Back to Journals » Infection and Drug Resistance » Volume 19
Vaginal Colonization by Streptococcus agalactiae Among Pregnant Women in Jordan: Antimicrobial Resistance, Virulence Genes, and Biofilm Formation
Authors Shakhatreh MAK, Atawneh FH, Swedan SF ![]() , Khabour OF
, Khabour OF ![]() , Alzoubi KH
, Alzoubi KH ![]()
Received 15 January 2026
Accepted for publication 8 April 2026
Published 15 May 2026 Volume 2026:19 590493
DOI https://doi.org/10.2147/IDR.S590493
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemant Joshi
Muhamad Ali K Shakhatreh,1 Farah H Atawneh,1 Samer F Swedan,1 Omar F Khabour,1 Karem H Alzoubi2
1Department of Medical Laboratory Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid, Jordan; 2Department of Pharmaceutical Sciences, College of Pharmacy, QU Health, Qatar University, Doha, Qatar
Correspondence: Muhamad Ali K Shakhatreh, Department of Medical Laboratory Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, P.O. Box 3030, Irbid, 22110, Jordan, Tel + 962-2 − 7201000, Fax + 962-2-7201071, Email [email protected]
Background: Streptococcus agalactiae is a major cause of neonatal sepsis. This research aims to determine the prevalence of vaginal colonization by Streptococcus agalactiae among pregnant women attending antenatal care at a tertiary hospital in Irbid, Jordan, and to characterize the antimicrobial resistance patterns, biofilm-forming capacity, and virulence and resistance gene profiles of the isolates.
Methods: A total of 346 pregnant women were included in the study. The antibiotic susceptibility of the isolates was determined using the Kirby–Bauer method. The ability to produce biofilms was evaluated qualitatively using the Congo red agar method and quantitatively using the tissue culture plate biofilm formation assay. PCR was used to screen the isolates for specific virulence (scpB, lmb) and antimicrobial resistance genes (ermB, ermTR, mefA, mefE, and linB).
Results: Thirty-nine pregnant women (11.3%) tested positive for S. agalactiae. The highest rate of antibiotic resistance was against tetracycline (87.2%), followed by erythromycin (33.3%), and then ofloxacin and levofloxacin (12.8% each). All isolates were susceptible (100%) to ampicillin, meropenem, vancomycin, cefotaxime, rifampin, and cefepime. All isolates demonstrated biofilm production. ScpB and lmb were present in 92.3% and 97.4% of the isolates, respectively. ScpB was significantly associated with lmb. Resistance genes were identified at the following rates: ermB, ermTR, and mefE at 15.4% each, mefA at 10.3%, and linB at 5.1%. The linB and the mefE genes were significantly associated with nonsusceptibility to erythromycin, whereas the mefA gene was significantly associated with susceptibility to tetracycline (P< 0.01).
Conclusion: The prevalence of S. agalactiae among pregnant women was relatively low. However, the ScpB and lmb virulence genes were frequently present among the isolates. In addition, all S. agalactiae were biofilm formers. Therefore, the implementation of rigorous, standardized, and timely intervention to manage S. agalactiae in women who test positive is vital to reduce vertical transmission of this pathogen to newborns.
