Back to Journals » Clinical Epidemiology » Volume 11
Vascular Diseases In Patients With Chronic Myeloproliferative Neoplasms – Impact Of Comorbidity
Authors Frederiksen H ![]() , Szépligeti S, Bak M
, Szépligeti S, Bak M ![]() , Ghanima W
, Ghanima W ![]() , Hasselbalch HC, Christiansen CF
, Hasselbalch HC, Christiansen CF ![]()
Received 23 May 2019
Accepted for publication 1 October 2019
Published 1 November 2019 Volume 2019:11 Pages 955—967
DOI https://doi.org/10.2147/CLEP.S216787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Eyal Cohen
Henrik Frederiksen,1–3 Szimonetta Szépligeti,1 Marie Bak,4 Waleed Ghanima,5,6 Hans Carl Hasselbalch,4 Christian Fynbo Christiansen1
1Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark; 2Department of Haematology, Odense University Hospital, Odense, Denmark; 3Department of Clinical Research, University of Southern Denmark, Odense, Denmark; 4Department of Haematology, Zealand University Hospital, Roskilde, Denmark; 5Departments of Oncology, Medicine and Research, Østfold Hospital Trust, Kalnes, Norway; 6Department of Haematology, Institute of Clinical Medicine, University of Oslo, Oslo, Norway
Correspondence: Henrik Frederiksen
Department of Haematology, Odense University Hospital, Kloevervaenget 6, Entrance 93, 12th Floor, Odense C DK-5000, Denmark
Email [email protected]
Background: Patients with chronic myeloproliferative neoplasms (MPNs), including essential thrombocythemia (ET), polycythemia vera (PV), and primary myelofibrosis (PMF), are at high risk of vascular complications. However, the magnitude of this is risk not well known and the possible effect of comorbidity is poorly understood.
Aim: Our aim was to compare the risk of vascular diseases in patients with MPNs and matched comparisons from the general population and to study the effect modification of comorbidity.
Methods: We followed 3087 patients with ET, 6076 with PV, 3719 with PMF or unspecified MPN, and age- and sex-matched general population comparisons to estimate the risks of cardiovascular diseases such as myocardial infarction and stroke. We computed 5-year cumulative incidences (risks) for vascular disease in patients with MPNs and comparisons as well as 1-year and 5-year risks, risk differences, and hazard ratios (HRs) for vascular diseases comparing rates in each group of patients with their comparison cohort by level of comorbidity based on the Charlson Comorbidity Index (CCI) [score of 0 (low comorbidity), of 1–2 (moderate comorbidity), and of >2 (severe comorbidity)], as well as other comorbid conditions.
Results: The overall 5-year risk of vascular disease ranged from 0.5% to 7.7% in patients with MPNs, which was higher than the risk in the general population. In the same period, the adjusted HRs for vascular disease were 1.3 to 3.7 folds higher in patients with MPNs compared to the general population. An increase in CCI score was associated with an equally increased rate of most types of vascular diseases during the first 5 years of follow-up in both MPN and comparisons.
Conclusion: Patients with MPNs have a higher risk of vascular diseases during the first 5 years than that of the general population; however, comorbidity modifies the rates similarly in MPN and in the general population.
Keywords: myeloproliferative neoplasms, thrombosis, comorbidity, stroke, epidemiology
Introduction
Chronic myeloproliferative neoplasms (MPNs), encompassing essential thrombocythemia (ET), polycythemia vera (PV), and primary myelofibrosis (PMF), are hematological cancers characterized by clonal proliferation of one or more myeloid cell lineages in the bone marrow.1
Increased rate of vascular complications among patients with MPNs has been recognized for decades,2 and recommendations for the management of patients are among others based upon the assessment of the risk of vascular complications.3–5 The criteria for high risk in PV include age above 60 and a previous thrombosis.6 Whereas in ET high risks of thrombosis are currently defined as having an IPSET score ≥3 based on previous thrombosis, age above 60, presence of JAK2V617F mutation, and also cardiovascular risk factors such as hypertension, smoking history, etc.6 Although established cardiovascular risk factors (CRFs) like hypertension, hypercholesterolemia, and diabetes occur in 42–46%, 18–21%, and 9% of patients with PV,7,8 they have not been found to impart a consistently increased risk of vascular complications for patients with MPN.8–10 Even with current medical management, survival among patients with MPNs is lower than in the general population7,11 with cardiovascular and cerebrovascular disorders being the leading causes of death in up to 45% of fatalities.12,13 It is therefore recommended that both risk factors for vascular complications associated with MPNs such as elevated hematocrit and leukocyte counts and other potential CRFs are considered in the management of these patients.2,6,8,13–15
Despite that vascular diseases in patients with MPNs have been long recognized, only one study has reported on the magnitude of this rate compared to the rate of vascular disease in the general population,16 and without including prevalent comorbidity or cardiovascular risk factors in analyses.
In this study, we, therefore, examined the risk of vascular disease in patients with ET, PV, MF, and unspecified MPN (MPN-U) compared to the risk in matched comparisons from the general population at different levels of comorbidity.
Materials And Methods
Data Sources
The Civil Registration System (CRS) and the Danish National Patient Registry (DNPR) provided data for this cohort study.17,18 Since 1968, all residents in Denmark have received a unique civil registration number (CRN) from the CRS, allowing unambiguous individual-level linkage between all Danish registries.17 The CRS records the date of birth, sex, date of emigration, date of death, and vital status of all Danish residents (8.3 million during the study period) and it is continuously updated.
