Back to Journals » Patient Preference and Adherence » Volume 17
Validation of the Working Alliance Inventory- Short Form for Patient (WAI-S-P) in Peruvian Adults
Authors Ramos-Vera C, Sánchez-Villena AR, Calle D, Calizaya-Milla YE ![]() , Saintila J
, Saintila J ![]()
Received 24 May 2023
Accepted for publication 10 August 2023
Published 25 September 2023 Volume 2023:17 Pages 2365—2376
DOI https://doi.org/10.2147/PPA.S422733
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Cristian Ramos-Vera,1 Andy R Sánchez-Villena,2 Dennis Calle,1 Yaquelin E Calizaya-Milla,3 Jacksaint Saintila4
1Área de Investigación, Universidad Cesar Vallejo (UCV), Lima, Perú; 2Facultad de Ciencias de La Salud, Universidad Privada del Norte, Cajamarca, Perú; 3Facultad de Ciencias de la Salud, Universidad Peruana Unión, Lima, Perú; 4Escuela de Medicina Humana, Universidad Señor de Sipán, Chiclayo, Perú
Correspondence: Jacksaint Saintila, Escuela de Medicina Humana, Universidad Señor de Sipán, Km 5, Carretera a Pimentel, Chiclayo, Lambayeque, 14001, Perú, Email [email protected]
Background: Although the importance of the therapeutic alliance in the treatment process and health outcomes is recognized, so far, there has been no evaluation in the Peruvian context that considers possible individual differences that could influence this assessment.
Purpose: This study assessed the psychometric properties of the WAI-S-P in a sample of individuals from Peru who are receiving psychological therapy. Furthermore, a network analysis was conducted to investigate the direct relationships between the therapeutic alliance and several relevant sociodemographic variables.
Methods: The short version of the Working Alliance Inventory was used in a sample of 241 participants (Mage=32.58, SD=12.67) that had attended less than 6 sessions. Three models were considered, including a three-factor and a two-factor correlated model, as well as a bifactor model. In addition, a network of partial associations was created including the overall therapeutic alliance, sex, age, and number of psychotherapeutic sessions.
Results: The bifactor model, with an overall therapeutic alliance factor and two specific factors (“contact” and “contract”), better fit the data. Invariance of the structure by sex and age showed equitable measurement. On the other hand, network analysis revealed a positive correlation between total session attendance and therapeutic alliance. Men reported higher therapeutic alliance, while women had higher total session attendance.
Conclusion: The results of this study suggest that the therapeutic alliance is better represented by a bifactor model and demonstrates invariance across sex and age in Peruvian adults. Additionally, findings indicate that differences in life experiences and the sex of patients may need to be verified in future studies to better understand nuanced needs in forming therapeutic alliances at least in the early stages of session attendance.
Keywords: Working Alliance Inventory, patients, psychotherapy, psychometric properties, network analysis
Introduction
The therapeutic alliance is an interactive process that has its roots in Freud’s ideas on transference and was later explored by Rogers in the context of humanistic therapy, emphasizing the importance of the therapist’s empathy towards the patient.1 The systematic study and conceptualization of the therapeutic alliance was carried out by Anderson,2 who introduced the term “rapport”. Since then, several researchers have contributed to the empirical testing of this concept.3,4
The therapeutic alliance can be described as a collaborative relationship that is established between an individual seeking treatment and the mental health professional, and is one of the key elements in both receiving and providing psychotherapy.5,6 In fact, the therapeutic alliance is considered a predictor of the success or failure of a psychotherapeutic treatment, regardless of the approach used.7 In addition, this factor is relevant in the appropriate management of various mental health disorders, such as schizophrenia,8 post-traumatic stress,9 depression and anxiety,10 personality disorders,11 addiction,12 eating disorders,13 and obsessive-compulsive disorder.14
Among the elements involved in the therapeutic alliance, previous research has highlighted its relationship with patient dropout,15,16 therapeutic failure,17,18 insight,8 participation in therapy and symptom reduction,19,20 commitment and satisfaction with therapy,21 and the results of the treatment.22 These findings indicate that the therapeutic alliance in psychotherapy is crucial for managing progress to prevent discontinuity and improve satisfaction outcomes. Additionally, as supported by a systematic review, these results suggest that therapeutic alliance plays a crucial role in influencing the effectiveness of the change process even across diverse patients, disorders, and settings.23
Previous research has found that sociodemographic aspects such as age and sex can play a significant role in the establishment of an adequate therapeutic alliance, particularly in the early stages of the sessions. For example, research with large samples has revealed significant differences according to sex in seeking psychological help,24 as well as a higher positive response to psychological therapy in older adults compared to young individuals.25 Despite these findings, differences according to sex and age in psychotherapy alliance have not been profoundly studied in the literature. Some research has identified that age may be a predictor of the quality of the therapeutic alliance in the context of online psychological therapy,26 while others have reported the effects of this variable on treatment improvement when therapists are younger than patients.27 Previous research with young adults, as a systematic review28 suggests that they are more willing to seek psychological support, particularly with therapists who establish a strong, friendly, and highly individualized relationship. This strengthened therapeutic alliance can play a significant role in motivating young adults to continue attending additional therapy sessions. However, studies specifically examining the influence of age on the therapeutic alliance are still limited in the scientific literature. Regarding sex, there is evidence that men are less likely to seek psychological care;29 however, when they do, they tend to focus more on intervention tasks than women.30 On the other hand, it has been observed that women tend to seek psychological help more than men,31 however, results regarding trust, commitment, and satisfaction with therapists of both sexes are mixed and vary across studies.27,32 Therefore, based on such evidence, it is necessary to continue investigating whether age and sex are relevant variables at the time of initiating or maintaining an adequate therapeutic relationship.
