")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Validation of the Arabic Version of the European Community Respiratory Health Survey Screening Questionnaire
Authors AlShareef SM
Received 31 May 2023
Accepted for publication 12 July 2023
Published 20 July 2023 Volume 2023:16 Pages 735—742
DOI https://doi.org/10.2147/JAA.S421175
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Saad Mohammed AlShareef
Department of Medicine, College of Medicine, Imam Mohammad Ibn Saud Islamic University (IMSIU), Riyadh, 13317-4233, Saudi Arabia
Correspondence: Saad Mohammed AlShareef, Email [email protected]
Purpose: The European Community Respiratory Health Survey (ECRHS) questionnaire has been widely used in epidemiological studies to quantify respiratory symptoms and screen for asthma, but there is no formally validated Arabic version. This study developed an Arabic ECRHS screening questionnaire, comprehensively evaluated its reliability and validity, and used it to estimate the population prevalence of respiratory symptoms and asthma in Saudi Arabia.
Methods: The ECRHS screening questionnaire was adapted to Arabic through translation and back-translation by bilinguals with consultation to a professional committee and lay panel. Reliability and validity were evaluated in a prospective, cross-sectional convenience sample of adults (> 18 years) between January and July 2022 in Riyadh, Saudi Arabia. A subgroup completed the questionnaire again three weeks later to assess test–retest reliability. All respiratory symptom-positive participants were invited for spirometry to diagnose asthma according to GINA criteria. Internal consistency was assessed using Cronbach’s α coefficient, test–retest reliability with Cohen κ coefficients, and reliability by calculating the sensitivity and specificity for diagnosing asthma.
Results: Of 2500 invited individuals, 1881 participated (75.2%). A total of 668 (35.5%) participants reported respiratory symptoms according to the ECRHS questionnaire, and 157/1881 (8.3%) had a current diagnosis of asthma on ECRHS questions. Cronbach’s α coefficient for internal consistency was 0.831, “good” internal consistency. The test–retest reliability (n = 303) was “excellent” for all questions (Cohen’s κ≥ 0.75). A total of 543 (81.3%) screening-positive participants underwent spirometry, of whom 278 (52%) were diagnosed with asthma according to GINA guidelines, an overall estimated prevalence of 14.8%. Most questions showed good-to-fair specificity and variable sensitivity for physician-diagnosed asthma.
Conclusion: This Arabic version of the ECRHS screening questionnaire is conceptually similar to the English version, comprehensible, and reliable. Many asthma cases remain hidden and undiagnosed. In addition to utility in epidemiological studies, the ECRHS screening questionnaire might be a simple, quick, and useful tool for asthma case finding.
Keywords: Arabic, asthma, European Community Respiratory Health Survey, reliability, validity
Introduction
Asthma is common, affecting between 0.2% and 21.0% adults worldwide,1 but its true population prevalence is probably underestimated.2 Anywhere between 20% and 73% of adult asthma cases remain undiagnosed,3 denying these individuals appropriate pharmacological and non-pharmacological management that could improve their quality of life and avoid adverse clinical outcomes.4,5 Historically, the diagnosis of asthma relied on symptoms, but the Global Initiative for Asthma (GINA) more recently recommended that asthma diagnosis should not be based on symptoms alone, instead requiring evidence of airflow limitation by spirometry,6 reflecting the clinical and physiological variability of the disease. Nevertheless, patients still frequently underreport their symptoms and spirometry is not globally available and is not recommended as a screening test,7 mandating a case-finding approach rather than population screening for asthma. Earlier detection of symptomatic asthma through case-finding with subsequent disease management could improve symptoms and ultimately health outcomes. Furthermore, gathering epidemiological data on asthma prevalence in different parts of the world and over time is important for health and policy planning. One way to detect cases and gather epidemiological data is by using validated questionnaires.