Keywords: Streptococcus agalactiae, asymptomatic vaginal colonization, biofilms, virulence genes
Introduction
Streptococcus agalactiae is a significant cause of neonatal sepsis.1,2 It is part of the female gastrointestinal and reproductive microbiota3 and is common (10–40%) among pregnant women.4 S. agalactiae can cause a wide range of infections, such as pneumonia, endometritis, bacteremia, bone infections, urosepsis, and neonatal sepsis.5,6 The infection with S. agalactiae can be transmitted from mother to child during delivery, or during gestation from the mother’s reproductive tract to the amniotic fluid.4,7 S. agalactiae has a variety of virulence genes such as scpB and lmb.8–10 ScpB is a serine protease that supports evading host immunity by cleaving and inactivating the human complement C5a protein.11,12 Lmb allows S. agalactiae to bind to human cell laminin, an essential step in the development of infection.11,13
In most cases, S. agalactiae is susceptible to penicillin, ampicillin, first generation cephalosporins, and vancomycin. In cases of allergy to penicillin and its derivatives, alternative antibiotics such as macrolides and lincosamides may be prescribed.14 However, S. agalactiae may harbor resistance genes that render antibiotics ineffective. These genes include ermB, ermTR, mefA, and mefE for macrolide resistance and linB for lincosamide resistance.4 ErmB and ermTR encode 23S rRNA methylases that modify 23S rRNA, thereby preventing macrolides from binding to their target molecules.15,16 MefA and mefE encode macrolide efflux pumps.15 LinB encodes a lincosamide nucleotidyl transferase, leading to the L phenotype associated with lincosamide resistance.15
S. agalactiae can produce biofilms, which are aggregates of cells attached to the surface and that are protected by extracellular polymeric substances. Biofilm formation by S. agalactiae contributes to its survival.17,18 S. agalactiae can adhere to various human cells and surfaces, such as the vaginal epithelium, placental membrane, respiratory tract, and blood–brain epithelium.19 These biofilms also increase resistance to host immunity and antimicrobial drugs.20
The S. agalactiae prevalence among pregnant women in the Middle East ranges from 14% to 32%.21,22 Key factors driving this include higher colonization in rectal over vaginal samples and increased risk associated with advanced maternal age. However, studies regarding S. agalactiae prevalence and its molecular and virulence profile are limited.23 Therefore, the aim of this study is to characterize the molecular and phenotypic profile of colonizing S. agalactiae in Jordanian women to inform local prevention strategies.
Methods
Sample Collection and Culture
The study was approved by the institutional review board of Jordan University of Science and Technology (approval # 1/102/2017, date: 23/01/2017). All the study procedures were in adherence with the Helsinki Declaration and all its amendments. A convenient sampling procedure was adopted in the study. Informed written consent was obtained from all study subjects. One low vaginal swab sample was obtained aseptically from each subject (n=346, age range 17–45 years). The gestation period ranged from 13 to 40 weeks, with the majority (99%) of them were in their ninth month of pregnancy. Exclusion criteria include disinfectant vaginal baths within the last 2 weeks prior to sample collection, and women with acute systemic diseases such as diabetes mellitus and cardiovascular diseases. Subjects were recruited from Princess Badea’ Hospital and King Abdullah University Hospital, in Irbid, Jordan, during the period from March to November 2017. Vaginal swabs were directly inoculated into HiCrome™ Strep B Selective Agar Base (Cat# M1966, HiMedia Laboratories, Mumbai, India), which were then incubated aerobically for 18–24 h at 37 °C. Isolates were confirmed as S. agalactiae using a Streptex rapid latex test for streptococcal grouping (Cat# R30950501 ZL50, Thermo Fisher Scientific, Waltham, MA, USA).
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing was performed using the Kirby-Bauer disk diffusion method on Muller-Hinton agar using erythromycin (15 µg), ampicillin (10 µg), cefepime (30 µg), meropenem (10 µg), vancomycin (30 µg), azithromycin (15 µg), tetracycline (30 µg), levofloxacin (5 µg), chloramphenicol (30 µg), and clindamycin (2 µg) disks.4,15,24,25 All antimicrobial disks were obtained from Oxoid (Basingstoke, United Kingdom). CLSI 2016 recommendations were used to interpret the diameter of antimicrobial disk inhibition zones.
