Back to Journals » Clinical Epidemiology » Volume 17
Validity of the Leading Causes of Death Classification for Premature Mortality in Inflammatory Bowel Disease: A Population-Based Comparison with ICD-10 Coding in Ontario, Canada
Authors Postill G ![]() , Kuenzig ME
, Kuenzig ME ![]() , Olivera PA, Itanyi IU, Harish V, Tang F, Buajitti E, Rosella LC, Benchimol EI
, Olivera PA, Itanyi IU, Harish V, Tang F, Buajitti E, Rosella LC, Benchimol EI ![]()
Received 10 June 2025
Accepted for publication 11 December 2025
Published 28 December 2025 Volume 2025:17 Pages 1163—1175
DOI https://doi.org/10.2147/CLEP.S546090
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Henrik Toft Sørensen
Gemma Postill,1– 5 M Ellen Kuenzig,3,4,6 Pablo A Olivera,1,7,8 Ijeoma Uchenna Itanyi,9 Vinyas Harish,1,2 Furong Tang,4,5 Emmalin Buajitti,5,9,10 Laura C Rosella,1,6,9,11 Eric I Benchimol1– 5,12
1Institute of Health Policy, Management and Evaluation, Dalla Lana School of Public Health, University of Toronto, Toronto, ON, Canada; 2Temerty Faculty of Medicine, University of Toronto, Toronto, ON, Canada; 3SickKids Inflammatory Bowel Disease Centre, Division of Gastroenterology, Hepatology and Nutrition, Department of Paediatrics, The Hospital for Sick Children, Toronto, ON, Canada; 4Child Health Evaluative Sciences, SickKids Research Institute, The Hospital for Sick Children, Toronto, ON, Canada; 5ICES, Toronto, ON, Canada; 6Departments of Paediatrics, Epidemiology and Biostatistics, Schulich School of Medicine and Dentistry, Western University, London, ON, Canada; 7Zane Cohen Centre for Digestive Diseases, Lunenfeld-Tanenbaum Research Institute, Sinai Health System, Toronto, ON, Canada; 8Division of Gastroenterology, Mount Sinai Hospital, University of Toronto, Toronto, ON, Canada; 9Department of Public Health Sciences, Dalla Lana School of Public Health, University of Toronto, Toronto, ON, Canada; 10Department of Epidemiology, Biostatistics and Occupational Health, McGill University, Montreal, Canada; 11Institute for Better Health, Trillium Health Partners, Mississauga, ON, Canada; 12Department of Paediatrics, University of Toronto, Toronto, ON, Canada
Correspondence: Eric I Benchimol, Division of Gastroenterology, Hepatology and Nutrition, The Hospital for Sick Children, 555 University Ave, Toronto, ON, M5G 1X8, Canada, Email [email protected]
Introduction: Studying patterns of death, particularly premature deaths (< 75 years), provides insights to address health inequities among those living. Multiple coding systems for cause of death (COD) exist. The Leading Causes of Death (LCD) scheme is designed for identifying priority COD for interventions in global populations. The extent to which such classification is effective for identifying priority causes of premature mortality among subpopulations with chronic health conditions, such as inflammatory bowel disease (IBD), is unknown.
Objective: To evaluate the usability of the LCD for characterizing premature mortality among those with IBD.
Methods: We conducted a population-based matched case control study of persons with IBD who died between 2010 and 2018 using linked health administrative data from Ontario, Canada. Individuals with IBD were matched with five decedents without IBD based on sex and years of birth and death. We compared COD for premature and overall mortality using two classification structures: the LCD scheme and the International Statistical Classification of Diseases and Related Health Problems, tenth revision (ICD-10) chapters.
Results: Among 7,919 decedents with IBD (39,414 matched controls), 47% died prematurely. With the LCD framework, COD differences for premature mortality were not detectable as 29% were allocated to the residual category (Standardized differences [SD]: 18%). Most residual deaths were due to neoplasms (34%) or diseases of the gastrointestinal system (32%). Using ICD-10 chapters, premature deaths were more commonly due to diseases of the digestive system than for matched controls (13% vs 5%, SD: 31%).
Discussion: The LCD coding scheme provides more granular COD details compared to the ICD-10 chapters. However, a larger proportion of deaths among people with IBD were allocated to the residual category, limiting its utility for enabling healthcare systems to identify priority targets to reduce premature mortality. Further work to develop and validate a framework for premature COD classification in populations with IBD is needed.
Keywords: premature death, health administrative data, diagnostic codes, death categorization, Crohn’s disease, ulcerative colitis
Introduction
Studying patterns of death at the population level provides critical insights for identifying and addressing health inequities among those living. In Canada, premature mortality – defined by Statistics Canada and the Canadian Institute for Health Information (CIHI) as deaths before 75 years of age – is a key indicator used in both research and national surveillance to monitor health system performance.1,2 Premature mortality is used as a measure of avoidable mortality, emphasizing that deaths before age 75 years are predominantly preventable through public health and primary prevention efforts or treatable through timely and effective healthcare.2–6 Individuals with chronic diseases or multimorbidity (2+ chronic conditions) represent a key population in premature mortality research, as premature deaths within these groups often reflect gaps in disease management, access to care, or treatment optimization.
Evaluating causes of premature mortality is important for identifying and prioritizing needed health interventions. However, little consensus exists on how to categorize and compare causes of premature mortality in subpopulations with chronic diseases. Cause of death (COD) reporting is commonly based on the International Classification of Diseases (ICD) coding system (often simplified into ICD Chapters). The Leading Causes of Death (LCD) framework is a derived categorization that reclassifies ICD-coded causes into a list of common COD globally, grouping less frequent causes into a residual category.7 This approach aims to provide greater specificity in reporting COD than ICD-10 chapters to better identify priority COD for interventions. However, the LCD scheme was derived on all-deaths (vs premature mortality) in a global setting (vs in populations with high burdens of multimorbidity). Determining its construct validity and usability for evaluating premature COD in populations with multimorbidity is needed to inform how health systems should monitor premature mortality to identify health disparities and improve population health.
Inflammatory bowel disease (IBD) is a group of chronic inflammatory disorders primarily affecting the gastrointestinal tract, including Crohn’s disease and ulcerative colitis. The prevalence of multimorbidity and of premature mortality among those with IBD is higher compared to the general population.8 Indeed, life expectancy and health-adjusted life expectancy are 5–8 years lower in people with IBD.9,10 Our objective was to evaluate the construct validity and usability of the LCD for characterizing overall and premature mortality in populations with IBD. Such study has direct applications for guiding how healthcare systems identify causes of, and subsequently prevent, premature mortality in populations with chronic conditions.
