Back to Journals » Nature and Science of Sleep » Volume 18

Validation of the Richards–Campbell Sleep Questionnaire Against Actigraphy in Hospitalized Patients and Its Association with Delirium Risk
Authors Milata M ![]() , Locihová H, Sonka K, Susta M
, Locihová H, Sonka K, Susta M
Received 8 March 2026
Accepted for publication 14 May 2026
Published 25 June 2026 Volume 2026:18 607779
DOI https://doi.org/10.2147/NSS.S607779
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Martin Milata,1 Hana Locihová,2,3 Karel Sonka,1 Marek Susta4
1Department of Neurology and Center of Clinical Neurosciences, First Faculty of Medicine, Charles University and General University Hospital, Prague, Czech Republic; 2Department of Anesthesiology, Resuscitation and Intensive Care Medicine, Faculty of Medicine and University of Ostrava, Ostrava, Czech Republic; 3Department of Nursing and Midwifery, Faculty of Medicine, University of Ostrava, Ostrava, Czech Republic; 4Proverbs a.s., Prague, Czech Republic
Correspondence: Martin Milata, Department of Neurology and Center of Clinical Neurosciences, First Faculty of Medicine, Charles University and General University Hospital, Kateřinská 30, Praha, 2, 12821, Prague, Czech Republic, Tel +420725054052, Email [email protected]
Purpose: To validate the Richards–Campbell Sleep Questionnaire (RCSQ) relative to actigraphy on general hospital wards and to examine the predictive value of sleep parameters for delirium.
Patients and Methods: This multicenter, prospective observational study was conducted on internal medicine, surgical, and neurology wards across seven healthcare institutions in the Czech Republic. The analysis included 133 patients (424 nights). Individual RCSQ items and corresponding nocturnal actigraphic sleep parameters (MotionWatch 8) were compared using linear mixed-effects models (LMM). Associations with delirium occurrence were evaluated using binary logistic regression.
Results: Patients rated their sleep as moderately good on the RCSQ despite objectively impaired sleep on actigraphy. Only the sleep-depth item showed significant associations, with higher scores linked to higher immobile time and lower fragmentation. No significant associations were found for remaining parameters. The RCSQ total score showed only weak associations with sleep efficiency and percent sleep. Subjective sleep ratings did not predict delirium, whereas higher actigraphic sleep efficiency was associated with lower delirium risk.
Conclusion: In hospitalized patients, only the RCSQ item assessing sleep depth showed meaningful correspondence with actigraphic measures. The RCSQ total score showed limited concurrent validity against actigraphy and was not useful for predicting delirium, whereas low actigraphy-measured sleep efficiency appeared to be a clinically relevant marker of delirium risk.
Keywords: actigraphy, RCSQ, sleep quality, general wards, sleep monitoring
Introduction
Adequate duration and quality of sleep represent a fundamental physiological need. The importance of sleep and the consequences of its impairment extend across the entire field of medicine, and insufficient or poor-quality sleep is among the risk factors for delirium.1 Monitoring sleep quantity and quality during illness is therefore clinically relevant. This can be achieved using objective methods, such as polysomnography (PSG) or actigraphy (ACT), which are generally more precise but resource-intensive, or by means of questionnaires, which are quick to administer but have more limited validity.2
Delirium is an acute disturbance of attention, orientation, and awareness, that represents a change from baseline, with a transient and often fluctuating course, and is not better explained by another medical or psychiatric condition or by medication. Delirium typically develops in the context of hospitalization, while its presence is subsequently associated with increased morbidity and mortality.3 Insufficient or poor-quality sleep increases the likelihood of delirium, and delirium, in turn disrupts sleep architecture; however, the causal relationship between sleep disturbances and delirium has not yet been fully clarified.4
The Richards–Campbell Sleep Questionnaire (RCSQ) was developed in 2000 by Kathryn C. Richards for the subjective assessment of sleep quality in intensive care units (ICUs).5 The questionnaire was developed and tested against concurrent polysomnography, demonstrating good internal consistency, and its total score was significantly associated with one of the simplest polysomnographic indicators of sleep quality—sleep efficiency.6 Despite its widespread use, the validity of the RCSQ outside intensive care settings remains insufficiently established. Most validation studies have been conducted in ICU populations, where environmental conditions, patient characteristics, and sleep architecture differ substantially from those in general inpatient wards. In routine ward settings, patients are typically less critically ill but are exposed to different patterns of sleep disruption, including environmental noise, clinical interventions, and variable daily routines.7 Importantly, no prior study has performed a detailed item-level comparison between individual RCSQ domains and corresponding actigraphic sleep parameters in general ward populations. Furthermore, the relationship between subjective sleep assessment using the RCSQ and clinically relevant outcomes, such as delirium, has not been adequately explored in this setting.
The primary aim of this study was to evaluate the concurrent criterion-related validity and convergent correspondence of individual RCSQ items and the total RCSQ score against conceptually corresponding actigraphic sleep parameters in general inpatient ward settings. Because the RCSQ represents a subjective patient-reported assessment and actigraphy provides an objective estimate of sleep–wake patterns rather than a direct gold-standard measure of subjective sleep quality, the analyses were interpreted as evidence of correspondence or association rather than strict measurement agreement. Secondary aims were to assess whether the RCSQ can predict delirium risk under standard ward conditions and to identify actigraphy-derived sleep parameters associated with delirium occurrence in the same patient population.
Methods
The study was conducted as a multicentre prospective observational study on general inpatient wards (internal medicine, surgery, and neurological) in seven hospitals in the Czech Republic under standard hospitalization conditions. Actigraphic monitoring and questionnaire assessments were performed at the beginning of hospitalization for a minimum of three consecutive days.
A total of 152 patients were initially enrolled. Inclusion criteria were age ≥18 years, planned hospitalization of at least 72 hours, provision of informed consent for participation in the study, and the ability to complete the RCSQ independently. Exclusion criteria were quantitative impairment of consciousness (Glasgow Coma Scale score <12) or qualitative disturbance of consciousness at admission, terminal stage of illness, previously diagnosed or known sleep disorder, communication impairment, dementia, inability to understand study instructions, and continuous sedation during hospitalization. All evaluated episodes of delirium therefore developed during the course of hospitalization.
Nineteen patients were excluded from the analysis due to technically inadequate actigraphic recordings, improperly completed sleep diaries, or incomplete accompanying activity logs.
