")
Back to Journals » Patient Preference and Adherence » Volume 15
Validation of the Chinese Version of the Patient’s Communication Perceived Self-Efficacy Scale (PCSS) in Outpatients After Total Hip Replacement
Authors Liu J, Zhao H, Capone V , Li Z, Wang J, Luo W
Received 12 January 2021
Accepted for publication 8 March 2021
Published 19 March 2021 Volume 2021:15 Pages 625—633
DOI https://doi.org/10.2147/PPA.S301670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Jing Liu,1,* Huiwen Zhao,2,* Vincenza Capone,3 Ziyi Li,1 Jing Wang,1 Wen Luo2
1Traumatic Orthopedics Department, The 3rd Ward of Hip Joint Surgery, Tianjin Hospital, Tianjin, People’s Republic of China; 2The 2nd Ward of Joint Surgery, Tianjin Hospital, Tianjin, People’s Republic of China; 3Department of Humanities, University of Naples ‘Federico II’, Napoli, Italy
*These authors contributed equally to this work
Correspondence: Wen Luo
The 2nd Ward of Joint Surgery, Tianjin Hospital, 406 Jiefangnan Road, Tianjin, 300211, People’s Republic of China
Tel +86 22-13116190054
Email [email protected]
Background: Among older people in the world, older patients’ communication has become a public health issue of vital importance. Such communication could be improved by different interventions. However, a means of measuring patient’s communication confidence in these measures has not been established in China. This study is aimed at translating and introducing the Patient’s Communication Self-Efficacy Scale for communication between doctors and patients after total hip replacement.
Method: (1) A questionnaire was completed after a consultation by 167 patients (mean age = 70.04 years; SD: 6.3 years; females/males: 94/73). Translation of the original English version PCSS into the Chinese; (2) Validation of the final Chinese version of the PCSS. Measurement indexes included item generation, reliability testing, construct validity and test–retest reliability. To actualize the above test, we used SPSS 19.0 software and LISREL 8.7. We build the Bayesian Network Model of the Chinese version of the PCSS and determined predictive variables.
Result: Confirmatory factor analysis showed that the Chinese version of the PCSS has fit a three-dimensional model. Meanwhile, the Chinese version of the PCSS has high internal consistency (Cronbach’s α coefficient 0.929) and test–retest reliability (Kappa coefficient 0.761). Analysis using Bayesian networks shows that the important predictors are education (0.4207), PEPPI 3(0.3951), and PCSS 1(0.1139). The connections between PCSS 3 and other variables do not indicate causality, conditional dependencies or inter-relatedness.
Conclusion: This is the first study to validate the Chinese version of the PCSS in outpatients after total hip replacement. Our results confirmed that the Chinese version of the scale has high internal consistency, construct validity and test–retest reliability. And the patient–doctor interaction and education are important predictors of patient’s communication self-efficacy.
Keywords: communication, self-efficacy, total hip replacement, validation
Background
Communication with other people is the important part of persons’ life, which is necessary for social activities, for example, working, learning and so on, taking the simple act of people can communicate in simple and routine tasks requiring a simple and direct exchange of information.1 As we know, the communication between the doctor and the patient is not always balanced, and the doctor has the power to dominate the whole conversation, so the patient plays a passive role in the talk, which leads to some obstruction of communication.2 The patient–doctor communication is central to the process of health education. Research on conflict between doctor and patient on overseas involve to: Social role theory, doctor-patient exchange theory, asymmetric information theory and health care system.3 In most industrialized countries, the main trend in health care is to pay more and more attention to the interests, needs and attributes of patients: patients are increasingly seen as the main body in doctor–patient interaction and influential actors in the health care system to help practitioners provide care that is consistent with the values, needs and preferences of patients, and to allow patients to provide advice and participate in health and health care Health decision-making activities.4,5
Self-efficacy concerns the individual’s belief that he/she is capable of performing a certain task and producing a desired effect: it reflects the person’s perceptions of their capability for specific tasks, as distinct from their actual ability. It is closely related to the result of expected action. An analysis of the literature shows that self-efficacy is a valuable and important structure for predicting behavior in clinical, academic and employment environments. According to Social Cognitive theory, self-efficacy has a great impact on human behaviour.6 Greater self‐efficacy has been shown to improve outcomes and function for a variety of geriatric conditions. Studies highlighted as, after cardiac surgery, a high level of self-efficacy is conducive to the rehabilitation, and has a beneficial impact on personal function and well-being.7 Communication self-efficacy has been confirmed that is the important method of improving patients’ satisfaction and reducing medical errors.8
Total hip replacement is effective in reducing pain, improving function and quality of life for persons with osteoarthritis or other joint diseases.9,10 In Sweden, more than 30,000 total hip and knee replacements are performed annually with an average age at surgery of about 68 years, almost 60% of whom are women.11 According to Kurtz,12 hip replacement will increase by 174% by 2030. In 2014, the number of total hip replacement in China was close to 240,000 cases. With the popularization of standardized surgical techniques and the improvement of patients’ acceptance of surgery, the volume of total hip replacement is expected to continue to grow at a faster speed.13 Health education and rehabilitation is the important part after total hip replacement. Communication is the central process of health education and rehabilitation. Effective patient–doctor communication has been shown to be associated with a broad range of improving outcomes of treatment.14
A literature review of patients’ experience in health care concluded that was necessary to develop and test a new questionnaire for related researches.15 For a long time, it was a lack of fully validated tools in the specific environment of outpatients’ hospital care, especially to assess the communication self-efficacy of patients in medical experience. The Patient’s Communication Perceived Self-Efficacy Scale (PCSS) has been developed by Capone and Petrillo, to measure outpatient confidence as regards the individuals’ ability to successfully master situations related to communication with doctors, in outpatients.16 The scale is composed of 16 items has a three-factor structure of self-efficacy, namely, self-efficacy in “Provide and Collect information”, “Express concerns and doubts”, “Verify information”, tapping a second-order factor, defined as patient communication self-efficacy. The results of the construction and validation study showed that the PCSS is a simple, valid and reliable measurement which can be used in clinical research to assess patients’ communication self-efficacy.16 In China, research on the confidence of patients’ communication is at an infancy stage, and, to the best of our knowledge, no questionnaire is available for measurement of outpatients’ communication self-efficacy with doctors.
