Back to Journals » Vascular Health and Risk Management » Volume 19
Validation of the Withings BPM Core Device for Self-Blood Pressure Measurements in General Population According to the Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization Universal Standard
Authors Hakobyan Z ![]() , Zelveian P
, Zelveian P ![]() , Topouchian J, Hazarapetyan L
, Topouchian J, Hazarapetyan L ![]() , Asmar R
, Asmar R ![]()
Received 19 March 2023
Accepted for publication 27 June 2023
Published 3 July 2023 Volume 2023:19 Pages 391—398
DOI https://doi.org/10.2147/VHRM.S413195
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Harry Struijker-Boudier
Zoya Hakobyan,1 Parounak Zelveian,1 Jirar Topouchian,2 Lusine Hazarapetyan,1,3 Roland Asmar4
1Institute of Cardiology After Levon Hovhannisyan, Yerevan, Armenia; 2Diagnosis and Therapeutic Center, Hôtel Dieu Hospital, Paris, France; 3Yerevan State Medical University After Mkhitar Heratsi, Yerevan, Armenia; 4Foundation-Medical Research Institutes (F-MRI), Geneva, Switzerland
Correspondence: Roland Asmar, Foundation-Medical Research Institutes, Place St Gervais 1, Geneva, Switzerland, Tel +33640142239, Email [email protected]
Background: Most of the scientific societies recommend assessing the accuracy of electronic devices for blood pressure (BP) measurements using established validation protocol.
Objective: To determine the accuracy of the BP measurements using the Withings BPM Core device in the general population according to the “Universal Standard (ISO 81060-2:2018/AMD 1:2020)”.
Methods: The Withings BPM Core is an oscillometric device measuring BP at the brachial level. The study was performed according to the “Universal Standard (ISO 81060-2:2018/AMD 1:2020) protocol” using the same-arm sequential BP measurement method. Subjects (n ≥ 85) fulfilling the age, gender, BP, and cuff distribution criteria of the protocol were included. Analysis was performed as required by the Universal protocol using Criterion 1 – differences between observers’ mercury sphygmomanometer reference measurements and test device BP values (test versus reference) and their standard deviation (SD); and Criterion 2 – The SD of the mean BP differences between the test device and reference BP per subject.
Results: Eighty-six subjects were selected, 85 of whom were included. The mean BP differences between the simultaneous two observers’ measurements were − 0.2 ± 2.1 mmHg for systolic BP (SBP) and 0.3 ± 2.1 mmHg for diastolic BP (DBP). For validation criterion 1, the mean difference ± SD between the reference and device BP values was − 0.6 ± 4.8 mmHg for SBP and 0.1 ± 3.7 mmHg for DBP (≤ 5 ± 8 mmHg for both SBP and DBP). For criterion 2, the SD of the mean BP differences between the test device and reference BP per subject was 3.2/2.6 mmHg for SBP and DBP (≤ 6.91/6.95 mmHg).
Conclusion: The results of this study showed that the Withings BPM Core oscillometric device for home BP measurement fulfilled the accuracy requirements of the (ISO 81060-2:2018/AMD 1:2020) Universal protocol in the general population.
