Back to Journals » International Journal of General Medicine » Volume 18
Variations in Poisoning Epidemiology and Management During the Initial COVID-19 Outbreak in a Taiwanese Emergency Department
Authors Chen LC, Mao CY, Cheong CW, Chen WC, Yen TH ![]() , Chen HY
, Chen HY
Received 14 February 2025
Accepted for publication 30 May 2025
Published 14 June 2025 Volume 2025:18 Pages 3175—3183
DOI https://doi.org/10.2147/IJGM.S520738
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Satish Nair
Lu-Chen Chen,1 Chih-Yang Mao,1 Chan-Wa Cheong,1 Wei-Chen Chen,1 Tzung-Hai Yen,2,3 Hsien-Yi Chen1,3
1Department of Emergency Medicine, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan (R.O.C.); 2Department of Nephrology and Clinical Poison Center, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan; 3College of Medicine, Chang Gung University, Taoyuan, Taiwan (R.O.C.)
Correspondence: Hsien-Yi Chen, Department of Emergency Medicine, Linkou Chang Gung Memorial Hospital, No. 5, Fuxing St., Guishan Dist, Taoyuan, 333, Taiwan (R.O.C.), Tel +886-3-3281200ext.2140, Fax +886-3-3287715, Email [email protected]
Purpose: The COVID-19 pandemic significantly impacted the epidemiology of emergency department (ED) presentations, including those for self-harm and poisoning. Taiwan, with its strict border controls and quarantine measures, experienced a delayed COVID-19 outbreak in late April 2022. We evaluated epidemiological changes in ED poisoning cases and assessed whether their management was affected during the early stages of the COVID-19 outbreak.
Patients and Methods: We conducted a retrospective cohort study of ED poisoning cases during the early phase of the COVID-19 outbreak (May 1–July 31, 2022) and the corresponding pre-COVID-19 periods (May 1–July 31, 2018, and 2019) at a tertiary medical center. Demographic data, poisoning characteristics, treatment efficiency, and clinical outcomes were compared between the two periods.
Results: In total, 145 poisoning cases (48.3 per month) were identified during the pandemic, compared to 572 (95.3 per month) in the pre-pandemic period. Poisoned patients were significantly older (median age: 48 vs 40.5 years, p = 0.009) during the pandemic compared to the pre-pandemic periods, with a significant decline in pediatric poisoning cases. Although an increase in prescription drug exposures and a slight decrease in other poisoning categories was observed, these differences were not statistically significant. The proportion of severe poisoning cases (poisoning severity score 3 or 4) was significantly higher during the pandemic than in the pre-pandemic period (14.5% vs 7.9%, p = 0.021), and was accompanied by increased rates of intubation and intensive care unit admissions. ED stays were significantly prolonged during the pandemic, particularly among patients at risk of concurrent COVID-19 infection. Mortality rates remained comparable between the two periods.
Conclusion: The epidemiology, disease severity, and management efficiency of poisoning cases were significantly affected during the early phase of the nationwide COVID-19 outbreak. Further large-scale studies are needed to validate these findings and inform future interventions.
