Back to Journals » Clinical Epidemiology » Volume 14
Validation of Postsurgical Venous Thromboembolism Diagnoses of Patients Undergoing Lower Limb Orthopedic Surgery in the Danish National Patient Registry
Authors Galsklint J, Kold S, Kristensen SR, Severinsen MT ![]() , Gade IL
, Gade IL ![]()
Received 11 November 2021
Accepted for publication 13 January 2022
Published 17 February 2022 Volume 2022:14 Pages 191—199
DOI https://doi.org/10.2147/CLEP.S345293
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor H Sorensen
Josephine Galsklint,1 Søren Kold,2,3 Søren Risom Kristensen,1,2 Marianne Tang Severinsen,2,4 Inger Lise Gade2,4,5
1Department of Clinical Biochemistry, Aalborg University Hospital, Aalborg, Denmark; 2Department of Clinical Medicine, Aalborg University, Aalborg, Denmark; 3Department of Orthopedic Surgery, Aalborg University Hospital, Aalborg, Denmark; 4Department of Hematology and Clinical Cancer Research, Aalborg University Hospital, Aalborg, Denmark; 5Department of Hematology, Aarhus University Hospital, Aarhus, Denmark
Correspondence: Marianne Tang Severinsen, Department of Hematology, University Hospital, Aalborg, Denmark, Email [email protected]
Background: Healthcare databases can be a valuable source of epidemiological research regarding postoperative venous thromboembolism (VTE), ie, deep vein thrombosis (DVT) and pulmonary embolism (PE), following orthopedic procedures, but only if the diagnoses are valid. We examined the validity of VTE diagnosis codes in the Danish National Patient Registry (DNPR) by calculating their positive predictive value (PPV) and negative predictive value (NPV) versus actual medical records.
Methods: We identified patients who had undergone lower limb surgery during the period 2009– 2019 at a hospital in the North Denmark Region. Of these, 420 patients had at least one VTE diagnosis registered in the DNPR within 180 days after lower limb surgery. Each patient with a VTE diagnosis was matched with two patients on age and sex, as well as type, location and period of surgery. The entire medical record and diagnostic imaging were reviewed to confirm VTE diagnosis.
Results: The overall PPVs was 85.2% (95% CI: 81.5– 88.5%) for first time VTE diagnosis following lower limb surgery, 82.6% (95% CI: 77.5– 82.8%) for DVT, and 90.3% (95% CI: 84.3– 94.6%) for PE. We found improvement in PPV during the study period when stratifying for three periods of the whole period. There were no significant differences when stratifying for sex, age, or surgery site. All negative predictive values were higher than 99%. A total of 113 additional VTE diagnoses were registered among 88 VTE patients during follow-up. Only four of the suspected recurrent VTEs were confirmed to be true recurrent VTEs.
Conclusion: The VTE diagnosis codes in the DNPR after lower limb orthopedic surgery were highly valid against the actual medical records, and we observed better PPV over recent years.
Keywords: epidemiology, venous thromboembolism, orthopedic procedures, positive predictive value, PPV, negative predictive value, NPV, validity
Introduction
Venous thromboembolism (VTE) comprising deep vein thrombosis (DVT) and pulmonary embolism (PE) is a known complication of orthopedic procedures that are commonly performed in healthcare services. As the population ages, more patients will undergo major orthopedic procedures of the lower limbs associated with risk of postsurgical VTE.1,2 Medical anticoagulant prophylaxis has been adopted for selected high-risk patients/surgical procedures to reduce the risk of VTE after orthopedic procedures.3–5 However, a recent study using Danish nationwide register data from 1 million orthopedic surgical procedures of the lower limb showed higher rates of VTE compared with matched controls.6
Administrative healthcare data are useful sources for examining associations between exposures and incident outcomes occurring at a relatively low frequency. The Danish healthcare system has a long history of collecting electronic data at an individual patient level with essentially no loss to follow up, and is therefore a valuable resource for epidemiological research.7 However, the quality of registry data varies considerably from disease to disease and poor data quality may invalidate epidemiological research outcomes.8 Previous studies have evaluated the quality of VTE discharge diagnoses in different contexts. The positive predictive values (PPV, defining the proportion of true positives among those with a positive diagnosis) of a VTE discharge diagnosis have ranged from 74.8% to 84% in various validation studies based on chart reviews.9–14 The validity of a VTE diagnosis registered in the Danish National Patient Registry (DNPR) may depend on the specific population observed. The validity of VTE discharge diagnoses in the DNPR after lower limb orthopedic surgery is currently unknown, and we therefore aim to validate VTEs registered in the DNPR within 180 days after orthopedic surgery in the lower limbs against the actual medical records.
