Back to Journals » International Journal of Women's Health » Volume 15
Vasomotor Symptoms During Menopause: A Practical Guide on Current Treatments and Future Perspectives
Authors Khan SJ, Kapoor E, Faubion SS, Kling JM
Received 28 July 2022
Accepted for publication 18 January 2023
Published 14 February 2023 Volume 2023:15 Pages 273—287
DOI https://doi.org/10.2147/IJWH.S365808
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Saira J Khan,1 Ekta Kapoor,2– 4 Stephanie S Faubion,2,5 Juliana M Kling2,6
1Department of Internal Medicine, Mayo Clinic, Phoenix, AZ, USA; 2Mayo Clinic Women’s Health, Rochester, MN, USA; 3Division of General Internal Medicine, Mayo Clinic, Rochester, MN, USA; 4Division of Endocrinology, Diabetes, Metabolism and Nutrition, Mayo Clinic, Rochester, MN, USA; 5Division of General Internal Medicine, Mayo Clinic, Jacksonville, FL, USA; 6Division of Women’s Health Internal Medicine, Mayo Clinic, Scottsdale, AZ, USA
Correspondence: Juliana M Kling, Division of Women’s Health Internal Medicine, Mayo Clinic, 13737 N 92 23 nd St, Scottsdale, AZ, 85260, USA, Tel +1-480-614-6001, Fax +1-480-614-6021, Email [email protected]
Abstract: Vasomotor symptoms affect as many as 80% of midlife women, but only about one in four women receive treatment due to many factors. Menopausal hormone therapy remains the most effective treatment for vasomotor symptoms, and current professional guidelines conclude that the benefits of treatment typically outweigh the risks for healthy, symptomatic women under age 60 years and those within 10 years from their final menstrual period. For women with medical comorbidities, an individualized approach to treatment is recommended. For women who cannot use or choose not to use menopausal hormone therapy, there are many evidence-based non-hormonal options available including pharmacologic therapies. This review aims to summarize treatment options for bothersome vasomotor symptoms to guide clinicians caring for midlife women.
Keywords: menopause, vasomotor symptoms, menopausal hormone therapy, non-hormonal treatments
Introduction
The menopause transition represents a significant change in a woman’s lifetime, marking the end of her reproductive years with the decline of the ovarian follicles and consequently endogenous estrogen.1 Menopause is defined as 12 months of amenorrhea, occurring at a median age of 51.3 years in the United States (US).1–3 Nearly 80% of women worldwide suffer from vasomotor symptoms (VMS) that can range in severity and affect quality of life and overall health.4–6
VMS persist for a median duration of 7 years and have been associated with significant comorbidities such as cardiovascular disease, bone disease, and cognitive complaints.7–10 Women who experience VMS during perimenopause may continue to have symptoms for much longer, with a median duration of almost 12 years.7 Other factors found to influence the risk of developing and duration of VMS include lower socioeconomic status, African American race, smoking, and baseline negative affect or mood.11 In the Study of Women’s Health Across the Nation (SWAN), African American and Hispanic women reported a median VMS duration of 10.1 years and 8.9 years, respectively, compared to non-Hispanic white, Chinese, and Japanese women who reported a median VMS duration of 6.5 years, 5.4 years, and 4.8 years, respectively.7
Lasting upwards of a decade for some women, VMS can have a significantly negative impact on overall health and wellbeing. Data show that women who experience frequent VMS (>6 days in the previous 2 weeks) also experience higher rates of anxiety, depression, difficulty sleeping, and overall impaired quality of life.12–15 Almost three out of four postmenopausal women in a multinational survey suffered from fatigue, and two out of three had difficulty sleeping.16 Although European, American, and Japanese women all reported that VMS impacted daily activities and work productivity, Japanese women felt the greatest impact particularly when menopausal sleep disturbances were included.16 Healthcare utilization and associated costs are also significantly higher for women with VMS.17 Despite these profound impacts, a survey of 1039 women ages 40–65 across the US showed that 73% of women had not received treatment for their VMS.18
Hormone therapy (HT) has been the cornerstone of VMS management and has been shown to be effective in reducing VMS severity and improving quality of life.19–21 Our understanding of the risks and benefits of HT has evolved over the last 20 years, in part due to publication of the initial results of the Women’s Health Initiative (WHI) trials and subsequent studies. However, based on subsequent analyses of the WHI data and publication of newer studies, the current guidelines suggest that the benefits of HT typically outweigh the risks for most symptomatic women under 60 years of age and within 10 years of their final menstrual period (FMP).19–21 For women who cannot or choose not to use HT, multiple nonhormone therapies are available. This review will evaluate the physiology of VMS and discuss hormonal and nonhormone options for treatment in addition to emerging therapies to guide clinicians caring for midlife women experiencing VMS.
Physiology of VMS
The menopause transition (MT) can be broken down into stages of progressive depletion of ovarian follicles and decreasing endogenous estradiol.22 During perimenopause, menses become increasingly variable in duration and frequency, and menopause occurs after complete cessation of menses for 12 months.22 VMS can begin during the perimenopausal stage, during which hormones have started to fluctuate, and last years past the FMP.7
Estrogen withdrawal during the menopause transition (MT) is associated with alterations in the hypothalamic thermoregulatory neutral zone, a group of neurons that regulate body temperature.23,24 Normally inhibited by estrogen, this group of hypothalamic neurons, known collectively as KNDy neurons for the co-expression of kisspeptin, neurokinin B (NKB), and dynorphin, are overstimulated during the MT and can lead to dysregulation of body temperature.23 These changes lead to an increased frequency of bodily reaction to both internal and environmental triggers that prevent heat loss.24 Feelings of flushing, warmth sensation, skin reddening, and perspiration can occur with resultant cutaneous vasodilation or constriction in a maladapted form of temperature homeostasis.24,25 In many women, the flushing of the skin and body can also be followed by profound chills as a side effect.26
Hormone Therapy
HT is the most effective treatment for VMS.19–21 HT use not only reduces symptom frequency but also intensity by nearly 90%, usually within one month of initiation.21,27 Generally well tolerated, the most common acute adverse effects of HT, particularly estrogen therapy, are breast pain and uterine bleeding.28
Considerations When Prescribing HT
For healthy, symptomatic women under the age of 60 years and less than 10 years from menopause onset, current evidence supports the use of HT.19–21 However, more than 80% of American women over the age of 50 years have at least one chronic medical condition that impacts decision-making regarding HT use.29 Globally, 55–98% of adults have more than one chronic condition, with women more likely than men to have multiple comorbidities.30 As such, most office visits focusing on menopause management will require an individualized approach when women have one or more chronic conditions that may impact decision-making and potential risks associated with HT use.
Cardiovascular Disease
Cardiovascular disease (CVD) is the leading cause of death in women worldwide, accounting for 35% of total deaths in women in 2019.31 Compared to men, women develop coronary artery disease (CAD) later in life, with increasing risk beginning in midlife and corresponding with the MT.32 The Heart and Estrogen/Progestin Replacement Study (HERS) and WHI trials showed an increased risk of CVD following initiation of conjugate equine estrogen (CEE) and medroxyprogesterone-acetate (MPA); in both trials, women who received CEE plus MPA had a significant increase in CVD events.33,34 However, subsequent follow-up of the WHI trials, plus newer trials such as the Kronos Early Estrogen Prevention Study (KEEPS) and Early Versus Late Intervention Trial with Estradiol (ELITE) that measured progression of atherosclerosis with HT use, showed that women who started HT early in menopause (within 36 months or less than 6 years from FMP, respectively) may not only avoid conferred CVD risks of HT but also have slower progression of atherosclerosis compared to women who utilized placebo.35,36 In 2015, a Cochrane review of randomized control trials (RCTs) demonstrated that women who started HT within 10 years of menopause had a 50% reduced risk of death from CAD and non-fatal myocardial ischemia, as well as a 30% reduced risk of all-cause mortality.37 CVD outcomes may also be affected by different HT routes, with transdermal estradiol being associated with lower CAD-related mortality compared to oral estrogens.38 Currently, HT is not indicated for primary or secondary prevention of CVD, including CAD.
Summary: In contrast to HT that is initiated in older women who are farther from the MT, when HT is started in women who are under the age of 60 years and within 10 years of menopause onset, CAD risks do not appear to be increased and there may be a cardioprotective effect. For women with a history of CAD, the risks of HT may exceed benefit, and non-hormonal options are recommended for VMS treatment.