Keywords: blood pressure measurements, accuracy, validation, home blood pressure, oscillometric, Withings
Introduction
Blood pressure (BP) measurement is the most common medical procedure in clinical practice. Usually, it is performed by healthcare professionals to define the BP level in individuals and its consequences in terms of hypertension and other health conditions.1,2 BP measurement is also performed by individuals to evaluate their cardiovascular conditions or by patients to perform home BP monitoring of their hypertension as recommended by the guidelines.3 Thus, the accuracy of BP measurements is of great importance to avoid errors, the consequences of which can be very harming in terms of misclassification, under or over treatment.4,5
For more than ten years, with the end of the marketing of mercury manometers, we have witnessed a proliferation of electronic devices for automatic measurement of BP. According to several scientific societies/authorities,1,2,5 these devices must undergo independent clinical validation following recognized protocol in experienced centers. Several protocols have been used to assess the accuracy of BP measuring devices.6–8 In 2018, a consensus has been reached among the members of the American Advancement of Medical Instrumentation (AAMI), the European Society of Hypertension (ESH) and the International Organization for Standardization (ISO) to adopt a single optimal validation standard, the “AAMI/ESH/ISO Universal Standard” (ISO 81060-2:2018) and its amendment in 2020 (ISO 81060-2:2018/AMD 1:2020).9–12 Therefore, for any new BP device, assessment of its accuracy according to this protocol, as well as the publication of its results, is needed for listing the device as “recommended” in selected professional websites.13
Recently, our team published in this journal the validation results of the Withings BPM Connect device in the general population14 and in pregnant women.15 The objective of this study is to determine the accuracy of a new different BP monitor, the Withings BPM Core device for home BP measurement in the general population, according to the Universal Standard (ISO 81060-2:2018/AMD 1:2020).10–12 This device has never been validated previously; this is the first study assessing its accuracy according to the (ISO 81060-2:2018/AMD 1:2020) protocol.
Methods
Study Design
This prospective non-interventional, non-randomized, study using a Type IIa medical device was approved by the ethics committee of the Institute of Cardiology (Yerevan, Armenia). The study was performed according to the Universal Standard (ISO 81060-2:2018/AMD 1:2020)10,12 in compliance with the Declaration of Helsinki and ICH Good Clinical Practice guidelines. The recommendations of the ISO 81060-2:2018/AMD 1:2020 for performing and reporting this validation study were strictly followed.
Study Population
The (ISO 81060-2:2018/AMD 1:2020) protocol requires a population of ≥85 subjects to be included, with 3 pairs of BP measurements per subject, thus a minimum of (85x3) 255 pairs of BP measurements using the reference sphygmomanometer and the tested device is needed. This population must meet the requirements of the protocol in terms of gender, BP ranges, and arm circumference distributions. The inclusion criteria were treated or untreated patients, age >18 years, arm circumference between 22 cm and 42 cm, the last 2 criteria being in accordance with the instructions for use of the Withings BPM Core device. The exclusion criteria were arrhythmia, poor quality of Korotkoff sounds, patient unable to give consent or properly understand the protocol information, patient with an open wound and/or damaged skin in both upper arms, patient wearing an implantable electrical medical device, the latter being in accordance with the instructions for use of the Withings BPM Core device. A written consent form was obtained from all included patients.
Test Device
The WITHINGS BPM CORE (WPM04) is a new digital automatic oscillometric device for home BP measurement at the brachial level developed by Withings SA (Issy-Les-Moulineaux France) (Figure 1). The device has a pressure range of 0–285 mmHg and pulse rate range of 40–180 beats/min. The BP measurement is performed during the inflation phase, while the pump increases the pressure linearly inside the cuff, at the end of the BP measurement, the cuff pressure is quickly released using the deflation release valve. The device includes:
- A rigid upper-arm cuff passed to the subject’s left arm and secured with velcro. The interior of the armband is made of an inflatable bladder; it can be used in subjects with arm circumference 22–42 cm.
- A stainless steel and plastic tube mounted on the outer part of the cuff, containing mechanical parts for the BP measurement (pump, valves, tubing, pressure sensor), a battery, a LED screen, and the electronic cards which host the conditioning channels of the analog signals, a microcontroller equipped with an analog/digital converter, a memory (1MB Flash, 128kB RAM), and a Wi-Fi and Bluetooth communication.
- An electronic stethoscope on the outside of the armband allows the recording of a phonocardiogram (PCG). This function of the device was not assessed in the present study.
- Stainless steel electrodes allowing the measurement of one lead ECG. This function of the device will not be assessed in the present study.
 |
Figure 1 The Withings BPM core device. |
For this study, three Withings BPM Core devices (hardware version 5c and firmware version FW 751) were provided by WITHINGS SA, one of which was randomly selected to conduct this study and used according to the manufacturer’s recommendations.