Molecular Techniques
Genomic DNA was extracted from pure broth cultures using the i-genomic BYF DNA Extraction Mini Kit (iNtRON Biotechnology, Korea) according to the manufacturer’s instructions. The detection of S. agalactiae virulence genes (scpB and lmb) was performed using PCR and the primers indicated in Table 1.26 Each PCR consisted of 95°C/10min, followed by 35 cycles of 95°C/30s, 50°C/1min, and 72°C/30s, and a final step at 72°C/7min. The mefE gene was identified using primers shown in Table 1.27 PCR conditions were 95°C/10min, followed by 35 cycles at 95°C/30s, 48°C/1min, and 72°C/1.5 min, and a final step at 72°C/7min. The ermB, ermTR, mefA, and linB genes were identified using multiplex PCR using the primers indicated in Table 1.4 Multiplex PCR conditions consisted of 95°C/10min, followed by 35 cycles at 95°C/30s, 57°C/1min, and 72°C/1.5 min, and a final step at 72°C/7min. In all PCR reactions, i-MAX II 2X master mix (iNtRON Biotechnology, Seongnam-Si, Gyeonggi-do, Korea), 10 μM of each primer, and 1μg of DNA template were used. Amplification products were separated by electrophoresis (150v/45min) on 2% agarose and visualized using EtBr/UV light. In all PCR runs, negative controls (reaction mix without template) were used. A representative image for the detection of scpB and lmb genes is shown in Figure 1.
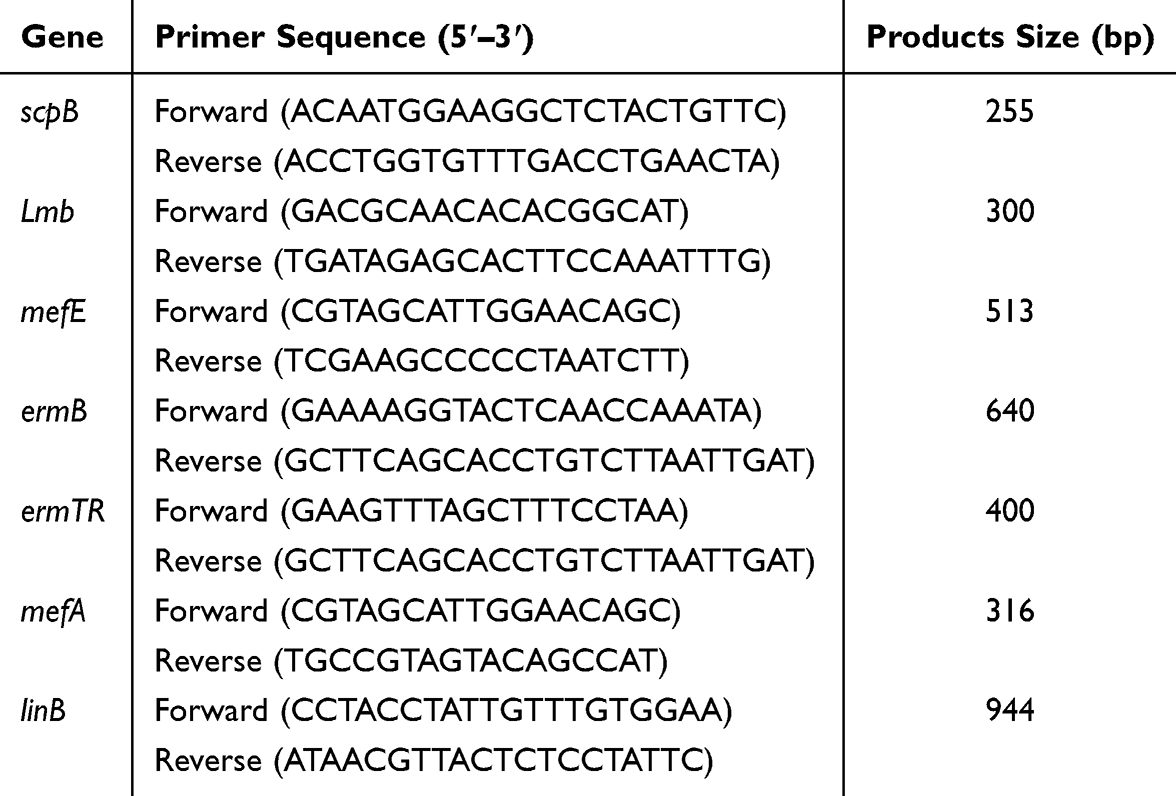 |
Table 1 PCR Primers |
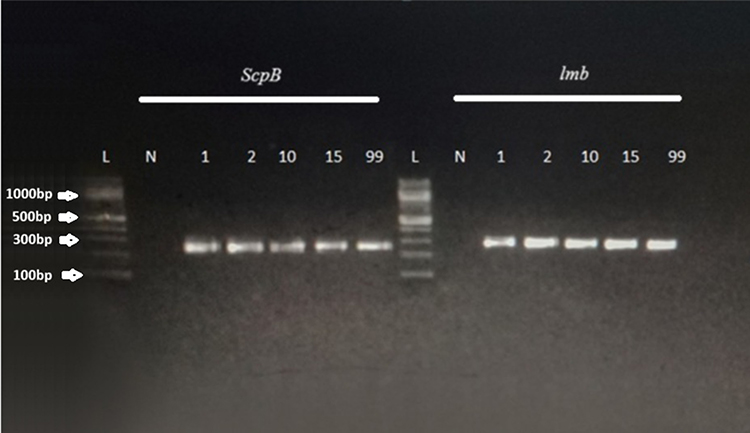 |
Figure 1 Representative gel for the detection of ScpB and lmb. Products of classical PCR were separated on 2% agarose containing ethedium bromide. A total of 5 μL of PCR product was loaded per well of the gel. Electrophoresis was done at 150 V for 28 min. DNA was visualized using a UV transilluminator provided with a gel documentation system using the Quantity One software (Biorad, USA). Fragment sizes of each PCR were determined by comparison with a 100 bp DNA ladder. Lane (L) 100 bp ladder. Lane (N) negative control. Lanes 1–99: samples demonstrating ScpB(255) and lmb (300). |
Biofilm Formation Assays
Isolates’ ability to produce biofilms was assayed qualitatively using the Congo red agar (CRA) method and quantitatively using the tissue culture plate biofilm formation assay (TCP).28,29