The DNPR contains information on all in-patient discharges from Danish public hospitals since 1977 and on outpatient specialist clinic and emergency room visits since 1995.18 Denmark has very few private hospitals and none are engaged in caring for patients with hematological cancer.19 Data recorded in the DNPR include the CRN, dates of outpatient specialist clinic visits, hospital admission and discharge dates, as well as up to 20 diagnoses coded by physicians according to the World Health Organisation’s International Classification of Diseases, Eighth Revision (ICD-8) during 1977–1993 and Tenth Revision (ICD-10), thereafter. The primary diagnosis in the DNPR is the most important condition treated during a given hospital contact and represents the main reason for this contact. Secondary diagnoses include other conditions that the physician considers important to a patient's disease and treatment.18
MPN Cohorts
We identified all patients with a first MPN diagnosis by means of ICD-8 or ICD-10 diagnosis codes recorded in the DNPR between 1 January 1980 and 30 November 2013. Based on the type of MPN diagnosis from 1980 and onwards, we created three cohorts: 1) an ET patient cohort, 2) a PV patient cohort, and 3) an MF/MPN-U patient cohort. The MF and MPN-U diagnoses were combined since patients with primary MF are likely to be assigned an MPN-U diagnosis until the diagnostic work-up is complete. Diagnoses of hematological malignancies in the DNPR have been reported to be valid.20 Patients who were assigned a single MPN diagnosis within the first 30 days after their first MPN diagnosis or patients who were subsequently assigned only an erythrocytosis diagnosis code were not included in the study. The index date was defined by adding 30 days to the first MPN diagnosis, in order to avoid conditioning on future events and also to define co-incident outcomes accurately. All ICD-8 and ICD-10 codes used in this study are presented in the Appendix, Supplementary Table 1.
Matched Population Comparison Cohorts
Using the CRS, each patient with MPN was matched with 10 persons from the general population by sex and year of birth in 1-year intervals. They were assigned an index date identical to their matched patient’s diagnosis date (MPN diagnosis date plus 30 days). Members of the comparison cohorts had to be free of an MPN diagnosis before the index date.21
Vascular Outcomes And Follow-Up
We used the DNPR to identify all defined cardiovascular events in each of the three MPN and comparison cohorts. These included acute myocardial infarction (MI), stroke, peripheral arterial disease in the lower extremities (PAD), venous thromboembolism (VTE) [deep venous thrombosis (DVT) in lower extremities and/or pulmonary embolism], and splanchnic venous thrombosis (SVT). ICD codes for these outcomes are provided in the Appendix, Supplementary Table 1.
Vascular diagnoses have been shown to be valid in the DNPR.22,23 Among stroke diagnoses, the highest validity has been documented for ischemic stroke.22 We therefore also analyzed ischemic stroke as a separate outcome. DVT diagnoses made solely in emergency rooms (ERs) have been suggested to be less reliable.24 For this reason, we excluded any diagnosis made solely in the ER.
We examined multiple vascular diseases with different pathophysiology, and therefore a vascular disease prior to MPN diagnosis or the index date did not lead to study exclusion. Thus, members of the patient and comparison cohorts who had a vascular disease prior to the index date were included in the study for follow-up of new events. However, a vascular disease may lead to a diagnosis of MPN, which could inflate the observed risks of vascular diseases in these patients. We therefore also performed sensitivity analyses restricted to patients and comparisons who had not previously been diagnosed with any vascular disease. Vascular diseases occurring prior to the index date were considered as prevalent or co-incident. In adjusted analyses, such events were included as covariates. Follow-up started at the index date and continued until recording of a defined vascular disease, death, emigration, or 30 November 2013, whichever came first. Patients and comparisons who developed one type of vascular disease continued to be followed up for other types.
Comorbidity
We computed the Charlson Comorbidity Index (CCI) score to study the effect modification of comorbidity on risks of vascular events in patients with MPN and members of the comparison cohort.25 The CCI score is a weighted index, summarizing both the number and seriousness of 19 chronic conditions. When computing CCI scores we excluded conditions in the CCI that were also an outcome of interest in our study. We also excluded the CCI leukemia category because it includes diagnosis codes that may overlap with MPN diagnoses. The CCI includes several vascular diagnoses in its disease categories and CCI calculations in our study therefore varied with the subtype of the vascular disease being examined. Information on CCI conditions was obtained from the DNPR, an approach that has been found to be valid.26 Individual CCI scores were based on diagnoses recorded before the index date and were grouped in three levels: CCI score of 0 (low comorbidity), CCI score of 1–2 (moderate comorbidity), and CCI score of >2 (severe comorbidity). We also used the DNPR to calculate the number of specified CRFs including hospital-based diagnoses of hypertension, obesity, hyperlipidemia, atrial fibrillation, and renal failure (Appendix, Supplementary Table 1).
Sensitivity Analyses
Because blood test results of heavy smokers can resemble those of patients with MPN, diagnostic misclassification could occur if heavy smokers were erroneously given an MPN diagnosis code. Thus, in order to examine the possible effect of diagnostic misclassification of ET, PV, and MF/MPN-U, we stratified analyses according to whether a diagnosis of COPD had been made before or concurrently with the MPN diagnosis (Appendix, Supplementary Table 1). Since we lacked direct information on smoking status, recording of chronic obstructive pulmonary disease (COPD) in the DNPR was used as an indicator of heavy smoking. We used the same approach to define diagnoses associated with alcohol overuse (Appendix, Supplementary Table 1), allowing us to study the effects of these diagnoses on risks of vascular diseases.
Statistical Analysis
We first computed frequency tables including sex, age, year of index date, former vascular episodes, and CCI conditions for patients and comparisons. We then used the cumulative incidence function to depict risks of vascular events treating death as a competing risk.27 We computed the risk during the first year and the following 1–5 years, and 0–5 years with 95% confidence intervals (CIs) per 100 persons for patients with MPN and members of the comparison cohorts, as well as risk differences. Finally, we also computed incidence rates for vascular disease per 1,000 person-years in patients and comparisons.
