Back to Journals » Psychology Research and Behavior Management » Volume 17
Validation and Psychometric Properties of the Chinese Version of the Binge Eating Scale in Young Adults
Authors Yan WS ![]() , Liu SJ, Liu MM
, Liu SJ, Liu MM
Received 25 January 2024
Accepted for publication 7 April 2024
Published 12 April 2024 Volume 2024:17 Pages 1611—1624
DOI https://doi.org/10.2147/PRBM.S456275
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Wan-Sen Yan,1,2 Su-Jiao Liu,1 Meng-Meng Liu1
1Department of Psychology, School of Medical Humanitarians, Guizhou Medical University, Guiyang, People’s Republic of China; 2Guizhou Research Institute for Health Development, Guizhou Medical University, Guiyang, People’s Republic of China
Correspondence: Wan-Sen Yan, Department of Psychology, School of Medical Humanitarians, Guizhou Medical University and Guizhou Research Institute for Health Development, Guizhou Medical University, 9 Beijing Road, Yunyan District, Guiyang, 550004, People’s Republic of China, Tel +86-136-4850-4644, Email [email protected]
Background: Although structured clinical interviews are considered the gold standard for assessing binge eating disorder (BED), the self-administered Binge Eating Scale (BES) has been widely used as a screening tool for BED in clinical research. However, the psychometric properties of the BES among Chinese young adults remain unclear. This study aimed to examine the validity of a Chinese version of the BES with a large sample.
Methods: A total of 2182 young adult college students were tested using the Simplified Chinese version of BES (SCBES), the 7-Item Binge-Eating Disorder Screener (BEDS-7), the Zung Self-Rating Depression Scale (SDS), the Generalized Anxiety Disorder Scale (GAD-7), and the Dual-Modes of Self-Control Scale (DMSC). The frequency of objective binge-eating episodes was used as a measure of severity. Validity and reliability of the SCBES were assessed through multiple analyses, along with the item analysis.
Results: The data revealed that the SCBES demonstrated reasonable reliability and validity. The Cronbach’s α value was 0.813, with a one-month test–retest reliability of 0.835. The exploratory factor analysis (EFA) extracted three first-order factors, which explained a total of 53.82% of the variance. The confirmatory factor analysis (CFA) confirmed the three-factor model (ie, Binge-eating behaviors, Lack of control, Negative affects related to overeating), with a good model fit. The SCBES also demonstrated excellent concurrent and criterion validity, significantly correlating with the BEDS-7 and frequency of objective binge-eating episodes (r= 0.760– 0.782, p< 0.001). Gender, body mass index, depression, anxiety, impulsivity, and self-control were significantly associated with the total score of SCBES.
Conclusion: The SCBES demonstrated sound psychometric properties and exhibited good cross-cultural adaptability in Chinese young adults, with a novel three-factor model fitting the data best. This scale could serve as a useful screening tool for identifying the severity of binge eating behaviors among Chinese youths.
Keywords: Binge eating, psychometric properties, Chinese adults, college students
Introduction
Binge eating disorder (BED), an important health issue, has been officially recognized as a diagnostic category in the Fifth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). BED is a complex condition characterized by recurrent episodes of overeating/binge-eating and a loss of control over eating, accompanied by emotional distress and discomfort.1,2 BED has been proven to be associated with numerous psychiatric and physical complications, resulting in impairments in quality of life and even increased mortality.3,4 The lifetime prevalence of BED in the general population worldwide is approximately 1.53%, with a higher rate observed among females (2.42%) compared to males (1.17%).5 The 12-month prevalence estimates for BED are 0.93% for females and 0.51% for males, respectively.5 The onset of BED may occur during late adolescence and early adulthood, but it carries a lifelong risk.6,7 The natural course of BED often lasts for a long time, with an average duration of 14–16 years.8,9 It is worth noting that young people are at a higher risk for BED, with a significantly greater incidence rate compared to other age groups.1,10 For instance, the lifetime prevalence of eating disorders, including BED, bulimia nervosa (BN), and anorexia nervosa (AN), is 5.12% among young adults aged 18–29 years, compared to 2.38% in the group aged 30–44 years old and 1.29% in the group aged 45+ years old.11 Unfortunately, BED has been largely invisible and overlooked in comparison to AN and BN, and individuals with BED are often underdiagnosed and undertreated, possibly due to societal biases and stigma associated with weight and body image.12 In this regard, timely and effective screening for BED is considered essential for further diagnosis, particularly among at-risk populations such as adolescents and young adults.2
Structured clinical interviews conducted by clinical experts are recognized as the gold standard for diagnosing BED. Frequently used instruments for the diagnostic assessment of BED include the Eating Disorder Examination (EDE) and the Structured Clinical Interview for DSM-5 Disorders (SCID).2 There are also a series of specific self-report instruments available for the early detection and screening of BED, including the Eating Disorder Examination Questionnaire (EDE-Q), the Eating Disorders Inventory (EDI-3), the 7-Item Binge-Eating Disorder Screener (BEDS-7), and the Binge Eating Scale (BES), among others.13 Given that structured interviews require specialized training and are time-consuming, lasting 1–2 hours, self-report measurements of BED have been widely used to screen and assess binge-eating pathology in clinical research.13 The BES, developed by Gormally et al,14 was specifically designed to screen for and evaluate problems related to binge eating. The BES is a self-report scale consisting of 16 items that assess behavioral, emotional, and cognitive symptoms of binge eating among individuals at risk. Each item contains three or four statements, which reflect a range of severity from no problems (scored as 0) to severe problems (scored as 3). The total possible score ranges from 0 to 46. The total score on the BES reflects the severity of binge-eating behavior, with a score of 18 or higher indicating probable BED.15,16 Furthermore, based on the BES scores, uncontrolled eating behaviors can be classified into three different severity categories: individuals scoring 0–17 are considered non-binge eaters; those scoring 18–26 are categorized as moderate binge eaters; and individuals with scores ranging from 27 to 46 are classified as severe binge eaters.17,18 In the BES, there are eight items that describe behavioral manifestations and another eight items that focus on feelings and cognition related to binge eating.14 However, this proposed two-dimensional structure for the original scale has not been consistently confirmed in other studies with translated versions. Instead, a one-factor model is often found and utilized,19,20 which indicates the necessity of conducting further research.
