Back to Journals » Journal of Blood Medicine » Volume 13
Variation in Platelet Activation State in Pre-Donation Whole Blood: Effect of Time of Day and ABO Blood Group
Authors Mousavi SA ![]() , Hermundstad B, Flesland AK, Llohn AH, Saether PC
, Hermundstad B, Flesland AK, Llohn AH, Saether PC
Received 22 February 2022
Accepted for publication 23 May 2022
Published 3 June 2022 Volume 2022:13 Pages 283—292
DOI https://doi.org/10.2147/JBM.S362461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
Seyed Ali Mousavi,1 Brita Hermundstad,1 Annika Kristina Flesland,1 Abid Hussain Llohn,1 Per Christian Saether2
1Department of Immunology and Transfusion Medicine, Akershus University Hospital, Lørenskog, Norway; 2Department of Multidisciplinary Laboratory Medicine and Medical Biochemistry, Akershus University Hospital, Lørenskog, Norway
Correspondence: Abid Hussain Llohn, Department of Immunology and Transfusion Medicine, Akershus University Hospital, Lørenskog, Norway, Tel +47 67961212, Fax +47 67961255, Email [email protected]
Background: Whilst there has been investigation into the effect of time of the day on platelet activation and function in healthy individuals, there is a lack of studies in the literature to examine this relationship among platelet donors.
Methods: We assessed the extent of platelet activation by percentage of platelets with surface-expressed P-selectin and flow cytometry in samples of whole blood from a group of qualified platelet donors (n = 84).
Results: The mean (SD) percentage of activated platelets in the pre-donation blood samples was 1.85 ± 1.57% (range 0.2– 7.5%). In univariate analyses, the percentage of activated platelets was significantly and inversely correlated with the collection time (ie, the time of day blood samples were collected) (r = – 0.35, p = 0.001) and positively correlated to mean platelet volume (MPV) (r = 0.29, p = 0.008). A weaker positive correlation was also observed with ABO blood group (r = 0.228, p = 0.036). Analysis of the collection time as a categorical variable showed a greater degree of activated platelets in samples collected between 8:00 h and 10:00 h than in samples collected during the hours of > 10:00 h ≤ 14:00 h (2.5 ± 1.8 versus 1.1 ± 0.74, p < 0.001). In the adjusted linear regression model, collection time was a significant independent predictor of platelet activation state in whole blood (β = – 0.26; p < 0.001), as did ABO blood group (β = 0.55; p = 0.019).
Conclusion: Our results show that collection time is the most important predictor of platelet activation state in pre-donation whole blood among platelet donors. This work may have implications for optimizing the timing of platelet donation.
Keywords: platelet activation state, surface P-selectin, donor variability
Introduction
Platelets, are anucleate cells produced by megakaryocytes in the bone marrow that circulate in the bloodstream for about 10 days. Circulating platelets play a central role in the hemostatic response to vascular injury. They are also involved in maintaining vascular integrity and contributed to immune and inflammatory responses.1–3 Within an individual, circulating platelets are heterogeneous regarding their number, size, age, buoyant density, and function.4,5 Evidence also suggests that circulating platelets in blood from healthy individuals consist of platelet subpopulations with different degrees of activation.6,7 The activation state of circulating platelets can be assessed by whole-blood flow cytometry of P-selectin (CD62P) and/or the activated form of integrin αIIbβ3 (CD41/CD61) expression on the surface of platelets8 or by measurement of granule release markers, such as beta-thromboglobulin (βTG) and platelet factor 4 (PF4).9 In addition, the evaluation of P-selectin expression and the active form of αIIbβ3 integrin (detected by PAC-1 binding, a specific antibody directed against the activated form of integrin αIIbβ3) are also considered as important markers of platelet activity during storage of platelet products.10
A number of factors may influence the in vivo platelet activation state in healthy individuals. In particular, platelet activation has been shown to vary according to the time of day, with the highest measured levels during the morning hours. For example, Musumeci et al11 measured the urinary excretion of βTG in a group of healthy individuals and found higher values in the morning than in the late afternoon. The study by Jafri et al12 reported diurnal variation in platelet activation, based on plasma levels of βTG and PF4 being higher in the early morning hours, which paralleled that of whole-blood platelet aggregation in response to epinephrine. Similarly, a significantly greater percentage of activated platelets, as assessed by P-selectin exposure,13 or increased agonist-induced platelet aggregation14–17 have been shown to occur during the early morning hours.