Blood Pressure Measurements
The study was conducted by an experienced supervisor and 2 observers who were trained in accurate BP measurements. The participants’ arms were measured at mid-arm to ensure that the cuff-size being used with the reference (mercury) method was adequate for the subject. In this regard, three cuffs with inflatable bladder dimensions 9 × 18 cm, 12 × 24 cm and 15 × 32 cm were available to ensure that the cuff length reached 75–100% and its width 37–50% of the participant’s arm circumference. BP readings were obtained by the two observers blinded to each other’s readings using 2 parallel connected mercury sphygmomanometers (KDM® Germany), calibrated before the study, and a dual-head teaching stethoscope (3MTM Littmann®, United States). After the observers’ BP readings, BP was measured by the supervisor using the tested device. Agreement between the 2 observers was checked by the supervisor to ensure that their BP measurements were within ±4 mmHg for SBP and DBP. In case of disagreement between the 2 observers, additional pairs of measurements were performed with a maximum of 8 pairs of BP determinations after which the subject was excluded. Korotkoff sound (K5) was used for reference diastolic BP.
The validation procedure started after at least 5 minutes rest. BP measurements were performed according to the “same arm, sequential measurements” method on the left arm supported at heart level as described in the (ISO 81060-2:2018/AMD 1:2020)10,12 and recommended by the manufacturer. As required, nine consecutive BP measurements were performed in each subject using the mercury sphygmomanometers (5 times: R0, R1, R2, R3, R4,) and the tested devices (4 times: T0, T1, T2, T3). All nine-sequential same-arm measurements were recorded at 1-minute intervals starting with the mercury sphygmomanometer. The first auscultatory and first device measurement (R0 and T0) were not considered in the accuracy analysis.
Statistical Analysis
Statistical analysis was performed using specific analysis software established by the International Society of Vascular Health (ISVH). Each reference BP measurements (R1, R2, R3, R4) represented the mean of the simultaneous readings of the two observers. Each of the test device measurements was compared against the mean of the previous and next reference BP readings (eg, T1 versus the mean of R1-R2). Differences were calculated by subtracting the reference BP measurements from the test device measurements.
The means and standard deviations of the absolute values of the differences between the BP measurements of the devices under test and the reference standard were calculated and compared to Criterion 1 of the ISO 81060-2:2018/AMD 1:2020 standard, namely whether the means were ≤5.0 mm Hg and the standard deviation was ≤8.0 mm Hg. The standard deviations of the differences of the averaged paired determinations of the device under test and the reference measurement for each subject were calculated and compared to Criterion 2 of the ISO 81060-2:2018/AMD 1:2020 standard. Standardized Bland-Altman scatter plots were used to illustrate device – observer differences versus mean device and observer BP values for all pairs of comparisons. Bland-Altman plots of the differences in SBP and DBP determinations by arm circumference values were also performed. The distributions of the population according to gender, BP values and arm circumference were calculated to check if they are in accordance with the protocol requirements.10,12
Results
Study Population
Eighty-six subjects from the Preventive Cardiology Department of the Institute of Cardiology were selected, 85 of whom were recruited and analyzed; 1 subject was excluded due to a device failure. The clinical characteristics of the participants are summarized in Table 1. Results showed that their characteristics are in accordance with the requirements of the validation protocol in terms of age and gender distribution.
