Back to Journals » Clinical Ophthalmology » Volume 17
Vector Analysis and Prognostic Factors for Femtosecond Arcuate Keratotomy in Post-Keratoplasty Astigmatism
Authors Alsaif BA, Al Somali A ![]() , Banaji SH, Alshaibani AK
, Banaji SH, Alshaibani AK
Received 7 July 2023
Accepted for publication 4 November 2023
Published 7 December 2023 Volume 2023:17 Pages 3747—3759
DOI https://doi.org/10.2147/OPTH.S429264
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr John Miller
Bayan A Alsaif,1,* Abdulaziz Al Somali,2,* Sumayah H Banaji,1 Askar K Alshaibani3
1Department of Ophthalmology, College of Medicine, King Fahd Hospital of the University, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2Department of Ophthalmology, College of Medicine, King Faisal University, Al-Ahsa, Saudi Arabia; 3Ophthalmology, Dhahran Eye Specialist Hospital, Dhahran, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Askar K Alshaibani, Email [email protected]
Purpose: To analyze different tomographic and refractive parameters for predicting successful visual outcome following femtosecond laser-assisted arcuate keratotomy (FSAK) for post-keratoplasty astigmatism.
Design: Retrospective.
Methods: Retrospective study evaluating patients with astigmatism following penetrating keratoplasty (PKP) or deep anterior lamellar keratoplasty (DALK) who underwent FSAK. Vector analysis using the Alpins method was done to calculate surgically induced astigmatism (SIA). An improvement of 3 lines of Early Treatment Diabetic Retinopathy Study (ETDRS) lines was used for successful outcome. Outcome was measured at 3 months and 17 months.
Results: This study included 106 eyes from 104 patients (65 males and 39 females). Mean age was 31.8± 8.6 years, and 89.4% (n=93) of cases were keratoconus (KC), 3.8% (n=4) scar, 3.8% (n=4) granular dystrophy, 1.9% (n=2) post-LASIK ectasia, and 1.0% (n=1) macular dystrophy. Uncorrected visual acuity (UCVA) improved from 1.02± 0.53 logarithm minimal angle of resolution (logMAR) to 0.87± 0.49 logMAR (p=0.01) at 3 months and to 0.92± 1.08 logMAR (p=0.57) at 17 months. Best spectacle-corrected visual acuity (BSCVA) improved from 0.41± 0.30 logMAR to 0.31± 0.19 logMAR (p< 0.01) at 3 months and to 0.23± 0.27 logMAR (p< 0.01) at 17 months. Success was achieved in 50% (n=53) and 49% (n=52) at 3 and 17 months follow-up, respectively. Success group showed worse preoperative UCVA (1.21± 0.56 vs 0.83± 0.44 logMAR; p< 0.01), worse preoperative BSCVA (0.50± 0.36 vs 0.33± 0.19 logMAR; p=0.01). Preoperative UCVA had an area under the curve of 0.721 (95% CI: 0.622– 0.820; p< 0.01). The Youden’s optimal cutoff point was 0.90 logMAR (equivalent Snellen 20/159) with 76.9% sensitivity and 35.2% specificity. Flattening index (FI) was 87% in DALK and 73% in PKP (p=0.14). Correction index (CI) was 99% and 86% (p=0.18) for DALK and PKP, respectively. Success of the astigmatic surgery for DALK and PKP was 44% vs 42% (p=0.29), respectively.
Conclusion: Improvement of at least three lines was achieved in 49% of patients who underwent FSAK following PKP or DALK; this improvement was achieved in patients who had a worse preoperative UCVA.
Keywords: DALK, PKP, femtosecond arcuate keratotomy, astigmatic keratotomy, keratoplasty astigmatism, vector analysis
Introduction
Post-keratoplasty astigmatism is a major confounding factor for the visual outcome. When keratoplasty results in high astigmatism, limited options are available to address the large amount of astigmatism as corneal based refractive procedures such as topography-guided custom ablation (T-CAT) photorefractive surgery are limited by a safe residual stromal bed thickness beyond which it cannot be used, or toric implantable collamer lens (ICL) which also has a maximum treatment limit. Alone or in combination, several interventions have been employed to address this issue, such as arcuate keratotomy, compression sutures, and the aforementioned procedures. Arcuate keratotomy is either made with a keratome or with the assistance of a femtosecond laser (FSAK). Femtosecond laser provides precise incision depth with safer and more predictable outcomes compared with arcuate keratotomy made with a keratome.1,2 However, AK remains unpredictable to some extent, especially in highly irregular astigmatic grafted corneas, further prolonging the visual rehabilitative journey of post-keratoplasty patients. In a retrospective data of 89 cases of post-keratoplasty astigmatism it has been found that 33% of the accuracy of post-keratoplasty astigmatism correction cannot be attributed to a known cause, with the remaining 67% being attributed to the amount of astigmatism preoperatively, arc length, depth, and incision diameter.3 Prognostic factors for the visual outcome post-keratoplasty astigmatism using AK are poorly studied and to our knowledge only one study had looked into some possible prognostic factors in which they have found that preoperative cylinder more than 6.75 D is associated with effective treatment.4 However, it had not been followed up beyond 6 months, and other possible factors such as corneal surface irregularity or posterior corneal astigmatism have never been addressed before. Hence we aimed at including more topographic parameters and a larger sample size and performing the vector analysis of early (less than 6 months) and late (beyond 6 months) results of FSAK.
Methods
This retrospective study had Research Ethics Board approval from Dhahran eye specialist hospital, and was conducted in accordance with the tenets of the Declaration of Helsinki. The requirement for informed consent was waived by the Research Ethics Board of Dhahran eye specialist hospital because this is a minimal risk retrospective chart review in which no patient interaction will occur, data were collected from 2014, in addition to the large number of patients. The data were maintained with confidentiality among authors in the study.
Study Participants
This study included patients that underwent FSAK for treating high regular astigmatism that could not be corrected with spectacles or intolerance to hard contact lenses following a suture-less PKP or DALK at the Dharana eye specialist.