Cox proportional hazard regression was used to compute hazard ratios (HRs) as a measure of relative risk for vascular events between each of the MPN cohorts and their comparison cohorts. This analysis controlled for the variables age, sex, and diagnosis year by study design, as well as for comorbidity (CCI score, prevalent vascular diagnosis, COPD, and alcohol-related diagnoses), in calculating the overall risk of each of the different vascular events (MI, stroke, PAD, VTE, and SVT). Similarly, Cox regression was used to compare rates between patients and comparisons within each of the three MPN cohorts. The analyses were stratified by CCI score, controlling for the following variables: age, sex, diagnosis year, prevalent vascular diagnosis, COPD, and alcohol-related diagnoses. Using the same approach, we also computed absolute and relative risks controlling for the number of predefined CRFs. Finally, analyses were repeated after excluding patients and matched comparisons who had experienced a vascular event before the index date. The assumption of proportional hazards was assessed graphically and was potentially violated in some subgroup analyses. We, therefore, repeated analyses of HRs for each 1-year period of follow-up to assess the influence of this, and HRs were generally comparable over the time span, although some became imprecise due to low numbers (Appendix, Supplementary Table 7).
Ethics
This study was approved by the Danish Data Protection Agency (record no. 1-16-02-1-08).
Results
Characteristics Of Patients And Comparisons
During a 33-year period (1980–2013), we followed 3,087 patients with ET, 6,076 patients with PV, 3,719 patients with MF/MPN-U, and 30,800, 60,700 and 39,530 age- and sex-matched comparisons, respectively. The 205 ET, 177 PV, and 38 MF/MPN-U patients who died during the first 30 days after their MPN diagnosis were not included in the study. Median follow-up ranged from 2.2 to 5.8 years in the three cohorts, with 0.7–2.4 years in the lower quartile and 5.0–10.5 years in the upper quartile. The median age at diagnosis was 66 years (interquartile range (IQR) 54–76 years) for ET patients, 68 years (IQR 58–76 years) for PV patients, and 72 years (IQR 63–80 years) for patients with MF/MPN-U. In all MPN subtypes, the majority of patients were diagnosed in the most recent study period, due to the later inclusion of diagnoses conferred during outpatient hospital contacts (Table 1).
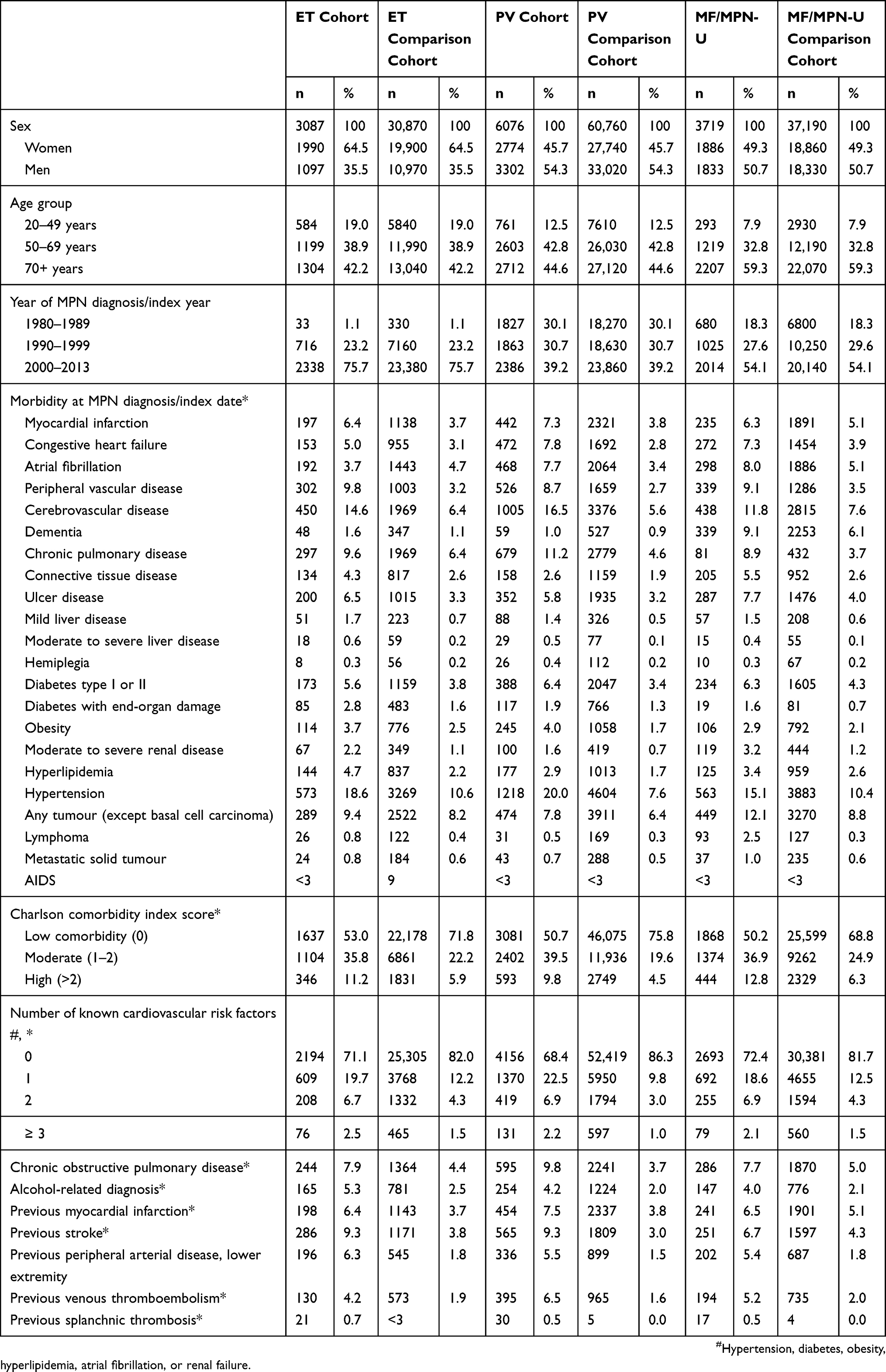 |
Table 1 Characteristics And Comorbidity Of Patients With Essential Thrombocythemia (ET), Polycythemia Vera (PV), And Myelofibrosis/Unclassified Myeloproliferative Neoplasm (MF/MPN-U), And Members Of The Age- And Sex-Matched General Population Comparison Cohort. Figures Are Counts (N) And Proportions In Percent With The Characteristic |
In general, a larger proportion of patients with MPNs had comorbidities and cardiovascular diseases prior to index date than comparisons (Table 1). Accordingly, the proportion of patients with moderate or severe comorbidity or presence of CRFs as of the index date was consistently higher in patients with MPNs, irrespective of subtype, than in matched comparisons (Table 1). For example, 27–33% of patients with MPN had at least one of the defined cardiovascular risk factors compared to 14–18% in comparisons (Table 1).