The Richards–Campbell Sleep Questionnaire (RCSQ) is a brief patient-reported self-assessment instrument. It consists of five items assessing sleep depth, sleep latency, number of awakenings, ability to return to sleep, and overall sleep quality, each rated on a 100-mm visual analogue scale, with higher scores indicating better perceived sleep quality. The total RCSQ score is calculated as the mean of the five items. The questionnaire is typically completed by patients in the morning following the assessed night and requires only a few minutes to administer.6 In the original validation study, the RCSQ demonstrated high internal consistency (Cronbach’s α = 0.90) and a unidimensional factor structure explaining approximately 70% of the variance, with its total score significantly correlating with polysomnography-derived sleep efficiency.6 Subsequent studies have confirmed good psychometric properties of the instrument, including high interrater reliability between patients and nurses.5 More recent diagnostic accuracy analyses suggest that a global RCSQ score of approximately 63–65 mm can be used to distinguish good from poor sleep quality in intensive care settings, with reported sensitivity of 87%, specificity of 81%, and an area under the receiver operating characteristic curve of 0.896.8 Furthermore, validation studies in different populations have consistently demonstrated high internal consistency, with Cronbach’s α typically exceeding 0.90.9 The validated Czech version of the RCSQ was used.10 The questionnaire was completed independently by patients in the morning following the assessed night, between 7:00 and 9:00 a.m. In patients who developed delirium and were unable to reliably complete the questionnaire independently, the RCSQ was completed with assistance from the night-shift nurse. In such cases, the nurse supported the patient in understanding and completing the items based on the patient’s responses whenever possible, while also incorporating observational input when necessary.
The presence of delirium was monitored continuously as part of routine clinical care, and structured delirium assessment was performed once daily using the Confusion Assessment Method–Standard (CAM-Standard). CAM-Standard is a rapid algorithm-based screening tool for delirium, derived from the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders, assessing four core features of delirium: acute onset and fluctuating course, inattention, disorganized thinking, and altered level of consciousness. Delirium is considered present based on their predefined combined positivity.11,12
Actigraphy is a non-invasive accelerometer-based method providing continuous measurement of motor activity, from which sleep–wake states are indirectly inferred.13 Sleep actigraphic monitoring was performed using the MotionWatch 8 device (CamNtech, Cambridge, UK). The recording unit was worn on the wrist of the non-dominant upper limb. The device incorporates a built-in photodiode (light sensor) to quantify ambient light exposure, allowing objective identification of lights-off (bedtime preparation) and lights-on (end of the sleep period). Actigraphic data were processed using the proprietary MotionWare software (CamNtech), version 1.3.33.
Actigraphic monitoring was performed continuously for three to five consecutive days and nights. Motor activity was recorded in triaxial mode and summarized in 60-second intervals, with the threshold for categorizing an episode as resting set at ≤20 counts per minute (cpm), which corresponds to the validated cut-off used for the MotionWatch device.14
Throughout the entire period of actigraphic monitoring, an activity/sleep diary was maintained to support the interpretation of actigraphic data. The diary included information on key daily activities such as bedtime (lights-off), wake-up time, and periods when the actigraph device was not worn (eg, during hygiene procedures or medical examinations) In cooperative patients, the diary was completed by the patients themselves, whereas in patients with delirium, the diary was completed by the attending nursing staff. These diary records were primarily used to determine and verify lights-off and getting-up times, which were subsequently cross-checked against actigraphy-derived light sensor (luxometry) data.
Lights-off (MotionWare “Lights Out”) and getting-up times were entered manually based on data from a sleep diary filled in by the patient independently or with assistance from nursing staff. The entered times were subsequently verified using the light sensor (luxmetry) data. If the reported lights-off time repeatedly (more than once) differed by more than 10 minutes from the objectively recorded decrease in ambient light, the diary entry was considered unreliable, and lights-off and getting-up times were determined exclusively based on luxometric data.
Sleep onset time was determined manually from the actigraphic graphical output as the point at which motor activity decreased to an individual resting level. This resting level was defined based on the average activity during a reliably identified uninterrupted sleep segment (confirmed both anamnestic and parameter-based) lasting at least 10 minutes.
Morning awakening time was defined as the moment of a sustained increase in motor activity to a level corresponding to wakefulness (confirmed both anamnestic and parameter-based), persisting for at least 10 minutes, followed by getting out of bed within 60 minutes without an intervening sleep episode.
This study used the following actigraphic parameters:
- Time in bed (min) – the total duration between “lights off” and “getting out of bed”.
- Actual sleep time (min) – the total time spent asleep in bed (the sum of epochs that were categorized as immobile within the time interval after sleep onset and before morning awakening).
- Sleep latency (min) – the time between lights off/going to bed and falling asleep, which within this interval was defined as the first time point marking the beginning of a continuous ≥10min segment of epochs scored as sleep, with a tolerance of at most 1 epoch scored as wake.
- Sleep efficiency (%) – the proportion of actual sleep time relative to time spent in bed.
- Fragmentation index (dimensionless) – the sum of Mobile time (%) and immobile bouts ≤1 min (%).
- Immobile bouts ≤1 min – the number of ≤1-min episodes rated as “immobile” out of the total number of all immobile episodes of all durations.
- Mean sleep bout (min) – the mean duration of individual sleep episodes.
- Sleep bout – a continuous sequence of consecutive epochs classified by the algorithm as sleep, bounded by a transition from wakefulness to sleep and a subsequent transition from sleep to wakefulness.
- Wake bouts – the number of continuous segments classified as wakefulness based on individual epochs.
- Mean wake bout (min) is the mean duration of wakefulness episodes according to the above definition.
- Assumed sleep time (min) is the total time elapsed between sleep onset and final awakening.
- Immobile time (%) is defined as time without movement expressed as a percentage of the assumed sleep time; it serves as a motor marker of sleep and is primarily used in fragmentation indicators. With increasing sleep fragmentation, the discrepancy between immobile time and actual sleep increases, as not every period of immobility represents sleep and not every movement represents wakefulness.
- Mean activity/epoch is the total activity score divided by the number of epochs within the assumed sleep period. This value is strongly dependent on the length of the epoch.15
The assignment of RCSQ items to actigraphic parameters was based on their conceptual correspondence (Table 1).