Venous Thromboembolism
Venous thromboembolism (VTE) has an annual incidence of 117 per 100,000 persons, with cumulative incidence increasing with age.39,40 The relationship between estrogen use and VTE is well established, and women with a prior history of thromboembolic event or those who have obesity are at greater risk.41,42 In the 13-year follow-up of the WHI trials that extended beyond the intervention phases, no significant difference in risk of VTE was found between either HT formulation compared to placebo.43 Unlike CVD, risk of VTE was not found to differ by age at initiation.37 Non-oral formulations with lower doses of estrogen are associated with lower risk of VTE.44 Estrogen products are considered low dose if they contain less than 0.625mg CEE or 1mg estradiol for oral formulations and less than 50 μg for transdermal formulations.45 Compared to oral estrogen, transdermal route may not confer additional risk of VTE in women with an increased BMI >25kg/m2.44 In addition to estrogen, progestogen formulation may also impact conferred risk of VTE. Synthetic progestogens, including MPA and norpregnane, are associated with an increased risk of VTE, while micronized progesterone and dydrogesterone do not appear to increase risk of VTE beyond that conferred by estrogen therapy.46 Women on therapeutic anticoagulation for VTE may consider HT for VMS treatment.47
Summary: HT, particularly oral estrogens and synthetic progestogens, may increase risk of VTE; these risks may be increased in women that are overweight or obese. Using lower doses and transdermal formulations of estrogen as well as micronized progesterone or dydrogesterone may limit this conferred risk.
Stroke
An increased risk of ischemic stroke was identified during the intervention phases of both the CEE plus MPA and CEE-alone WHI trials for women aged 50 to 79 years of age.43 Ischemic stroke risk is affected by timing of initiation, as well as route and dose of estrogen. If HT is initiated in women less than 60 years of age or within 10 years of menopause, meta-analysis of RCTs shows no increased risk of stroke.37 Unlike oral estrogen which has an increased risk of ischemic stroke, transdermal estrogen does not confer the same risk.48 Risk of stroke appears dose-dependent with oral estrogens, with high doses (>0.625mg CEE, >2mg estradiol) being associated with greatest risk.49
Summary: For women who initiate treatment after age 60 years, HT may increase risk of stroke. Risk of stroke is greatest for high-dose oral (>0.625mg CEE, >2mg estradiol) estrogen formulations.
Breast Cancer
After publication of the WHI trials, overall use of HT substantially declined due to fear of increasing breast cancer risk.50 Although prospective WHI trial data showed that CEE plus MPA correlated with an increase in breast cancer events, a later retrospective systematic review showed that women taking CEE plus MPA had a cumulative increased incidence of breast cancer over time, increasing after about 3 years for women with prior HT use and 5 years for women without prior HT use.43,51 However, unlike CEE plus MPA, estrogen alone in women without a uterus did not appear to increase breast cancer risk if taken for less than 5 years.52,53 In fact, the 20-year follow-up of the WHI trials demonstrated a lower incidence of breast cancer and lower breast cancer mortality in women on CEE alone compared to placebo.54 Estrogen type, whether 17-beta estradiol or CEE, also does not seem to be associated with increased risk of breast cancer when taken alone; overall, the risk of breast cancer with HT use seems to increase with long term (>5 years) use.55–57
Multiple studies have shown an increased risk of breast cancer conferred by all estrogen plus progestogen combinations, though synthetic progestogens may have the highest risk.57 This risk can be decreased by using cyclic progestogen dosing.58–60 Synthetic progestogens, including norethisterone, levonorgestrel, and norgestrel, have been found to increase risk of breast cancer.55 Micronized progesterone and dydrogesterone may not produce the same degree of breast cancer risk as the synthetic progestogens.61 Other factors that may influence risk of breast cancer outside of hormone therapy include body habitus, alcohol consumption, and family history.57
The safety of HT use in women with a history of breast cancer is questionable with a concern regarding an increased risk of recurrence.62,63 For women with a prior history of breast cancer, HT should be avoided.
Summary: Though the risk is overall low, HT formulation may impact conferred risk of breast cancer. For women on estrogen alone, there does not appear to be an increased risk of breast cancer in the short term (<5 years). In women with an intact uterus requiring combined estrogen plus progestogen, cyclic dosing of micronized progesterone or dydrogesterone may confer the least risk of breast cancer.
Other Common Conditions
Many medical conditions can impact, or be impacted by the use of HT. Because diabetes is considered a CAD-equivalent, clinicians may be reluctant to prescribe HT.64 However, HT use has been shown to improve glycemic control and insulin resistance in women with and without type 2 diabetes, as well as other CVD risk factors such as lipid profile.65,66 Route and dose-dependent, HT can decrease low-density lipoprotein cholesterol (LDL-C) and lipoprotein(a) while increasing high-density lipoprotein cholesterol (HDL-C).67 In the short term, oral estrogen monotherapy appears to lower LDL-C and increase HDL-C, while transdermal estrogen may result in lower LDL-C without affecting HDL-C in the long term.68 More evaluation is needed regarding the impact of HT use on risk and severity of autoimmune conditions such as systemic lupus erythematosus (SLE) or rheumatoid arthritis (RA), but those with antiphospholipid syndrome, a hypercoagulable state associated with SLE, should avoid HT.69,70
Formulations and Approach to Prescribing
HT Formulation and Route of Administration
Formulations of estrogen include oral tablets, transdermal patches, topical gels/lotions, subcutaneous implants, and vaginal rings (Table 1). For women with an intact uterus, systemic estrogens must be paired with a progestogen or selective estrogen receptor antagonist (for example, bazedoxifene) to prevent the risk of endometrial hyperplasia and endometrial cancer associated with unopposed estrogen use (Table 2).63 Low dose vaginal estrogens, which are effective for management of genitourinary symptoms related to menopause, are insufficient for vasomotor symptom management.19
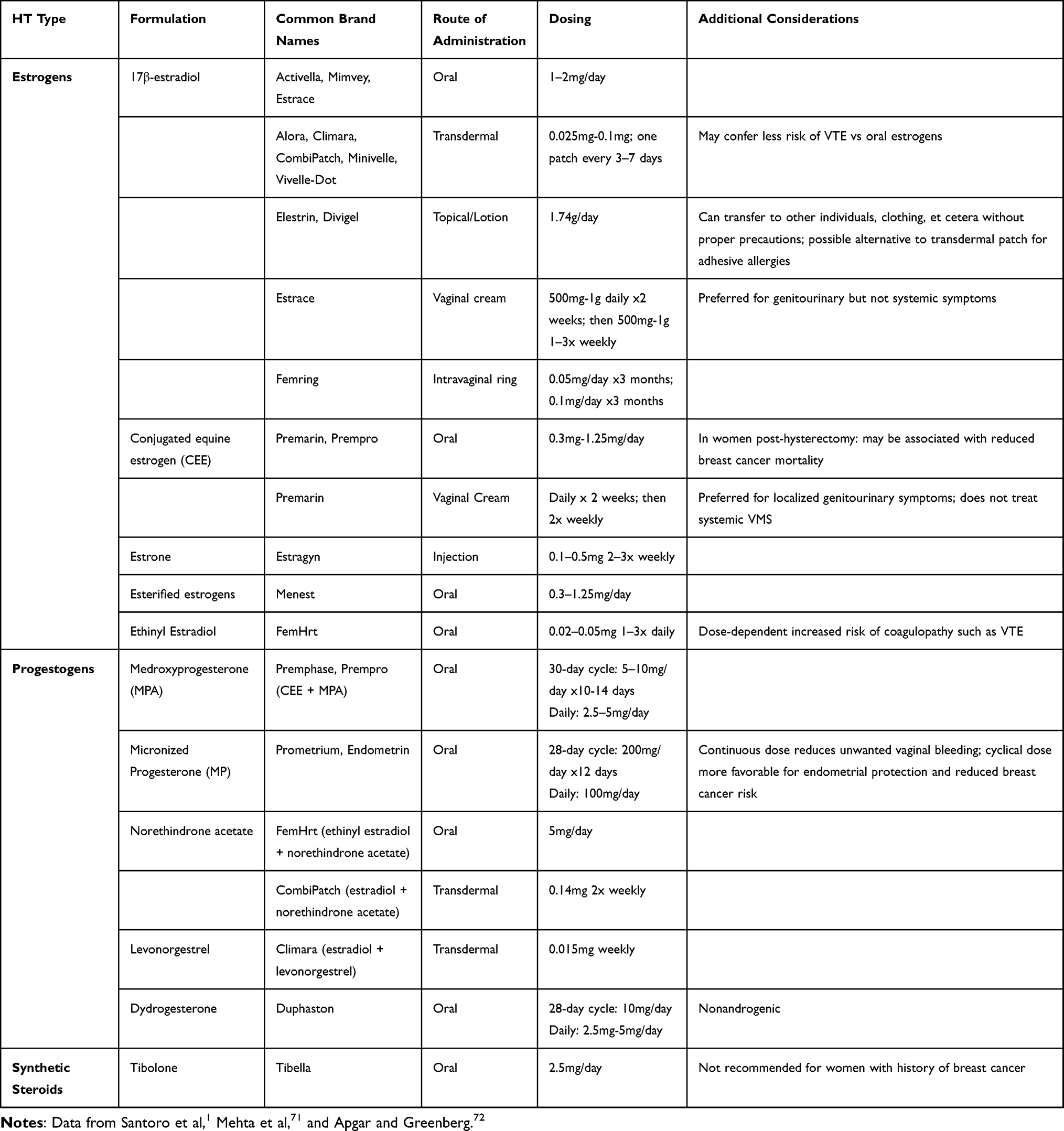 |
Table 1 Common HT Formulations |
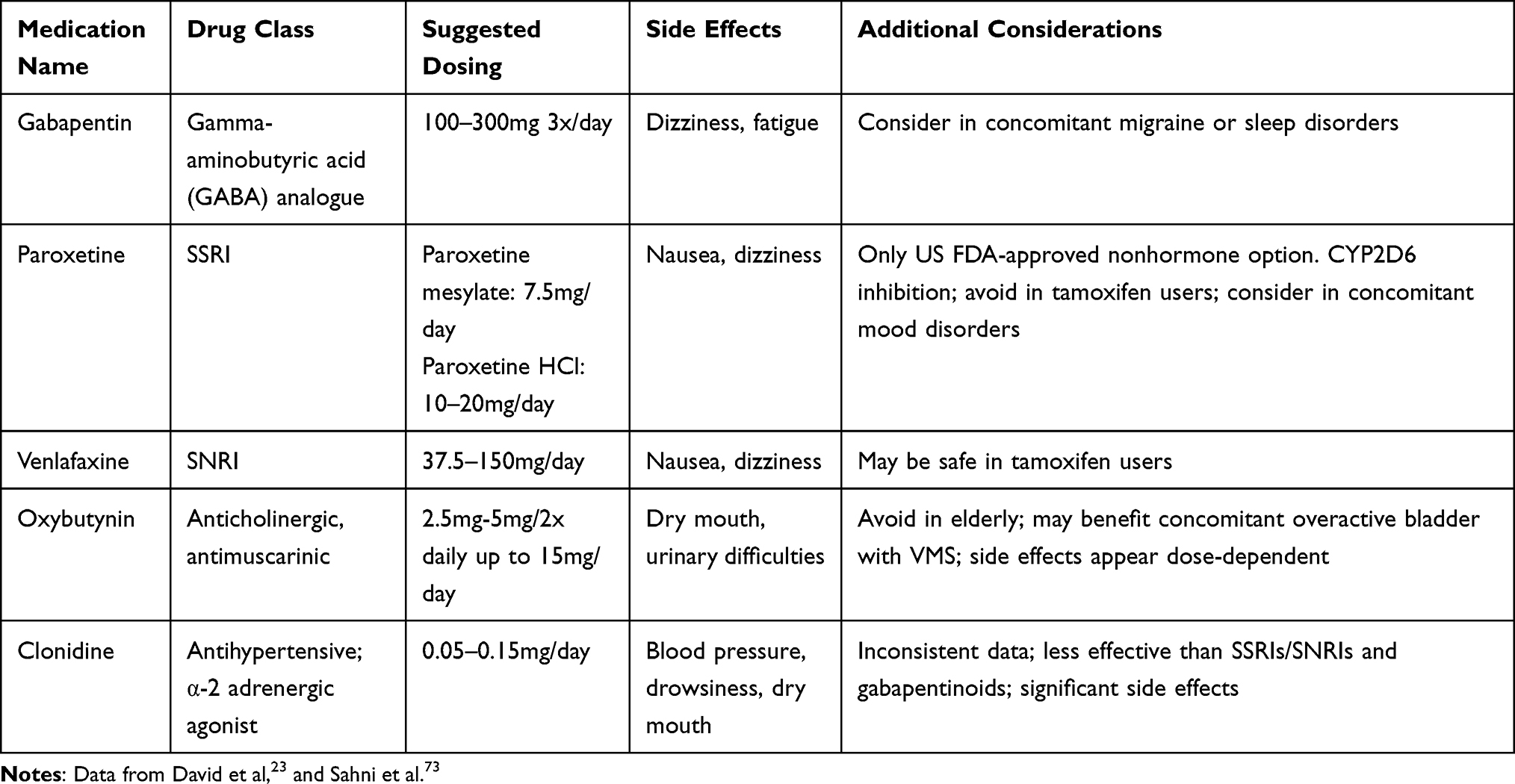 |
Table 2 Nonhormone Pharmacologic Therapies for Menopausal VMS |
Women can choose between a cyclic or continuous progestogen allowing for an individualized VMS treatment approach. Continuous combined therapies offer convenience, but cyclic therapy reduces progestogen exposure with the potential advantage of a lower risk of breast cancer and other unwanted side effects, particularly with synthetic progestogen use.74,75 Due to a possible side effect of drowsiness, it is suggested that micronized progesterone be taken at night.63 When comparing the various available formulations of systemic estrogen, transdermal formulations remain the preferred route of administration for women with obesity and a higher risk of VTE, and those with diabetes mellitus or increased risk of CVD.19
Tibolone
Although not currently available in the US, Tibolone is a synthetic steroid with metabolites possessing estrogenic, progestogenic, and androgenic properties often utilized in European countries for VMS treatment.20 Tibolone doses of 1.25 mg to 2.5 mg daily offer significant relief of VMS with lower breast tenderness rates compared to HT.76 Current data are conflicting regarding the endometrial cancer risk associated with the use of tibolone. The Tibolone Histology of the Endometrium and Breast Endpoints Study (THEBES) suggests that tibolone use does not seem to increase risk of endometrial hyperplasia or cancer, but the United Kingdom-based Million Women Study showed an increased risk of endometrial cancer in postmenopausal women using tibolone.77,78 Women with a history of breast cancer may have higher risk of recurrence when taking tibolone.79 While HT comprising estrogen plus progestogen may increase breast density, tibolone does not.20 Although additional data are needed, limited evidence suggests that tibolone may increase the risk of stroke in women over 60 years of age.80
