Back to Journals » Clinical Interventions in Aging » Volume 18
Variables Associated with 30-Day Mortality in Very Elderly COVID-19 Patients
Authors Xing Y ![]() , Sun Y, Tang M
, Sun Y, Tang M ![]() , Huang W, Luo J
, Huang W, Luo J ![]() , Ma Q
, Ma Q ![]()
Received 14 April 2023
Accepted for publication 11 July 2023
Published 25 July 2023 Volume 2023:18 Pages 1155—1162
DOI https://doi.org/10.2147/CIA.S417282
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Yunli Xing, Ying Sun, Mei Tang, Wei Huang, Jia Luo, Qing Ma
Department of Geriatrics, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Qing Ma, Department of Geriatrics, Beijing Friendship Hospital, Capital Medical University, No. 95, Yongan Road, Xicheng District, Beijing, 100050, People’s Republic of China, Tel +86 13801019331, Fax +86 10 6313 8040, Email [email protected]
Background: Advanced age increases the risk for severe COVID-19. However, the risk factors for mortality from COVID-19 in very elderly patients (≥ 80-years-old) are unknown.
Objective: Investigate the relationship of mortality with the clinical characteristics of very elderly COVID-19 patients.
Materials and Methods: Very elderly patients who were hospitalized with COVID-19 from December 3, 2022 to January 1, 2023 were retrospectively examined. Sociodemographic and clinical variables were recorded and survival was recorded after 30 days.
Results: We examined 181 patients (median age: 90.84 years; 114 older than 90 years). The median Barthel index was 30.69, and 55.8% of patients had severe or critical COVID-19 pneumonia. Forty-two patients (33.2%) received a high-flow nasal cannula or non-invasive ventilation, and only 4.4% received mechanical ventilation. The overall mortality was 35.9%, and there was no significant difference in mortality for the 80 to 90-year-old group and the over 90-year-old group (37.7% vs 32.8%, P=0.508). A multivariate analysis showed that the Barthel index (OR, 0.975; 95% CI, 0.962– 0.989), serum creatinine (SCr) level (OR, 1.003; 95% CI, 1.000– 1.006), white blood cell (WBC) count (OR, 1.160; 95% CI, 1.056– 1.276), D-dimer level (OR, 1.060; 95% CI, 1.009– 1.113), and corticosteroid use (OR, 0.268; 95% CI, 0.124– 0.582) were significantly and independently related to 30-day mortality. A binary classification model based on the multivariate analysis had good predictive value (area under the curve, 0.794).
Conclusion: Very elderly COVID-19 patients have a high risk for mortality. The Barthel index, SCr, WBC count, D-dimer level, and corticosteroid use were independently associated with mortality.
Keywords: COVID-19, over-80-year-old, characteristic, mortality
Introduction
There have been 240 million confirmed cases and nearly 5 million deaths worldwide from coronavirus disease 2019 (COVID-19). Beginning in December 2022, there was a dramatic increase in the prevalence of COVID-19 in Beijing. The clinical severity of COVID-19 ranges from asymptomatic or mildly symptomatic to critical illness with multi-organ failure. There is evidence that lymphocytopenia, elevated levels of inflammatory biomarkers, and especially advanced age are associated with poor prognosis in patients with COVID-19.1 In particular, elderly adults are more likely to have severe disease and fatal outcome.
Early data from China demonstrated that the case fatality rate (CFR) increased with age, in that it was 0.4% or lower for patients who were 40-years-old or younger, 1.3% for those in their 50s, 3.6% for those in their 60s, 8% for those in their 70s, and 14.8% for those in their 80s or older.2 The mortality rate in patients who are 80-years-old or more is therefore more than 6-times higher than in younger patients. The data on COVID-19 cases and deaths in nursing homes is also very striking. There are up to 1.5 million nursing home residents in the US, less than 0.5% of its population, but these individuals accounted for 40% of all COVID deaths.3 Age-related immune system remodeling and immuno-senescence are the major reasons for the increased susceptibility to infections, particularly respiratory infections, in the elderly.4,5 However, only a few studies have focused on COVID-19 in patients who were 80-years-old or more (henceforth “very elderly”). Instead, most of these previous studies focused on middle-aged patients (in their 50s or 60s),1 or compared the mortality of different age groups. Very few studies have specifically examined the characteristics of very elderly patients with COVID-19. It is therefore unclear if the clinical characteristics or prognostic factors associated with severe COVID-19 are different for these very elderly patients.
Here, we present a retrospective analysis of the clinical characteristics of very elderly patients who were hospitalized with COVID-19 in an effort to identify risk factors associated with 30-day mortality.
Materials and Methods
Patients who were very elderly (≥80-years-old), diagnosed with COVID-19, and admitted to the Geriatric Department of Beijing Friendship Hospital between December 3, 2022 and January 3, 2023 were retrospectively examined. All patients were in a cadre ward that provides care to elderly and retired government officials, most of whom are senile males. The included patients met the China CDC definition for COVID-196 and had evidence of infection by the severe acute respiratory coronavirus 2 (SARS-CoV-2) based on RT-PCR or antigen testing. The inclusion criteria were: (i) age of at least 80 years and (ii) positive results for SARS-CoV-2 from RT-PCR or antigen testing. The exclusion criteria were: (i) age less than 80 years; (ii) negative RT-PCR results in two consecutive samples taken 48 h apart; or (iii) loss to follow up. Although data on the SARS-CoV-2 variants in these patients were unavailable, the Omicron variant was dominant in Beijing during the study period.