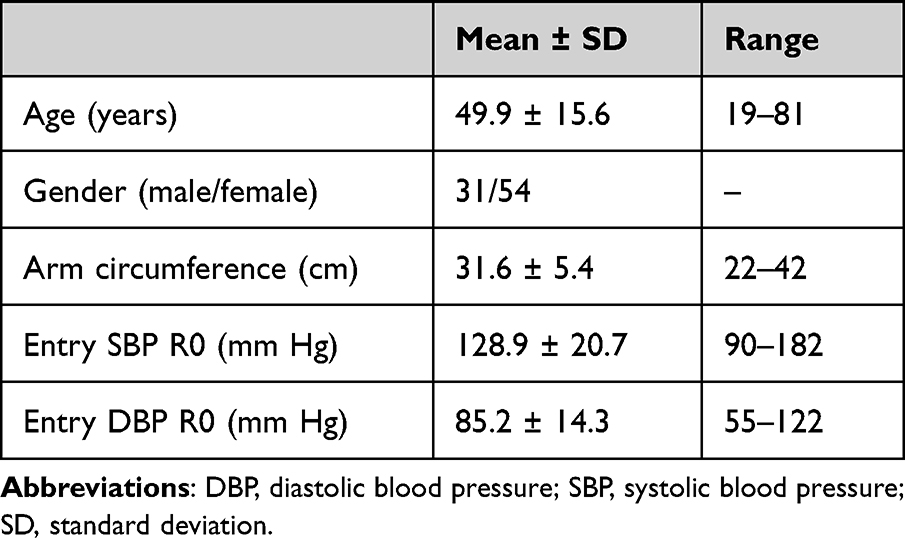 |
Table 1 Characteristics of Study Participants (n = 85) |
BP Measurements
Table 2 shows the distribution of BP levels measured using the reference method which are in accordance with the protocol requirements, namely:
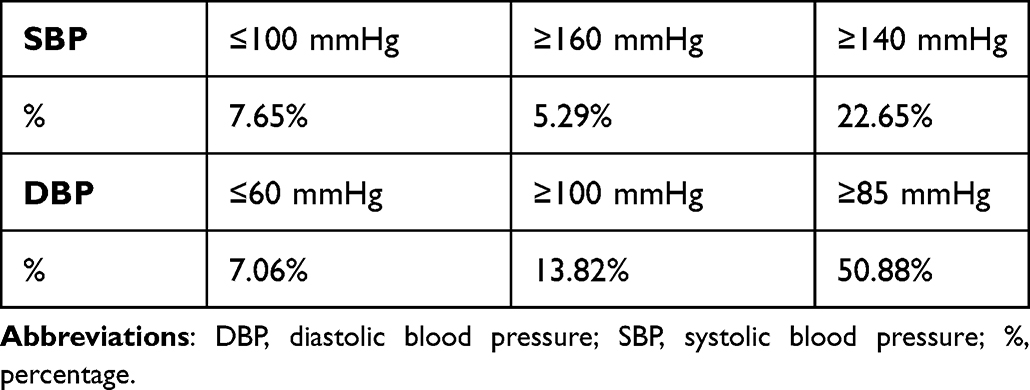 |
Table 2 Distribution in Percentages of Reference Blood Pressure Measurements |
For SBP readings: ≥5% readings must be ≤100 mmHg, ≥5% readings must be ≥160 mmHg and ≥20% readings ≥140 mmHg.
For DBP readings: ≥5% readings must be ≤60 mmHg, ≥5% readings must be ≥100 mmHg and ≥20% readings ≥85 mmHg.
The mean BP differences between the simultaneous observers’ measurements were −0.2 ± 2.1/0.3 ± 2.1 mmHg (systolic/diastolic, range −4 to 4 mmHg).
The accuracy analysis is shown in Table 3. For criterion 1, the mean differences between the tested device and reference BP values (test device minus reference BP values) were −0.6 ± 4.8 mmHg for SBP and 0.1 ± 3.7 mmHg for DBP. For criterion 2 (for individual subjects): the SD of 85 mean BP differences was 3.2 mmHg for SBP and 2.6 mmHg for DBP, calculated to be ≤6.91/6.95 for SBP/DBP (Table 4). These results show that the tested device fulfills the requirements (criteria 1 and 2) of the ISO 81060-2:2018/AMD 1:2020 Universal protocol10,12 and is qualified as having successfully “PASSED” the validation.