Risk Of Vascular Diseases
After being diagnosed with MPN, patients with ET or PV generally experienced higher rates of both arterial and venous vascular diseases, than members of the comparison cohorts (Figures 1 and 2). The general risk of vascular disease during the first 5 years ranged from 0.5% to 7.7% in patients with MPN. These 5-year risks were consistently higher among patients with ET or PV than among their comparisons with five-year increases in risk ranging from 0.6% to 4.3% points (Appendix, Supplementary Table 2). In addition, the adjusted HRs for vascular diseases were 1.3 to 3.7 fold elevated during the first 5 years and across the different MPN subtypes and the different vascular diseases – e.g., the adjusted HR for stroke in patients with ET vs comparisons was 1.6 (95% CI 1.4–1.9) (Appendix, Supplementary Table 2). Similar results were seen in patients with MF/MPN-U for VTE and PAD (Figure 3, Appendix Supplementary Table 2). SVT, a rare disease, was mainly observed prior to or within 30 days following an MPN diagnosis (Table 1, Figures 1–3). During 1980–1989, 1990–1999, and 2000–2013 the 5-year risks of vascular disease were much the same although the low number of patients included during 1980–1989 resulted in imprecise risk estimates in this period (Appendix, Supplementary Table 2). The incidence rates of all subtypes of vascular disease were higher in patients with MPN than in members of the comparison cohorts during the first 5 years of follow-up (Supplementary Table 3).
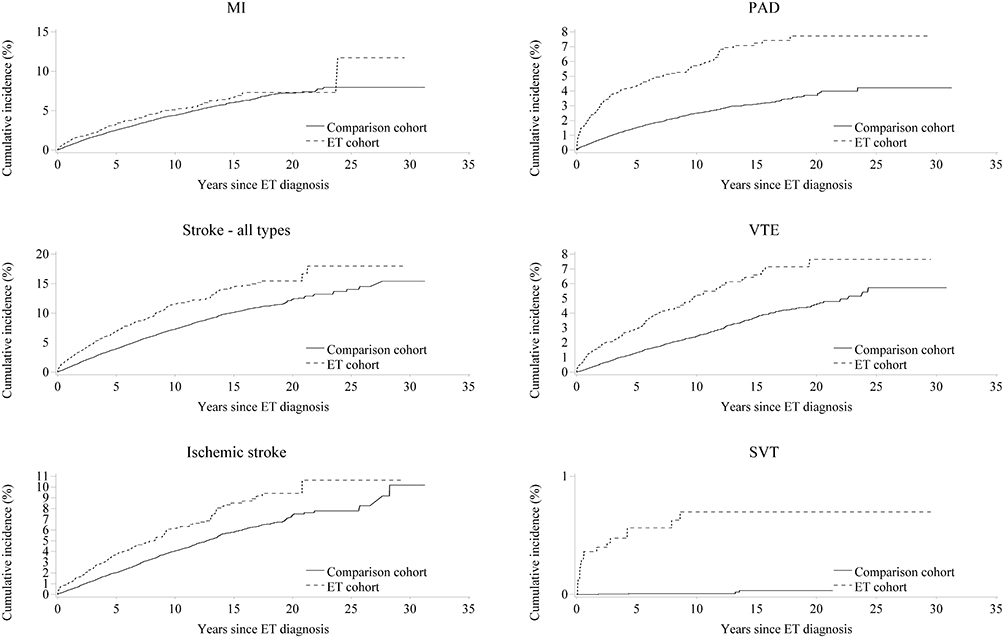 |
Figure 1 Cumulative incidences of vascular events in patients with essential thrombocythemia (ET) and age- and sex-matched members of general population comparison cohorts. Abbreviations: MI, myocardial infarction; PAD, peripheral arterial disease lower extremity; VTE, venous thromboembolism; SVT, splanchnic venous thrombosis. |
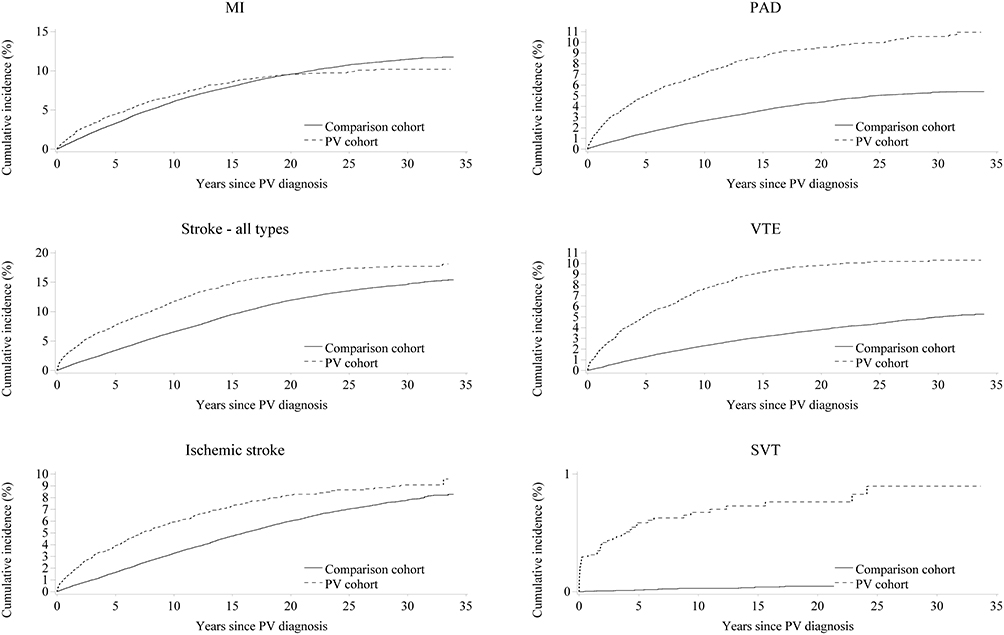 |
Figure 2 Cumulative incidences of vascular events in patients with polycythemia vera (PV) and age- and sex-matched members of general population comparison cohorts. Abbreviations: MI, myocardial infarction; PAD, peripheral arterial disease lower extremity; VTE, venous thromboembolism; SVT, splanchnic venous thrombosis. |
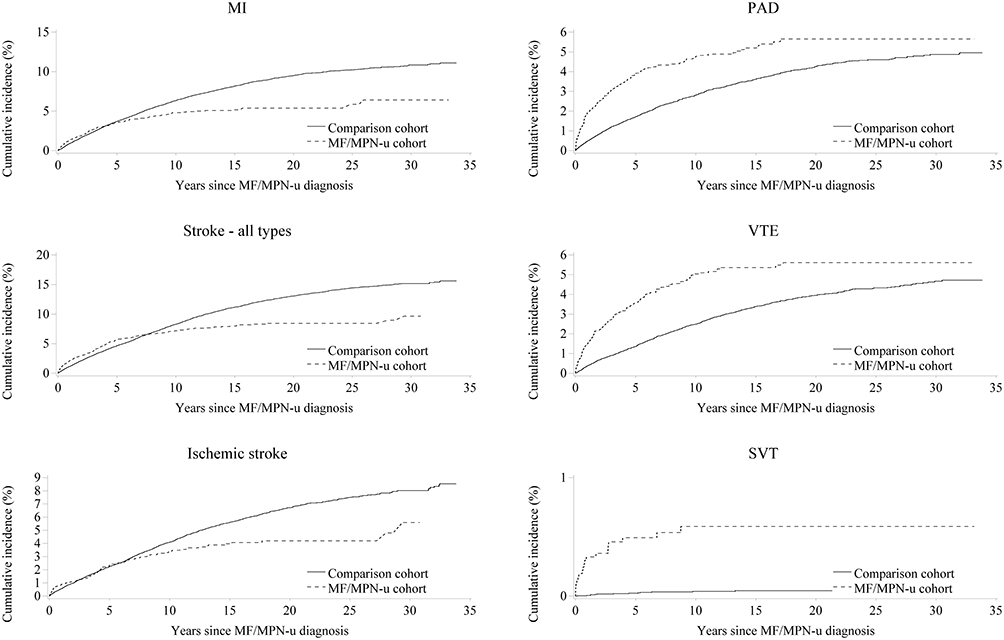 |
Figure 3 Cumulative incidences of vascular events in patients with myelofibrosis or unclassified myeloproliferative neoplasm and age- and sex-matched comparisons from the general population. Abbreviations: MI, myocardial infarction; PAD, peripheral arterial disease lower extremity; VTE, venous thromboembolism; SVT, splanchnic venous thrombosis. |
