all cases, both blinatumomab and venetoclax were administered at full doses throughout the induction phase without interruption. Transfusion support was required in a subset of patients: 4 received platelet transfusions (median: 20 units; range: 10–60 units) and 8 required red blood cell transfusions (median: 3.5 units; range: 2–10 units). Basically, patients who required transfusion had relatively lower baseline blood-cell counts before treatment, hemoglobin and platelet levels before the initiation of treatment and the corresponding transfusion volumes are presented in Table 3.
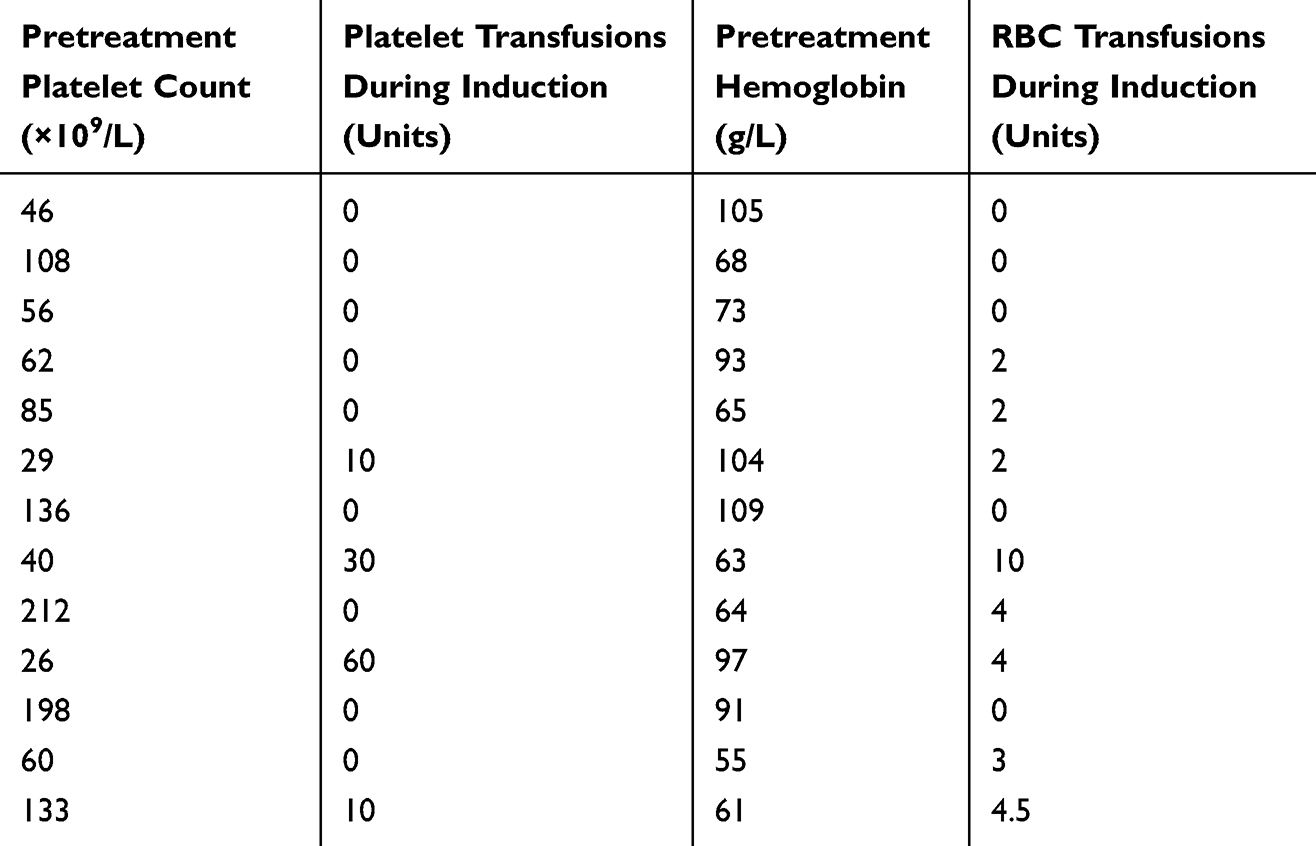 |
Table 3 Baseline Blood Counts and Blood Product Transfusions During Induction Therapy |
It is noteworthy that ten patients (76.9%) experienced hepatic toxicity, manifested as transaminase elevation, but grade 3 event occurred in only one case. No cases experienced dose modification or treatment suspension with supportive care. No tumor lysis syndrome or other severe non-hepatic organ toxicity occurred in the whole group, and there was no treatment-related mortality. AEs occurring during the induction therapy are summarized in Table 4.