Due to the importance of the therapeutic alliance, several instruments have been developed for its study and measurement. These instruments have been designed in versions intended to be completed by both the therapist and the patient. A systematic review identified 32 different scales, questionnaires, and inventories to measure therapeutic alliance. Among these options, the Working Alliance Inventory in its patient version (WAI-P) stands out due to its solid theoretical support and psychometric properties tested in various populations.1,33 The WAI-P, developed by Horvath and Greenberg, is a widely used scale to assess therapeutic alliance.34 The original version consists of 36 items that are grouped into three main dimensions. The first dimension, called “Bonds”, refers to the establishment of an interpersonal bond based on trust, acceptance, and confidence between patient and the therapist. The second dimension, called “Goals”, involves the agreement between the patient and the therapist on therapeutic goals, which should be perceived as relevant and effective. The third dimension, called “Tasks”, focuses on the specific activities or tasks that will be carried out to achieve the therapeutic objectives and agreements previously established.34,35 However, there is also a short version called WAI-SP, which consists of 12 items developed by Tracey & Kokotovic.36
Although the WAI-SP is widely used, research that has evaluated the psychometric properties of the instrument has revealed inconsistencies in its internal structure; which were mostly examined by means of exploratory and confirmatory factor analysis, yielding divergent results of 1, 2, and 3 factors, including proposals for bifactor models.6,20,37 For example, the original WAI-SP study found that the bifactor model, which includes one general factor and three specific factors, had a better fit in both the patient and therapist versions,36 This measurement model has also been replicated in a study conducted in Norway.38 In addition, the three-factor correlated structure of the WAI-SP has been validated in different countries. For example, in Canada,39 Turkey,40 and Poland.41 Recent research also confirms this factorial model in Asian participants from China42 where favorable results were obtained for the bifactor model, and Thailand, where both the unidimensional and three-dimensional models are plausible, suggesting that both structures are equally valid for explaining the nature of the therapeutic alliance in that context.43 It has even been observed that the factor structure of the WAI-SP remains invariant over time, ie, it does not vary between different psychotherapeutic sessions.44 While other research focused only on evaluating the internal consistency of the instrument.33,45
On the other hand, an example of a study that proposed an alternative psychometric-theoretical model for the WAI-SP was carried out in Belgium, where a two-factor model was developed: contact and contract. These factors represent the interpersonal bond of trust and commitment to achieve the objectives agreed upon and positively accepted by the patient.46 This model has also been evaluated in other studies involving mental health professionals.47 It is important to note that, so far, none of the studies have investigated the invariance of the WAI-SP in relation to sex and age, despite evidence suggesting that both variables may influence the therapeutic alliance.26,27,32,48 Measurement invariance refers to the equivalence in the measurement of the therapeutic alliance between different groups, which is relevant to understanding whether the instrument measures consistently in different populations.
In Japan, evidence has been found to support the existence of two dimensions in the therapeutic alliance, which has led to the development of a unidimensional version of the WAI-SP with five items.45 In China, it has been observed that the three-dimensional model of the WAI-SP does not present a clear conceptual distinction due to the high correlations between its factors. As a result, a two-dimensional model of the instrument has been proposed, in which items 2 and 4 were eliminated.49
The main objective of this study is to analyze the psychometric properties of the WAI-SP in a sample of people from Peru who are receiving psychological therapy. This research is justified due to the lack of previous studies that have examined the validity and reliability of the WAI-SP in the Peruvian population. Therefore, having a brief tool that meets these characteristics can be very useful to assess the therapeutic alliance from the patient’s perspective in an easier and faster way. This is especially relevant, since the therapeutic alliance is a predictor of better outcomes in therapy and a lower dropout rate.15,16,22,23 As a second objective of the study, a network analysis was conducted to investigate the direct relationships between the therapeutic alliance and relevant sociodemographic variables, such as sex, age, and total session attendance. This complementary analysis seeks to take into account the differentiation of attributes that may influence trust and commitment in psychological interventions in Peruvian patients, which would help psychologists and psychiatrists to achieve better results in clinical practice.
Materials and Methods
Participants
The study included 241 participants (50.6% female) aged 18 to 72 years (M= 32.58, SD =12.67). Among them, 97.5% had secondary education, while 2.5% had higher education. Regarding the overall psychotherapeutic sessions, it was observed that 66% of the participants had attended between two and three sessions, 32% had attended between four and five sessions, and only 2% had attended six sessions or more. A non-probabilistic purposive convenience sampling approach was used, in which the sample selection was based on specific criteria of the researchers, taking into account the ease of access of the participants.50 The inclusion criteria used for the selection of participants were the following: to be over 17 years of age, to be Peruvian nationals, to have attended a minimum of 2 therapy sessions, and to reside in Lima. The sample size complied with the minimum required according to the calculator for models based on structural equation analysis. This calculator takes into account the number of variables used, both observable and latent, as well as the minimum predicted effect size (0.30, minimum for factor loadings), probability level (0.05), and statistical power (0.95).51
Measurement Instrument
Working Alliance Inventory-Short:36 It is a self-report instrument consisting of 12 items grouped into three dimensions, called task (1, 2, 10, and 12), bonds (3, 5, 7, and 9) and goals (4, 6, 8, and 11) measured through a Likert-type scale with scores ranging from 1 = Never to 7 = Always. There are versions for both therapists and patients. In this research, the version adapted to Spanish by Andrade-González & Fernández-Liria was used.52 Regarding the psychometric properties, the original research indicates a structure with three correlated and second-order dimensions, with adequate goodness-of-fit indices, which had a high internal consistency in general (α = 0.98) and in each of its components with 0.90, 0.92, and 0.90 for task, bond, and goal, respectively.36 In addition, the translated version showed that the WAI-SP was related to therapeutic changes in the client (R2 = 0.16).52
Procedure
First, permission for the use and administration of the instrument was requested via e-mail from the authors who translated it.52 Then, the linguistic adaptation process of the WAI-SP to the Peruvian context was carried out using the criteria of judges. This was done with the help of four psychologists specialized in psychotherapy and clinical psychology, who reside in the city of Lima. Each of the psychologists evaluated the 12 items that constitute the instrument on three criteria: relevance, pertinence, and clarity, which refer to the degree of importance, belonging to the dimension, and comprehension of the items, respectively. Then, the agreement between jurors was quantified with Aiken’s V, for which a cut-off point of 0.80 was taken into account.53
Data collection was carried out during the second semester of 2021 due to the persistence of the state of emergency in Peru due to COVID-19, which made it difficult to conduct face-to-face interviews or surveys. Instead of traditional face-to-face data collection methods, an online data collection method was used. Participants were recruited from a population-wide survey. For this purpose, a Google Form was implemented, which is a widely used tool in psychological research and follows the guidelines of the Internet-Based Methodology. In addition, it was ensured to comply with all ethical recommendations necessary to protect the privacy and confidentiality of the participants.