To date, the structural validity and test–retest reliability of the PCSS have been confirmed in the population.16 Therefore, the aim of this study was to test the structural validity, internal consistency, test–retest reliability, and build the Bayesian networks modeling of the Chinese version PCSS in a clinical sample of outpatients after total hip replacement.
We expect to confirm the correlated three-factor structure as found in the original study (Provide and Collect information”, “Express concerns and doubts”, “Verify information) and that a higher-order latent factor for communication self-efficacy can be empirically validated.
Availability of data and material: No additional data are available.
Method
Design
This is the methodological study which used the cross-sectional survey method and divided into two steps: (1) translation of the English version PCSS into Chinese and (2) validation of the Chinese version PCSS in outpatients after total hip replacement between June and August in 2020.
According to the Chinese law for medical research with humans, Hospital Medical ethics committee gave approval for this survey study (TJYY-2020-YLS-043).
Data Collection
Based on the requirements of the confirmed factor analysis (CFA), we need enough outpatients after total hip replacement in this survey.17
The Requirements of Sample Size in Factor Analysis
The ratio between the collected samples and the items of the scale should be above 5:1. In practice, the ideal number of participants should be achieved 10~25 times of the items.18 In this research, the number of samples has more than 150, which met the ideal condition.
According to the Chinese law for medical research with humans, ethical approval was indicated for this survey study.
Participants
Patients
The Hospital Research Ethics Committee approved the study protocol and patients provided informed consent before participation. At the beginning of the study, the respondents were informed about the investigated aim, participants’ rights, and researchers’ obligations to participants. The investigators used uniform language to explain the points for filling the scales in this survey. All questionnaires have been filled out by outpatients independently. The privacy of the participants was protected during the whole study. The survey was conducted between June and August in 2020, involving outpatients after total hip replacement through the orthopedic trauma department. We randomly selected patients in the database.
Inclusion criteria: (1) outpatients after unilateral primary total hip replacement, who have not complications; (2) conscious and have enough comprehension ability; (3) aged >60 years; (4) no deformed limb, Barthel Index19 (BI) >60; (5) written informed consent before the survey.
Exclusion criteria: (1) Through the medical history and preoperative examination, who has nervous system diseases, such as Alzheimer’s disease that influenced reading, comprehension and so on; (2) inability to communicate with others such as deafness, aphasia and so on.
According to the Chinese law for medical research with humans, Tianjin Hospital Medical ethics committee gave approval for this research (TJYY-2020-YLS-043).
The survey was performed self-administered. Previously, the investigators explained the aim of the survey, participants’ rights and obligations and gained consent from the participants. The privacy of the participants was protected during the whole investigation process, and all the scales were collected in 10 min. At the end of the survey, patients were asked if they were willing to complete the second (approximately two weeks) and the third (approximately two months) questionnaire survey later.
Adaptation of the Original Version PCSS into Chinese
The original version PCSS has been translated into Chinese according to the cross-cultural adaptation methodology. This methodology includes 5 stages: initial translation, synthesis of translation, back-translation, the assessment of experts, field testing.20 Firstly, the PCSS has been translated into Chinese by two senior translators, who are the professional bilingual translators with medical educational background. They worked out a report, respectively (T1 and T2). Secondly, the third translator with medical educational background joined the team to discuss the translated reports. Subsequently, they summarized the third translation report (T3). Thirdly, T3 has been back-translated by two other translators who studied in England more than one year, generating the back-translated report, respectively (BT1 and BT2). Fourthly, the expert committee met for discussion and reached a consensus on all translated items. Following this meeting, five participants were recruited to help in a preliminary test to determine the readability and feasibility of the final version PCSS. The participants and researchers evaluated the specific contents of the scale and produced a draft ready for testing (Table S1).