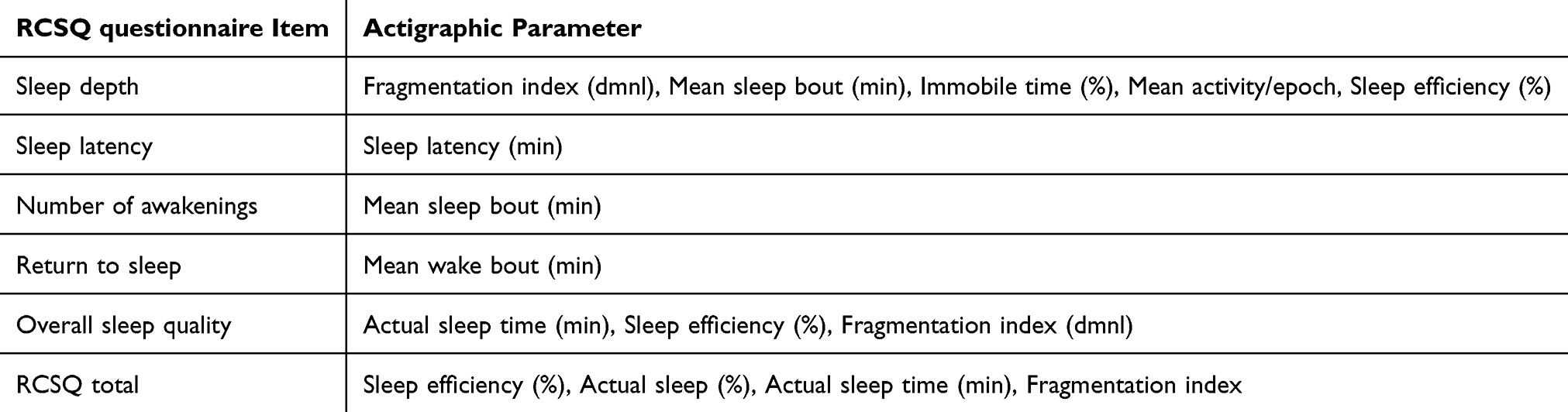 |
Table 1 Conceptual Assignment of RCSQ Items to Actigraphic Parameters |
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics software (version 27). Basic demographic and clinical characteristics of the study sample (eg., age, sex, type of ward) were evaluated using descriptive statistics. Continuous variables are presented as mean ± standard deviation (SD), and categorical variables as absolute and relative frequencies (%).
For the validation analyses, actigraphic sleep parameters were treated as concurrent external criteria because they were recorded during the same nights as the corresponding morning RCSQ assessments. Associations between conceptually matched RCSQ items and actigraphic metrics were therefore interpreted as evidence of concurrent criterion-related validity and, more broadly, convergent correspondence between subjective and objective sleep measures. Given that RCSQ and actigraphy assess related but non-identical aspects of sleep, the term “agreement” was used only in a conceptual sense, while the statistical results are reported as associations based on standardized fixed-effect estimates from the mixed models.
To assess the relationship between subjective sleep evaluation (individual RCSQ items and the RCSQ total score) and objective actigraphic parameters, linear mixed models (LMMs) were applied. This approach was chosen due to the hierarchical structure of the data with repeated measurements (nights) nested within individual patients (a total of 424 nights in 133 patients). The models included a random intercept for patient identity to account for inter-individual variability. Within-patient correlation across consecutive nights was modeled using a first-order autoregressive covariance structure AR(1), specified for the repeated residuals across ordered nights. To allow comparison of association strength across different metrics, all continuous variables entered into the LMMs were transformed into z-scores (standardized to a mean of 0 and an SD of 1). The fixed-effect regression coefficient (β) therefore represents the expected change in the dependent variable (in SD units) associated with a 1 SD change in the predictor (ie., a standardized effect size) facilitating comparison across models. For each fixed effect, Type III F-tests with corresponding degrees of freedom and p-values were reported. Models were fitted using all available cases for each variable pair, without imputation. All tests were two-sided with a significance level of α = 0.05.
General form of the linear mixed model with a random intercept:

 – dependent variable expressed as the z-score of the actigraphic metric for patient i on night j
– dependent variable expressed as the z-score of the actigraphic metric for patient i on night j – predictor expressed as the z-score of the corresponding RCSQ item for patient i on night j
– predictor expressed as the z-score of the corresponding RCSQ item for patient i on night j – fixed intercept, representing the mean value of the dependent variable at the mean value of the predictor (ie., when z(x) = 0)
– fixed intercept, representing the mean value of the dependent variable at the mean value of the predictor (ie., when z(x) = 0) – fixed effect (slope), expressing the change in the dependent variable associated with a one–standard deviation change in the predictor
– fixed effect (slope), expressing the change in the dependent variable associated with a one–standard deviation change in the predictor – random intercept for patient i, capturing the individual deviation from the population mean; assumed to be normally distributed;
– random intercept for patient i, capturing the individual deviation from the population mean; assumed to be normally distributed; 
 – residual error for patient i on night j, assumed to be independent and normally distributed;
– residual error for patient i on night j, assumed to be independent and normally distributed; 
The relationship between sleep quality and delirium occurrence was analysed using binary logistic regression. Delirium was defined as a combined outcome: the presence of at least one positive Confusion Assessment Method–Standard (CAM-Standard) assessment and/or administration of antidelirium medication during the study period. Predictors were patient-level mean values of sleep parameters across the monitoring period. Results are presented as odds ratios (ORs) with 95% confidence intervals (95% CI). Due to multicollinearity among individual RCSQ items, models using questionnaire data were limited to the patient-level RCSQ total score. Given the exploratory nature of these analyses, no adjustment for multiple comparisons was applied.
Results
A total of 133 patients (424 nights in total) were included in the analysis. The mean age of the patients was 71.2 ± 13.5 years, with a balanced sex distribution (48.9% men, 51.1% women). Most patients were hospitalised in internal medicine wards (43.6%), followed by surgical wards (29.3%) and neurology wards (27.1%). The mean number of monitored nights was 3.2 ± 1.1 (range 3–5 nights). The incidence of delirium in this cohort was substantial: 27.8% of patients (n = 37) had at least one positive CAM screening result, and in 15.8% (n = 21) the clinical condition - specifically delirium - required pharmacological treatment for the management of delirious symptoms (see Table 2).