Materials and Methods
Study Design and Data Sources
We conducted a retrospective, population-based matched case control study using health administrative and population data from Ontario, Canada’s most populous province. Canada has one of the highest incidence and prevalence of IBD globally; 1 in 91 Canadians are forecasted to be living with IBD by 2035.11,12 The data used are housed at ICES for residents of Ontario eligible for its universal healthcare coverage at any point since April 1991 (>99% of the population). ICES is a prescribed entity under section 45 of Ontario’s Personal Health Information Protection Act, allowing it to collect and analyze health care and demographic data, without additional consent, for health system evaluation and improvement. The use of data in this project was authorized under section 45 and did not require additional informed consent nor ethics approval. Data are available in an uncleaned, unedited format to researchers and data analysts.
The linked ICES datasets used were the Registered Persons Database (RPDB), the Ontario Crohn’s and Colitis Cohort (OCCC), the Office of the Registrar General-Deaths databases (ORG-D), the Census, and the 2016 Ontario Marginalization Index (ON-Marg). Datasets were deterministically linked using unique encoded identifiers based on encrypted health card number and analyzed at ICES. All data were de-identified prior to access.
Study Population
The study population included decedents with IBD residing in Ontario, Canada at death, with death dates between January 1, 2010, and December 31, 2018, inclusively (Supplemental Figure A). Diagnosis of IBD was identified from the OCCC using validated age-specific algorithms applied to inpatient hospitalization records, same-day surgery records, physician billing claims, and medication data (Supplemental Table A).13,14 All individuals who met the case definition for prevalent IBD since 1991 (date of earliest data) were included. We matched eligible decedents with IBD with up to 5 decedents without IBD from the general population (captured in RPDB) at random, based on exact matches of sex, year of birth, and year of death. We excluded decedents with an invalid health card or missing age of death, date of death, or COD (Supplemental Figure A).
Outcome
The primary outcome of interest was COD (captured in the ORG-D), derived from the Medical Certificate of Death. The RPDB was linked to the ORG-D with an overall linkage success rate of 96.5%.15 Cause of death was coded using two approaches: (1) Becker’s LCD7 (Supplemental Table B) and (2) the International Statistical Classification of Diseases and Related Health Problems, tenth revision (ICD-10) chapters. In the ICD-10 framework, individual codes are combined into buckets which are then combined into chapters based on anatomy. We combined ICD-10 chapters with counts of <6 persons when stratified by premature death into an “Other” category (Supplemental Table C).
Premature Death
In Canada, premature mortality is defined as any death before age 75 years.2,16,17 Such definition is also widely used in the literature.2,4 In Ontario, 37% of all deaths between 2018 and 2022 occurred prematurely.18
Sociodemographic Characteristics
We captured area-based sociodemographic measures (quintiles of income, material resources and education, as well as rurality score) using Census data based on postal code at death. Area-level measures were applied to individual decedents according to their residential dissemination area, the smallest geographic area for which census data are reported.19 Material resources (captured in ON-Marg) is derived from data on unemployment, education, income, and dwellings in need of repair (among other data),19 and is the domain of ON-Marg most strongly associated with health outcomes.20 Rurality was defined using the Rurality Index of Ontario (RIO 2008) scores with scores ≥40 indicating rural residency.21
Statistical Analyses
We summarized characteristics of the cohort, stratified by decedents’ IBD status. The frequency and proportion for each COD among people with and without IBD were reported using both classification systems, for all deaths and then stratified by premature death (<75 years).2,4 Within the ICD-10 digestive disease chapter, we also examined prevalence across the ten pre-specified ICD-10 cause buckets (Supplemental Table D). Standardized differences (SD) were used to compare the relative prevalences of each COD among those with and without IBD, with a priori defined SD >10% indicating meaningful differences (a threshold equivalent to having a phi coefficient of 0.05).22 We used SD because of the cohort size; statistical measures of tendency are not as useful as p-values are sensitive and often misleading in larger samples.
To assess consistency between the LCD-coding system and ICD-10 chapters, we cross-tabulated the numbers of deaths for people with IBD and those without IBD and used a heatmaps and alluvial plots to qualitatively assess coding system alignment. Throughout, cell sizes of 1 to 5 people were suppressed due to privacy regulations. All analyses were conducted in Python version 3.7 (Python Software Foundation, Beaverton, USA). Study reporting followed The REporting of studies Conducted using Observational Routinely collected health Data (RECORD) Statement guidelines.23
Results
Cohort Characteristics
The study cohort consisted of 7,919 decedents with IBD matched to 39,414 decedents without IBD, with a match success (mean number of controls per case) of >4.99; only 6 decedents with IBD did not match 5 controls (Table 1). Nearly half (47%) of decedents with IBD died prematurely. Those without IBD were matched on age of death and thus, had the same proportion of premature deaths.
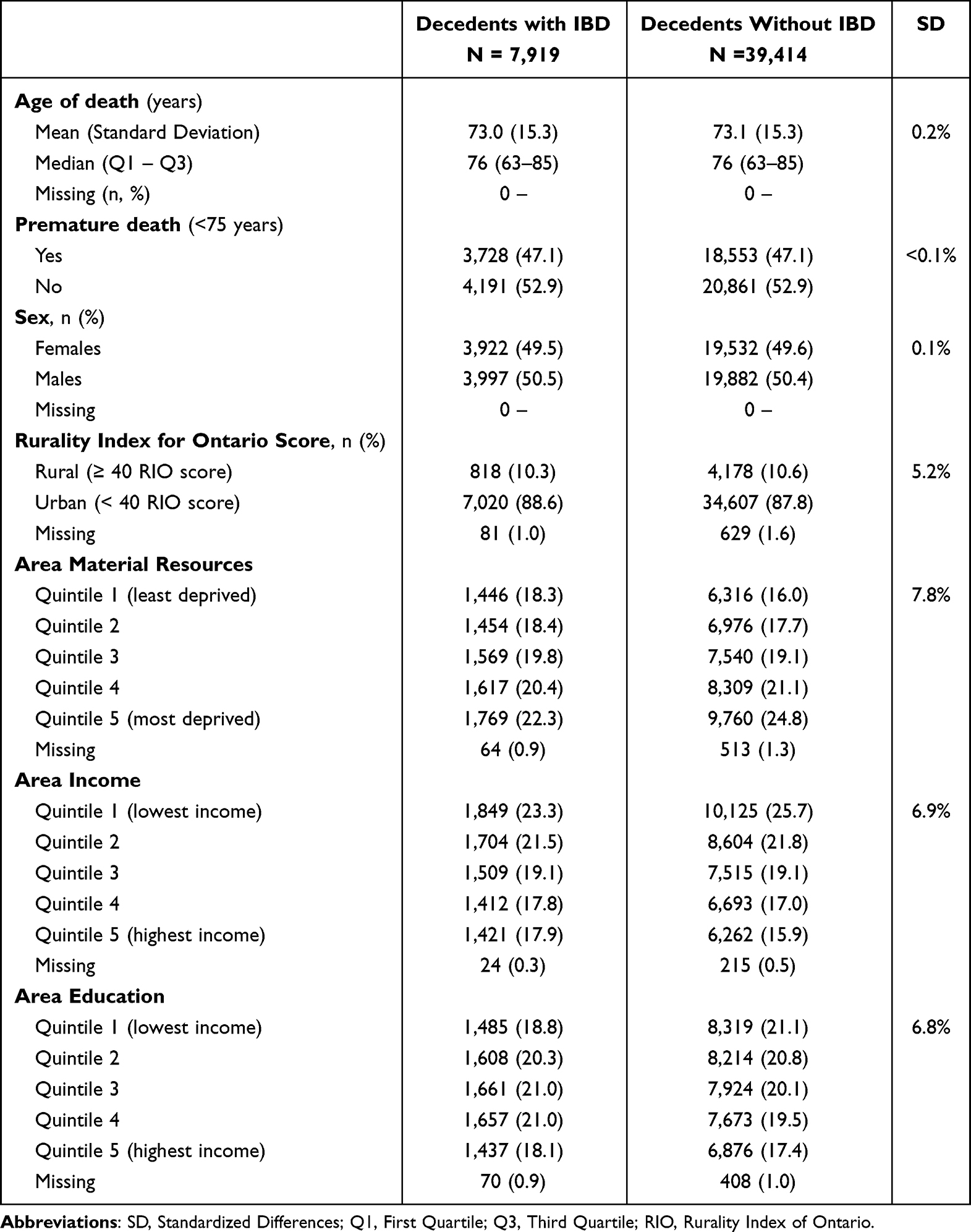 |
Table 1 Causes of Death According to Leading Causes of Death (LCD) Category Across People with IBD and Matched Controls, 2010–2018 |
Causes of Death with ICD-10 Chapters
For all deaths, the top COD, both for those with and without IBD, were neoplasms (28% vs 31%, SD: 7%) and diseases of the circulatory system (21% vs 25%, SD: 9%) (Figure 1A). Among those with IBD, there was a higher prevalence of deaths attributed to digestive system-related causes (11% vs 4%, SD: 25%). Among those with IBD, 46% of deaths due to digestive system-related causes were attributed to disease of the liver (Supplemental Table E).