Keywords: SARS-CoV-2, COVID-19 pandemic, intoxication, overdose
Introduction
The COVID-19 pandemic, caused by the novel coronavirus SARS-CoV-2, had a profound global impact, significantly altering human lifestyles and healthcare dynamics. This pandemic influenced the epidemiology of patients presenting to emergency departments (EDs) with injuries, self-harm, or poisoning.1–3 Furthermore, delayed patient presentation and the overwhelming strain on healthcare systems during this period significantly impacted the management of non-COVID-19 conditions.4–6
Social changes induced by the COVID-19 pandemic may have influenced the characteristics of poisoning cases; lockdown measures may have delayed hospital arrivals, exacerbating poisoning severity and increasing mortality rates.3,7 In North America, overdose deaths escalated during the early phase of the pandemic, primarily driven by fentanyl- or stimulant-related fatalities.8–11 Furthermore, poison-control centers experienced an increase in unintentional exposures to household disinfectants and hand sanitizers, particularly among young children.12–18 In Iran, a severe outbreak of methanol poisoning, stemming from the misuse of disinfectants during the early stages of the pandemic, led to a significant increase in poisoning-related deaths.19,20 In Taiwan, a previous study reported a decline in cases of animal envenomation and plant poisoning during the COVID-19 pandemic, accompanied by an increase in suicidal drug overdoses.21
Taiwan successfully mitigated the initial waves of COVID-19 through stringent border controls and quarantine measures. The first outbreak occurred in northern Taiwan in May 2021, with lockdown measures from May 15 to July 27 effectively curbing the spread. However, the emergence of the highly contagious Omicron variant in late April 2022 triggered a nationwide outbreak.22 Most EDs established outdoor treatment zones to accommodate patients considered at risk of having COVID-19 temporarily, such as those with fever, flu-like symptoms, or recent exposure. Health authorities mandated COVID-19 nucleic acid testing for all hospitalized patients, prolonging ED stays and delaying treatment procedures. In addition, the establishment of specialized COVID-19 wards significantly reduced the capacity to admit patients with other medical conditions. The rapid escalation of the pandemic placed significant strain on the healthcare system. Several studies in Taiwan have emphasized disruptions in the management of non-COVID conditions during the pandemic, including acute myocardial infarction and trauma.23,24 It is likely that the care of poisoned patients was similarly affected, particularly during the early phase of the outbreak.
Limited studies have evaluated the changes in the epidemiology and outcomes of poisoning cases during the COVID-19 pandemic in Taiwan. To our knowledge, no prior study has investigated whether management of poisoning was affected during this period. We evaluated epidemiological shifts in ED poisoning cases during the early stages of the nationwide COVID-19 outbreak and evaluated differences in poisoning management and its efficiency compared to the pre-pandemic period.
Materials and Methods
Settings and Patient Selection
We conducted a retrospective cohort study in the ED of Linkou Chang Gung Memorial Hospital, a tertiary medical center with approximately 180,000 annual ED visits. We included poisoning cases from the early phase of the COVID-19 outbreak, defined as the 3-month period from May 1 to July 31, 2022, and a pre-COVID control period covering the corresponding months in 2018 and 2019. The sources of patient referrals, paramedic transfer protocols for specific medical conditions, and hospital admission criteria remained unchanged before and during the COVID-19 pandemic. Potential participants were identified through the electronic medical record system using the International Classification of Diseases, 10th Revision codes related to poisoning (F19, T36–T65). All potential participants were systematically reviewed, and those who did not meet the criteria for poisoning were excluded. Poisoning was defined as the development of any physical or psychological symptoms following exposure to a substance, including drugs, chemicals, animal venoms, or biotoxins. Asymptomatic patients with a clearly documented exposure history of exposure were also included. Patients were excluded if they presented to the ED with any of the following conditions: foreign-body ingestion, simple alcohol intoxication or uncomplicated alcohol withdrawal, food poisoning not involving a specific toxin, anaphylactic reactions, isolated ocular chemical exposure, or common side effects of prescription drugs.
Data Collection and Study Protocol
We collected data on patient demographics (age and sex), exposure routes, time from exposure to ED arrival, initial vital signs, Glasgow Coma Scale (GCS) scores, substances involved in poisoning, and poisoning-related treatments such as gastric lavage, activated charcoal, whole bowel irrigation, hemodialysis or hemoperfusion (HD/HP), and endotracheal intubation. In addition, to evaluate the efficiency of poisoning management, we recorded treatment delays in mechanical ventilation and HD/HP (defined as the time between order submission and treatment initiation) and the durations of ED stays. Poisoning severity scores (PSS),25 ED flow metrics, and outcomes were also recorded.
We compared patient characteristics, treatment delays, ED stay durations, and clinical outcomes between cases of poisoning during the COVID-19 pandemic and in the pre-COVID period. Furthermore, during the early phase of the pandemic, ED patients with potential COVID-19 infection risks were initially managed in an outdoor treatment zone if they exhibited fever or flu-like symptoms, had a suspected or confirmed COVID-19 infection, or had a history of contact with a COVID-19 case or exposure to a cluster. Poisoned patients treated in the outdoor zone were classified as the “COVID-19 risk group”, whereas others were categorized as the “Non-COVID-19 risk group”. Due to limited resources and the need for enhanced personal protective equipment in the outdoor zone, the “COVID-19 risk group” was more likely to experience procedural delays and longer ED stays. We compared key parameters between these groups during the pandemic phase.