Additionally, it is recognized that the construct BED has deep roots in Western culture. Our current understanding of the epidemiology of BED mainly comes from clinical and community-based studies conducted in North America and Europe.2,21 Nevertheless, research interest and data on BED continue to emerge from other parts of the world, including Asia.5,22 For instance, binge eating behaviors have increased among Chinese adolescents and young adults, possibly due to rapid economic development and intensifying societal competition. In a large sample of adolescents aged 11–17 years (n=1177), the rate of binge eaters was 32.23% among overweight/obese individuals, compared to 0.54% in those with a normal weight.23 Among 1013 Chinese young adult college students, approximately 8.39% were identified as individuals with binge-eating problems.24 However, there is still an urgent need for a validated tool in Chinese culture to assess and monitor binge eating disorder among clinical and non-clinical populations. Considering that the BES is a concise and useful tool for screening and assessing binge-eating problems, a Simplified Chinese version of the BES (SCBES) has been translated and preliminarily validated among adolescents aged 12 to 18 years old.25 In this sample, the SCBES demonstrated a satisfactory and acceptable one-factor model, with a Cronbach’s α value of 0.805 and a two-week test–retest reliability coefficient of 0.768. However, this sample mainly consisted of high school students, with over 20% of them being overweight or obese.25 In comparison to children and adolescents, young adults (eg, college students) actually have easier access to food in China and appear to be at a higher risk of developing binge-eating problems, particularly when they face heavy academic pressure and social competition.24,26,27 Unfortunately, the validation and psychometric properties of the SCBES in Chinese young adults remain unclear. Moreover, the cross-cultural adaptability of the BES among young populations in China has limited evidence available. Recently, the psychometric properties of the BES and variables associated with binge eating were examined among overweight college students aged 18 to 24 years in Taiwan.28,29 However, a translated Traditional Chinese version of BES was used and only overweight and obese students were included.28,29 Considering the significant differences associated with the utilization of Simplified and Traditional Chinese, further studies are required to assess the adaptability of the Simplified Chinese version of BES in young adults.
The purpose of this study was to assess the psychometric properties of the SCBES in a large non-clinical sample of Chinese young adults who are at risk for BED. This is important because most previous studies have focused on clinical populations and were conducted in Western cultures.2 A total of 2182 young adult college students were tested using the SCBES, the 7-Item Binge-Eating Disorder Screener (BEDS-7), the Zung Self-Rating Depression Scale (SDS), the Generalized Anxiety Disorder Scale (GAD-7), and the Dual-Modes of Self-Control Scale (DMSC). Objective frequency of binge-eating episodes was employed as a severity specifier. The factorial structure, validity, and reliability of the scale were examined through multiple analyses.
Materials and Methods
Participants
All participants were young adult college students who were randomly recruited from six local universities in Guiyang, China, between September and December 2021. Firstly, a list of 12 universities was created in the University Town, and then six random universities were selected from that list. In each of the six universities, 400 undergraduate students were randomly selected based on their student registration numbers, with an approximate proportion of 5%. All 2400 students were invited to complete a series of self-report scales through the online survey programming platform (ie, WenJuanXing). All the students participated in this study voluntarily. Among them, 67 students failed to complete the online survey, and thus were excluded from the study. Besides, 53 students were excluded due to invalid arbitrary responses or a large number of omissions (>5%) on the scale items, and 98 students were excluded because they were under 18 years old. As a result, a total of 2182 participants (mean age: 19.06 ± 1.03 years, ranging from 18 to 25 years; 1383 females, 63.4%) were included in the final data analysis. All subjects provided the online informed consent, and were compensated with a coupon equal to RMB ¥ 20 each.
Measurements
Demographics. A brief questionnaire was used to collect demographic data (eg, age, gender, ethnicity, years of education, weight, and height) through self-reports. Body Mass Index (BMI) was then calculated by weight divided by the square of height (kg/m2). Smoking and drinking behaviors were assessed using one single yes/no question each: “Have you smoked at least one cigarette in the past 14 days”; “Did you take at least one drink in the past 14 days”, respectively.
Weekly Frequency of Binge-Eating Episodes
The participants reported their average weekly frequency of objective binge-eating episodes over the past three months. The main question was “On average, how many times did you experience actual episodes of excessive overeating per week during the last three months?”. According to the DSM-5, the objective frequency of binge-eating episodes was used as a severity specifier. Specifically, five severity groups were defined as follows: no binge-eating (0 episodes/week), mild (1–3 episodes/week), moderate (4–7 episodes/week), severe (8–13 episodes/week), and extreme (≧14 episodes/week).30
Binge Eating Scale
The SCBES has previously been validated in Chinese adolescents.25 To develop the SCBES, classical back-translation methods were used. After obtaining permission from its authors, the original BES14 was translated from English into Simplified Mandarin Chinese by two bilingual Chinese-native psychologists. Following discussion and revision by the translators and another two bilingual researchers, an earlier version of the SCBES was developed. Subsequently, this version was back translated into English by one independent bilingual psychologist, who was blind to the original BES. In the third stage, all translators and researchers reviewed the original and back-translated versions, and resolved their discrepancies before finalizing this scale. The SCBES showed reasonable psychometric properties with a one-factor model in Chinese adolescents.25 Consistent with the original BES, the SCBES has 16 items, each with three or four statements that reflect a range of severity of binge eating. Higher total scores indicate more severe binge eating problems. In the present study, we further tested the psychometric properties of the SCBES among Chinese young adults with a large sample.