Platelet donors, like whole blood and plasma donors, are considered to be one of the healthiest groups of the general population.18,19 However, to our knowledge, the association of time of the day with estimates of the in vivo state of platelet activation in platelet donors has not been previously investigated. Therefore, the aim of this study was to investigate the temporal variation in platelet activation in pre-donation whole blood samples from a group of qualified platelet donors during normal daytime blood bank hours, typically between 08:00 and 14:00 hours, and whether this varied by demographic (eg, gender, age, and ABO blood group) and hematological factors (ie, platelet and red blood cell indices). As lifestyle factors are shown to influence platelet activation,20–23 we also examined if differences in platelet activation state could be influenced by recent (ie, past 24 hours) lifestyle behaviors.
Materials and Methods
Eighty-six platelet donors presenting at the Blood Bank in Akershus University Hospital, Norway, between April 2019 and February 2020 participated in the study. Ethical approval was obtained from the Institutional Review Board at Akershus University Hospital, Norway, and the study complied with the Declaration of Helsinki. Informed written consent was obtained from each participant prior to platelet donation. No donor had taken medications known to alter platelet function within five days of platelet donation. Information on donation time, donation history, and hematologic parameters was available in the donor database. Self-reported recent (past 24 hours) physical activity, smoking, alcohol intake, and sleep quality (see Table 1) were obtained using an anonymous questionnaire. Briefly, donors were asked whether they have had smoked (yes/no), have had physical activity (yes/no), or had consumed alcohol in the past 24 hours (yes/no). Sleep quality was assessed on a five-point scale (1, “very good”; 5, “very poor”) and was dichotomized as very good/good versus moderate. Further details of the survey and results have been described previously.19
 |
Table 1 Donation History, Results of Laboratory Analyses, and Percentage Distribution of Responses to Questionnaire Items by Gender and Age Group (n = 86) |
Blood Collection Procedure
Whole-blood samples were collected from the attached sampling bags (containing 42 mL whole blood collected immediately before plateletpheresis) using standard vacutainers (BD Biosciences). For each donor, two pre-donation blood samples were collected. A blood sample was collected into a citrated tube for flow cytometric determination of platelet surface P-selectin expression. Preliminary measurements performed on blood samples from four donors who agreed to undergo a separate pre-donation venipuncture showed that the percentages of activated platelets were similar regardless of whether citrated blood samples were obtained from the sampling bags or collected from the antecubital vein after the first 3 mL of blood was discarded (data not shown). All pre-donation citrated blood samples for flow cytometric analysis were therefore collected from the attached sampling bags and analyzed within 2 hours of collection. A second sample was collected into an EDTA tube for full blood count that included platelet count and hematological parameters as a routine part of the donor testing, and for determination of platelet indices ordered for the purpose of this study (Table 1). The analyses were performed in the central laboratory at Akershus University Hospital using the Sysmex XE-5000 automated hematology analyzer.
Flow Cytometric Analysis of the Platelet Activation
For flow cytometry, 100 µL of citrated blood (diluted 1:20 with phosphate-buffered saline [PBS] containing 0.1% bovine serum albumin [BSA], pH 7.4) was incubated at room temperature with FITC-conjugated anti-CD61 (5 µL) and PE-conjugated anti-CD62P (10 µL) for 15 min. Background fluorescence was assessed by labeling diluted samples with 10 µL PE-conjugated isotype control antibody (all antibodies from Beckman Coulter, USA). After incubating, the samples were diluted to 4 mL with PBS/BSA and analyzed immediately on a FACS Canto II flow cytometer (BD Bioscience). The percentage of activated platelets (ie, CD61 and CD62P double-positive platelets) was obtained from a total of 10000 recorded events with the CD61+ gate. Representative FACS plots are shown in Figure 1. In one series of experiments (n = 4), these analyses were performed on pre-donation blood samples that were pre-treated with adenosine diphosphate (ADP, 10 µM). Pre-incubation of whole-blood samples with ADP was associated with a marked increase in the percentage of activated platelets (78.7 ± 5.3% compared to 1.9 ± 2.0% in unstimulated samples), indicating that platelet activation measured in pre-donation blood samples represents basal, circulating, activation states. In a pilot study among five donors, we also compared the percentage of platelets expressing P-selectin in pre-donation blood samples that were collected into vacutainer tubes containing EDTA (known to cause platelet activation) with those collected in sodium citrate (both samples collected from the attached sampling bags). The results showed a clear increase in the percentage of P-selectin positive platelets: 36.7% ± 31.8% (range 5.7–84.2%) compared with 1.6% ± 1.6% (range 0.11–3.5%) in blood samples collected in sodium citrate.