International Guidelines and Long-Term Management of Patients on HT
International Guidelines for HT
Current guidelines support the use of HT in symptomatic menopausal women with consideration of age, time since menopause, and individual risk factors.19–21 The use of non-oral (transdermal) estrogen formulations as opposed to the oral route of administration may reduce the conferred risk of VTE, stroke, and CVD.81 For the duration of VMS treatment, progestogen therapy must be utilized in women with an intact uterus for endometrial protection.82 Unscheduled bleeding (outside the context of withdrawal bleeding) in women with an intact uterus using HT requires evaluation.19 When a progestogen is used, micronized progesterone may provide some safety advantages over synthetic progestogens, but RCT comparative data are limited.82 Guideline-based breast cancer and cervical cancer screening should be continued while women are on HT.
Contraindications for HT
Clinicians should be aware of several contraindications for HT. Women with a prior history of CAD, stroke, myocardial infarction, unprovoked VTE, or those who are at high risk for CVD should avoid HT.19,21 Unexplained vaginal bleeding should be evaluated prior to consideration of HT.19,21 In the setting of prior estrogen-sensitive cancers, such as breast cancer, systemic HT should be avoided.19,21
Long-Term Management of HT
Ultimately, individualizing therapy with the appropriate dose and duration of HT to treat a woman’s VMS is recommended. While HT does not need to be routinely discontinued at the age of 60 years, continued monitoring for new health concerns, periodic trials of tapered HT doses, and attempts at HT discontinuation should be made for women nearing the age of 60–65 years old.19 Currently, data are insufficient to suggest an optimal way to discontinue HT, but gradual tapering is generally favored over stopping abruptly.19 Regardless of age or treatment duration, at the time of HT cessation, approximately 50% of women experience recurrence of VMS.83 Longer duration of HT use can be considered in women older than 65 years old who experience persistent VMS impacting quality of life, or for bone density protection, though regular reassessment of the risk to benefit balance and shared decision should be used.19 For women who are fearful about discontinuing HT, clinicians could consider a slow taper over months and provide reassurance that the last effective dose may be restarted if bothersome symptoms return.84
Non hormone Therapies for VMS Management
Although HT is the mainstay of VMS treatment, nonhormone options should be made available for women who have medical contraindications to HT use or a personal preference to avoid it. Surveys have shown that 50% to 80% of midlife women use nonhormone therapies as treatment for VMS.19,85 Although many large-scale studies have shown evidence that alternative therapies may help mitigate VMS, low-dose paroxetine (Brisdelle™) is the only nonhormone treatment approved by the US Food and Drug Administration (FDA) for the treatment of VMS.86
Lifestyle Modifications
Exercise, weight loss, and cooling techniques may be associated with improvement in VMS, although there are less conclusive data compared to other treatment modalities. Early observational studies showed that physically active women had less severe hot flashes compared to those who were less active or sedentary.87,88 However, Cochrane review of studies on the impact of physical activity on VMS severity suggests that there is insufficient evidence supporting the efficacy of exercise in management of VMS.89 The overall quality of evidence is poor due to inconsistent exercise interventions as well as inconsistent comparisons between intervention and no intervention and lack of direct comparison with HT use.89 As such, the current evidence does not support physical activity as a treatment for VMS.90
While physical activity may not directly alleviate VMS, weight loss induced by better lifestyle choices does seem to be associated with reduced symptoms.91 Perimenopausal women with obesity are more likely than their normal or overweight counterparts to experience menopausal symptoms.92 In an RCT of 40 overweight or obese women, those who were randomized to 6 months of behavioral weight loss intervention not only lost more weight, but they also reported fewer episodes of hot flashes.91 However, even as the frequency of hot flashes improved with weight loss, symptom severity was not statistically different between the two groups.91
Finally, with the underlying pathophysiology of VMS revolving around body temperature regulation, it would seem intuitive that cooling techniques may provide symptom relief. When comparing the effect of a handheld mechanical cooling device at the base of the neck during a hot flash, no statistical difference was found in VMS compared to sham-device.93 Altogether, there is insufficient evidence to support body cooling techniques as an effective treatment for VMS.90
Mind-Body Techniques
Cognitive Behavioral Therapy
Cognitive behavioral therapy (CBT) is a form of psychotherapy well studied in mental health conditions such as depression and anxiety, and health conditions such as chronic pain.94,95 Relatively risk-free, it offers women a non-pharmaceutical option that has shown effectiveness in alleviating VMS.83 In an RCT assessing CBT for menopausal symptoms (CBT-Meno), symptomatic women who received CBT reported a significant improvement in their VMS symptom interference and bother compared to no active intervention.96
CBT has been shown to be effective in reducing the severity but not the frequency of VMS in 2 randomized, double-blind, controlled trials: MENOS 1 and MENOS 2.97,98 In clinical practice, limited access and the cost of CBT may be prohibitive factors in its use. However, internet-delivered CBT adapted from the MENOS protocols has been shown to have high compliance rates and is associated with reduced VMS severity, which may provide a reasonable option for management.99
Clinical Hypnosis
Clinical hypnosis is a mind-body technique that induces a tranquil state using mental imagery and suggestion.20,90 A randomized, single-blind, controlled clinical trial comparing hypnosis to structured-attention control, hypnosis showed a reduction in hot flash frequency and overall reduction in severity by week 6 and continuing into week 12.100 Approaching the efficacy of HT, hypnotherapy reduced hot flashes by 80%, and participants reported high treatment satisfaction.100 Like CBT, lack of availability may limit the utility of clinical hypnosis, but newer online self-management programs may make hypnotherapy more accessible.101
Pharmacologic Therapies
Multiple clinical trials have identified therapeutic effects of SSRIs and SNRIs in treating VMS. In the practical setting, these benefits must be weighed against the dose-dependent significant adverse effects such as dry mouth, nausea, constipation, decreased libido, and weight gain.102 Additionally, because SSRIs and SNRIs may lead to inhibition of cytochrome P450 enzyme pathways (CYP450: CYP2D6), special consideration should also be given to potential medication interactions when prescribing these medications.23
Low dose paroxetine is currently the only US FDA-approved nonhormone treatment of moderate-to-severe VMS.103 Taken at a dose of 7.5mg daily, paroxetine has shown improvements in VMS frequency and severity, as well as improvement in sleep disruption without negative effects such as decreased libido or weight gain.104–106 After 4 weeks of use, women taking paroxetine 7.5mg daily had 33% fewer hot flashes compared to 23% for those using placebo.106 This benefit continued through 12 weeks of use but was not statistically significant at 24 weeks.106 Because of CYP2D6 inhibition, paroxetine should be used with caution in breast cancer patients taking tamoxifen.107