Congo Red Agar (CRA) Method
CRA medium was prepared as previously described.28 Plates were inoculated with the isolates and incubated aerobically at 37°C for 24 h. The plates were visualized for the development of colored colonies at 24 and 48 h. A positive biofilm-formation result was indicated by the development of black colonies with a dry crystalline consistency. Non-biofilm producers appeared as red colonies.28 All isolates were tested in triplicate.
Tissue Culture Plate Biofilm Formation Assay
Quantitative biofilm production was evaluated using the tissue culture plate biofilm formation assay.29 Briefly, 10 mL of TSB with 1% glucose was inoculated with a loopful of the test organism from an overnight culture on nutrient agar. TSB broth was incubated at 37 °C for 24 h. The culture was further diluted 1:100 with fresh medium, and flat-bottom tissue culture plates (96 wells) were filled with 200 μL of the diluted culture per well. Uninoculated sterile broth served as a blank. The culture plates were incubated at 37 °C for 48 h. The plates were inverted and gently tapped to discard the culture broth. The wells were washed with 200 μL of PBS (pH 7.2) four times to remove non-adherent bacteria. Biofilms adhering to the walls and bottom of the wells were fixed with 200 μL of 2% sodium acetate for 15 minutes and stained with 200 μL of 0.1% crystal violet for 30 minutes. Excess stain was washed with deionized water three times, and the plates were dried. Next, 200 μL of 95% ethanol was added to each well to release the dye. The optical density (OD) of each well was measured using a micro-ELISA reader at 570 nm. All isolates were tested in triplicate. The average OD values of the sterile medium were calculated and subtracted from all test values. Interpretation of biofilm production data was as previously described.29 In brief, if OD ≤ the optical density cutoff (ODc), the isolate was considered a non-biofilm producer. Weak, moderate, and strong biofilm producers were considered if OD was (1-<2X), (2X-4X), ≥4X of ODC, respectively.