Patients who only had poor vision explained by post-keratoplasty astigmatism were included. Those who had other ocular pathologies such as glaucoma, other corneal pathology, retinal pathology, cataract, optic neuropathy, or amblyopia were excluded. Different indications for keratoplasty were included, namely keratoconus, therapeutic keratoplasty, corneal dystrophies (granular and macular), post-LASIK ectasia, corneal scar. Furthermore, patients who had interventions before or during follow-up period, such as T-CAT or other corneal surface-based refractive procedures, placement of ICL, toric intraocular lens (IOL) that could affect visual outcome, were excluded. For the purpose of isolating the effect of FSAK only, patients who had had compression sutures or suturing of gaping wounds, or graft–host opening to account for excessive astigmatism were excluded. Also, patients who had a repeat FSAK were followed up until the first AK only. Data for patients who underwent FSAK to address high regular astigmatism post-PKP or DALK done from 2014 to 2021 at Dhahran eye specialist hospital were collected after at least 6 months from removing all sutures of keratoplasty.
Data Collection
Data collected included baseline demographics (age, sex). Preoperative and postoperative data include uncorrected visual acuity (UCVA), best spectacle-corrected visual acuity (BSCVA), manifest cylinder, manifest sphere, autorefractometer measurements of sphere and cylinder (Tonoref II ARK-510A autorefractometer; Nidek Inc., Aichi, Japan). Corneal topography was obtained using the Pentacam-HR (Oculus GmbH, Wetzlar, Germany), and data included: k max, flat k, steep k, anterior corneal cylinder, posterior corneal cylinder, presence of peripheral steepening defined as a steepening of ≥48 D in 6–8 mm zone on axial curvature, presence of complete ring defined as the former present in 360° of the cornea, keratometry power deviation (KPD), index of surface variance (ISV), index of height asymmetry (IHA), index of vertical asymmetry (IVA), index of height decentration (IHD), keratoconus index (KI), minimum radius of curvature (Rmin), central keratoconus index (CKI), and topographic keratoconus classification (TKC). Data were obtained preoperatively and early postoperatively within 1–5 months, and late within 6–57 months postoperatively.
Outcome Measure
Improvement in UDVA or BSCVA post-AK by three lines of ETDRS lines (doubling of the visual angle, ≥0.3 logMAR) a definition adopted by a previous study.4 Safety index was calculated as (postoperative BSCVA/preoperative BSCVA), and efficacy index was calculated as (postoperative UDVA/preoperative BSCVA). Alpins vector analysis5,6 was carried out using VECTrAK, v.2.3.0 (ASSORT Pty Ltd, Cheltenham, Victoria, Australia) of topographic corneal astigmatism with the following measures: Target-induced astigmatism (TIA), which is the astigmatic change in magnitude and axis intended for treatment to fully correct the astigmatism. Surgically induced astigmatism (SIA), which is the actual change in astigmatism magnitude and axis by the surgery. Correction index (CI), calculated by dividing the actual effect (SIA) by the intended effect (TIA); it has an ideal value of 1. Magnitude of error (ME) arithmetic deviation of SIA from TIA in magnitude and axis; positive value for over-correction and negative value for under-correction. Difference vector (DV) ideally zero, index of success (IOS) calculated as DV/TIA and is ideally zero, flattening effect (FE) calculated as (SIA Cos2 × AE), and flattening index calculated as (FE/TIA) and is preferably 1.
Statistical Analysis
Quantitative data were summarized with mean, standard deviation, and range, while qualitative data were summarized with count and percentages. The normality of data was checked with Shapiro–Wilk. Qualitative data were compared with the chi-square test. Factors associated with success were assessed by binary logistic regression with back elimination. Independent non-normally distributed data were compared with Mann–Whitney U-test. Dependent non-normally distributed data were compared with Wilcoxon signed ranks test. Missing data were replaced by expectation maximization. Visual acuity was converted to a logarithm of the minimum angle of resolution (logMAR) for analysis. Statistical analysis was performed with IBM SPSS for Windows (v.22; IBM Corp, Armonk, NY, USA). All figures were constructed with Microsoft Excel (2019, Microsoft Corp., USA). A P-value less than 0.05 was considered statistically significant.
Surgical Technique
FSAK was created using iFS laser (Advanced Medical Optics, Inc.). Before going to the procedure room, the subject was seated upright and corneal marking was done along the horizontal meridian and along the topographic steep axis. After that, in the procedure room, the case was started with cleaning using povidone iodine 5% (Betadine) then anesthetized using topical benoxinate hydrochloride 0.4% (BNX, Alcon Laboratories, Inc.). Paired cuts centered on the steep axis based on topographic axial curvature map of the Pentacam-HR were made, corneal thickness at intended AK cuts 0.5 mm inside host graft junction was determined using ultrasonic pachymeter, and incision depth, arch length, and optical zone were determined using the Hanna nomogram for post-keratoplasty astigmatism.7 After completion of procedure, incisions were opened using a Sinskey hook. Subjects were then treated with moxifloxacin 0.5% (Vigamox, Alcon Laboratories, Inc.) four times daily for 1 week and prednisolone acetate 1% drops (Pred Forte; Allergan, Irvine, CA), one drop four times daily with tapering dose weekly until kept on a maintenance dose according to their needs.
Results
A total of 106 eyes from 104 patients (65 males and 39 females) were included in this study. The mean age was 31.8±8.6 years (13.0–70.0 years). Altogether 89.4% (n=93) eyes were diagnosed with KC, 3.8% (n=4) with scar, 3.8% (n=4) with granular dystrophy, 1.9% (n=2) with post-LASIK ectasia, and 1.0% (n=1) with macular dystrophy. The UCVA improved from 1.02±0.53 logMAR at baseline to 0.87±0.49 logMAR (p=0.01) at 3 months and to 0.92±1.08 logMAR (p=0.57) at 17 months. The BSCVA improved from 0.41±0.30 logMAR at baseline to 0.31±0.19 logMAR (p<0.01) at 3 months and to 0.23±0.27 logMAR (p<0.01) at 17 months. The front corneal astigmatism improved from 9.01±2.88 D at baseline to 5.47±4.53 D (p<0.01) at 3 months and to 5.04±2.76 D (p<0.01) at 17 months. The back corneal astigmatism improved from 1.85±4.58 D at baseline to 1.01±0.61 D (p<0.01) at 3 months and to 0.92±0.54 D (p<0.01) at 17 months. In total, 37.7% (n=40) of the eyes were post-DALK, and 62.3% (66) were post-PKP.
In subjects who underwent DALK, UCVA changed from 1.01±0.54 logMAR to 0.92±0.59 logMAR (p=0.43) at 3 months and to 1.06±0.67 logMAR (p=0.94) at 17 months postoperatively. BSCVA changed from 0.36±0.28 logMAR to 0.30±0.19 logMAR (p=0.25) at three months and to 0.20±0.32 logMAR (p<0.01) at 17 months postoperatively. Front corneal astigmatism reduced from 8.33±3.23 D to 4.55±3.68 D at 3 months (p<0.01) and to 4.55±2.72 D (p<0.01) at 17 months postoperatively.