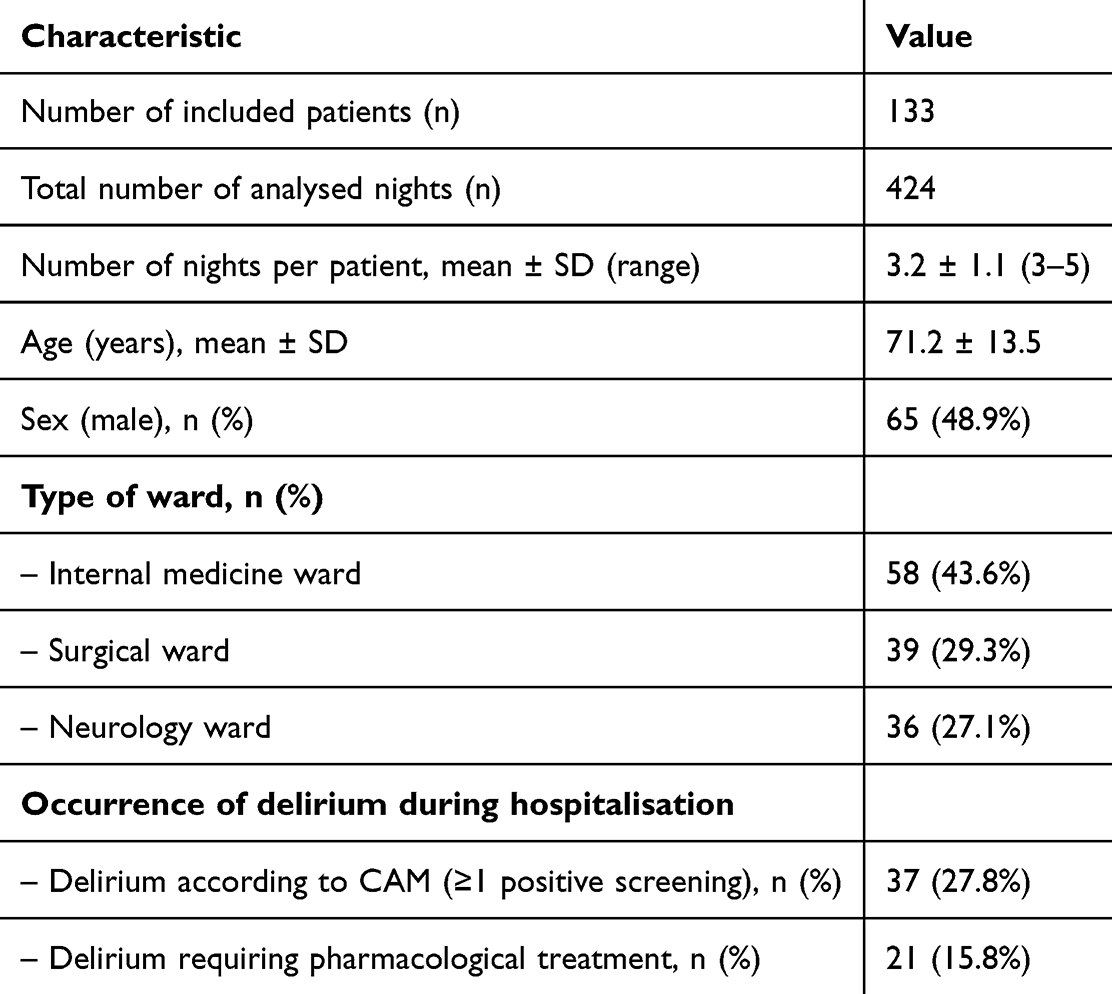 |
Table 2 Basic Demographic and Clinical Characteristics of the Study Sample |
Descriptive characteristics of subjective sleep assessment using the RCSQ questionnaire are presented in Table 3. Both the total RCSQ score and individual items showed a comparable range of variability across the study sample, with no single item exhibiting a markedly wider distribution of values than the others.
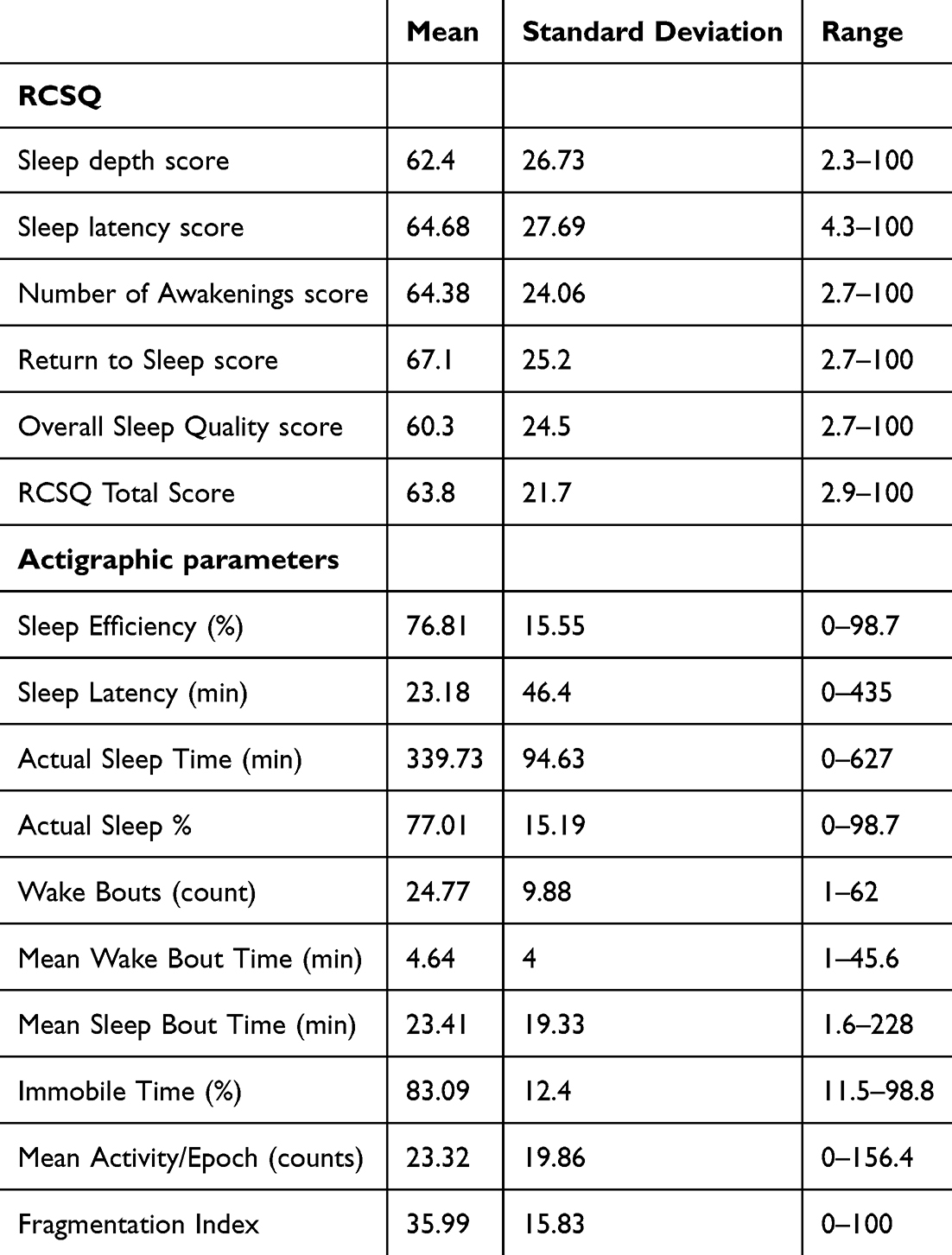 |
Table 3 Descriptive Statistics of the RCSQ Questionnaire and Actigraphic Parameters |
Summary descriptive statistics of the actigraphic parameters are also presented in Table 3. The data demonstrate substantial interindividual variability in the main sleep indicators (actual sleep time, sleep efficiency, sleep fragmentation index and wake bouts), with a wide dispersion of values for sleep latency and wake bouts across patients and nights.
