Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Validation of the Dutch Version of the Brief Negative Symptom Scale
Authors Seelen-de Lang BL ![]() , Boumans CE
, Boumans CE ![]() , Nijman HLI
, Nijman HLI
Received 8 July 2020
Accepted for publication 19 September 2020
Published 29 October 2020 Volume 2020:16 Pages 2563—2567
DOI https://doi.org/10.2147/NDT.S269037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Birgit L Seelen-de Lang,1 Christien E Boumans,2 Henk LI Nijman3
1Flexible Assertive Community Treatment-Team, GGZ Oost Brabant, Boekel, the Netherlands; 2Long-Term Clinical Care, GGZ Oost Brabant, Boekel, the Netherlands; 3Behavioural Science Institute, Radboud University, Nijmegen, the Netherlands
Correspondence: Birgit L Seelen-de Lang
GGZ Oost Brabant, PO Box 3, Boekel 5427 ZG, the Netherlands
Tel +31 6 52612286
Email [email protected]
Purpose: The Brief Negative Symptom Scale (BNSS) was developed to measure negative symptoms of schizophrenia. However, the Dutch translation of this instrument, called the “Korte Schaal voor Negatieve Symptomen” (KSNS), has not yet been validated. This study investigates the validity and reliability of this Dutch version of the instrument.
Patients and Methods: The Psychotic Symptom Rating Scale (PSYRATS), Calgary Depression Scale for Schizophrenia (CDSS), the Health of the Nation Scale (HoNOS) and the KSNS were used for routine outcome monitoring to measure symptoms in 28 patients with a psychotic disorder who were being treated on a long-stay ward.
Results: The internal consistency of the KSNS is fair to good. The inter-rater reliability is excellent. The concurrent validity is moderate but acceptable. The correlations between the KSNS and scales for depression and positive symptoms were not significant, which indicate good divergent validity.
Conclusion: Despite the small sample size of the current study, we conclude that the BNSS, called the KSNS in Dutch, appears to be a reliable and valid tool for investigating negative symptoms in detail in patients with psychotic disorders.
Keywords: BNSS, Dutch translation, negative symptoms, schizophrenia, validation
Introduction
Patients with a disorder in the schizophrenia spectrum can suffer from a broad range of symptoms. Positive symptoms like hallucinations and delusions have traditionally received much attention in diagnostics, treatment and scientific research. Various pharmacological, psychosocial and psychotherapeutic interventions are available to treat positive symptoms and improve functioning.2 Other core symptoms of schizophrenia, such as negative symptoms and disorganization, can be at least as debilitating.3
While positive symptoms reflect an excess or distortion of normal function, negative symptoms refer to a diminution or absence of normal behaviors related to motivation and interest or expression.4 The term negative symptoms is a general descriptive term that is used without consideration of the cause, longitudinal stability, or duration of the symptoms.4 The prevalence of negative symptoms in patients with schizophrenia is estimated at 15–20% in outpatients and 20–25% in clinical patients.5 Negative symptoms result in a poorer prognosis6,7 and no treatments have yet been shown to be effective for negative symptoms.8,9
Early studies indicated that negative symptoms were unidimensional and distinct from psychosis and disorganization in patients with schizophrenia. Later factor analysis on the construct of negative symptoms alone however, discovered that negative symptoms can be regarded as multidimensional.10
In 2005, an international meeting reached consensus on five domains in which negative symptoms can be distinguished:5,10 reduced ability to experience pleasure (anhedonia), inability to associate with others (asociality), reduced motivation and purposefulness (avolition), reduced expression of emotion (blunted affect) and impaired speech (alogia). As these five domains were not measured sufficiently by the existing instruments, a new instrument was developed, the Brief Negative Symptom Scale (BNSS). Recent cross-cultural research revealed that the latent structure of negative symptoms is still best conceptualized in the five domains mentioned above.3,10,11
Validation studies of the BNSS have demonstrated that it has good psychometric qualities: inter-rater reliability (ICC 0.96), test-retest reliability (r = 0.81) and internal consistency (Cronbach’s alpha 0.93) are all excellent. The convergent and divergent validity are also good.1,12
The BNSS has been translated and validated into various languages namely: Spanish, Italian, Turkish, German, Brazilian, Danish, Japanese, Polish and Korean.13–21 A Dutch translation of the BNSS was made by Staring et al22 which is called the “Korte Schaal voor Negatieve Symptomen”, or KSNS in short. This Dutch version of the scale has not yet been validated. The aim of this pilot study was to determine the reliability and validity of the KSNS.