Venlafaxine, an SNRI, is one of few nonhormone agents that has been studied head-to-head against HT in an RCT.108 The study showed that venlafaxine 75mg daily was as effective as low-dose oral estradiol (0.5 mg daily) in reducing frequency of hot flashes, with a reduction of 1.8/day versus 2.3/day, respectively.108 However, dose escalation of estradiol was not performed in this study, which might have been expected to improve hot flashes by 77% on average.28 One particular advantage of venlafaxine is that it does not interact with the CYP450 system and therefore can be safely prescribed in tamoxifen users.107
Other SSRI/SNRIs available for consideration in VMS treatment include citalopram, escitalopram, and desvenlafaxine, each having shown statistically significant improvement in VMS in multiple meta-analyses and systematic reviews.109–111 Others including sertraline and fluoxetine have not shown statistically significant results and therefore may not be the first-choice options.109,112
Gabapentin is a gamma-aminobutyric acid (GABA) analogue that shows promising efficacy in relieving VMS.113 Initially used in the 1990s for treatment of seizures, gabapentin’s use has since broadened to neuropathic pain, various mood disorders, and essential tremor.114 The mechanism underlying gabapentin and pregabalin’s effect on VMS is not well understood, but it is hypothesized that they reduce the hyperadrenergic response and widening of the hypothalamic thermoregulatory neutral zone.113 Currently, clinical guidelines from American, European, and Asian countries support the use of these two medications as nonhormone alternatives in managing VMS.83,102,115
In a recent systematic review and meta-analysis of 19 RCTs and 2 randomized cross-over studies, gabapentin was found to reduce hot flash frequency after just 4 weeks of treatment in postmenopausal women, including breast cancer survivors, but there was no difference in hot flash duration.113 The recommended total daily dose of gabapentin for this indication is 900 mg/day split between three 300 mg doses.90 Although promising, gabapentin is inferior to estrogen therapy in reducing hot flash frequency and severity.113 It may be a preferred nonhormone option in women with other indications for its use, including migraine and sleep disorders.
Oxybutynin is an anticholinergic, antimuscarinic medication that the US FDA approved for the treatment of urge incontinence overactive bladder.116 A 12-week, multicenter, double-blind, placebo-controlled Phase II clinical trial comparing 15 mg extended-release oxybutynin to placebo showed significant reductions in frequency and severity of moderate-to-severe VMS through week 12 in the oxybutynin users.116 Women receiving oxybutynin reported improvement in VMS, sleep, and quality of life at 4 weeks, with persistent efficacy at 12 weeks.116 At a dose of 15 mg, oxybutynin was associated with side effects including dry mouth and urinary difficulties. A subsequent trial utilizing lower doses of 2.5 or 5 mg twice a day showed a reduction in hot flash frequency and severity with fewer side effects.117 Oxybutynin should be used with caution in older women due to anticholinergic side effects including the potential risk for impaired cognition.118,119 However, use in young women experiencing VMS is a reasonable and effective option, especially for women who also suffer from overactive bladder symptoms.
Clonidine
Clonidine is a centrally acting α-adrenergic agonist that reduces norepinephrine release and potentially raises the sweating threshold set by the hypothalamic regulatory center.120 In a randomized, double-blind, controlled trial of 110 women with a history of breast cancer, those who received 0.1 mg transdermal clonidine patch reported a 20% reduction in VMS compared to placebo.121 These findings were replicated in a second study where 149 postmenopausal women reported a reduction in frequency of hot flashes by 38% after 8 weeks compared to 24% reduction with placebo.122 Both studies revealed that clonidine was associated with significant side effects such as dry mouth, constipation, pruritus, and drowsiness.121,122 Overall, the limited efficacy and significant side effects limit the clinical use of clonidine for VMS management.
Non-Pharmacologic Therapies
Stellate ganglion block (SGB) is a nonhormone treatment option for VMS. The stellate ganglion is a cluster of sympathetic nerves in the lower-cervical and upper-thoracic area, encompassing the C6 region of the anterior cervical spine.123 By administering a local anesthetic such as lidocaine under fluoroscopic and ultrasonographic guidance, SGB has been used for the past 50 years as a targeted treatment for pain syndromes such as migraine, upper extremity and upper body pain, as well as complex regional pain syndromes.124 While data show that SGB may improve VMS, the mechanism is unclear. Several small studies have shown that, whether approached unilaterally or bilaterally, SGB reduces hot flash severity by 45% to 90% in about 4–24 weeks.123,125 In an RCT of bupivacaine SGB compared to sham-control, only those who suffered moderate-to-severe VMS had significant reduction in symptom frequency.123 Most studies reported no significant adverse events, although there are rare risks associated with the injection itself.124 These complications can include damage to the surrounding areas, such as the vasculature, neural tissue, esophagus, or trachea.124 Risk of complications can be mitigated with imaging guidance. The use of SGB in clinical practice is limited by high cost and limited availability.
Isoflavones, most commonly consumed in soy, are phytochemicals within a group of nonsteroidal compounds that bind to estrogen receptors.126 They possess both estrogen-agonist and estrogen-antagonist properties due to varying affinity for different estrogen receptors.125 Common examples include genistein and daidzein that are found in high amounts in soy products, among other foods.126 A systematic literature review of 17 RCTs showed conflicting data for dietary consumption of genistein 54 mg daily in VMS treatment, and isoflavone use has significant side effects including bloating, flatulence, and diarrhea.90,127
Acupuncture is a potential non-medication alternative for the treatment of VMS. It is a form of Chinese medicine in which small needles are inserted into the skin, targeting specific areas to balance the flow of energy in the body.128 Unlike traditional acupuncture, sham acupuncture is the placement of needles in unrelated points on the body without piercing the skin.128 Many clinical trials have suggested that while acupuncture is superior to no treatment for VMS, when compared head-to-head, acupuncture is not superior to sham acupuncture.128
New and Novel Therapies for VMS Treatment
Estetrol (E4)
Estetrol (E4) is a natural human fetal estrogen with selective action in the tissues that works by activating nuclear estrogen receptor α (ERα) leading to a cascade of coregulator activators and repressors similar to estradiol (E2) and estriol (E3) but in a different pattern than tamoxifen or raloxifene.129 In mouse models, it acts synergistically with endogenous estrogens in bone, vasculature, vaginal tissues, and endometrium with fewer effects on the liver and breast than E2.129 In an early human trial evaluating escalating doses of E4 from 2 mg to 10 mg over a period of 8 weeks, E4 use appeared to be safe without any evidence for significant adverse events.130 Although VMS frequency seems to be reduced with as low as 2 mg E4, a minimum dose of 15 mg was needed to reduce VMS severity.129,130 Currently marketed as a contraceptive agent, the possibility of an improved safety profile compared to E2 makes E4 a promising future option for VMS treatment.