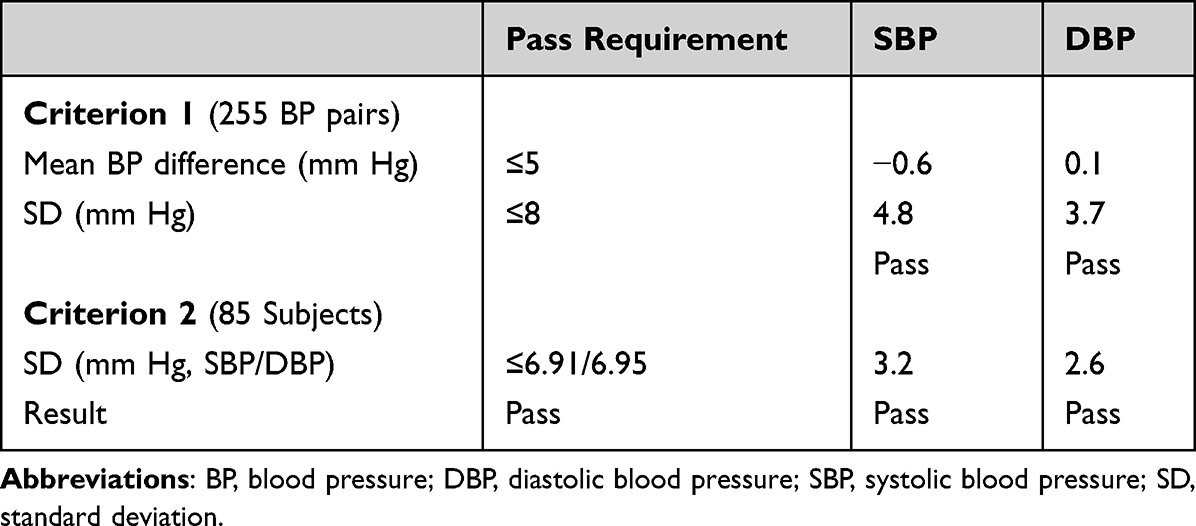 |
Table 3 Validation Results – Comparison Between the Reference and the Test Device Blood Pressure Measurements |
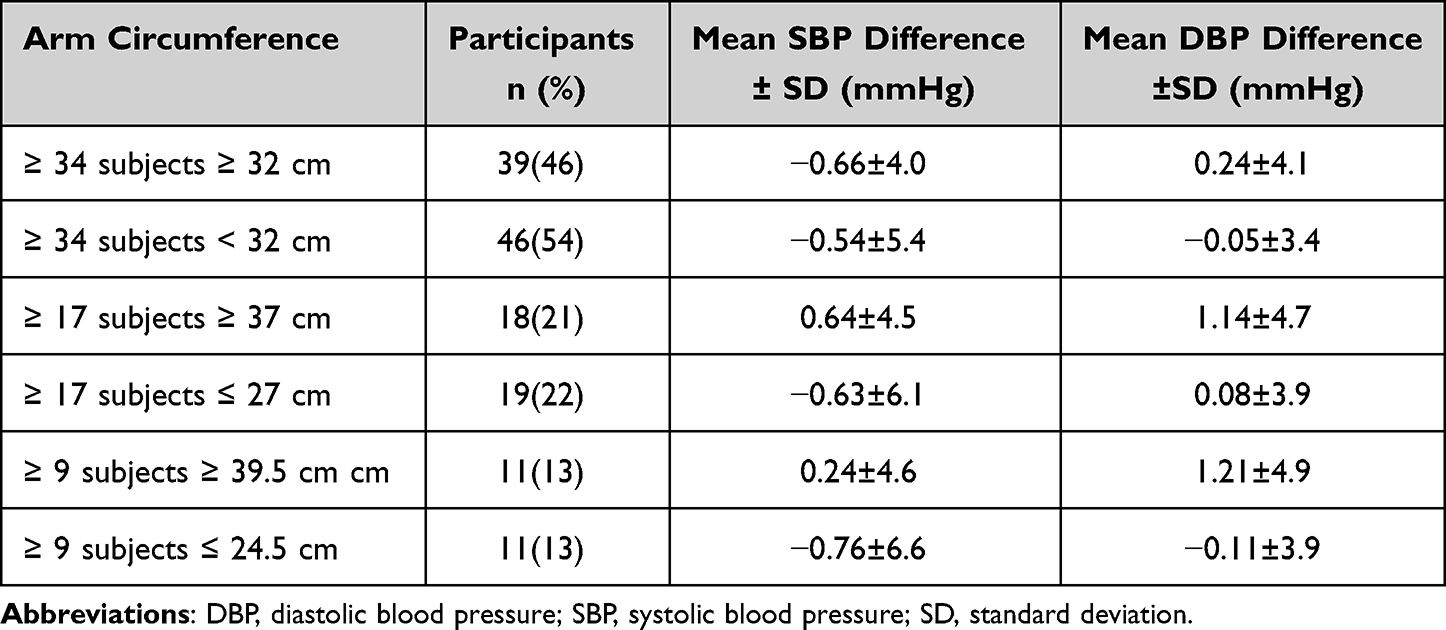 |
Table 4 Blood Pressure Differences According to the Arm Circumference |
Assessment of the accuracy of the tested device according to the arm circumference is shown in Table 4. Arm circumference distribution was in accordance with the requirements of the Universal protocol, namely: ≥40% of the subjects with arm circumference within the upper half of the specified range of use of the cuff, ≥40% within the lower half, ≥20% within the higher quarter, ≥20% within the lower quarter, ≥10% within the higher octal, and ≥10% within the lower octal of the specified range of use of the cuff (22–42 cm). The differences between BP values (test device minus reference) according to arm circumference are shown in Table 4 for both SBP and DBP.
Standardized Bland-Altman scatter plots of the test-reference BP differences against their mean are shown in Figure 2 for SBP and DBP. The Bland-Altman scatter plots showing the relationships between test-reference BP differences according to arm circumference are illustrated in Figure 3 for SBP and DBP.
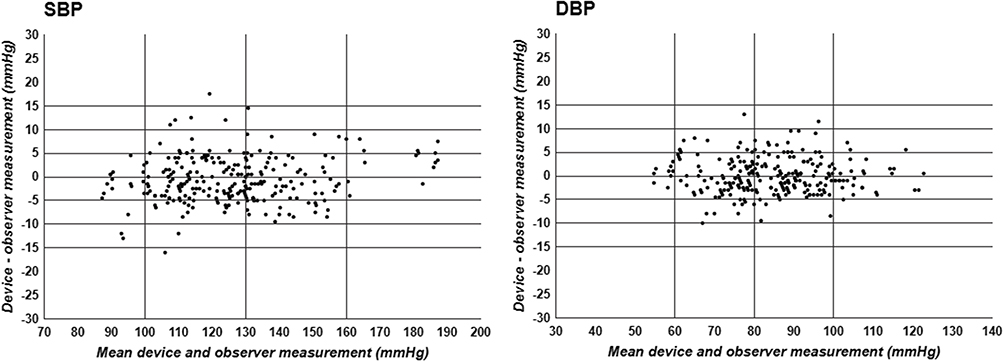 |
Figure 2 Standardized Bland-Altman scatter plots of test-reference BP differences against their mean values. Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure. |
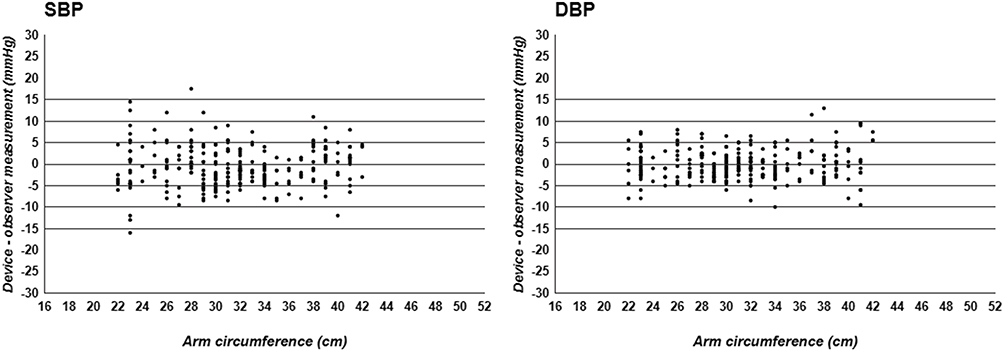 |
Figure 3 Scatter plots showing the differences between test-reference BP values according to the arm circumferences. Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure. |
Discussion