Tables 2 and 3 show the risks, risk differences, and adjusted HRs by type of vascular disease in patients and comparisons during the first year of follow-up and the next two to 5 years according to the level of comorbidity. An incremental comorbidity score was associated with increased absolute risks of most types of vascular diseases of the same magnitude in both patients with MPN and members of the comparison cohorts (Tables 2 and 3). For MI, stroke, and PAD, a stepwise increased rate of vascular disease was observed by increasing comorbidity level in parallel for both patients with MPN and matched comparisons (Tables 2 and 3). Generally, the increased risk of vascular diseases, from the first year to the following 1–5 years, and the adjusted HRs were similar among patients with MPN and comparisons (Tables 2 and 3) and also between the three MPN subtypes the risks of each type of vascular disease and HRs were generally similar (Appendix, Supplementary Table 2, and Tables 2 and 3).
 |
Table 2 Risk Of Vascular Disease In Percent, Risk Difference And Hazard Ratio (HR) During The First Year Following Diagnosis In Patients With Essential Thrombocythemia (ET), Polycythemia Vera (PV), And Myelofibrosis (MF) Or Unclassified Myeloproliferative Neoplasm (MPN-U), Compared To Members Of Age- And Sex-Matched General Population Comparison Cohorts. The Risks And HRs Are Stratified By Type Of Vascular Event And Level Of Comorbidity Based On Charlson Comorbidity Index (CCI) Scores. The HRs Are Adjusted For Age, Sex, Diagnosis Year, Prevalent Vascular Diagnosis, Chronic Obstructive Pulmonary Disease, And Alcohol-Related Diagnoses |
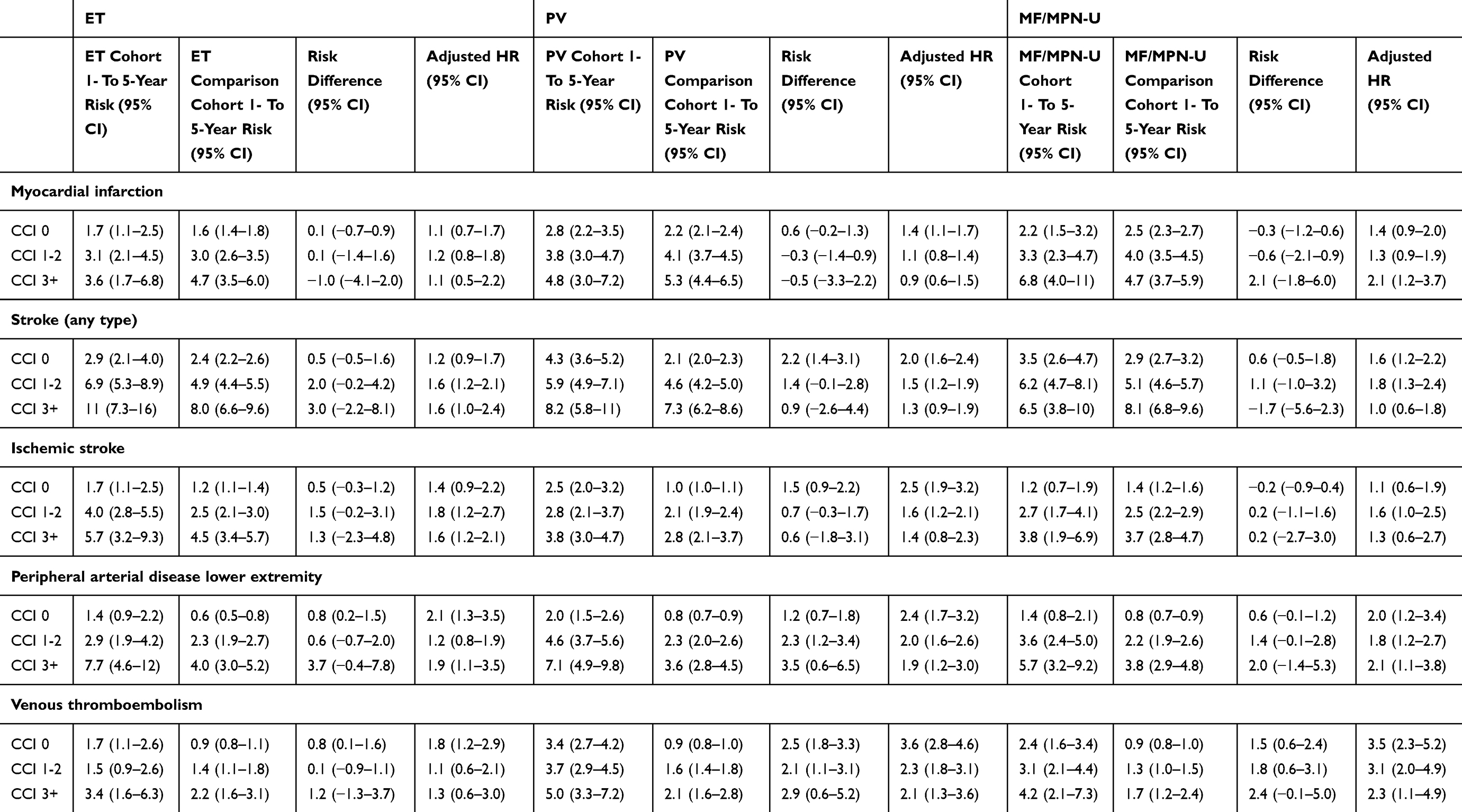 |
Table 3 Risk Of Vascular Event In Percent, Risk Difference And Hazard Ratio (HR) During Years 1–5 Following Diagnosis In Patients With Essential Thrombocythemia (ET), Polycythemia Vera (PV), And Myelofibrosis (MF) Or Unclassified Myeloproliferative Neoplasm (MPN-U), Compared To Members Of Age- And Sex-Matched General Population Comparison Cohorts. The Risks And HRs Are Stratified By Type Of Vascular Event And Level Of Comorbidity Based On Charlson Comorbidity (CCI) Scores. The HRs Are Adjusted For Age, Sex, Diagnosis Year, Prevalent Vascular Diagnosis, Chronic Obstructive Pulmonary Disease, And Alcohol-Related Diagnoses |
Sensitivity Analyses
Five-year cumulative risks for cardiovascular diseases stratified by presence vs absence of a previous COPD diagnosis are presented in Supplementary Table 4. The risks were elevated in all MPN subgroups, with no clear differences attributable to the COPD diagnosis.
In the Supplementary Table 5 risks of vascular diseases are shown by the number of specified CRFs and these results are almost identical to those of the subgroups defined by CCI score. Finally, analyses restricted to patients and comparisons without a previous vascular diagnosis lowered the 5-year risks among patients, leading to lower risk differences between patients with MPN and their matched comparisons (Supplementary Table 6).