Methods
Data Setting/Source
The Danish healthcare system is fully provided by taxes, making it accessible to all Danish citizens, regardless of socioeconomic status, providing equal access to general practitioners and hospitals.15 All Danish residents are provided a unique civil personal registration (CPR) number at birth or immigration and registered in the Danish Civil Registration System. Vital, immigration, and emigration status have been registered for every individual CPR number since 1968.7,16 The DNPR contains information about hospital admissions since 1978 with dates of admission and discharge and discharge diagnosis with one primary and up to 22 secondary diagnoses. Diagnoses have been coded in the DNPR with the Danish version of the International Classification of Diseases (ICD) Revision 8th, which was replaced by the 10th revision in 1994. Surgical procedures and therapies are registered in the DNPR using the Nordic Medico-Statistical Committee (NOMESCO) classification from 1996.15–17
This study including reviews of medical records was approved by the North Denmark Region (ID: 2020-093) in accordance with the General Data Protection Regulation. Medical record review was furthermore approved. Since there was no contact with patients or any interventions performed, permission from the Danish Scientific Ethics committee was not required by Danish law. Study data will not be shared due to Danish data protection legislation.
Study Population
The study source population consists of adult patients (≥18 years of age) from the North Denmark Region having a first-time orthopedic surgery on the lower limb performed between January 1, 2009, and December 29, 2019 identified using the following NOMESCO codes: KNEx (pelvis), KNFx (hip/femur), KNGx (knee/crus), KNHx (foot/ankle). Participants registered with a VTE discharge diagnosis within 180 days after the surgery procedures were identified as VTE cases. ICD-10 VTE diagnoses were identified in the DNPR by the following codes: I26, I80.1-I80.9, T817c, and T817D. Each VTE case was matched with two comparators from the study population without VTE using incidence-density sampling. Comparators were randomly sampled from the study source population matched on age, sex, surgery period, surgery site, and type of surgery. Comparators with VTE before the date of surgery were excluded.
The entire medical record of all the VTE cases and their comparators were manually reviewed for a follow-up period which comprised the 180 days after the surgery. Follow-up started at the date of surgery (index date) and ended with either death of the patient, emigration from the North Denmark Region, or 180 days after the index date, whichever came first. Subjects who emigrated before the end of follow-up or moved to another region of Denmark were excluded from the study.
Extract of Medical Records Information/Medical Record Review
Information from the medical records was systematically extracted using a predefined algorithm. The data were stored using Research Electronic Data Capture (REDCap) hosted at Aalborg University Hospital.18
We extracted all relevant information on possible first-time and recurrent VTE events during follow-up for both VTE cases and their comparators. This included symptoms of VTE, location of VTE, diagnostic test results and choice of treatment. Furthermore, for each participant, we registered VTE history. Previous VTE discharge diagnoses were confirmed by review of medical records or by earlier positive diagnostic scans. A VTE discharge diagnosis was confirmed if the treating physicians concluded that a VTE event was diagnosed based on symptoms and the results of relevant diagnostic scans. Relevant diagnostic scans were analyzed by trained physicians and comprise ultrasonography scans for DVTs and CT-pulmonary angiography or ventilation-perfusion lung scans for PEs.
Statistical Analysis
Data analyses were performed in STATA version 16.0 (StataCorp, Texas).19 Baseline characteristics were summarized using descriptive statistics (median and interquartile range for continuous variables and percentage for categorical variables). For each VTE diagnosis (VTE, DVT, or PE) we calculated the PPV and the negative predictive value (NPV), with 95% confidence intervals (95% CI) as i) the number of confirmed diagnoses after review of the medical records divided by the number of diagnoses registered in the DNPR (PPV), and ii) the number of patients without a VTE-diagnosis after review of the medical records divided by the number of patients without a VTE diagnosis registered in the DNPR (NPV). We calculated PPV and NPV for VTE overall, and DVT and PE using the diagt package in STATA.20 Furthermore, the PPV and NPV were estimated stratified by age group, sex, surgery (calendar) period, and anatomic site of the surgery.
Results
Figure 1 shows a flowchart regarding the selection and sampling process in this study. We identified 429 patients with a VTE discharge diagnosis within 180 days after surgery. These were matched with 782 comparators without registered VTE diagnosis. Nine of the 429 patients with a VTE diagnosis in the DNPR were excluded as they did not fulfill the inclusion criteria. Among the 782 comparators, 30 did not fulfill the inclusion criteria, leaving a total of 1172 patients for this study.
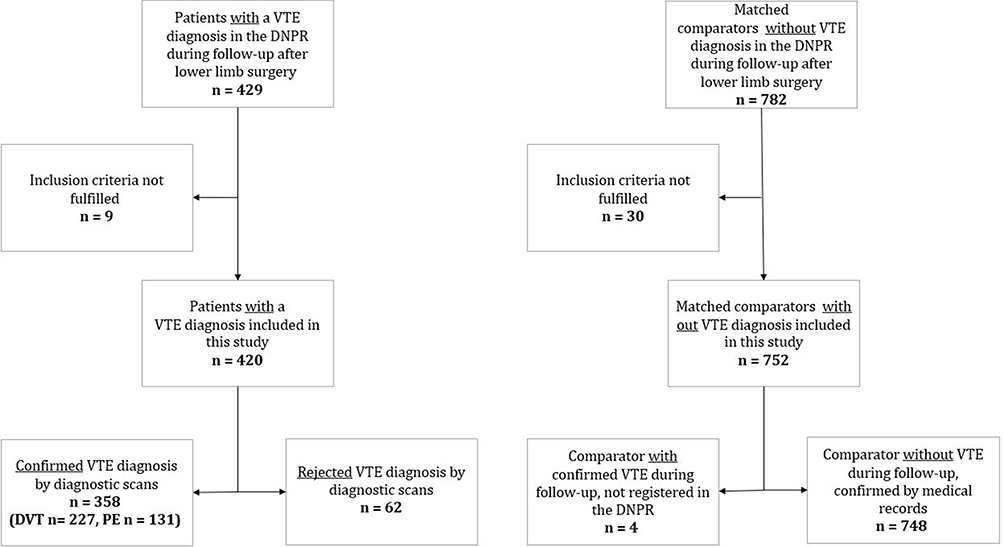 |
Figure 1 Flowchart displaying the selection of study population. |
Table 1, summarizes the descriptive statistics for the study population, including information on age, sex, prior VTE history, and location of surgery on limb. Among patients with at VTE discharge diagnosis, 48 (11.4%) had a history of previous confirmed VTE, whereas 24 (3.2%) patients in the comparator group had a previous confirmed VTE.