Neurokinin B Antagonism (NK3R Antagonists)
Our understanding of VMS pathophysiology has expanded with the identification of specialized hypothalamic KNDy neurons that utilize neurokinin B (NKB) signaling on neurokinin 3 receptor (NK3R).131 This signaling pathway appears influential in the development of hot flashes within the hypothalamic thermoregulatory neutral zone.131 Through NK3R antagonism, the signaling pathway can be disrupted and potentially attenuate VMS.
Several NK3R antagonists are in Phase 3 and 4 trials.131 In a 12-week double-blind study comparing varying doses of fezolinetant (15, 30, 60, or 90 mg twice daily or 30, 60, or 120 mg daily) to placebo, 93% of women in the active medication arm showed improvement in moderate-to-severe VMS compared to 39% of women receiving placebo.132 Even more promising is its rapid onset: the mean duration of treatment to achieve a 50% reduction in VMS was about 8.4 days for the 15 mg BID dose and 2.2 days for 90 mg BID dose, compared to an average of 6 to 8 weeks for HT to provide adequate symptom relief.19,132 Adverse events were generally mild and not dose dependent, the most common being nausea, upper respiratory tract infection, headache, diarrhea, urinary tract infection, and cough.133
Another novel selective antagonist of the neurokinin pathway focusing on NK1 and NK3 receptors is NT-814.134 In RELENT-1, a 14-day, Phase II, RCT of the safety and efficacy of 50, 100, 150, and 300 mg daily of NT-814, women who received the 150 mg dose had an 84% reduction in hot flashes compared to 37% in the placebo group. The women who received other doses of the active medication had a 20–60% reduction in their hot flashes.134 SWITCH-1 was a 12-week, phase IIb, double-blind RCT designed to assess optimal dosing of NT-814 using the doses 40, 80, 120, or 160 mg daily compared to placebo.135 All groups showed promising reductions in VMS compared to placebo, with the greatest improvements in the 120 and 160 mg groups after 12 weeks with 7.8 and 6.9 fewer moderate/severe VMS per day, respectively.135 Similar to the NK3R antagonists, no serious adverse events were reported.135
Conclusion
Despite the high prevalence, significant impact on quality of life, and a variety of safe and effective treatment options, VMS remain undertreated. HT remains the gold-standard, most effective treatment for VMS, but many symptomatic women do not use it for a variety of reasons, including perceived safety concerns. The benefits of HT outweigh the risks for healthy women under age 60 and/or within 10 years from their FMP. While HT use is a consideration for a majority of symptomatic, healthy, and recently menopausal women, nonhormone options may be utilized for women with contraindications to HT use, or for those who prefer to avoid HT use for any reason. Emerging therapies may provide additional options for women with bothersome VMS.
Abbreviations
VMS, vasomotor symptoms; HT, hormone therapy; WHI, Women’s Health Initiative; FMP, final menstrual period; MT, menopause transition; NKB, neurokinin B; CVD, cardiovascular disease; CAD, coronary artery disease; CEE, conjugate equine estrogen; MPA, medroxyprogesterone-acetate; RCT, randomized control trial; VTE, venous thromboembolism; CBT, cognitive behavioral therapy; SSRI/SNRI, selective serotonin reuptake inhibitor/serotonin-norepinephrine reuptake inhibitor; SBG, stellate ganglion block; E4, estetrol; E2, estradiol; NK3R, neurokinin 3 receptor.
Disclosure
Dr. Kling reports personal fees from Proctor and Gamble and Triangle Insights Group outside the submitted work. Dr. Kapoor reports personal fees from Astellas Pharmaceuticals and Womaness and grants and personal fees from Mithra Pharmaceuticals outside the submitted work. Otherwise, no other conflicts of interest exist to be reported.
References
1. Santoro N, Roeca C, Peters BA, Neal-Perry G. The menopause transition: signs, symptoms, and management options. J Clin Endocrinol Metab. 2021;106(1):1–15. PMID: 33095879. doi:10.1210/clinem/dgaa764
2. Soules MR, Sherman S, Parrott E, et al. Executive summary: stages of Reproductive Aging Workshop (STRAW). Climacteric. 2001;4(4):
3. U.S. Preventive Services Task Force. Hormone therapy for the primary prevention of chronic conditions in postmenopausal women: recommendation statement. Am Fam Phys. 2018;97(8):540A–540D.
4. Pinkerton JV, Santen RJ. Managing vasomotor symptoms in women after cancer. Climacteric. 2019;22(6):544–552. doi:10.1080/13697137.2019.1600501
5. Freeman EW, Sherif K. Prevalence of hot flushes and night sweats around the world: a systematic review. Climacteric. 2007;10(3):197–214. doi:10.1080/13697130601181486
6. Whiteley J, Wagner JS, Bushmakin A, Kopenhafer L, Dibonaventura M, Racketa J. Impact of the severity of vasomotor symptoms on health status, resource use, and productivity. Menopause. 2013;20:518–524.
7. Avis NE, Crawford SL, Greendale G, et al.; Study of Women’s Health Across the Nation. Duration of menopausal vasomotor symptoms over the menopause transition. JAMA Intern Med. 2015;175(4):531–539. PMID: 25686030; PMCID: PMC4433164. doi:10.1001/jamainternmed.2014.8063
8. Thurston RC, Sutton-Tyrrell K, Everson-Rose SA, Hess R, Matthews KA. Hot flashes and subclinical cardiovascular disease: findings from the Study of Women’s Health Across the Nation Heart Study. Circulation. 2008;118:1234–1240.
9. Crandall CJ, Aragaki A, Cauley JA, et al. Associations of menopausal vasomotor symptoms with fracture incidence. J Clin Endocrinol Metab. 2015;100:524–534.
10. Maki PM. Verbal memory and menopause. Maturitas. 2015;82(3):288–290. PMID: 26433715. doi:10.1016/j.maturitas.2015.07.023
11. Thurston RC, Joffe H. Vasomotor symptoms and menopause: findings from the Study of Women’s Health across the Nation. Obstet Gynecol Clin North Am. 2011;38(3):489–501. doi:10.1016/j.ogc.2011.05.006
12. Bromberger JT, Kravitz HM, Chang Y, et al. Does risk for anxiety increase during the menopausal transition? Study of Women’s Health Across the Nation. Menopause. 2013;20(5):488–495.
13. Bromberger JT, Matthews KA, Schott LL, et al. Depressive symptoms during the menopausal transition: the Study of Women’s Health Across the Nation (SWAN). J Affect Disord. 2007;103(1–3):267–272.
14. Kravitz HM, Zhao X, Bromberger JT, et al. Sleep disturbance during the menopausal transition in a multi-ethnic community sample of women. Sleep. 2008;31(7):979–990.
15. Avis NE, Colvin A, Bromberger JT, et al. Change in health-related quality of life over the menopausal transition in a multiethnic cohort of middle-aged women: study of Women’s Health Across the Nation. Menopause. 2009;16(5):860–869.
16. Nappi RE, Kroll R, Siddiqui E, et al. Global cross-sectional survey of women with vasomotor symptoms associated with menopause: prevalence and quality of life burden. Menopause. 2021;28(8):875–882. doi:10.1097/GME.0000000000001793
17. Sarrel P, Portman D, Lefebvre P, et al. Incremental direct and indirect costs of untreated vasomotor symptoms. Menopause. 2015;22(3):260–266. PMID: 25714236. doi:10.1097/GME.0000000000000320
18. Bonafide Health LLC. State of menopause survey. Bonafide website; 2021. Available from: https://cdn.shopify.com/s/files/1/0011/8590/6751/files/Bonafide_State_of_Menopause.pdf?v=1624280664.
19. The NAMS 2022 Hormone Therapy Position Statement Advisory Panel. The 2022 hormone therapy position statement of The North American Menopause Society. Menopause. 2022;29(7):767–794. doi:10.1097/GME.0000000000002028
20. Mintziori G, Lambrinoudaki I, Goulis DG, et al. EMAS position statement: non-hormonal management of menopausal vasomotor symptoms. Maturitas. 2015;81(3):410–413. doi:10.1016/j.maturitas.2015.04.009
21. Baber RJ, Panay N, Fenton A; IMS Writing Group. 2016 IMS recommendations on women’s midlife health and menopause hormone therapy. Climacteric. 2016;19(2):109–150. PMID: 26872610. doi:10.3109/13697137.2015.1129166
22. Harlow SD, Gass M, Hall JE, et al. Executive summary of the Stages of Reproductive Aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging. Menopause. 2012;19(4):387–395.