Analysis of the agreement between individual RCSQ items and actigraphy using linear mixed models revealed substantial differences in the accuracy of subjective estimation of various aspects of sleep (Table 4).
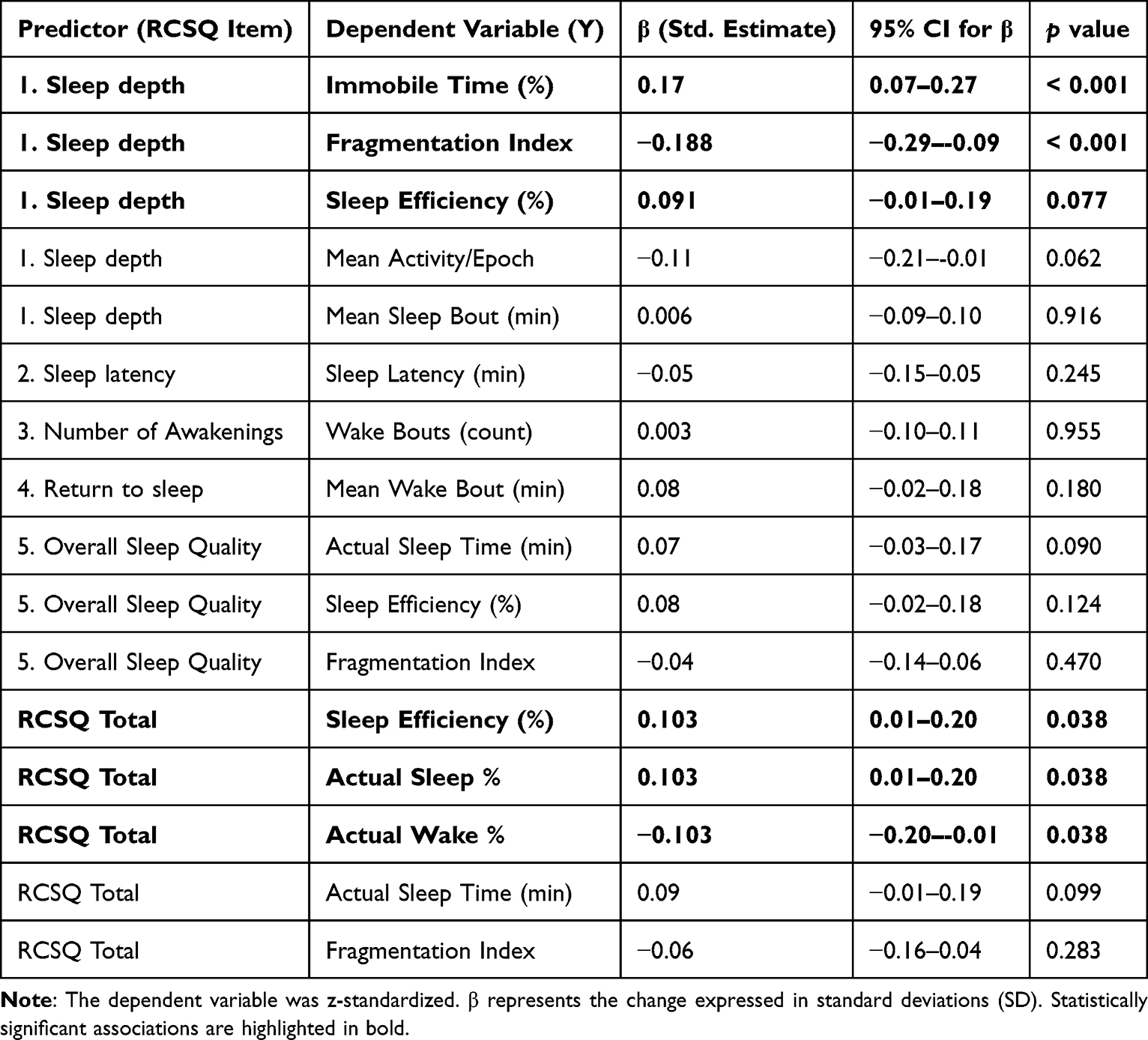 |
Table 4 Item-Level Analysis of the RCSQ Questionnaire in Relation to Actigraphic Sleep Parameters (Linear Mixed Models) |
For the item sleep latency, no statistically significant association with actigraphically measured sleep latency was found. Similarly, sleep fragmentation as perceived by the RCSQ did not reflect the number of awakenings recorded by actigraphy. The RCSQ item assessing the ability to return to sleep after awakening showed only a non-significant trend toward an association with the mean duration of nocturnal awakenings measured by actigraphy. Subjective sleep quality assessed by the RCSQ did not correlate with any of the corresponding actigraphic metrics (total sleep time, sleep efficiency, or fragmentation index).