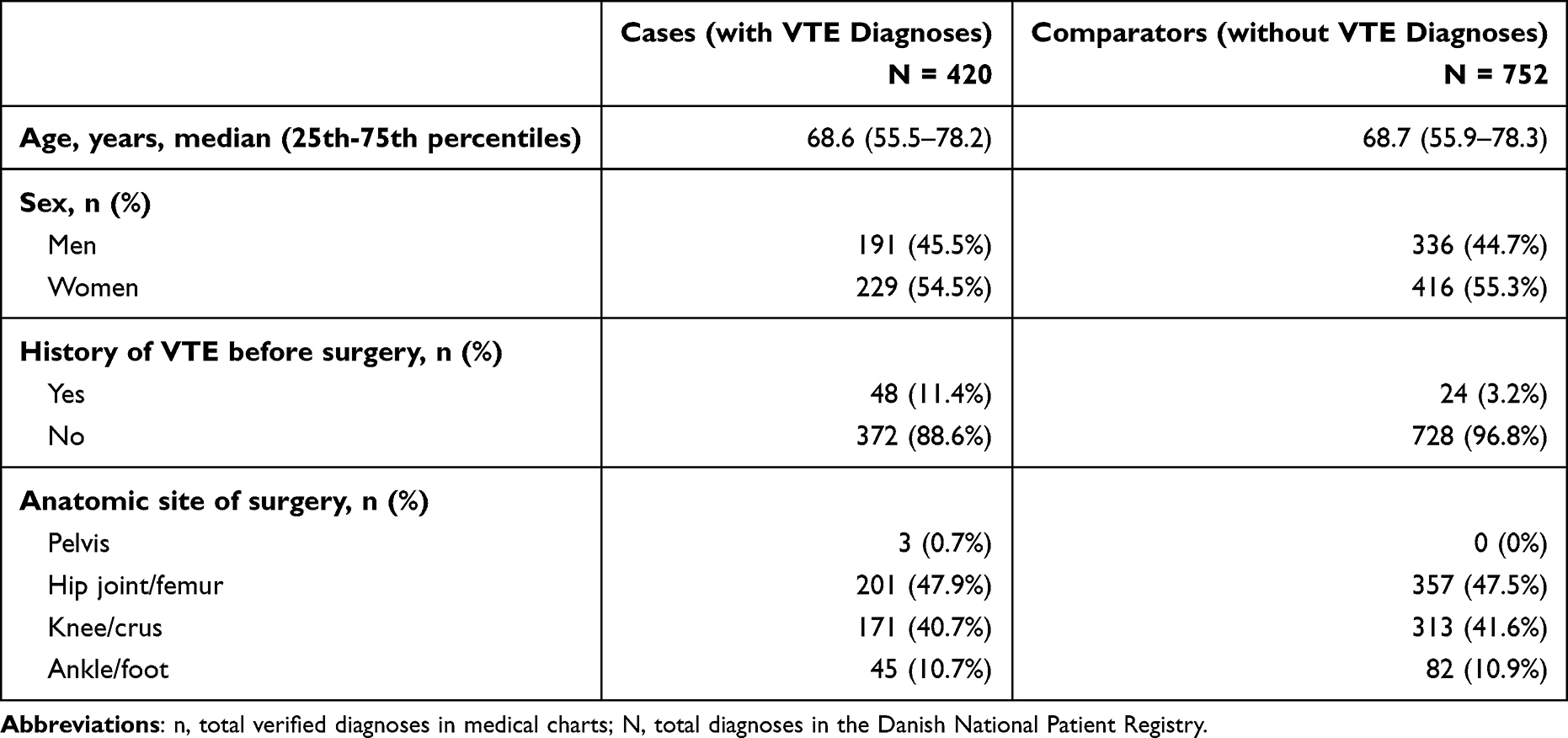 |
Table 1 Descriptive Statistics of Baseline Characteristics of Included Cases and Comparators Registered in the Danish National Patient Registry During 2009 to 2019 (n = 1172) |
Table 2 shows the PPVs and NPVs of VTE diagnoses in the DNPR in total and according to sex and surgery period. Overall, we confirmed 358 VTE diagnoses of the 420 patients with a VTE discharge diagnosis following lower limb surgery, giving a PPV of 85.2% (95% CI: 81.58–88.5%). Four of the 752 comparator patients had an unregistered VTE during the follow-up period resulting in NPV of 99.5% (95% CI: 98.6–99.9%). DVT was confirmed in 227 of 275 patients giving a PPV of 82.6% (95% CI: 77.5–86.8%). PE was confirmed in 131 of 145 patients (14 cases of PE diagnoses were excluded by diagnostic scans) resulting in PPV of 90.3% (95% CI: 84.3–94.6%). Since no comparators had any (unregistered) PE diagnosis, we found NPV for PE to be 100% (95% CI: 99.5–100%).