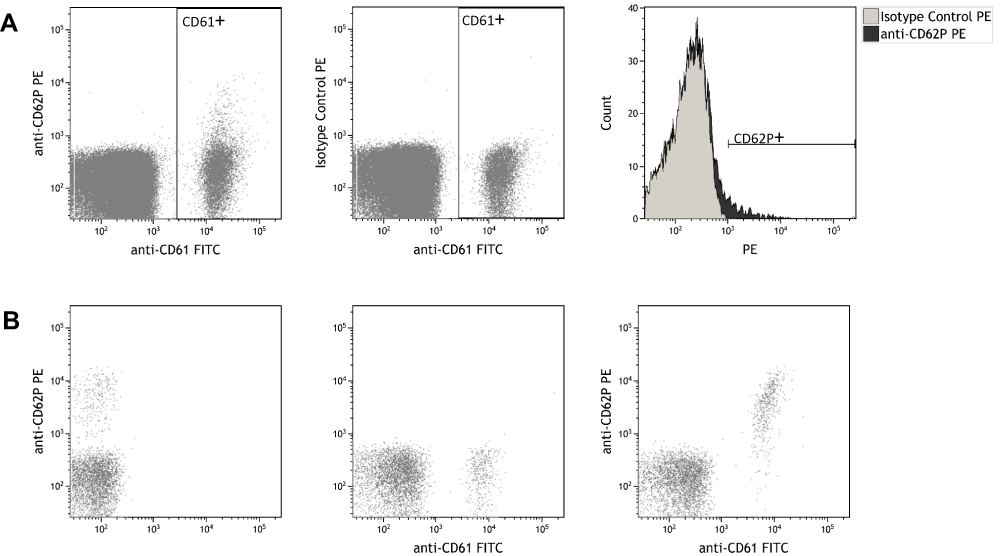 |
Figure 1 Representative flow cytometry plots of activated platelets in pre-donation whole blood samples. (A) Whole blood samples were incubated with anti-CD61 and anti-CD62P (left) or isotype control (middle), washed and analyzed by flow cytometry. Histogram overlay of CD61-positive events is shown to the right. (B) Flow cytometry dot plots showing whole blood samples stimulated with ADP. |
Statistical Analysis
Continuous variables are summarized with mean ± standard deviation (SD) and median with interquartile range (IQR). Mean values were compared using unpaired. Categorical variables were compared using Chi-square or Fisher’s exact test, as appropriate. The effect of donation time on platelet activation state was assessed either as a continuous variable or as a dichotomous variable using the median value of collection time as a cut point. Associations between platelet activation state and the other study variables were assessed using Pearson’s correlation coefficients. Multivariate linear regression modeling (backward stepwise) was used to determine whether the timing of blood collection was an independent predictor of platelet activation state. Variables included were those significant at p < 0.1 in the univariate analysis. ABO blood group was included as a dichotomous variable (A group versus O group) in the model. The relative contribution of the independent variables in the regression analysis is presented as the standardized regression coefficient (Beta). Statistical significance was assumed at p < 0.05. Because the data for platelet activation were not normally distributed, they were logarithmically transformed, and p values derived from log-transformed data were used in statistical analyses. Analyses were performed using SPSS 25 software.
Results
Donor Characteristics
The donation history, pre-donation laboratory data, and the donor-reported recent (ie, past hours) lifestyle behaviors stratified by gender and age are shown in Table 1. The mean age was 50.8 ± 9.7 years with 56% of donors being female. All donors had previously made at least four donations (whole blood and/or apheresis donations combined) and had donated platelets at least once during the past six years. The mean time since the last donation was 10.6 ± 7.3 weeks. Most (>90%) donors with longer-than-average donation interval had, however, other concurrent donations, mostly plasma. There were significant differences between average values for males and females for both hemoglobin and hematocrit. Older donors had donated a higher number of both combined and platelet donations. They also had higher values for hemoglobin and hematocrit than younger donors. No significant differences were found in other variables between the demographic subgroups. The donors in this study were ambulatory prior to platelet donation and most likely followed their usual daily activities. They had adequate sleep duration and most (85%) reported good sleep quality the previous night. Four donors had smoked ~70 minutes prior to donation and 38 reported recent physical activity within 13.0 ± 6.8 hours before donation. Nine donors had consumed alcohol the previous night.
Platelet Activation State
Eighty-six pre-donation whole-blood samples were analyzed for platelet activation. One blood sample was excluded because no anti-CD61-binding platelets could be detected, and another was excluded because of failed assay, resulting in a total of 84 samples analyzed. The percentage of activated (ie, P-selectin-expressing) platelets in pre-donation blood samples ranged from 0.2% to 7.5% (1.85 ± 1.57%; median, 1.3%; IQR, 0.8–2.3%). Twenty-seven donors (32%) had less than 1.0% activated platelets, and five donors (6%) had more than 5.0% activated platelets, indicating considerable donor variability in the levels of circulating activated platelets.
