")
Back to Journals » Journal of Healthcare Leadership » Volume 14
Values-Based Leadership: A Survey of Academic Medical Leaders to Inform Curriculum Development
Authors Antoine EB , Rocha AM, McGinty G
Received 24 June 2022
Accepted for publication 13 September 2022
Published 19 September 2022 Volume 2022:14 Pages 137—142
DOI https://doi.org/10.2147/JHL.S379737
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pavani Rangachari
Emma B Antoine,1 Arelys M Rocha,2 Geraldine McGinty3
1School of Public Policy, Cornell University Graduate School, Ithaca, NY, USA; 2Department of Population Health Sciences, Weill Cornell Graduate School of Medical Sciences, New York, NY, USA; 3Departments of Radiology and Population Health Sciences, Weill Cornell Medicine, New York, NY, USA
Correspondence: Geraldine McGinty, Departments of Radiology and Population Health Sciences, Weill Cornell Medicine, 1300 York Avenue, Ste F-100, New York, NY, 10021, USA, Tel +1 646 962 5952, Fax +1 212 746 8424, Email [email protected]
Purpose: The COVID-19 pandemic highlighted the importance of effective leaders across all spheres but especially in healthcare. Many Academic Medical Centers (AMCs) offer leadership programming, but these programs have been criticized for lacking impact. In developing a Master’s-level leadership course at an AMC, we sought to inform the curriculum with the values, both personal and shared, as well as the competencies defined as essential by a group of leaders who successfully steered their organizations through the pandemic.
Methods: Study participants included selected leaders from a medical school, its hospital partner and parent university. We used a combination of semi-structured interviews, conducted virtually, and a rank-order survey to identify values and competencies to be used to inform course content.
Results: Our surveyed leaders relied on personal values that prioritized the organization’s mission, aligning their teams around that mission and vision as well as leading with empathy and respect. As a group, these leaders valued a highly collegial and collaborative process as well as diversity and equity. Competencies essential to leadership, according to our participants, were the ability to create the environment that supports collaboration, including team development, and to uphold the organization’s mission.
Conclusion: The surveyed leaders’ organizations treated some of the highest numbers of COVID-19 patients of any hospital system and needed to make difficult decisions in order to provide patient care safely. Study participants were therefore uniquely experienced health care system leaders currently meeting unprecedented challenges. Our study suggests that applying a values-based approach to the development of future leaders will positively influence the impact of leadership education in a Master’s-level healthcare leadership program.
Keywords: healthcare, education, competency, pandemic
Introduction
Most health systems and large companies offer professional development programming to emerging leaders in the organization,1 with some academic medical centers offering more formal business education. These programs have been described as “not [being] based on theoretical grounding [and with] a narrow focus on cognitive domains”.2 It remains unclear when evaluating these kinds of programs which contained elements contribute positively to the development of improved healthcare leadership. Previous work has suggested that “programs can improve by basing content on a leadership competency model”.1 Lucas et al also state that
Physician LDPs [Leadership Development Programs] have demonstrated only modest impact on outcomes important to AHCs [Academic Health Centers] and that more rigorous program evaluation is needed.
The COVID-19 pandemic starkly highlighted the importance of effective leaders across all spheres but especially in healthcare.3 This provided a unique opportunity to gain insights into the personal and shared values of our healthcare organizations’ leaders during a time of stress, the protracted second wave of the COVID-19 pandemic in New York City. We sought to identify the specific factors that those leaders found to be essential competencies for effective leadership. To allow these insights to inform future leaders, we propose to embed the values and competencies within an institutional healthcare leadership curriculum.
Materials and Methods
Study Design
This was a mixed method study that incorporated qualitative and quantitative processes to thematically categorize personal leadership values, shared leadership values and core competencies needed by healthcare leaders. We obtained Weill Cornell Medicine’s (WCM).
Institutional Review Board (IRB) approval prior to conducting any human subjects research. All participants provided informed consent. The two-part study was conducted over a period of three months. The first part of the study included conducting semi-structured interviews. Due to the pandemic and social distancing efforts, the interviews were conducted virtually (Zoom.us (San Jose, CA)) during the months of February to March 2021.
Two months later, all participants were invited to complete a rank-order survey for their personal leadership values, shared leadership values, and core competencies using Qualtrics XM (Qualtrics (Seattle, WA). Upon completion of the rank-order survey, the participants completed their participation in the study.
