Back to Journals » International Journal of Women's Health » Volume 14
Vaginal Infections’ Etiologies in South-Eastern Gabon – An Overview
Authors Bignoumba M ![]() , Mbombe Moghoa KH, Muandze-Nzambe JU
, Mbombe Moghoa KH, Muandze-Nzambe JU ![]() , Kassa Kassa RF, Mouanga Ndzime Y, Gafou A, Longo Pendy NM, Onanga R
, Kassa Kassa RF, Mouanga Ndzime Y, Gafou A, Longo Pendy NM, Onanga R ![]() , Kumulungui BS
, Kumulungui BS
Received 23 November 2021
Accepted for publication 23 February 2022
Published 12 April 2022 Volume 2022:14 Pages 505—515
DOI https://doi.org/10.2147/IJWH.S349754
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Michelle Bignoumba,1,2 Kelly H Mbombe Moghoa,1,3 Jean Ulrich Muandze-Nzambe,1,4 Roland Fabrice Kassa Kassa,1 Yann Mouanga Ndzime,1 Amahani Gafou,1 Neil Michel Longo Pendy,3 Richard Onanga,1 Brice Serge Kumulungui1,2
1Medical Analysis Research Unit (URAM)/Bacteriology, International Center for Medical Research (CIRMF), Franceville, BP 769, Gabon; 2Doctoral School of Science and Technology, Masuku University of Science and Technology (USTM), Franceville, BP 067, Gabon; 3Central African Regional Doctoral School in Tropical Infectiology (ECODRAC), Masuku University of Science and Technology (USTM), Franceville, BP 876, Gabon; 4Laboratory of Biochemistry and Applied Immunology (LABIA), Department de Biochimie-Microbiologie, Joseph KI-ZERBO University, Ouagadougou 03, 03 BP 7021, Burkina Faso
Correspondence: Michelle Bignoumba, Tel +24162521247, Email [email protected]
Introduction: Discomfort in women of childbearing age associated with vaginal infections, namely bacterial vaginosis (BV), aerobic vaginitis (AV), vulvovaginal candidiasis (VVC), and trichomoniasis (TV), represent a serious and ongoing gynecological complication throughout the world.
Objective: This study aimed to investigate the etiologies of vaginal infections among outpatients in south-eastern Gabon.
Methodology: A cross-sectional study was designed using participants referred directly by their treating doctor for a vaginal swab. Socio-demographic data were collected using a structured questionnaire. Microscopic examinations were used for TV and BV diagnostic. All vaginal swabs were cultured for AV and VVC isolates using standard microbiology methods.
Results: A total of 573 women of reproductive age participated in the study. The most common identified vaginal infections were BV (62.8%) and AV (51.1%) followed by VVC (34.1%). No significant difference was observed for each etiology compared to socio-demographic data. Streptococcus B (23.9%), Staphylococcus aureus (17.7%), Klebsiella spp. (11.6%), and E. coli (5.8%) were the bacteria most associated with AV. A high incidence of non-C. albicans Candida (NCAC) strains causing vulvovaginitis were found. The prevalence of TV (2.1%) was low. Mixed infections had been common among participants. No association was found with TV and other vaginal infections, unlike others studies. The present study identified BV 228 (83.5%) and AV 227 (83.2%) as the main cause of mixed infections. The mixed infection AV-BV 113 (41.4%) was the most represented.
Conclusion: Also that simultaneous AV-BV-VVC represented 69 (25.3%) of mixed infections. Molecular analyses would be needed to identify the key species commonly associated with these vaginal infections.
Keywords: bacterial vaginosis, aerobic vaginitis, vulvovaginal candidiasis, trichomonal vaginitis, vaginitis
Introduction
In healthy women, the vaginal mucosa is covered by a complex microflora dominated by lactobacilli.1 The balance of this ecosystem is essential because it constitutes the main element of defense against genital infections. Some forms of vaginal infections have been well defined to date, namely Bacterial Vaginosis (BV); VulVovaginal Candidiasis (VVC), and Trichomoniasis (TV).2 In the meantime, the term Aerobic Vaginitis (AV) was described for the first time by Donders et al (2002) to meet the need to describe another condition of vaginal dysbiosis.3 These infections would be responsible for as many as 50% of all gynecologic visits and represent a major contributor to health care expenses.4 According to some authors, BV and VVC during pregnancy would increase the risk of preterm birth and miscarriage. While TV and AV can increase the transmission of human immunodeficiency virus, VVC, or other sexually transmitted infections.5 Some studies suggest a variety of risk factors. Ethnicity and geographical location would influence the prevalence of vaginal infections. Several authors reported different inventory of the situation about vaginal’s pathobionts, namely in Asia, Europe, Africa, and Latin America.6–8 As for Sub-Saharan Africa, Kenyon et al reported a higher prevalence of BV than other parts.9 Sub-Saharan African women may therefore be less protected from vaginal dysbiosis.10 Given the specificity of women’s vaginal microbiota from one region to another, it would be interesting to assess vaginal infection in Gabon, a tropical equatorial country. Also, the semiological approach used by medical practitioners often fails due to the absence or lack of symptoms specificity.11 Few studies reported in Gabon to date are limited either by the limitations of the diagnostic techniques12 or by the size13 and the type of sampling.14,15 In this study, existing data were completed and would allow for a better understanding of microbial dysbiosis in the vagina to help improve the care of women in tropical countries.
Materials and Methods
Study Area
Our study was conducted at CIRMF (Centre Interdisciplinaires de Recherche Médicales de Franceville). This center is a sentinel in terms of public health. The CIRMF is located in Franceville, Haut-Ogooué province’s administrative center from southeastern Gabon. This province is the second most populous in Gabon and borders the Republic of Congo.
Design and Subject Selection
Over one year period, between June 2019 and 2020, a cross-sectional study was designed. Women who agreed to participate in this study had been referred by a general practitioner to the Laboratoire d’Analyses Médicale (LAM) at the CIRMF for vaginal sampling. All participants reported different vaginal abnormalities.