Patients and Methods
Study Design and Subjects
GGZ Oost Brabant (a large mental health-care institute located in the South of the Netherlands) initiated dimensional, more detailed, diagnostics in the long-term clinical care setting for patients with schizophrenia spectrum disorder. For this purpose, symptom-specific instruments were added to the generic instruments of Routine Outcome Monitoring (ROM). The KSNS was one of these symptom-specific instruments.
Practitioners were trained to use these instruments. In one component of the training, pairs of practitioners conducted the interviews with the patients, and scored the results independently of each other (duo measurements). Afterwards, consensus was reached through discussion and the result was recorded in the patient file. Video recordings of interviews were also viewed jointly by all practitioners and – after independent scoring – were discussed. The scores of the separate practitioners were included as data in this study.
Data from patients diagnosed outside the schizophrenia spectrum and from patients who objected to the use of their data for scientific research were excluded. Patients who participated in the video recordings had given their written informed consent. To determine the reliability and validity of the KSNS we used this data retrospectively. At the introduction of the symptom-specific instruments into the ROM, all patients were asked whether they objected to the use of their anonymous data for research purposes. The written answer was kept in the patient file. This procedure was according to the then prevailing Dutch legal regulations and was approved by the institutional review board. To protect the privacy of the patients, only global and anonymous patient characteristics, along with the KSNS, PSYRATS, CDSS and HoNOS scores were stored in the research data file.
From the 37 patients residing at this long-stay psychiatric department, 28 patients who were diagnosed with a schizophrenia spectrum disorder were included in the current study. For these 28 patients, 17 independent assessments with the KSNS of pairs of two clinicians were available to explore the inter-rater reliability. Four patients also provided written consent to record the interview on video, so that the interview could also be scored by multiple raters. These recordings were scored by eight different raters.
Measuring Instruments
The KSNS is a semi-structured interview developed to measure the level of negative symptoms in schizophrenia spectrum disorders. The scale consists of 13 items in six sub-scales. Items are scored on 7-point scales (range 0 to 6). Approximately 15 minutes are required to complete the instrument. As mentioned earlier, the KSNS is a Dutch translation of the BNSS.1 The translation into Dutch was made Staring and colleagues22 after having received approval for this from the original authors of the scale. This first Dutch translation of the instrument was then sent to a certified independent translator for back translation into English. The differences between the English translation of the translator and the original English version of the BNSS were then assessed and discussed by the original authors of the BNSS together with the translating Dutch research group of Staring et al, and issues concerning differences were resolved and agreed upon (Staring, personal communication, August 31st, 2020).
In addition to the KSNS, the Psychotic Symptom Rating Scale (PSYRATS),23,24 Calgary Depression Scale for Schizophrenia (CDSS25 Dutch translation by Dingemans), and the Health of the Nation Scale (HoNOS)26 were used. The PSYRATS provides separate scores for hallucinations (AHRS) and delusions (DRS).
Data Analysis
The internal consistency of the KSNS was determined by means of Cronbach’s alpha and the correlation between the scores on individual scales and the total score.
The inter-rater reliability was determined on the basis of the duo measurements and the video measurements. The degree of agreement was calculated by the intraclass correlation coefficient (ICC) of the total score and the individual subscales. To determine the convergent validity we calculated the correlation between the KSNS score and the score on the item of the HoNOS that assesses withdrawal of social relationships. The correlations between the KSNS and the CDSS and PSYRATS and the item of the HoNOS that relates to depression and suicidal tendencies were calculated to assess the divergent validity.
Results
Subjects
Of the 28 subjects, 22 were men. The average age was 44.8 years (sd = 13.6). The average treatment duration was 166 months (sd = 112). Schizophrenia was most frequently diagnosed (75%) in the sample, followed by schizoaffective disorder (17.9%), and psychotic disorder NOS (7.1%).