Statistical Analysis
Statistical analyses were performed using SAS software (version 9.4; SAS Institute, Cary, NC, USA). The normality of continuous variables was assessed using the Kolmogorov–Smirnov test. Depending on the distribution, either the Mann–Whitney U-test or t-tests were applied to analyze continuous variables. Categorical variables were analyzed using the chi-square or Fisher’s exact test when any expected count of the binary variables was less than 5. P-values < 0.05 were considered statistically significant.
Results
During the early phase of the COVID-19 outbreak (May 1–July 31, 2022), 38,598 patients presented to the ED. Of these, 145 cases (0.38%, 48.3 per month) were identified as poisoning incidents. In the pre-COVID period (May 1–July 31, 2018 and 2019), 87,948 ED visits were recorded, with 572 poisoning cases (0.65%, 95.3 per month). Significant reductions in ED visits and poisoning cases were observed during the pandemic. Table 1 presents the baseline demographics, clinical characteristics, outcomes, and a comparative analysis between the two periods.
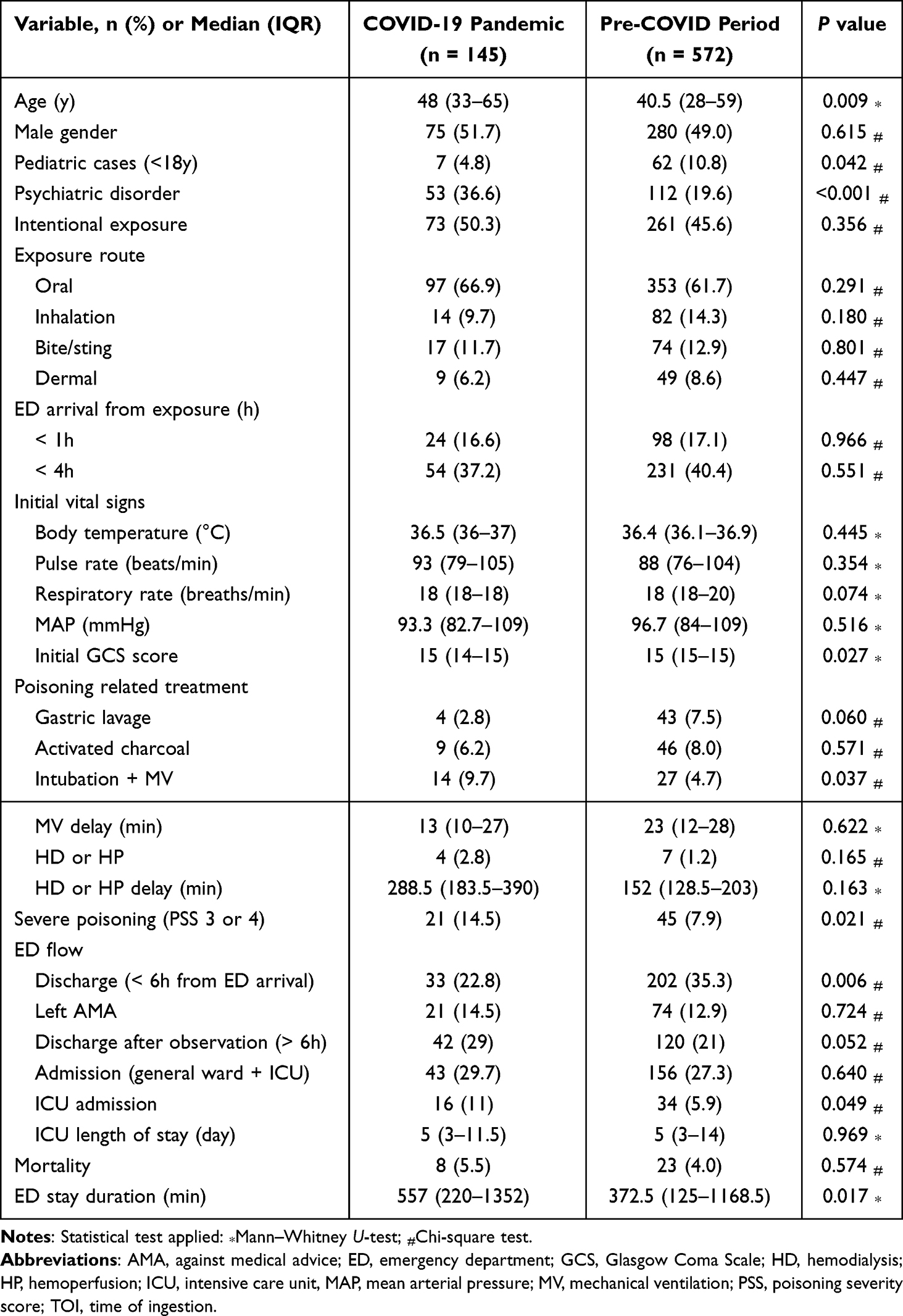 |
Table 1 Demographic Data, Treatment Delays, Clinical Outcomes, and Emergency Department Stay Durations of Poisoning Cases During the Pandemic Compared to the Pre-Pandemic Period |
Demographic Data
The median age of patients was significantly higher during the pandemic (48 years, interquartile range [IQR] 33–65) compared to the pre-pandemic period (40.5 years, IQR 28–59; p = 0.009). A significant decline in pediatric poisoning cases was observed