All patients had symptoms or signs of COVID-19 and were classified according to disease severity:7 mild illness (any of the various signs and symptoms of COVID-19, but no abnormal chest imaging results); moderate illness (evidence of lower respiratory disease during clinical assessment or imaging, and oxygen saturation of 93% or more measured by pulse oximetry [SpO2] in room air at sea level); severe illness: SpO2 below 93%, or radiological evidence of lung infiltrates accounting for more than 50% of the lung field; and critical illness (septic shock, and/or multiple organ dysfunction and need for mechanical ventilation or admission to an intensive care unit [ICU]).
The Barthel scale was used to measure activities of daily living (ADL) at admission. This scale considers several daily activities (feeding, bathing, grooming, dressing, bowel and bladder control, ability to use a toilet, transfer from bed to chair and vice-versa, mobility on level-surfaces, and ability to climb stairs) and classifies individuals as independent (80–100 points), minimally dependent (60–79 points), partially dependent (40–59 points), very dependent (20–39 points), or totally dependent (<20 points).
All data were retrieved from clinical and epidemiological records, including comorbidities, symptoms, laboratory data at admission, and treatments. All patients received follow-up for 30 days after diagnosis. The primary end-point was all-cause death.
Ethical approval was obtained from the Ethical Committee of Beijing Friendship Hospital. Due to the anonymized and retrospective design of this study, informed consent was not required. This study was in compliance with the Declaration of Helsinki.