A statistically significant association was observed for the RCSQ sleep-depth item only in relation to selected actigraphic parameters. Specifically, sleep depth showed a positive association with immobile time and a negative association with the fragmentation index. No statistically significant associations were observed between sleep depth and other conceptually related actigraphic parameters, including sleep efficiency, mean activity per epoch, or mean sleep bout duration.
The total RCSQ score demonstrated a weak but statistically significant positive association with objective sleep efficiency and the corresponding percentage of sleep. In contrast, its relationship with total sleep time and with sleep fragmentation was not statistically significant (Table 4).
Analysis of the relationship between sleep quality and the risk of delirium showed that subjective sleep assessment using the RCSQ (including the RCSQ total score) was not a significant predictor of delirium, whereas actigraphic measures - particularly low sleep efficiency - were significantly associated with an increased risk of delirium (Table 5).
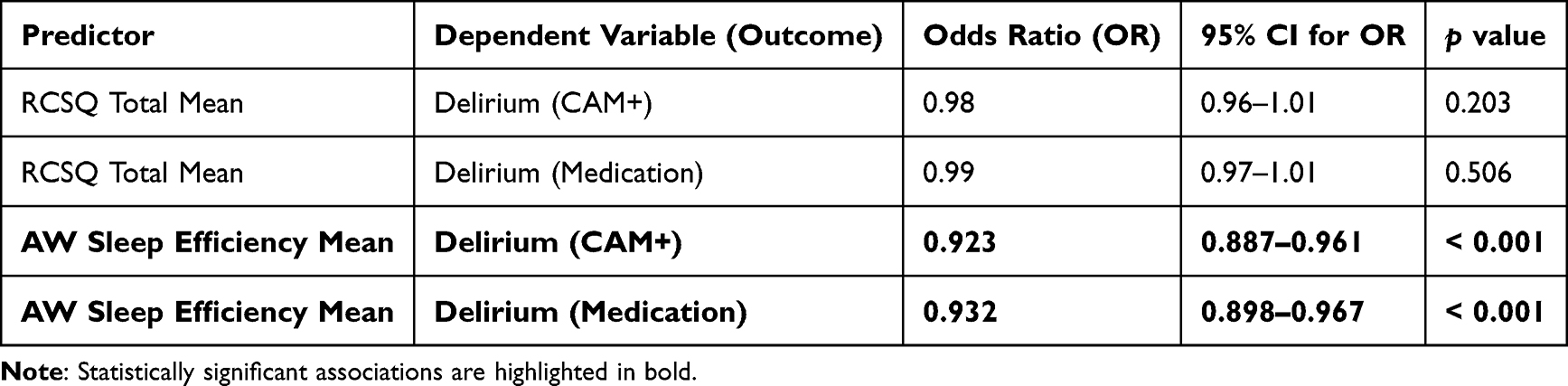 |
Table 5 Prediction of Delirium – Binary Logistic Regression |
Discussion
This is the first study to perform item-level validation of the RCSQ against actigraphy and the first to examine in general inpatient wards, the relevance of sleep assessment using the RCSQ and actigraphy in relation to the subsequent development of delirium. Overall, our findings indicate that most RCSQ items do not correspond well with actigraphy in general ward patients, while actigraphy-derived sleep efficiency shows clinical relevance for delirium risk.
Of all RCSQ items, only sleep depth showed a consistent association with its corresponding actigraphic parameter (immobile time and fragmentation index). The RCSQ total score demonstrated only a weak association with actigraphic sleep efficiency and actual sleep percentage. The remaining RCSQ items showed no meaningful correspondence with actigraphic measures. Furthermore, we found that the RCSQ had no predictive value for the development of delirium, in contrast to the actigraphic parameter sleep efficiency.
The absence of an association between sleep latency assessed by the RCSQ and actigraphic sleep latency is not surprising, as sleep latency is among the least reliable actigraphic parameters and at the same time, subjective estimation of sleep latency is inherently imprecise.16 Sleep latency exhibited substantial variability, reflecting differences in underlying medical conditions, varying ward environments across participating hospitals, and individual tolerance of the hospital setting.
A low number of awakenings reported by the RCSQ that does not correspond to the high number detected by actigraphy can likely be explained, at least in part, by sleep misperception in the disrupted hospital environment.17,18
The limited agreement between individual RCSQ items and actigraphic parameters may be attributed to three main factors: limitations of the RCSQ itself, limitations of actigraphy, and the well-established weak correlation between subjective and objective sleep assessment. The RCSQ relies on vaguely defined constructs that may be interpreted by respondents more as a global impression of sleep rather than as evaluations of specific sleep characteristics. In this respect, the item assessing overall sleep quality appears particularly problematic: although the RCSQ total score showed a weak correlation with actigraphic sleep efficiency, this specific item demonstrated no association with any objective parameter. The inclusion of an item assessing overall sleep quality within the total score is therefore conceptually questionable. In addition, the use of visual analogue scales in the RCSQ may contribute to inconsistent responding in the absence of clear reference anchors.19
Patients in our study rated the RCSQ items with substantial variability across the full range of the RCSQ scale (0–100 points). However, the presence of extreme values, including repeated minimum and maximum scores, may reflect difficulties in item interpretation or in the use of the visual analogue scale rather than true differences in sleep quality. This finding is consistent with the weak agreement between the RCSQ and objective actigraphic parameters and suggests limited reliability of extreme subjective ratings in this clinical context.
The weak and statistically non-significant relationship between overall sleep quality and actigraphy may reflect both the multidimensional nature of subjective sleep evaluation and methodological limitations of actigraphy, which may fail to capture brief quiescent awakenings, arousals, or prolonged wakefulness before sleep onset; moreover, measurement accuracy can be expected to be lower in bedridden patients than in fully active individuals.16
Subjective sleep assessment is typically only weakly to moderately correlated with objectively measured parameters such as actigraphy or polysomnography.20 Subjective evaluation of sleep is influenced by psychological and personality-related factors, including mood, expectations, attitudes, and the way questionnaire items are interpreted. Limited agreement between subjective and objective methods has been repeatedly reported across different populations and may lead to patient misclassification, as has also been demonstrated in the home environment.20–22
Multiple regression analysis using the total RCSQ score identified several clinical and demographic factors associated with subjective sleep quality, including ward type, administration of hypnotics or anxiolytics, age, and pain. However, these variables explained only approximately 18% of the variability in RCSQ scores,23 suggesting a substantial contribution of additional individual factors and, in the context of the present findings, a limited explanatory value of the RCSQ.