23. David PS, Smith TL, Nordhues HC, Kling JM. A clinical review on paroxetine and emerging therapies for the treatment of vasomotor symptoms. Int J Womens Health. 2022;14:353–361. PMID: 35300283; PMCID: PMC8921794. doi:10.2147/IJWH.S282396
24. Deecher DC, Dorries K. Understanding the pathophysiology of vasomotor symptoms (hot flushes and night sweats) that occur in perimenopause, menopause, and postmenopause life stages. Arch Womens Ment Health. 2007;10(6):247–257. PMID: 18074100. doi:10.1007/s00737-007-0209-5
25. Rapkin AJ. Vasomotor symptoms in menopause: physiologic condition and central nervous system approaches to treatment. Am J Obstet Gynecol. 2007;196(2):97–106. PMID: 17306645. doi:10.1016/j.ajog.2006.05.056
26. Kronenberg F. Hot flashes: epidemiology and physiology. Ann N Y Acad Sci. 1990;592:52–86;discussion 123–33. PMID: 2197954. doi:10.1111/j.1749-6632.1990.tb30316.x
27. Nelson HD, Haney E, Humphrey L, et al. Management of menopause-related symptoms. Evid Rep Technol Assess. 2005;120:1–6. PMID: 15910013; PMCID: PMC4782129.
28. Maclennan AH, Broadbent JL, Lester S, Moore V. Oral oestrogen and combined oestrogen/progestogen therapy versus placebo for hot flushes. Cochrane Database Syst Rev. 2004;2004(4):CD002978. doi:10.1002/14651858.CD002978.pub2
29. Boersma P, Black LI, Ward BW. Prevalence of multiple chronic conditions among US adults, 2018. Prev Chronic Dis. 2020;17:200130. doi:10.5888/pcd17.200130
30. Marengoni A, Angleman S, Melis R, et al. Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev. 2011;10(4):430–439. doi:10.1016/j.arr.2011.03.003
31. Vogel B, Acevedo M, Appelman Y, et al. The Lancet women and cardiovascular disease Commission: reducing the global burden by 2030. Lancet. 2021;397(10292):2385–2438. doi:10.1016/S0140-6736(21)00684-X
32. El Khoudary SR, Aggarwal B, Beckie TM, et al. Menopause transition and cardiovascular disease risk: implications for timing of early prevention: a scientific statement from the American Heart Association. Circulation. 2020;142(25):e506–e532. doi:10.1161/CIR.0000000000000912
33. Chester RC, Kling JM, Manson JE. What the Women’s Health Initiative has taught us about menopausal hormone therapy. Clin Cardiol. 2018;41(2):247–252. doi:10.1002/clc.22891
34. Hulley S, Grady D, Bush T, et al.; Heart and Estrogen/progestin Replacement Study (HERS) Research Group. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. JAMA. 1998;280:605–613.
35. Miller VM, Naftolin F, Asthana S, et al. The Kronos Early Estrogen Prevention Study (KEEPS): what have we learned? Menopause. 2019;26(9):1071–1084. doi:10.1097/GME.0000000000001326
36. Hodis HN, Mack WJ, Henderson VW, et al. Vascular effects of early versus late postmenopausal treatment with estradiol. N Engl J Med. 2016;374(13):1221–1231. doi:10.1056/NEJMoa1505241
37. Boardman HM, Hartley L, Eisinga A, et al. Hormone therapy for preventing cardiovascular disease in post-menopausal women. Cochrane Database Syst Rev. 2015;(3):CD002229. doi:10.1002/14651858.CD002229.pub4
38. Simon JA, Laliberté F, Duh MS, et al. Venous thromboembolism and cardiovascular disease complications in menopausal women using transdermal versus oral estrogen therapy. Menopause. 2016;23(6):600–610. doi:10.1097/GME.0000000000000590
39. Silverstein MD, Heit JA, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ. Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med. 1998;158(6):585–593. doi:10.1001/archinte.158.6.585
40. ESHRE Capri Workshop Group. Venous thromboembolism in women: a specific reproductive health risk. Hum Reprod Update. 2013;19(5):471–482. doi:10.1093/humupd/dmt028
41. Cushman M, Kuller LH, Prentice R, et al. Estrogen plus progestin and risk of venous thrombosis. JAMA. 2004;292(13):1573–1580. doi:10.1001/jama.292.13.1573
42. Abou-Ismail MY, Citla Sridhar D, Nayak L. Estrogen and thrombosis: a bench to bedside review. Thromb Res. 2020;192:40–51. doi:10.1016/j.thromres.2020.05.008
43. Manson JE, Chlebowski RT, Stefanick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA. 2013;310(13):1353–1368. doi:10.1001/jama.2013.278040
44. Canonico M, Oger E, Conard J, et al.; The ESTHER Study. Obesity and risk of venous thromboembolism among postmenopausal women: differential impact of hormone therapy by route of estrogen administration. J Thromb Haemost. 2006;4(6):1259–1265. doi:10.1111/j.1538-7836.2006.01933.x
45. Renoux C, Dell’Aniello S, Suissa S. Hormone replacement therapy and the risk of venous thromboembolism: a population-based study. J Thromb Haemost. 2010;8(5):979–986. doi:10.1111/j.1538-7836.2010.03839.x
46. Canonico M, Plu-Bureau G, Scarabin PY. Progestogens and venous thromboembolism among postmenopausal women using hormone therapy. Maturitas. 2011;70(4):354–360. doi:10.1016/j.maturitas.2011.10.002
47. Martinelli I, Lensing AW, Middeldorp S, et al. Recurrent venous thromboembolism and abnormal uterine bleeding with anticoagulant and hormone therapy use. Blood. 2016;127(11):1417–1425. doi:10.1182/blood-2015-08-665927
48. Canonico M, Carcaillon L, Plu-Bureau G, et al. Postmenopausal hormone therapy and risk of stroke: impact of the route of estrogen administration and type of progestogen. Stroke. 2016;47(7):1734–1741. doi:10.1161/STROKEAHA.116.013052
49. Parkin DM. Cancers attributable to exposure to hormones in the UK in 2010. Br J Cancer. 2011;105(Suppl2):S42–S48. doi:10.1038/bjc.2011.483
50. Anderson GL, Chlebowski RT, Rossouw JE, et al. Prior hormone therapy and breast cancer risk in the Women’s Health Initiative randomized trial of estrogen plus progestin. Maturitas. 2006;55(2):103–115. doi:10.1016/j.maturitas.2006.05.004
51. Chen WY, Manson JE, Hankinson SE, et al. Unopposed estrogen therapy and the risk of invasive breast cancer. Arch Intern Med. 2006;166(9):1027–1032. doi:10.1001/archinte.166.9.1027
52. Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291(14):1701–1712. doi:10.1001/jama.291.14.1701
53. Chlebowski RT, Anderson GL, Aragaki AK, et al. Association of menopausal hormone therapy with breast cancer incidence and mortality during long-term follow-up of the women’s health initiative randomized clinical trials. JAMA. 2020;324(4):369–380. doi:10.1001/jama.2020.9482
54. Yang Z, Hu Y, Zhang J, Xu L, Zeng R, Kang D. Estradiol therapy and breast cancer risk in perimenopausal and postmenopausal women: a systematic review and meta-analysis. Gynecol Endocrinol. 2017;33(2):87–92. doi:10.1080/09513590.2016.1248932
55. Abenhaim HA, Suissa S, Azoulay L, Spence AR, Czuzoj-Shulman N, Tulandi T. Menopausal hormone therapy formulation and breast cancer risk. Obstet Gynecol. 2022;139(6):1103–1110. doi:10.1097/AOG.0000000000004723
56. Vinogradova Y, Coupland C, Hippisley-Cox J. Use of hormone replacement therapy and risk of breast cancer: nested case-control studies using the QResearch and CPRD databases. BMJ. 2020;371:m3873. doi:10.1136/bmj.m3873
57. Beral V; Million Women Study Collaborators. Breast cancer and hormone-replacement therapy in the Million Women Study. Lancet. 2003;362(9382):419–427. doi:10.1016/s0140-6736(03)14065-2
58. Fournier A, Berrino F, Riboli E, Avenel V, Clavel-Chapelon F. Breast cancer risk in relation to different types of hormone replacement therapy in the E3N-EPIC cohort. Int J Cancer. 2005;114(3):448–454. doi:10.1002/ijc.20710
59. Collaborative Group on Hormonal Factors in Breast Cancer. Type and timing of menopausal hormone therapy and breast cancer risk: individual participant meta-analysis of the worldwide epidemiological evidence. Lancet. 2019;394(10204):1159–1168. doi:10.1016/S0140-6736(19)31709-X
60. Asi N, Mohammed K, Haydour Q, et al. Progesterone vs. synthetic progestins and the risk of breast cancer: a systematic review and meta-analysis. Syst Rev. 2016;5(1):121. doi:10.1186/s13643-016-0294-5
61. von Schoultz E, Rutqvist LE; Stockholm Breast Cancer Study Group. Menopausal hormone therapy after breast cancer: the Stockholm randomized trial. J Natl Cancer Inst. 2005;97(7):533–535. doi:10.1093/jnci/dji071
62. Holmberg L, Iversen OE, Rudenstam CM, et al. Increased risk of recurrence after hormone replacement therapy in breast cancer survivors. J Natl Cancer Inst. 2008;100:475–482. doi:10.1093/jnci/djn058
63. Effects of hormone replacement therapy on endometrial histology in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. The Writing Group for the PEPI Trial. JAMA. 1996;275(5):370–375. doi:10.1001/jama.1996.03530290040035
64. Slopien R, Wender-Ozegowska E, Rogowicz-Frontczak A, et al. Menopause and diabetes: EMAS clinical guide. Maturitas. 2018;117:6–10.