While several validated questionnaires exist to measure asthma control,8,9 few tools are available to detect and diagnose the disease.10 However, one widely used questionnaire for estimating asthma prevalence is the European Community Respiratory Health Survey (ECRHS) questionnaire, which was developed for the seminal epidemiological study of the same name.11 The ECRHS was the first study to investigate asthma prevalence in adults using standardized protocols, and, together with follow-on studies, the ECRHS has now provided important insights into the geographical variability in prevalence, risk factors, and treatment of adult asthma.11,12 The ECRHS questionnaire is a well validated and accepted epidemiological instrument for the population-based detection of asthma,13,14 but its reliability and validity depend on being comprehensible in the target population language. While the ECRHS has been validated in Korean,15 Brazilian-Portuguese,16 and Japanese17 and has been used in Arabic to estimate the prevalence of asthma in the United Arab Emirates18 and in Saudi Arabia,19 the questionnaire has yet to be formally validated for use in Arabic-speaking countries.
This prompted the development of the Arabic version of the ECRHS screening questionnaire. In doing so, this study comprehensively evaluates its reliability and validity and uses it to estimate the population prevalence of respiratory symptoms and asthma in Saudi Arabia to facilitate the detection and study of asthma in the general populations of Arab-speaking countries.
Methods
Translation Process
The ECRHS questionnaire is a self-administered questionnaire originally developed in English for the European Community Respiratory Health Survey (ECRHS), which surveyed individuals between 20 and 44 years to understand the worldwide distribution of asthma in young adults.11 This study used the same screening questionnaire developed and used for the original ECRHS (Table 1).11
 |
Table 1 Symptom Prevalence According to the ECRHS Screening Questionnaire |
The translation process followed the methodology used by Tsang et al20 and Ferrer et al21 for adapting health questionnaires. Briefly, this approach uses translation and back-translation by bilinguals with consultation to a professional committee and to a lay panel (Figure 1).20,21 In this study, the first translation into Arabic was carried out by two independent bilingual professional translators with Arabic as their mother tongue to better reflect the nuances of the target language. They were asked to keep conceptual equivalence rather than linguistic uniformity. Discrepancies between the two translators were discussed and resolved between the original translators. Then, the first version of the Arabic translation was back-translated into English by two other bilingual independent professional translators. The committee of professionals included two specialist physicians, a methodologist, and both the forward and backward translators, who reviewed all versions of the translations and determined whether the translated and original versions achieved semantic, idiomatic, experiential, and conceptual equivalence. Any discrepancies were resolved, and members of the expert committee reached a consensus on all items used for a prefinal version of the translate questionnaire. Since the adaptation of the ECRH aimed to reflect the concerns and the usual language of adults in the general population for asthma screening rather than those of the professionals, 100 volunteers were asked to respond to each questionnaire item and report any difficulty in interpreting or answering the questions. Finally, making any changes through piloting, we determined that the Arabic translation process was valid. The Arabic version of the questionnaire is provided in the Supplementary.
 |
Figure 1 Phases of adaptation of the European Community Respiratory Health Survey in Arabic. |
Study Design, Participants, and Ethical Approval
This study is reported according to the STROBE statement for cross-sectional studies (see Supplementary Checklist).22 This was a prospective, cross-sectional, longitudinal study of adults in the general population (aged >18 years). Other inclusion criteria were agreement to participate and mentally competent to complete a questionnaire.
Recruitment was carried out between January and July 2022 in Riyadh, Saudi Arabia. Participants were convenience sampled from shopping malls, public gardens, university campuses, and in the streets in Riyadh, Saudi Arabia. The sample size was calculated based on a target population of 2 million and an estimated asthma prevalence of 10% with 95% confidence intervals. This study used a cluster-based sample, and the sample size was powered by a design effect of 2 to allow for cluster sampling (n = 1728). The sample size was further increased to account for a 20% non-response rate. Although the samples were convenient, they were randomly selected and were within the age and gender of the study population. Fifteen medical students trained in the study objectives and the ECRHS questionnaire conducted the interviews.
Four hundred respiratory symptom-positive participants were invited to complete the questionnaire three weeks later to assess the test–retest reliability, and all respiratory symptom-positive participants were invited for spirometry to follow-up their symptoms.