Before completing the questionnaire, each potential participant was provided with detailed information about the purpose of the study, the confidentiality of the data collected, and the voluntary and anonymous nature of their participation. In addition, it was ensured that all procedures carried out in the study adhered to the ethical standards established by article 81 of the Code of Ethics of the Peruvian College of Psychologists and the Declaration of Helsinki. The research protocol was reviewed and approved by the Research Ethics Committee of the Faculty of Health Sciences of the Universidad Peruana Unión (Approval number: N°00124-2020/UPeU/FCS/CIISA). Additionally, informed consent was obtained from the participants. Finally, the scores were imported into an Excel spreadsheet and then analyzed in the statistical software JAMOVI 2.3.24.
Data Analysis
The sociodemographic analysis of the participants was carried out by calculating frequencies, which made it possible to describe and summarize the sociodemographic characteristics of the sample. The quantification of the judges’ criteria was performed with Aiken’s V based on the scores obtained from the four expert judges in three criteria: relevance, clarity, and pertinence, where values greater than 0.80 were considered.53
Then, a preliminary analysis of the items was made using univariate statistics, such as kurtosis and skewness in order to determine whether the data follow a normal distribution. For this purpose, a cut-off point of ±1.5 was used.54 Next, a confirmatory factor analysis (CFA) was performed to examine the internal structure of the WAI-SP in accordance with previous studies. For this purpose, an oblique two-dimensional model and a bifactor model were created, due to the high correlations between them. Within the bifactor model, hierarchical omega coefficient measures were calculated for the specific factors (ωh) and for the general factor (ωH), since they allow considering the maximum reliability of the specific factors with a control of the influence of the overall factor, for which a ωH > 0.80 would indicate unidimensionality and a ωh > 0.30 would indicate substantiality of the specific factors. Calculation of the Extracted Common Variance (ECV) and the Percentage of Uncontaminated Correlations (PUC) with a value greater than 0.70 would provide additional evidence to conclude that the model is mainly unidimensional.55 The Dueber online calculator was used to analyze these additional indices of the bifactor model.56
The Unweighted Least Squares (ULS) estimator was used throughout due to its robustness to the assumption of normality of the data and its good performance in the analysis of ordinal variables.57 To evaluate the models, a CFI > 0.95, RMSEA < 0.06, and SRMR < 0.08 were taken into account.58 The model with the best fit was subjected to invariance according to sex and age, since both variables have been found to be involved in the therapeutic alliance;27,48 for this purpose, a cut-off point of CFI > 0.001 and RMSEA < 0.015 was taken into account.59 Internal consistency was evaluated with the omega coefficient, taking into account a cut-off point > 0.70.60
Finally, to evaluate the relationships with other categorical variables, network analysis was used. In this analysis, the connections between variables represent partial correlations, allowing the influence of the other variables in the network to be controlled. Network analysis is a useful tool for visualizing and understanding the interactions between variables and examining how they relate to each other. By using this approach, the structure and patterns of the network can be identified, as well as the relative importance of each variable in the context of the others. This provides a more complete understanding of the relationships between categorical variables and their influence on the phenomenon studied.61,62 In addition, the accuracy and robustness of the association weights were evaluated by running 3000 bootstrap samples.63
Finally, to assess the relationships between all study variables and sociodemographics, network analysis was employed as the methodology. This technique represents connections (edges or lines) between nodes (circles representing variables), forming a global system that activates each variable to a varying degree. The network analysis module of the JASP software was used, applying the partial correlation estimator to control for the influence of all introduced variables, isolating only the “true” partial relationships between each variable.58,59 In the network, blue paths are interpreted as positive partial correlations, and red paths, negative partial correlations. Additionally, to evaluate the stability and precision60 of the associations, 2000 bootstrap samples were generated, producing multiple network samples from the observed data. This demonstrated a tendency to obtain the same associations reported in this study.
Results
The results of the CFA are shown in Table 1. It is observed that both the two and three correlated dimensions models presented the same fit indices (CFI = 0.965; TLI = 0.955; SRMR = 0.085; RMSEA = 0.082). However, in the original three-factor model, saturations of lower magnitude were observed (between 0.330 and 0.862), and the dimensions presented reliability values between 0.62 and 0.70. Furthermore, these dimensions showed a high correlation with each other (between 0.931 and 1.094). These questionable findings could indicate a poor fit of the data to the proposed model.64 Regarding the two-dimensional model, item 3 presented lower saturation (λ = 0.333), while item 8 had higher factorial weight (λ = 0.863). However, the interfactor correlation was r= 0.98, therefore a bifactor model was created (general factor and three specific dimensions), whose goodness-of-fit indices were optimal (CFI = 0.983; TLI = 0.973; SRMR = 0.067; RMSEA = 0.064). As for the factor loadings of specific dimensions, there are items with saturations below 0.30, such as items 4, 8, 10, 11, and 12, which are part of the “contract” factor, and 7 and 9, which belong to the “contact” factor. In contrast, the general factor reports factor loadings greater than 0.30.
 |
Table 1 Factorial Models of the Short Version of the Work Alliance Inventory |
On the other hand, other goodness-of-fit indices that allow a more precise interpretation were calculated, such as the ECV, PUC, and ωH. The results showed a ωH value of 0.830, an ECV of 0.748, and a PUC of 0.485. Based on these values, it can be concluded that the WAI-SP is essentially unidimensional.
Because the bifactor model had better fits, factorial invariance was carried out with this structure. The results are shown in Table 2, where it is observed that metric, scalar and strict invariance are met, when sex was taken into account, thus the variance was < 0.01 and < 0.015 for ΔCFI and ΔRMSEA, respectively. Regarding age, the results were similar. Therefore, it is concluded that the WAI-SP meets with the equivalence of measurement according to sex and age.