Other Scales for Validation
The perceived efficacy of patient–physician interactions (PEPPI-10) was developed to assess individuals’ self-efficacy in obtaining medical information and attention to their chief health concern from a physician or doctor.21 The PEPPI had two English versions: 10-item full-scale and 5-item simple-scale. Cronbach’s α coefficients of PEPPI-10 were 0.91, which exhibited reliable theoretical basis and feasibility in clinical research. The Chinese version PEPPI has good validity and reliability in patients with severe knee osteoarthritis (Cronbach’s α coefficient 0.907).22 The Chinese version PEPPI has been consisted of 10 items. All items are rated on an 11-point Likert-type scale, ranging from 0 = “not at all confident” to 10=“completely confident”.A total score is calculated by summing the item scores and converted to a range from 0 to 100, where 100 is the best score, which indicates that the individual has a better ability on patient–physician interaction.22
Statistical Analysis
Started by using the statistical methods of SPSS 19.0 software (IBM, 2010) and LISREL 8.7 (Science and software international, Lincoln wood, IL, USA). After collecting the questionnaires, we analyzed the missing data and frequency of the scales. Then, we performed confirmatory factor analysis (CFA) to test the structural validity by LISREL 8.70. Then, we checked the distribution characteristics of the score of the Chinese version PCSS, tested the normality of the total score and determined the possible lower and upper limit effects, evaluating if more than 15% of the participants scored the worst or best on the Chinese version PCSS, which was a lower or upper limit effect.23 CFA was used to test whether the score of the Chinese version PCSS was suitable for the three-factor modeling. In addition, non-standard fitting index (NNFI), comparative fitting index (CFI) and standard root mean square residual (SRMR) have been used to assess the model fitting. NNFI and CFI values ≥0.90 and SRMR values ≤0.08 were considered as sufficient model fitting.24,25 In this study, we used the Cronbach’s α coefficient to examine the internal consistency of the Chinese version PCSS. Cronbach’s α coefficient represents the average split-half reliability coefficient of all items, which is the most common effectiveness measurement index in validate study.26 The score of Cronbach’s α coefficient score is from 0 to 1, 0 means that is no correlation of the items in the scale, and 1 means that is the best correlation of all items in the scale. Many researches proved that Cronbach’s α coefficient is the good index to measure the internal consistency of the scale.27 When the Cronbach’s α coefficient exceeds 0.7 that represents the scale has good internal consistency, which can be used in clinical research.28 The Cohen’s kappa was used to calculate the test–retest reliability in validated study.29 The value of Cohen’s kappa has been used to examine the level of test–retested consistency:29 <0 represents inconsistency; 0.0–0.20 represents slight consistency; 0.21–0.40 represents fair agreement; 0.41–0.60 represents moderate agreement; 0.61–0.80 represents basically consistent; 0.81–1.0 represents completely consistent.