BEDS-7
The BEDS-7 is a patient-reported screening tool designed to identify individuals with probable BED.31 It consists of seven items, which were developed based on the DSM-5 diagnostic criteria for BED. This scale was validated in general community residents with and without BED characteristics, with a sensitivity of 100% and a specificity of 38.7%.31 In the BEDS-7, the first two items assess whether the participants have engaged in excessive eating over the past three months (YES=1 and NO=0), such as item 1
During the last three months, did you have any episodes of excessive overeating, i.e., eating significantly more than what most people would eat in a similar period of time
And item 2 “Do you feel distressed about your episodes of excessive overeating”. The items 3–7 used a 4-point Likert scale (Never/rarely=0, Sometimes=1, Often=2, and Always=3) to measure relevant symptoms (ie, out of control over eating, continue eating even though not hungry, embarrassed by how much eaten, disgusted or guilty afterward, and make self vomit to control weight or shape). The BEDS-7 total score was employed as an indicator of concurrent validity for the SCBES. Cronbach’s α of the scale was 0.823 in this study.
SDS
The SDS32 was used to measure depression symptoms over the past two weeks. There are 20 items rated on a 4-point Likert scale from 1 (None or a little of the time) to 4 (Most or all of the time). Higher total scores reflect heavier depression symptoms. Cronbach’s α of the SDS was 0.890 in this study.
GAD-7
The GAD-7 is a self-rating scale for detecting anxiety symptoms during the last two weeks, which is widely used in both clinical practice and research.33 There are seven items rated on a 4-point Likert scale (Not at all=0, Several days=1, More than half the days=2, and Nearly every day=3). A higher total score reflects heavier anxiety symptoms. Cronbach’s α of the GAD-7 was 0.763 in this study.
DMSC
The DMSC is a self-report scale for assessing the dual-system processes of behavioral control (ie, impulsivity and self-control).34,35 It consists of 21 items rated on a 5-point Likert scale from 1 (Not at all true) to 5 (Always true). The impulsivity subscale with 12 items includes three factors (impulsiveness, easy distraction, and inability to delay gratification), and the self-control subscale with 9 items includes two factors (problem solving and future-oriented time view). Higher total scores indicate a higher level of impulsivity or self-control. Cronbach’s α values were 0.938 and 0.891 for the two subscales in this study, respectively.
Statistical Analyses
Data analysis was performed with the Statistical Package for Social Sciences for Windows Version 22.0 and AMOS Version 24.0 (SPSS Inc., Chicago, IL, USA). The exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were used to determine the potential factor structure of the SCBES. The total sample (n=2182) was randomly separated into two subgroups for EFA (n=1091) and CFA (n=1091), respectively. In EFA, principal component analysis (PCA) with varimax rotation was conducted based on factorability analysis using Kaiser–Meyer–Olkin (KMO) measurement and Bartlett test of sphericity. The CFA was used to test the fitting of the proposed models in EFA, using structural equation modeling (SEM) from the AMOS. Concurrent and criterion validity were tested with Pearson correlation coefficients, which were conducted between the SCBES and the BEDS-7 scores and between the SCBES score and the objective frequency of binge-eating episodes. Reliability for internal consistency of the SCBES was detected using Cronbach’s α coefficient. Test–retest reliability was evaluated to test temporal stability, using the intraclass correlation coefficient (ICC). Two hundred and twenty participants (about 10%) of the total sample were randomly selected to complete the SCBES again one month after their first test. Besides, a multivariate linear regression analysis was performed to explore the relationships between demographics (eg, age, gender, ethnicity, BMI), depression, anxiety, impulsivity, self-control, and binge eating. Statistical significance was set as p < 0.05, two-tailed.
Results
Demographic Characteristics and Scale Scores
As seen in Table 1, this sample had an average BMI of 20.81 ± 2.76 kg/m2, with 78.0% displaying a normal weight and 6.9% being overweight or obese. The mean of the SCBES scores was 8.98 ± 6.40 (ranging from 0 to 42). All of the scale scores (ie, SCBES, BEDS-7, SDS, GAD-7, DMSC) had an approximately normal distribution according to the skewness and kurtosis.
 |
Table 1 Demographic Characteristics and Scale Scores of the Sample (n=2182) |
Item Analysis and Scale Reliability
Item analysis was conducted to analyze the item effectiveness in the SCBES. The top and bottom 27% of the SCBES total scores were designated into the high-score group (n=589) and low-score group (n=589), respectively. Then, the scores of each item in these two groups were compared using t-test. Table 2 revealed that each of the 16 items exhibited significant difference between the two groups with excellent item effectiveness (all p<0.001). Furthermore, the item-total score correlations were tested using Pearson correlation. The correlation coefficients of the 16 items with the SCBES total score were all higher than 0.3 (from 0.311 to 0.631, all p<0.001).
 |
Table 2 Item Analysis (M±SD) and Item-Total Score Correlations (r) of the SCBES |
As shown in Table 3, the internal consistency reliability of the SCBES was 0.813, indicated by Cronbach’s α. After removing any individual item, Cronbach’s α of the total scale ranged from 0.793 to 0.811, indicating good internal consistency of the items. Evaluated with the ICC (n=220), one-month test–retest reliability for this scale was 0.835 (p<0.001), higher than the standard 0.75.
 |
Table 3 Cronbach’s α and Test–Retest Reliability of the SCBES |
Construct Validity from the EFA and CFA
Based on the KMO value (0.913) and Bartlett test of sphericity (χ2=3317.44, df=120, p<0.001), EFA was performed for factor analysis of the SCBES. Three factors with an Eigenvalue over 1 were extracted from the PCA using the varimax rotation, explaining a total of 53.82% of the variance (see Table 4). The first factor (including items 2, 7, 8, 9, 10, 11, 13, and 16) appears to represent a series of behavioral manifestations of binge eating, such as eating quickly, excessive and uncomfortable overeating, bipolar eating model (ie, feast or famine), uncontrolled urges, continual eating without plans, and unconsciousness for hunger. As a result, it is named as “Binge-eating behaviors”. The second factor (including items 3, 4, 5, 14, and 15) embodies the key symptoms of loss of control, overeating habits (when boring or even not hungry), and cognitive hijacking/preoccupation in BED, thus it is named as “Lack of control”. The third factor (including items 1, 6, and 12) refers mainly to the feelings of shame, disgust, guilt, or self-hate due to overeating, so named as “Negative affects related to overeating”.