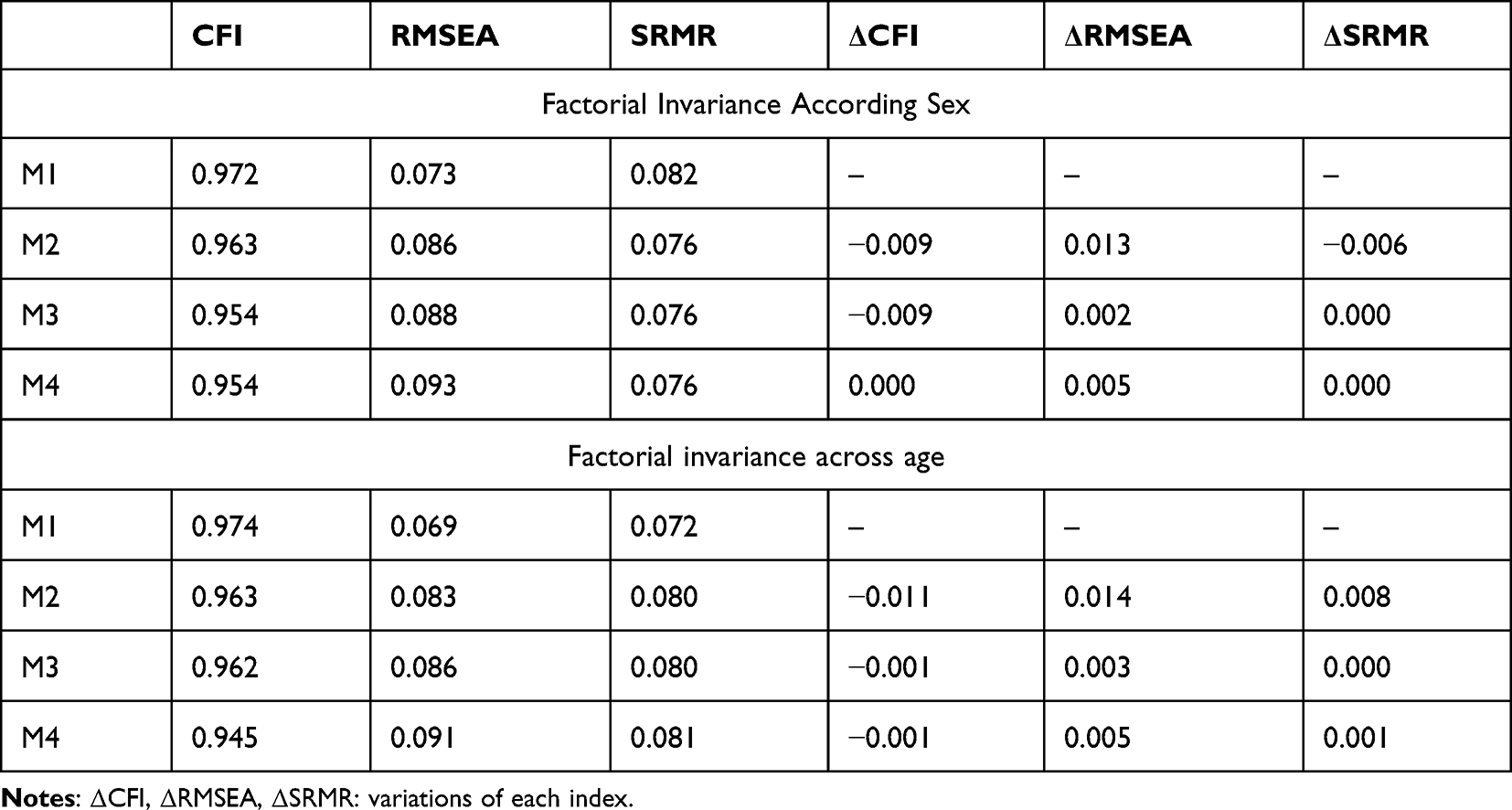 |
Table 2 Factorial Invariance According Sex and Age of the Short Version of the Working Alliance Inventory |
In addition, a network was estimated that included the therapeutic alliance variables along with other sociodemographic variables such as sex and age. This network is illustrated in Figure 1. In the network analysis, a positive relationship was identified between the total session attendance and the therapeutic alliance, suggesting that as participants attended more sessions, their alliance related to compromise and achieving therapy goals was also greater. In addition, it was observed that men reported a higher therapeutic alliance compared to women, while women showed a higher total psychotherapy session attendance. On the other hand, data revealed a negative association between age and total session attendance, indicating that younger individuals tended to have a higher total number of therapy sessions. Finally, a small but significant direct relationship was found between age and therapeutic alliance.
 |
Figure 1 Network analysis including therapeutic alliance, sex, age, and total session attendance. Notes: Blue paths indicate positive associations; red paths indicate negative associations. Regarding sex, dummy codes were 1=men, 2=women. |
Discussion
The therapeutic alliance is one of the fundamental factors that influence the success or failure of psychotherapy regardless of the therapeutic approach, the reason for consultation, and diagnosis.7 Different instruments have been developed to assess the therapeutic alliance; however, one of the most widely used is the short version of the Working Alliance Inventory for Patients (WAI-SP), which has not yet been validated in the Peruvian context. In this sense, the first objective of this research was to examine the psychometric properties of this tool in the Peruvian population who attend psychological therapy.
Initially, after performing the analyses with three different factorial structures, it was observed that the bidimensional model showed good fit indices compared to the trifactorial model. The bidimensional model was generated from two main dimensions: “contact” (resulting from the high correlation between the original “task” and “goals” factors) and “contract”. This factorial model was also used in adults in Belgium46 and the Netherlands.47 In the Japanese context, favorable results supporting the two-dimensional structure of the instrument were observed in patients with musculoskeletal conditions.45 Similarly, in China, significant correlations were found between the dimensions of the instrument, supporting a bidimensional model.49 This finding has also been replicated in Spain, where evidence of two-dimensional structure was obtained through exploratory factor analysis.6 However, it is important to note that in the two-factor solution, high correlations were also observed between the “contact” and “contract” dimensions, suggesting a lack of a clear conceptual distinction between these dimensions. Therefore, the possibility of considering bifactor structures that include general and specific components instead of a completely bidimensional model is raised.