Using the Bayesian network function of SPSS Modeler 18.0. The neural network builds the model by learning the potential correlation between the independent variable (the third score of the Chinese version PCSS) and the dependent variable. Then, the model results are verified by comparing the predicted values with the actual values. In such applications, the neural network system is better than the traditional computer which solves the problem according to a set of instructions.30,31
Results
Participants
Of the 175 participants recruited in the first investigation, 8 were excluded because of missing items in the Chinese version PCSS, leaving 167 for analysis in the structural validity. The demographic and clinical characteristics of the enrolled patients are shown in Table 1. The median (IQR) score of the patients in the Chinese version PCSS was 57 (8). Six patients have been lost follow-up in the second and the third time. Hence, 161 patients have been included in the test–retest reliability and Bayesian networks study. The participants did not have known cognitive impairments, literacy and reading problems.
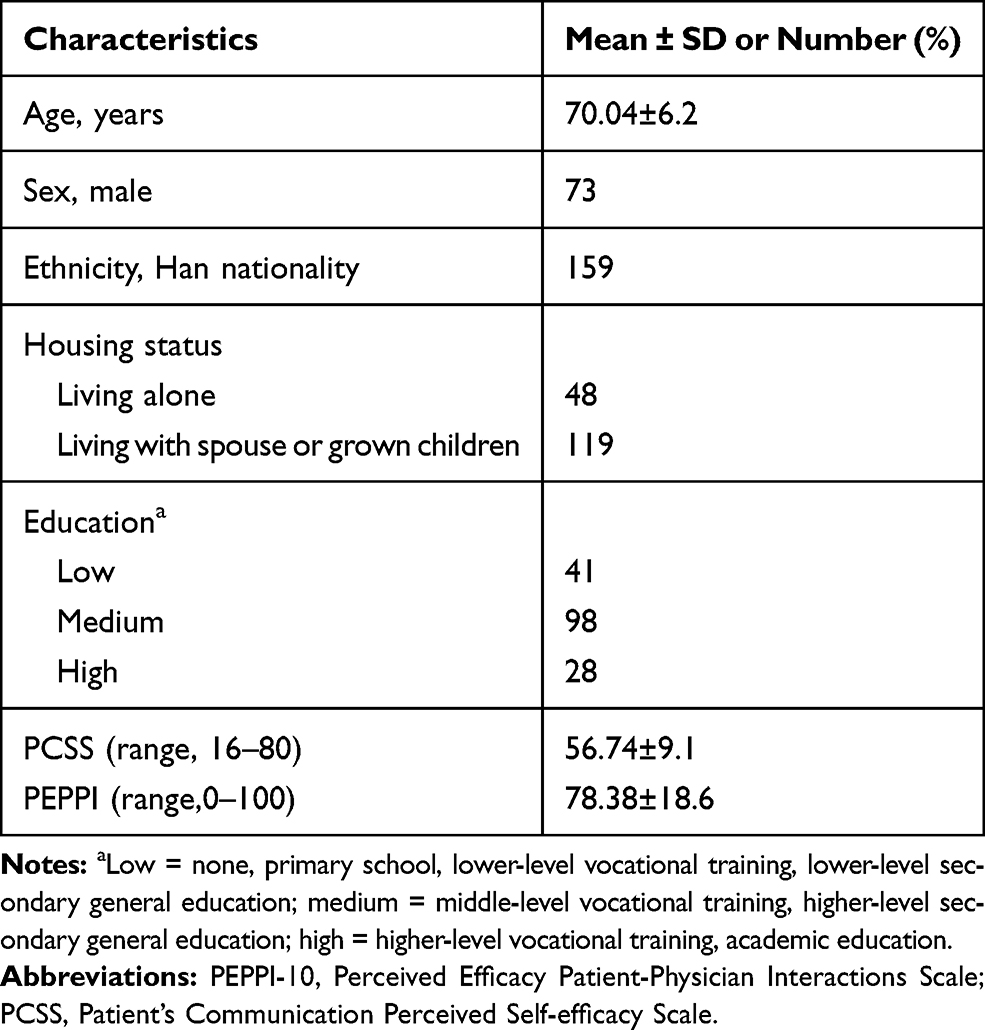 |
Table 1 Sample Characteristics (N=167) |
Structural Validity and Internal Consistency
In our study, the results showed that the Chinese version PCSS has good fit indices for three-factor modeling by Confirmatory factor analysis (CFA)(SRMR=0.073, NNFI=0.90, CFI=0.992), with the exception of the root mean square error of approximation. Standardized factor loading ranged between 0.59 for item 5 and 0.87 for item 2 (Figure 1). Our results showed that the Cronbach’s α coefficient of the Chinese version PCSS was 0.929 with higher internal consistency. Consequently, the results of this research confirmed that the Chinese version PCSS fits three-dimensional (Goodness of Fit Index (GFI) = 0.80).
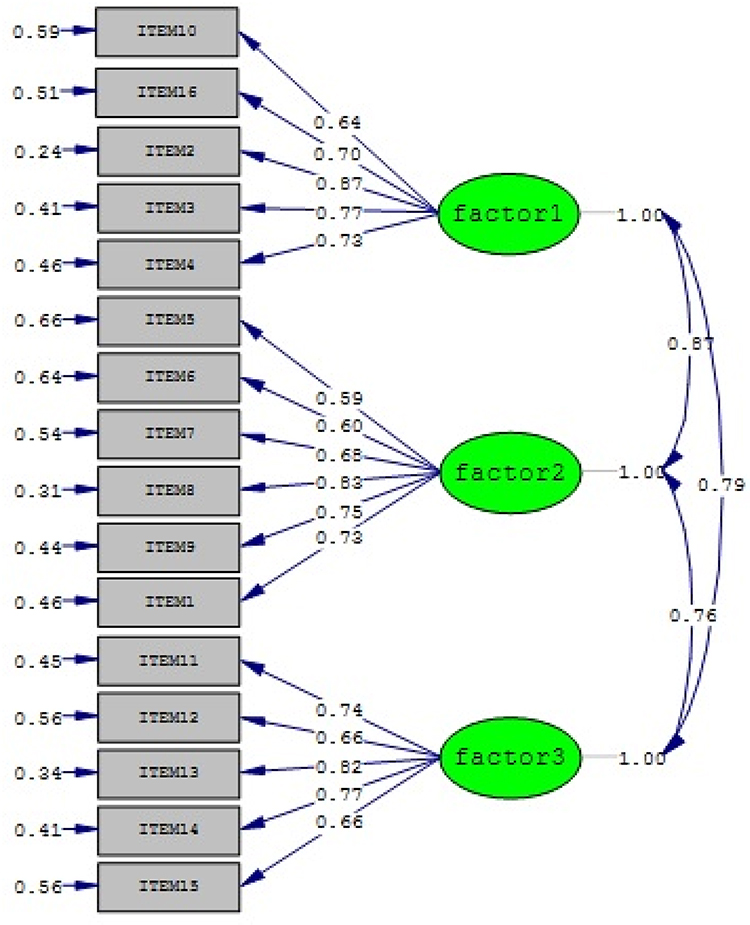 |
Figure 1 Standardized factor loading and residuals for the items of the PCSS. |
Test–Retest Reliability
In this research, we carried out the test–retest reliability of the Chinese version PCSS in outpatients after total hip replacement. Six cases were excluded because of loss to follow-up in the test–retest reliability of the Chinese version PCSS, leaving 161 cases for analysis. The substantial kappa coefficient is 0.761 (Table 2) in test–retest reliability of the C-PCSS, which was over-top the cut-off point for group-level comparisons. So, we carried out the Bland–Altman analysis, which confirmed that the limits of agreement between the two time points were rather narrow, ranging from −7.6 to 7.2 (Figure 2).