Reliability
Internal Consistency
The internal consistency of the KSNS was 0.79 (see Table 1). The correlations between scores on the various scales of the KSNS and the KSNS total score were all significant.
 |
Table 1 Descriptive Statistics and Correlations of the Scales with the KSNS Total Score |
Inter-Rater Reliability
The ICC’s based on the 17 patients for whom duo measurements were available varied from 0.84 to 0.92 (average measures) and from 0.73 to 0.86 (single measures), with exception of the blunted affect sub-scale, which was 0.55 (average measures) and 0.37 (single measures). Based on the video measurements of four patients assessed by eight raters, the ICC (average measures) of both the KSNS total score and the sub-scales was excellent (0.88–0.97) and the ICC (single measures) was fair to good (0.61–0.81), except for the avolition sub-scale (0.48) (see Table 2).
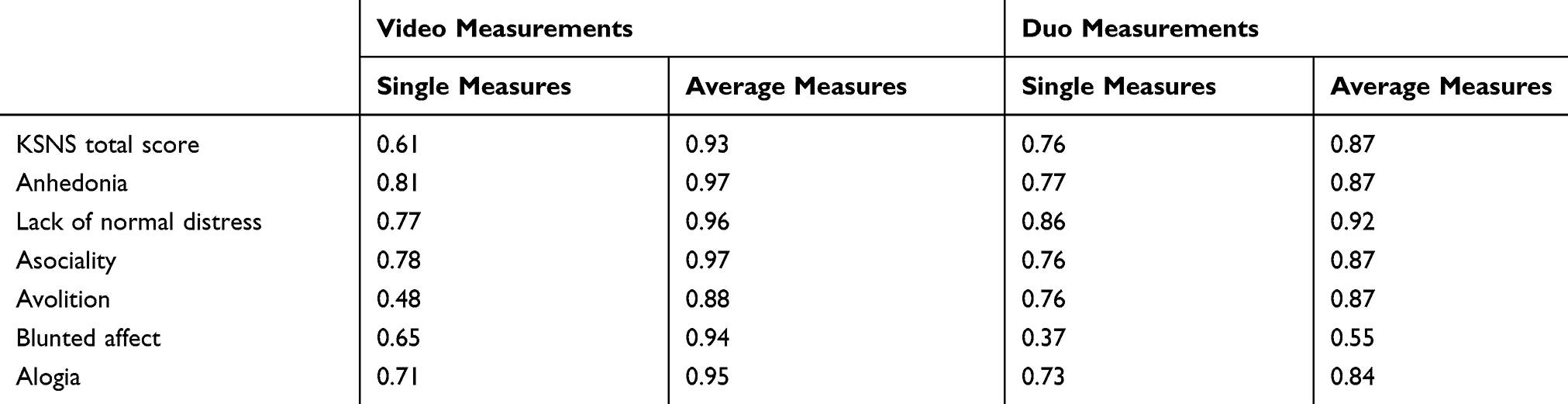 |
Table 2 ICCs of the Video Measurements and Duo Measurements |
Convergent Validity
The Spearman correlation between the KSNS total score and the score on the HoNOS concerning “withdrawal from relationships” was 0.49 (p <0.05).
Divergent Validity
The correlations between the KSNS total score and both HoNOS question 7 (“depression and suicidal tendencies”) and the CDSS total score were not significant (r = 0.20, p = 0.37; r = 0.17, p = 0.40, respectively). The correlations between the KSNS total score and both the DRS and the AHRS were also not significant (r = 0.20, p = 0.41; r = −0.03, p = 0.90).
Discussion
The BNSS previously was translated and tested in various other languages. In the current study, we investigated the psychometric qualities of the Dutch translation made by Staring and colleagues,22 called the KSNS.
It was found that the internal consistency of the KSNS is good (0.79). A Cronbach’s alpha of around 0.8 is considered almost optimal by Field.27 The inter-rater reliability of the KSNS, based on both average and single measures, was also found to be high.