After considering the significant correlations between the factors, we proceeded to evaluate a bifactor model, which provided a better representation of the factor structure of the therapeutic alliance scale. This model includes the dimensions of “contact” (bonding) and “contract” (therapeutic goal orientation), which showed some overlap between them. The bifactor approach is a valuable tool to describe more precisely the structure of psychological variables, allowing the analysis of complementary and more complex dimensions. Unlike other factor models, the bifactor model offers the advantage that items can belong to both a general factor and specific factors at the same time.65 This representation at the psychometric level is consistent in capturing the integrative model of the therapeutic alliance proposed by Bordin.3 According to Bordin, the therapeutic alliance has a common general characteristic and encompasses several more specific domains that influence the quality and strength of the patient-therapist relationship. In this context, the affective component of the bond with the therapist and the active commitment to self-improvement can be considered complementary, as both aspects influence the patient’s overall perception of the ongoing therapeutic relationship.66 These findings indicated evidence in favor of the estimated model, thus the WAI-SP should be considered as essentially unidimensional.55 Such results were previously reported in different countries, including the original WAI-SP model in the United States, which had a strong influence of the general factor on the items, although indices such as ECV or hierarchical omega were not reported.66 In China, favorable results were obtained for the bifactor model, indicating that this model is adequate to describe the structure of the therapeutic alliance in that population.42 On the other hand, in Thailand, both the unidimensional and three-dimensional models are plausible, suggesting that both structures are equally valid for explaining the nature of the therapeutic alliance in that context.43 Regarding reliability, the results showed a coefficient above what was suggested to conclude that the unidimensionality of the WAI-SP would be more appropriate, which coincides with the antecedents.36,42,43 These findings highlight the importance of considering cultural and contextual differences when investigating the structure of the therapeutic alliance, as there may be variations in how patients perceive and experience the relationship with their therapist.
To date, there have been no studies examining the invariance of the therapeutic alliance according to sex and age, despite the fact that a relationship between these variables and the therapeutic alliance has been observed.26 Concerning to sex, studies have found that there tends to be a greater alliance when the sex of the therapist and the patient coincide.67 Consequently, the results obtained from the equivalence analysis of the WAI-SP provide an opportunity to evaluate the effects of sex and age, as the instrument has been shown to be invariant with respect to these two factors. This means that any differences found in the therapeutic alliance between different demographic groups cannot be attributed to measurement bias.
Regarding the results of associations through network analysis, the therapeutic alliance was mainly correlated with male participants, which could have some explanatory hypotheses. Previous research has reported that men tend to show lower emotional expression and seek less psychological help.29,68 However, when engaged in therapy, this group may exhibit higher therapeutic commitment from the beginning due to the culturally associated role of problem-solving quickly and showing efficacy, avoiding feelings of vulnerability in front of others.29 This tendency could also be supported by studies suggesting that men tend to have a greater task orientation and focus on achieving practical outcomes during therapy, which might foster increased collaboration in tasks and goals with the therapist.30 In addition, correlations were found between women and higher session attendance. This finding is in line with previous studies that report a higher prevalence of women seeking psychological help for various reasons (eg, sex of the therapist, need to be heard, among others).27 This tendency may be related to women’s predisposition to explore and express emotions, which may motivate them to seek professional help to address and manage their problems, even if they are not necessarily related to mental disorders.69
An additional finding revealed that the therapeutic alliance showed a direct association both with age and total session attendance. Older people tend to accumulate more life experiences and have greater emotional maturity, which may lead them to show a greater willingness and commitment to work on their well-being through therapy.70 In addition, it is important to note that as more therapeutic sessions are conducted, the opportunity to establish a trusting and collaborative relationship increases, which may contribute to better intervention outcomes. However, these findings need to be corroborated in larger samples to obtain more solid conclusions.71 Finally, the negative relationship between age and attendance at network sessions indicates that younger patients attended a greater number of psychotherapy sessions. Finally, the negative relationship between age and total attendance sessions suggests that there may be differences in the perception and needs of interventions compared to older adults. These findings highlight the importance of considering the specific characteristics and demands of different age groups when designing and delivering psychotherapy services. In the Peruvian context, young adults often face socioeconomic challenges and are in a transitional stage in which they must assume new responsibilities and make important decisions. This combination of factors can generate a greater need for personal exploration and psychological support.72 In addition, young adults are often more willing to seek counseling or psychological support, especially when they find therapists who establish a strong, friendly relationship tailored to their individual needs. This age group may be more receptive to participating in the therapeutic process and exploring emotional and personal issues in a safe and trusting environment. When a strong therapeutic alliance is established and they feel understood and supported, young adults can make the most of the psychotherapy sessions and work on areas of personal development and emotional well-being.28 Indeed, the strength of the therapeutic relationship may be a motivating factor for young adults to continue to attend more therapy sessions.
Strengths and Limitations
This research has limitations in terms of the generalizability of the results due to the use of a non-probability sampling method. In addition, being a cross-sectional study, neither the temporal stability of internal consistency nor longitudinal invariance can be assessed.44 Another relevant limitation was the relatively low total number of psychotherapy sessions, specifically fewer than six sessions. Caution should be exercised when interpreting the results, or at least, considering that therapeutic alliance was primarily assessed during the initial five sessions, also focusing on Peruvian adults in a context of post-pandemic recovery. Additionally, this research did not take into account certain variables that could influence the association findings, such as the type of psychotherapy used, the sex or age of the therapists, as well as the severity of the patients’ diagnosis. These variables can play a significant role in the therapeutic relationship and psychotherapy outcomes. For example, different psychotherapy approaches may have different emphases on the therapeutic relationship and the strategies used. Similarly, the severity of the diagnosis may affect the duration and intensity of therapy, as well as the perception of the therapeutic alliance.
It is important to consider these variables in future research to obtain a more complete and accurate understanding of the therapeutic relationship and its effects. These factors can provide additional information on how the therapeutic alliance is developed and maintained, as well as its impact on treatment outcomes. By taking these variables into account, a more complete picture of the influence of various factors on the therapeutic relationship can be obtained and ultimately improve the quality of psychotherapy and outcomes for patients. However, the main objective was to validate a therapeutic alliance assessment instrument in Peruvian patients, offering a relevant tool for evaluating the quality therapeutic relationships in Latin America.