65. de Lauzon-Guillain B, Fournier A, Fabre A, et al. Menopausal hormone therapy and new-onset diabetes in the French Etude Epidemiologique de Femmes de la Mutuelle Generale de l’Education Nationale (E3N) cohort. Diabetologia. 2009;52(10):2092–2100.
66. Salpeter SR, Walsh JM, Ormiston TM, Greyber E, Buckley NS, Salpeter EE. Meta-analysis: effect of hormone-replacement therapy on components of the metabolic syndrome in postmenopausal women. Diabetes Obes Metab. 2006;8(5):538–554.
67. Koh KK, Shin MS, Sakuma I, et al. Effects of conventional or lower doses of hormone replacement therapy in postmenopausal women. Arterioscler Thromb Vasc Biol. 2004;24(8):1516–1521.
68. Kopper NW, Gudeman J, Thompson DJ. Transdermal hormone therapy in postmenopausal women: a review of metabolic effects and drug delivery technologies. Drug Des Devel Ther. 2009;2:193–202.
69. Walitt B, Pettinger M, Weinstein A, et al. Effects of postmenopausal hormone therapy on rheumatoid arthritis: the women’s health initiative randomized controlled trials. Arthritis Rheum. 2008;59(3):302–310.
70. Grygiel-Gorniak B, Limphaibool N, Puszczewicz M. Clinical implications of systemic lupus erythematosus without and with antiphospholipid syndrome in peri- and postmenopausal age. Prz Menopauzalny. 2018;17(2):86–90.
71. Mehta J, Kling JM, Manson JE. Risks, benefits, and treatment modalities of menopausal hormone therapy: current concepts. Front Endocrinol. 2021;12:564781. doi:10.3389/fendo.2021.564781
72. Apgar BS, Greenberg G. Using progestins in clinical practice. Am Fam Physician. 2000;62(8):1839–1850.
73. Sahni S, Lobo-Romero A, Smith T. Contemporary non-hormonal therapies for the management of vasomotor symptoms associated with menopause: a literature review. touchREV Endocrinol. 2021;17(2):133–137. doi:10.17925/EE.2021.17.2.133
74. Shoupe D. HRT dosing regimens: continuous versus cyclic-pros and cons. Int J Fertil Womens Med. 2001;46(1):7–15.
75. Stahlberg C, Pedersen AT, Lynge E, et al. Increased risk of breast cancer following different regimens of hormone replacement therapy frequently used in Europe. Int J Cancer. 2004;109(5):721–727. doi:10.1002/ijc.20016
76. Hammar ML, van de Weijer P, Franke HR, et al. Tibolone and low-dose continuous combined hormone treatment: vaginal bleeding pattern, efficacy and tolerability. BJOG. 2007;114(12):1522–1529. doi:10.1111/j.1471-0528.2007.01537.x
77. Archer DF, Hendrix S, Ferenczy A, et al. Tibolone histology of the endometrium and breast endpoints study: design of the trial and endometrial histology at baseline in postmenopausal women. Fertil Steril. 2007;88(4):866–878. doi:10.1016/j.fertnstert.2006.12.052
78. Beral V, Bull D, Reeves G; Million Women Study Collaborators. Endometrial cancer and hormone-replacement therapy in the Million Women Study. Lancet. 2005;365(9470):1543–1551. doi:10.1016/S0140-6736(05)66455-0
79. Formoso G, Perrone E, Maltoni S, et al. Short-term and long-term effects of tibolone in postmenopausal women. Cochrane Database Syst Rev. 2016;10(10):CD008536. doi:10.1002/14651858.CD008536.pub3
80. Cummings SR, Ettinger B, Delmas PD, et al. The effects of tibolone in older postmenopausal women. N Engl J Med. 2008;359(7):697–708. doi:10.1056/NEJMoa0800743
81. Cobin RH, Goodman NF; AACE Reproductive Endocrinology Scientific Committee. American Association of clinical endocrinologists and American College of Endocrinology position statement on menopause-2017 update. Endocr Pract. 2017;23(7):869–880. doi:10.4158/EP171828.PS
82. Stanczyk FZ, Hapgood JP, Winer S, Mishell DR
83. American College of Obstetricians and Gynecologists. Management of menopausal symptoms. Practice Bulletin No. 141. Obstet Gynecol. 2014;123(1):202–216. doi:10.1097/01.AOG.0000441353.20693.78
84. Faubion SS, Kaunitz AM. Stopping systemic menopausal hormone therapy: why, when and how. Maturitas. 2016;89:3–4. doi:10.1016/j.maturitas.2016.03.020
85. Ma J, Drieling R, Stafford RS. US women desire greater professional guidance on hormone and alternative therapies for menopause symptom management. Menopause. 2006;13(3):506–516. doi:10.1097/01.gme.0000179047.00748.53
86. Brisdelle (paroxetine). Prescribing information. US FDA. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/204516s004lbl.pdf.
87. Ivarsson T, Spetz AC, Hammar M. Physical exercise and vasomotor symptoms in postmenopausal women. Maturitas. 1998;29(2):139–146. doi:10.1016/s0378-5122(98)00004-8
88. Hammar M, Berg G, Lindgren R. Does physical exercise influence the frequency of postmenopausal hot flushes? Acta Obstet Gynecol Scand. 1990;69(5):409–412. doi:10.3109/00016349009013303
89. Daley A, Stokes-Lampard H, Thomas A, MacArthur C. Exercise for vasomotor menopausal symptoms. Cochrane Database Syst Rev. 2014;11:CD006108. doi:10.1002/14651858.CD006108.pub4
90. Nonhormonal management of menopause-associated vasomotor symptoms. 2015 position statement of The North American Menopause Society. Menopause. 2015;22(11):1155–1174. doi:10.1097/GME.0000000000000546
91. Thurston RC, Ewing LJ, Low CA, Christie AJ, Levine MD. Behavioral weight loss for the management of menopausal hot flashes: a pilot study. Menopause. 2015;22(1):59–65. doi:10.1097/GME.0000000000000274
92. Koo S, Ahn Y, Lim JY, Cho J, Park HY. Obesity associates with vasomotor symptoms in postmenopause but with physical symptoms in perimenopause: a cross-sectional study. BMC Womens Health. 2017;17(1):126. doi:10.1186/s12905-017-0487-7
93. Reid RL, Magee B, Trueman J, Hahn PM, Pudwell J. Randomized clinical trial of a handheld cooling device (Menopod®) for relief of menopausal vasomotor symptoms. Climacteric. 2015;18(5):743–749. doi:10.3109/13697137.2015.1042856
94. Butler AC, Chapman JE, Forman EM, Beck AT. The empirical status of cognitive-behavioral therapy: a review of meta-analyses. Clin Psychol Rev. 2006;26(1):17–31. doi:10.1016/j.cpr.2005.07.003
95. Ehde DM, Dillworth TM, Turner JA. Cognitive-behavioral therapy for individuals with chronic pain: efficacy, innovations, and directions for research. Am Psychol. 2014;69(2):153–166. doi:10.1037/a0035747
96. Green SM, Donegan E, Frey BN, et al. Cognitive behavior therapy for menopausal symptoms (CBT-Meno): a randomized controlled trial. Menopause. 2019;26(9):972–980. doi:10.1097/GME.0000000000001363
97. Mann E, Smith M, Hellier J, Hunter MS. A randomised controlled trial of a cognitive behavioural intervention for women who have menopausal symptoms following breast cancer treatment (MENOS 1): trial protocol. BMC Cancer. 2011;11:44. doi:10.1186/1471-2407-11-44
98. Ayers B, Smith M, Hellier J, Mann E, Hunter MS. Effectiveness of group and self-help cognitive behavior therapy in reducing problematic menopausal hot flushes and night sweats (MENOS 2): a randomized controlled trial. Menopause. 2012;19(7):749–759. doi:10.1097/gme.0b013e31823fe835
99. Duijts SF, van Beurden M, Oldenburg HS, et al. Efficacy of cognitive behavioral therapy and physical exercise in alleviating treatment-induced menopausal symptoms in patients with breast cancer: results of a randomized, controlled, multicenter trial. J Clin Oncol. 2012;30(33):4124–4133. doi:10.1200/JCO.2012.41.8525
100. Elkins GR, Fisher WI, Johnson AK, Carpenter JS, Keith TZ. Clinical hypnosis in the treatment of postmenopausal hot flashes: a randomized controlled trial. Menopause. 2013;20(3):291–298. doi:10.1097/gme.0b013e31826ce3ed