Interviews
Twenty-five leaders were identified across the WCM, New York Presbyterian Hospital (NYPH), and Cornell University (CU) systems. These leaders were chosen because, through their operational or governance roles, they had played a key role in the response to the COVID-19 pandemic. The leaders surveyed included Deans, Academic Chairs, and non-physician administrative leaders. Three invitees did not respond, we were unable to successfully schedule interviews with two additional invitees, and one declined the interview. The remaining 19 interviewees comprised 11 men and 8 women and included 12 physicians. We conducted approximately 30-minute, semi-structured interviews. Due to the pandemic and social distancing guidelines, interviews were conducted virtually using Zoom (Zoom.us, San Jose CA) and were recorded with the permission of the interviewees. Each interview included three central questions: (1) what are your personal leadership values or what values inform your leadership; (2) what do you think are the shared values and culture of the leadership at WCM/NYPH; and (3) what are the competencies that you think are necessary for effective healthcare leaders? Using an online, automated, third-party transcription tool (Rev.com (San Francisco, CA)), we transcribed the interviews into manuscripts. Each manuscript was coded (using the online tool from Dedoose.com, Hermosa Beach, CA) based on thematic considerations that the authors derived from the participants’ responses for their own personal leadership values, perceived shared leadership values, and competencies for healthcare leaders. No value or competency was assigned a higher weight than any other. Using the relative frequency of their appearing in the transcripts, the top ten themes for each category: personal leadership values, shared leadership values, and core competencies of healthcare leaders were then extracted from the manuscripts.
Rank-Order Survey
Next, we conducted a rank-order survey, followed by analysis and interpretation. Participants were asked to rank the top 10 attributes for each question pertaining to personal leadership values, shared values, and core competencies of effective healthcare leaders. The summation of ranked placement per attribute was taken in order to derive the relative placement of each attribute per question. Participants were given sufficient time to complete the survey at their leisure. Twelve of the interviewees completed the survey.
Results
Analysis of the coded transcripts yielded a set of 30 data elements, ten for each line of enquiry, that informed the rank order survey. In Table 1 we show the results of the semi-structured interviews, revealing the most common themes that were elicited by the three questions heading each column. These results were used as the input for the surveys subsequently administered to the study participants. The themes are listed in the order that they were ranked by the survey participants with the most highly ranked listed first. The primary data are also available as a PDF in the Supplementary Data.
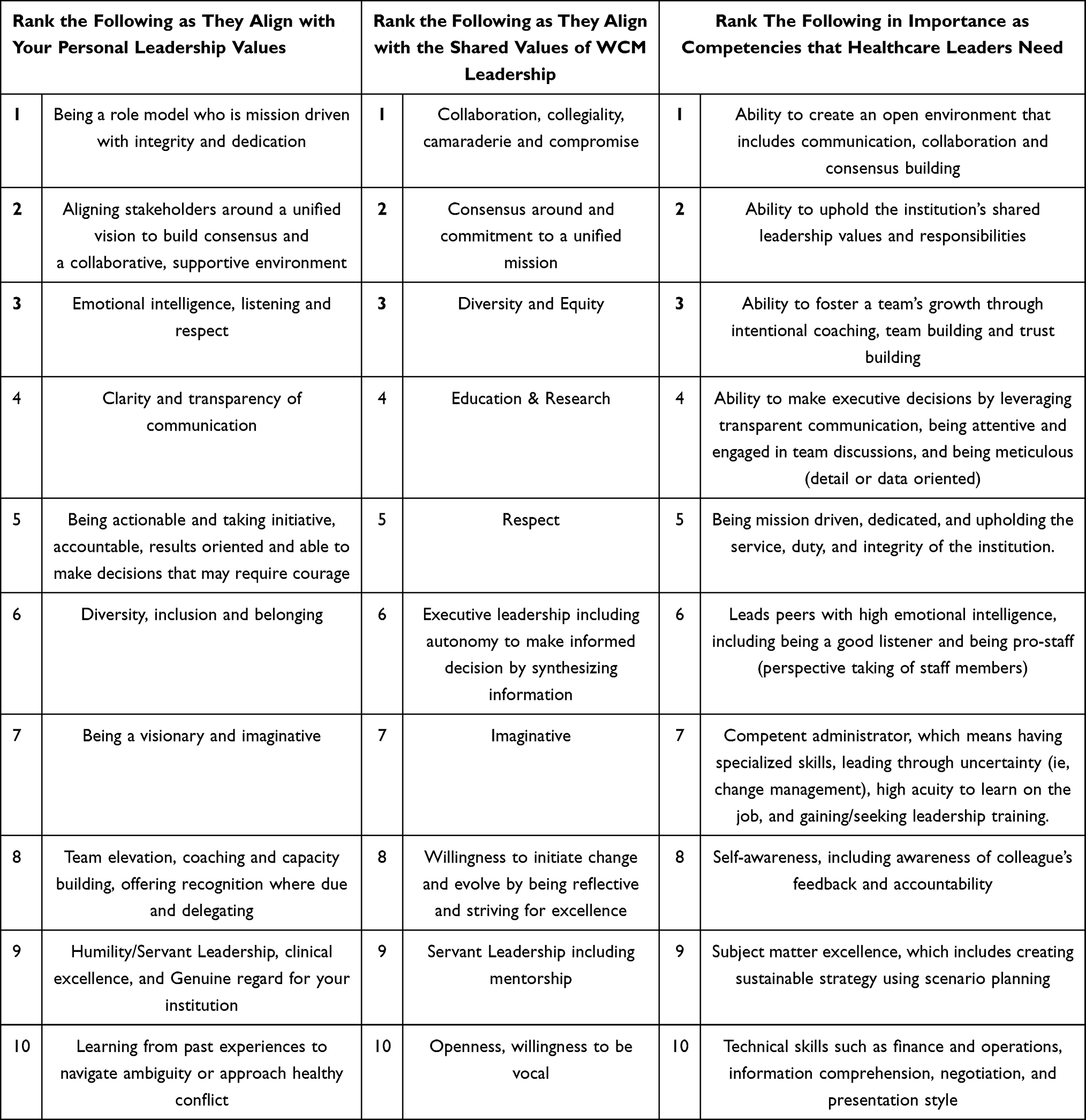 |
Table 1 Ranked Survey Results |
Discussion
Our study identified three areas of confluence across the surveyed leaders’ personal and shared values, and the competencies that they identified to be important for effective leaders. These centered on the mission of the organization, the processes by which the organization executes its mission, and the optimal engagement of people within the organization.