The Institutional Review Board of Imam Mohammad Ibn Saud Islamic University approved the study protocol. All participants were fully informed of the study protocol and provided written, signed statements of informed consent.
Reliability and Validity Assessment and Statistical Analysis
Internal consistency was assessed in the entire study population using Cronbach’s α coefficient. To assess test–retest reliability, four hundred participants were invited to complete the questionnaire again after three weeks. Test–retest reliability was determined by Cohen κ coefficients. Cronbach’s α coefficients are considered good if ≥0.70 (excellent if ≥0.90), and Cohen κ coefficients as excellent if ≥0.75.15,16
All respiratory symptom-positive participants were invited for spirometry to follow-up their symptoms, thereby also providing an opportunity to assess the validity of the Arabic version ECRHS questionnaire for diagnosing asthma as assessed by a physician based on clinical symptoms and spirometry values. Portable spirometry was performed within three months of completing the questionnaire at Imam Mohammad Ibn Saud University HealthCare Center. Physician-diagnosed asthma was defined as the proportion of observed over predicted FEV1, FVC, and FEV1/FVC according to the norms published by the Global Lung Function Initiative (GLI)23 and GINA 2022 guidelines:6 (i) documented expiratory airflow limitation: FEV1 reduced and FEV/FVC confirmed reduced compared to the lower limit of normal and (ii) documented excessive variability in lung function using post-bronchodilator responsiveness (reversibility) testing: increase in FEV1 of >12% and >200 mL 10 minutes after 400 µg albuterol (Ventolin). In asymptomatic patients already taking controller treatment, we considered spirometry after withholding bronchodilators (4 hours for SABA, 24 hours for twice-daily ICS-LABA, 36 hours for once daily ICS-LABA).
Sensitivity (true positives/(true positives + false negatives)) and specificity (true negatives/(true negatives + false positives)) were calculated. As a marker of diagnostic performance, the Youden index was calculated (sensitivity + specificity – 1). Fisher’s exact test was used to compare differences in gender between screening positive and negative individuals, and Student’s t-test was used to compare differences in age between screening positive and negative individuals. IBM Statistics v29 (IBM Statistics, Armonk NY) was used for statistical analyses, and a p-value <0.05 was considered statistically significant.
Results
Population Prevalence of Asthma Based on the ECRHS
Of 2500 invited individuals, 1881 agreed to take part, a response rate of 75.2%. The average age of the 1881 participants was 29.7 ± 7.7 years, and 44.3% were female. The prevalence of individual respiratory symptoms according to each ECRHS question was between 5.7% and 25.8%. Overall, 668 (35.5%) of participants screened positive (at least one question positive) for asthma and reported respiratory symptoms according to the ECRHS screening questionnaire.
157/1881 (8.3%) individuals answered “yes” to questions 5 and 6 relating to asthma attacks and current asthma medications so were regarded as having a current diagnosis of asthma. While individuals screening positive were more frequently male (57.9%), there was no significant difference in gender between screening-positive and screening-negative groups (Fisher’s exact test p = 0.15). Similarly, there were no significant differences between screening-positive and screening-negative groups with respect to age (Student’s t-test p = 0.15).
Reliability of the Arabic Version of the ECRHS Screening Questionnaire
Across the entire study population (n = 1881), Cronbach’s α coefficient for internal consistency was 0.831, denoting “good” internal consistency.
Four hundred individuals were invited to repeat the questionnaire three weeks later, and 303 agreed to do so (75.8%). Test–retest reliability was assessed in these 303 individuals positive for respiratory symptoms after a three-week interval assessed by Cohen’s κ ranged between 0.844 and 0.982 (Table 2). All questions showed “excellent” test–retest reliability (Cohen’s κ ≥ 0.75).