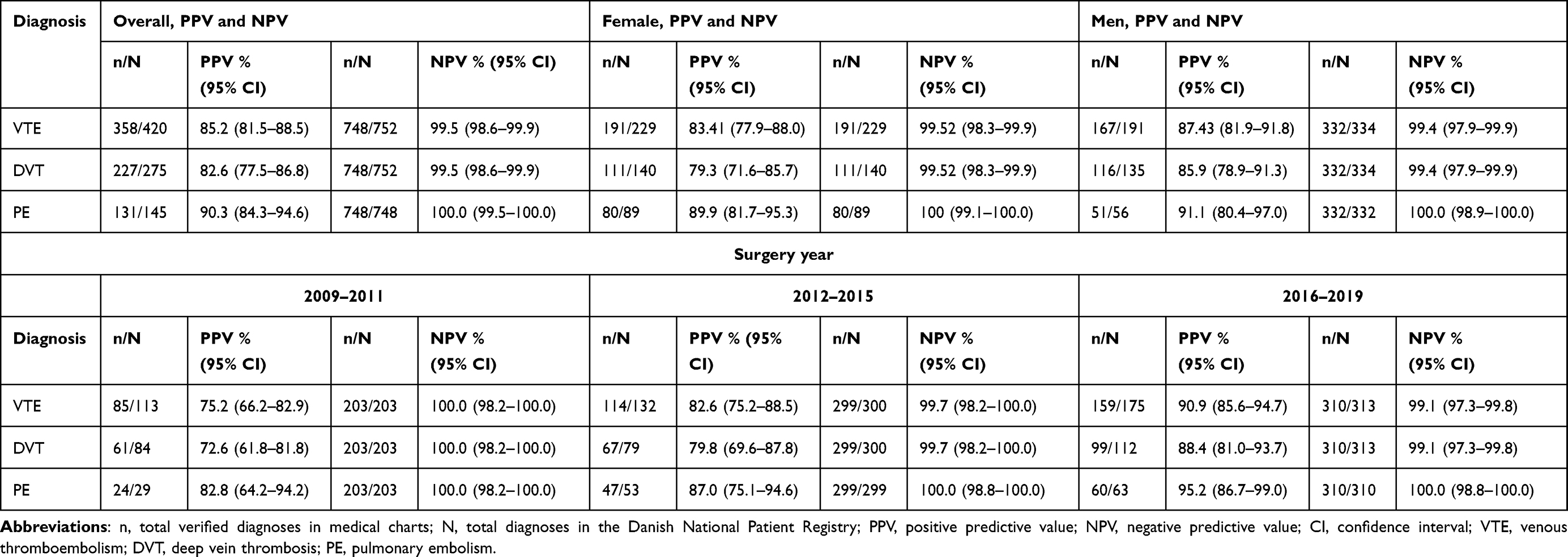 |
Table 2 Positive Predictive Value and Negative Predictive Value of Overall Diagnoses of Venous Thromboembolism Including Deep Venous Thrombosis and Pulmonary Embolism in the Danish National Patient Registry Stratified by Overall, Sex and Surgery Year |
When stratifying on surgery period we found an increase in overall VTE PPVs from 2009 to 2011 showing PPV of 75.2% (95% CI: 66.2–82.9%), 2012–2015 with PPV of 82.6% (95% CI: 75.2–88.5%), and lastly 2016–2019 having the highest PPV of 90.9% (95% CI: 85.6–94.7%). A similar trend was observed for the PPV values for both DVT, and PE stratified on surgery periods. The lowest PPV for any strata was for DVT registered in 2009–2011 (72.62% (95% CI: 61.8–81.8)). In general, all NPV values were higher than 99%, with the lowest associated to DVT surgery site for knee/crus which had an NPV of 99.0% (95% CI: 97.2–99.8%).
Table 3 shows the PPVs and NPVs stratified by age groups, and Table 4 shows the PPVs and NPVs stratified by location of surgery. When stratifying the analysis according to age group, sex, and anatomical site for surgery in the lower limb we saw a slight variation, but generally the PPVs and the NPVs were within the same range as for the overall analysis and with overlapping CIs.