Discussion
Our results showed that 5-year risks of arterial or venous vascular disease ranged from 0.5% to 7.7% for patients with MPN and were elevated compared to the general population with adjusted HRs ranging from 1.3 to 3.7. In most groups, increased comorbidity was associated with a similarly increased risk of vascular disease among patients with MPN and among their comparisons during the first 5 years.
Some features of our study may have affected the observed risks of vascular disease. First, patients with MPN were identified using population-based registries with complete follow-up.10,13 Patients with MPN without a hospital admission could not be identified in DNPR before 1995. Therefore, patients from this period with more severe MPN disease, possibly also with a higher risk of vascular complications, could have been selected disproportionately. We did, however, not detect the effects of this shortcoming since risks of vascular events in patients were much the same across different time periods. In the MF/MPN-U subtype, some of the cumulative incidence curves cross after 5–15 years of follow-up (Figure 3); this probably reflects a survivorship bias, i.e., that in this group with high early mortality the patients who remain alive at a given time are selected for good health.28
Patients with MPN were identified using ICD diagnosis codes which could have led to diagnostic misclassification, for instance, if patients with secondary polycythemia were erroneously given a PV diagnosis code. Although we cannot rule out that this constraint influenced our results, our stratified analyses indicated that risks of vascular events were nearly the same for patients with and without COPD. As well, in a previous study with almost identically defined patients, we demonstrated that ET and PV patients had the expected later occurrence of hematological transformation.29
Another concern is that we defined the MPN subtype based on the first MPN diagnosis code. It is well known that the specific MPN subtype may not always be determined during a first hospital visit, and that patients with MPNs may later be assigned a different MPN subtype due to progression or emergence of new clinical or para-clinical results. Our definition probably explains the relatively high proportion of patients with the MPN-U subtype. The capture of the rare patients with primary MF was probably in particular affected by the MPN subtype definition, and our results from our aggregated MF/MPN-U group may not reflect vascular risks in patients with primary MF accurately.