101. Evia. Take control of menopause, naturally. Available from: https://www.eviamenopause.com/.
102. Woyka J. Consensus statement for non-hormonal-based treatments for menopausal symptoms. Post Reprod Health. 2017;23(2):71–75. doi:10.1177/2053369117711646
103. Orleans RJ, Li L, Kim MJ, et al. FDA approval of paroxetine for menopausal hot flushes. N Engl J Med. 2014;370(19):1777–1779. doi:10.1056/NEJMp1402080
104. David PS, Smith TL, Nordhues HC. Paroxetine (Brisdelle) for hot flashes. Med Lett Drugs Ther. 2013;55(1428):85–86.
105. Capriglione S, Plotti F, Montera R, et al. Role of paroxetine in the management of hot flashes in gynecological cancer survivors: results of the first randomized single-center controlled trial. Gynecol Oncol. 2016;143(3):584–588. doi:10.1016/j.ygyno.2016.10.006
106. Simon JA, Portman DJ, Kaunitz AM, et al. Low-dose paroxetine 7.5 mg for menopausal vasomotor symptoms: two randomized controlled trials. Menopause. 2013;20(10):1027–1035. doi:10.1097/GME.0b013e3182a66aa7
107. Desmarais JE, Looper KJ. Managing menopausal symptoms and depression in tamoxifen users: implications of drug and medicinal interactions. Maturitas. 2010;67(4):296–308. doi:10.1016/j.maturitas.2010.08.005
108. Joffe H, Guthrie KA, LaCroix AZ, et al. Low-dose estradiol and the serotonin-norepinephrine reuptake inhibitor venlafaxine for vasomotor symptoms: a randomized clinical trial. JAMA Intern Med. 2014;174(7):1058–1066. doi:10.1001/jamainternmed.2014.1891
109. Nelson HD, Vesco KK, Haney E, et al. Nonhormonal therapies for menopausal hot flashes: systematic review and meta-analysis. JAMA. 2006;295(17):2057–2071. doi:10.1001/jama.295.17.2057
110. Shams T, Firwana B, Habib F, et al. SSRIs for hot flashes: a systematic review and meta-analysis of randomized trials. J Gen Intern Med. 2014;29(1):204–213. doi:10.1007/s11606-013-2535-9
111. Sun Z, Hao Y, Zhang M. Efficacy and safety of desvenlafaxine treatment for hot flashes associated with menopause: a meta-analysis of randomized controlled trials. Gynecol Obstet Invest. 2013;75(4):255–262. doi:10.1159/000348564
112. Kerwin JP, Gordon PR, Senf JH. The variable response of women with menopausal hot flashes when treated with sertraline. Menopause. 2007;14(5):841–845. doi:10.1097/GME.0b013e31802e7f22
113. Shan D, Zou L, Liu X, Shen Y, Cai Y, Zhang J. Efficacy and safety of gabapentin and pregabalin in patients with vasomotor symptoms: a systematic review and meta-analysis. Am J Obstet Gynecol. 2020;222(6):564–579.e12. doi:10.1016/j.ajog.2019.12.011
114. Guttuso T, Kurlan R, McDermott MP, Kieburtz K. Gabapentin’s effects on hot flashes in postmenopausal women: a randomized controlled trial. Obstet Gynecol. 2003;101(2):337–345. doi:10.1016/s0029-7844(02)02712-6
115. Menopause Subgroup. Chinese society of obstetrics and gynecology, Chinese Medical Association. Zhonghua Fu Chan Ke Za Zhi. 2018;53(11):729–739. doi:10.3760/cma.j.issn.0529-567x.2018.11.001
116. Simon JA, Gaines T, LaGuardia KD; Extended-Release Oxybutynin Therapy for VMS Study Group. Extended-release oxybutynin therapy for vasomotor symptoms in women: a randomized clinical trial. Menopause. 2016;23(11):1214–1221. doi:10.1097/GME.0000000000000773
117. Leon-Ferre RA, Novotny PJ, Wolfe EG, et al. Oxybutynin vs placebo for hot flashes in women with or without breast cancer: a randomized, double-blind clinical trial (ACCRU SC-1603). JNCI Cancer Spectr. 2020;4:pkz088.
118. Katz IR, Sands LP, Bilker W, DiFilippo S, Boyce A, D’Angelo K. Identification of medications that cause cognitive impairment in older people: the case of oxybutynin chloride. J Am Geriatr Soc. 1998;46(1):8–13. doi:10.1111/j.1532-5415.1998.tb01006.x
119. Yang YW, Liu HH, Lin TH, Chuang HY, Hsieh T. Association between different anticholinergic drugs and subsequent dementia risk in patients with diabetes mellitus. PLoS One. 2017;12(4):e0175335. doi:10.1371/journal.pone.0175335
120. Freedman RR, Dinsay R. Clonidine raises the sweating threshold in symptomatic but not in asymptomatic postmenopausal women. Fertil Steril. 2000;74(1):20–23. doi:10.1016/s0015-0282(00)00563-x
121. Goldberg RM, Loprinzi CL, O’Fallon JR, et al. Transdermal clonidine for ameliorating tamoxifen-induced hot flashes. J Clin Oncol. 1994;12(1):155–158. doi:10.1200/JCO.1994.12.1.155
122. Pandya KJ, Raubertas RF, Flynn PJ, et al. Oral clonidine in postmenopausal patients with breast cancer experiencing tamoxifen-induced hot flashes: a University of Rochester Cancer Center Community Clinical Oncology Program study. Ann Intern Med. 2000;132(10):788–793. doi:10.7326/0003-4819-132-10-200005160-00004
123. Walega DR, Rubin LH, Banuvar S, Shulman LP, Maki PM. Effects of stellate ganglion block on vasomotor symptoms: findings from a randomized controlled clinical trial in postmenopausal women. Menopause. 2014;21(8):807–814. doi:10.1097/GME.0000000000000194
124. Lee YS, Wie C, Pew S, Kling JM. Stellate ganglion block as a treatment for vasomotor symptoms: clinical application. Cleve Clin J Med. 2022;89(3):147–153. doi:10.3949/ccjm.89a.21032
125. Lipov E, Lipov S, Stark JT. Stellate ganglion blockade provides relief from menopausal hot flashes: a case report series. J Womens Health. 2005;14(8):737–741. doi:10.1089/jwh.2005.14.737
126. Vincent A, Fitzpatrick LA. Soy isoflavones: are they useful in menopause? Mayo Clin Proc. 2000;75(11):1174–1184. doi:10.4065/75.11.1174
127. Jacobs A, Wegewitz U, Sommerfeld C, Grossklaus R, Lampen A. Efficacy of isoflavones in relieving vasomotor menopausal symptoms - A systematic review. Mol Nutr Food Res. 2009;53(9):1084–1097. doi:10.1002/mnfr.200800552
128. Dodin S, Blanchet C, Marc I, et al. Acupuncture for menopausal hot flushes. Cochrane Database Syst Rev. 2013;2013(7):CD007410. doi:10.1002/14651858.CD007410.pub2
129. Gaspard U, Taziaux M, Mawet M, et al. A multicenter, randomized study to select the minimum effective dose of estetrol (E4) in postmenopausal women (E4Relief): part 1. Vasomotor symptoms and overall safety. Menopause. 2020;27(8):848–857. doi:10.1097/GME.0000000000001561
130. Coelingh Bennink HJ, Verhoeven C, Zimmerman Y, Visser M, Foidart JM, Gemzell-Danielsson K. Clinical effects of the fetal estrogen estetrol in a multiple-rising-dose study in postmenopausal women. Maturitas. 2016;91:93–100. doi:10.1016/j.maturitas.2016.06.017
131. Prague JK, Roberts RE, Comninos AN, et al. Neurokinin 3 receptor antagonism rapidly improves vasomotor symptoms with sustained duration of action. Menopause. 2018;25(8):862–869. doi:10.1097/GME.0000000000001090
132. Santoro N, Waldbaum A, Lederman S, et al. Effect of the neurokinin 3 receptor antagonist fezolinetant on patient-reported outcomes in postmenopausal women with vasomotor symptoms: results of a randomized, placebo-controlled, double-blind, dose-ranging study (VESTA). Menopause. 2020;27(12):1350–1356. doi:10.1097/GME.0000000000001621
133. Fraser GL, Lederman S, Waldbaum A, et al. A phase 2b, randomized, placebo-controlled, double-blind, dose-ranging study of the neurokinin 3 receptor antagonist fezolinetant for vasomotor symptoms associated with menopause. Menopause. 2020;27(4):382–392. doi:10.1097/GME.0000000000001510
134. Trower M, Anderson RA, Ballantyne E, et al. Effects of NT-814, a dual neurokinin 1 and 3 receptor antagonist, on vasomotor symptoms in postmenopausal women: a placebo-controlled, randomized trial. Menopause. 2020;27:498–505.
135. Simon J, Anderson RA, Ballantyne E, et al. OR11-03 NT-814, a non-hormonal dual neurokinin 1,3 receptor antagonist markedly improves vasomotor symptoms in post-menopausal women; results of a randomised, double-blind, placebo- controlled, dose-finding study (SWITCH-1). J Endocr Soc. 2020;4(Suppl.1):OR11–OR103.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.