In subjects who underwent PKP, UCVA changed from 1.02±0.53 logMAR to 0.83±0.42 logMAR (p<0.01) at 3 months and to 0.84±1.26 logMAR (p=0.45) at 17 months postoperatively. BSCVA changed from 0.44±0.31 logMAR to 0.31±0.19 logMAR (p<0.01) at 3 months to 0.24±0.23 logMAR (p<0.01) at 17 months postoperatively. Front corneal astigmatism reduced from 9.42±2.59 D to 6.03±4.93 D at 3 months (p<0.01) and to 5.34±2.76 D (p<0.01) at 17 months postoperatively.
Table 1 compares preoperative parameters for eyes between success and non-success groups at early (3 months) postoperative time. The early success group had worse UCVA (1.25±0.54 vs 0.78±41 logMAR; p<0.01) and worse BSCVA (0.50±0.36 vs 0.32±0.18 logMAR; p<0.01). Table 2 compares preoperative parameters between success and non-success groups at late (17 months) postoperative time. The late success group had worse UCVA (1.21±0.56 vs 0.83±0.44 logMAR; p<0.01) and worse BSCVA (0.50±0.36 vs 0.33±0.19 logMAR; p=0.01).
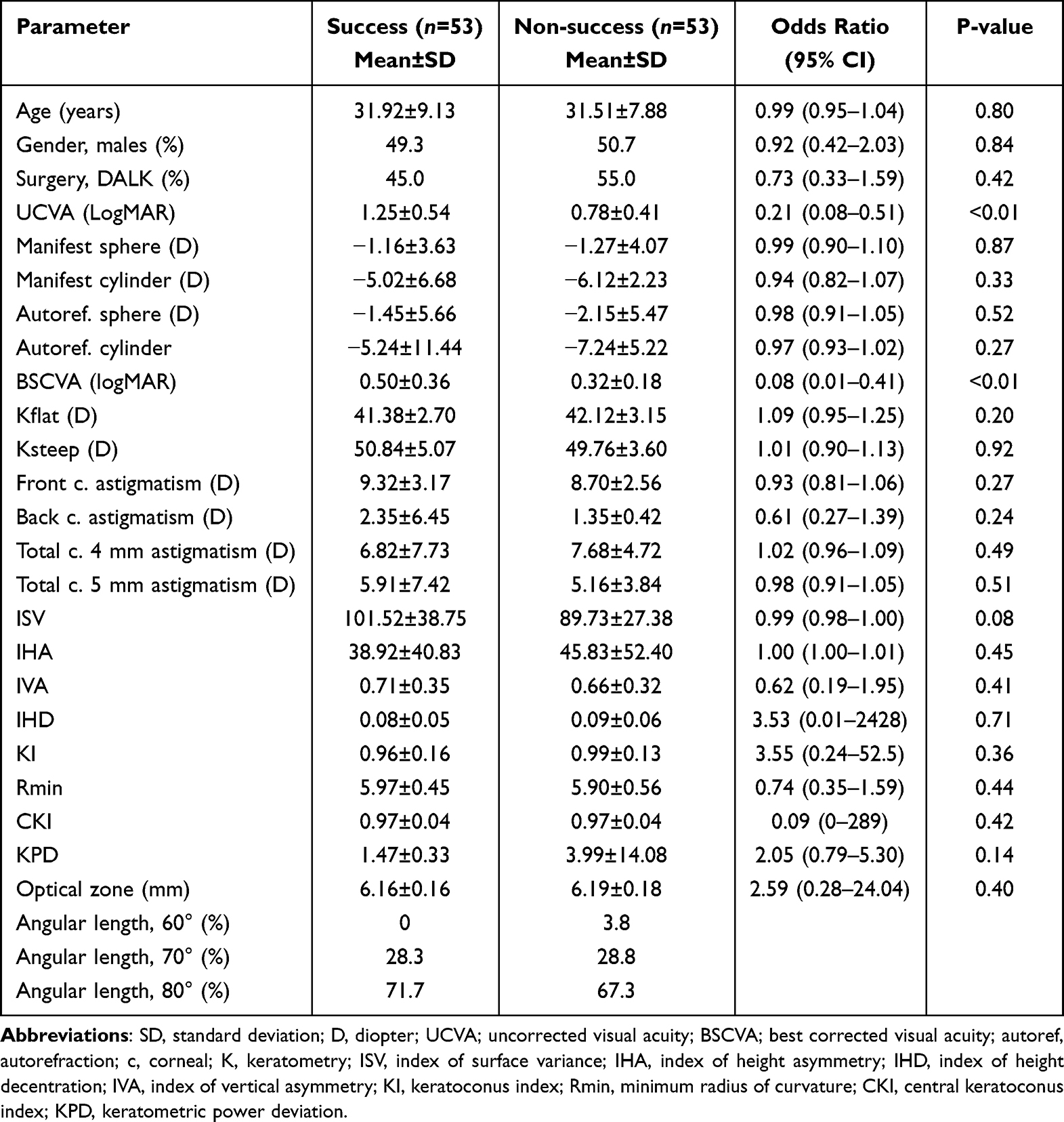 |
Table 1 Comparisons of Preoperative Parameters Between Success and Non-Success Groups Three Months Postoperatively |
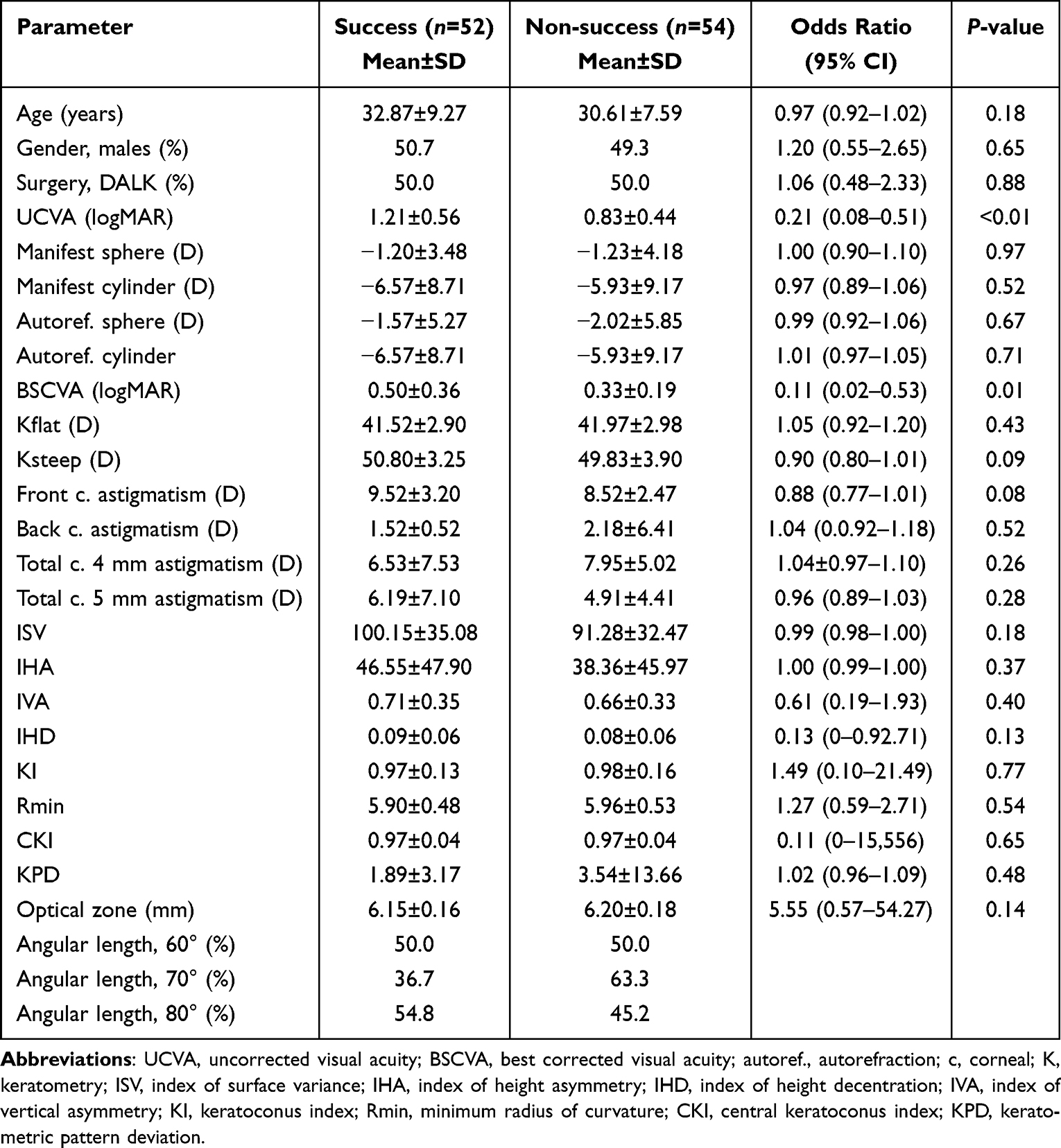 |
Table 2 Comparisons of Preoperative Parameters Between Success and Non-Success Cases 17 Months Postoperatively |
Table 3 depicts the results of binary logistic regression with back elimination performed to assess the combinations of factors associated with early and late success. Worse UCVA was a significant factor associated with early (p<0.01) and late (p=0.03) success. Also, worse BSCVA was a significant factor associated with early (p=0.02) and late (p=0.03) success.
 |