By univariate analysis, the percentage of activated platelets was significantly and inversely correlated with the time of day at which blood samples were collected (hereafter collection time, Table 2 and Figure 2) and positively correlated with mean platelet volume (MPV), a surrogate marker of platelet activation, platelet distribution width (PDW), platelet-large cell ratio (P-LCR), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and red blood cell distribution width (RDW), a measure of variability in red blood cell size (Table 2). Collection time was also marginally negatively (p = 0.075) associated with MPV (Table 2 and Figure 2). Platelet count, immature platelet fraction (IPF), a measure of young, reticulated platelets, and immature platelet count (IPC) showed no correlations with the percentage of activated platelets or collection time. IPF and IPC were, however, highly correlated (r = 0.95) and both were significantly correlated with MPV, P-LCR and PDW, as expected (Table 2). In the multivariate model with all correlates (Table 3), collection time, RDW, and ABO blood group were each independently correlated with the percentage of activated platelets, whereas MPV remained marginally significant (p = 0.056). The model accounted for 30% (R2 = 0.298) of the variance in platelet activation in pre-donation blood.
 |
Table 2 Correlation of Platelet Activation in Pre-Donation Blood Samples with Collection Time and Other Covariates (n = 84) |
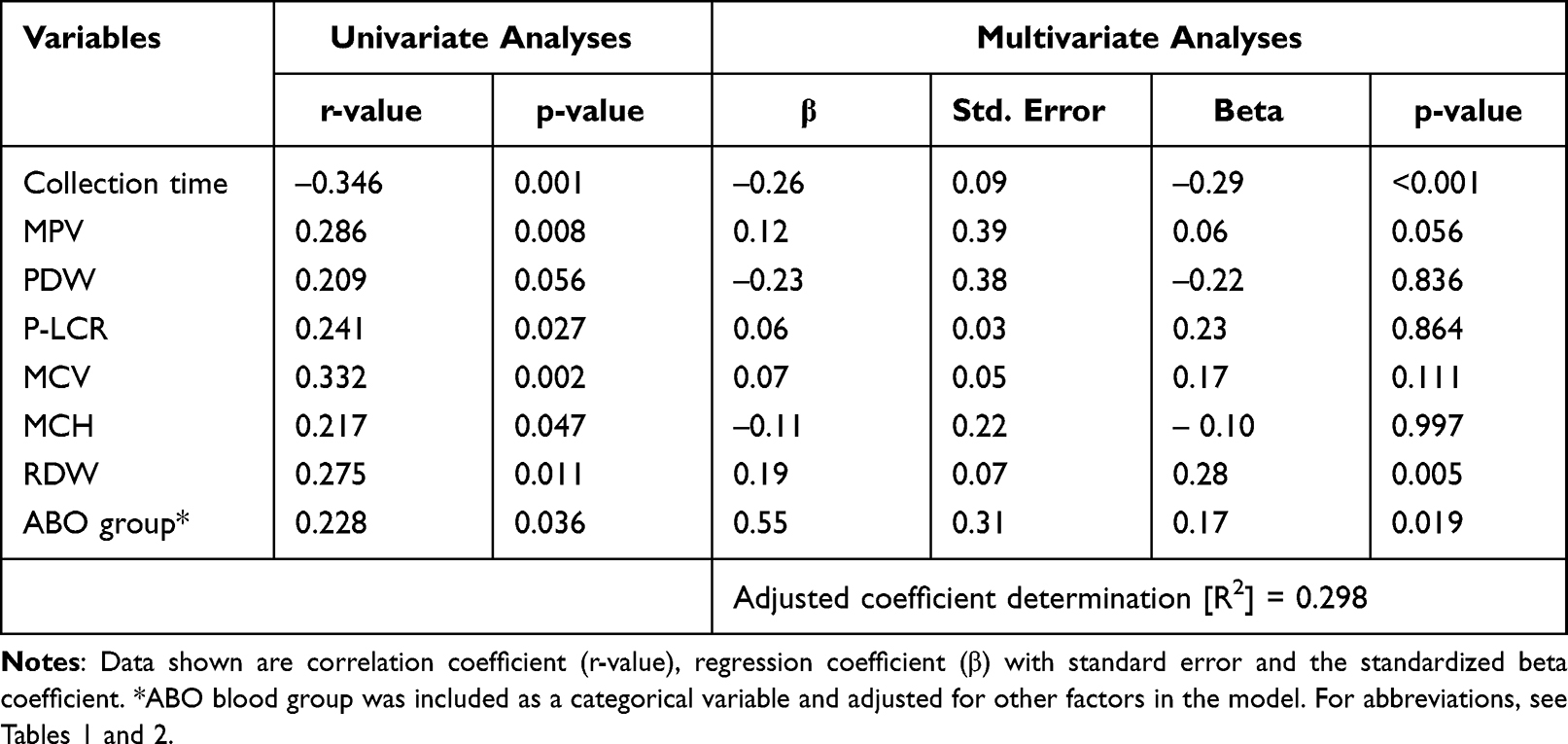 |
Table 3 Results of Univariate (Unadjusted) and Backward Multivariable Linear (Adjusted) Models for Association of Platelet Activation in Whole Blood (n = 84) to Collection Time and Other Factors |
 |
Figure 2 Relationship between (A) the percentage of P-selectin-positive platelets and (B) mean platelet volume (MPV, a surrogate marker of platelet activation) with the time of day at which blood samples were collected (collection time). The percentage of P-selectin-positive platelets, as assessed by flow cytometry, correlated inversely (r = –0.35), with the collection time. MPV, as measured via a Sysmex XE-5000 analyzer, was also inversely correlated with the collection time, although it did not reach statistical significance in this study. |
The inverse association between platelet activation and collection time suggests that a higher proportion of circulating platelets occurs in the earlier hours of the day. To further analyze this association, collection time was dichotomized according to whether the pre-donation samples were collected between 8:00 h and 10:00 h (n = 46) or during >10:00 h ≤14:00 h (n = 38), using the median value of collection time as the cut-off point. The mean percentage of activated platelets between 8:00 h and 10:00 h (2.5 ± 1.8%) was significantly higher than during the hours of >10:00 h ≤14:00 h (1.1 ± 0.74%, p < 0.001), suggesting higher levels of circulating platelet activity at this time of day.
In univariate analyses, there were no statistically significant associations between the percentage of activated platelets in pre-donation blood and gender, age, or BMI, but an association with ABO blood group was observed (Table 3); group A donors had slightly but significantly higher levels of activated platelets than did group O donors (2.1 ± 1.7 versus 1.6 ± 1.4, p = 0.037). Tobacco smoking, physical activity, and alcohol consumption have been associated with increased platelet reactivity in healthy persons.20–22 Donors who had smoked prior to donation had a higher mean platelet activation than did non-smokers (3.0 ± 3.0% versus 1.8 ± 1.5% in non-smokers), but this difference was not statistically significant (p = 0.32). The mean platelet activation did not differ significantly between donors who engaged and those who did not engage in physical activity in the past 24 hours (1.7% ± 1.4% versus 2.0 ± 1.7%, p = 0.48). There was also no significant difference in platelet activation between those who reported recent alcohol consumption and those who did not (1.8 ± 1.3 versus 1.9 ± 1.6; p = 0.95).
Discussion