Statistical Analysis
Statistical analysis was carried out using the SPSS version 16.0 (SPSS Inc., Chicago, IL, USA). A descriptive univariate analysis of all variables was carried out. Qualitative variables are presented as absolute and relative frequencies, and quantitative variables as medians and interquartile ranges (IQRs). For comparisons of independent samples, Pearson’s chi-square test was used for qualitative variables, and the Mann–Whitney U-test or the Kruskal–Wallis test was used for quantitative variables. Time-at-risk was measured from the enrollment date to the date of death. Time-to-event analysis was used to identify predictors of death. Receiver operator characteristic (ROC) analysis and calculation of area under the curve (AUC) were used to analyze the overall diagnostic performance of combined risk factors.
Results
Demographic Characteristic
We retrospectively examined 181 very elderly patients who had COVID-19 and were hospitalized in the Geriatric Department of Beijing Friendship Hospital during the 1 month study period, a period during which the Omicron variant of SARS-CoV-2 was predominant in this region (Table 1). Overall, the median age was 90.84 years (range: 80–103), 114 patients (63.0%) were older than 90 years, 145 patients (80.1%) were male, the median Barthel (ADL) score was 30.69 (range: 0–60), and the mean time from symptom onset to hospitalization was 5 days. There were 167 patients (92.3%) who had at least one comorbidity. Comparison