during the pandemic (4.8% vs 10.8%; p = 0.042). A significantly higher proportion of poisoned patients during the pandemic had psychiatric disorders (36.6% vs 19.6%; p < 0.001). No significant differences were observed in sex, intent of poisoning, exposure routes, or early ED presentations (ED arrival < 1 h or < 4 h after exposure). Figure 1 illustrates the categories of exposure during the study period. Although an increase in prescription drug exposures and a slight decrease in other categories, including household cleaner poisonings, were observed during the pandemic, these differences were not statistically significant. The frequencies and comparative analysis of common prescription drug exposures between the two periods are presented in the Supplemental Table.
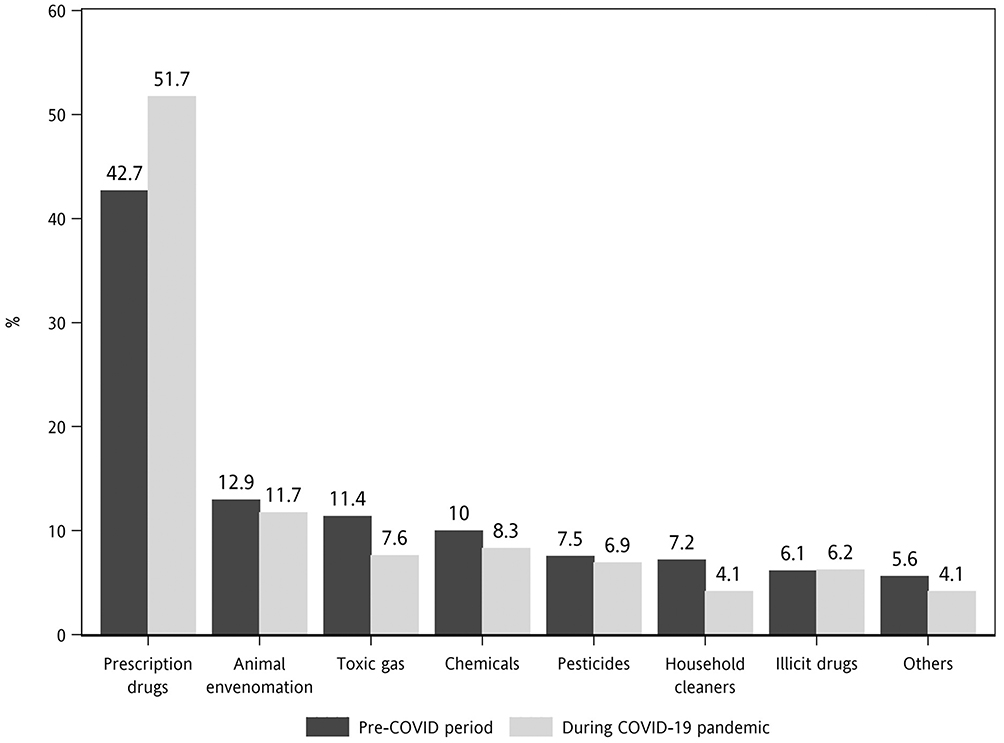 |
Figure 1 Comparison of poisoning categories and their frequencies between the COVID-19 pandemic and the pre-COVID-19 period. |
Poisoning Severity, Outcomes and Management Efficiency
Patients poisoned during the pandemic exhibited increased poisoning severity, indicated by lower GCS scores, higher intubation rates (9.7% vs 4.7%; p = 0.037), a greater proportion of severe poisonings (PSS 3 or 4; 14.5% vs 7.9%; p = 0.021), and higher ICU admission rates (11% vs 5.9%; p = 0.049) compared to the pre-pandemic period. Mortality rates were comparable between the two periods. Although treatment delays for mechanical ventilation and HD/HP were comparable, the duration of ED stay were significantly longer for poisoned patients during the pandemic (Table 1).