All socio-cultural and demographic information on the patients was collected by following a set of tailored questions. The survey questionnaire was organized in separate sections to obtain information on age, employment status, marital status, symptoms, and contraceptive use. The study led according to inclusion and exclusion criteria. The inclusion criteria were defined as follows: (1) outpatients with vaginal complaints referred by a local general practitioner (2) outpatients with voluntary consent; (3) outpatients of reproductive age; and (4) outpatients who had been menstruating for at least 2 days and had not had sexual intercourse in the 2 days before sample collection. The exclusion criteria were defined as follows: (1) outpatients under the legal age and (2) outpatients with clinically apparent herpes simplex infection. These selected variables were based on the literature.4,6,7,16–20
Ethical Considerations
Female participants were recruited to our study set, after having read and signed individually the informed consent or from their parents or legal representatives. To ensure confidentiality, numbers were assigned to participants via their survey sheets and then plotted on the corresponding samples. Once the diagnosis is done, the results of all participants were transmitted with strict anonymity. This study was conducted in accordance with the Declaration of Helsinki.
Laboratory Processing
Once the form was completed, sampling through the vaginal route were performed for each woman. Vaginal swabs were taken using ESwab Collection. Transport System (Copan Diagnostics, Inc., Brescia, Italy) were used to prepare the smear for microscopic examination of the vaginal microbiota and inoculation onto agar plates. The comparison of microscopic observations and cultures was used for the isolates identification. Swabs collected were transported and delivered immediately for analysis. Vaginal swabs were used to prepare smears on clean, grease-free slides. The Gram and MGG staining were used for diagnostic. The Gram-stained smear was used to assess the intensity of a possible imbalance in the vaginal microbiota based on Nugent score, gold-standard method diagnostic.21 Slides were read according to Nugent’s score as described by the authors in their study.22 A score in the range 0–3 indicated normal flora, 4–6 indicated mixed vaginal flora, which is not constituted BV, and 7–10 was constituted of BV.23,24 The smear stained with MGG made it possible to observe the presence of inflammatory cells, to identify Trichomonas vaginalis and the presence of yeasts or pseudomycelium.
Isolation and Identification of Microorganisms
Microbiological analyses were performed according to standard procedures of clinical laboratory to characterize pathogenic microorganisms. Different culture media were used for the microbiological investigations. Briefly, blood and chocolate agar were used as a general non-selective medium, Columbia CNA + 5% Sheep Blood agar (bioMérieux, France) for Gram-positives bacteria, BCP dextrose agar (BIOKAR Diagnostics, France) for bacilles gram-negative and SAB-CHL agar (Sabouraud chloramphenicol, bioMérieux, France) for presumptive Candida spp.
All characteristic colonies isolated were identified by the VITECK 2 compact (VITEK-2 automatique système, bioMérieux, France). The VITEK is an automated biochemical system that enabled the fast and accurate identification of medically relevant yeasts via fluorescence technology.25 It allows the fast and accurate identification of medically relevant yeasts to species level via fluorescence technology. Briefly, the inocula in the VITEK 2 use were prepared in sterile saline to a turbidity equal respectively to 0.5 and 2.0 McFarland standard for bacteria and yeast according to a densitometer (DensiChek instrument, bioMérieux, France). Each standardized inoculum suspension was placed into a VITEK 2 cassette, namely VITEK 2 GN for Gram-Negative organisms’ inoculum, VITEK 2 GP for Gram-Positive organisms’ inoculum, and VITEK 2 YST for yeast or yeast-like organisms’ inoculum, along with a sterile polystyrene test tube. The cassettes were placed in the VITEK 2 instrument and the respective microbial suspensions were diluted appropriately. Then, the cards were filled, incubated, and read automatically by the VITEK 2. The time of incubation varied from 10 to 30 h based on the growth rate in the free control well.
Data Analysis
Data were entered into Microsoft Excel 2016 and exported into the statistical software R version 4.0.2 for data analyses. Descriptive statistics such as percentages were carried out. Percent prevalence was determined by multiplying the number of the positive sample by 100 and dividing by the total samples number. Comparison of genital infection etiology between age group, employed status, marital status, symptoms, and contraceptive use was determined using the X2 test. The statistical level of significance was considered at p≤0.05. Venn diagrams were generated using InteractiVenn.26 A generalized linear model was made using the function GLM of the package stats version 3.6.2. and the step function of the MuMin package was used to select the best model
Results
Characteristics of Study Participants
Microscopic examination characteristics of the most common vaginal infections microbiomes in the outpatient cohort from this study have been outlined. A total of 573 participants with vaginal discomforts have been involved in the study.
Table 1 shows the socio-demographic characteristics of women screened through this study for the period. These outpatient has been divided into four groups for age. The first group with an age range of 12–15 years comprised 1.4% of the patients; the second group with an age range of 16–30 years 40.0%; the third group with an age range of 31–45 years 44.3%; and the last group representing patients over 46 years constituted 7.1% of the patients. Most of them were symptomatic 478 (83.4%). Also, 189 (33%) of them had used a means of contraception. A proportion of 39.1% of patients lived with a person in an unmarried cohabiting relationship. Furthermore, a large number of participants (37.3%) reported having a job. Regarding the learners, the majority 80 (14%) had a secondary education level (Table 1).