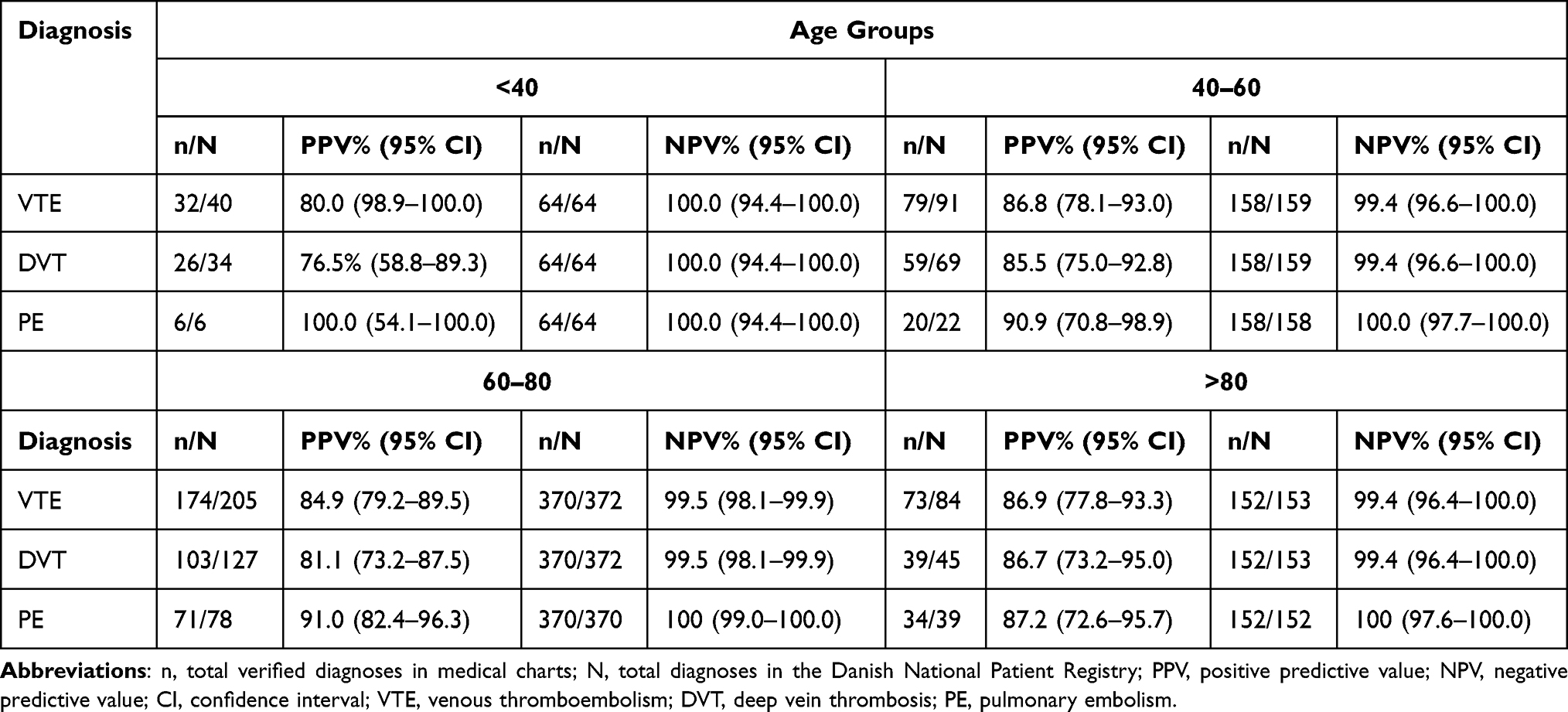 |
Table 3 Predictive Values Stratified by Participants Age Groups |
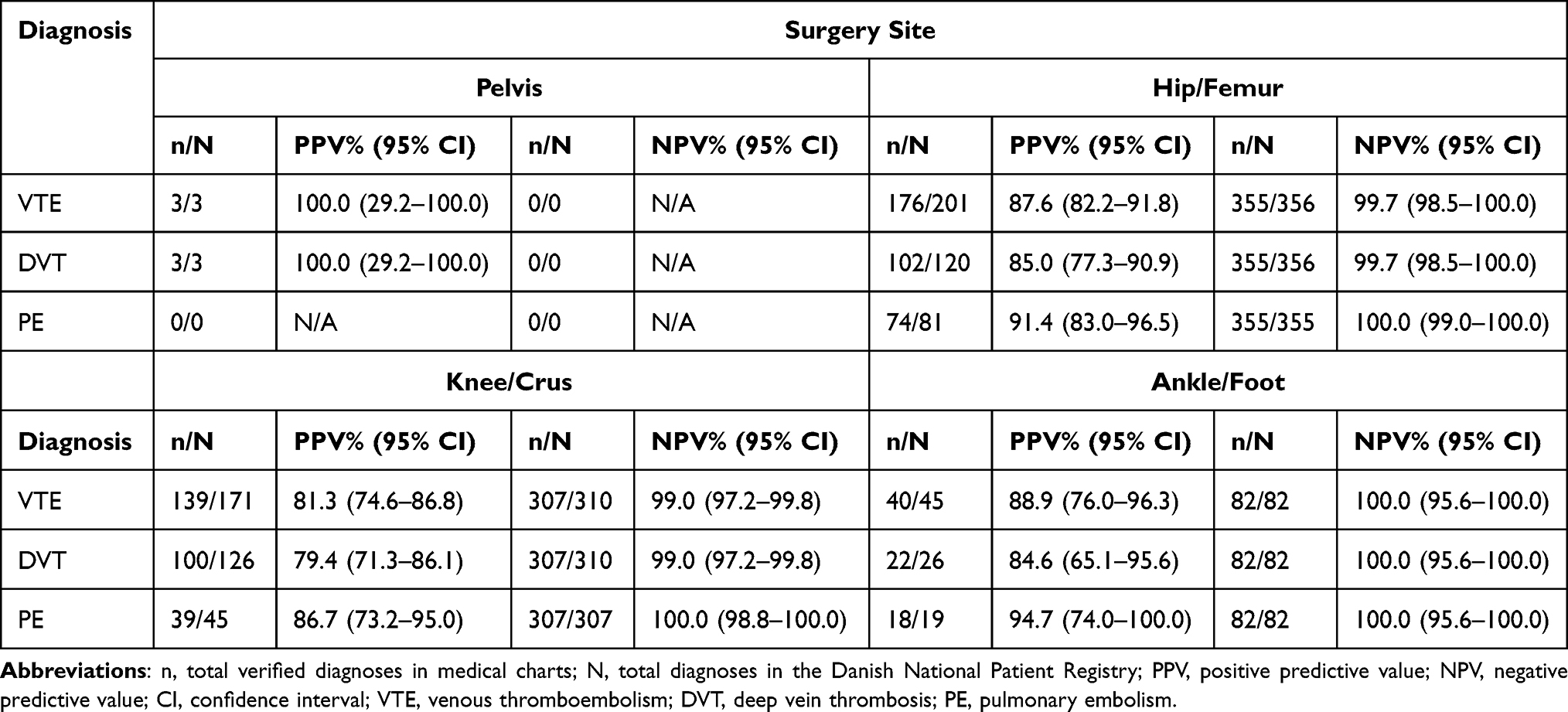 |
Table 4 Predictive Values Stratified by Location of Surgery on Limb |
We identified 88 patients with more than one VTE diagnosis registered in the DNPR during the follow-up of 180 post-surgical days, corresponding to a total of 113 additional VTE diagnoses. Only four of these suspected recurrent VTEs were confirmed to be recurrent VTEs, characterized by completed treatment of the first registered VTE, a renewed positive diagnostic scanning and initiation of treatment with anticoagulant therapy.
Discussion
Based on the review of 1172 participants' medical records, the PPV for VTE overall was 85.2%, 82.6% for DVT, and 90.3% for PE. We found an increase in PPV during the study period with at PPV for VTE discharge diagnosis overall of 75.2% in the period 2009–2011 and of 90.9% in the period 2016–2019. Our observations indicate that the validity of the VTE diagnoses in DNPR has improved over the years. We have no explanation for this. All NPVs were found to be higher than 99%. We found no significant variations when stratifying the data by sex, age, or surgical site.
Administrative Data in Research
We used the DNPR to identify our study subjects. DNPR was initially established for administrative purposes rather than research and the diagnoses can be incorrect for various reasons. Multiple different diagnoses have been validated in the DNPR. Schmidt et al performed a systematic review to create a bibliography of validated administrative data in the DNPR, where they reported PPVs of different diagnoses in the DNPR ranging between 