Comparisons Between the COVID-19 Risk Group and the Non-COVID-19 Risk Group
Of the 145 poisoned patients during the pandemic, 10 were classified into the COVID-19 risk group. This group experienced significantly longer ED stays, and higher rates of severe poisoning (40% vs 12.6%; p = 0.039) and mortality (30% vs 3.7%; p = 0.011), compared to the Non-COVID-19 risk group (Table 2). All intubations and deaths in the COVID-19 risk group were attributable to poisoning rather than to COVID-19 infection.
 |
Table 2 Comparison Between Poisoned Patients with and Without Concurrent COVID-19 Infection Risks During the Pandemic |
Discussion
Our study provides insights into the changes in epidemiology, disease severity, management efficiency, and clinical outcomes of poisoning cases that presented to EDs in Taiwan during the early phase of the COVID-19 outbreak. We observed a significant decline in poisoning cases during the pandemic. In addition, the median age of poisoned patients was higher compared to the pre-pandemic period, largely attributable to a decline in pediatric patients. Although the proportion of severe poisonings (PSS 3 or 4) was higher during the pandemic, the mortality rates remained comparable. The efficiency of poisoning management was affected during the pandemic, as evidenced by longer ED stays, particularly among patients at risk for COVID-19 infection.
We observed significant reductions in the numbers of ED visits and poisoning cases during the pandemic, consistent with global trends.26–28 However, delayed ED presentation among poisoned patients, reported in several previous studies, was not observed in our cohort.3,7 These reductions may reflect patients’ reluctance to visit EDs due to concerns about contracting COVID-19 in crowded healthcare settings. However, such reluctance raises concerns about the potential negative impact of delayed or missed care. Similarly, some poison-control centers reported a decrease in consultation calls from hospitals during the early stages of the pandemic.15,18 Health authorities should emphasize the importance of seeking timely medical attention for poisoning cases with warning symptoms. In addition, enhancing the visibility and accessibility of poison-control centers can facilitate prompt public consultation and help reduce unnecessary ED visits.29
A significant demographic shift during the pandemic was the older age of poisoned patients compared to the pre-pandemic period, accompanied by a significant decline in pediatric cases; this trend aligns with a more pronounced reduction in pediatric ED visits compared to adults.26 Previous studies have demonstrated that most pediatric poisonings are unintentional and typically result in minor toxicities.30 Parental concerns regarding COVID-19 exposure during the pandemic led to a reduction in ED visits for children with minor or asymptomatic conditions; this may have resulted in a shift toward seeking guidance from poison-control centers. Several studies have demonstrated an increase in public consultation calls during the COVID-19 lockdown period.12,15,18 In contrast, older adults demonstrated a higher propensity for ED visits during the pandemic, likely attributable to the higher rates of intentional poisonings and greater vulnerability to overdoses or poisonings.
We observed a higher proportion of prescription drug exposures during the pandemic (51.7%) compared to the non-pandemic period (42.7%), reflecting changes in the availability of substances or toxins. In addition, a higher proportion of poisoned patients had a history of psychiatric disorders during the pandemic, although the overall rate of intentional poisonings, potentially influenced by multiple factors, did not differ significantly between the two periods. Pandemic-related stressors, such as fear, self-isolation, physical distancing, and financial hardship, may have had a negative impact on the population’s mental health, leading to increased demand for psychotropic drugs.31 This, in turn, may have contributed to the increased frequency of exposure or overdose involving these drugs (Supplemental Table). Conversely, the implementation of work-from-home policies and the reduction in industrial activities likely contributed to a decline in occupational chemical exposures. A reduction in cases of animal envenomation during the COVID-19 pandemic, as reported in a previous Taiwanese study, was observed in our cohort, although the difference was not statistically significant.21 A large-scale study with a larger sample size is needed to clarify these findings.