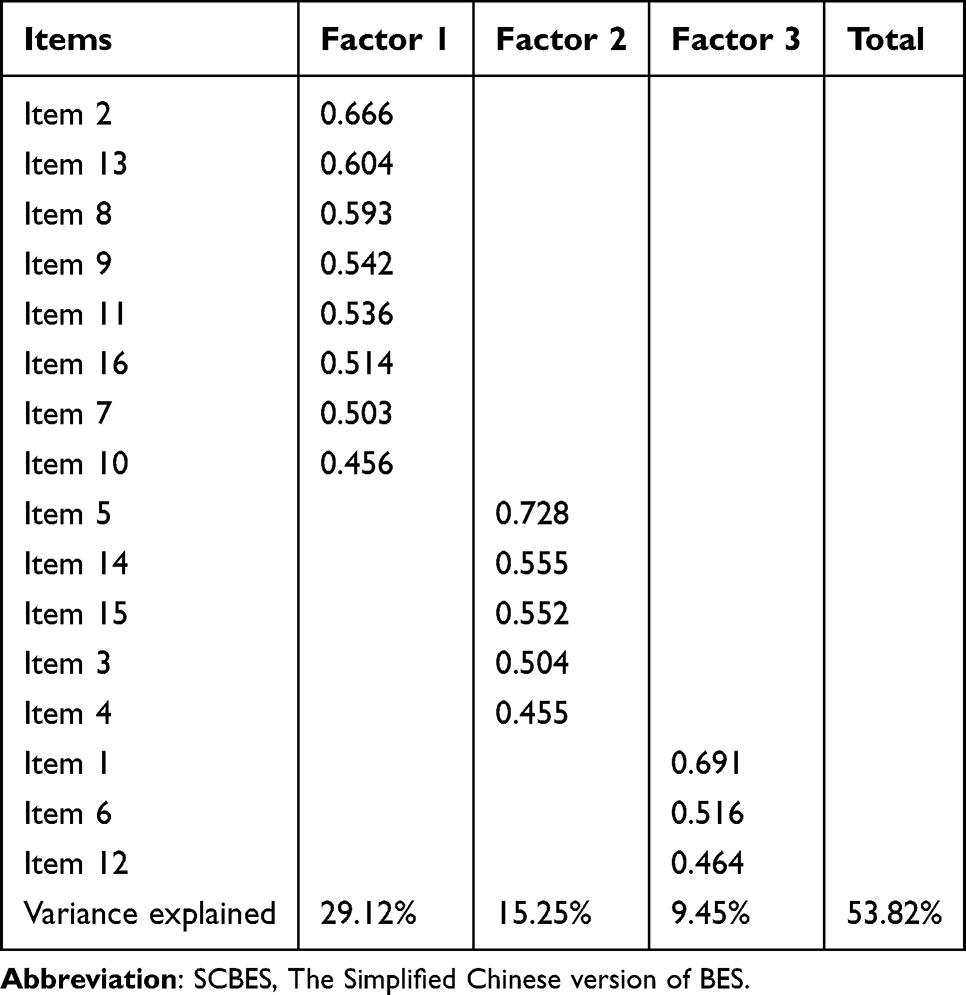 |
Table 4 Varimax Rotated Factor Loadings of the SCBES (n=1091) |
The CFA was further performed to confirm the three-factor model derived from the EFA. The following indices for model fit were used: (a) χ2/df, the ideal value of 1 to 3; (b) goodness-of-fit index (GFI), the ideal value over 0.90; (c) adjusted goodness-of-fit index (AGFI), the ideal value over 0.90; (d) root mean square error of approximation (RMSEA), the ideal value below 0.05; (e) standardized root mean square residual (SRMR), the ideal value below 0.05; (f) comparative fit index (CFI), the ideal value over 0.95; and (g) non-normed fit index (NNFI), the ideal value over 0.95.36 Table 5 revealed that all of these indices in the three-factor model were good for ideal model fit (χ2/df = 2.796, RMSEA = 0.041, SRMR = 0.021, with GFI, AGFI, CFI, and NNFI all over 0.95). Considering the BES is always used as a single uni-dimensional measure for probable BED, we further compared the three-factor model with the one-factor model of the SCBES, which was previously proposed in Chinese adolescents. As displayed in Table 5, although the one-factor model appeared to have an acceptable model fit, the three-factor model demonstrated a better fit with the sample, superior on each of these indices. The factor structure of the three-factor model was clearly depicted for the SCBES in Figure 1. The three first-order factors (ie, “Binge-eating behaviors”, “Lack of control”, “Negative affects related to overeating”) were closely linked to each other, showing a reasonable construct validity.
 |
Table 5 Model Fit Between the Three-Factor and One-Factor Models of the SCBES (n=1091) |
 |
Figure 1 Factor structure of the three-factor model for the Simplified Chinese version of BES (SCBES). Factor 1=Binge-eating behaviors, Factor 2=Lack of control, Factor 3=Negative affects related to overeating. |
Concurrent and Criterion-Related Validity
Based on the approximately normal distributions of all the scale scores, Pearson correlations were used to investigate concurrent validity between the SCBES and the BEDS-7, and criterion validity between the SCBES and objective frequency of binge-eating episodes, respectively. Data in Table 6 revealed that there were significant positive correlations of the SCBES scores with the BEDS-7 (r=0.782, p<0.001) and weekly frequency of binge-eating episodes (r=0.760, p<0.001).
 |
Table 6 Pearson Correlations (r) Between the SCBES, the BEDS-7, and Binge-Eating Episodes (n=2182) |
The weekly frequency of binge-eating episodes was further used for diagnostic evaluation. According to the DSM-5, “none to mild” binge-eating was defined as 0–3 episodes per week, while “moderate to extreme” binge-eating was defined as ≥4 episodes per week. Therefore, a cut-off score of 4 episodes per week was utilized in this study. As shown in Figure 2, the receiver operating characteristic (ROC) curve revealed that the area under the curve (AUC) was 0.935 (95% CI = 0.916–0.953, p<0.001), suggesting that the SCBES demonstrated a significant effect in predicting the severity of binge-eating symptoms. The Youden index was used to determine the best SCBES cut-off score, showing an optimal cut-off score of 17.5 with a sensitivity of 0.946 and a specificity of 0.905 (Supplementary Table S1), in line with the original BES cut-off score (ie, ≧18 points for probable BED).