15% and 100%.21 The type of diagnosis and the prevalence of it may influence its validity. Lymphoma patients’ coverage and quality have been assessed in both the DNPR and the Danish national lymphoma registry in a study of Arboe et al, reporting overall PPVs ranging from 93.4% to 100% in both databases.22 Another study investigated the validity of rheumatoid arthritis in the corresponding clinical database (DANBIO) and the DNPR, showing a difference between DANBIO having a PPV of 92% and DNPR with a PPV of 79%, which both improved over the study period.23 Thus, DANBIO is apparently better than DNPR and this difference may be due to how the databases record data and how they validate it concerning their inclusion criteria, as well as what purpose the data serve in the registers. This is a key point when using data from different databases for research, and the data should be validated against the gold standard (ie, the actual medical record) before use to ensure the data quality. Multiple international studies have reported predictive values regarding VTE diagnosis, with values ranging from 29% to 97%, ie, a large difference between the databases.12,13,24–26 Many factors may influence the validity of the data; ICD code used, setting (hospital, emergency room, outpatient), medical prescriptions, radiology reports, other codes as NOMESCO, or simply another diagnosis.
Comparison to Other Studies
To our knowledge, this is the first study validating VTE diagnosis after lower limb surgery registered in DNPR against the individual medical records. Prior studies have validated the VTE diagnosis in DNPR either in random population samples, in pregnant women, or in cancer patients.