Agreeing with previous studies in healthy donors,24–26 low levels of activated platelets (0.2–7.5%) were detected in unstimulated pre-donation blood samples. Our study extended these results by showing that platelet activation in pre-donation blood samples is inversely correlated with the collection time. Collection time also showed an inverse though statistically not significant correlation with another marker of platelet activation, namely MPV. The temporal variation in platelet activation was also evident when collection time was treated as a categorical variable, being significantly higher in blood samples collected between 8:00 h and 10:00 h than those collected during the hours of >10:00 h ≤14:00 h, suggesting that there may be a temporal component in the regulation of activation state of circulating platelets, consistent with previous literature.27
In the adjusted regression model, collection time was shown to be independently associated with the percentage of activated platelet, as did ABO blood group and RDW (Table 3). We note, however, that the variables associated with the percentage of platelet activation together explain 30% of the variation in platelet activation, indicating that other, unmeasured, donor and/or environmental factors28,29 must play a major role in determining the in vivo platelet activation state.
The physiologic mechanisms that mediate diurnal variation in circulating levels of activated platelets are unclear. Using a forced desynchrony protocol in which 12 healthy volunteers (6 males and 6 females) were studied on a 20-hour recurring cycle in dim-light for 10 days, Scheer and coworkers27 have shown that surface expression of platelet activation-dependent markers P-selectin and the activated form of αIIbβ3 is under circadian (~24 hour) control, with peaks occurring around 09:00 h and nadir around 17:00 h. However, since platelets are devoid of nuclei and have limited de novo protein synthesis capacity,30 they may not contain the necessary components for rhythmic expression of clock gene products.31,32 However, platelets may be affected by physiological factors that are not intrinsic to platelets themselves. In fact, several studies in healthy subjects have shown a diurnal variation in a number of hemostatic parameters. For example, a higher clotting tendency and a lower fibrinolytic activity have been reported during the morning hours.33,34 In particular, plasma levels of von Willebrand factor (VWF)35,36 and prothrombin fragment 1+2, markers of thrombin generation37 have been shown to be higher in the morning/midday in comparison with afternoon/night, which may affect platelet activation pathways, and thereby levels of circulating activated platelets over the course of the day. Diurnal variation in other plasma factors may also have the potential to influence platelet activation pathways. For example, plasma cortisol and adrenalin levels have been shown to have somewhat similar circadian patterns (the timing of highest values approximately at 9:00 AM and 8:00 AM, respectively),38 and may likely contribute to the enhanced platelet activation in early morning hours.27
Of further note is that plasma levels of VWF have been shown to be significantly higher in non-O than in group O individuals.39 Our finding of higher platelet activation in blood samples from group A donors compared to group O donors could therefore be due to elevated VWF levels in these donors, which can lead to increased platelet activation via the platelet-specific GPIb-IX-V receptor. RDW, a measure of variability in red blood cell size, was the only hematologic variable that is independently associated with the percentage of activated platelets (Table 3). One possible explanation for this observation may be erythrocyte modulation of platelet activation via platelet–erythrocyte interactions. For example, Valles et al40 have shown that supernatants of collagen-stimulated platelets after co-incubation with erythrocytes induced far more platelet activation (as measured by P-selectin exposure and PAC-1 binding) than did supernatants of collagen-stimulated platelets in the absence of erythrocytes.