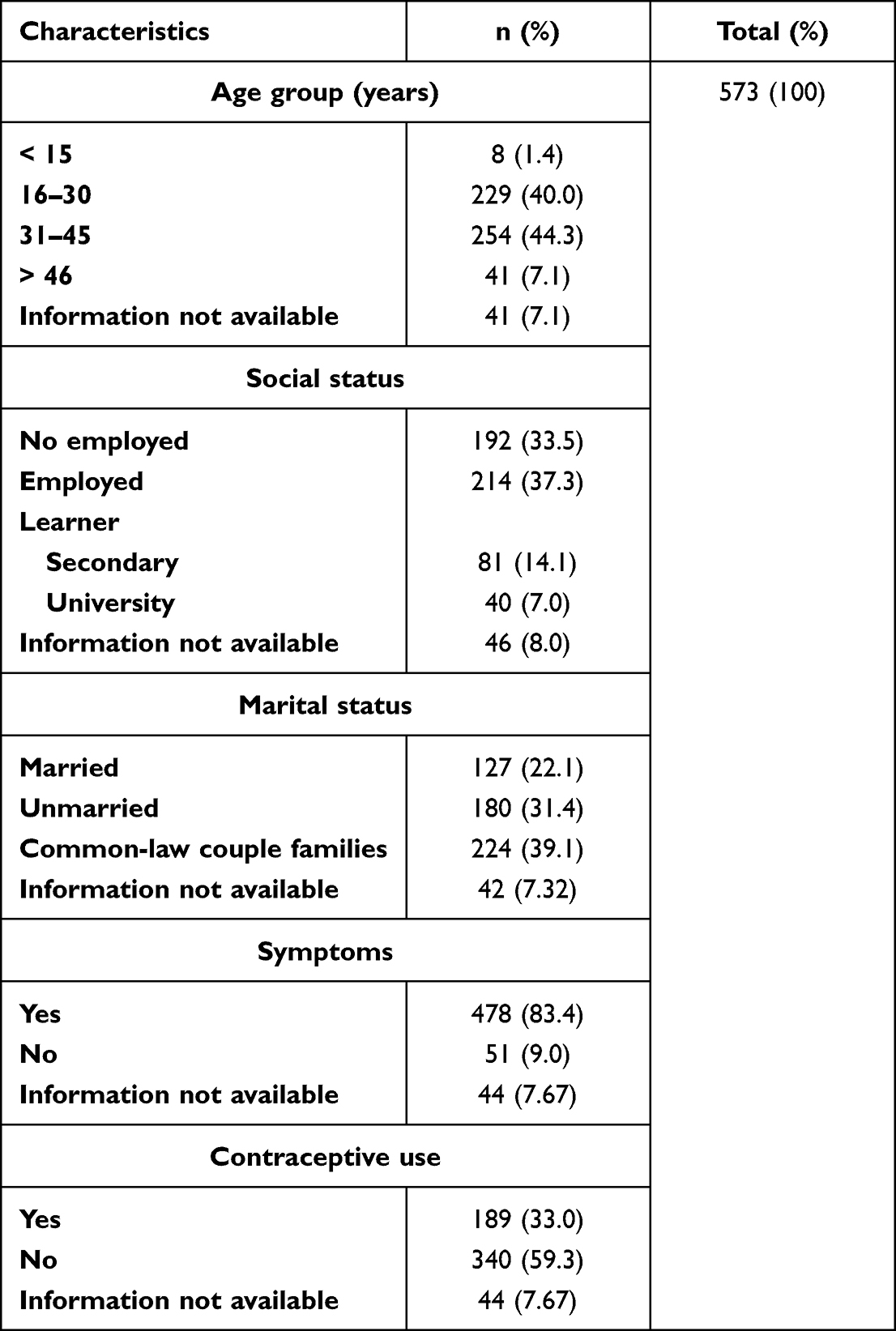 |
Table 1 Overview of Socio-Cultural and Demographic Characteristics on Outpatients |
Etiology of Vaginal Infections
Figure 1 shows most of the microscopic characteristics found among abnormal microbiomes namely “clue cells” which illustrate suspected BV microbes; “pseudofilaments” which illustrate suspected VVC microbes; “clue cell-associated pseudofilaments” indicating mixed infection, and trichomonas-like microbes.
 |
Figure 1 Microscopic examination characteristics of most common infectious vaginal microbiomes (1000 X) legend: (A) clues cells; (B) pseudofilament; (C) pseudofilament associate with clues cells; (D) Trichomonas infections. |
The study reveals that BV 360 (62.8%) is the most involved infectious etiology of vaginal infections in patients. Other infectious etiologies were detected, namely AV 293 (51.1%), VVC 195 (34.1%), and TV 12 (2.1%). Data obtained from this research reveal variability in mixed infections. The distribution of infectious vaginitis etiologies is shown in Table 2. Yet no mixed infectious etiologies with TV have been found in this study. As the Table 3 illustrates, Candida albicans also observed in microscopy (Figure 1A) was the predominant species 128 (65.7), the NCAC species were Candida famata 26 (13.33%), Candida glabrata 23 (11.79%), Candida krusei 8 (4.1%), Candida tropicalis 5 (2.56%), Candida parapsilosis 3 (1.53%), Candida dubliniensis 3 (1.53%) and Candida guillermondis1 (0.51%). As regards AV-like infections, outpatients were colonized by Staphylococcus aureus 52 (17.7), of Streptococcus B 70 (23.9), E. coli 17 (5.8), Klebsiella spp 34 (11.6) and other bacteria species 120 (41.0).