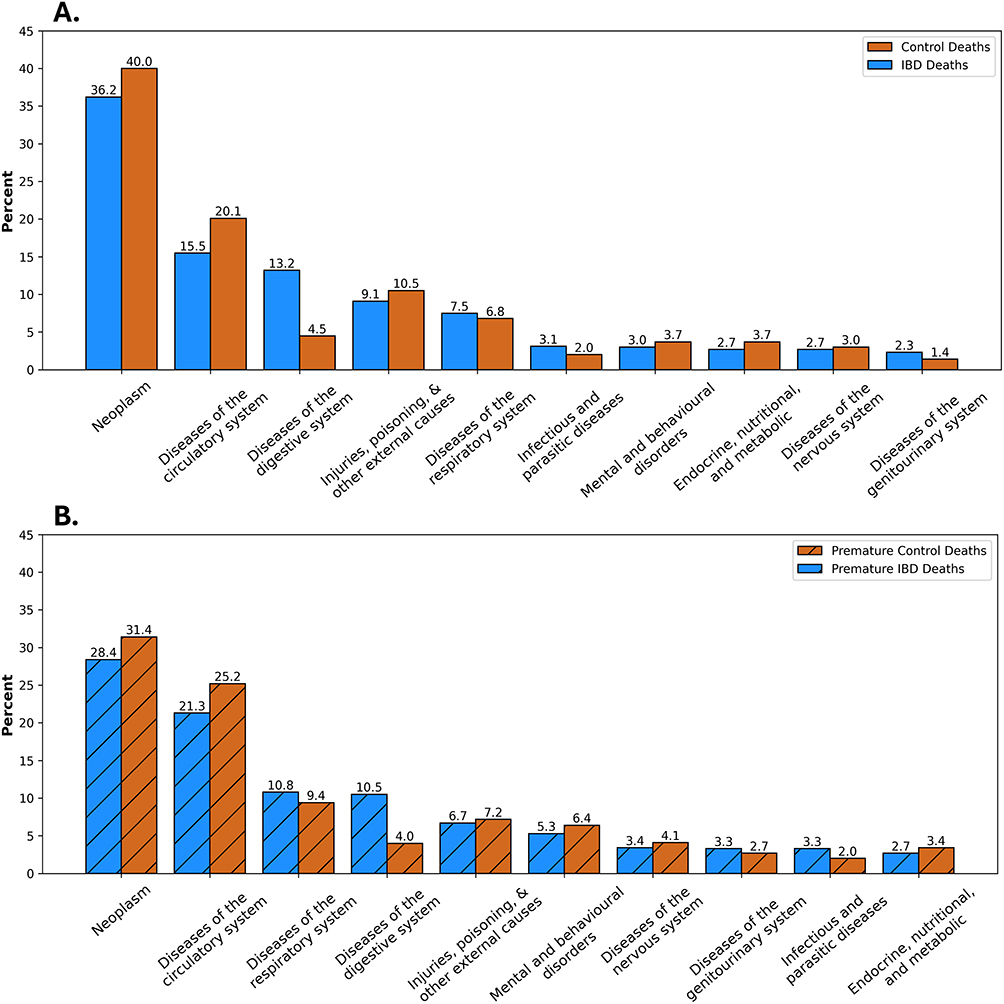 |
Figure 1 Causes of death according to ICD-10 categories for (A) all deaths among those with IBD and their controls and (B) premature deaths among those with IBD and their controls. The ICD-10 categories included in this figure are those with proportions >1%. The categories of other were also excluded from the image as it is a derived category for suppression of small cells. Figure data available in Supplemental Tables E and F. |
Our baseline categorization was ICD-10 chapters. The top 3 causes of premature death for those with IBD based on ICD-10 coding were neoplasms (36%), diseases of the circulatory system (16%), and diseases of the gastrointestinal system (13%) (Figure 1B). People with IBD had a lower prevalence of deaths due to diseases of the circulatory system (16% vs 20%, SD: 12%) but a higher prevalence of diseases of the digestive system (13% vs 5%, SD: 31%) (Supplemental Table F).
Causes of Death with LCD Classification
Using the LCD coding scheme for all deaths, both those with and without IBD had the same top 10 COD (Figure 2A and B), differing only in rank order. The top three were ischemic heart disease (10% vs 11%, SD: 5%), cancer of the lungs and bronchus (6% vs 7%, SD: 6%), and dementia/Alzheimer’s disease (5% vs 6%, SD: 6%) (Supplemental Table G). For premature deaths, the top causes for those with and without IBD were similar and without significant differences in prevalence; the exception to this was the residual category (Figure 2C, D and Supplemental Table H).