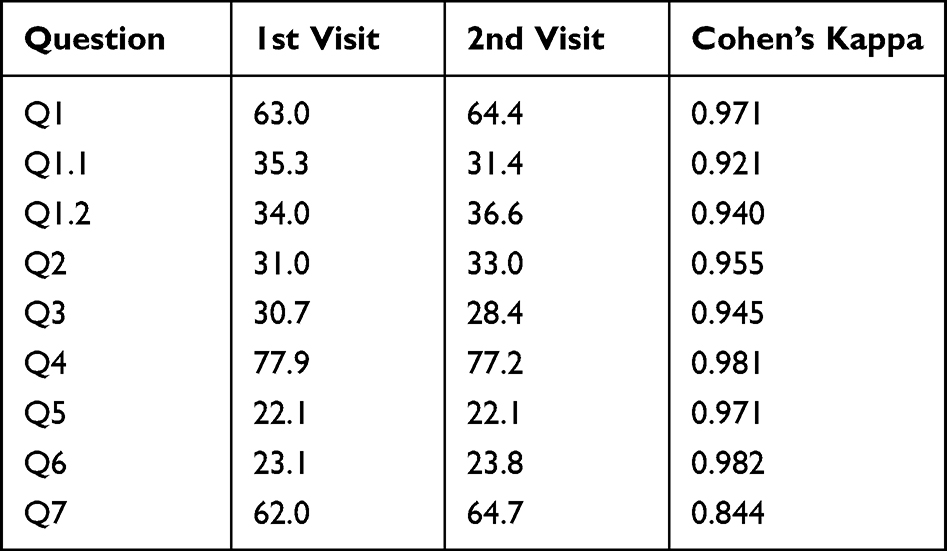 |
Table 2 Test–Retest Reliability of the Arabic Version of the ECRHS Screening Questionnaire (n = 303) |
Validity of the Arabic Version of the ECRHS Screening Questionnaire and Prevalence of Physician-Diagnosed Asthma
Of the 668 individuals screening positive with the ECRHS, 543 (81.3%) underwent spirometry (Table 3). Of these individuals undergoing spirometry, 278 (52%) were diagnosed with asthma according to GINA 2022 guidelines,6 giving an overall estimated prevalence of physician-diagnosed asthma in the study population of 14.8%. With respect to the validity of the questionnaire, in this population, and as expected, questions 5 and 6 (“Have you had an attack of asthma in the last 12 months?” and “Are you currently taking any medicine (including inhalers, aerosols or tablets) for asthma?”) were highly specific for a diagnosis of asthma (specificity 0.91–1.00). All other questions showed good-to-fair specificity for physician-diagnosed asthma (specificity 0.61–0.9), except for question 4 (“Have you been woken by an attack of coughing at any time in the last 12 months?”; specificity 0.242) and question 7 (“Do you have any nasal allergies including hay fever?”; specificity 0.366), which were poorly specific for physician-diagnosed asthma. According to the Youden index, only question 1 (“Have you had wheezing or whistling in your chest at any time?”) acceptably balanced sensitivity and specificity for accurately diagnosing asthma clinically (Youden index 0.584).
 |
Table 3 Validity of the Arabic Version of the ECRHS Screening Questionnaire |
Discussion
This study developed and formally validated an Arabic version of the ECRHS screening questionnaire. The data suggest that the translated version is conceptually similar to the English version, comprehensible, and reliable. Validating the new Arabic version of the questionnaire in a large cohort of individuals screening positive, the study confirms the generally very high specificity of the questionnaire for detecting physician-diagnosed asthma, ie, the questions in the questionnaire are very good at identifying individuals without the disease. We also provide the first population-level data on the prevalence of adult asthma in Saudi Arabia validated according to GINA guidelines, uncovering that over a third of randomly selected individuals in the general Saudi population have respiratory symptoms and that about half of these individuals meet the latest criteria for a diagnosis of asthma, giving an overall estimated prevalence of physician-diagnosed asthma in the study population of 14.8%.