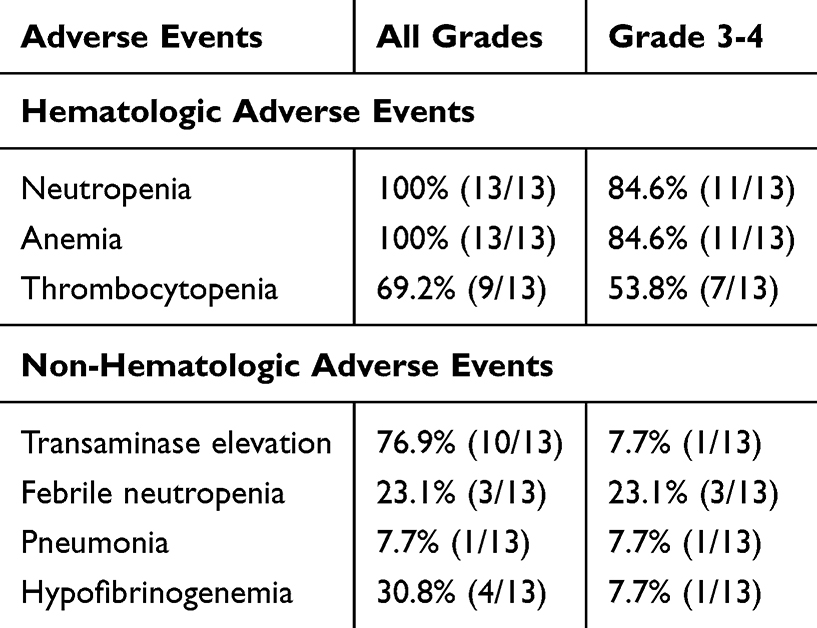 |
Table 4 Adverse Events During Induction Therapy |
CRS developed in 6 patients (46.2%) following blinatumomab initiation. One patient experienced grade 3 CRS, characterized by hypotension, which occurred within 24 hours of blinatumomab infusion. The event resolved within 48 hours following management with dexamethasone (10 mg for 2 days) and norepinephrine for vasopressor support. Five other patients experienced grade 1–2 CRS within 24 hours of blinatumomab infusion. All the events presented with fever, which were managed with dexamethasone (ranging from 2 to 10 mg per day). One patient developed grade 2 immune effector cell-associated neurotoxicity syndrome, manifesting as tremor and disorientation, concurrently with grade 2 CRS. The symptoms resolved after treatment with dexamethasone (10 mg/day). Critically, all these events were resolved within 48 hours of onset. Tocilizumab was not administrated in any patient, and blinatumomab infusion was not interrupted in any of these cases. Of note, the Venetoclax-Blinatumomab Concurrent Group (5/8) demonstrated a higher incidence of CRS compared to the Venetoclax-Blinatumomab Sequential Group (1/5), although there is no statistical significance (62.6% vs 20.0%, p = 0.226).
Consolidation therapy strategy was determined according to personal condition. Two patients received blinatumomab single agent (28 days per cycle), other eleven patients underwent multidrug combination chemotherapy including high-dose cytarabine or methotrexate-based regimens. As of May 2025, with a median follow-up of 283 days (range: 87–437 days), two patients developed bone marrow relapse at 95 and 282 days post-CR, respectively. One patient did not receive regular consolidation therapy due to poor treatment adherence, while the other had undergone allogeneic hematopoietic stem cell transplantation during remission, but relapsed 86 days post-transplantation (Figure 3). The median relapse-free survival (RFS) and overall survival (OS) were not reached in the overall cohort, with 1-year RFS and OS rates of 60.6% and 83.3%, respectively (Figure 4).