Table 3 Analysis of Factors Associated with Success Cases |
Figure 1 shows the ROC curve of preoperative UCVA and BSCVA as early success predictors. The area under the curve was 0.765 (95% CI: 0.675–0.855; p<0.01) for preoperative UCVA and 0.642 (95% CI: 0.537–0.746; p=0.012) for preoperative BSCVA. Preoperative UCVA has a bigger area under the curve. The Youden’s optimal cutoff point was 0.85 logMAR (Snellen 20/142) with 83.0% sensitivity and 39.6% specificity. Figure 2 shows the ROC curve of preoperative UCVA and BSCVA as predictor factors for late success. The area under the curve was 0.721 (95% CI: 0.622–0.820; p< 0.01) for preoperative UCVA and 0.605 (95% CI: 0.497–0.713; p=0.063) for preoperative BSCVA. Preoperative UNCVA has a bigger area under the curve that is statistically significant. The Youden’s optimal cutoff point was 0.90 logMAR (Snellen 20/159) with 76.9% sensitivity and 35.2% specificity.
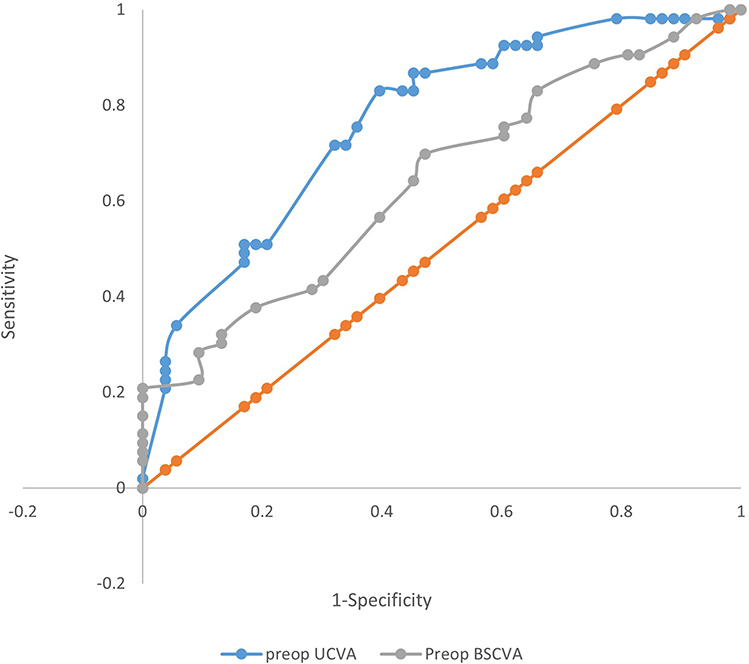 |
Figure 1 ROC Curve for Best Corrected and Uncorrected Visual Acuity Predicting Early success. |
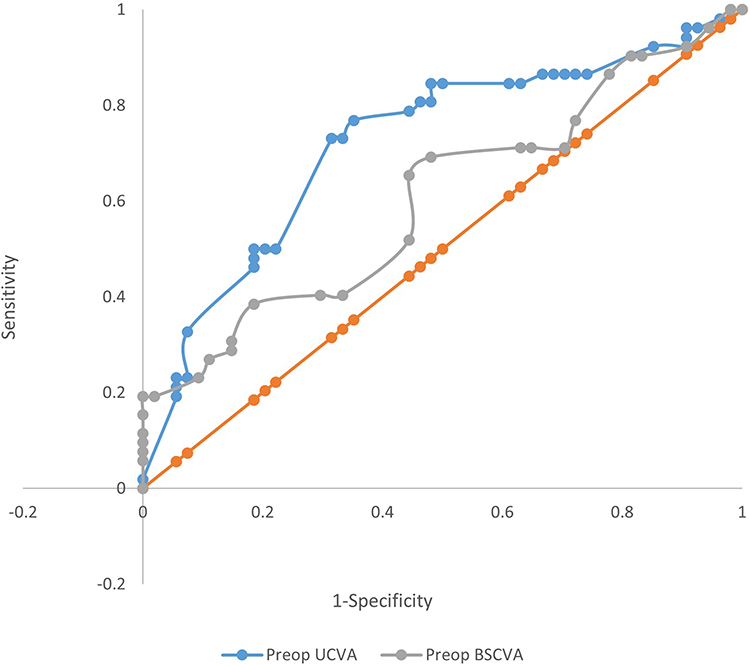 |
Figure 2 ROC Curve for Best Corrected and Uncorrected Visual Acuity Predicting Late Success. |
Table 4 compares SIA between DALK and PKP at early and late postoperative times per length of the incision. For an incision length of 70°, the SIA was greater in DALK compared with PKP (7.23±4.20 vs 4.52±3.40; p=0.04), while there was no significant difference in SIA between the two surgeries for an incision length of 80° at early 3 months postoperative time. At late 17 months postoperative time, there was no significant difference between the two surgeries for 70° and 80° (p>0.05 for all).