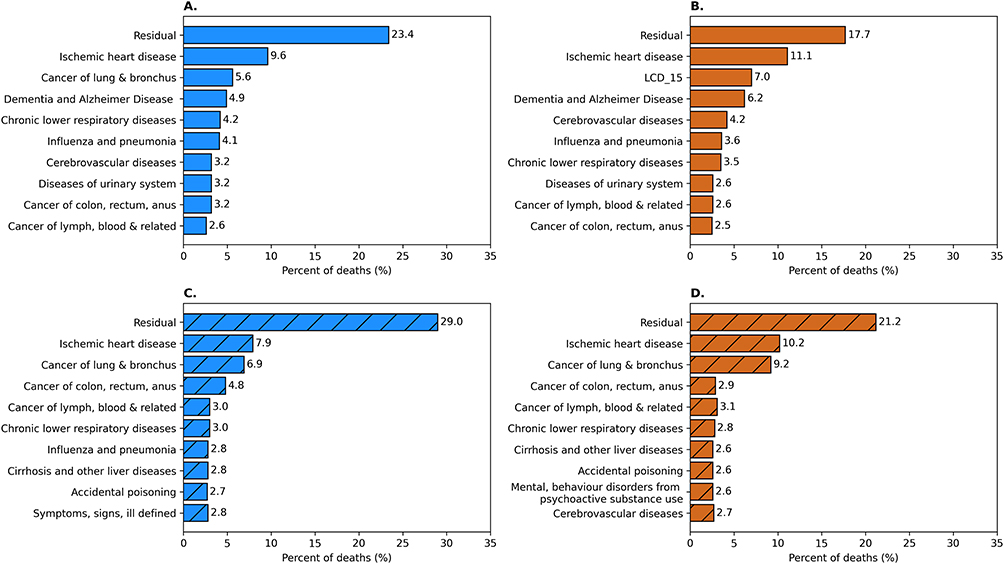 |
Figure 2 Top Leading Causes of Death (LCD) for (A) all deaths among individuals with IBD, (B) all deaths among matched controls, (C) premature deaths among individuals with IBD, and (D) premature deaths among matched controls. The LCD categories included are categories with the 10 highest prevalences. Figure data available in Supplemental Tables G and H. |
Notably, decedents with IBD had a higher prevalence of COD being residual (effectively not categorized) than controls (23% vs 18%, SD: 14%). For premature deaths, the proportion attributable to residual was even greater compared to overall mortality, particularly for individuals with IBD as compared to matched controls (29% vs 21%, SD: 18%) (Supplemental Table H).
Mapping LCD to ICD-10
For those with and without IBD, general consistency in coding construct was observed across coding schemes (ie, deaths classified into analogous causes in each framework) except for the residual category (Figure 3). For both premature and overall mortality, most IBD deaths attributed to residual were classified under diseases of the digestive system (34%) and neoplasm (29%) ICD-10 chapters. In contrast, for matched controls, residual causes were more likely to be predominantly attributed to neoplasms (42%) (Figure 4).
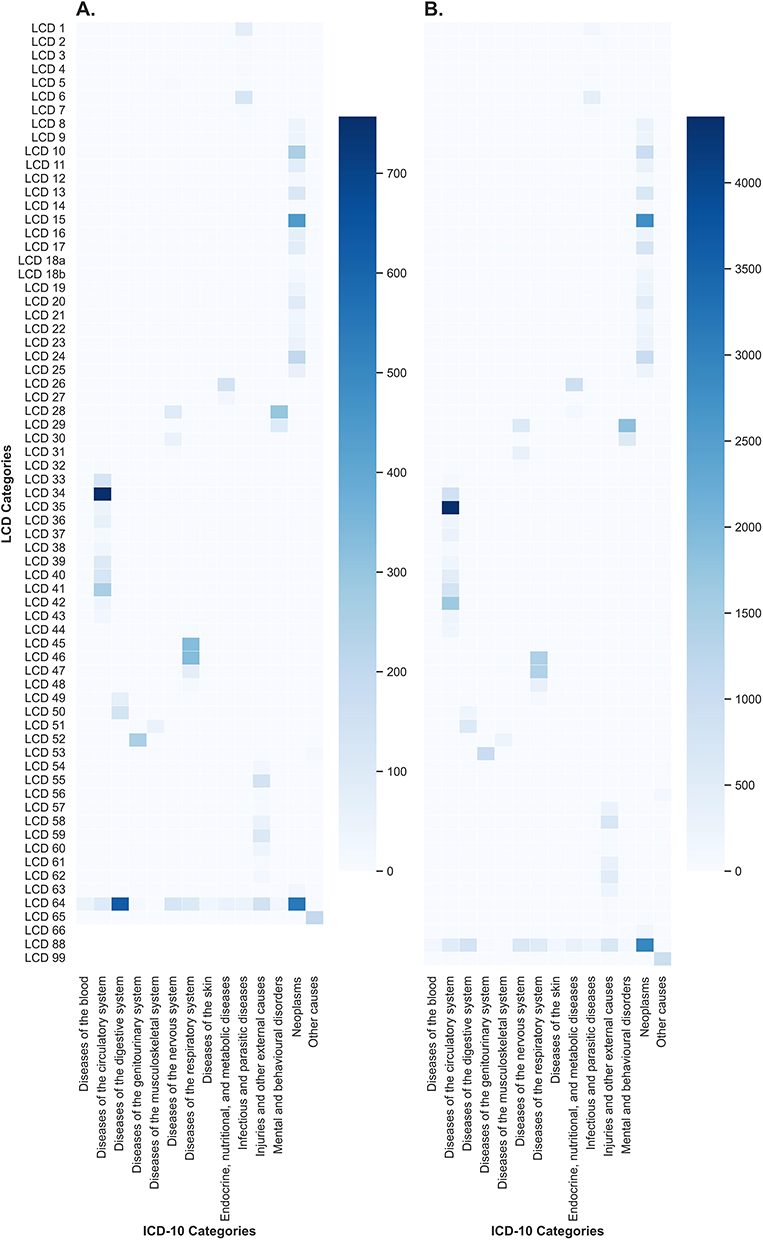 |
Figure 3 Heatmap plots mapping the concordance of causes of deaths categorized with the Leading Causes of Death (LCD) to the ICD-10 chapters among those with IBD (A) and matched controls (B) according to their ICD-10 chapters and Leading Causes of Death (LCD) categories. Data available in Supplemental Table I. |
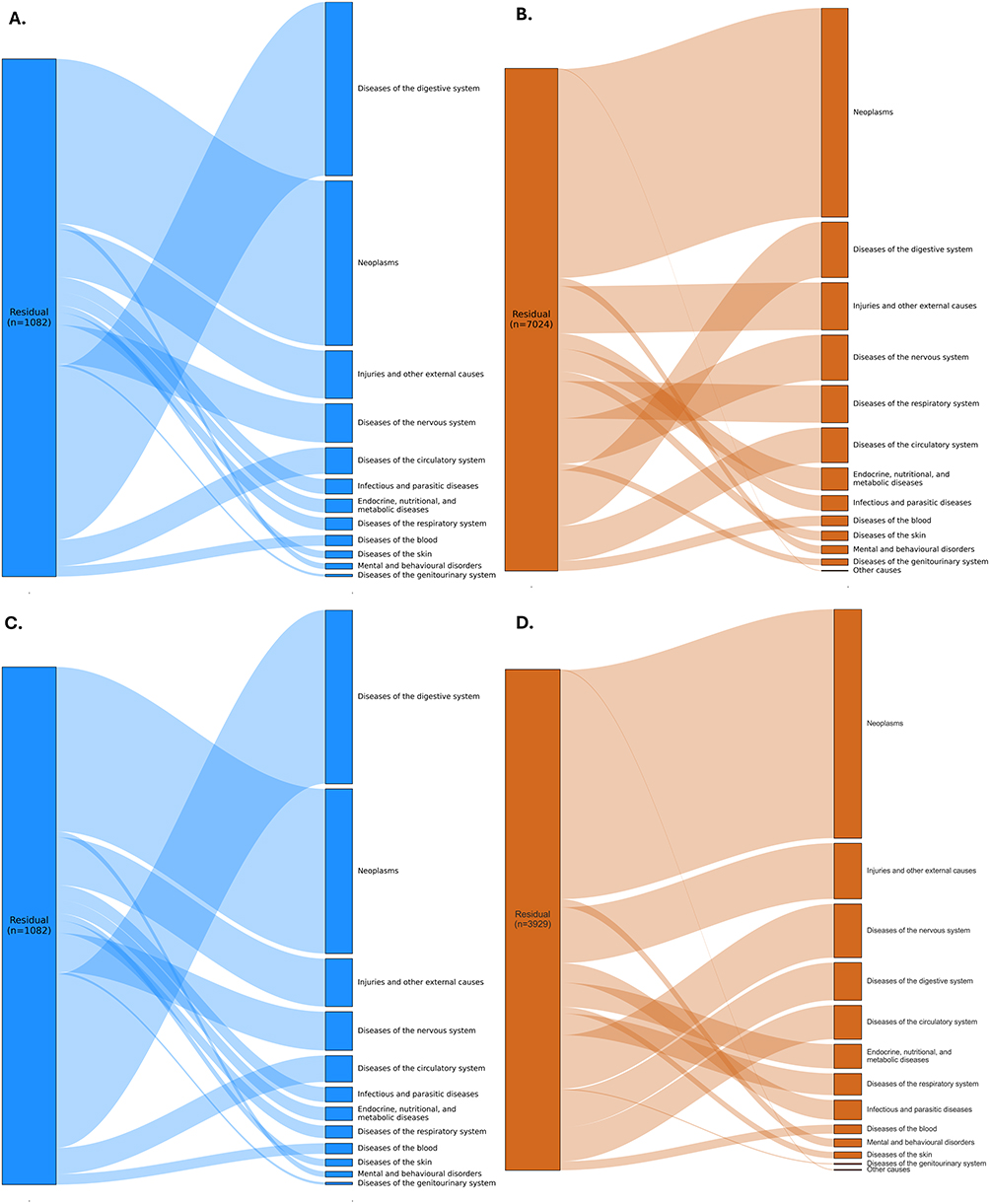 |
Figure 4 Alluvial plots displaying the mapping of deaths classified as residuals in the Leading Causes of Death (LCD) scheme and the ICD-10 chapter that the deaths categorized as residual in the LCD scheme map to when using that classification system. Subplots display the mapping of residual deaths for (A) all deaths among those with IBD, (B) all deaths among matched controls, (C) premature deaths among those with IBD, and (D) premature deaths among matched controls. |
Discussion
To better understand how causes of premature mortality should be categorized to identify priority areas for intervention, we conducted a population-based comparison of two COD classification systems: ICD-10 and the LCD framework. We observed notable differences between the two systems in the top causes identified and their ability to detect variation in COD between individuals with IBD and matched controls. Based on ICD-10 coding, the top COD, both in populations with IBD and in matched controls, were neoplasms and diseases of the circulatory system. Among deaths in those with IBD, particularly in premature deaths, there was a higher proportion attributed to diseases of the digestive systems than in matched controls. In contrast, when applying the LCD framework, differences in COD between those with and without IBD were not detectable as a disproportionately large share of deaths among individuals with IBD were classified into the residual category, obscuring condition-specific mortality patterns.