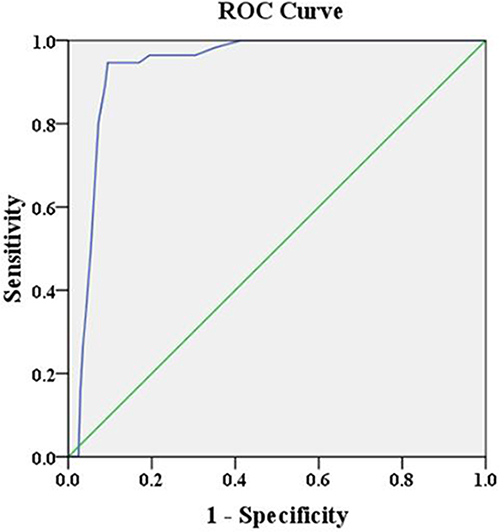 |
Figure 2 The receiver operating characteristic (ROC) curve that displayed the accuracy of the Simplified. Chinese version of BES (SCBES) as a screening tool for objective severity of binge-eating symptoms, with an area under the curve (AUC) of 0.935 (95% CI = 0.916–0.953, p < 0.001, n = 2182). |
Multivariate Linear Regression Outcomes
The multivariate linear regression analysis was further performed to test the relationships between demographics, depression, anxiety, impulsivity, self-control, and SCBES scores. Table 7 shows that age, years of education, ethnicity, home locality, smoking and drinking status were not related to the SCBES total score (all p>0.05). Gender and BMI had a positive effect on binge eating (β=0.205, p<0.001; β=0.196, p<0.001, respectively). Higher levels of depression, anxiety, and impulsivity were associated with elevated SCBES scores (β=0.057–0.289, all p<0.001), while a higher level of self-control was related to a lower SCBES score (β= −0.288, p<0.001). Totally, this regression model was significant with 33.5% variance explained (Δ R2=0.335, p<0.001).
 |
Table 7 Multivariate Linear Regression Analysis for the SCBES Total Score (n=2182) |
Discussion
In this study, we tested psychometric properties of the Chinese version of the BES in a large non-clinical sample of young adults. The data revealed that the SCBES had reasonable reliability and validity. A new three-factor model (ie, Binge-eating behaviors, Lack of control, Negative affects related to overeating) of the scale was confirmed by the CFA, showing a good model fit. Totally, the SCBES demonstrated good cross-cultural adaptability in the Chinese young adults.
Despite the high prevalence of BED in general populations, there remains a low level of public awareness regarding this disorder, and at times, a large research-practice gap exists.2 The screening, prevention, and management for BED do not seem to be well established worldwide; therefore, the global significance of BED remains unclear.37 In recent years, research interest and publications on BED have been emerging in China, despite great limitations in the available epidemiological data.5 The lack of convenient, validated, and effective screening tools may be an important reason. The BES was developed and extensively utilized in Western cultures, and its original English version has been translated into other languages and validated in cross-cultural samples, including Spanish, Portuguese, Italian, French, Malay, and Arabic.19,20,38–41 A Traditional Chinese version of BES was also translated and tested among overweight college students in Taiwan.28 Additionally, a Simplified Chinese version of the BES (ie, SCBES) has been translated, whereas it was only examined among a sample of middle school students in Mainland China.25 Validation of the BES in Chinese young adults needs further research.
In the present study, we found that the SCBES demonstrated good psychometric properties in the Chinese young people aged 18–25 years. The Cronbach’s α was 0.813 for the SCBES, and after removing any individual item, Cronbach’s α ranged from 0.793 to 0.811, indicating good internal consistency of the scale. Furthermore, the one-month test–retest reliability of the scale was 0.835. These reliability data were consistent with findings in previous studies.40,41 Notably, our data for the SCBES were comparable to that of the Traditional Chinese version of BES,28 which had a Cronbach’s α of 0.83 and a one-month test–retest reliability of 0.83. Although this previous study28 included only overweight or obese students with an adequate sample size (n=300), the age of the participants ranged from 18 to 24 years, which is almost identical to that in our sample. Therefore, these converging data suggest that the BES may possess an excellent reliability estimate among Chinese young adults. However, considering the explicit cultural and habitual differences associated with the utilization of glyph images, the Simplified (or Traditional) Chinese version of the BES might not be properly used in Taiwan (or Mainland China). Future comparative studies on these two versions of the BES will be necessary.