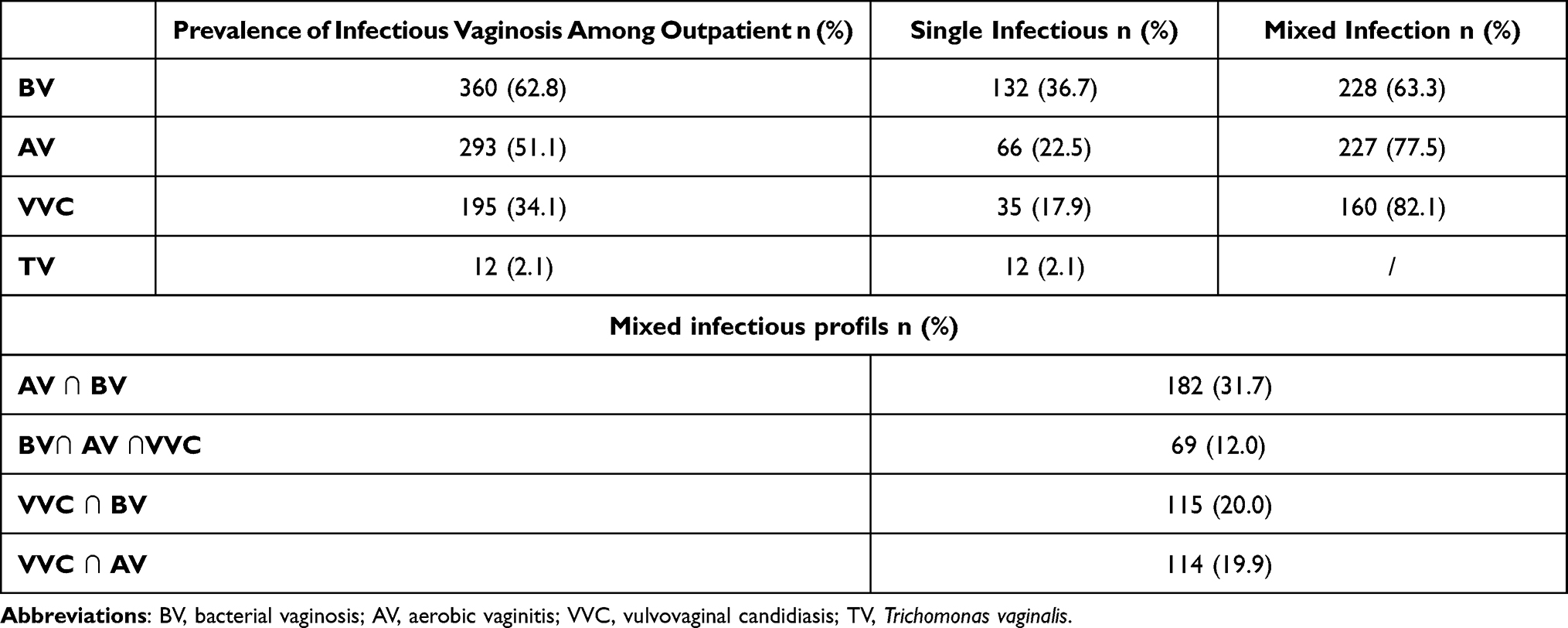 |
Table 2 Occurrence of the Different Infectious Vaginosis Among Outpatient |
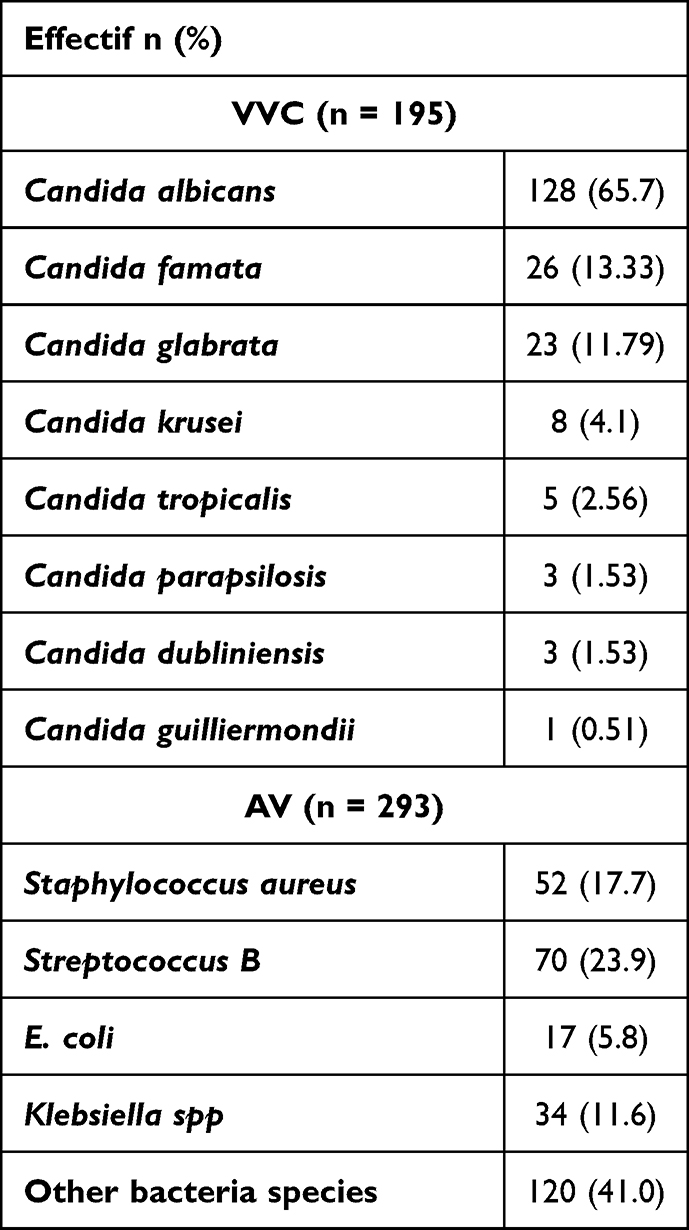 |
Table 3 Occurence of Microorganism for VVC-Like Infections and AV-Like Infections |
Figure 1 Shows most of the microscopic characteristics found among abnormal microbiomes such as clues cells that illustrate a suspicion BV-like microbes; pseudofilament that illustrate a suspicion VVC-like microbes; pseudofilament associate with clues cells indicate mixed infection and trichomonas-like microbes occurrences.
The occurrences of single and mixed infections within the framework of vaginal infections were illustrated in the Venn diagram (Figure 2). According to the GLM model, there is a statistically significant association between BV and vaginal infection in south-eastern Gabon outpatients (p˂0.0001).
 |
Figure 2 Mapping the distribution of vaginal infections among outpatients. The ellipses illustrate the number of vaginal infectious etiologies, whether exclusive or mixed. |
Table 4 sets out the distribution of each infectious etiology related to outpatients’ socio-demographic data and risk factors. No significant difference was observed for each etiology compared to the outpatient’s age group, employed status, marital status, symptoms, and contraceptive use.