The importance of a shared vision and mission was clear in the rankings for both personal and shared leadership values, and the ability to execute around that mission were seen as an important competency for leaders. The participants’ most highly ranked personal value was to be “a role model who is mission-driven with integrity and dedication” and “to align stakeholders around (that) unified vision to build consensus”, while challenging themselves to be competent to “uphold the institution’s shared leadership values and responsibilities”. The leaders also valued the process involved in the creation of a unified vision. The desirable foundation for this process was proposed to include “collaboration, collegiality, camaraderie, and compromise”, while being competent in creating a “supportive environment (underpinned by) emotional intelligence, listening and respect”. Diversity and equity were identified as key shared organizational values. Highly ranked personal values of emotional intelligence and respect, and the associated competency to “foster a team’s growth through intentional coaching, team building, and trust building” aligns with this organizational shared culture.
Unexpected/Surprising Results
Technical skills such as such as negotiations, strategy, financial acumen, and subject matter expertise (including clinical expertise) were identified as important competencies, but they were not as highly ranked as skills that might be considered “soft”, such as team building.4 In an AMC environment, such subject matter expertise might have been assumed, and have caused these valuable skills to be less highly ranked in our surveys.
In 2003, a report commissioned by the Institute of Medicine titled “Health professions education: A bridge to quality” opined that “Evaluation of the effects of health professions education requires increased attention”.5 Among the extensive body of literature on healthcare leadership,6–10 our review found a paucity of work on the elements of a curriculum that would underpin an effective outcomes-driven program. Hargett et al used similar methods to inform curriculum development at the undergraduate and graduate medical education levels.11 Our work focused on a Master’s-level curriculum designed for mid-career professionals already in leadership roles and, uniquely, leveraged the experience of senior leaders at a time of unprecedented crisis.
Strengths
Our research was conducted during the protracted second wave of the COVID-19 pandemic in New York City. Leaders across our organizations made unprecedented decisions in order to provide patient care safely while treating some of the highest numbers of COVID-19 individuals of any health system. For example, elective care was shut down for several months, causing a significant revenue loss. A decision to briefly bar the presence of laboring mothers’ partners and families from the delivery room attracted significant negative press coverage as well as intervention by the State’s Governor.12 Policies had to be created around requirements for staff vaccination, including management of those who declined to be vaccinated. Our study participants were therefore uniquely experienced health system leaders who were currently meeting the major challenges of a global pandemic. Reflecting on the leadership challenges presented by the COVID-19 pandemic, Stoller observed that
Overall, a crisis heightens the need for great leadership and underscores needed leadership competencies, both through success in their presence and through failure in their absence.13
Limitations
Our sample size was small. Therefore, the study was not powered for discovery with assessment of the statistical significance of results. The majority of those interviewed were physicians, which may not be typical for other healthcare organizations.