Our study had some limitations. First, platelet activation in blood samples was assessed only once, whereas ≥4 measurements on the same day are required in order to determine whether the observed changes in platelet activation truly reflect a diurnal variation, an experimental design clearly not feasible in blood banking research. However, our results showed that there was a 2.3-fold decrease in the percentage of activated platelets in whole blood during the hours of >10:00 h ≤ 14:00 h relative to the percentage of activated platelets detected in blood samples taken between 08:00 h and 10:00 h (p < 0.001), indicating that there is still a chance of finding a difference related to diurnal variation in platelet activation. Nevertheless, further well-designed studies which include blood sampling time points during afternoon/evening will be required to more fully characterize the effect of donation time on platelet activation states. Second, platelet activation could also be influenced by dietary composition. However, our study could not control the impact of recent food consumption on platelet activation because donors are recommended to eat/drink prior to their donation. Third, the number of donors who reported recent smoking and alcohol consumption was small, and therefore not powered to detect significant differences.
Conclusions
To our knowledge, this is the first study to investigate the association of time of day with platelet activation state, as measured by P-selectin exposure, among platelet donors during normal daytime blood bank hours. We also investigated the associations of platelet activation with a range of hematologic factors, demographic subgroups defined by age group, gender, and ABO blood group, as well as three donor-reported lifestyle behaviors. Our results showed that platelet activation was significantly and inversely associated with the collection time by univariate analysis and after adjustment for covariates. Our study also showed that blood group A was associated with higher platelet activation. This work may have implications for optimizing the timing of platelet donation, if, for example, the temporal variation in platelet activation at the time of donation can impact the final heterogeneity of the stored platelet concentrates and, potentially, transfusion outcomes. Further studies would be needed to see if the same relationship between donation time and platelet activation state, as we observed in this initial study of pre-donation blood samples, would also be reflected in platelet activation in the corresponding apheresis platelet concentrates and to determine the relative contribution of variability in platelet donation time to the total variation in platelet activation in the final platelet products.
Abbreviations
MPV, mean platelet volume; PDW, platelet distribution width; P-LCR, platelet-large cell ratio; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; RDW, red blood cell distribution width; IPF, immature platelet fraction; IPC, immature platelet count.
Acknowledgments
We wish to thank the platelet donors for their participation in this study and the interviewing/apheresis staff at our Blood Bank for help with recruiting donors and preparation of the blood samples for flow cytometry analysis. We also thank the staff of the Hematology laboratory for measurement of platelet indices and the staff of the Department of Epigen at Akershus University Hospital for hematological analyses and flow cytometry access.