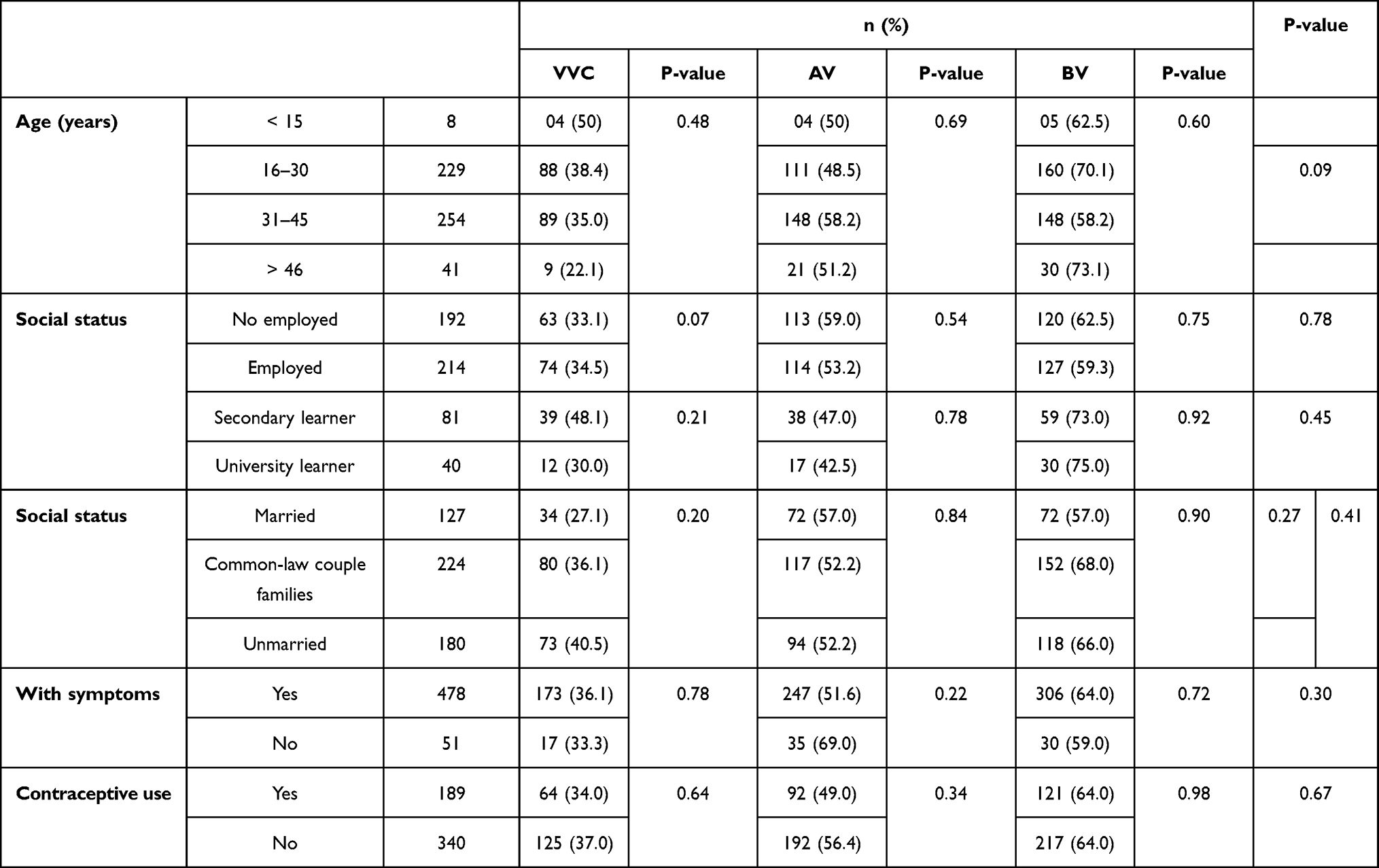 |
Table 4 Disribution of Each Infectuous Etiology Related to Outpatients’ Socio-Demographic Data and Risk Factors |
Discussion
The most common causes of vaginal infections among reproductive women are usually associated with infectious diseases, namely BV, VVC, AV, and TV.1–3 The diagnosis is often made based on the symptoms and the physical examination results or the biological tests carried out in the office or the laboratory.27 Microbiological analyses of vaginal swabs were systematically carried from women after healthcare providers’ examination as described.28 Once the infection profile was determined, we looked for close relationships between several socio-demographic elements of the outpatients and the vaginal infections. In the study, the socio-demographic data provide various information including an overview of the context (Table 1). Franceville is a town in the southeast of Gabon, a semi-urban area in a developing country that has the particularity of being located in the heart of the African inter-tropical forest. Table 4 sets out the distribution of each infectious etiology related to outpatients’ socio-demographic data and risk factors. No significant difference was observed for each etiology compared to the outpatient’s age group, employed status, marital status, symptoms, and contraceptive use.
Our study represents the BV as the most frequent vaginal infection (63.1%) (Table 2) in south-eastern Gabon outpatients. Despite some kind of standardization by using the Nugent score that is considered as the gold standard for BV diagnosis,29 the BV prevalence varies internationally.9,30,31 However, our results are in line with the study of Bruins et al which presents the BV-like infections with the highest prevalence in women from the Netherlands.32 Similar results were also found in Yemen and Ethiopia.2,33 In our study, no statistically significant difference was found between different vaginal infections and outpatient age groups, employed status, marital status, symptoms, and contraceptive use. In some countries,2,32,33 religion, age, living in a rural area, and having lower abdominal pain was significantly associated with bacterial vaginosis. These Varying prevalence could be due to multiple factors, including socio-demographic characteristics, immune status of patients, treating patients with broad-spectrum antibiotics and immune suppressive drugs, and hormonal influences, etc.34 Also, the bad practice in terms of sanitary napkins use with the accumulation of menstrual blood could contribute to the vaginal ecosystem’s enhancements.16,35 Another important but obvious point would be the involvement of the women’s ethnicity and body hormone level in the diversity of the vaginal microbial community. It has been shown that the decrease in estrogen levels would imply the maintenance of the vaginal pH neutrality which would be at the origin of the vaginal microbiota destabilization.36 Furthermore, current literature suggests that the decrease in estrogen that would be associate with an elevation of the vaginal pH a few hours after coitus would increase the adhesion of Gardnerella vaginalis to the epithelial cells of the mucosa while simultaneously replacing the lactobacilli from their attachment sites on this same mucosa.37 Although Nugent score’s techniques are highly sensitive and specific for evaluating an imbalance of the vaginal microbiota,21 they are not sensitive to characterize the composition of the vaginal microbiota.29 Without losing sight of all these complexities, it would be interesting to characterize the microbiota present in the vaginal epithelium of women in south-eastern Gabon using molecular analysis to better understand these infectious diseases.