Our registry-based data did not include detailed information on patient-specific characteristics such as blood pressure, smoking habits, body mass index, or molecular or treatment-specific factors that would have allowed us to investigate other factors that could influence thrombosis risk among patients with MPNs. As well, our CCI calculation was based on diagnoses made in outpatient specialist clinics and during hospital admissions. This approach may not capture all comorbid diagnoses, such as type 2 diabetes, hypertension, or dementia followed in general practice without a hospital referral. However, these limitations affect both patients and members of the comparison cohorts. Our primary goal was to assess the risk of vascular disease conveyed through comorbid conditions that to some extent represent “end-stage” conditions associated with some of the unknown risk factors for vascular disease in the causal pathway. We also cannot rule out that patients with MPNs were more likely to have comorbid diagnoses registered during their hospital stay compared with members of the general population cohort. This could have given a conservative bias to our estimates of the effects of comorbidity on the risk of vascular disease. Similarly, we include only patients who have an inpatient recording of a vascular disease. Due to advances in diagnosis and treatment of DVT, this is now often managed in the out-patient setting. Therefore, our absolute risk estimates for DVT may be conservative – particularly in more recent time periods.
At index date, the proportion of patients with cardiovascular morbidity was highest in patients with MPN. This was observed both for cardiovascular diagnoses such as stroke, myocardial infarction, and peripheral vascular disease and for other risk factors such as obesity, hypertension, etc. This skewed distribution of underlying risk factors was controlled in the multivariate analysis but unmeasured and residual confounding from unmeasured and incompletely measured risk factors may still influence our results. When we exclude patients with prevalent vascular diseases the risk differences became smaller; however, the HRs for patients vs comparisons were much the same, emphasizing that the MPN is a risk factor in itself.
Although vascular complications of MPNs have long been recognized, it was not until recently that a study found that patients with MPNs identified in the Swedish Cancer Register had a 3-month HR for arterial thrombosis that was 3-fold elevated and 9-fold elevated for venous thrombosis among patients with MPNs compared to age- and sex-matched comparisons from the general population.16 The magnitude of this relative increase was comparable across MPN subtypes for arterial events. In contrast, patients with PV exhibited a higher rate of venous thromboembolic events compared to patients with other MPNs.16 Throughout the study period, HRs for both arterial and venous thromboses remained elevated. In line with these results, 16 we found that HRs were somewhat lower but still elevated for all types of vascular diseases.
Thrombotic risks, thrombotic deaths, or major thrombotic events have previously been reported to occur among 2.8% to 9.8% of 365 patients with PV after a median follow-up of 31 months.30 In another study, the incidence of both fatal and nonfatal thrombotic events was 1.9/100 person-years among 891 patients with ET followed for a median of 6.2 years.10 In the latter study, the incidence of nonfatal arterial thrombotic events was 1.2/100 person-years and that of venous events was 0.6/100 person-years. More specifically, the incidence of MI was 0.3/100 person-years and 0.7/100 person-years for stroke.10 In the ECLAP trial, a cohort of 1,638 patients who had been diagnosed with PV within the previous 0–2 years (35.5%) or earlier was followed from inclusion at 94 hematological centers across 12 countries.13 In this study, the incidence of fatal and nonfatal thrombosis after study inclusion was 5.5/100 person-years, the incidence of MI and stroke was 0.3/100 and1.4/100 per person-years, respectively.13 Our incidence rates of MI and stroke were somewhat higher than these previous studies possibly reflecting both the complete follow-up in our cohort and inclusion of patients from the time of MPN diagnosis. In a previous study, some patients have already received treatment for MPN before inclusion.13 The proportion of patients in our study who suffered an SVT before or after MPN diagnosis was approximately 0.5–1%. This proportion is considerably lower than another observational study from the Mayo clinic were 53/587 (9.4%) of patients with PV suffered this rare complication.8 The discrepancy probably reflects that the risk profile in patients from tertiary referral centers may not be comparable to the general MPN patients.
Pathophysiology of vascular complications in patients with MPN is complex involving multiple factors such as inflammation, age, high blood counts, cardiovascular risk factors, but also MPN driver mutations may directly or indirectly increase risks.13,30–32 Recently, a study among 20,000 general population adults revealed that a JAK2V617F or a CALR mutation was identified in 3.1%.33 These persons were more likely to be smokers, to have prior thrombosis, and had higher blood counts than population. The study emphasizes that pre-diagnostic phase in MPN may be long, and that some of the pre-MPN vascular events may be preventable through screening and management of shared risk factors.33
Conclusion
We conclude that vascular diseases and cardiovascular risk factors are more prevalent in patients with MPNs, compared to the general population, and that patients have an 1.3 to 3.7 times increased rate of a new arterial and venous vascular diseases, depending on MPN subtype, and type of vascular disease. The rate seems to be modified to the same extent by comorbidity in patients with MPNs as in the general population.
Acknowledgements
We thank Professor Henrik Toft Sørensen for dedicated help, inspiring comments, and interpretation of results for this study. This work was supported by the Program for Clinical Research Infrastructure (PROCRIN) established by the Lundbeck Foundation and the Novo Nordisk Foundation and administered by the Danish Regions.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Professor Waleed Ghanima reports grants, personal fees from Novartis, personal fees from Amgen, grants, personal fees from Bayer, and grants from Pfizer, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. SH S, Campo E, NL H, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues.