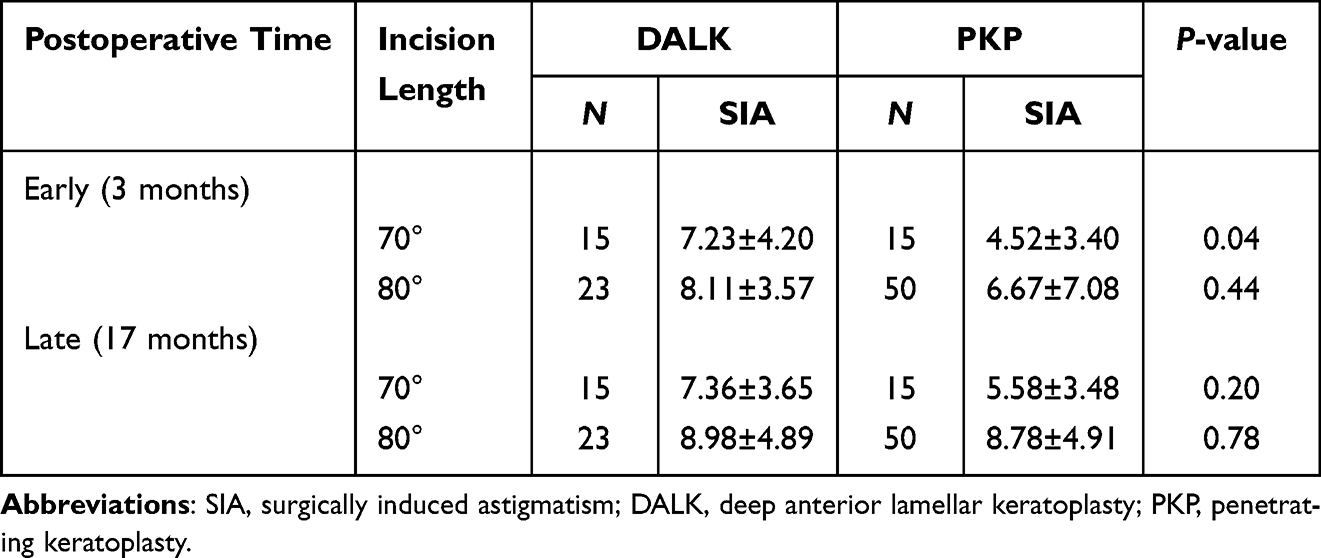 |
Table 4 Surgically Induced Astigmatism Stratified by Surgery, Length of the Incision, and Postoperative Time |
Table 5 compares safety and efficacy indices and vector analysis between DALK and PKP at early 3 months. There was no significant difference between the two surgeries in terms of safety and efficacy. The TIA was significantly lower in DALK than in PKP (8.34±3.24 D vs 9.43±2.63 D; p=0.01). There was a systemic error of magnitude toward under-correction for DALK and PKP (−1.21±4.35 D vs −3.44±7.56 D; p=0.04). FI indicates that flattening at the intended steep meridian was 84% in DALK compared with 53% in PKP (p=0.01). From CI, the correction of astigmatism was under-corrected (90% in DALK and 65% in PKP; p=0.03). The success of astigmatic surgery, (1-IOS) *100, was 46% for DALK and 32% for PKP (p=0.43). COA suggests that for future FSAK the astigmatism should be adjusted by 1.91 and 2.95 for DALK and PKP, respectively (p=0.05).
 |
Table 5 Comparison of Outcomes Between DALK and PKP 3 Months Postoperatively |
Table 6 compares safety and efficacy indices and vector analysis between DALK and PKP at the late 17 months. There was no significant difference between the two surgeries in terms of safety and efficacy. The TIA was lower in DALK compared with PKP (8.22±3.27 vs 9.21±2.77; p=0.01). There was a systemic error in the angle in DALK and PKP (−4.28° vs −1.69°; p=0.38) where the achieved correction was clockwise to the intended axis. FI indicates that flattening at the intended steep meridian was 87% in DALK compared with 73% in PKP (p=0.14). From CI, the correction of astigmatism was under-correction in DALK and PKP (99% vs 86%; p=0.18). The success of the astigmatic surgery for DALK and PKP was 44% vs 42%; p=0.29).