In the present study, VVC-like infections among reproductive-age women were 195 (34.1%). Another study, made in the same population for VVC-like infections have revealed a 28.52% occurrence.38 In the Southeast Asia context -and more specifically Vietnam, an equatorial forest country like Gabon, Do Ngoc Anh et al reported a very high VVC-like infections prevalence in 51.3% of patients with signs and symptoms of vaginal infection.34 Our results are of the same order as the prevalence rates found in Congo Brazzaville, a neighboring country of the study area.19 Microbial culture-based techniques and automated identification were used in this study have allowed us to identify responsible VVC Candida spp. which were distributed as follows (Table 3): Candida albicans 65.7%; Candida famata 13.33%; Candida glabrata 11.79%; Candida krusei 4.1%; Candida tropicalis 2.56%; Candida parapsilosis 1.53%; Candida dubliniensis 1.53% and Candida guilliermondii 0.51%. Our findings show a high incidence of Non-C. albicans Candida (NCAC) strains causing vulvovaginitis in the study population. This contrasts with the results described in the literature. Traditionally, Candida albicans is responsible for 85–95% of vaginal Candida infections.34,39 In the same population over the different periods, Ndong Atome et al and Bignoumba et al found Candida albicans at 93.77% then 82.73%, and NCAC at 6.22% and then 17.27% in patients with VVC.12,17 Indeed, this data may sound alarming. Thus, extensive surveillance studies of changes in species distribution should be routinely screened to improve patient care and effective management. In the Figure 1C we have observed the pseudofilament which is characteristic of Candida albicans. Candida albicans is a dimorphic fungus which has the ability to switch between yeast and hyphal growth forms (dimorphism) C. albicans yeast-to-hypha transition occurs in response to various signals such as temperature (37°C) presence of serum, physiological CO2 concentration, neutral or alkaline pH, nutrient limitation and presence of amino acids. Several studies have linked the switch from yeast to hyphal form with pathogenicity.40,41
In this research, aerobic bacteria play a significant role in the etiology of vaginal infections. AV-like infections with an occurrence of 51.1% were more commonly observed than VVC-like infections. However, the prevalence of AV-like infections was less prevalent than BV-like infections. According to Donders et al, it is a clinical entity quite distinct from bacterial vaginosis and causes a significant host response.3 Despite a late description, on this date, AV is better evaluated. Many recent publications allow a better understanding of it.37 Compared to the finding of the present study, a similar prevalence (51.0%) was reported for AV among examinees women with signs of vaginitis in Bosnia and Herzegovina.4 Recently, Salinas et al found among Ecuadorian women that had a vulvovaginitis infection AV as the main diagnosed vaginal infection (51.6%), followed by BV (24.2%) and finally VVC (7.4%).6 A high AV prevalence has been postponed in China (65.49%) among sexually active patients who underwent routine gynecological examination.18 AV is a common form of vaginal infection that is distinguished from BV. The microflora in AV comprises commensal aerobic microorganisms of intestinal and mucosa origin (Table 3), principally Escherichia coli, Staphylococcus aureus, and Staphylococci.3,5,18 Data from our work on outpatients in south-eastern Gabon show that Streptococcus B (23.9%), Staphylococcus aureus (17.7%), Klebsiella spp. (11.6%), and E. coli (5.8%) as the bacteria most associated with AV. A report in Gabon had shown Streptococcus agalactiae isolates colonizing pregnant women with serotype distribution in line with other reports from Africa.14 In a country close to Gabon, namely Cameroon, the distribution of AV was as follows: Staphylococcus spp. 8.82%; Streptococcus spp. 1.96% and Enterobacteria 11.78%.20 AV-like infections are easily mixed with other pathogens, especially with BV, VVC, or TV.8
A low prevalence of TV was found in our study. We were able to observe under microscopy (Figure 1D) a trichomonas among this low rate observed. Also notable was that the lack of diagnostic technique sensitivity used in our study may explain these low TV-like infections rates. According to Abdul Aziz et al relying on microscopic examination for the diagnosis of TV could underestimate the prevalence of the infection, and the use of more sensitive techniques is recommended.2 However, we did not find an association with TV, unlike other studies where the mixed infections between TV, VVC, or BV were found to be 0.1; 0.3%; 25%, and 30% respectively in Cameroun, Yemen, China, and Bosnia and Herzegovina.2,4,8 While mixed infections had been very common in this study among outpatient (Figure 2). AV-like infections and VVC-like infections with respectively 227 (77.5) and 160 (82.1) were most involved in mixed infections. About BV-like infections, single infections (31.9%) were also less frequent than mixed infections (68.1%). The results contradict the Jahic et al and Zhang et al studies that found fewer mixed infections than single infection.4,18 The present study identified BV 228 (83.5%) as the main cause of mixed infections (Table 2). Although, AV 227 (83.2%) is also a key component of mixed infections, no statistically significant association was found between AV and vaginal infections in our population set according to the GLM model (p˃0.05). However, there is a statistically significant association between BV and vaginal infections (p˂0.0001). This observation confirms that when the vaginal ecosystem is disturbed, the vaginal epithelium is less protected and vaginal infections would set in.6 According to others studies, AV is more commonly associated with BV.3,4,18 Therefore, the absence of lactobacilli would be an AV characteristic.4 More generally, BV would represent a common cause of disturbance in the normal vaginal flora in favor of the agents in vaginal infections.32 It is important to mention that the 69 participants had been simultaneously diagnosed with BV, AV, and VVC in the study. As reported by Salinas et al and many authors, several sexual partners could represent a risk factor.6 Further analysis would be done in the population set to identify the main key species commonly associated with each mixed infection.