Previously, we published in this journal the validation results of the WITHINGS BPM CONNECT device in the general population and in pregnant women.14,15 This is the first study assessing the accuracy of the newly developed WITHINGS BPM CORE device from WITHINGS SA for BP measurement at the arm (brachial) level in patients with an arm circumference 22–42 cm in the general population. The results of the study show that the WITHINGS BPM CORE device successfully fulfilled both criteria 1 and 2 required by the (ISO 81060-2:2018/AMD 1:2020) Universal protocol. This is important to ensure the accuracy of the BP measurements before using such a device or prescribing it for home self-BP measurement. In fact, only monitors that have been validated for accuracy are recommended for BP measurement; consumers are advised to check such accuracy validation before purchasing or using any BP measurement device on the available websites.13
Other points related to the tested device, or to the validation protocol warrant further consideration:
Oscillometric devices overcome many biases related to the auscultatory method. Despite these advantages, there are some persistent concerns with these devices including the inter-individual variability of oscillometric BP measurements: in some patients, the oscillometric methods may show high variability among the repeated measurements in comparison to the auscultatory method. Reasons for such discrepancy and variability remain unclear. Therefore, it is recommended to check the accuracy of the oscillometric BP readings at the individual level.4
Special Populations
The ISO 81060-2:2018/AMD 1:202010,12 protocol recommends clinical validation of automatic devices for BP measurements in the general population but also in other special populations. In the present study, the WITHINGS BPM CORE was exclusively validated in the general population; the generalizability of these findings to other populations (pregnant women, children, arrhythmia) is unknown and would be incorrect and arbitrary.