Poisoning cases during the pandemic exhibited a higher rate of severe toxicity (PSS 3 or 4), lower initial GCS scores, and a greater need for intubation compared to the pre-pandemic period. However, the absolute numbers of severely poisoned patients remained comparable between the two periods (7 vs 7.5 cases per month). The increased proportion of severe poisoning cases during the pandemic was likely attributable to the avoidance of ED visits by patients with mild or asymptomatic exposures; this is supported by a significant reduction in the number of patients discharged from the ED within 6 h.
Despite an increase in poisoning severity and prolonged ED stays during the early phase of the COVID-19 pandemic, no significant difference in mortality rates was observed compared to the pre-pandemic period. Prolonged ED stays have been reported to be associated with adverse clinical outcomes, particularly in older and severely ill patients.32 In Taiwan, comprehensive infection control measures, including universal mask-wearing, hand hygiene, border control, digital technology integration, quarantine policies, and restrictions on travel and gatherings, were implemented early during the pandemic.22 These interventions effectively controlled disease transmission and delayed the major outbreak, enabling the healthcare system to prepare and adapt protocols for non-COVID conditions. In addition, a 16–23% decline in ED patient volumes allowed medical staff to focus more on critically ill patients;28 these factors may have contributed to the similar mortality rates observed. However, poisoned patients with concurrent COVID-19 infection risks experienced significantly longer ED stays and higher mortality rates compared to those without such risks. Although limited by a small sample size in the COVID-19 risk group, these findings emphasize the need for developing robust management algorithms for critically poisoned patients with potential or confirmed COVID-19 infection.
Limitations
Our study has several limitations. First, its retrospective design, relatively small sample size, and short study duration may limit the generalizability of the findings. Second, the low numbers of fatalities in both groups limited our ability to evaluate differences in mortality adequately. Third, the identification of poisoning cases and categorization of exposures were primarily based on clinical histories, which are subject to potential inaccuracies. Fourth, treatment delays were assessed using documented times in medical records, which may not accurately reflect real-world scenarios. Finally, as this study was conducted at a tertiary care center, the findings may not be fully representative of the characteristics at other levels of healthcare.
Conclusion
During the early phase of the nationwide COVID-19 outbreak in Taiwan, significant declines in ED visits and poisoning cases were observed. Poisoned patients had a higher median age during the pandemic compared to the pre-pandemic period, largely attributable to a decline in pediatric patients. Although the proportion of severe poisoning cases was higher during the pandemic, the overall mortality rates remained comparable. However, the efficiency of poisoning management was affected, as manifested by prolonged ED stays, particularly among poisoned patients at risk for COVID-19 infection. This study offers valuable insights for optimizing poisoning management protocols and policies in future public-health emergencies. To confirm and expand these findings, further large-scale studies involving additional healthcare facilities and larger sample sizes are warranted.
Data Sharing Statement
The datasets supporting the results reported in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Chang Gung Medical Foundation (IRB No. 202300660B0). The requirement for informed consent was waived due to the retrospective design of the study, which involved data collection from patients’ medical records. All patient data were de-identified prior to analysis to ensure confidentiality and privacy in accordance with applicable ethical and data protection guidelines.
Acknowledgments
The authors thank Prof. Chung-Hsien Chaou (College of Medicine, Chang Gung University, Taoyuan, Taiwan) for providing statistical consultation.