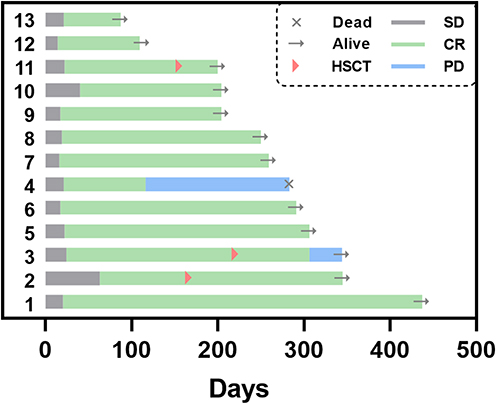 |
Figure 3 Treatment outcomes and clinical course of patients receiving blinatumomab and venetoclax. Abbreviations: HSCT, hematopoietic stem cell transplantation; SD, stable disease; CR, complete remission; PD, progression disease. |
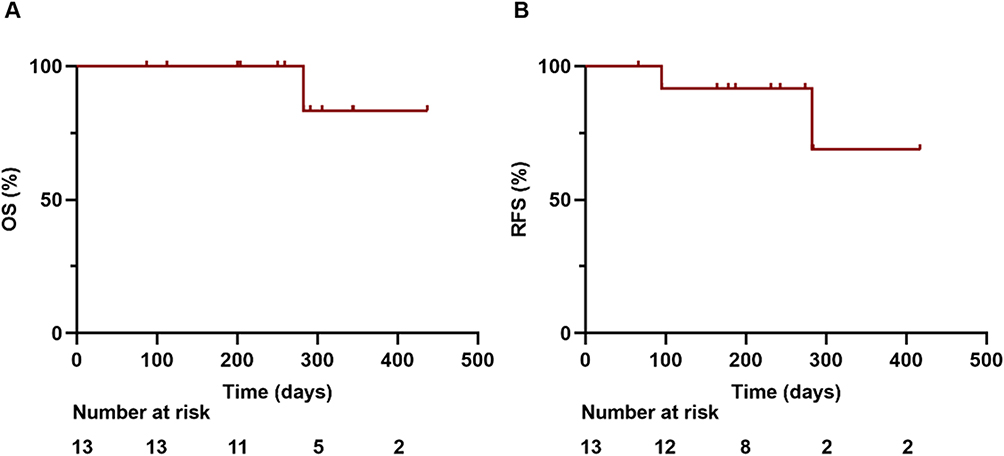 |
Figure 4 Overall survival and relapse-free survival for patients treated with blinatumomab and venetoclax. (A) overall survival; (B) relapse-free survival. |
Discussion
Blinatumomab is a bispecific monoclonal antibody designed to target CD3 and CD19, which recruits CD3-positive effector T cells to eliminate CD19-positive ALL blasts.13 There have been attempts to apply it in the induction treatment for newly diagnosed patients. The SWOG 1318 trial evaluated blinatumomab monotherapy for induction treatment in elderly patients with Ph-negative B-ALL, achieving a CR/CR with incomplete blood count recovery rate of 66% with good safety.14 Despite its better tolerance, response rate was not satisfying compared to multi-agent chemotherapy. Given the higher incidence of adverse disease biology and poor tolerance to intensive chemotherapy in elderly B-ALL patients, we believe that blinatumomab-based induction treatment is still worth exploring.
In a Phase II HOVON trial, blinatumomab was combined with chemotherapy as induction therapy for newly diagnosed CD19+ ALL patients aged <70 years. The protocol was amended due to toxicity, leading to a reduction of chemotherapy intensity. Fifteen patients discontinued treatment; among the 56 patients completing the treatment, the CR rate was 98%, and the MRD negativity rate reached 91%.15 Obviously, chemotherapy promotes remission and MRD negativity achievement during induction treatment for newly diagnosed Ph-negative B-ALL, but it also increases the risk of comorbidities. Particularly for elderly patients, myelosuppression and organ toxicity of intensive chemotherapy are often intolerable, leading to early mortality. Additionally, frequent drug reductions and treatment delays due to chemotherapy toxicity are usually associated with poorer outcomes.16 An effective and tolerable blinatumomab-based regimen is needed for Ph-negative ALL, especially in frail patients.