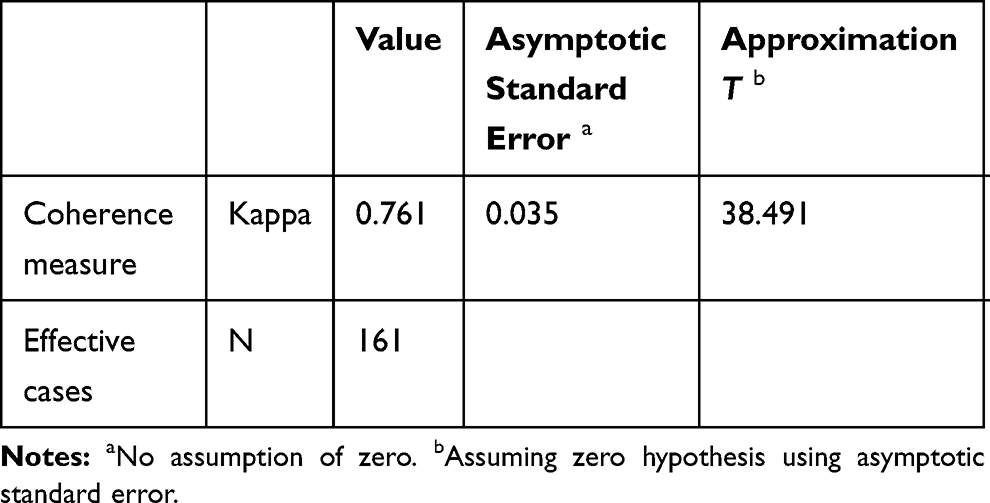 |
Table 2 Symmetry Measure of the Chinese Version PCSS |
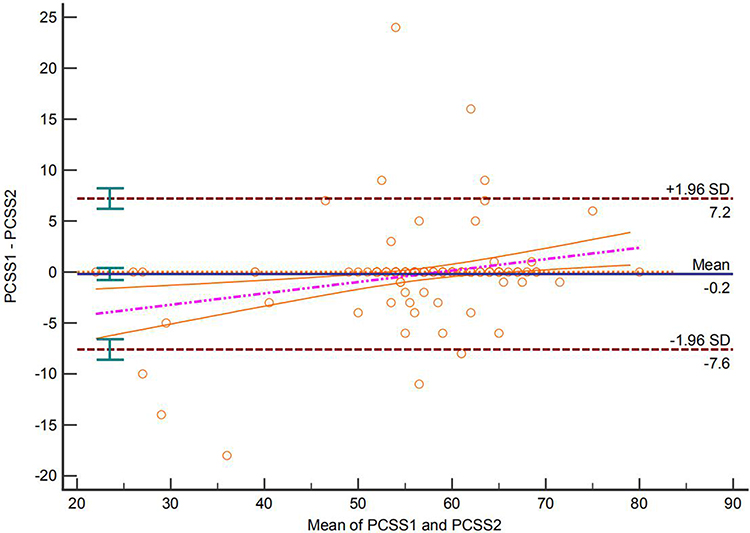 |
Figure 2 Individual agreement between test and retest scores of the Chinese version PCSS. The horizontal solid line represents the mean difference between both scores. The dashed line represents the linear regression line through the data points. The outer dashed lines represent the 95% limits of agreement (mean difference±1.96 SD of the difference). |
Bayesian Networks
First of all, we assigned values to the main variables before building the Bayesian networks (Table 3). Analysis using Bayesian networks shows that the important predictors are education (0.4207), the score of PEPPI in the third time (PEPPI 3)(0.3951), and the score of PCSS in the first time (PCSS 1)(0.1139). The connections between the score of PCSS in the third time (PCSS 3) and other variables do not significantly indicate causality, conditional dependencies or inter-relatedness (Figures 3, and 4).