The key implication of our study is that the LCD categories obscure condition-specific COD in IBD by placing a substantial proportion in the residual category. The proportion of deaths allocated to the residual category was greater for those with IBD and matched controls (23% vs 18%, SD: 14%), a difference even larger for premature deaths (29% vs 21%, SD: 18%). Much of the residual causes for overall and premature in Becker’s LCD coding system were digestive diseases and neoplasms. In the context of the broader literature, the observed pattern helps explain inconsistencies regarding the leading COD among individuals with IBD. Several studies have reported negligible differences in COD among those with IBD compared to those without, with top causes being cancers and diseases of the circulatory system.24–31 However, increased proportions of digestive COD among those with IBD, relative to the general population, have also been observed in Manitoba (Canada),32 the United States,33 Italy,34 Sweden,35 Denmark,36 and Finland.37 Taken together, our findings reflect that people living with IBD have different predominant causes than global populations and the ability to identify differences depends on classification system.
Predominant strategies for conducting population-level COD analyses include all-cause mortality,38–42 ICD Chapters,27,36,37,43–45 select amenable-causes,46 or study-selected disease-relevant causes.38,47,48 While the ICD-10 chapters are more effective in demonstrating excess gastrointestinal mortality, it is difficult to identify avenues to address such disparities given the many diseases of the gastrointestinal systems captured within the ICD chapter. Likewise, when using the ICD-10 chapters for comparing death, negligible differences in prevalence do not inherently reflect similarity COD owing to the large grouping of causes, and thus the potential to mask within chapter differences. Development of a framework for categorizing common, preventable, and/or amenable causes for IBD would be pertinent moving forward. Using a rank-based approach analogous to the LCD framework, but tailored to premature mortality among those with IBD, would guide research and policy interventions as the framework could identify specific causes relevant to premature mortality in populations with IBD. Such an approach is of relevance globally given the burden of IBD is growing worldwide.11
Other approaches for categorizing COD emphasize that causes are necessary but not sufficient, meaning death occurs due to a constellation of causes rather than as the result of a single insult; in other words, mortality is the results of multiple COD.49 A systematic review of analytic methods for COD research (n=434 studies) noted four analytic approaches to account for multiple COD: any–mention of COD (87%), pairwise combinations of causes (57%), cluster analysis (2%), and multiple-cause weights (1%).50 Digestive diseases are an under-researched focus in the multiple COD studies, with only 13 of the 434 studies focusing on digestive diseases.50 The interplay between coding systems and multiple COD should be a priority in future IBD research.