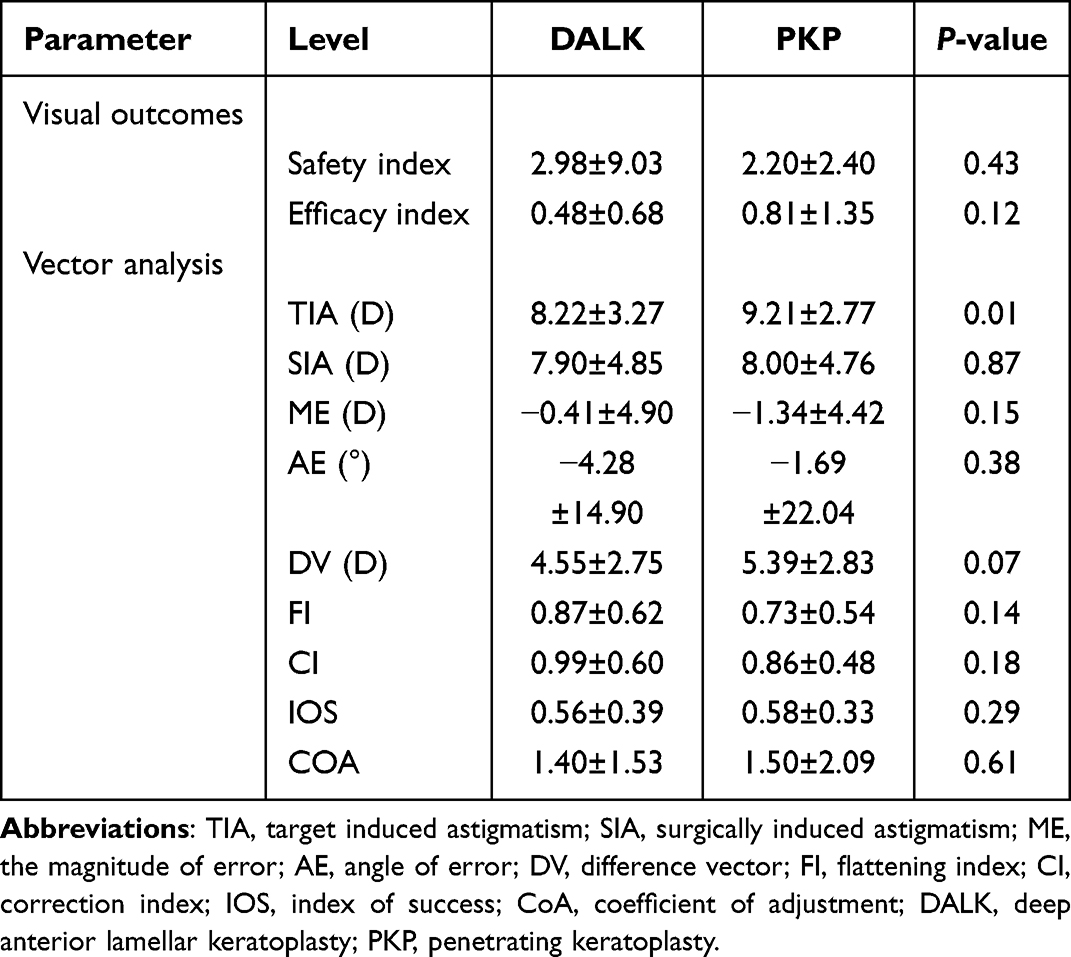 |
Table 6 Comparison of Outcomes Between DALK and PKP 17 Months Postoperatively |
COA suggests that for future FSAK the astigmatism should be adjusted by 1.40 and 1.50 for DALK and PKP, respectively (p=0.61).
The complications of FSAK were as follows: 9.4% (n=10) had repeated FSAK, 0.9% (n=1) had regraft, 0.9% (n=1) had a recurrence of dystrophy, and 88.7% (n=94) had none.
Discussion
In this study subjective refraction and tomographic and topometric parameters have been analyzed for the possible predictive value of a successful visual outcome in patients who underwent PKP or DALK for different reasons over a median follow-up period of 17 months (range from 6–57 months). The pure effect of FSAK on post-keratoplasty astigmatism was assured by excluding any prior interventions, including the use of compression sutures or sutures addressing gaping wounds, corneal based interventions such as, but not limited to, topo-guided PRK, implantation of intracolumnar lens, and Toric intraocular lens. In this study we have found that a worse preoperative UCVA was associated with more visual acuity improvement, with a cut-off value of 0.85 logMAR (Snellen equivalent of 20/142). Until today, scarce data are available for predicting a successful outcome following arcuate keratotomy whether it be femtosecond assisted or mechanical AK (Table 7). One study by Mimouni et al4 retrospectively reviewed 56 eyes over a follow-up period of 6 months and found that a higher preoperative manifest cylinder and a worse UCVA were predictors of a visual improvement following FSAK. However, in their cohort there were five cases (8.9%) that underwent suturing of AK incisions to address overcorrection. Also Wetterstrand et al8 conducted a prospective study of 16 eyes and found a significant correlation between having a worse preoperative CDVA and the outcome result of more improvement in postoperative CDVA. In agreement with previous studies, we have found that FSAK resulted in a significant improvement of UCVA over a median follow-up of 3 months.4,9–13 Also in accordance with previous studies the BSCVA improved at 3 months and results were maintained at 17 months.4,9–11,13 Corneal astigmatism significant reduction has been also demonstrated as in previous studies4,10,12,13 over 3 months and maintained over 17 months. Although Wetterstrand et al used different incision planning with a fixed non-penetrating length of incision that was 90°, 90% depth of incision, different incision diameters of 6.0 mm, 6.5 mm, and 7 mm, they demonstrated a comparable mean reduction of 5.1±4.7 D of anterior corneal cylinder to our mean reduction of 5.04±2.76 D. They have also found a mean reduction of posterior cylinder by 0.7±0.6 D comparable to what we found, 0.92±0.54 D.