The convergent validity with the question from the HoNOS that relates to withdrawal from relationships was moderate, but acceptable. The insignificant correlations with the CDSS, DRS, AHRS and HoNOS depression and suicidal tendencies question indicate that the KSNS can adequately distinguish negative symptoms from depressive symptoms, as well as from positive symptoms such as delusions and hallucinations. This is important for decisions about treatment. In case of negative symptoms, it is important to support the patient from a disability model approach. Treatment and support can help patients to accept their limitations and help can be provided so they are hampered as little as possible by their negative symptoms in their activities of daily living. If the KSNS gives no indication of negative symptoms, further diagnosis of the origin of impaired functioning is important, so that adequate treatment of a potential depression, delusions or hallucinations is offered.
The small sample size is a clear limitation of the current study. All the studied associations however were significant in the directions hypothesized beforehand, and the current results give further support to earlier findings of reliability and validity of the BNSS. Significant results in the expected and hypothesized direction in a limited sample as was used in the current sample in fact indicate that the effect sizes, and the clinical relevance, of the instrument are rather large.
A second limitation is that only one question from one questionnaire, the HoNOS, was used for convergent validity instead of using the SANS or PANSS-negative scale. As the long-term clinical population is difficult to involve in research, we avoided to include an extra questionnaire. In this way, we aimed to optimize the response rate and to improve ecological validity.
Conclusion
The Dutch version of the BNSS, called the KSNS, seems to be a suitable instrument with sufficient psychometric qualities to identify (and distinguish) negative symptoms in clinical practice.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
The study was approved by the institutional scientific board named CWOI of GGZ Oost Brabant. Because it was a retrospective non-interventional study, no additional ethical approval was required. More details are included in the method section (study design and subjects).
Disclosure
None of the authors report conflicts of interest in this work.
References
1. Kirkpatrick B, Strauss GP, Nguyen L, et al. The brief negative symptom scale: psychometric properties. Schizophr Bull. 2011;37(2):300–305. doi:10.1093/schbul/sbq059
2. Alphen C, Ammeraal M, Blanke C, et al. Multidisciplinaire Richtlijn Schizofrenie. Utrecht: De Tijdstroom; 2012.
3. Strauss GP, Esfahlani FZ, Galderisi S, et al. Network analysis reveals the latent structure of negative symptoms in schizophrenia. Schizophr Bull. 2018;45(5):1033–1041. doi:10.1093/schbul/sby133
4. Correll CU, Schooler NR. Negative symptoms in schizophrenia: a review and clinical guide for recognition, assessment, and treatment. Neuropsychiatr Dis Treat. 2020;16:519–534. doi:10.2147/NDT.S225643
5. Kirkpatrick B, Fenton WS, Carpenter WT, Marder SR. The NIMH-MATRICS consensus statement on negative symptoms. Schizophr Bull. 2006;32(2):214–219. doi:10.1093/schbul/sbj053
6. Rabinowitz J, Levine SZ, Garibaldi G, Bugarski-Kirola D, Berardo CG, Kapur S. Negative symptoms have greater impact on functioning than positive symptoms in schizophrenia: analysis of CATIE data. Schizophr Res. 2012;137(1–3):147–150. doi:10.1016/j.schres.2012.01.015
7. Fervaha G, Foussias G, Agid O, Remington G. Impact of primary negative symptoms on functional outcomes in schizophrenia. Eur Psychiatr. 2014;29(7):449–455. doi:10.1016/j.eurpsy.2014.01.007
8. Fusar-Poli P, Papanastasiou E, Stahl D, et al. Treatments of negative symptoms in schizophrenia: meta-analysis of 168 randomized placebo-controlled trials. Schizophr Bull. 2015;41(4):892–899.