The study also presents strengths, such as being the first psychometric study that analyzes the WAI-SP in Peruvian patients, which is valuable for psychologists and psychiatrists in their clinical and research practice. In addition, it is important to note that this research is pioneering in providing evidence on the invariance of WAI-SP in relation to sex and age, which contributes significantly to the existing knowledge in this field. Likewise, associations with relevant variables such as sex, age, and total session attendance have been evidenced, which complements information for future comparative studies and administration to patients with different characteristics. These findings open new perspectives for understanding how sex and age may influence the perception and experience of the therapeutic alliance, and may have important implications for clinical practice and the tailoring of therapeutic interventions.
Conclusion
In conclusion, the results of this study indicate that the Peruvian version of the WAI-SP presents a good fit for a bifactor model, which is invariant according to the sex and age of the participants. Therefore, it should be interpreted as essentially unidimensional. Likewise, this structure has an adequate internal structure. Consequently, it is valid, reliable, and invariant.
Finally, in addition to the psychometric examination, network analysis findings suggest that the sex and age of Peruvian patients may represent significant variables to improve specific trust needs and psychotherapeutic goals. However, these preliminary results require further investigation to determine if such sociodemographic variables need to be considered in tailoring interventions to strengthen the therapeutic alliance in adults based on age groups or sexes. This approach, in future studies, will optimize therapeutic outcomes and foster greater effectiveness in the psychological treatment process.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Elvins R, Green J. The conceptualization and measurement of therapeutic alliance: an empirical review. Clin Psychol Rev. 2008;28(7):1167–1187. doi:10.1016/j.cpr.2008.04.002
2. Anderson RP, Anderson GV. Development of an instrument for measuring rapport. Pers Guid J. 1962;41(1):18–24. doi:10.1002/j.2164-4918.1962.tb02226.x
3. Bordin ES. The generalizability of the psychoanalytic concept of the working alliance. Psychotherapy. 1979;16(3):252–260. doi:10.1037/h0085885
4. Luborsky L, Crits-Christoph P, Alexander L, Margolis M, Cohen M. Two helping alliance methods for predicting outcomes of psychotherapy. A counting signs vs. a global rating method. J Nerv Ment Dis. 1983;171(8):480–491. doi:10.1097/00005053-198308000-00005
5. Luis Botella SC. Alianza terapéutica evaluada por el paciente y mejora sintomática a lo largo del proceso terapéutico. Boletín Psicol. 2011;101:21–33.
6. Corbella S, Botella L, Gómez AM, Herrero O, Pacheco M. Psychometric characteristics of the Spanish version of the Working Alliance Inventory-Short (WAI-S). An Psicol Ann Psychol. 2011;27(2):298–301.
7. Impala T, Dobson KS, Kazantzis N. Does the working alliance mediate the therapist competence-outcome relationship in cognitive behavior therapy for depression? Psychother Res. 2022;32(1):16–28. doi:10.1080/10503307.2021.1946195
8. Misdrahi D, Petit M, Blanc O, Bayle F, Llorca PM. The influence of therapeutic alliance and insight on medication adherence in schizophrenia. Nord J Psychiatry. 2012;66(1):49–54. doi:10.3109/08039488.2011.598556
9. Keller SM, Zoellner LA, Feeny NC. Understanding Factors associated with early therapeutic alliance in PTSD treatment: adherence, childhood sexual abuse history, and social support. J Consult Clin Psychol. 2010;78(6):974. doi:10.1037/a0020758
10. Pihlaja S, Stenberg JH, Joutsenniemi K, Mehik H, Ritola V, Joffe G. Therapeutic alliance in guided internet therapy programs for depression and anxiety disorders - A systematic review. Internet Interv. 2017;11:1–10. doi:10.1016/j.invent.2017.11.005
11. Bedics JD, Atkins DC, Harned MS, Linehan MM. The therapeutic alliance as a predictor of outcome in dialectical behavior therapy versus nonbehavioral psychotherapy by experts for borderline personality disorder. Psychotherapy. 2015;52(1):67–77. doi:10.1037/a0038457
12. van Benthem P, Spijkerman R, Blanken P, Kleinjan M, Vermeiren RRJM, Hendriks VM. A dual perspective on first-session therapeutic alliance: strong predictor of youth mental health and addiction treatment outcome. Eur Child Adolesc Psychiatry. 2020;29(11):1593–1601. doi:10.1007/s00787-020-01503-w
13. Zaitsoff S, Pullmer R, Cyr M, Aime H. The role of the therapeutic alliance in eating disorder treatment outcomes: a systematic review. Eat Disord. 2015;23(2):99–114. doi:10.1080/10640266.2014.964623
14. Wheaton MG, McIngvale E, Van Meter AR, Björgvinsson T. Quality of the therapeutic working alliance as a factor in intensive residential treatment of obsessive-compulsive disorder. Psychother Res. 2023;33(4). doi:10.1080/10503307.2022.2138618
15. Murphy ST, Garcia RA, Cheavens JS, Strunk DR. The therapeutic alliance and dropout in cognitive behavioral therapy of depression. Psychother Res. 2022;32(8):995–1002. doi:10.1080/10503307.2021.2025277
16. Sharf J, Primavera LH, Diener MJ. Dropout and therapeutic alliance: a meta-analysis of adult individual psychotherapy. Psycho Theory Res Pract Train. 2010;47(4):637–645. doi:10.1037/a0021175
17. Moshe-Cohen R, Kivity Y, Huppert JD, et al. Agreement in patient-therapist alliance ratings and its relation to dropout and outcome in a large sample of cognitive behavioral therapy for panic disorder. Psychother Res. 2022;2022:1–3.