2. Barbui T, Carobbio A, Rumi E, et al. In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology. Blood. 2014;124(19):3021–3023. doi:10.1182/blood-2014-07-591610
3. McMullin MF, Wilkins BS, Harrison CN. Management of polycythaemia vera: a critical review of current data. Br J Haematol. 2016;172(3):337–349. doi:10.1111/bjh.13812
4. Harrison CN, Garcia NC. Management of MPN beyond JAK2. Hematology Am Soc Hematol Educ Program. 2014;2014(1):348–354. doi:10.1182/asheducation-2014.1.348
5. Tefferi A, Barbui T. Polycythemia vera and essential thrombocythemia: 2015 update on diagnosis, risk-stratification and management. Am J Hematol. 2015;90(2):162–173. doi:10.1002/ajh.23895
6. Barbuil T, Tefferi A, Vannucchi AM, et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia. 2018;32(5):1057–1069. doi:10.1038/s41375-018-0077-1
7. Tefferi A, Rumi E, Finazzi G, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia. 2013;27(9):1874–1881. doi:10.1038/leu.2013.163
8. Cerquozzi S, Barraco D, Lasho T, et al. Risk factors for arterial versus venous thrombosis in polycythemia vera: a single center experience in 587 patients. Blood Cancer J. 2017;7:662
9. Landolfi R, Di Gennaro L, Barbui T, et al. Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera. Blood. 2007;109(6):2446–2452. doi:10.1182/blood-2006-08-042515
10. Carobbio A, Thiele J, Passamonti F, et al. Risk factors for arterial and venous thrombosis in WHO-defined essential thrombocythemia: an international study of 891 patients. Blood. 2011;117(22):5857–5859. doi:10.1182/blood-2011-02-339002
11. Tefferi A, Guglielmelli P, Larson DR, et al. Long-term survival and blast transformation in molecularly annotated essential thrombocythemia, polycythemia vera, and myelofibrosis. Blood. 2014;124(16):2507–2513. doi:10.1182/blood-2014-05-579136
12. Hultcrantz M, Wilkes SR, Kristinsson SY, et al. Risk and cause of death in patients diagnosed with myeloproliferative neoplasms in Sweden between 1973 and 2005: a population-based study. J Clin Oncol. 2015;33(20):2288–2295. doi:10.1200/JCO.2014.57.6652
13. Marchioli R, Finazzi G, Landolfi R, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol. 2005;23(10):2224–2232. doi:10.1200/JCO.2005.07.062
14. Landolfi R, Cipriani MC, Novarese L. Thrombosis and bleeding in polycythemia vera and essential thrombocythemia: pathogenetic mechanisms and prevention. Best Pract Res Clin Haematol. 2006;19(3):617–633. doi:10.1016/j.beha.2005.07.011
15. Barbui T, Barosi G, Birgegard G, et al. Philadelphia-negative classical myeloproliferative neoplasms: critical concepts and management recommendations from european leukemianet. J Clin Oncol. 2011;29(6):761–770. doi:10.1200/JCO.2010.31.8436
16. Hultcrantz M, Bjorkholm M, Dickman PW, et al. Risk for arterial and venous thrombosis in patients with myeloproliferative neoplasms: a population-based cohort study. Ann Intern Med. 2018;168(5):317–325.
17. Schmidt M, Pedersen L, Sorensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
18. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
19. Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/CLEP.S179083
20. Norgaard M, Skriver MV, Gregersen H, Pedersen G, Schonheyder HC, Sorensen HT. The data quality of haematological malignancy ICD-10 diagnoses in a population-based hospital discharge registry. Eur J Cancer Prev. 2005;14(3):201–206. doi:10.1097/00008469-200506000-00002
21. Heide-Jorgensen U, Adelborg K, Kahlert J, Sorensen HT, Pedersen L. Sampling strategies for selecting general population comparison cohorts. Clin Epidemiol. 2018;10:1325–1337. doi:10.2147/CLEP
22. Luhdorf P, Overvad K, Schmidt EB, Johnsen SP, Bach FW. Predictive value of stroke discharge diagnoses in the Danish National Patient Register. Scand J Public Health. 2017;45(6):630–636. doi:10.1177/1403494817716582
23. Sundboll J, Adelborg K, Munch T, et al. Positive predictive value of cardiovascular diagnoses in the Danish National Patient Registry: a validation study. BMJ Open. 2016;6(11):e012832. doi:10.1136/bmjopen-2016-012832
24. Severinsen MT, Kristensen SR, Overvad K, Dethlefsen C, Tjonneland A, Johnsen SP. Venous thromboembolism discharge diagnoses in the Danish National Patient Registry should be used with caution. J Clin Epidemiol. 2010;63(2):223–228. doi:10.1016/j.jclinepi.2009.03.018
25. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
26. Thygesen SK, Christiansen CF, Christensen S, Lash TL, Sorensen HT. The predictive value of ICD-10 diagnostic coding used to assess Charlson comorbidity index conditions in the population-based Danish National Registry of Patients. BMC Med Res Methodol. 2011;11:83. doi:10.1186/1471-2288-11-83
27. Belot A, Remontet L, Launoy G, Jooste V, Giorgi R. Competing risk models to estimate the excess mortality and the first recurrent-event hazards. BMC Med Res Methodol. 2011;11:78. doi:10.1186/1471-2288-11-78
28. Hernan MA. The hazards of hazard ratios. Epidemiology. 2010;21(1):13–15. doi:10.1097/EDE.0b013e3181c1ea43
29. Frederiksen H, Farkas DK, Christiansen CF, Hasselbalch HC, Sorensen HT. Chronic myeloproliferative neoplasms and subsequent cancer risk: a Danish population-based cohort study. Blood. 2011;118(25):6515–6520. doi:10.1182/blood-2011-04-348755
30. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22–33. doi:10.1056/NEJMoa1208500
31. Barbui T, Carobbio A, Finazzi G, et al. Elevated C-reactive protein is associated with shortened leukemia-free survival in patients with myelofibrosis. Leukemia. 2013;27(10):2084–2086. doi:10.1038/leu.2013.207
32. Barbui T, Carobbio A, Finazzi G, et al. Inflammation and thrombosis in essential thrombocythemia and polycythemia vera: different role of C-reactive protein and pentraxin 3. Haematologica. 2011;96(2):315–318. doi:10.3324/haematol.2010.031070
33. Cordua S, Kjaer L, Skov V, Pallisgaard N, Hasselbalch HC, Ellervik C. Prevalence and phenotypes of JAK2 V617F and calreticulin mutations in a Danish general population. Blood. 2019;134(5):469–479. doi:10.1182/blood.2019001113
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.