of two age groups (80–89 years vs ≥90 years) indicated there were significant differences in the sex ratio, coronary heart disease (CHD), diabetes mellitus (DM), chronic pulmonary disease (CPD), duration of symptoms before hospitalization, diastolic blood pressure (DBP), and C reactive protein (CRP; all P < 0.05).
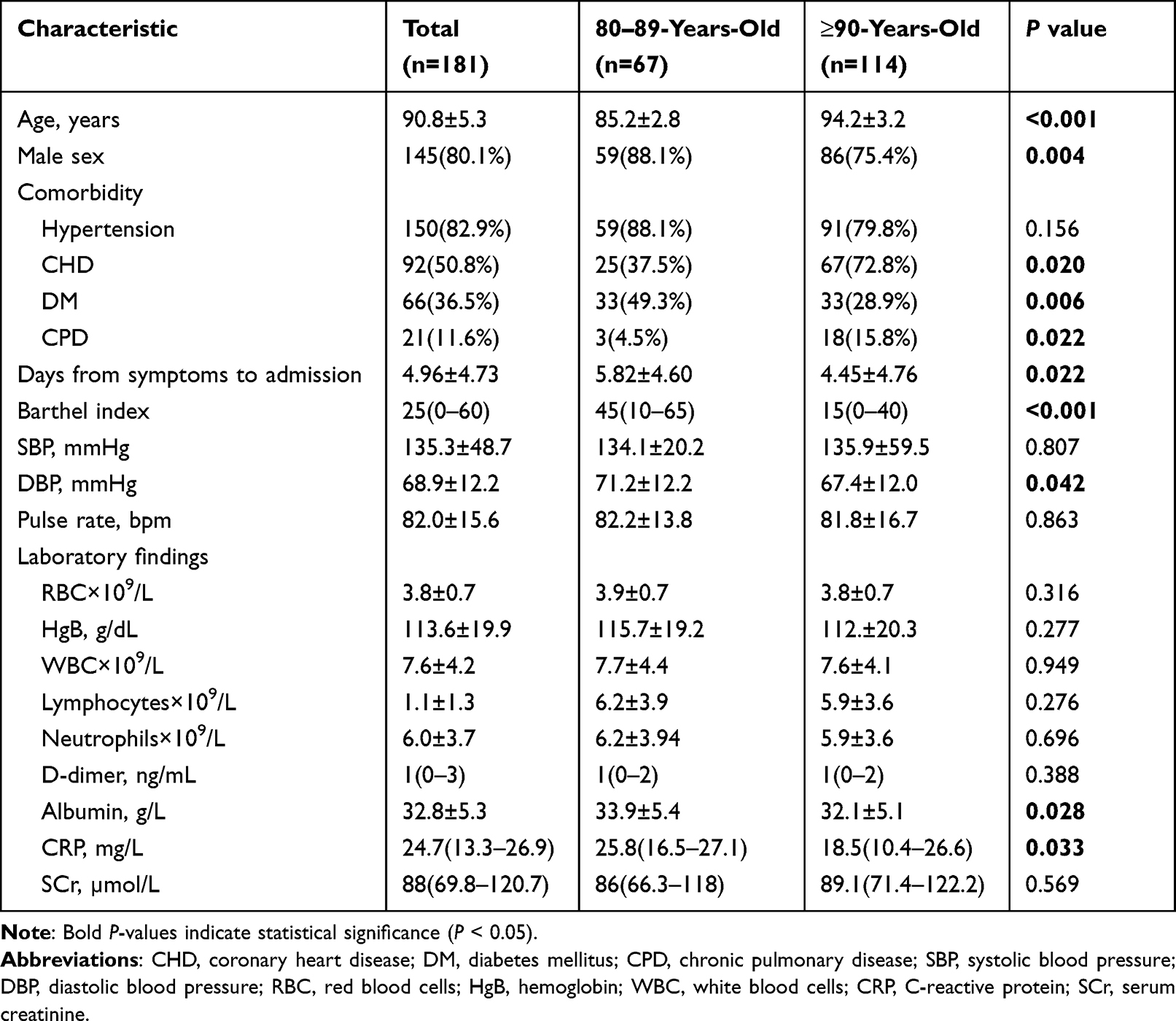 |
Table 1 Demographic and Clinical Characteristics of Patients at Baseline |
Clinical Characteristics and Outcomes
All patients received thorax computed tomography (CT) or X-ray examinations (Table 2). Twenty-five patients (13.8%) had mild illness, 55 (30.4%) had moderate illness, 35 (19.3%) had severe illness, and 66 (36.5%) had critical illness. Overall, 86 patients (47.5%) received anti-viral treatment (paxlovid or azvudine), 61 (33.7%) received a corticosteroid (dexamethasone or methylprednisolone), 5 (2.8%) received baricitinib, and 3 (2.8%) received tocilizumab.
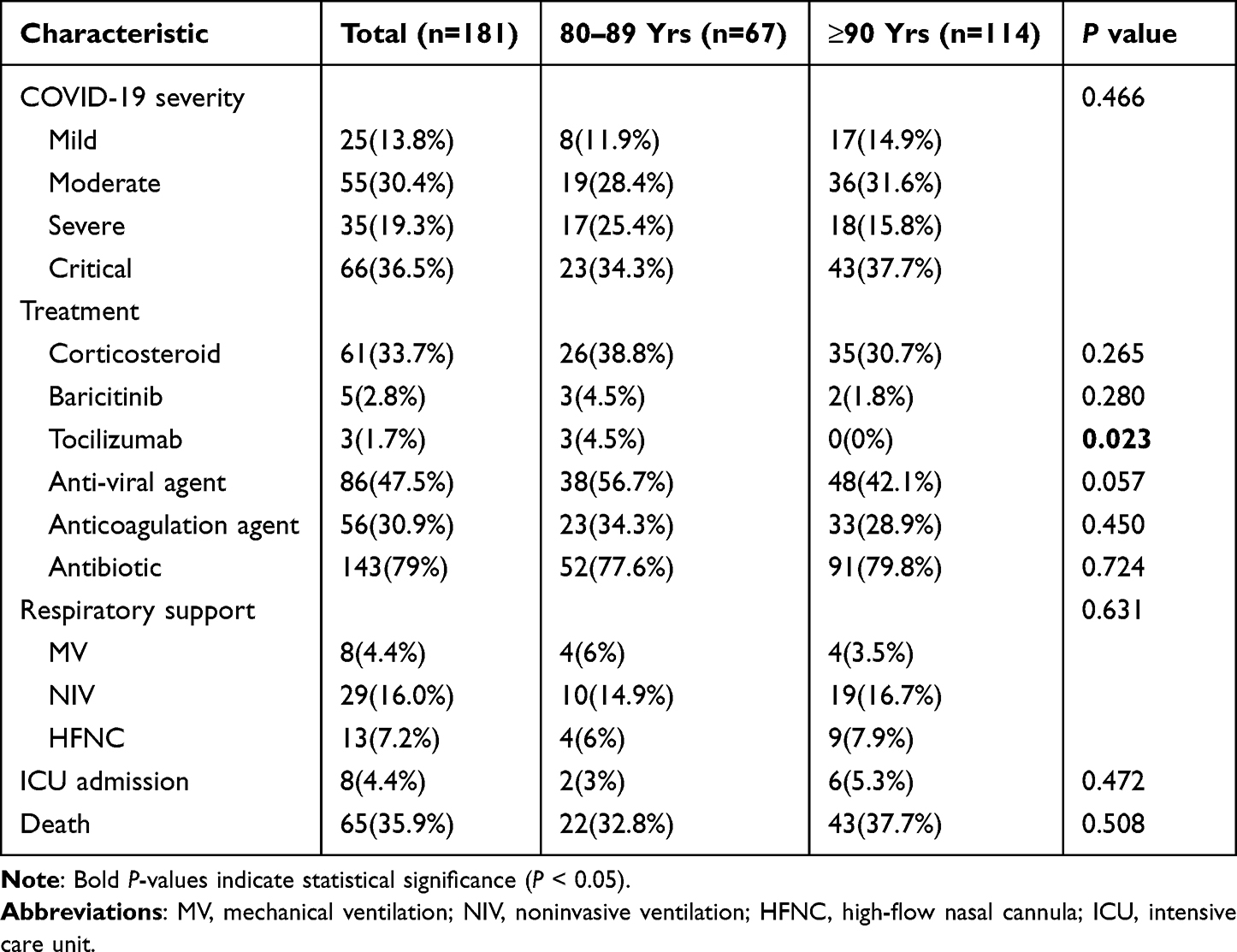 |
Table 2 Clinical Characteristics and Outcomes of Patients |
A total of 13 patients (7.2%) were treated with a high-flow nasal cannula, 29 (16.0%) received non-invasive ventilation, and 8 (4.4%) received mechanical ventilation in the ICU. The overall mortality rate was 35.9%, and was 37.7% in those 90-years-old or more and 32.8% in those 80 to 89-years-old. Tocilizumab use was significantly more common in the 80 to 89-year-old group (4.5% vs 0%, P = 0.023).
Factors Associated with Mortality