More interesting findings in our study were from the EFA and CFA. Based on the randomly-separated half of the whole sample, we firstly performed the EFA, through which three factors with an Eigenvalue over 1 were extracted, explaining a total of 53.82% of the variance. The CFA using the other half of the whole sample further confirmed this three-factor model of the SCBES, with an ideal model fit (Table 5). More importantly, when compared with the one-factor model proposed among Chinese adolescents,25 our three-factor model detected in the Chinese young adults also displayed superior model fit indices. In previous studies, results regarding the factorial dimension of the BES have been controversial. The one-factor model was proposed in some,19,20,39 while a two-factor model was found in others.28,40,41 Besides, one study conducted in overweight and obese patients demonstrated that both the one-factor and two-factor models exhibited a good model fit.38 Among specific samples of bariatric surgery candidates, the two-factor structure of the BES was replicated, although some of the items were not loaded.42,43 In the original BES, the 16 items were divided into two broad and somewhat vague constructs (ie, emotions/cognition and behavioral manifestations related to binge eating), mainly based on theoretical supposition, but without strict empirical verification.14 Therefore, these inconsistent findings regarding the factor structure of the BES may be attributed to cultural variations, sample characteristics, and different research time points.13,30 For instance, a two-factor model of the BES was more likely to be found in obese subjects, both clinical and non-clinical.14,28,42,43 Additionally, the presence of different samples with varying ages and BMI statuses in the general population may also be an important confounding factor contributing to nonuniform results.28 More interestingly, in some European study samples such as Spanish, Portuguese, and French, the one-dimensional factorial structure of the BES was confirmed;19,20,39 however, in the Asian adult samples including Malaysian, Arabian (Lebanese), and Chinese (Taiwanese), the original two-factor model was provided.28,40,41 Nevertheless, even for the confirmed two-factor models (eg),40,41 significant disparities regarding the results of grouped items in the BES can be observed among studies conducted in different samples from diverse cultures. In the Malay version, there are eight items grouped into each of the two factors, consistent with the original BES;40 while in the Arabic version, twelve items are loaded into the first factor and four items are loaded into the second factor, respectively.41 Therefore, cultural factors should be given greater consideration in future studies when testing the factorial models of the BES. In our study, a three-factor model of the BES was found, which seems to be a brand-new factor model that differs from the existing ones. In this model, the Factor 1 “Binge-eating behaviors” represents a range of behavioral symptoms such as eating quickly, excessive and uncomfortable overeating; the Factor 2 “Lack of control” embodies the symptoms of overeating habits, loss of control, and cognitive hijacking (ie, preoccupation) in BED; and the Factor 3 “Negative affects related to overeating” covers negative feelings due to overeating, such as shame, disgust, guilt, and self-hate. Symptoms in these factors are at the core of BED pathology,2 thus this model may be more closely aligned with the diagnostic systems of BED in the DSM-5. Nevertheless, our study sample primarily consisted of non-clinical college students aged 18–25 years in China; therefore, it remains unclear whether these findings could be replicated in different samples and cultures, which necessitates further studies. Especially, in our three-factor model, the Factor 1 is consistent with the first factor (ie, behavioral manifestations of binge eating) in the two-factor model; similarly, the Factor 3 comprises three negative emotion items that are part of the second factor (ie, emotions/cognition related to binge eating) in the two-factor model.40,42,43 In contrast, our Factor 2 includes four items of behavioral manifestations and one item of cognition related to binge eating in the two-factor model, all of which are symptoms of loss of control. Therefore, it appears that the new factor “Lack of control” is more explicit than the original factor, considering that diminished control over binge-eating behavior is a characteristic feature of BED.44 But remarkably, it is important to consider different research time points when explaining this new model of binge-eating problems, especially in the aftermath of a global pandemic such as the coronavirus disease 2019 (COVID-19), which has revealed a significant impact on the onset and course of BED.45 In one of our earlier studies published in 2018 (prior to the COVID-19 outbreak), we identified 85 individuals (8.4%) with binge-eating problems using the SCBES among a group of 1013 Chinese young adult college students aged 18 to 24 years.24 However, in the present study with a similar but larger sample collected in 2021 (after the outbreak), we detected binge-eating problems among 254 individuals (11.6%) out of the 2182 college students (Table 1), representing an increase of 3.2% in the incidence rate compared to the earlier study. More importantly, the previous study24 employed the one-factor model of the BES that was proposed and tested in Chinese adolescents,25 which demonstrated a reasonable model fit; however, our current study highlighted a new factor that portrays the symptoms of loss of control in BED in the novel three-factor model, compared to the prior one-factor and two-factor models. It is believed that the COVID-19 pandemic and related confines including social restrictions and lockdown have promoted dysfunctional eating behaviors and worsened binge-eating episodes, in which affective symptoms and a sense of lack of control are specific salient features.45 Thus, more attention should be paid to different comparative studies conducted before, during, and after the COVID-19 when investigating the dynamic course of BED and factorial models of the BES.
Regarding concurrent and criterion-related validity, we tested the correlations between the SCBES score with the BEDS-7 score as well as objective frequency of binge-eating episodes. Data revealed that there were high positive correlations (r=0.760–0.782, p<0.001) between them, indicating a pretty good concurrent and criterion validity. This was consistent with previous reports30,41 and supported the idea that the BES could be an effective tool for evaluating binge-eating problems among Chinese college students.24 Moreover, objective weekly frequency of binge-eating episodes was used for diagnostic evaluation of the SCBES. The ROC curve indicated an AUC of 0.935 (Figure 2), suggesting that the SCBES might significantly predict the moderate to extreme binge-eating problems (sensitivity=0.946, specificity=0.905), with a cut-off score of 18. These data were similar to, but slightly better than, those in previous reports (ie, a sensitivity of 0.846–0.889 and a specificity of 0.818–0.949).28,38 Our study, along with previous studies, suggests that the BES is suitable and valid for both clinical and non-clinical populations.39,46
In this study, we conducted a multivariate linear regression analysis to examine the relations between demographics, psychological variables, and SCBES scores. As expected, gender (female) and a higher BMI were the significant risk factors associated with binge-eating behaviors.2,47 Furthermore, our data also revealed a significant relationship between higher levels of depression and anxiety symptoms, as well as increased impulsivity traits, with higher SCBES total scores. This further supports the current understanding that BED often co-occurs with mental health conditions such as mood disorders, anxiety disorders, and impulse control disorders.48 By contrast, a higher level of self-control was associated with a lower SCBES score, indicating an important role of the prefrontal cortex-dependent cognitive control implicated in the development of BED, especially for the youths.49,50 More attention should be paid to these issues in the future.
Several limitations should also be noted. Firstly, our study had a cross-sectional design, which means that the findings could not establish a causal conclusion. Therefore, future follow-up studies are still necessary. Secondly, the sample primarily consisted of young adult college students from a single province in China; therefore, it may not represent the entire population accurately. Our findings of this study should be carefully explained and examined in other samples and cultures. Additionally, the participants were not diagnosed using the structured clinical interview, and all of the scales used in this study were self-reported tools. As a result, the potential presence of subjective bias may impact the findings. More objective and comprehensive measurements should be incorporated in future similar studies. Finally, although our study presented a relatively new three-factor model of the BES, it remains unclear whether this model can be generalized to clinical samples of BED or specific individuals with severe binge-eating problems. Further in-depth research is necessary to test its feasibility.
Conclusions
Our study findings suggested that the SCBES demonstrated sound psychometric properties and exhibited good cross-cultural adaptability in Chinese young adult college students. A novel three-factor model of this scale, which includes Binge-eating behaviors, Lack of control, and Negative affects related to overeating, demonstrated the best fit for the data. The SCBES appears to be an effective screening tool for identifying binge-eating issues among these Chinese youths.
Data Sharing Statement
Data could be obtained by contacting the corresponding author.