The percentage prevalence of individual respiratory symptoms in our cohort almost perfectly mirrored the median proportions and distribution pattern reported in the original ECRHS data from 48 different centers in 22 countries (Europe, Scandinavia, Australia, and the US):11 wheeze 18.9 vs 20.7%, wheeze with breathlessness 9.3 vs 7.7%, wheeze without a cold 10.9 vs 9.3%, waking with chest tightness 10.1 vs 9.7%, waking with breathlessness 8.9 vs 4.7%, waking with cough 23.9 vs 25.6%, asthma attack 5.7 vs 2.6%, current asthma medication 6.8 vs 2.4%, and nasal allergies and hay fever 25.8 vs 16.6%. The data also reflect the findings of a previous study applying the ECRHS questionnaire to a similar population in Saudi Arabia,19 which similarly reported a high prevalence of wheeze (21.7%) and particularly waking with coughing (43.0%). One of the main results of the ECRHS was the wide geographic variation in respiratory symptoms, asthma, allergic rhinitis, atopic sensitization, and bronchial responsiveness. The current data suggest that Saudi Arabia is representative of the distribution of respiratory symptoms globally, with wheeze, nighttime cough, and rhinitis and hay fever relatively common. However, there was an overall relatively high burden of asthma in the general Saudi population: the prevalence of current asthma in the sample according to the ECRHS questionnaire was 8.3%, comparable to the prevalences observed in some parts of the UK, Australia, and New Zealand in the ECRHS.11 Although there are little other directly comparable data from the Middle East, our prevalence is lower than a previous study from the United Arab Emirates, which reported that 12.1% of 1220 participants fulfilled ECRHS criteria for asthma,18 and another study from Saudi Arabia reporting an 11.3% prevalence of self-reported physician-diagnosed asthma (at any time).19 Overall, the detected prevalence of asthma in Saudi Arabia seems to be consistent with that reported in Europe and North America as well as other large-scale cross-sectional epidemiological analyses in the region (SNAPSHOT), which reported an asthma prevalence of 7.3% in the Gulf cluster countries.24
Perhaps more importantly, after formal testing, the overall physician-diagnosed asthma prevalence was 14.8% of the study population. Even taking into account that about one-fourth of questionnaire-positive participants did not attend for spirometry, meaning that 14.8% might be an over- or underestimate, our data confirm that there is a high burden of undiagnosed asthma in the general population in Saudi Arabia, a situation that is likely to be found elsewhere. Given the high specificity of the ECRHS questionnaire (ie, ability to exclude patients without the disease), our results show empirically for the first time that the ECRHS questionnaire is not only useful for epidemiological purposes but as a simple, fast (it takes <5 minutes to complete), and practical tool for finding undiagnosed asthma cases in the general population.
A primary objective of this study was to develop an Arabic version of the ECRHS questionnaire that was equivalent to the widely used English version. The analysis shows that the new Arabic version is internally consistent and reproducible, consistent with the original13,14 and other versions translated into Korean,15 Brazilian-Portuguese,16 and Japanese.17 Similarly, its validity was equivalent to previous studies of both English25 and translated versions,15,17 with generally very high specificity and variable sensitivity. These properties – the ability to exclude negative cases (ie, people in the population who definitely do not have asthma) and enrich for positive cases again support the use of the ECRHS questionnaire for case finding in addition to its traditional use as an epidemiological tool for assessing respiratory symptoms and current asthma prevalence. This work now paves the way for future studies assessing the real-world value of applying the ECRHS questionnaire in the community setting to detect undiagnosed asthma.