Sixty-five patients (35.9%) died within 30 days after hospital admission (Table 3). The univariate analysis showed that the survivors had a higher Barthel (ADL) score and were less likely to have a status of “dependence” (both P < 0.05). The survivors also had a lower pulse rate, and lower levels of white blood cells (WBCs), neutrophils, D-dimer, troponin T (TNT), pro-brain natriuretic peptide (Pro-BNP), and CRP (all P < 0.001). Survival was positively associated with antiviral treatment, but negatively associated with corticosteroid treatment (both P < 0.05). Only 9.2% of the patients who died received mechanical ventilation, but the survival rate was better for those who received no respiratory support (P < 0.001).
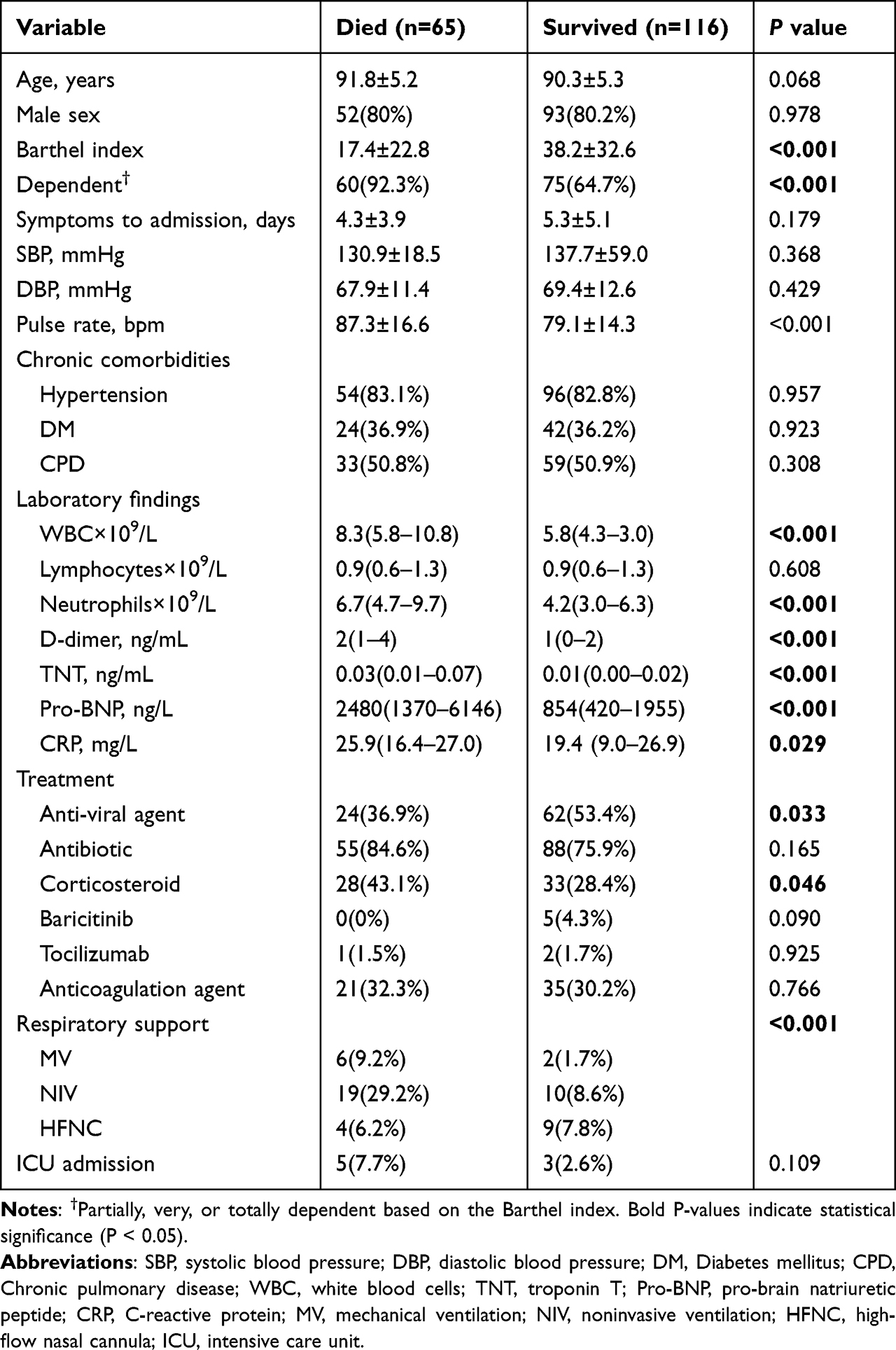 |
Table 3 Univariate Analysis of Factors Associated with 30-Day Patient Mortality |
The multivariate model showed that the Barthel (ADL) score (OR: 0.975; 95% CI, 0.962–0.989), SCr level (OR: 1.003; 95% CI, 1.000–1.006), WBC count (OR: 1.160; 95% CI, 1.056–1.276), D-dimer level (OR: 1.060; 95% CI, 1.009–1.113), and corticosteroid use (OR: 0.268; 95% CI, 0.124–0.582) were significantly and independently associated with 30-day mortality (Table 4).
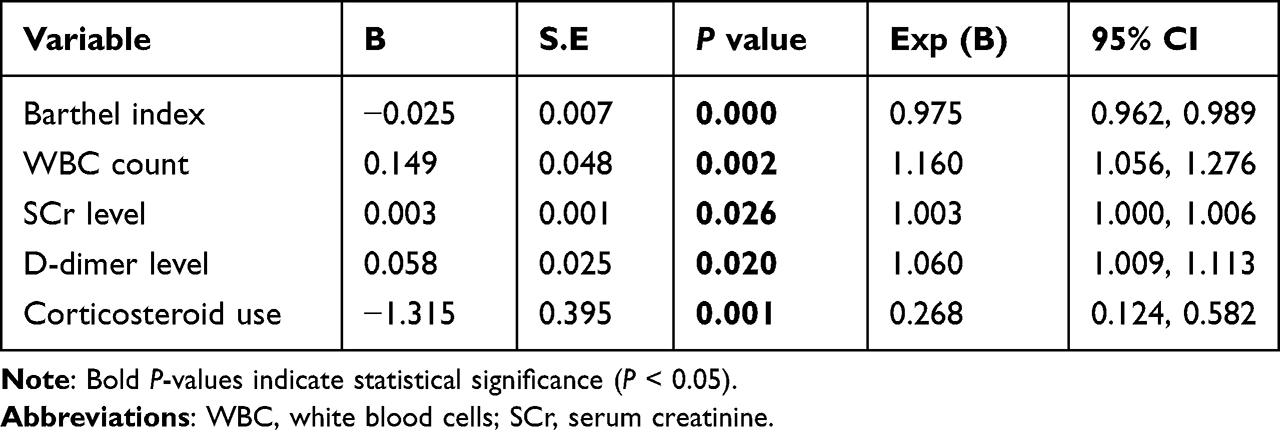 |
Table 4 Multivariable Analysis of Factors Associated with 30-Day Patient Mortality |
ROC analysis that used the combination of all five factors from the multivariate analysis indicated that the sensitivity was 0.578, the specificity was 0.862, and the AUC was 0.794 (95% CI: 0.727–0.861, P < 0.001; Figure 1A). However, the two age groups (80–89 years vs ≥90 years) had similar 30-day mortality rates (Log rank test: 0.417, Figure 1B).