We explored the combination of blinatumomab and venetoclax, a totally chemo-free regimen as induction therapy for Ph-negative ALL, which has greatly reduced the duration and dosage of glucocorticoid administration and abandoned cytotoxic agents. This regimen enables patients to achieve rapid and deep remission within a relatively short treatment duration while maximally preserving organ function, especially in Concurrent Group, making it a highly recommended option for patients unfit for intensive chemotherapy. In addition to excellent tolerance, this regimen achieved a CR rate of 92.3% with MRD negativity after one treatment cycle. Remarkably, flow cytometry failed to detect residual leukemia cells in 11 patients within the initial 14–21 days, demonstrating that this drug combination can rapidly induce deep remission, and these patients maintained sustained MRD negativity thereafter. Although blinatumomab was administered for only 14 days in our study, we observed superior efficacy compared to the standard 28-day monotherapy in the SWOG 1318 trial (CR rate: 90.9% vs 66%)14 and equivalent outcomes to chemotherapy-reduced blinatumomab combinations reported in other induction studies.17 In this study, we found that this treatment was able to avoid conventional chemotherapy-induced severe bone marrow suppression, achieve CR and MRD clearance quickly, decrease the risk of complications and shorten the length of hospital stay. Moreover, this approach reduces exposure to cytotoxic drugs before HSCT in genetically high-risk patients, which preserves organ function and facilitates the timely progression to HSCT. This rapid MRD clearance strongly correlates with superior long-term outcomes, including improved RFS and OS, as established in previous literature.18 A study confirmed that venetoclax can synergistically enhance the anti-tumor efficacy of T cell-based immunotherapies against B-cell malignancies.9 This synergistic effect may be a potential mechanism in our study that patients achieved higher response rate compared to those receiving monotherapy of blinatumomab.
The adverse event profile was primarily characterized by acute, manageable toxicities such as CRS and myelosuppression during the induction phase. No new or unexpected long-term safety signals emerged during the follow-up. We find, quite interestingly, in our study that Venetoclax-Blinatumomab Concurrent Group demonstrated a higher incidence of CRS compared to the Venetoclax-Blinatumomab Sequential Group. This may share mechanistic similarities with CAR T-cell therapy for ALL, where higher tumor burden correlates with increased CRS severity.19 All CRS events in our study were mild and transient, with no severe complications or early mortality. This suggests that simultaneous administration of these two agents is feasible in newly diagnosed patients following adequate pretreatment. Based on these cohort results, we have initiated a prospective clinical trial to validate the efficacy of this regimen, which is currently ongoing.
Although this study proposed a new non-cytotoxic treatment, there are still some limitations. The retrospective design and small sample size limited the statistical power. Median follow-up duration was relatively short, which caused the reliability of survival outcome worth reconfirming. The heterogeneity of post-remission consolidation therapy (such as blinatumumab monotherapy, multi-drug chemotherapy or allogeneic HSCT) introduced a confounding variable, making it difficult to determine the impact of induction regimens on long-term survival. It is worth noting that our work specifically focuses on the induction phase, aiming to improve frontline therapy for patients with newly diagnosed B-ALL who have poor tolerance to conventional chemotherapy.
Conclusion
This retrospective study demonstrates that the combination of blinatumomab and venetoclax represents an effective and safe induction regimen for patients with newly diagnosed Ph-negative B-ALL. The regimen facilitates rapid CR with favorable tolerability, providing a valuable therapeutic alternative for patients ineligible for intensive chemotherapy. These findings warrant further investigation into blinatumomab as frontline therapy for B-ALL and the therapeutic potential of venetoclax in B-ALL management.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
The study protocol complied with the Declaration of Helsinki and was approved by the Institutional Review Board of Jiangsu Province Hospital (approval No. 2025-SR-551). Written informed consent was waived due to the retrospective nature of the study, with all patient data anonymized prior to analysis.
Consent to Participate
Not applicable because of the retrospective nature of the study. The patients were informed through the medical letters about the use of their data for research purposes.
Consent to Publish
All authors provided consent for publication.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors have no relevant financial or non-financial interests to disclose for this work.