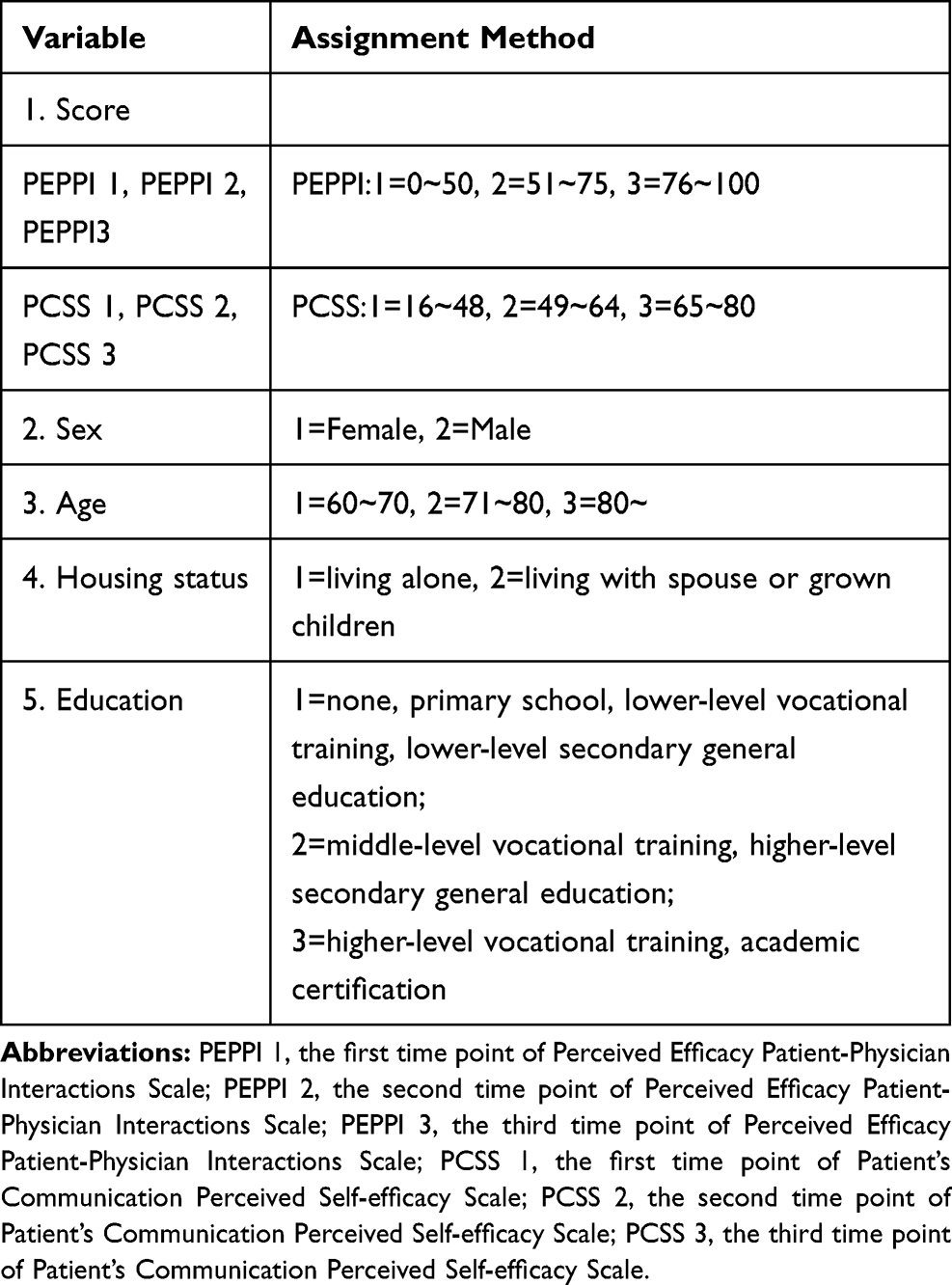 |
Table 3 The Main Variables and Assignments |
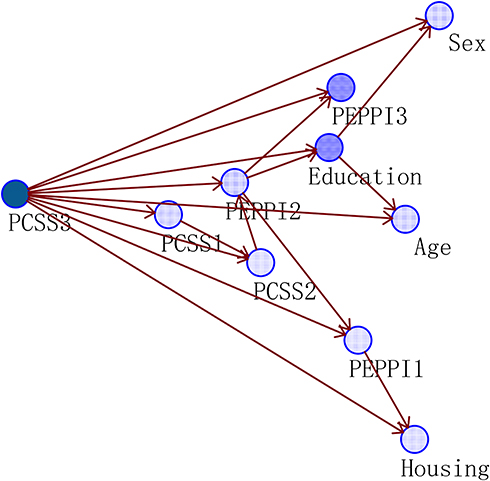 |
Figure 3 Bayesian networks: model summary. |
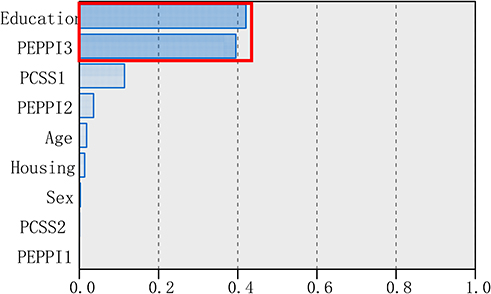 |
Figure 4 Bayesian networks: predictor importance. Important predictors in the red box. |
In summary, we show that behavioral habits such as education and the ability of interaction with physicians make a significant contribution to the incidence of the communication with doctors. People with higher education and good ability of interaction with health workers are more likely to be good confidence in communication with doctors. In comparing various data mining techniques, many researchers found that in a biased data set, only the Bayesian network model worked well because the majority of the predictors in the project were categorical.31,32
Discussion
This is the first study that totally measures the validity and reliability of the Chinese version PCSS in outpatients after total hip replacement. The results of this study confirmed that the Chinese version PCSS has enough validity and reliability to assess the outpatients’ self-efficacy on communication with doctors or nurses. The Chinese version PCSS can be used as a tool for measuring the ability of communication in outpatients after total hip replacement because this scale is simple and valid.