Ethics Approval and Informed Consent
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Human Research Ethics Committee of the Guizhou Medical University (2020LS05). Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors are thankful for all the participants in this study. We thank Dr Richard Tossell for his proofreading on our manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (Nos: 32060195 and 31560284) to Dr Wan-Sen Yan.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Keski-Rahkonen A. Epidemiology of binge eating disorder: prevalence, course, comorbidity, and risk factors. Curr Opin Psychiatry. 2021;34(6):525–531. doi:10.1097/YCO.0000000000000750
2. Giel KE, Bulik CM, Fernandez-Aranda F, et al. Binge eating disorder. Nat Rev Dis Primers. 2022;8(1):16. doi:10.1038/s41572-022-00344-y
3. Udo T, Grilo CM. Psychiatric and medical correlates of DSM-5 eating disorders in a nationally representative sample of adults in the United States. Int J Eat Disord. 2019;52(1):42–50. PMID: 30756422. doi:10.1002/eat.23004
4. Santomauro DF, Melen S, Mitchison D, Vos T, Whiteford H, Ferrari AJ. The hidden burden of eating disorders: an extension of estimates from the Global Burden of Disease Study 2019. Lancet Psychiatry. 2021;8(4):320–328. doi:10.1016/S2215-0366(21)00040-7
5. Qian J, Wu Y, Liu F, et al. An update on the prevalence of eating disorders in the general population: a systematic review and meta-analysis. Eat Weight Disord. 2022;27(2):415–428. doi:10.1007/s40519-021-01162-z
6. Kjeldbjerg ML, Clausen L. Prevalence of binge-eating disorder among children and adolescents: a systematic review and meta-analysis. Eur Child Adolesc Psychiatry. 2023;32(4):549–574. doi:10.1007/s00787-021-01850-2
7. Mangweth-Matzek B, Kummer KK, Hoek HW. Update on the epidemiology and treatment of eating disorders among older people. Curr Opin Psychiatry. 2023;36(6):405–411. doi:10.1097/YCO.0000000000000893
8. Udo T, Grilo CM. Prevalence and Correlates of DSM-5-Defined Eating Disorders in a Nationally Representative Sample of U.S. Adults. Biol Psychiatry. 2018;84(5):345–354. doi:10.1016/j.biopsych.2018.03.014
9. Lalonde JK, Pindyck LJ, et al. Binge eating disorder: a stable syndrome. Am J Psychiatry. 2006;163(12):2181–2183. doi:10.1176/ajp.2006.163.12.2181
10. Tsappis M, Freizinger M, Forman SF. Binge-eating disorder: emerging treatments for a new diagnosis. Curr Opin Pediatr. 2016;28(4):415–420. doi:10.1097/MOP.0000000000000367
11. Preti A, Girolamo GD, Vilagut G, et al.; ESEMeD-WMH Investigators. The epidemiology of eating disorders in six European countries: results of the ESEMeD-WMH project. J Psychiatr Res. 2009;43(14):1125–1132. doi:10.1016/j.jpsychires.2009.04.003
12. Ali K, Farrer L, Fassnacht DB, Gulliver A, Bauer S, Griffiths KM. Perceived barriers and facilitators towards help-seeking for eating disorders: a systematic review. Int J Eat Disord. 2017;50(1):9–21. doi:10.1002/eat.22598
13. Burton AL, Abbott MJ, Modini M, Touyz S. Psychometric evaluation of self-report measures of binge-eating symptoms and related psychopathology: a systematic review of the literature. Int J Eat Disord. 2016;49(2):123–140. doi:10.1002/eat.22453
14. Gormally J, Black S, Daston S, Rardin D. The assessment of binge eating severity among obese persons. Addict Behav. 1982;7(1):47–55. doi:10.1016/0306-4603(82)90024-7
15. Greeno CG, Marcus MD, Wing RR. Diagnosis of binge eating disorder: discrepancies between a questionnaire and clinical interview. Int J Eat Disord. 1995;17(2):153–160. doi:10.1002/1098-108x(199503)17:2<153::aid-eat2260170208>3.0.co;2-v
16. Ricca V, Mannucci E, Moretti S, et al. Screening for binge eating disorder in obese outpatients. Compr Psychiatry. 2000;41(2):111–115. doi:10.1016/s0010-440x(00)90143-3
17. Marcus MD, Wing RR, Hopkins J. Obese binge eaters: affect, cognitions, and response to behavioural weight control. J Consult Clin Psychol. 1988;56(3):433–439. doi:10.1037//0022-006x.56.3.433
18. Timmerman GM. Binge eating scale: further assessment of validity and reliability. J Appl Biobehav Res. 1999;4(1):1–12. doi:10.1111/j.1751-9861.1999.tb00051.x
19. Escrivá-Martínez T, Galiana L, Rodríguez-Arias M, Baños RM. The binge eating scale: structural equation competitive models, invariance measurement between sexes, and relationships with food addiction, impulsivity, binge drinking, and body mass index. Front Psychol. 2019;10:530. doi:10.3389/fpsyg.2019.00530
20. Duarte C, Pinto-Gouveia J, Ferreira C. Expanding binge eating assessment: validity and screening value of the Binge Eating Scale in women from the general population. Eat Behav. 2015;18:41–47. doi:10.1016/j.eatbeh.2015.03.007
21. Meule A. The psychology of overeating: food and the culture of consumerism. Food Culture Soc. 2016;19(4):735–736. doi:10.1080/15528014.2016.1235839
22. Pike KM, Hoek HW, Dunne PE. Cultural trends and eating disorders. Curr Opin Psychiatry. 2014;27(6):436–442. doi:10.1097/YCO.0000000000000100
23. He J, Zhu H, Wu S, et al. Binge eating and health-related quality of life in overweight and obese adolescents. Chin J Clin Psychol. 2014;22(4):635–637. doi:10.16128/j.cnki.1005-3611.2014.04.015
24. Yan WS, Zhang RR, Lan Y, Li ZM, Li YH. Questionnaire-based maladaptive decision-coping patterns involved in binge eating among 1013 college students. Front Psychol. 2018;9:609. doi:10.3389/fpsyg.2018.00609