This study is strengthened by its prospective design, the large number of participants recruited from the general population, and the large number of participants who subsequently agreed to repeat the questionnaire and who underwent clinical evaluation. To our best knowledge, this is also the first study using the ECRHS questionnaire to test validity (ie, that the questionnaire detects the population of interest, namely individuals with asthma) using contemporary, spirometry-led diagnostic criteria. However, the study also has limitations. The convenience sampling, although random, may have had unintended selection bias. Similarly, the response rate of 75% may have led to significant selection bias and there may also have been selection bias in the group who decided to attend for follow-up spirometry. As noted above, the estimated prevalence of asthma in the entire cohort might be an over- or under-estimate for the same reason. The ECRHS questionnaire is self-reporting and asks respondents to recall symptoms occurring over the previous 12 months, which might introduce recall and response bias. Although this study did not directly test comprehension of questionnaire, instead inferring cultural appropriateness and understandability from statistical equivalence with other published data, taken together the internal equivalence, reliability, and robust, clinically correlated validity data suggest that the Arabic version of the questionnaire is fit for purpose. Finally, the sample was taken from one city in Saudi Arabia and therefore may not be representative of the population as a whole, especially those in rural areas.
In conclusion, this study developed an Arabic version of the ECRHS screening questionnaire that is conceptually similar to the English version, comprehensible, and reliable. By applying this new questionnaire to a large study population and by following up screening-positive individuals with spirometry, this study provides new and accurate insights into the overall burden of asthma in the general population, including a significant proportion of hidden and undiagnosed cases. The performance metrics of the questionnaire generated through application of current clinical diagnostic criteria also suggest that, in addition to being useful in epidemiological studies, the ECRHS screening questionnaire might be a simple, quick, and useful tool for active case finding in the general population to ensure that every asthmatic patient receives optimal care.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The ethical approval of this study was granted from Imam Mohammad Ibn Saud Islamic University, (HAPO-01-R-011). The consent was obtained from each participant.
Acknowledgments
The author extends his appreciation to the Deanship of Scientific Research, Imam Mohammad Ibn Saud Islamic University (IMSIU), Saudi Arabia, for funding this research work through Grant No. (221413002).
Author Contributions
Saad Mohammed AlShareef made significant contributions to the work reported and was involved in the conception, study design, execution, acquisition of data, and analysis and interpretation; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; he agreed on the journal to which the article has been submitted and agreed to be accountable for all aspects of the work.
Funding
This study was funded by Imam Mohammad Ibn Saud Islamic University (IMSIU) with grant No. (221413002).
Disclosure
The author declares that they have no competing interests.
References
1. To T, Stanojevic S, Moores G, et al. Global asthma prevalence in adults: findings from the cross-sectional world health survey. BMC Public Health. 2012;12(1):204. doi:10.1186/1471-2458-12-204
2. Lamprecht B, Soriano JB, Studnicka M, et al. Determinants of underdiagnosis of COPD in national and international surveys. Chest. 2015;148(4):971–985. doi:10.1378/chest.14-2535
3. Aaron SD, Boulet LP, Reddel HK, Gershon AS. Underdiagnosis and overdiagnosis of asthma. Am J Respir Crit Care Med. 2018;198(8):1012–1020. doi:10.1164/rccm.201804-0682CI
4. AlShareef S. Allergic bronchopulmonary aspergillosis: a systematic review of its management with a call to action in Saudi Arabia. J Nat Sci Med. 2020;3(2):91.
5. AlShareef S, McDonald CF, Lee J. Clinical and lung function outcomes after anti-IgE or anti-IL5 therapy in severe asthma. J Asthma Allergy. 2022;15:209–217. doi:10.2147/JAA.S348137
6. Reddel HK, Bacharier LB, Bateman ED, et al. Global initiative for asthma strategy 2021: executive summary and rationale for key changes. Am J Respir Crit Care Med. 2022;205(1):17–35. doi:10.1164/rccm.202109-2205PP
7. Force USPST, Mangione CM, Barry MJ, et al. Screening for chronic obstructive pulmonary disease: US preventive services task force reaffirmation recommendation statement. JAMA. 2022;327(18):1806–1811. doi:10.1001/jama.2022.5692
8. Juniper EF, Svensson K, Mork AC, Stahl E. Measurement properties and interpretation of three shortened versions of the asthma control questionnaire. Respir Med. 2005;99(5):553–558. doi:10.1016/j.rmed.2004.10.008
9. Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113(1):59–65. doi:10.1016/j.jaci.2003.09.008
10. Shin B, Cole SL, Park SJ, Ledford DK, Lockey RF. A new symptom-based questionnaire for predicting the presence of asthma. J Investig Allergol Clin Immunol. 2010;20(1):27–34.