In cross-cultural research, simplistic translation without cross-cultural adaptation and validation is inadequate.33 Confirmatory factor analysis (CFA) is a powerful test method in terms of structural validity.34 We found that the Chinese version PCSS fits three-dimensional construct by confirmatory factor analysis, which was consistent with the study of the original version PCSS.16 These factors offer a context-specific and patient-centered means of examining perceived control related to important roles patients are expected to fulfill in the medical encounter. In this study, the results confirmed that the model of the Chinese version PCSS adequately consistent with the sample data. Although we are unable to explain why the findings are above/below the recommended cut-off, the Chinese version PCSS has high internal consistency, which indicates that all items of scale can explain the same concept, and it should be noted that for simple models with few degrees of freedom could be inflated.35
The test–retest reliability is an important part of the cross-cultural study on evaluation tools. Higher test–retest reliability can discriminate good value of application in the clinical study.29 Bases on the internal consistency and structural validity of the Chinese version PCSS have assumed to indicate that the scale is sufficiently reliable for clinical comparisons. The kappa coefficient of the test–retest reliability was 0.761, which indicating a substantial agreement between two investigations. Meanwhile, the Bland–Altman analysis showed that the predominant source of error has been not significant. Because of the limitation of experimental condition, two weeks between the repeated scales are used to examine test–retest reliability in our study, which might occur the inter-individual variation.36
In this study, we showed that the Bayesian network model can work well in a biased data set because a large number of predictor variables are categorical. The results of Bayesian networks showed that the important predictors are education, PEPPI 3 and PCSS 1. The connections between the PCSS3 and other variables do not indicate causality, conditional dependencies or inter-relatedness. So the results confirm our hypothesis, which the communication’s self-efficacy would be changed over time and had the potential relationship with the efficacy on patient–physician interaction.
The limitations of this study are that (1) the results may lack effective persuasion because the number of samples is limited, especially in Bayesian network model study; (2) this study has not undertook more powerful analyses such as item-response theory; (3) the evidence of criterion-related validity was limited and sensitivity has not been measured. Although the positioning accuracy of all items in the scale must be sufficient in the research,37 But the Chinese version PCSS has targeted clearly, so the requirements would be reduced the number of samples.
Conclusion
This study confirmed that the Chinese version PCSS has a good construct validity and test–retest reliability. The Chinese version PCSS is a valid and reliable scale that can be used in clinical to assess communication’s self-efficacy in outpatients after total hip replacement. Its scale is easy to implement and possesses measurement accuracy. Hence, it could be useful to identify patients’ level of communication self-efficacy in each of its facets, allowing the definition and the design of specific intervention programs. Further study will measure other psychometric properties, especially sensitivity.
Data Sharing Statement
The datasets generated and analysed during the current study are not publicly available because the Ethical Guidelines for Epidemiological Research by the Chinese Government and prohibit researchers from providing their research data to other third-party individuals.
Ethics Approval and Consent to Participant
The current study was approved by the Institutional Ethical Review Board of Tianjin Hospital (No. TJYY-2020-YLS-043) and has been conducted in accordance with the Ethical Guidelines for Epidemiological Research by the Chinese Government and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All study participants provided written informed consent by the completion and submission of the survey.
Consent to Publish
Not applicable.
Acknowledgments
This is a cross-cultural study. The original version of the PCSS was published by Pro. Vincenza Capone in Patient Education and Counseling: Capone V, Petrillo G. Patient’s Communication Perceived Self-efficacy Scale (PCSS): construction and validation of a new measure in a socio-cognitive perspective. Patient Educ Couns, 2014, 95: 340-347. The Chinese version of the PCSS has not been previously published.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. Huiwen Zhao is the co-first author in the article.
Funding
This study was supported by the Tianjin Academy of Nursing (TAN) Grant-in-Aid for Scientific Research (No: tjhlky2020YB01; PI: Miss Huiwen Zhao).
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Kemp KA, Santana MJ, Southern DA, et al. Association of inpatient Hospital experience with patient safety indicators: a cross-sectional, Canadian study. BMJ Open. 2016;6:e011242.
2. Rao JK, Anderson LA, Inui TS, et al. Communication interventions make a difference in conversations between physicians and patients: a systematic review of evidence. Med Care. 2007;45:340–349.
3. Orth JE, Stiles WB, Scherwitz L, et al. Patient exposition and provider explanation on routine interviews and hypertensive patients’ blood pressure control. Health Psychol. 1987;62:29–42.
4. Gruman J, Rovner MH, French EM, et al. From patient education to patient engagement: implications for the field of patient education. Patient Educ Couns. 2010;78:350–356.
5. Van Dam HA, van der Horst F, van den Borne B, et al. Provider-patient interaction in diabetes care: effects on patients self-care and outcome: a systematic review. Patient Educ Couns. 2003;41:17–28.
6. Bandura A. Self-Efficacy: The Exercise of Control. New York: W.H.Freeman; 1997.
7. Scherer Y, Bruce S. Knowledge, attitudes, and self-efficacy and compliance with medical regimen, number of emergency department visits, and hospitalizations in adults with asthma. Heart Lung. 2001;30:250–257.