Funding
This study was supported by research grants from Chang-Gung Memorial Hospital (grant number CMRPG3N0051).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Law RK, Wolkin AF, Patel N, et al. Injury-related emergency department visits during the COVID-19 pandemic. Am J Prev Med. 2022;63(1):43–50. doi:10.1016/j.amepre.2022.01.018
2. Holland KM, Jones C, Vivolo-Kantor AM, et al. Trends in US emergency department visits for mental health, overdose, and violence outcomes before and during the COVID-19 pandemic. JAMA Psychiatry. 2021;78(4):372–379. doi:10.1001/jamapsychiatry.2020.4402
3. Shrestha R, Siwakoti S, Singh S, Shrestha AP. Impact of the COVID-19 pandemic on suicide and self-harm among patients presenting to the emergency department of a teaching hospital in Nepal. PLoS One. 2021;16(4):e0250706. doi:10.1371/journal.pone.0250706
4. Kobayashi S, Sakakura K, Jinnouchi H, et al. Comparison of door-to-balloon time and in-hospital outcomes in patients with ST-elevation myocardial infarction between before versus after COVID-19 pandemic. Cardiovasc Interv Ther. 2022;37(4):641–650. doi:10.1007/s12928-022-00836-4
5. Aldujeli A, Hamadeh A, Briedis K, et al. Delays in presentation in patients with acute myocardial infarction during the COVID-19 pandemic. Cardiol Res. 2020;11(6):386–391. doi:10.14740/cr1175
6. Garcia S, Stanberry L, Schmidt C, et al. Impact of COVID-19 pandemic on STEMI care: an expanded analysis from the United States. Catheter Cardiovasc Interv. 2021;98(2):217–222. doi:10.1002/ccd.29154
7. Fayed MM, Sharif AF. Impact of lockdown due to COVID-19 on the modalities of intoxicated patients presenting to the emergency room. Prehosp Disaster Med. 2021;36(2):145–162. doi:10.1017/S1049023X20001533
8. Imtiaz S, Nafeh F, Russell C, Ali F, Elton-Marshall T, Rehm J. The impact of the novel coronavirus disease (COVID-19) pandemic on drug overdose-related deaths in the United States and Canada: a systematic review of observational studies and analysis of public health surveillance data. Subst Abuse Treat Prev Policy. 2021;16(1):87. doi:10.1186/s13011-021-00423-5
9. Palis H, Bélair MA, Hu K, Tu A, Buxton J, Slaunwhite A. Overdose deaths and the COVID-19 pandemic in British Columbia, Canada. Drug Alcohol Rev. 2022;41(4):912–917. doi:10.1111/dar.13424
10. Appa A, Rodda LN, Cawley C, et al. Drug overdose deaths before and after shelter-in-place orders during the COVID-19 pandemic in San Francisco. JAMA Network Open. 2021;4(5):e2110452. doi:10.1001/jamanetworkopen.2021.10452
11. DiGennaro C, Garcia GP, Stringfellow EJ, Wakeman S, Jalali MS. Changes in characteristics of drug overdose death trends during the COVID-19 pandemic. Int J Drug Policy. 2021;98:103392.
12. Raffee L, Daradkeh HM, Alawneh K, et al. Impact of COVID-19 lockdown on the incidence and patterns of toxic exposures and poisoning in Jordan: a retrospective descriptive study. BMJ Open. 2021;11(12):e053028. doi:10.1136/bmjopen-2021-053028
13. du Plessis CE, Mohamed F, Stephen CR, et al. A retrospective review of calls to the poisons information helpline of the Western Cape during the first 6 months of the COVID-19 pandemic in South Africa. S Afr J Infect Dis. 2022;37(1):391. doi:10.4102/sajid.v37i1.391
14. Mahmoud NF, Al-Mazroua MK, Afify MM. Toxicology practice during COVID-19 pandemic: experience of the Dammam poison control Center-Eastern Province, Saudi Arabia. Int J Toxicol. 2021;40(4):388–394. doi:10.1177/10915818211017128
15. Milella MS, Boldrini P, Vivino G, Grassi MC. How COVID-19 lockdown in Italy has affected type of calls and management of toxic exposures: a retrospective analysis of a Poison Control Center Database from March 2020 to May 2020. J Med Toxicol. 2021;17(3):250–256. doi:10.1007/s13181-021-00839-2