Number of Studies
This study is the only one assessing the accuracy of the Withings BPM Core device. The ISO 81060-2:2018/AMD 1:202010,12 validation protocol does not specify the reproducibility of such studies neither the number of validation studies needed to approve a device’s accuracy. For instance, one clinical validation, if successful would seemingly be sufficient to consider the BP device as validated or approved.
Conclusion
The Withings BPM Core, an automatic oscillometric upper-arm BP monitor for home BP measurement, fulfils the accuracy validation requirements of the ISO 81060-2:2018/AMD 1:2020 for both SBP and DBP measurements in the general population with 22–42 cm arm circumference. Consequently, this device can be recommended for home BP measurements in the general population.
Acknowledgments
Our heartfelt thanks to all of the patients who took part in the study. Our grateful thanks to the Foundation-Medical Research Institutes® (F-MRI) and the International Society of Vascular Health for their support.
Funding
The study was supported by Withings® SA France, the International Society of Vascular Health (ISVH®) France and the Foundation-Medical Research Institutes (F-MRI) ® Switzerland. The study, including its design, conduct, analysis, and reporting, was performed completely independently from the manufacturer Withings SA.
Disclosure
All authors conducted validation studies for various manufacturers; they received honorarium for this validation study from The Foundation-Medical Research Institutes (F-MRI) ® Switzerland. The authors report no other conflicts of interest in this work.