Conclusions
This research indicates a polymicrobial etiology of vaginitis in south-eastern Gabon. The most frequently identified vaginal infections were BV and AV, followed by VVC, while the TV was very low. Mixed infections were found in many of these women of reproductive age. Data show a statistically significant association between BV and vaginal infection in south-eastern Gabon outpatients (p˂0.0001). Further studies should be conducted in the monitoring of vaginal infections among women. BV and AV infections are known to be one of the main causes of frequent antibiotic use in women. A limitation of this study is the data’s lack about the antibiotic susceptibility of diverse etiologies. It would undoubtedly be useful the level of antibiotic resistance in vaginal isolates. The use of molecular tools could allow us to assess the colonization status of different microbial taxa and thus identify the species present in the vaginal microbiota with greater reliability among women from south-eastern Gabon. These molecular tools could lead to improved knowledge of the vaginal microbiota of women in south-eastern Gabon, which could result in the development of new context-specific therapeutic approaches such as the use of probiotics.
Ethical Considerations and Consent to Participate
The study protocol was reviewed and approved by the Ethics Committee of CIRMF. The female participants were recruited to our study set, after having read and signed individually the informed consent or from their parents or legal representatives. To ensure confidentiality, numbers were assigned to participants via their survey sheets and then plotted on the corresponding samples. Once the diagnosis is done, the results of all participants were transmitted with strict anonymity.
Acknowledgment
This work is a part of the Ph.D. thesis of the first author. We would thank URAM (Unité de Recherche en Analyse Médicale) of CIRMF (Centre International de Recherches Médicales de Franceville), for technical support and hosting this project. The CIRMF is funded by the Gabonese government, Total-Final-Elf Gabon and Ministère des Affaires Etrangères, France.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest.
References
1. Ling Z, Liu X, Luo Y, et al. Associations between vaginal pathogenic community and bacterial vaginosis in Chinese reproductive-age women. PLoS One. 2013;8(10):e76589. doi:10.1371/journal.pone.0076589
2. Abdul-Aziz M, Mahdy MAK, Abdul-Ghani R, et al. Bacterial vaginosis, vulvovaginal candidiasis and trichomonal vaginitis among reproductive-aged women seeking primary healthcare in Sana’a city, Yemen. BMC Infect Dis. 2019;19(1):879. doi:10.1186/s12879-019-4549-3
3. Donders GG, Vereecken A, Bosmans E, Dekeersmaecker A, Salembier G, Spitz B. Definition of a type of abnormal vaginal flora that is distinct from bacterial vaginosis: aerobic vaginitis. BJOG. 2002;109(1):34–43. doi:10.1111/j.1471-0528.2002.00432.x
4. Jahic M, Mulavdic M, Nurkic J, Jahic E, Nurkic M. Clinical characteristics of aerobic vaginitis and its association to vaginal candidiasis, trichomonas vaginitis and bacterial vaginosis. Med Arch. 2013;67(6):428–430. doi:10.5455/medarh.2013.67.428-430
5. Donders GGG, Bellen G, Grinceviciene S, Ruban K, Vieira-Baptista P. Aerobic vaginitis: no longer a stranger. Res Microbiol. 2017;168(9–10):845–858. doi:10.1016/j.resmic.2017.04.004
6. Salinas AM, Osorio VG, Pacha-Herrera D, Vivanco JS, Trueba AF, Machado A. Vaginal microbiota evaluation and prevalence of key pathogens in ecuadorian women: an epidemiologic analysis. Sci Rep. 2020;10(1):18358. doi:10.1038/s41598-020-74655-z
7. Juliana NCA, Suiters MJM, Al-Nasiry S, Morre SA, Peters RPH, Ambrosino E. The association between vaginal microbiota dysbiosis, bacterial vaginosis, and aerobic vaginitis, and adverse pregnancy outcomes of women living in sub-saharan Africa: a systematic review. Front Public Health. 2020;8:567885. doi:10.3389/fpubh.2020.567885
8. Fan AP, Xue FX. Clinical characteristics of aerobic vaginitis and its mixed infections. Zhonghua Fu Chan Ke Za Zhi. 2010;45(12):904–908.
9. Kenyon C, Colebunders R, Crucitt T. The global epidemiology of bacterial vaginosis: a systematic review. Am J Obstet Gynéco. 2013;209(6):505–523. doi:10.1016/j.ajog.2013.05.006
10. Jespers V, van de Wijgert J, Cools P, et al. The significance of Lactobacillus crispatus and L. vaginalis for vaginal health and the negative effect of recent sex: a cross-sectional descriptive study across groups of African women. BMC Infect Dis. 2015;15:115. doi:10.1186/s12879-015-0825-z
11. Jespers V, Kyongo J, Joseph S, et al. A longitudinal analysis of the vaginal microbiota and vaginal immune mediators in women from sub-Saharan Africa. Sci Rep. 2017;7(1):11974. doi:10.1038/s41598-017-12198-6
12. Ndong Atome GR, Sima Obiang C, Onanga R. Ecology of microbial germs of the urogenital tract in women in southeast Gabon. Int J Curr Res. 2017;9(12):63028–63032.
13. Lendamba RW, Onanga R, Bigoumba M, et al. Bacterial vaginosis:: prévalence in sexually active women living in the city of Franceville (Gabon) and its surroundings. J Women's Health. 2020;10:501–509.
14. Belard S, Toepfner N, Capan-Melser M, et al. Streptococcus agalactiae serotype distribution and antimicrobial susceptibility in pregnant women in Gabon, Central Africa. Sci Rep. 2015;5:17281. doi:10.1038/srep17281
15. Yvert F, Riou JY, Frost E, Ivanoff B, Ossari S, Bouatsia P. Gonococcal infections in Gabon (Haut-Ogooue). Pathol Biol. 1984;32(2):80–84.