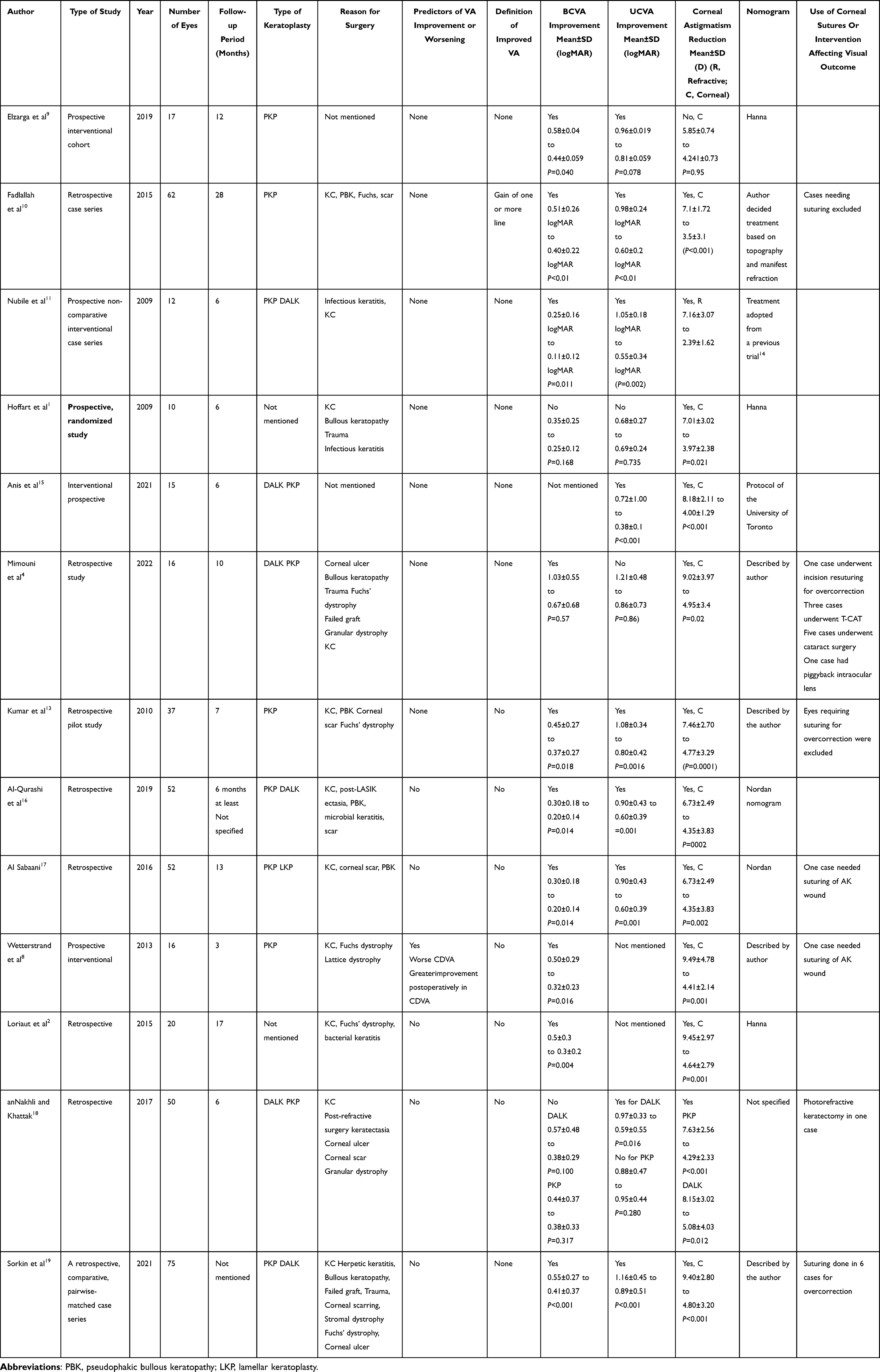 |
Table 7 Previous studies with arcuate keratotomy |
We have found a higher safety index for PKP and DALK compared with previous reports. Safety index was 2.98 and 2.20 for DALK and PKP, respectively, with no difference, compared with Mimouni et al4 with a safety index of 1.45 and 1.66 for DALK and PKP, respectively (p=0.45) and anNakhli and Khattak 18 with a safety index of 1.50 and 1.27 for DALK and PKP, respectively (p=0.325). For the efficacy index, results were conflicting between Mimouni et al who found a statistically significant higher efficacy for PKP 0.74 compared with DALK 0.33 (p<0.001) and anNakhli and Khattak who found a statistically significant higher efficacy for DALK 1.00 compared with PKP 0.31 (p=0.001).4,18 In our study, although PKP showed a relatively higher efficacy index compared with DALK (0.8 vs 0.48), respectively, we did not find a difference between them, p=0.12.
**In the early follow-up period (range 1–5 months, median of 3 months), DALK showed better results than PKP in terms of vector analysis with statistical significance evident from higher correction index 0.9 vs 0.65, more flattening effect along the steep meridian 0.84 vs 0.53, and a lower magnitude of error −1.21 vs −3.44. However, this superiority was not maintained over a longer follow-up period with a median of 17 months when PKP correction index improved to 0.86 and the flattening index along the steep meridian increased to 0.73, and the magnitude of error reduced to −1.34. The continuous change with improvement in PKP vector analysis, could be explained by the different vectorial powers created by the new limbus at the host graft junction of a penetrating keratoplasty that might influence wound healing with late changes in corneal curvature.
Although PKP had a higher mean TIA, the surgical effect of FSAK was statistically insignificant between DALK and PKP evident from a relatively similar index of success between both procedures, 0.56±0.39 and 0.58±0.33 for DALK and PKP, respectively. Moreover, both procedures exhibited a trend toward undercorrection, although statistically insignificant, the correction index for DALK was closer to ideal ratio of 1 compared with PKP (0.99 vs 0.86). Although anNakhli and Khattak18 found a statistically significant better performance of FSAK with DALK compared with PKP in terms of vector analysis, their follow-up period was limited to the first 6 months following FSAK. On the other hand Mimouni et al’s4 analysis uggested PKP as a favorable prognostic factor of visual outcome compared with DALK. But in their study they have included keratoconus cases only, and the follow up was limited to 6 months after FSAK. Furthermore, there were 23.8% cases in Mimouni et al’s4 study in which they needed suturing due to overcorrection in the DALK group; it was also not mentioned when the suturing done was to address the effect of FSAK alone and to account for the final outcome and wound stability that might extend beyond 6 months. Healing of FS created keratotomy starts with epithelial plug formation that fills the wound with subsequent regression of that epithelial plug and replacement by a loose fibrotic scar formation. After 6 months following FSAK, the AK wounds were still found to be occupied with epithelium along the upper one third of the wound.11 Furthermore, although in agreement with Mimouni et al.4 DALK showed a significantly higher SIA for an incision length of 70° compared with PKP over a 6 month follow-up period, this statistical difference was no longer demonstrated over a longer follow-up median of 17 months in our cohort; it is worth mentioning that Mimouni et al have also demonstrated this difference over a follow-up period of 6 months.