9. Aleman A, Lincoln TM, Bruggeman R, Melle I, Arends J, Knegtering H. Treatment of negative symptoms: where do we stand, and where do we go? Schizophr Res. 2017;186:55–62. doi:10.1016/j.schres.2016.05.015
10. Ahmed AO, Kirkpatrick B, Galderisi S, et al. Cross-cultural validation of the 5-factor structure of negative symptoms in schizophrenia. Schizophr Bull. 2018;45(2):305–314. doi:10.1093/schbul/sby050
11. Strauss GP, Nunez A, Ahmed AO, et al. The latent structure of negative symptoms in schizophrenia. JAMA Psychiatr. 2018;75(12):1271–1279. doi:10.1001/jamapsychiatry.2018.2475
12. Strauss GP, Hong LE, Gold JM, et al. Factor structure of the brief negative symptom scale. Schizophr Res. 2012;142(1–3):96–98. doi:10.1016/j.schres.2012.09.007
13. Mane A, Garcia-Rizo C, Garcia-Portilla MP, et al. Spanish adaptation and validation of the brief negative symptoms scale. Compr Psychiatry. 2014;55(7):1726–1729.
14. Mucci A, Galderisi S, Merlotti E, et al. The Brief Negative Symptom Scale (BNSS): independent validation in a large sample of Italian patients with schizophrenia. Eur Psychiatry. 2015;30(5):641–647. doi:10.1016/j.eurpsy.2015.01.014
15. Polat Nazli I, Ergul C, Aydemir O, Chandhoke S, Ucok A, Gonul AS. Validation of Turkish version of brief negative symptom scale. Int J Psychiatry Clin Pract. 2016;20(4):265–271. doi:10.1080/13651501.2016.1207086
16. Bischof M, Obermann C, Hartmann MN, et al. The brief negative symptom scale: validation of the German translation and convergent validity with self-rated anhedonia and observer-rated apathy. BMC Psychiatr. 2016;16(1):415. doi:10.1186/s12888-016-1118-9
17. de Medeiros HLV, Vasconcelos SC, Elkis H, et al. The brief negative symptom scale: validation in a multicenter Brazilian study. Compr Psychiatry. 2018;85:42–47. doi:10.1016/j.comppsych.2018.06.007
18. Gehr J, Glenthoj B, Odegaard Nielsen M. Validation of the Danish version of the brief negative symptom scale. Nord J Psychiatry. 2019;73(7):425–432. doi:10.1080/08039488.2019.1648549
19. Hashimoto N, Toyomaki A, Oka M, et al. Pilot validation study of the Japanese translation of the Brief Negative Symptoms Scale (BNSS). Neuropsychiatr Dis Treat. 2019;15:3511–3518. doi:10.2147/NDT.S237449
20. Wojciak P, Gorna K, Domowicz K, et al. Polish version of the Brief Negative Symptom Scale (BNSS). Psychiatr Pol. 2019;53(3):541–549. doi:10.12740/PP/OnlineFirst/91490
21. Jeakal E, Park K, Lee E, Strauss GP, Choi KH. Validation of the Brief Negative Symptom Scale in Korean patients with schizophrenia. Asia Pac Psychiatry. 2020;e12382.
22. Staring T, Velthorst E, Berg DVD, Meijer C, Haan LD, Gaag MVD. Korte Schaal voor Negatieve Symptomen (KSNS). Nederlandse vertaling van de Brief Negative Symptom Scale. Dutch Manual. 2018.
23. Drake R, Haddock G, Tarrier N, Bentall R, Lewis S. The Psychotic Symptom Rating Scales (PSYRATS): their usefulness and properties in first episode psychosis. Schizophr Res. 2007;89:119–122. doi:10.1016/j.schres.2006.04.024
24. Haddock G, McCarron J, Tarrier N, Faragher EB. Scales to measure dimensions of hallucinations and delusions: the psychotic symptom rating scales (PSYRATS). Psychol Med. 1999;29(4):879–889. doi:10.1017/S0033291799008661
25. Lako IM, Bruggeman R, Knegtering H, et al. A systematic review of instruments to measure depressive symptoms in patients with schizophrenia. J Affect Disord. 2012;140(1):38–47. doi:10.1016/j.jad.2011.10.014
26. Mulder CL, Staring ABP, Loos J, Buwalda VJA, Kuijpers WAI. De Health of the Nation Outcome Scales (HONOS) als instrument voor ‘routine outcome assessment’ [The Health of the Nation Outcome Scales (HONOS) in Dutch translation as an instrument for Routine Outcome Assessment]. Tijdschr Psychiatr. 2004;46:273–284.
27. Field A. Discovering Statistics Using SPSS. Los Angeles: Sage; 2009.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.