References
1. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European society of cardiology and the European society of hypertension: the task force for the management of arterial hypertension of the European society of cardiology and the European society of hypertension. J Hypertens. 2018;36(10):1953–2041. doi:10.1097/HJH.0000000000001940
2. Unger T, Borghi C, Charchar F, et al. 2020 international society of hypertension global hypertension practice guidelines. Hypertension. 2020;75(6):1334–1357. doi:10.1161/HYPERTENSIONAHA.120.15026
3. Parati G, Stergiou G, Bilo G, et al. Home blood pressure monitoring methodology, clinical relevance and practical application: a 2021 position paper by the working group on blood pressure monitoring and cardiovascular variability of the European society of hypertension. J Hypertens. 2021;39(9):1742–1767. doi:10.1097/HJH.0000000000002922
4. Stergiou GS, Palatini P, Parati G, et al. 2021 European society of hypertension practice guidelines for office and out-of-office blood pressure measurement. J Hypertens. 2021;39(7):1293–1302. doi:10.1097/HJH.0000000000002843
5. Sharman J, O’Brien E, Alpert B, et al. Lancet commission on hypertension group position statement on the global improvement of accuracy standards for devices that measure blood pressure. J Hypertens. 2020;38(1):21–29. doi:10.1097/HJH.0000000000002246
6. O’Brien E, Atkins N, Stergiou G, et al. European society of hypertension international protocol revision 2010 for the validation of blood pressure measuring devices in adults. Blood Press Monit. 2010;15(1):23–38. doi:10.1097/MBP.0b013e3283360e98
7. O’Brien E, Petrie J, Littler W, et al. An outline of the revised British hypertension society protocol for the evaluation of blood pressure measuring devices. J Hypertens. 1993;11(6):677–679. doi:10.1097/00004872-199306000-00013
8. Association for the Advancement of Medical Instrumentation. ANSI/AAMI/ISO 11137-2; 2013.
9. Stergiou GS, Alpert B, Mieke S, et al. A universal standard for the validation of blood pressure measuring devices: association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO) collaboration statement. J Hypertens. 2018;36(3):472–478. doi:10.1097/HJH.0000000000001634
10. Stergiou G, Palatini P, Asmar R, et al. Recommendations and practical guidance for performing and reporting validation studies according to the universal standard for the validation of blood pressure measuring devices by the association for the advancement of medical instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO). J Hypertens. 2019;37(3):459–466. doi:10.1097/HJH.0000000000002039
11. Stergiou GS, Alpert B, Mieke S, et al. A universal standard for the validation of blood pressure measuring devices: association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO) collaboration statement. Hypertension. 2018;71(3):368–374. doi:10.1161/HYPERTENSIONAHA.117.10237
12. International Organization for Standardization. ISO 81060-2:2018/AMD 1:2020 non-invasive sphygmomanometers – part 2: clinical investigation of intermittent automated measurement type – amendment 1; 2020. Available from: https://www.iso.org/standard/75432.html.
13. Stergiou G, O’Brien E, Myers M, et al. Stride BP: an international initiative for accurate blood pressure measurement. J Hypertens. 2020;38(3):395. doi:10.1097/HJH.0000000000002289
14. Topouchian J, Zelveian P, Hakobyan Z. Clinical accuracy of the Withings BPM connect for self-blood pressure measurements in the general population: validation according to the association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization Universal Standard. Vasc Health Risk Manag. 2022;18:191–200. doi:10.2147/VHRM.S350006
15. Zelveian P, Topouchian J, Hakobyan Z, Asmar J, Gharibyan H, Asmar R. Clinical accuracy of the Withings BPM connect for self-blood pressure measurements in pregnancy and pre-eclampsia: validation according to the association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization Universal Standard. Vasc Health Risk Manag. 2022;18:181–189. doi:10.2147/VHRM.S351313
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Accuracy of the Combei BP880W Wrist Device for Self-Blood Pressure Measurements in General Population According to the International Organization for Standardization Universal Standard (ISO 81060-2:2018/AMD 1:2020) Protocol
Hakobyan Z, Zelveian P, Gharibyan H, Topouchian J, Asmar R
Vascular Health and Risk Management 2025, 21:75-84
Published Date: 18 February 2025