11. Chinn S, Luczynska C, Jarvis D, et al. Variations in the prevalence of respiratory symptoms, self-reported asthma attacks, and use of asthma medication in the European Community Respiratory Health Survey (ECRHS). Eur Respir J. 1996;9(4):687–695. doi:10.1183/09031936.96.09040687
12. Janson C, Anto J, Burney P, et al. The European community respiratory health survey: what are the main results so far? European community respiratory health survey II. Eur Respir J. 2001;18(3):598–611. doi:10.1183/09031936.01.00205801
13. Burney PG, Laitinen LA, Perdrizet S, et al. Validity and repeatability of the IUATLD (1984) Bronchial Symptoms Questionnaire: an international comparison. Eur Respir J. 1989;2(10):940–945. doi:10.1183/09031936.93.02090940
14. Sunyer J, Basagana X, Burney P, Anto JM. International assessment of the internal consistency of respiratory symptoms. European Community Respiratory Health Study (ECRHS). Am J Respir Crit Care Med. 2000;162(3 Pt 1):930–935. doi:10.1164/ajrccm.162.3.9911062
15. Song WJ, Lee SH, Kang MG, et al. Validation of the Korean version of the European community respiratory health survey screening questionnaire for use in epidemiologic studies for adult asthma. Asia Pac Allergy. 2015;5(1):25–31. doi:10.5415/apallergy.2015.5.1.25
16. Ribeiro M, Angelini L, Robles-Ribeiro PG, Stelmach R, Santos Ude P, Terra-Filho M. Validation of the Brazilian-Portuguese version of the European community respiratory health survey in asthma patients. J Asthma. 2007;44(5):371–375. doi:10.1080/02770900701364015
17. Watanabe J, Taniguchi M, Takahashi K, et al. 成人喘息-調査用紙日本語版の作成と検証 セイジン ゼンソク [Validation of ECRHS questionnaire in Japanese to use for nation-wide prevalence study of adult asthma]. Arerugi. 2006;55(11):1421–1428. Japan.
18. Mahboub BH, Al-Hammadi S, Rafique M, et al. Population prevalence of asthma and its determinants based on European community respiratory health survey in the United Arab Emirates. BMC Pulm Med. 2012;12:4. doi:10.1186/1471-2466-12-4
19. Al Ghobain MO, Algazlan SS, Oreibi TM. Asthma prevalence among adults in Saudi Arabia. Saudi Med J. 2018;39(2):179–184. doi:10.15537/smj.2018.2.20974
20. Tsang S, Royse CF, Terkawi AS. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J Anaesth. 2017;11(Suppl 1):S80–S89. doi:10.4103/sja.SJA_203_17
21. Ferrer M, Alonso J, Prieto L, et al. Validity and reliability of the St George’s respiratory questionnaire after adaptation to a different language and culture: the Spanish example. Eur Respir J. 1996;9(6):1160–1166. doi:10.1183/09031936.96.09061160
22. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
23. Cooper BG, Stocks J, Hall GL, et al. The Global Lung Function Initiative (GLI) network: bringing the world’s respiratory reference values together. Breathe. 2017;13(3):e56–e64. doi:10.1183/20734735.012717
24. Tarraf H, Aydin O, Mungan D, et al. Prevalence of asthma among the adult general population of five Middle Eastern countries: results of the SNAPSHOT program. BMC Pulm Med. 2018;18(1):68. doi:10.1186/s12890-018-0621-9
25. Galobardes B, Sunyer J, Anto JM, Castellsague J, Soriano JB, Tobias A. Effect of the method of administration, mail or telephone, on the validity and reliability of a respiratory health questionnaire. The Spanish Centers of the European Asthma Study. J Clin Epidemiol. 1998;51(10):875–881. doi:10.1016/s0895-4356(98)00063-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.