The mean total RCSQ score in our cohort was approximately 65/100. In the ICU literature, a value <50 is generally considered indicative of poor sleep, which was exceeded in our data, whereas values >75 are regarded as reflecting excellent sleep quality. At the same time, more recent ROC analyses have suggested a cut-off for good sleep around 63–65 mm, a range in which the mean value of our cohort lies exactly.8,10,24 This subjective classification of sleep as moderately good is in contrast with the actigraphic findings, which showed that patients slept for only approximately 340 minutes, with a sleep efficiency of approximately 77%, a mean number of wake bouts of about 25 (reference range 2–6), actual wake time of 23% (reference <15%), and actual sleep of approximately 77% (reference >85%).25
In the general adult population, large epidemiological and polysomnographic studies indicate that total sleep time (TST) typically ranges between approximately 7 and 8 hours per night, sleep efficiency usually exceeds 80%, and sleep onset latency most commonly remains within 20 minutes, although with substantial interindividual variability.26 Compared with these values, sleep in our hospitalized patients was worse across several parameters, including lower mean total sleep time and sleep efficiency, together with greater variability in sleep latency. Actigraphic data further demonstrated increased sleep fragmentation, characterized by a higher number of nocturnal wake episodes, although individual wake episodes were on average short. For parameters such as wake bouts or the fragmentation index, population-based actigraphic norms are currently not available. However, existing epidemiological data suggest that healthy adults in the home environment generally exhibit lower levels of sleep fragmentation than during hospitalization.27
The finding that the RCSQ failed to detect sleep changes predictive of delirium, whereas actigraphy did so, further underscores the limitations of self-monitoring compared with objective assessment methods. The role of cognitive status is debatable, as patients in the early stages of delirium may have impaired introspection, altered perception of time or reduced motivation to fully cooperate with questionnaire completion. In such cases, patients may not be able to reliably assess their own sleep. In clinical populations with fluctuating cognitive status, assisted administration of patient-reported measures is commonly used to facilitate data collection, although it may introduce additional variability in responses.28
The observed association between sleep efficiency and the risk of delirium, whereby a 1% increase in sleep efficiency corresponded to an approximately 7–8% reduction in delirium risk, suggests that sleep efficiency represents a clinically relevant indicator of sleep quality.
A similar comparison of the RCSQ with actigraphy was performed in a Czech study conducted in a multidisciplinary intensive care unit, where no statistically significant concordance between the RCSQ and actigraphic parameters was demonstrated.29 The authors attributed this finding to limitations of actigraphic measurement in that specific clinical setting. Comparable conclusions were reported in a recent study involving 228 ICU patients, which likewise failed to demonstrate good agreement between the RCSQ and actigraphy and highlighted the limited applicability of actigraphy in critically ill patients.9
Limitations of our study include the restricted availability of detailed clinical and nursing-related information, as well as limited data on patients’ pre-hospital sleep history. On the other hand, the study was conducted in a relatively large patient cohort, which partially compensates for the lack of detailed individual data. In patients who developed delirium and were unable to complete the RCSQ independently, the questionnaire was completed with nursing assistance, which may have introduced variability in the degree to which responses reflected subjective versus observational assessment.13 Actigraphic assessment is further limited by generally low levels of overall motor activity during hospitalization. Actigraphy has known limitations in distinguishing quiet wakefulness from sleep, which may have influenced the observed associations. Specific environmental and contextual sleep conditions for individual patients were not systematically recorded. Although the estimated β coefficients were within a realistic range and were associated with meaningful standard errors, 95% confidence intervals, and p-values, the chosen covariance structure (AR1) may not have been optimally estimated by the numerical algorithm in some of the models.
Conclusion
The individual RCSQ items showed a differential pattern of correspondence with actigraphy in hospitalized patients. The sleep-depth was the only item that demonstrated consistent associations with conceptually corresponding actigraphic measures, particularly fragmentation index and immobile time, whereas the remaining items showed weak or no evidence of correspondence with their matched objective parameters. The total RCSQ score showed only weak associations with actigraphic sleep efficiency and percentage of sleep and did not predict delirium occurrence. These findings suggest that in general inpatient ward settings the RCSQ may provide limited bedside information on perceived sleep depth, but its total score and most individual items should not be interpreted as reliable substitutes for objective sleep monitoring. In contrast, actigraphic measure of sleep efficiency appears to be a clinically relevant marker of delirium risk. From a clinical perspective, these findings suggest that reliance on subjective sleep assessment alone may be insufficient for risk stratification, and that objective monitoring may help identify patients at increased risk of delirium in routine hospital practice.
Data Sharing Statement
The datasets generated and analysed during this work are available from the corresponding author on reasonable request.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Faculty of Medicine, University of Ostrava (Ref. No. R2/2021), the Ethics Committee of University Hospital Ostrava (Ref. No. 524/21), and the Ethics Committee of the General University Hospital in Prague (Ref. No. 54/21; Grant AVZ VES 2022 VFN). The study is also registered in the at ClinicalTrials.gov (NCT05402280).
Author Contributions
Martin Milata: Conceptualization; Methodology; Formal analysis; Investigation; Writing – original draft; Writing – review & editing.
Hana Locihová: Conceptualization; Methodology; Investigation; Project administration; Writing – original draft; Writing – review & editing.
Marek Šusta: Data curation; Investigation; Writing – original draft; Writing – review & editing.
Karel Šonka: Conceptualization; Methodology; Supervision; Project administration; Funding acquisition; Writing – original draft; Writing – review & editing.
All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project was funded by a Proverbs grant (NEURO23-B), the Cooperatio Program in Neurosciences, Charles University, and General University Hospital in Prague, MH CZ-DRO-VFN64165.
Disclosure
Prof. Dr. Karel Sonka reports grants from Czech Health Research Council, during the conduct of the study; All other authors report no further conflicts of interest in relation to this work.