Funding
This study received no funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Becker RC, Sexton T, Smyth SS. Translational implications of platelets as vascular first responders. Circ Res. 2018;122(3):506–522. doi:10.1161/CIRCRESAHA.117.310939
2. Gupta S, Konradt C, Corken A, et al. Hemostasis vs. homeostasis: platelets are essential for preserving vascular barrier function in the absence of injury or inflammation. Proc Natl Acad Sci USA. 2020;117(39):24316–24325. doi:10.1073/pnas.2007642117
3. van der Meijden PEJ, Heemskerk JWM. Platelet biology and functions: new concepts and clinical perspectives. Nat Rev Cardiol. 2019;16(3):166–179. doi:10.1038/s41569-018-0110-0
4. Lesyk G, Jurasz P. Advances in platelet subpopulation research. Front Cardiovasc Med. 2019;6:138. doi:10.3389/fcvm.2019.00138
5. Thompson CB, Jakubowski JA. The pathophysiology and clinical relevance of platelet heterogeneity. Blood. 1988;72(1):1–8. doi:10.1182/blood.V72.1.1.1
6. Handtke S, Steil L, Greinacher A, Thiele T. Toward the relevance of platelet subpopulations for transfusion medicine. Front Med. 2018;5:17. doi:10.3389/fmed.2018.00017
7. Tomaiuolo M, Brass LF, Stalker TJ. Regulation of platelet activation and coagulation and its role in vascular injury and arterial thrombosis. Interv Cardiol Clin. 2017;6(1):1–12. doi:10.1016/j.iccl.2016.08.001
8. Spurgeon BEJ, Linden MD, Michelson AD, Frelinger AL 3rd:. Immunophenotypic analysis of platelets by flow cytometry. Curr Protoc. 2021;1(6):e178. doi:10.1002/cpz1.178
9. Kaplan KL, Owen J. Plasma levels of beta-thromboglobulin and platelet factor 4 as indices of platelet activation in vivo. Blood. 1981;57(2):199–202. doi:10.1182/blood.V57.2.199.199
10. Beshkar P, Hosseini E, Ghasemzadeh M. Superior integrin activating capacity and higher adhesion to fibrinogen matrix in buffy coat-derived platelet concentrates (PCs) compared to PRP-PCs. Transfus Apher Sci. 2018;57(1):76–81. doi:10.1016/j.transci.2017.12.003
11. Musumeci V, Rosa S, Caruso A, Zuppi C, Zappacosta B, Tutinelli F. Abnormal diurnal changes in in-vivo platelet activation in patients with atherosclerotic diseases. Atherosclerosis. 1986;60(3):231–236. doi:10.1016/0021-9150(86)90170-X
12. Jafri SM, VanRollins M, Ozawa T, Mammen EF, Goldberg AD, Goldstein S. Circadian variation in platelet function in healthy volunteers. Am J Cardiol. 1992;69(9):951–954. doi:10.1016/0002-9149(92)90799-5
13. Undar L, Akkoç N, Alakavuklar MN, Cehreli C, Undar L. Flow cytometric analysis of circadian changes in platelet activation using anti-GMP-140 monoclonal antibody. Chronobiol Int. 1999;16(3):335–342. doi:10.3109/07420529909116862
14. Dalby MC, Davidson SJ, Burman JF, Davies SW. Diurnal variation in platelet aggregation with the PFA-100 platelet function analyser. Platelets. 2000;11(6):320–324. doi:10.1080/09537100050144731
15. Jovicić A, Mandić S. Circadian variations of platelet aggregability and fibrinolytic activity in healthy subjects. Thromb Res. 1991;62(1–2):65–74. doi:10.1016/0049-3848(91)90669-N
16. May JA, Fox S, Glenn J, Craxford S, Heptinstall S. Platelet function reduces significantly during the morning. Platelets. 2008;19(7):556–558. doi:10.1080/09537100802195405
17. Wiens L, Lutze G, Luley C, Westphal S. Platelet count and platelet activation: impact of a fat meal and day time. Platelets. 2007;18(2):171–173. doi:10.1080/09537100600930946
18. Atsma F, de Vegt F. The healthy donor effect: a matter of selection bias and confounding. Transfusion. 2011;51(9):1883–1885. doi:10.1111/j.1537-2995.2011.03270.x
19. Mousavi SA, Hermundstad B, Saether PC, Nybruket MJ, Knutsen TR, Llohn AH. Health behavior and lifestyle trends among platelet donors: results from a questionnaire-based survey in Norway. Biomed Res Int. 2021;2021:1–12. doi:10.1155/2021/8891885
20. Hilberg T, Menzel K, Gläser D, Zimmermann S, Gabriel HH. Exercise intensity: platelet function and platelet-leukocyte conjugate formation in untrained subjects. Thromb Res. 2008;122(1):77–84. doi:10.1016/j.thromres.2007.08.018
21. Mukamal KJ, Massaro JM, Ault KA, et al. Alcohol consumption and platelet activation and aggregation among women and men: the Framingham Offspring Study. Alcohol Clin Exp Res. 2005;29(10):1906–1912. doi:10.1097/01.alc.0000183011.86768.61