Broadly speaking, the purpose of comparing COD across and within populations is to identify discrepancies that may highlight priority areas to improve the care.10 Clinical and policy-based consideration of findings direct attention to causes that need to be prioritized in care of IBD. We found deaths in the population with IBD were commonly caused by neoplasm, diseases of the digestive system (particularly liver disease), and diseases of the respiratory system. Increased proportions of digestive causes among premature deaths with IBD has been noted elsewhere.51 Increased proportion of deaths attributable to respiratory diseases among those with IBD (1999–2008) has also been observed in Québec, Canada.52 In Ontario, Canada, 46% and 43% of decedents with IBD were previously diagnosed with a cancer and chronic obstructive pulmonary disorder, respectively.8 These findings underscore the importance of strengthening integrated approaches to multidisciplinary management for people with IBD. Specifically, for respiratory causes, integrated care of pulmonary comorbidities, vaccination against respiratory pathogens (eg, influenza and pneumococcus), and proactive management of smoking and medication-related lung toxicity represent key opportunities to prevent premature deaths in this population.53–56 For digestive causes, interventions such as enhanced colorectal cancer surveillance, early detection of hepatobiliary complications, and optimization of disease activity monitoring may help reduce mortality risk.57–60 However, only 10% of deaths in our study were attributable to digestive diseases. Similarly, Chu et al also reported only approximately 10% of deaths among those with IBD as attributable to gastrointestinal causes (excluding gastrointestinal cancers).61 These and other COD trends may be influenced by the underlying inflammatory processes, treatment regimens, and clinical care—all of which are evolving with higher uptake of biologics, increased cancer surveillance, improved mental health care, and vascular prophylaxis.62,63 Together, this emphasizes the need for holistic care and ongoing mortality research.
Strengths and Limitations
The strengths of this study include its large sample size, population-based nature, and the use of validated algorithms to identify people with IBD.13,14 However, our study has limitations. First, the algorithm for identifying pediatric cases of IBD has a lower positive predictive value than for adults, which may have led to greater misclassification of IBD status for deaths <18 years; however, such misclassification would suppress differences in usability of LCD by IBD status, and thus, observed differences in classification effectiveness are conservative. Second, we used health administrative data to identify COD among individuals with IBD; all studies using health administrative data are at risk of misclassification bias.23 In particular, without a clear reference standard to define “truth” in the two COD systems, we cannot definitively determine which coding system is superior. Additionally, our findings are sensitive to the method of categorization and as demonstrated, each system comes with its own limitations in terms of specific conditions it identifies. Becker’s LCD approach was not designed for specific use among IBD, though in the absence of a digestive disease LCD framework, we used it to explore leading COD among those with IBD. Our findings do not indicate an optimal approach for classifying COD. Rather, our study lays the groundwork for such future research.
Conclusion
Identifying an optimal approach for studying causes of premature mortality is important for informing care, resource allocation, and prioritization of future research. The LCD coding scheme provides more granular COD details than the commonly used ICD-10 chapters. However, its usability is limited among people with IBD because COD is disproportionately allocated to the residual category, which prevents the identification of priorities for health policy interventions. Causes allocated to the residual category predominantly included neoplasms and diseases of the digestive system. Most premature deaths among those with IBD were not due to digestive diseases. These findings highlight the need for future research to develop systems of COD classification that provide sufficient granularity for evaluating premature mortality among those with IBD and priority diseases to improve the quality of research on COD using routinely collected health data.
Data Sharing Statement
The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (eg, healthcare organizations and government) prohibit ICES from making the dataset publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at https://www.ices.on.ca/DAS (email: [email protected]). The full dataset creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Ethics Approval
The data used are housed at ICES for residents of Ontario eligible for its universal healthcare coverage at any point since April 1991 (>99% of the population). ICES is a prescribed entity under section 45 of Ontario’s Personal Health Information Protection Act, allowing it to collect and analyze health care and demographic data, without additional consent, for health system evaluation and improvement. The use of data in this project was authorized under section 45 and did not require additional informed consent nor ethics approval.
Acknowledgments
This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). Parts of this material are based on data and/or information compiled and provided by CIHI and the Ontario Ministry of Health. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. The document was adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File (PCCF), which contains data copied under license from Canada Post Corporation and Statistics Canada, adapted from Statistics Canada. This does not constitute an endorsement by Statistics Canada of this product. We thank the Toronto Community Health Profiles Partnership for providing access to the Ontario Marginalization Index. Part of this report is based on Ontario Registrar General (ORG) information on deaths, the original source of which is ServiceOntario. The views expressed therein are those of the author and do not necessarily reflect those of ORG or the Ministry of Public and Business Service Delivery.
Funding
Gemma Postill received funding for this study from the 2023 American College of Gastroenterology Medical Student Research Award. Laura Rosella is funded by a Canada Research Chair in Population Health Analytics (72051628) and Stephen Family Chair in Community Health from Trillium Health Partners. Eric Benchimol holds the Northbridge Financial Corporation Chair in Inflammatory Bowel Disease, a joint Hospital-University Chair between the University of Toronto, The Hospital for Sick Children, and the SickKids Foundation.
Disclosure
Eric Benchimol has acted as a consultant for the Canadian Drug Agency. He has received speaking fees for academic/educational presentations from HMP Global and Catrile & Associates, Ltd, and personal fees from Dairy Farmers of Ontario. The authors report no other conflicts of interest in this work.
References
1. Canadian Institute for Health Information. Avoidable Deaths. Canadian Institute for Health Information; 2023. Available from: https://www.cihi.ca/en/indicators/avoidable-deaths.
2. Statistics Canada. Premature and potentially avoidable mortality, Canada, provinces and territories. Statistics Canada; 2023. Available from: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310074401.