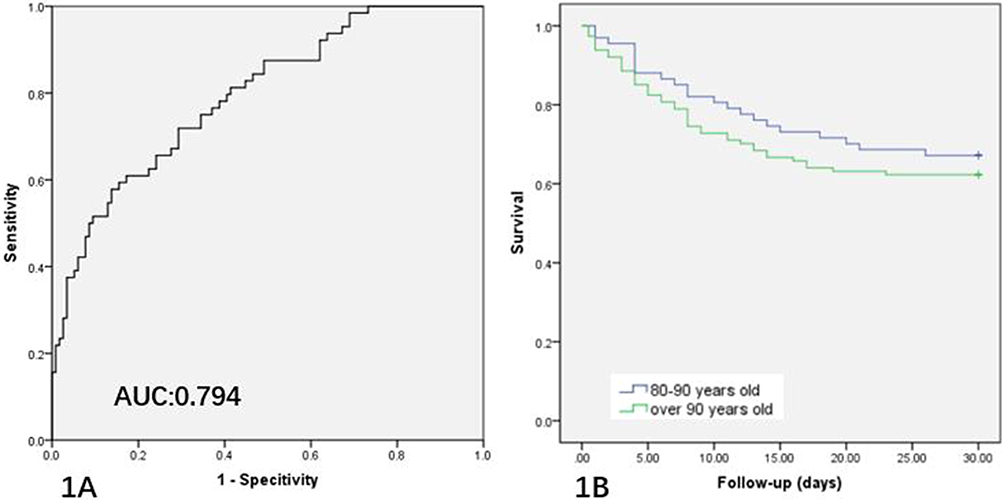 |
Figure 1 (A) Receiver operating characteristic (ROC) analysis of the multivariate model for predicting 30-day patient mortality (AUC: 0.794, 95% CI: 0.727–0.861, P < 0.001; sensitivity: 0.578; specificity: 0.862). (B) Kaplan-Meier survival analysis of the two age groups (80–89 years vs ≥90 years; Log rank test: 0.417). |
Discussion
This retrospective study of 181 very elderly patients with COVID-19 had three major findings. First, these patients had high incidences of mortality (35.9%) and comorbidities (especially hypertension [82.9%] and CHD [50.8%]), and 55% of them had severe or critical COVID-19 even though only 4.4% received mechanical ventilation. Second, compared with patients who were 80 to 90-years-old, those who were over 90-years-old had poorer immune function and nutritional status, but received similar treatments and respiratory support and had a similar 30-day mortality rate (32.8% vs 37.7%). Finally, we found that Barthel (ADL) score, SCr level, WBC count, D-dimer level, and corticosteroid use were significantly and independently associated with 30-day mortality.
Age is a significant factor that affects the susceptibility to COVID-19 and the prognosis of infected patients.8 A meta-analysis of 59 studies that examined 36,470 patients showed that patients aged 70 years or more appeared to have a 65% increased risk for COVID-19 (relative risk: 1.65, 95% CI: 1.50–1.81). Our study focused on the most vulnerable age group (very elderly patients) who were hospitalized with COVID-19, a population only rarely examined in previous clinical studies. The mortality rate among our very elderly patients was high (35.9%), and almost all of them had multiple comorbidities and low Barthel (ADL) scores. In our study, 55.8% of the patients had severe or critical disease, and 20.4% received non-invasive mechanical ventilation or ventilatory support. A weakened immune defense against infectious diseases, age-related chronic pro-inflammatory status, and persistent low-grade innate immune activation can increase the tissue damage caused by infections.9
Although comorbidities can contribute to a decrease in functional reserve and hinder the fight against infections, we found only a few differences between patients aged 80 to 90 years and those over 90 years. Patients over 90 years had higher rates of CHD and CPD than the younger group (72.8% vs 37.5%, P = 0.02; 15.8% vs 4.5%, P = 0.022, respectively). Additionally, our older group had a lower Barthel (ADL) score and a lower serum albumin level. However, our two age groups were similar in terms of pharmaceutical treatments and oxygen support, and they also had no significant difference in 30-day mortality (37.7% vs 32.8%, P = 0.508).
Notably, anti-viral agents, anticoagulants, and corticosteroids were given to less than half of our patients because of our limited experience in treating COVID-19 and insufficient medical resources at that time. Over time, with the accumulation of experience and resources, more patients received these treatments. Therefore, the mortality of our very elderly patients (35.9%) was less than reported for this age group during the first wave of the COVID-19 pandemic, from 25 February to 19 April 2020. Borobia et al investigated the first 2226 adult COVID-19 patients who were admitted to a single hospital in Spain during January 2020 and reported the mortality rate was 52.9% for those aged 80 to 89 years and 63.3% for those aged 90 years or more.7 Palaiodimos et al studied the first 200 COVID-19 patients who were admitted to an emergency room in New York City during March 2020 and reported the in-hospital mortality rate was 40% for those aged 74 years or more.8 Earlier use of oxygen therapy, improvements in general supportive care, and increased use of steroids, tocilizumab, or baricitinib might account for this improvement. Only 4.4% of our patients received mechanical ventilation, much lower than previously reported. For example, Alharthy et al3 studied critically ill COVID-19 patients and reported that 56.8% of them received mechanical ventilation. Another study reported a large age difference for those who did not and did receive mechanical ventilation (50.63 ± 13.3 vs 90.8 ± 5.3 years), and that most elderly patients selected palliative care. The high percentage of elderly patients receiving enhanced respiratory support and lower ventricular support is a reflection that this group of patients is more inclined to receive palliative care rather than more positive measures.