Conclusion
FSAK is an effective, safe procedure for post-keratoplasty astigmatism over a median follow up of 17 months with a gain of vision noted in 65% and nearly one third gaining more than 3 lines. A worse preoperative UCVA with a cut-off value of 20/159 Snellen was found to be a predictor of improvement in vision by at least 3 lines of ETDRS lines over a follow-up median of 17 months. This study has shown no differences in vector analysis between DALK and PKP over an extended follow-up period beyond 6 months. It had also shown no correlation between type of surgery, refractive, topometric or tomographic corneal parameters and visual improvement after FSAK. Limitations to our study include its retrospective nature.
Acknowledgment
We would like to thank Professor Noel Alpins for his contribution in data analysis.
Disclosure
The authors declare no conflict of interest in this work.
References
1. Hoffart L, Proust H, Matonti F, Conrath J, Ridings B. Correction of postkeratoplasty astigmatism by femtosecond laser compared with mechanized astigmatic keratotomy. Am J Ophthalmol. 2009;147(5):779–787.e1. doi:10.1016/j.ajo.2008.12.017
2. Loriaut P, Borderie VM, Laroche L. Femtosecond-assisted arcuate keratotomy for the correction of postkeratoplasty astigmatism: vector analysis and accuracy of laser incisions. Cornea. 2015;34(9):1063–1066. doi:10.1097/ICO.0000000000000487
3. Clair RM, Sharma A, Huang D, et al. Development of a nomogram for femtosecond laser astigmatic keratotomy for astigmatism after keratoplasty. J Cataract Refract Surg. 2016;42(4):556–562. doi:10.1016/j.jcrs.2015.12.053
4. Mimouni M, Kreimei M, Sorkin N, et al. Factors associated with improvement in vision following femtosecond astigmatic keratotomy in post-keratoplasty keratoconus patients. Am J Ophthalmol. 2020;219:59–65. doi:10.1016/j.ajo.2020.06.007
5. Alpins N. Astigmatism analysis by the Alpins method. J Cataract Refract Surg. 2001;27(1):31–49. doi:10.1016/S0886-3350(00)00798-7
6. Alpins NA. A new method of analyzing vectors for changes in astigmatism. J Cataract Refract Surg. 1993;19(4):524–533. doi:10.1016/S0886-3350(13)80617-7
7. Hanna KD, Hayward JM, Hagen KB, Simon G, Parel JM, Waring GO. Keratotomy for astigmatism using an arcuate keratome. Arch Ophthalmol. 1993;111(7):998–1004. doi:10.1001/archopht.1993.01090070118030
8. Wetterstrand O, Holopainen JM, Krootila K. Treatment of postoperative keratoplasty astigmatism using femtosecond laser-assisted intrastromal relaxing incisions. J Refract Surg. 2013;29(6):378–382. doi:10.3928/1081597X-20130515-01
9. Elzarga AAA, Osman AA, Gamal M, Khafagy MM, Osman IS. Vector analysis of femtosecond laser-assisted arcuate keratotomy for post-keratoplasty astigmatic correction. Ophthalmic Res. 2019;62(3):150–156. doi:10.1159/000499859
10. Fadlallah A, Mehanna C, Saragoussi JJ, Chelala E, Amari B, Legeais JM. Safety and efficacy of femtosecond laser-assisted arcuate keratotomy to treat irregular astigmatism after penetrating keratoplasty. J Cataract Refract Surg. 2015;41(6):1168–1175. doi:10.1016/j.jcrs.2014.08.046
11. Nubile M, Carpineto P, Lanzini M, et al. Femtosecond laser arcuate keratotomy for the correction of high astigmatism after keratoplasty. Ophthalmology. 2009;116(6):1083–1092. doi:10.1016/j.ophtha.2009.01.013
12. Hashemian MN, Ojaghi H, Mohammadpour M, et al. Femtosecond laser arcuate keratotomy for the correction of postkeratoplasty high astigmatism in keratoconus. J Res Med Sci. 2017;22(1):11–14. doi:10.4103/1735-1995.200267
13. Kumar NL, Kaiserman I, Shehadeh-Mashor R, Sansanayudh W, Ritenour R, Rootman DS. IntraLase-enabled astigmatic keratotomy for post-keratoplasty astigmatism: on-axis vector analysis. Ophthalmology. 2010;117(6):1228–1235.e1. doi:10.1016/j.ophtha.2009.10.041
14. Karabatsas C, Cook S, Figueiredo F, Diamond J, Easty D. Surgical control of late postkeratoplasty astigmatism with or without the use of computerized video keratography - A prospective, randomized study. Ophthalmology. 1998;105:1999–2006. doi:10.1016/S0161-6420(98)91115-0
15. Anis M, Howaidy A, Azzam S. Femtosecond laser-assisted arcuate keratotomy for correction of postkeratoplasty astigmatism. Delta J Ophthalmol. 2021;22(2):111. doi:10.4103/djo.djo_63_20
16. Al-Qurashi M, Al Sabaani N, Al Malki S. Comparison of manual and femtosecond laser arcuate keratotomy procedures for the correction of post-keratoplasty astigmatism. Saudi J Ophthalmol. 2019;33(1):12–17. doi:10.1016/j.sjopt.2018.11.001
17. Al Sabaani N, Al Malki S, Al Jindan M, Al Assiri A, Al Swailem S. Femtosecond astigmatic keratotomy for postkeratoplasty astigmatism. Saudi J Ophthalmol. 2016;30(3):163–168. doi:10.1016/j.sjopt.2016.04.003
18. anNakhli F, Khattak A. Vector analysis of femtosecond laser-assisted astigmatic keratotomy after deep anterior lamellar keratoplasty and penetrating keratoplasty. Int Ophthalmol. 2019;39(1):189–198. doi:10.1007/s10792-017-0803-0
19. Sorkin N, Mimouni M, Santaella G, et al. Comparison of manual and femtosecond astigmatic keratotomy in the treatment of postkeratoplasty astigmatism. Acta Ophthalmol. 2021;99(5):e747–e752. doi:10.1111/aos.14653
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Three-Month Outcomes of SMILE Pro with the VISUMAX 800 for Myopic Astigmatism in a Large Population
Cung HS, Tran LHT, Tran TN
Clinical Ophthalmology 2025, 19:417-425
Published Date: 7 February 2025
Initial Visual and Refractive Outcomes of Keratorefractive Lenticule Extraction Using 2MHz Femtosecond Laser Platform
Desai A, Kinkhabwala R, Mehta P, Prajapati B
Clinical Ophthalmology 2025, 19:3431-3437
Published Date: 18 September 2025