3. Bowes M, Strang R, Huyer D. Use of data from death investigation systems to support community health and prevent premature deaths in Canada. Can Med Assoc J. 2024;196(15):E527–E529. doi:10.1503/cmaj.231386
4. Buajitti E, Watson T, Norwood T, et al. Regional variation of premature mortality in Ontario, Canada: a spatial analysis. Popul Health Metr. 2019;17(1):9. doi:10.1186/s12963-019-0193-9
5. Norheim OF, Jha P, Admasu K, et al. Avoiding 40% of the premature deaths in each country, 2010–30: review of national mortality trends to help quantify the UN Sustainable Development Goal for health. The Lancet. 2015;385(9964):239–252. doi:10.1016/S0140-6736(14)61591-9
6. Shiels MS, Chernyavskiy P, Anderson WF, et al. Trends in premature mortality in the USA by sex, race, and ethnicity from 1999 to 2014: an analysis of death certificate data. The Lancet. 2017;389(10073):1043–1054. doi:10.1016/S0140-6736(17)30187-3
7. Ma Fat D. A method for deriving leading causes of death. Bull World Health Organ. 2006;2006(4):297–304. doi:10.2471/BLT.05.028670
8. Postill G, Itanyi IU, Kuenzig ME, et al. Machine learning prediction of premature death from multimorbidity among people with inflammatory bowel disease: a population-based retrospective cohort study. Can Med Assoc J. 2025;197(11):E286–E297. doi:10.1503/cmaj.241117
9. Card T, Hubbard R, Logan RFA. Mortality in inflammatory bowel disease: a population-based cohort study. Gastroenterology. 2003;125(6):1583–1590. doi:10.1053/j.gastro.2003.09.029
10. Kuenzig ME, Manuel DG, Donelle J, Benchimol EI. Life expectancy and health-adjusted life expectancy in people with inflammatory bowel disease. Can Med Assoc J. 2020;192(45):E1394–E1402. doi:10.1503/cmaj.190976
11. Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. The Lancet. 2017;390(10114):2769–2778. doi:10.1016/S0140-6736(17)32448-0
12. Coward S, Benchimol EI, Kuenzig ME, et al. The 2023 impact of inflammatory bowel disease in Canada: epidemiology of IBD. J Can Assoc Gastroenterol. 2023;6(Supplement_2):S9–S15. doi:10.1093/jcag/gwad004
13. Benchimol EI, Guttmann A, Griffiths AM, et al. Increasing incidence of paediatric inflammatory bowel disease in Ontario, Canada: evidence from health administrative data. Gut. 2009;58(11):1490–1497. doi:10.1136/gut.2009.188383
14. Benchimol EI, Guttmann A, Mack DR, et al. Validation of international algorithms to identify adults with inflammatory bowel disease in health administrative data from Ontario, Canada. J Clin Epidemiol. 2014;67(8):887–896. doi:10.1016/j.jclinepi.2014.02.019
15. Chiu M, Lebenbaum M, Lam K, et al. Describing the linkages of the immigration, refugees and citizenship Canada permanent resident data and vital statistics death registry to Ontario’s administrative health database. BMC Med Inform Decis Mak. 2016;16(1):135. doi:10.1186/s12911-016-0375-3
16. Subedi R, Greenberg TL, Roshanafshar S. Does geography matter in mortality? An analysis of potentially avoidable mortality by remoteness index in Canada. Health Rep.Government of Canada, Statistics Canada. 2019;30(5):3–15. doi:10.25318/82-003-X201900500001-ENG
17. The Canadian Institute for Health Information. Avoidable deaths from preventable causes. The Canadian Institute for Health Information; 2023. Available from: https://www.cihi.ca/en/indicators/avoidable-deaths-from-preventable-causes.
18. Statistics Canada. Deaths, by age group and sex. Statistics Canada; 2023. Available from: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310070901&pickMembers%5B0%5D=1.7&pickMembers%5B1%5D=3.1&cubeTimeFrame.startYear=2018&cubeTimeFrame.endYear=2022&referencePeriods=20180101%2C20220101.
19. Van Ingen T, Matheson FI. The 2011 and 2016 iterations of the Ontario Marginalization Index: updates, consistency and a cross-sectional study of health outcome associations. Can J Public Health. 2022;113(2):260–271. doi:10.17269/s41997-021-00552-1
20. Matheson FI, Dunn JR, Smith KLW, Moineddin R, Glazier RH. Élaboration de l’indice de marginalisation canadien: un nouvel outil d’étude des inégalités. Can J Public Health. 2012;103(S2):S12–S16. doi:10.1007/BF03403823
21. Boris K, Association OM. Measuring Rurality - RIO 2008_BASIC: Methodology and Results. Ontario Medical Association Economics Department; 2009.
22. Austin PC. Using the standardized difference to compare the prevalence of a binary variable between two groups in observational research. Commun Stat - Simul Comput. 2009;38(6):1228–1234. doi:10.1080/03610910902859574
23. Benchimol EI, Smeeth L, Guttmann A, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLOS Med. 2015;12(10):e1001885. doi:10.1371/journal.pmed.1001885
24. Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet. 2018;392(10159):1736–1788. doi:10.1016/S0140-6736(18)32203-7
25. Naghavi M, Ong KL, Aali A, et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet. 2024;403(10440):2100–2132. doi:10.1016/S0140-6736(24)00367-2
26. Laurberg T, Graversen SB, Sandbæk A, Wild SH, Vos RC, Støvring H. Trends in cause-specific mortality among people with type 2 and type 1 diabetes from 2002 to 2019: a Danish population-based study. Lancet Reg Health - Eur. 2024;41:100909. doi:10.1016/j.lanepe.2024.100909
27. Tetzlaff F, Sauerberg M, Grigoriev P, et al. Age-specific and cause-specific mortality contributions to the socioeconomic gap in life expectancy in Germany, 2003–21: an ecological study. Lancet Public Health. 2024;9(5):e295–e305. doi:10.1016/S2468-2667(24)00049-5
28. Schumacher AE, Kyu HH, Aali A, et al. Global age-sex-specific mortality, life expectancy, and population estimates in 204 countries and territories and 811 subnational locations, 1950–2021, and the impact of the COVID-19 pandemic: a comprehensive demographic analysis for the Global Burden of Disease Study 2021. The Lancet. 2024;403(10440):1989–2056. doi:10.1016/S0140-6736(24)00476-8
29. Qi J, Li M, Wang L, et al. National and subnational trends in cancer burden in China, 2005–20: an analysis of national mortality surveillance data. Lancet Public Health. 2023;8(12):e943–e955. doi:10.1016/S2468-2667(23)00211-6
30. Murthy SS, Trapani D, Cao B, et al. Premature mortality trends in 183 countries by cancer type, sex, WHO region, and World Bank income level in 2000–19: a retrospective, cross-sectional, population-based study. Lancet Oncol. 2024;25(8):969–978. doi:10.1016/S1470-2045(24)00274-2
31. Feigin VL, Stark BA, Johnson CO, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795–820. doi:10.1016/S1474-4422(21)00252-0
32. Bernstein CN, Nugent Z, Targownik LE, Singh H, Lix LM. Predictors and risks for death in a population-based study of persons with IBD in Manitoba. Gut. 2015;64(9):1403–1411. doi:10.1136/gutjnl-2014-307983
33. Jess T. Survival and cause specific mortality in patients with inflammatory bowel disease: a long term outcome study in Olmsted County, Minnesota, 1940–2004. Gut. 2006;55(9):1248–1254. doi:10.1136/gut.2005.079350