Previous research found that a lower Barthel (ADL) score was significantly related to higher mortality in COVID-19 patients.10 In agreement, we found that the percentage of patients with a low Barthel (ADL) score was much greater for patients who died (92.3% vs 64.7%). Frailty is another major risk factor for death from COVID-19, particularly in the elderly.11,12 Frailty is usually related to old age, poor ADL, and dementia. A previous study of COVID-19 patients identified the clinical frailty scale (CFS) as a potentially useful and practical tool to evaluate patient status, and reported that each 1-point increase in the CFS was associated with 12% increase in mortality (OR: 1.12, 95% CI = 1.04–1.20, P = 0.003).12
Prognostic factors may be useful for guiding patient stratification according to risk of severe disease or death. For example, we found that a high WBC count was related to mortality. Considering the possibility of bacterial co-infection in patients, 79% patients of our patients received antibiotics. A low lymphocyte count is one of the major characteristics of COVID-19 infection, and patients with severe COVID-19 pneumonia usually have bacterial co-infections. Previous research reported that deceased COVID-19 patients were more likely to have received antibiotics (84.6% vs 75.9%).13,14 Another study of 81 patients with COVID-19 reported that an elevated neutrophil-to-lymphocyte ratio (>9.8) was related to acute respiratory distress syndrome (ARDS) and was also related to receipt of non-mechanical and mechanical ventilation.15
An increased D-dimer level is an indication of thrombosis. Previous studies reported increased D-dimer and fibrinogen concentrations during the early stages of COVID-19, and that a 3- to 4-fold rise in the D-dimer level was linked to poor prognosis.16,17 An elevated D-dimer level is indicative of venous thromboembolisms, a condition that may lead to ventilation-perfusion mismatch. In addition, underlying conditions, such as diabetes, cancer, stroke, and pregnancy, may increase the D-dimer level in COVID-19 patients. Thus, measuring the level of D-dimer and coagulation parameters during the early stage of COVID-19 may help clinicians to provide better management of these patients. A study of 343 patients with COVID-19 showed that 12/67 patients with D-dimer levels of 2.0 μg/mL or more at admission died, but only 1/267 patients with D-dimer levels below 2.0 μg/mL died (P < 0.001; hazard ratio: 51.5; 95% CI, 12.9–206.7).18 Another study of COVID-19 patients found that a D-dimer level of 1.0 μg/mL or more on admission was associated with increased in-hospital mortality.19
Moreover, kidney damage, as indicated by a higher SCr level, also increases the risk of severe disease or death in patients with COVID-19.20,21 Although renal dysfunction may be indicative of systemic vascular and inflammatory complications, histopathologic analyses suggested the possibility that SARS-CoV-2 can directly infect the renal tubular epithelium.22 Our results showed that deceased patients were more likely to have used a corticosteroid (43.1% vs 28.4%, P = 0.046), presumably because patients with more severe disease are more likely to receive corticosteroid treatment.
Conclusions
In summary, our results confirmed that very elderly COVID-19 patients have a greatly increased risk for death. The Barthel (ADL) score, SCr level, WBC count, D-dimer level, and corticosteroid use were independently and significantly related to 30-day mortality, and use of these variables in ROC analysis led to an AUC value of 0.794. Our results might help future researchers to develop multivariable prognostic models that could facilitate decision-making for very elderly COVID-19 patients.
Our study has some limitations. Firstly, all data were from one hospital in Beijing, so the findings may not be generalizable to other populations. Secondly, we only performed follow-up for 30 days, and the mortality rate might be greater for longer follow-up periods. Thirdly, we did not investigate the effect of vaccination on survival. Finally, genetic factors could play a role in senility and in the course of COVID-19 progression. A future study that examines the effects of different genetic variants on the severity of COVID-19 in very elderly patients would provide important information that could aide in combating this disease in this highly vulnerable population.
Acknowledgments
This research was supported by the National Key R&D Program of China (2021ZD0111000).
Disclosure
No potential conflict of interest relevant to this article was reported.
References
1. Bonanad C, García-Blas S, Tarazona-Santabalbina F, et al. The effect of age on mortality in patients with COVID-19: a meta-analysis with 611,583 subjects. J Am Med Dir Assoc. 2020;21(7):915–918. doi:10.1016/j.jamda.2020.05.045
2. Wu C, Chen X, Cai Y, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med. 2020;180(7):934–943. doi:10.1001/jamainternmed.2020.0994
3. National Institutes of Health. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available from: https://www.covid19treatmentguidelines.nih.gov/.
4. Chen Y, Klein SL, Garibaldi BT, et al. Aging in COVID-19: vulnerability, immunity and intervention. Ageing Res Rev. 2021;65:101205. doi:10.1016/j.arr.2020.101205
5. Alharthy A, Aletreby W, Faqihi F, et al. Clinical characteristics and predictors of 28-day mortality in 352 critically ill patients with COVID-19: a retrospective study. J Epidemiol Glob Health. 2020;11(1):98–104. doi:10.2991/jegh.k.200928.001
6. 中华人民共和国国家卫生健康委员会办公厅, 中华人民共和国国家中医药管理局综合司 [General Office of National Health Commission of the People's Republic of China]. 新型冠状病毒感染诊疗方案(试行第十版) [Diagnosis and treatment of the coronavirus disease 2019 (the 10th version)]. 中国医药. 2023;18(2):161–166.
7. Coronavirus disease 2019 (COVID-19) treatment guidelines. Available from: https://www.covid19treatmentguidelines.nih.gov/.