25. Wu S, He J, Cai T. Validation of the binge eating scale in a sample of Chinese adolescents. J Neurosci Mental Health. 2019;19(3):273–276. doi:10.3969/j.issn.1009-6574.2019.03.013
26. Yan WS, Zheng DH, Liu MM. Trait impulsivity and choice impulsivity in young adult students with probable binge eating disorder. Front Psychiatry. 2022;13:838700. doi:10.3389/fpsyt.2022.838700
27. Yan J, Su H, Li C. Effect of body dissatisfaction on binge eating behavior of Chinese university students: a moderated mediation model. Front Psychol. 2022;13:995301. doi:10.3389/fpsyg.2022.995301
28. Yan HY, Lin FG, Tseng MM, Fang YL, Lin HR. The psychometric properties of Binge Eating Scale among overweight college students in Taiwan. J Eat Disord. 2023;11(1):47. doi:10.1186/s40337-023-00774-3
29. Yan HY, Liu CY, Tseng MM, Lee TY, Mu PF, Lin HR. Severity of binge eating behavior among overweight college students in Taiwan and associated factors. Healthcare. 2023;11(3):338. doi:10.3390/healthcare11030338
30. Dakanalis A, Colmegna F, Riva G, Clerici M. Validity and utility of the DSM-5 severity specifier for binge-eating disorder. Int J Eat Disord. 2017;50(8):917–923. doi:10.1002/eat.22696
31. Herman BK, Deal LS, DiBenedetti DB, Nelson L, Fehnel SE, Brown TM. Development of the 7-Item Binge-Eating Disorder Screener (BEDS-7). Prim Care Companion CNS Disord. 2016;18(2):25291. doi:10.4088/PCC.15m01896
32. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12:63–70. doi:10.1001/archpsyc.1965.01720310065008
33. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
34. Hofmann W, Friese M, Strack F. Impulse and Self-Control From a Dual-Systems Perspective. Perspect Psychol Sci. 2009;4(2):162–176. doi:10.1111/j.1745-6924.2009.01116.x
35. Yang C, Zhou Y, Cao Q, Xia M, An J. The relationship between self-control and self-efficacy among patients with substance use disorders: resilience and self-esteem as mediators. Front Psychiatry. 2019;10:388. doi:10.3389/fpsyt.2019.00388
36. Gonzalez R, Griffin D. Testing parameters in structural equation modeling: every ”one” matters. Psychol Methods. 2001;6(3):258–269. doi:10.1037/1082-989x.6.3.258
37. Treasure J, Hübel C, Himmerich H. The evolving epidemiology and differential etiopathogenesis of eating disorders: implications for prevention and treatment. World Psychiatry. 2022;21(1):147–148. doi:10.1002/wps.20935
38. Imperatori C, Innamorati M, Lamis DA, et al. Factor structure of the binge eating scale in a large sample of obese and overweight patients attending low energy diet therapy. Eur Eat Disord Rev. 2016;24(2):174–178. doi:10.1002/erv.2384
39. Brunault P, Gaillard P, Ballon N, et al. Validation of the French version of the Binge Eating Scale: examination of its factor structure, internal consistency and construct validity in a non-clinical and a clinical population. Encephale. 2016;42(5):426–433. doi:10.1016/j.encep.2016.02.009
40. Robert SA, Rohana AG, Suehazlyn Z, Maniam T, Azhar SS, Azmi KN. The validation of the Malay version of binge eating scale: a comparison with the structured clinical interview for the DSM-IV. J Eat Disord. 2013;1:28. doi:10.1186/2050-2974-1-28
41. Zeidan RK, Haddad C, Hallit R, et al. Validation of the Arabic version of the binge eating scale and correlates of binge eating disorder among a sample of the Lebanese population. J Eat Disord. 2019;7:40. doi:10.1186/s40337-019-0270-2
42. Hood MM, Grupski AE, Hall BJ, Ivan I, Corsica J. Factor structure and predictive utility of the Binge Eating Scale in bariatric surgery candidates. Surg Obes Relat Dis. 2013;9(6):942–948. doi:10.1016/j.soard.2012.06.013
43. Marek RJ, Tarescavage AM, Ben-Porath YS, Ashton K, Heinberg LJ. Replication and evaluation of a proposed two-factor Binge Eating Scale (BES) structure in a sample of bariatric surgery candidates. Surg Obes Relat Dis. 2015;11(3):659–665. doi:10.1016/j.soard.2014.09.015
44. Colles SL, Dixon JB, O’Brien PE. Loss of control is central to psychological disturbance associated with binge eating disorder. Obesity. 2008;16(3):608–614. doi:10.1038/oby.2007.99
45. Caldiroli A, La Tegola D, Manzo F, et al. The impact of the COVID-19 pandemic on Binge Eating Disorder: a systematic review. Nutrients. 2023;15(17):3777. doi:10.3390/nu15173777
46. Mina A, Hallit S, Rogoza R, Obeid S, Soufia M. Binge eating behavior in a sample of Lebanese Adolescents: correlates and Binge Eating Scale validation. J Eat Disord. 2021;9(1):134. doi:10.1186/s40337-021-00493-7
47. Olsen EM, Koch SV, Skovgaard AM, Strandberg-Larsen K. Self-reported symptoms of binge-eating disorder among adolescents in a community-based Danish cohort-A study of prevalence, correlates, and impact. Int J Eat Disord. 2021;54(4):492–505. doi:10.1002/eat.23458
48. Citrome L. Binge eating disorder revisited: what’s new, what’s different, what’s next. CNS Spectr. 2019;24(S1):4–13. doi:10.1017/S1092852919001032
49. Yan WS, Liu MM, Liu SJ. A behavioral and event-related potentials study of food-related inhibitory control in probable binge eating disorder. Psychol Res Behav Manag. 2023;16:4737–4748. doi:10.2147/PRBM.S441949
50. Carr MM, Wiedemann AA, Macdonald-Gagnon G, Potenza MN. Impulsivity and compulsivity in binge eating disorder: a systematic review of behavioral studies. Prog Neuropsychopharmacol Biol Psychiatry. 2021;110:110318. doi:10.1016/j.pnpbp.2021.110318
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.