18. Weck F, Grikscheit F, Jakob M, Höfling V, Stangier U. Treatment failure in cognitive-behavioural therapy: therapeutic alliance as a precondition for an adherent and competent implementation of techniques. Br J Clin Psychol. 2015;54(1):91–108. doi:10.1111/bjc.12063
19. Bartle-Haring S, Walsh L, Blalock J, Bryant A. using therapeutic alliance to predict treatment attendance among couples. Contemp Fam Ther. 2021;43(4):370–381. doi:10.1007/s10591-021-09602-9
20. Fayed C, Bartle-Haring S, VanBergen A. Interpersonal Trauma, therapeutic alliance and relationship satisfaction: a dyadic examination. Contemp Fam Ther. 2021;1–14. doi:10.1007/s10591-021-09595-5
21. Thompson SJ, Bender K, Lantry J, Flynn PM. Treatment engagement: building therapeutic alliance in home-based treatment with adolescents and their families. Contemp Fam Ther. 2007;29(1–2):39. doi:10.1007/s10591-007-9030-6
22. Lin T, Anderson T, Austin M, Mischkowski D. Early trajectories of symptom change and working alliance as predictors of treatment outcome. Psychother Res. 2023;33(2):185–197. doi:10.1080/10503307.2022.2080028
23. Doorn K A-V, Bar-Sella A, Zilcha-Mano S, et al. Within-patient perceptions of alliance and attunement: associations with progress in psychotherapy. Clin Psychol Psychother. 2022;29(5):1717–1727. doi:10.1002/cpp.2737
24. Nam SK, Chu HJ, Lee MK, Lee JH, Kim N, Lee SM. A meta-analysis of gender differences in attitudes toward seeking professional psychological help. J Am Coll Health. 2010;59(2):110–116. doi:10.1080/07448481.2010.483714
25. Saunders R, Buckman JEJ, Stott J, et al. Older adults respond better to psychological therapy than working-age adults: evidence from a large sample of mental health service attendees. J Affect Disord. 2021;294:85–93. doi:10.1016/j.jad.2021.06.084
26. Herrero R, Vara MD, Miragall M, et al. Working alliance inventory for online interventions-short form (WAI-TECH-SF): the role of the therapeutic alliance between patient and online program in therapeutic outcomes. Int J Environ Res Public Health. 2020;17(17):1–16. doi:10.3390/ijerph17176169
27. Behn A, Davanzo A, Errázuriz P. Client and therapist match on gender, age, and income: does match within the therapeutic dyad predict early growth in the therapeutic alliance? J Clin Psychol. 2018;74(9):1403–1421. doi:10.1002/jclp.22616
28. Kim HS, Munson MR, McKay MM. Engagement in mental health treatment among adolescents and young adults: a systematic review. Child Adolesc Soc Work J. 2012;29(3):241–266. doi:10.1007/s10560-012-0256-2
29. Van Der Heijden B, Mahoney CB, Xu Y. Impact of job demands and resources on nurses’ burnout and occupational turnover intention towards an age-moderated mediation model for the nursing profession. Int J Environ Res Public Heal. 2019;16(11):2011. doi:10.3390/ijerph16112011
30. Seidler ZE, Rice SM, Ogrodniczuk JS, Oliffe JL, Dhillon HM. Engaging men in psychological treatment: a scoping review. Am J Mens Health. 2018;12(6):1882–1900. doi:10.1177/1557988318792157
31. José F, Javier F, Paz M. Sistema de Información Científica A study of patients who go to a psychology clinic seeking treatment. Span J Psychol. 2012;15(1):275–285. doi:10.5209/rev_SJOP.2012.v15.n1.37334
32. Bedi RP, Richards M. What a man wants: the male perspective on therapeutic alliance formation. Psychotherapy. 2011;48(4):381–390. doi:10.1037/a0022424
33. Ribeiro NS, Colugnati FAB, Kazantzis N, Sartes LMA. Observing the working alliance in videoconferencing psychotherapy for alcohol addiction: reliability and validity of the Working Alliance Inventory short revised observer. Front Psychol. 2021;12:647814. doi:10.3389/fpsyg.2021.647814
34. Horvath AO, Greenberg LS. Development and Validation of the Working Alliance Inventory. J Couns Psychol. 1989;36(2):223–233. doi:10.1037/0022-0167.36.2.223
35. Horvath AO, Luborsky L. The role of the therapeutic alliance in psychotherapy. J Consult Clin Psychol. 1993;61(4):561–573. doi:10.1037/0022-006X.61.4.561
36. Tracey TJ, Kokotovic AM. Factor Structure of the Working Alliance Inventory. Psychol Assess. 1989;1(3):207–210. doi:10.1037/1040-3590.1.3.207
37. Paap D, Karel YH, Verhagen AP, Dijkstra PU, Geertzen JHB, Pool G. The Working Alliance Inventory’s measurement properties: a systematic review. Front Psychol. 2022;13. doi:10.3389/fpsyg.2022.945294
38. Hukkelberg S, Ogden T. General and specific factors of working alliance in parent training: a bifactor exploratory structural equation modelling approach. Psychother Res. 2019;29(2):267–276. doi:10.1080/10503307.2017.1330574
39. Milot-Lapointe F, Le Corff Y, Savard R. Factor Structure of the short version of the Working Alliance Inventory and its longitudinal measurement invariance across individual career counseling sessions. J Career Assess. 2020;28(4):693–705. doi:10.1177/1069072720925048
40. Gülüm IV, Uluç S, Soygüt G. Psychometric properties of the Turkish Working Alliance Inventory - Short form. Turk Psikiyatr Derg. 2018;29:1.
41. Prusiński T. Patients’ and psychotherapists’ combined and separate evaluations of the psychotherapeutic relationship: the structure of Working Alliance and Polish Versions of the WAI. J Contemp Psychother. 2021;51(4):323–329. doi:10.1007/s10879-021-09500-z
42. Li X, Zhao H, Wu M, Li F, Hill CE. The development of a Brief Working Alliance Inventory for clients and therapists using multilevel factor analysis and item response theory in the United States and China. J Couns Psychol. 2023;70(2). doi:10.1037/cou0000655
43. Leangsuksant T, Taephant N. Development and validation of the Working Alliance Inventory short form Thai client version. Asia Pacific J Couns Psychother. 2022;13(1):40–52.