Sundbøll et al reviewed 49 medical records from patients with a PE diagnosis and 51 medical records from patients with a DVT diagnosis in the DNPR. Twenty-two of the 100 possible VTE patients did not have an ultrasound or CT scan performed. They reported a PPV for VTE overall to 88%, DVT 86%, and PE 90%, which is higher than our results from the periods 2009–2011 and 2012–2015, but slightly lower than our results from the period 2016–19, and our overall validation matches their reported values.25 Another recent study from Sweden performed validation of VTE diagnoses during the recent years in a large population-based cohort. Their study reported a PPV of overall VTE (72.3%) along with PE (80.7%) and DVT (59.2%). While their PPV for PE was close to the value we reported, their PPV for DVT was substantially lower, and when they stratified by the years 2009–2014 it was even lower for DVT (54.1%) but increased for PE (85.8%).24
Danish studies have previously examined the validity of VTE in specific patient groups including pregnant and pediatric patients, where various PPVs have been reported. Validation of the VTE diagnosis in the general population may differ from validation when combining it with, for example, other diagnostic codes.13,27,28 Our study population contains orthopedic surgical patients, which are also known to have a higher risk of VTE, which could explain the higher PPVs we have found compared to the other studies. This corresponds to a study from Drljevic et al, which investigated the quality of VTE diagnoses among prostate cancer patients in the DNPR. Cancer patients are also known to have increased risk of developing VTE, and they reported the overall PPV to be 86.1%.29 Restriction to high-risk patients or specialized departments like hematology could likely result in higher PPVs than reported in the general population. A study reported sex disparities in VTE diagnosis predictive values in the DNPR in a general population, but in this study of orthopedic surgical patients we could not replicate those findings.13 Neither did we find a difference depending on age or location of surgery on limb.
In our study, we included 22 different ICD codes for both PE and DVT to extract all events. The specific ICD-10 code for postsurgical deep vein thrombosis (DT817C) was used in one patient. However, it is important to use all relevant codes for PE and DVT.
Other Findings
We identified 62 false-positive VTE diagnoses. The main reason for this was patients admitted to the hospital due to suspected VTE, in whom the diagnosis was rejected after the diagnostic workup. This indicates that the false-positive findings were caused by a systematic coding error by physicians, who should use a diagnosis more representative like “observational for VTE” rather than the VTE diagnosis. We identified 88 cases with more than one diagnosis for VTE following the lower limb surgery resulting in a total of 113 additional diagnoses, where only four were confirmed to be true recurrent VTE events. The majority of the additional diagnoses were given during the treatment course of a diagnosed VTE, most often DVT. Only four of the additional VTE codes represented legitimate recurrent VTE events. Use of DNPR data in studies regarding recurrent VTE after lower limb surgery must be used with caution, if used at all.25
Strength/Limitations
A major strength of this study is the fact that medical records of all included participants, cases as well as comparators, were reviewed for the entire follow-up period. Most studies only investigate PPVs, but our study also reported NPVs, which is important knowledge ensuring that the number of false negatives is low. Another strength is the stringent use of objective criteria to validate VTE diagnoses; we only considered a valid VTE diagnosis if the patient had a conclusive imaging report confirming the VTE. A limitation of our study is that we only included participants with residency in one region of Denmark, which might limit the generalizability, but the different regions of Denmark seem to be comparable in terms of socioeconomic characteristics and healthcare utilization and therefore should be considered generalizable to the entire country.30 When restricting to one region, we could ensure complete follow-up of the participants, which is a major strength. However, our findings may not be generalizable to all countries due to differences in coding practice or systems, disease definitions, and various diagnostic criteria. We designed the REDCap database in this study in order to clearly identify typing errors in the dataset, leading to immediate manual correction. However, human error is always a possibility.
Conclusion
Our results confirm that the DNPR is a valuable resource for epidemiology research concerning orthopedic post-surgical VTE diagnosis and show that the validity has improved during the last decade. Despite this improvement, researchers should be aware of the overestimation of acute VTE events when using data from the DNPR, especially in high-incidence populations. Importantly, we also observed that additional VTE diagnosis codes after the first VTE event cannot stand alone when searching for recurrent VTE.
Acknowledgment
The authors wish to thank all the involved departments and all the individual surgeons, physicians, and other healthcare professionals for their contribution in submitting clinical data to the national administrative registry.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Ms Josephine Galsklint reports grants from Svend Andersen Fonden and Region Nordjyllands Sundhedsvidenskabelige Forskningsfond, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Pedersen AB, Johnsen SP, Sørensen HT. Increased one-year risk of symptomatic venous thromboembolism following total hip replacement. J Bone Joint Surg Br. 2012;94-B(12):1598–1603. doi:10.1302/0301-620X.94B12.29358
2. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Jt Surg. 2007;89(4):780–785. doi:10.2106/00004623-200704000-00012
3. Keller K, Tesche C, Gerhold-Ay A, et al. Quality of life and functional limitations after pulmonary embolism and its prognostic relevance. J Thromb Haemost. 2019;17(11):1923–1934. doi:10.1111/jth.14589
4. Næss IA, Christiansen SC, Romundstad P, Cannegieter SC, Rosendaal FR, Hammerstrøm J. Incidence and mortality of venous thrombosis: a population-based study. J Thromb Haemost. 2007;5(4):692–699. doi:10.1111/j.1538-7836.2007.02450.x
5. Heit JA, Silverstein MD, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ. Predictors of survival after deep vein thrombosis and pulmonary embolism: a population-based, cohort study. Arch Intern Med. 1999;159(5):445–453. doi:10.1001/archinte.159.5.445
6. Gade IL, Kold S, Severinsen MT, et al. Venous thromboembolism after lower extremity orthopedic surgery: a population‐based nationwide cohort study. Res Pract Thromb Haemost. 2021;5(1):148–158. doi:10.1002/rth2.12449
7. Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/CLEP.S179083
8. Jutte DP, Roos LL, Brownell MD. Administrative record linkage as a tool for public health research. Annu Rev Public Health. 2011;32:91–108. doi:10.1146/annurev-publhealth-031210-100700
9. Arnason T, Wells PS, van Walraven C, Forster AJ. Accuracy of coding for possible warfarin complications in hospital discharge abstracts. Thromb Res. 2006;118(2):253–262. doi:10.1016/j.thromres.2005.06.015
10. Fang MC, Fan D, Sung SH, et al. Validity of using inpatient and outpatient administrative codes to identify acute venous thromboembolism. Med Care. 2017;55(12):e137–43. doi:10.1097/MLR.0000000000000524
11. Baumgartner C, Go AS, Fan D, et al. Administrative codes inaccurately identify recurrent venous thromboembolism: the CVRN VTE study. Thromb Res. 2020;189:112–118. doi:10.1016/j.thromres.2020.02.023
12. Zhan C, Battles J, Chiang YP, Hunt D. The validity of ICD-9-CM codes in identifying postoperative deep vein thrombosis and pulmonary embolism. Jt Comm J Qual Patient Saf. 2007;33(6):326–331. doi:10.1016/s1553-7250(07)33037-7
13. Severinsen MT, Kristensen SR, Overvad K, Dethlefsen C, Tjønneland A, Johnsen SP. Venous thromboembolism discharge diagnoses in the Danish National Patient Registry should be used with caution. J Clin Epidemiol. 2010;63(2):223–228. doi:10.1016/j.jclinepi.2009.03.018
14. Lawrenson R, Todd JC, Leydon GM, Williams TJ, Farmer RDT. Validation of the diagnosis of venous thromboembolism in general practice database studies. Br J Clin Pharmacol. 2000;49(6):591–596. doi:10.1046/j.1365-2125.2000.00199.x
15. Mainz J, Hess MH, Johnsen SP. The Danish unique personal identifier and the Danish Civil Registration System as a tool for research and quality improvement. Int J Qual Health Care. 2019;31(9):717–720.
16. Pedersen CB. The Danish Civil Registration System. Scand J Public Health. 2011;39(7):22–25. doi:10.1177/1403494810387965
17. Schmidt M, Pedersen L, Sørensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
18. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
19. StataCorp. Stata Statistical Software. College Station, TX: StataCorp LLC; 2019.
20. Seed P. DIAGT: stata module to report summary statistics for diagnostic tests compared to true disease status [Internet]. Vol. 3. Statistical Software Components. Boston College Department of Economics; 2010 [cited 2021 Aug 8]. Available from: https://ideas.repec.org/c/boc/bocode/s423401.html.
21. Schmidt M, Schmidt SAJ, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449. doi:10.2147/CLEP.S91125
22. Arboe B, El-Galaly TC, Clausen MR, et al. The Danish National Lymphoma Registry: coverage and Data Quality. PLoS One. 2016;11(6):e0157999. doi:10.1371/journal.pone.0157999
23. Ibfelt EH, Sørensen J, Jensen DV, et al. Validity and completeness of rheumatoid arthritis diagnoses in the nationwide DANBIO clinical register and the Danish National Patient Registry. Clin Epidemiol. 2017;9:627–632. doi:10.2147/CLEP.S141438
24. Öhman L, Johansson M, Jansson JH, Lind M, Johansson L. Positive predictive value and misclassification of diagnosis of pulmonary embolism and deep vein thrombosis in Swedish patient registries. Clin Epidemiol. 2018;10:1215–1221. doi:10.2147/CLEP.S177058
25. Sundbøll J, Adelborg K, Munch T, et al. Positive predictive value of cardiovascular diagnoses in the Danish National Patient Registry: a validation study. BMJ Open. 2016;6(11):e012832. doi:10.1136/bmjopen-2016-012832
26. Tamariz L, Harkins T, Nair V. A systematic review of validated methods for identifying venous thromboembolism using administrative and claims data. Pharmacoepidemiol Drug Saf. 2012;21(SUPPL. 1):154–162. doi:10.1002/pds.2341
27. Larsen TB, Paaske Johnsen S, Møller CI, Larsen H, Sørensen HT. A review of medical records and discharge summary data found moderate to high predictive values of discharge diagnoses of venous thromboembolism during pregnancy and postpartum. J Clin Epidemiol. 2005;58:316–319. doi:10.1016/j.jclinepi.2004.07.004
28. Tuckuviene R, Risom Kristensen S, Helgestad J, Christensen AL, Johnsen P. Clinical Epidemiology Dovepress Predictive value of pediatric thrombosis diagnoses in the Danish national Patient registry. Clin Epidemiol. 2010;2:107–122. doi:10.2147/CLEP.S10334
29. Drljevic A, Borre M, Ehrenstein V, Nguyen-Nielsen M, Hoyer M. Quality of venous thromboembolism diagnoses among prostate cancer patients in the Danish National Registry of Patients. Clin Epidemiol. 2014;6:351. doi:10.2147/CLEP.S65681
30. Henriksen DP, Rasmussen L, Hansen MR, Hallas J, Pottegård A. Comparison of the Five Danish Regions regarding demographic characteristics, healthcare utilization, and medication use—A Descriptive Cross-Sectional Study. PLoS One. 2015;10(10):e0140197. doi:10.1371/journal.pone.0140197
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.