16. Keane FE, Ison CA, Taylor-Robinson D. A longitudinal study of the vaginal flora over a menstrual cycle. Int J STD AIDS. 1997;8(8):489–494. doi:10.1258/0956462971920631
17. Fan A, Yue Y, Geng N, Zhang H, Wang Y, Xue F. Aerobic vaginitis and mixed infections: comparison of clinical and laboratory findings. Arch Gynecol Obstet. 2013;287(2):329–335. doi:10.1007/s00404-012-2571-4
18. Zhang T, Xue Y, Yue T, et al. Characteristics of aerobic vaginitis among women in Xi’an district: a hospital-based study. BMC Women's Health. 2020;20(1):138. doi:10.1186/s12905-020-00997-5
19. Potokoué Mpia NSB, Sékangué Obili G, Ossibi Ibara BR, et al. Vaginal candidiasis in women of childbearing age at the university hospital of Brazzaville: prevalence and associated factors. Microbiol Infect Dis. 2021;5(3):1–5.
20. Ngaba GP, Essomba EN, Kedy Koum C, Ndzengue L, Bika C, Adiogo D. profile of germs involved in cervicovaginal infections in women of childbearing age in the bonassama district hospital. Rev Med Pharmacy. 2014;4(1):400–408.
21. Nugent RP, Krohn MA, Hillier SL. Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J Clin Microbiol. 1991;29(2):297–301. doi:10.1128/jcm.29.2.297-301.1991
22. Bitew A, Mengist A, Belew H, Aschale Y, Reta A. The prevalence, antibiotic resistance pattern, and associated factors of bacterial vaginosis among women of the reproductive age group from felege hiwot referral hospital, Ethiopia. Infect Drug Resist. 2021;14:2685–2696. doi:10.2147/IDR.S305329
23. Hoffman MK, Bellad MB, Charantimath US, et al. A comparison of colorimetric assessment of vaginal ph with Nugent score for the detection of bacterial vaginosis. Infect Dis Obstet Gynecol. 2017;2017:1040984. doi:10.1155/2017/1040984
24. Mohanty SSS, Kapil A, Mittal S, Mittal S. Interobserver variation in the interpretation of Nugent scoring method for diagnosis of bacterial vaginosis. Indian J Med Res. 2010;131(1):88–91.
25. Kassim A, Pfluger V, Premji Z, Daubenberger C, Revathi G. Comparison of biomarker based matrix assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) and conventional methods in the identification of clinically relevant bacteria and yeast. BMC Microbiol. 2017;17(1):128. doi:10.1186/s12866-017-1037-z
26. Heberle H, Meirelles GV, da Silva FR, Telles GP, Minghim R. InteractiVenn: a web-based tool for the analysis of sets through venn diagrams. BMC Bioinform. 2015;16:169. doi:10.1186/s12859-015-0611-3
27. Paladine HL, Desai UA. Vaginitis: diagnosis and treatment. Am Fam Physician. 2018;97(5):321–329.
28. Hainer BL, Maria V, Gibson MV. Vaginitis: diagnosis and treatment. Am Fam Physician. 2011;83:7.
29. Oliveira LMA, Diniz CG, Fernandes AAS, et al. Assessment of vaginal microbiota in Brazilian women with and without bacterial vaginosis and comparison with Nugent score. J Infect Dev Ctries. 2018;12(2):127–136. doi:10.3855/jidc.9532
30. Peebles K, Velloza J, Balkus JE, McClelland RS, Barnabas RV. high global burden and costs of bacterial vaginosis: a systematic review and meta-analysis. Sex Transm Dis. 2019;46(5):304–311. doi:10.1097/OLQ.0000000000000972
31. Coudray MS, Madhivanan P. Bacterial vaginosis-A brief synopsis of the literature. Eur J Obstet Gynecol Reprod Biol. 2020;245:143–148. doi:10.1016/j.ejogrb.2019.12.035
32. Bruins MJ, Dos Santos CO, Damoiseaux R, Ruijs G. Bacterial agents in vulvovaginitis and vaginal discharge: a 10-year retrospective study in the Netherlands. Eur J Clin Microbiol Infect Dis. 2021;40:2123–2128. doi:10.1007/s10096-021-04265-8
33. Mulu W, Yimer M, Zenebe Y, Abera B. Common causes of vaginal infections and antibiotic susceptibility of aerobic bacterial isolates in women of reproductive age attending at felegehiwot referral hospital, Ethiopia: a cross sectional study. BMC Women's Health. 2015;15:42. doi:10.1186/s12905-015-0197-y
34. Faye-Kette YH, Kouassi AA, Sylla-Koko DF, et al. Prevalence of 4 agents of sexually transmitted diseases in leukorrhea In Abidjan (Ivory Coast). Bull Soc Pathol Exot. 1993;86(4):245–247.
35. Russo R, Karadja E, De Seta F. Evidence-based mixture containing Lactobacillus strains and lactoferrin to prevent recurrent bacterial vaginosis: a double blind, placebo controlled, randomised clinical trial. Benef Microbes. 2019;10(1):19–26. doi:10.3920/BM2018.0075
36. Barrientos-Duran A, Fuentes-Lopez A, de Salazar A, Plaza-Diaz J, Garcia F. Reviewing the composition of vaginal microbiota: inclusion of nutrition and probiotic factors in the maintenance of eubiosis. Nutrients. 2020;12:2. doi:10.3390/nu12020419
37. Lepagneur JP, Béné M, Viraben R, Bohbot J-M. La flore vaginale et ses troubles. [The vaginal flora and its disorders]. Edition ESKA; 2016: 152. French.
38. Bignoumba M, Onanga R, Bivigou Mboumba B, et al. Vulvovaginal candidiasis among symptomatic women of childbearing age attended at a Medical Analysis Laboratory in Franceville, Gabon. J Mycol Med. 2019;29(4):317–319. doi:10.1016/j.mycmed.2019.100895
39. Sobel JD. Vulvovaginal candidosis. Lancet. 2007;369(9577):1961–1971. doi:10.1016/S0140-6736(07)60917-9
40. Vediyappan G, Dumontet V, Pelissier F, d’Enfert C. Gymnemic acids inhibit hyphal growth and virulence in candida albicans.. PLoS One. 2013;8(9):e74189. doi:10.1371/journal.pone.0074189
41. Arkowitz RA, Bassilana M. Recent advances in understanding candida albicans hyphal growth. F1000Res. 2019;8:700. doi:10.12688/f1000research.18546.1
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.