References
1. Jabbour E, Short NJ, Jain N, et al. Ponatinib and blinatumomab for Philadelphia chromosome-positive acute lymphoblastic leukaemia: a US, single-centre, single-arm, Phase 2 trial. Lancet Haematol. 2023;10(1):e24–e34. doi:10.1016/S2352-3026(22)00319-2
2. Foà R, Bassan R, Elia L, et al. Long-term results of the dasatinib-blinatumomab protocol for adult Philadelphia-positive ALL. J Clin Oncol. 2024;42(8):881–885. doi:10.1200/JCO.23.01075
3. Logan AC. Lower leukemia burden maximizes the impact of blinatumomab therapy. Cancer. 2023;129(9):1316–1318. doi:10.1002/cncr.34666
4. Queudeville M, Stein AS, Locatelli F, et al. Low leukemia burden improves blinatumomab efficacy in patients with relapsed/refractory B-cell acute lymphoblastic leukemia. Cancer. 2023;129(9):1384–1393. doi:10.1002/cncr.34667
5. Hao Z, Fei Y, Chen J, et al. Combination of venetoclax and azacitidine in relapsed/refractory acute B-cell lymphoblastic leukemia: a case series from a single center. Hematology. 2024;29(1):2344998. doi:10.1080/16078454.2024.2344998
6. Canaani J, Frisch A, Pollyea DA, et al. Venetoclax-based salvage therapy for adult patients with relapsed/refractory acute lymphoblastic leukemia. Eur J Haematol. 2023;111(3):365–372. doi:10.1111/ejh.14015
7. Luskin MR, Shimony S, Keating J, et al. Venetoclax plus low-intensity chemotherapy for adults with acute lymphoblastic leukemia. Blood Adv. 2025;9(3):617–626. doi:10.1182/bloodadvances.2024014405
8. Chang J, Shen YJ, Shi T, Wang HF, Jin J, Zhu HH. Venetoclax and blinatumomab based chemotherapy-free treatment in a patient with Philadelphia chromosome-negative acute lymphoblastic leukemia. Ann Hematol. 2023;102(5):1275–1277. doi:10.1007/s00277-023-05127-3
9. Murakami S, Suzuki S, Hanamura I, et al. Combining T-cell-based immunotherapy with venetoclax elicits synergistic cytotoxicity to B-cell lines in vitro. Hematol Oncol. 2020;38(5):705–714. doi:10.1002/hon.2794
10. NCCN clinical practice guidelines in oncology-acute lymphoblastic leukemia (Version 3.2024). Available from: www.nccn.org.
11. Lee DW, Santomasso BD, Locke FL, et al. ASTCT consensus grading for cytokine release syndrome and neurologic toxicity associated with immune effector cells. Biol Blood Marrow Transplant. 2019;25(4):625–638. doi:10.1016/j.bbmt.2018.12.758
12. Kantarjian H, Thomas D, O’Brien S, et al. Long-term follow-up results of hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (Hyper-CVAD), a dose-intensive regimen, in adult acute lymphocytic leukemia. Cancer. 2004;101(12):2788–2801. doi:10.1002/cncr.20668
13. Kantarjian H, Stein A, Gökbuget N, et al. Blinatumomab versus chemotherapy for advanced acute lymphoblastic leukemia. N Engl J Med. 2017;376(9):836–847. doi:10.1056/NEJMoa1609783
14. Advani AS, Moseley A, O’Dwyer KM, et al. SWOG 1318: a phase II trial of blinatumomab followed by POMP maintenance in older patients with newly diagnosed Philadelphia chromosome-negative B-cell acute lymphoblastic leukemia. J Clin Oncol. 2022;40(14):1574–1582. doi:10.1200/JCO.21.01766
15. Rijneveld A, Gradowska P, Bellido M, et al. P366: blinatumomab added to prephase and consolidation therapy in newly diagnosed precursor b-all in adults. A phase II hovon trial. HemaSphere. 2022;6:266–267. doi:10.1097/01.HS9.0000844352.62588.a4
16. Sive JI, Buck G, Fielding A, et al. Outcomes in older adults with acute lymphoblastic leukaemia (ALL): results from the international MRC UKALL XII/ECOG2993 trial. Br J Haematol. 2012;157(4):463–471. doi:10.1111/j.1365-2141.2012.09095.x
17. Lu J, Qiu H, Wang Y, et al. Reduced-dose chemotherapy and blinatumomab as induction treatment for newly diagnosed Ph-negative B-cell precursor acute lymphoblastic leukemia: a phase 2 trial. J Hematol Oncol. 2024;17(1):79. doi:10.1186/s13045-024-01597-8
18. Bassan R, Spinelli O, Oldani E, et al. Improved risk classification for risk-specific therapy based on the molecular study of minimal residual disease (MRD) in adult acute lymphoblastic leukemia (ALL). Blood. 2009;113(18):4153–4162. doi:10.1182/blood-2008-11-185132
19. Sheth VS, Gauthier J. Taming the beast: CRS and ICANS after CAR T-cell therapy for ALL. Bone Marrow Transplant. 2021;56(3):552–566. doi:10.1038/s41409-020-01134-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.