8. Street RL. Active patients as powerful communication. In: Robinson WP, Giles H, editors. The New Handbook of Language and Social Psychology. New York: Wiley; 2001:541–560.
9. Rolfson O, Karrholm J, Dahlberg LE, Garellick G. Patient-reported outcomes in the Swedish Hip Arthroplasty Register: results of a nationwide prospective observational study. J Bone Joint Surg Br. 2011;93(7):867–875.
10. Baker PN, van der Meulen JH, Lewsey J, Gregg PJ. The role of pain and function in determining patient satisfaction after total knee replacement. Data from the National Joint Registry for England and Wales. J Bone Joint Surg Bri. 2007;89(7):893–900.
11. Garellick GKJ, Lindahl H, Malchau H, Rogmark C, Rolfson OSHPR Swedish Hip Arthroplasty Register, Annual report.2014.
12. Kurtz SM, Ong KL, Lau E, et al. Impact of the economic downturn on total joint replacement demand in the United States: updated projections to 2021. J Bone Joint Surg Am. 2014;96:624–630.
13. Wang QJ, Zhang XL. The current status and hot points of total hip arthroplasty. Chin J Joint Surg. 2015;9(6):718–724.
14. Hern Á ndez-Padilla JM, Cort É s-Rodr Í Guez AE, Granero-Molina J, et al. Design and psychometric evaluation of the ‘clinical communication self-efficacy toolkit’. Int J Environ Res Public Health. 2019;16:4534.
15. Krantz DS, Baum A, von Wideman M. Assessment of preferences for self-treatment and information in health care. J Pers Soc Psychol. 1980;39:977–990.
16. Capone V, Petrillo G. Patient’s Communication Perceived Self-efficacy Scale (PCSS): construction and validation of a new measure in a socio-cognitive perspective. Patient Educ Couns. 2014;95:340–347.
17. Byrne BM, Shavelson RJ, Muthen B. Testing for the equivalence of factor covariance and mean structures—The issue of partial measurement invariance. Psychol Bull. 1989;105:456–466.
18. McDonald RP. Comments on D.J. Bartholomew, Foundations of factor analysis: some practical implications. Brit J Math Stat Psychol. 1985;38:134–137.
19. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61–65.
20. Ramada-Rodilla JM, Serra-Pujadas C, Delclós-Clanchet GL. Cross-cultural adaptation and health questionnaires validation: revision and methodological recommendation. Salud Publica Mex. 2013;55(1):57–66.
21. Maly RC, Frank JC, Marsball GN, et al. Perceived efficacy in patient-physician interactions (PEPPI): validation of an instrument in older persons. J Am Geriatr Soc. 1998;46:889–894.
22. Zhao HW, Luo W, Maly RC, et al. Validation of the Chinese version 10-item perceived efficacy in patient-physician interactions scale in patients with osteoarthritis. Patient Prefer Adher. 2016;10:2189–2195.
23. Terwee CB, Bot SD, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60:34–42.
24. Browne MW, Cudeck R. Alter native ways of assessing model fit. In: Bollen KA, Long JS, editors. Testing Structural Equation Models. Newbury Park: Sage Publications; 1993:136–162.
25. Hu LT, Bentler PM. Cut-off criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. 1999;6:1–55.
26. Cronbach LJ. Co-efficient alpha and the internal structure of tests. Psychometrika. 1951;16:297–334.
27. Crotina JM. What is co-efficient alpha? A examination of theory and applications. J Applied Psychol. 1993;78:98–104.
28. Lohr KN. Assessing health status and quality-of-life instruments: attributes and review criteria. Qual Life Res. 2002;11:193–205.
29. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–174.
30. Kneib T, Hennerfeind A. Bayesian semiparametric multi-state models. Stat Modelling. 2008;8(2):169–198.
31. Verduijn M, Peek N, Rosseel PM, et al. Prognostic Bayesian networks I: rationale, learning procedure, and clinical use. J Biomed Inform. 2007;40(6):609–618.
32. Nagarajan R, Scutari M, Lèbre S. Bayesian Networks in R. New York: Springer-Verlag; 2013.
33. Schutte NS, Malouff JM. General and realm-specific self-efficacy: connections to life functioning. Curr Psychol. 2016;361–369.
34. Hooper D, Coughlan J, Mullen MR. Structural equation modelling: guidelines for determining model fit. J Bus Res. 2008;6:53–60.
35. Claramita M, Tuah R, Riskione P, et al. Comparison of communication skills between trained and untrained students using a culturally sensitive nurse-client communication guideline in Indonesia. Nurse Educ Today. 2016;36:236–241.
36. Wong HJ, Bierbrier R, Ma P, et al. An analysis of messages sent between nurses and physicians in deteriorating internal medicine patients to help identify issues in failures to rescue. Int J Med Inform. 2017;100:9–15.
37. Hernández-Padilla JM, Granero-Molina J, Márquez-Hernández, et al. Development and psychometric evaluation of the arterial puncture self-efficacy scale. Nurse Educ Today. 2016;40:45–51.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.