16. Norvill A, Elliott RA, Wong A. Exposure to hand sanitisers and other cleaning products in Victoria, Australia during the COVID-19 pandemic. Clin Toxicol. 2022;60(6):745–749. doi:10.1080/15563650.2022.2032128
17. Phillips T, Schulte JM, Smith EA, Roth B, Kleinschmidt KC. COVID-19 and contamination: impact on exposures to alcohol-based hand sanitizers reported to Texas poison control centers, 2020. Clin Toxicol. 2021;59(10):926–931. doi:10.1080/15563650.2021.1887491
18. Le Roux G, Sinno-Tellier S, Puskarczyk E, et al. Poisoning during the COVID-19 outbreak and lockdown: retrospective analysis of exposures reported to French poison control centres. Clin Toxicol. 2021;59(9):832–839. doi:10.1080/15563650.2021.1874402
19. Mousavi-Roknabadi RS, Arzhangzadeh M, Safaei-Firouzabadi H, et al. Methanol poisoning during COVID-19 pandemic; A systematic scoping review. Am J Emerg Med. 2022;52:69–84. doi:10.1016/j.ajem.2021.11.026
20. Behnoush AH, Bazmi E, Forouzesh M, Koehler SA, Monabati SJ, Behnoush B. Impact of COVID-19 on poisoning-related mortality in Iran: an interrupted time series study. Int J Drug Policy. 2023;117:104051. doi:10.1016/j.drugpo.2023.104051
21. Tan ST, Chen TH, Yang HW, Su YJ. Changes in poisoning during the COVID-19 pandemic worldwide. Am J Emerg Med. 2022;56:291–293. doi:10.1016/j.ajem.2021.07.027
22. Lai CC, Lee PI, Hsueh PR. How Taiwan has responded to COVID-19 and how COVID-19 has affected Taiwan, 2020-2022. J Microbiol Immunol Infect. 2023;56(3):433–441. doi:10.1016/j.jmii.2023.04.001
23. Hsu CL, Hung SH, Munkhtogoo D, Wang PC. The impact of the COVID-19 pandemic on emergency care of acute myocardial infarction: findings from the Taiwan clinical performance indicator. Int J Qual Health Care. 2023;35(2). doi:10.1093/intqhc/mzad034
24. Ma HH, Tsai SW, Chen CF, et al. Impact of screening COVID-19 on orthopedic trauma patients at the emergency department: a consecutive series from a level I trauma center. J Chin Med Assoc. 2021;84(4):423–427. doi:10.1097/JCMA.0000000000000503
25. Persson HE, Sjoberg GK, Haines JA, Pronczuk de Garbino J. Poisoning severity score. grading of acute poisoning. J Toxicol Clin Toxicol. 1998;36(3):205–213. doi:10.3109/15563659809028940
26. Smith AR, DeVies J, Carey K, et al. COVID-19 pandemic-associated changes in overall emergency department visits by age group, race, and ethnicity - United States, January 2019-April 2022. Am J Emerg Med. 2023;69:121–126. doi:10.1016/j.ajem.2023.04.005
27. Reschen ME, Bowen J, Novak A, et al. Impact of the COVID-19 pandemic on emergency department attendances and acute medical admissions. BMC Emerg Med. 2021;21(1):143. doi:10.1186/s12873-021-00529-w
28. Lin PH, Su HY, Tsai IT, et al. Impact of COVID-19 pandemic on emergency department volume and acuity in low incidence area: Taiwan’s experience in three hospitals. J Acute Med. 2022;12(3):105–112. doi:10.6705/j.jacme.202209_12(3).0003
29. Neumann NR, Chai PR, Wood DM, Greller HA, Mycyk MB. Medical toxicology and COVID-19: our role in a pandemic. J Med Toxicol. 2020;16(3):245–247. doi:10.1007/s13181-020-00778-4
30. Lee J, Fan NC, Yao TC, et al. Clinical spectrum of acute poisoning in children admitted to the pediatric emergency department. Pediatr Neonatol. 2019;60(1):59–67. doi:10.1016/j.pedneo.2018.04.001
31. Torales J, O’Higgins M, Castaldelli-Maia JM, Ventriglio A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int J Soc Psychiatry. 2020;66(4):317–320. doi:10.1177/0020764020915212
32. Ackroyd-Stolarz S, Read Guernsey J, Mackinnon NJ, Kovacs G. The association between a prolonged stay in the emergency department and adverse events in older patients admitted to hospital: a retrospective cohort study. BMJ Qual Saf. 2011;20(7):564–569. doi:10.1136/bmjqs.2009.034926
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.