22. Nocella C, Biondi-Zoccai G, Sciarretta S, et al. Impact of tobacco versus electronic cigarette smoking on platelet function. Am J Cardiol. 2018;122(9):1477–1481. doi:10.1016/j.amjcard.2018.07.029
23. Peace AJ, Egan K, Kavanagh GF, et al. Reducing intra-individual variation in platelet aggregation: implications for platelet function testing. J Thromb Haemost. 2009;7(11):1941–1943. doi:10.1111/j.1538-7836.2009.03593.x
24. Becker RC, Tracy RP, Bovill EG, Mann KG, Ault K. The clinical use of flow cytometry for assessing platelet activation in acute coronary syndromes. TIMI-III thrombosis and anticoagulation group. Coron Artery Dis. 1994;5(4):339–345. doi:10.1097/00019501-199404000-00010
25. Holme S, Sweeney JD, Sawyer S, Elfath MD. The expression of p-selectin during collection, processing, and storage of platelet concentrates: relationship to loss of in vivo viability. Transfusion. 1997;37(1):12–17. doi:10.1046/j.1537-2995.1997.37197176945.x
26. Wyant TL, Smith PC, Brown B, Kantor AB. Whole blood microvolume laser scanning cytometry for monitoring resting and activated platelets. Platelets. 2001;12(5):309–318. doi:10.1080/09537100120068206
27. Scheer FA, Michelson AD, Frelinger AL 3rd, et al. The human endogenous circadian system causes greatest platelet activation during the biological morning independent of behaviors. PLoS One. 2011;6(9):e24549. doi:10.1371/journal.pone.0024549
28. Jones CI, Garner SF, Angenent W, et al. Mapping the platelet profile for functional genomic studies and demonstration of the effect size of the GP6 locus. J Thromb Haemost. 2007;5(8):1756–1765. doi:10.1111/j.1538-7836.2007.02632.x
29. Yee DL, Bergeron AL, Sun CW, Dong JF, Bray PF. Platelet hyperreactivity generalizes to multiple forms of stimulation. J Thromb Haemost. 2006;4(9):2043–2050. doi:10.1111/j.1538-7836.2006.02089.x
30. Schubert P, Devine DV. De novo protein synthesis in mature platelets: a consideration for transfusion medicine. Vox Sang. 2010;99(2):112–122. doi:10.1111/j.1423-0410.2010.01333.x
31. Curtis AM, Fitzgerald GA. Central and peripheral clocks in cardiovascular and metabolic function. Ann Med. 2006;38(8):552–559. doi:10.1080/07853890600995010
32. Westgate EJ, Cheng Y, Reilly DF, et al. Genetic components of the circadian clock regulate thrombogenesis in vivo. Circulation. 2008;117(16):2087–2095. doi:10.1161/CIRCULATIONAHA.107.739227
33. Haus E. Chronobiology of hemostasis and inferences for the chronotherapy of coagulation disorders and thrombosis prevention. Adv Drug Deliv Rev. 2007;59(9–10):966–984. doi:10.1016/j.addr.2006.11.002
34. West AS, Schønsted MI, Iversen HK. Impact of the circadian clock on fibrinolysis and coagulation in healthy individuals and cardiovascular patients – a systematic review. Thromb Res. 2021;207:75–84. doi:10.1016/j.thromres.2021.09.011
35. Rudnicka AR, Rumley A, Lowe GD, Strachan DP. Diurnal, seasonal, and blood-processing patterns in levels of circulating fibrinogen, fibrin D-dimer, C-reactive protein, tissue plasminogen activator, and von Willebrand factor in a 45-year-old population. Circulation. 2007;115(8):996–1003. doi:10.1161/CIRCULATIONAHA.106.635169
36. Timm A, Fahrenkrug J, Jørgensen HL, Sennels HP, Goetze JP. Diurnal variation of von Willebrand factor in plasma: the Bispebjerg study of diurnal variations. Eur J Haematol. 2014;93(1):48–53. doi:10.1111/ejh.12298
37. Kapiotis S, Jilma B, Quehenberger P, Ruzicka K, Handler S, Speiser W. Morning hypercoagulability and hypofibrinolysis. Diurnal variations in circulating activated factor VII, prothrombin fragment F1+2, and plasmin-plasmin inhibitor complex. Circulation. 1997;96(1):19–21. doi:10.1161/01.CIR.96.1.19
38. Scheer FA, Hu K, Evoniuk H, et al. Impact of the human circadian system, exercise, and their interaction on cardiovascular function. Proc Natl Acad Sci USA. 2010;107(47):20541–20546. doi:10.1073/pnas.1006749107
39. Gill JC, Endres-Brooks J, Bauer PJ, Marks WJ Jr, Montgomery RR. The effect of ABO blood group on the diagnosis of von Willebrand disease. Blood. 1987;69(6):1691–1695. doi:10.1182/blood.V69.6.1691.1691
40. Vallés J, Santos MT, Aznar J, et al. Platelet-erythrocyte interactions enhance alpha(IIb)beta(3) integrin receptor activation and P-selectin expression during platelet recruitment: down-regulation by aspirin ex vivo. Blood. 2002;99(11):3978–3984. doi:10.1182/blood.V99.11.3978
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.