8. Ayoub HH, Chemaitelly H, Mumtaz GR, et al. Characterizing key attributes of COVID-19 transmission dynamics in China’s original outbreak: model-based estimations. Glob Epidemiol. 2020;2:100042. doi:10.1016/j.gloepi.2020.100042
9. Shaw AC, Joshi S, Greenwood H, Panda A, Lord JM. Aging of the innate immune system. Curr Opin Immunol. 2010;22:507–513. doi:10.1016/j.coi.2010.05.003
10. Da Costa JC, Manso MC, Gregório S, Leite M, Pinto JM. Barthel’s index: a better predictor for COVID-19 mortality than comorbidities. Tuberc Respir Dis. 2022;85(4):349–357. doi:10.4046/trd.2022.0006
11. Zhang XM, Jiao J, Cao J, et al. Frailty as a predictor of mortality among patients with COVID-19: a systematic review and meta-analysis. BMC Geriatr. 2021;21:186. doi:10.1186/s12877-021-02138-5
12. Pranata R, Henrina J, Lim MA, et al. Clinical frailty scale and mortality in COVID-19: a systematic review and dose-response meta-analysis. Arch Gerontol Geriatr. 2021;93:104324. doi:10.1016/j.archger.2020.104324
13. Paula HSC, Santiago SB, Araújo LA, et al. An overview on the current available treatment for COVID-19 and the impact of antibiotic administration during the pandemic. Braz J Med Biol Res. 2021;55:e11631. doi:10.1590/1414-431x2021e11631
14. Gallo Marin B, Aghagoli G, Lavine K, et al. Predictors of COVID-19 severity: a literature review. Rev Med Virol. 2021;31(1):1–10. PMID: 32845042; PMCID: PMC7855377. doi:10.1002/rmv.2146
15. Ma A, Cheng J, Yang J, Dong M, Liao X, Kang Y. Neutrophil-to-lymphocyte ratio as a predictive biomarker for moderate-severe ARDS in severe COVID-19 patients. Crit Care. 2020;24(1):288. doi:10.1186/s13054-020-03007-0
16. Rostami M, Mansouritorghabeh H. D-dimer level in COVID-19 infection: a systematic review. Expert Rev Hematol. 2020;13(11):1265–1275. doi:10.1080/17474086.2020.1831383
17. Zhan H, Chen H, Liu C, et al. Diagnostic value of D-dimer in COVID-19: a meta-analysis and meta-regression. Clin Appl Thromb Hemost. 2021;27:10760296211010976. doi:10.1177/10760296211010976
18. Zhang L, Yan X, Fan Q, et al. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19. J Thromb Haemost. 2020;18(6):1324–1329. doi:10.1111/jth.14859
19. Docherty AB, Harrison EM, Green CA, et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO clinical characterisation protocol: prospective observational cohort study. BMJ. 2020;369:m1985. doi:10.1136/bmj.m1985
20. Izcovich A, Ragusa MA, Tortosa F, et al. Prognostic factors for severity and mortality in patients infected with COVID-19: a systematic review. PLoS One. 2020;15(11):e0241955. doi:10.1371/journal.pone.0241955
21. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
22. Cheng Y, Luo R, Wang K, et al. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020;97(5):829–838. doi:10.1016/j.kint.2020.03.005
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 Case Fatality Rate and Factors Contributing to Mortality in Ethiopia: A Systematic Review of Current Evidence
Girma D, Dejene H, Adugna L, Tesema M, Awol M
Infection and Drug Resistance 2022, 15:3491-3501
Published Date: 4 July 2022
Remdesivir Reduces Mortality in Hemato-Oncology Patients with COVID-19
Aksak-Wąs BJ, Chober D, Serwin K, Scheibe K, Niścigorska-Olsen J, Niedźwiedź A, Dobrowolska M, Żybul K, Kubacka M, Zimoń A, Hołda E, Mieżyńska-Kurtycz J, Gryczman M, Jamro G, Szakoła P, Parczewski M
Journal of Inflammation Research 2022, 15:4907-4920
Published Date: 25 August 2022
Mortality Risk Factors of Early Neonatal Sepsis During COVID-19 Pandemic
Kolesnichenko SI, Kadyrova IA, Lavrinenko AV, Zhumadilova ZA, Avdienko OV, Vinogradskaya YV, Fominykh YA, Panibratec LG, Akhmaltdinova LL
Infection and Drug Resistance 2022, 15:6307-6316
Published Date: 31 October 2022
Platelet-to-White Blood Cell Ratio as a Predictor of Mortality in Patients with Severe COVID-19 Pneumonia: A Retrospective Cohort Study
Thungthienthong M, Vattanavanit V
Infection and Drug Resistance 2023, 16:445-455
Published Date: 24 January 2023
Neutrophil/Lymphocyte Ratio (NLR) and Lymphocyte/Monocyte Ratio (LMR) – Risk of Death Inflammatory Biomarkers in Patients with COVID-19
Dymicka-Piekarska V, Dorf J, Milewska A, Łukaszyk M, Kosidło JW, Kamińska J, Wolszczak-Biedrzycka B, Naumnik W
Journal of Inflammation Research 2023, 16:2209-2222
Published Date: 23 May 2023