34. Masala G. Divergent patterns of total and cancer mortality in ulcerative colitis and Crohn’s disease patients: the Florence IBD study 1978–2001. Gut. 2004;53(9):1309–1313. doi:10.1136/gut.2003.031476
35. Persson P, Bernell O, Leijonmarck C, Farahmand B, Hellers G, Ahlbom A. Survival and cause-specific mortality in inflammatory bowel disease: a population-based cohort study. Gastroenterology. 1996;110(5):1339–1345. doi:10.1053/gast.1996.v110.pm8613037
36. Jess T, Winther KV, Munkholm P, Langholz E, Binder V. Mortality and causes of death in Crohn’s disease: follow-up of a population-based cohort in Copenhagen County, Denmark. Gastroenterology. 2002;122(7):1808–1814. doi:10.1053/gast.2002.33632
37. Jussila A, Virta LJ, Pukkala E, Färkkilä MA. Mortality and causes of death in patients with inflammatory bowel disease: a nationwide register study in Finland. J Crohns Colitis. 2014;8(9):1088–1096. doi:10.1016/j.crohns.2014.02.015
38. Chesney TR, Coburn N, Mahar AL, et al. All-cause and cancer-specific death of older adults following surgery for cancer. JAMA Surg. 2021;156(7):e211425. doi:10.1001/jamasurg.2021.1425
39. Rosella LC, Kornas K, Negatu E, Zhou L. Variations in all-cause mortality, premature mortality and cause-specific mortality among persons with diabetes in Ontario, Canada. BMJ Open Diabetes Res Care. 2023;11(3):e003378. doi:10.1136/bmjdrc-2023-003378
40. Egeberg A, Gislason GH, Hansen PR. Risk of major adverse cardiovascular events and all-cause mortality in patients with hidradenitis suppurativa. JAMA Dermatol. 2016;152(4):429–434. doi:10.1001/jamadermatol.2015.6264
41. Bournia VK, Fragoulis GE, Mitrou P, et al. All-cause mortality in systemic rheumatic diseases under treatment compared with the general population, 2015–2019. RMD Open. 2021;7(3):e001694. doi:10.1136/rmdopen-2021-001694
42. Haddad A, Saliba W, Lavi I, et al. the association of psoriatic arthritis with all-cause mortality and leading causes of death in psoriatic arthritis. J Rheumatol. 2022;49(2):165–170. doi:10.3899/jrheum.210159
43. Jess T, Frisch M, Simonsen J. Trends in overall and cause-specific mortality among patients with inflammatory bowel disease from 1982 to 2010. Clin Gastroenterol Hepatol. 2013;11(1):43–48. doi:10.1016/j.cgh.2012.09.026
44. Winkler V, Ott JJ, Becher H. Reliability of coding causes of death with ICD-10 in Germany. Int J Public Health. 2010;55(1):43–48. doi:10.1007/s00038-009-0053-7
45. Opstelten JL, Vaartjes I, Bots ML, Oldenburg B. Mortality after first hospital admission for inflammatory bowel disease: a nationwide registry linkage study. Inflamm Bowel Dis. 2019;25(10):1692–1699. doi:10.1093/ibd/izz055
46. Nolte E. Measuring the health of nations: analysis of mortality amenable to health care. BMJ. 2003;327(7424):1129. doi:10.1136/bmj.327.7424.1129
47. Wang JS, Wu YL, Ou HY, Yang YS, Hsu CC, Hwu CM. Trends in all-cause mortality and major causes of death between 2007 and 2018 among patients with diabetes in Taiwan. Front Endocrinol. 2022;13:984137. doi:10.3389/fendo.2022.984137
48. Follin-Arbelet B, Cvancarova Småstuen M, Ø H, Jelsness-Jørgensen LP, Moum B. Mortality in patients with inflammatory bowel disease: results from 30 years of follow-up in a Norwegian Inception Cohort (the IBSEN study). J Crohns Colitis. 2023;17(4):497–503. doi:10.1093/ecco-jcc/jjac156
49. Grippo F, Frova L, Pappagallo M, et al. Beyond the underlying cause of death: an algorithm to study multi-morbidity at death. Popul Health Metr. 2024;22(1):36. doi:10.1186/s12963-024-00356-8
50. Bishop K, Balogun S, Eynstone-Hinkins J, et al. Analysis of multiple causes of death: a review of methods and practices. Epidemiology. 2023;34(3):333–344. doi:10.1097/EDE.0000000000001597
51. Nocerino A, Feathers A, Ivanina E, Durbin L, Swaminath A. Mortality risk of inflammatory bowel disease: a case–control study of New York State Death Records. Dig Dis Sci. 2019;64(6):1604–1611. doi:10.1007/s10620-018-5430-8
52. Bitton A, Vutcovici M, Sewitch M, Suissa S, Brassard P. Mortality trends in Crohn’s disease and ulcerative colitis: a population-based study in Québec, Canada. Inflamm Bowel Dis. 2016;22(2):416–423. doi:10.1097/MIB.0000000000000608
53. Ji XQ. Pulmonary manifestations of inflammatory bowel disease. World J Gastroenterol. 2014;20(37):13501. doi:10.3748/wjg.v20.i37.13501
54. Farraye FA. Vaccination updates for patients with inflammatory bowel disease. Gastroenterol Hepatol. 2022;18(9):538–541.
55. Cavalli CAM, Gabbiadini R, Dal Buono A, et al. Lung involvement in inflammatory bowel diseases: shared pathways and unwanted connections. J Clin Med. 2023;12(19):6419. doi:10.3390/jcm12196419
56. Dan L, Xie Y, Fu T, et al. Increased risk of chronic respiratory disease among individuals with inflammatory bowel disease in a prospective cohort study. Am J Med. 2025;138(1):42–50.e5. doi:10.1016/j.amjmed.2024.09.001
57. Axelrad JE, Rubin DT. The management of colorectal neoplasia in patients with inflammatory bowel disease. Clin Gastroenterol Hepatol. 2024;22(6):1181–1185. doi:10.1016/j.cgh.2024.01.030
58. Sato Y, Tsujinaka S, Miura T, Kitamura Y, Suzuki H, Shibata C. Inflammatory bowel disease and colorectal cancer: epidemiology, etiology, surveillance, and management. Cancers. 2023;15(16):4154. doi:10.3390/cancers15164154
59. East JE, Gordon M, Nigam GB, et al. British Society of Gastroenterology guidelines on colorectal surveillance in inflammatory bowel disease. Gut. 2025:gutjnl–2025–335023. doi:10.1136/gutjnl-2025-335023
60. Zauber AG. The impact of screening on colorectal cancer mortality and incidence: has it really made a difference? Dig Dis Sci. 2015;60(3):681–691. doi:10.1007/s10620-015-3600-5
61. Chu TPC, Moran GW, Card TR. The pattern of underlying cause of death in patients with inflammatory bowel disease in England: a record linkage study. J Crohns Colitis. 2016;jjw192. doi:10.1093/ecco-jcc/jjw192
62. Alatab S, Sepanlou SG, Ikuta K, et al. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):17–30. doi:10.1016/S2468-1253(19)30333-4
63. Olén O, Askling J, Sachs MC, et al. Mortality in adult-onset and elderly-onset IBD: a nationwide register-based cohort study 1964–2014. Gut. 2020;69(3):453–461. doi:10.1136/gutjnl-2018-317572
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Variation in the Care of Children with Inflammatory Bowel Disease Within and Across Canadian Provinces: A Multi-Province Population-Based Cohort Study
Kuenzig ME, Stukel TA, Carroll MW, Kaplan GG, Otley AR, Singh H, Bitton A, Fung SG, Spruin S, Coward S, Cui Y, Nugent Z, Griffiths AM, Mack DR, Jacobson K, Nguyen GC, Targownik LE, El-Matary W, Bernstein CN, Dummer TJB, Jones JL, Lix LM, Murthy SK, Peña-Sánchez JN, Nasiri S, Benchimol EI
Clinical Epidemiology 2024, 16:91-108
Published Date: 14 February 2024