44. Stefens M, Rondeel E, Templin J, et al. Longitudinal measurement invariance of the Working Alliance Inventory - Short form across coaching sessions. BMC Psychol. 2022;10(1):1–13. doi:10.1186/s40359-022-00968-5
45. Takasaki H, Miki T, Hall T. Development of the Working Alliance Inventory-Short Form Japanese version through factor analysis and test-retest reliability. Physiother Theory Pract. 2020;36(3):444–449. doi:10.1080/09593985.2018.1487492
46. Smits D, Luyckx K, Smits D, Stinckens N, Claes L. Structural characteristics and external correlates of the Working Alliance Inventory-Short Form. Psychol Assess. 2015;27(2):545–551. doi:10.1037/pas0000066
47. Oudshoorn CEM, Frielink N, Riper H, Embregts PJCM. Measuring working alliance and technical alliance from the perspective of healthcare professionals working with people with mild intellectual disabilities: adaptation, factor structure and reliability. J Intellect Disabil Res. 2023;67(1):49–63. doi:10.1111/jir.12986
48. Graves TA, Tabri N, Thompson-Brenner H, et al. A meta-analysis of the relation between therapeutic alliance and treatment outcome in eating disorders. Int J Eat Disord. 2017;50(4):323–340. doi:10.1002/eat.22672
49. Hsu S, Zhou RD-H, Yu -CK-C. A Hong Kong validation of Working Alliance Inventory – short form – client. Asia Pacific J Couns Psychother. 2016;7(1–2):69–81.
50. Otzen T, Manterola C. Sampling Techniques on a Population Study. Int J Morphol. 2017;35(1):227–232. doi:10.4067/S0717-95022017000100037
51. Ramos-Vera CA, Ramos-Vera CA. A sample size calculation method for a priori power analysis in structural equation models. Rev Cuerpo Med Hosp Nac Almanzor Aguinaga. 2021;14(1):104–105.
52. Andrade-González N, Fernández-Liria A. Spanish Adaptation of the Working Alliance Inventory (WAI): psychometric properties of the patient and therapist forms (WAI-P and WAI-T). An Psicol. 2015;31(2):524–533. doi:10.6018/analesps.31.2.177961
53. Mayaute LME. Cuantificación de la validez de contenido por criterio de jueces. Rev Psicol. 1988;6(1–2):103–111.
54. Pérez ER, Medrano L. Exploratory factor analysis: conceptual and methodological bases. Rev Argent Cienc Comport. 2010;2(1):58–66.
55. Dominguez-Lara S, Rodriguez A. Statistical indices of bifactor models. Interacciones Rev Av en Psicol. 2017;3(2):59–65.
56. Dueber DM. Bifactor Indices calculator: a Microsoft Excel-based tool to calculate various indices relevant to bifactor CFA models. Educ Sch Couns Psychol Res Tools. 2017;2017:1.
57. Forero CG, Maydeu-Olivares A, Gallardo-Pujol D. Factor analysis with ordinal indicators: a monte carlo study comparing DWLS and ULS estimation. Struct Equ Model a Multidiscip J. 2009;16(4):625–641. doi:10.1080/10705510903203573
58. Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Structural Equ Model a Multidiscip J. 2009;6(1):1–55.
59. Chen FF. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct Equ Model. 2007;14(3):464–504. doi:10.1080/10705510701301834
60. Viladrich C, Angulo-Brunet A, Doval E. A journey around alpha and omega to estimate internal consistency reliability. An Psicol. 2017;33(3):755–782. doi:10.6018/analesps.33.3.268401
61. Ramos-Vera C. Statistical relationship networks in nutrition research. Nutr Hosp. 2021;38:671–672. doi:10.20960/nh.03522
62. Ramos-Vera C, Barrientos AS, Baños-Chaparro J, Saldarriaga JV, Saintila J. Enneagram typologies and healthy personality to psychosocial stress: a network approach. Front Psychol. 2022;13:7517. doi:10.3389/fpsyg.2022.1051271
63. Borsboom D, Robinaugh DJ, Rhemtulla M, Cramer AOJ. Robustness and replicability of psychopathology networks. World Psychiatry. 2018;17:143–144. doi:10.1002/wps.20515
64. Freiberg Hoffmann A, Stover JB, De la Iglesia G, Fernández Liporace M. Development of an instrument for measuring rapport Polychoric and tetrachoric correlations in exploratory and confirmatory factorial studies. Ciencias Psicológicas. 2013;151–164. doi:10.22235/cp.v7i1.1057
65. Rodriguez A, Reise SP, Haviland MG. Applying bifactor statistical indices in the evaluation of psychological measures. J Pers Assess. 2016;98(3):223–237. doi:10.1080/00223891.2015.1089249
66. Corbière M, Bisson J, Lauzon S, Ricard N. Factorial validation of a French short-form of the Working Alliance Inventory. Int J Methods Psychiatr Res. 2006;15(1):36–45. doi:10.1002/mpr.27
67. Wintersteen MB, Mensinger JL, Diamond GS. Do gender and racial differences between patient and therapist affect therapeutic alliance and treatment retention in adolescents? Prof Psychol Res Pract. 2005;36(4):400–408. doi:10.1037/0735-7028.36.4.400
68. Wendt D, Shafer K. Gender and attitudes about mental health help seeking: results from national data. Health Soc Work. 2016;41(1):e20–8. doi:10.1093/hsw/hlv089
69. Thompson AE, Anisimowicz Y, Miedema B, Hogg W, Wodchis WP, Aubrey-Bassler K. The influence of gender and other patient characteristics on health care-seeking behaviour: a QUALICOPC study. BMC Fam Pract. 2016;17(1):1–7. doi:10.1186/s12875-016-0440-0
70. Knight BG, Poon CYM. Contextual adult life span theory for adapting psychotherapy with older adults. J Ration Cogn Ther. 2008;26(4):232–249. doi:10.1007/s10942-008-0084-7
71. Tiemens B, Kloos M, Spijker J, Ingenhoven T, Kampman M, Hendriks GJ. Lower versus higher frequency of sessions in starting outpatient mental health care and the risk of a chronic course; a naturalistic cohort study. BMC Psychiatry. 2019;19(1):228. doi:10.1186/s12888-019-2214-4
72. Kielmann K, Vidal N, Riekstina V, et al. “Treatment is of primary importance, and social assistance is secondary”: a qualitative study on the organisation of tuberculosis (TB) care and patients’ experience of starting and staying on TB treatment in Riga, Latvia. PLoS One. 2018;13(10):e0203937. doi:10.1371/journal.pone.0203937
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychometric Properties of the Chinese Version of 20-Item Zimbardo Time Perspective Inventory (C-ZTPI-20) in Chinese Adolescent Population
Chen Y, Liu TH, Xia Y, Ma Z
Psychology Research and Behavior Management 2024, 17:1271-1282
Published Date: 20 March 2024