References
1. Kuhlmann J, Alhammadi E, Mevissen A, et al. Delirium and sleep disturbances-A narrative review. Z Gerontol Geriatr. 2023;56(7):539–11. doi:10.1007/s00391-023-02228-6
2. Buysse DJ, Hall ML, Strollo PJ, et al. Relationships between the Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), and clinical/polysomnographic measures in a community sample. J Clin Sleep Med. 2008;4(6):563–571. doi:10.5664/jcsm.27351
3. American Psychiatric, A. Diagnostic and Statistical Manual of Mental Disorders. DSM-5-TR. Washington, DC: American Psychiatric Publishing; 2022.
4. Farasat S, Dorsch JJ, Pearce AK, et al. Sleep and delirium in older adults. Curr Sleep Med Rep. 2020;6(3):136–148. doi:10.1007/s40675-020-00174-y
5. Kamdar BB, Shah PA, King LM, et al. Patient-nurse interrater reliability and agreement of the Richards-Campbell sleep questionnaire. Am J Crit Care. 2012;21(4):261–269. doi:10.4037/ajcc2012111
6. Richards KC, O’Sullivan PS, Phillips RL. Measurement of sleep in critically ill patients. J Nurs Meas. 2000;8(2):131–144. doi:10.1891/1061-3749.8.2.131
7. Kamdar BB, Needham DM, Collop NA. Sleep deprivation in critical illness: its role in physical and psychological recovery. J Intensive Care Med. 2012;27(2):97–111.
8. Elliott R, Axelin A, Richards KC, et al. Sensitivity and specificity of proposed Richards-Campbell Sleep Questionnaire cut-off scores for good quality sleep during an ICU stay. J Clin Nurs. 2023;32(11–12):2700–2708. doi:10.1111/jocn.16348
9. Lkoul A, Oumbarek K, Bouchriti Y, et al. Sleep quality assessment in intensive care units: comparing actigraphy and the Richards Campbell sleep questionnaire-a pilot study in the moroccan context. Clocks Sleep. 2025;7(3):49. doi:10.3390/clockssleep7030049
10. Locihová H, Žiaková K, Šerková D, et al. The reliability of the Czech version of the Richards-Campbell Sleep Questionnaire. Kontakt. 2019;21(2):128–134. doi:10.32725/kont.2019.001
11. American Psychiatric A. Diagnostic and statistical manual of mental disorders: DSM-5-TR. In: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision. Washington, DC: American Psychiatric Association Publishing; 2022.
12. Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. An Internal Med. 1990;113(12):941–948. doi:10.7326/0003-4819-113-12-941
13. Ancoli-Israel S, Cole R, Alessi C, et al. The role of actigraphy in the study of sleep and circadian rhythms. Sleep. 2003;26(3):342–392. doi:10.1093/sleep/26.3.342
14. Elbaz M, Yauy K, Metlaine A, et al. Validation of a new actigraph motion watch versus polysomnography on 70 healthy and suspected sleep-disordered subjects. J Sleep Res. 2012;21(Suppl 1):218.
15. CamNtech. MotionWare software user guide. 2024.
16. Marino M, Li Y, Rueschman MN, et al. Measuring sleep: accuracy, sensitivity, and specificity of wrist actigraphy compared to polysomnography. Sleep. 2013;36(11):1747–1755. doi:10.5665/sleep.3142
17. Smith MG, Cordoza M, Basner M. Environmental noise and effects on sleep: an update to the WHO systematic review and meta-analysis. Environ Health Perspect. 2022;130(7):76001. doi:10.1289/EHP10197
18. Aluzaite K, Wu H, Hyslop B, et al. Perceived versus objective sleep quality in long-stay hospitalised older adults-a mixed methods study. Age Ageing. 2021;50(3):955–962. doi:10.1093/ageing/afaa292
19. Hawker GA, Mian S, Kendzerska T, et al. Measures of adult pain: visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011;63(Suppl 11):S240–52. doi:10.1002/acr.20543
20. Alfano CA, Patriquin MA, De Los Reyes A. Subjective – objective sleep comparisons and discrepancies among clinically-anxious and healthy children. J Abnorm Child Psychol. 2015;43(7):1343–1353. doi:10.1007/s10802-015-0018-7
21. Krizan Z, Hisler G. Personality and sleep: neuroticism and conscientiousness predict behaviourally recorded sleep years later. Euro J Personality. 2019;33(2):133–153. doi:10.1002/per.2191
22. O’Brien E, Hart C, Wing RR. Discrepancies between self-reported usual sleep duration and objective measures of total sleep time in treatment-seeking overweight and obese individuals. Behav Sleep Med. 2016;14(5):539–549. doi:10.1080/15402002.2015.1048447
23. Locihova H, Jarošová D, Šrámková K, et al. Sleep quality of patients on a general department during the first days of hospitalization. Nat Sci Sleep. 2025;17:505–515. doi:10.2147/NSS.S501743
24. Ritmala-Castren M, Axelin A, Richards KC, et al. Investigating the construct and concurrent validity of the Richards-Campbell Sleep Questionnaire with intensive care unit patients and home sleepers. Aust Crit Care. 2022;35(2):130–135. doi:10.1016/j.aucc.2021.04.001
25. Fekedulegn D, Andrew ME, Shi M, et al. Actigraphy-based assessment of sleep parameters. Ann Work Expo Health. 2020;64(4):350–367. doi:10.1093/annweh/wxaa007
26. Ohayon M, Wickwire EM, Hirshkowitz M, et al. National sleep foundation’s sleep quality recommendations: first report. Sleep Health. 2017;3(1):6–19. doi:10.1016/j.sleh.2016.11.006
27. Boulos MI, Jairam T, Kendzerska T, et al. Normal polysomnography parameters in healthy adults: a systematic review and meta-analysis. Lancet Respir Med. 2019;7(6):533–543. doi:10.1016/S2213-2600(19)30057-8
28. Buchholz M, Engel L, Kleinke F, et al. Discrepancies between self- and proxy-rated quality of life in people living with dementia. Alzheimers Dement. 2024;10(2):e12486.
29. Locihová H, Axmann K, Žiaková K, et al. Sleep quality assessment in intensive care: actigraphy vs. Richards-Campbell sleep questionnaire. Sleep Sci. 2020;13(4):235–241.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.