Implications Plus Further Research
Despite the return to greater normality, the future remains uncertain. The pace of economic recovery, the impact of COVID variants and pressure to increase value in healthcare will continue to test all healthcare leaders’ resilience. At the same time, those leaders must support a culture of innovation in care delivery, research and education. The lessons learned by those who led a large health system during a time of extreme crisis can be used to inform the development of their successors as effective leaders. We intend to use the elements identified in our survey to create a values-based model of healthcare leadership in a refreshed curriculum for an institutional healthcare leadership course, focusing on teaching the key competencies identified in this study, to maintain an institutional memory of the lessons learned during the pandemic.
Conclusion
Effective healthcare leadership is critical to the health and safety of our global population. Significant extant investment in developing the healthcare leaders of the future may not provide the return we expect if the programming does not incorporate critical concepts and competencies.11 We must ensure that our curricula are effective in delivering those concepts within a model that is compelling and based in the real-world experience of successful organizations. This project to discover the values, both personal and shared, of a group of leaders who steered an academic medical center through a global pandemic, as well as the competencies that underpinned their performance, will inform our curriculum development process as we seek to guide emerging leaders in their professional development journey.
Abbreviations
AHC, Academic Health Centers; AMC, Academic Medical Centers; CU, Cornell University; IRB, Institutional Review Board; LDP; Leadership Development Programs, MBA, Masters in Business Administration, NYC, New York City; NYPH, New York-Presbyterian Hospital; WCM, Weill Cornell Medicine.
Data Sharing Statement
The terms of the IRB protocol required that recordings, transcripts and all other records be destroyed at the conclusion of the study. There are no data and materials to share.
Ethics Approval and Consent to Participate
Ethical approval has been granted for studies involving human subjects by Institutional Review
Board at the Weill Cornell Medicine, protocol number 20-09022632, date January 25 2021.
Consent for Publication
The study consent includes publication of the study results.
Acknowledgments
The authors wish to thank the leaders at Weill Cornell Medicine and the New York Presbyterian Hospital and Cornell University for their participation in this study as well as Dr. Erika Abramson who provided valuable guidance on the survey structure.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by internal funding from the Department of Population Health Sciences at Weill Cornell Medicine, New York NY.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lucas R, Goldman EF, Scott AR, Dandar V. Leadership development programs at academic health centers: results of a national survey. Acad Med. 2018;93(2):229–236. doi:10.1097/ACM.0000000000001813
2. Sultan N, Torti J, Haddara W, Inayat A, Inayat H, Lingard L. Leadership development in postgraduate medical education: a systematic review of the literature. Acad Med. 2019;94(3):440–449. doi:10.1097/ACM.0000000000002503
3. Kevin W, Lobdell MD. Improving Health Care Leadership in the Covid-19 Era | catalyst non-issue content; 2020. Available from: https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0225.
4. Matteson ML, Anderson L, Boyden C. “soft skills”: a phrase in search of meaning. Portal. 2016;16(1):71–88. doi:10.1353/pla.2016.0009
5. Greiner AC, Knebel E. Health Professions Education: A Bridge to Quality. Washington (DC): National Academies Press (US); 2003. doi:10.17226/10681
6. Lee TH. Turning doctors into leaders. Harv Bus Rev. 2010;88(4):50–58.
7. Scott ES. Perspectives on healthcare leader and leadership development. JHL. 2010;83. doi:10.2147/JHL.S8292
8. Bhardwaj A. Organizational culture and effective leadership in academic medical institutions. J Healthc Leadersh. 2022;14:25–30. doi:10.2147/JHL.S358414
9. Brownfield E, Cole DJ, Segal RL, et al. Leadership development in academic health science centers: towards a paradigm shift. J Healthc Leadersh. 2020;12:135–142. doi:10.2147/JHL.S263533
10. Lerman C, Jameson JL. Leadership development in medicine. N Engl J Med. 2018;378(20):1862–1863. doi:10.1056/NEJMp1801610
11. Hargett CW, Doty JP, Hauck JN, et al. Developing a model for effective leadership in healthcare: a concept mapping approach. J Healthc Leadersh. 2017;9:69–78. doi:10.2147/JHL.S141664
12. ‘Women Will Not Be Forced to Be Alone When They Are Giving Birth’ - The New York Times. Available from: https://www.nytimes.com/2020/03/28/parenting/nyc-coronavirus-hospitals-visitorslabor.html.
13. Stoller JK. Reflections on leadership in the time of COVID-19. leader. 2020;leader2020–000244. doi:10.1136/leader-2020-000244
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.