Statistical Analysis
The Statistical Package for Social Sciences (SPSS) software version 23 (IBM, Armonk, New York, USA) was used for data analysis. Frequency results (antibiotic susceptibility, frequency of antibiotic resistance genes, and virulence genes) were compared using the Chi-square test. Means (biofilm optical density) were compared using the Student’s t-test. A P value equal to or less than 0.05 was considered statistically significant.
Results
Study Isolates
Three hundred and forty-six vaginal swabs were collected from pregnant women. Their ages ranged from 17 to 45 years. Thirty-nine swabs tested positive for S. agalactiae. Therefore, the prevalence of S. agalactiae was 11.3% among pregnant women. No significant associations were observed regarding the risk of carrying S. agalactiae bacteria with the age of participants (Chi square = 2.41, P = 0.121), the number of times they had been pregnant (pregnancy count, Chi square = 0.098, P = 0.753), previous abortions (Chi square = 1.367, P = 0.242) and antibiotic use (Chi square = 1.145, P = 0.285) (Table 2).
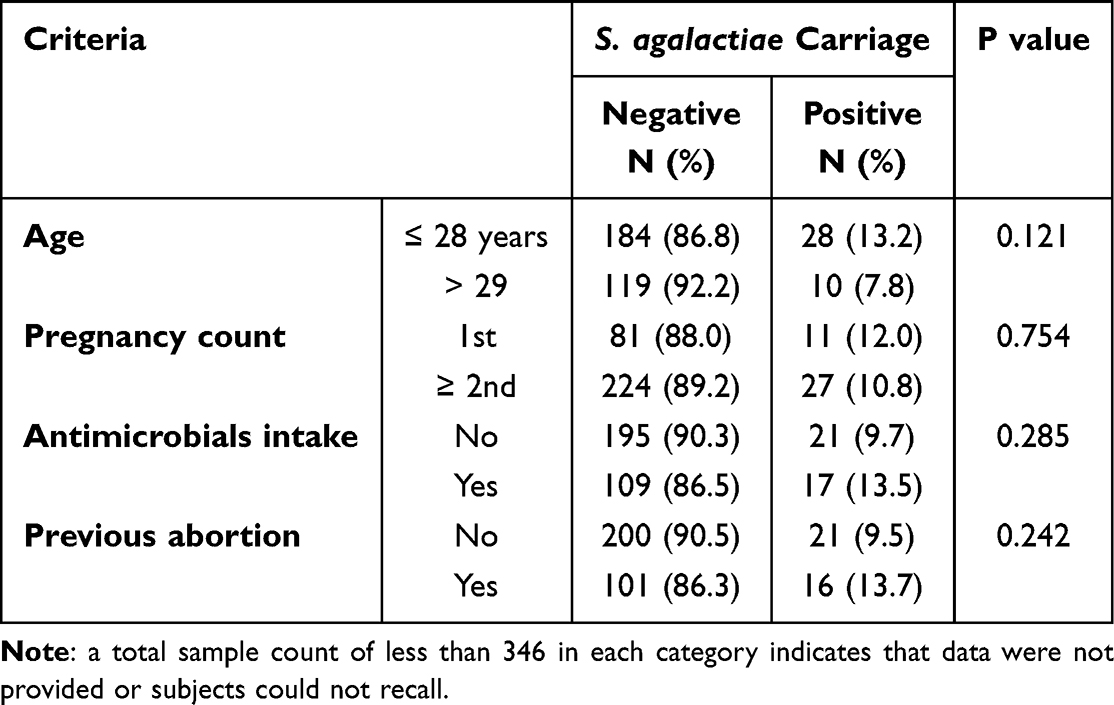 |
Table 2 Characteristics of Participating Women in Association with S. agalactiae Carriage |
Antimicrobial Susceptibility
The antimicrobial susceptibility profile of S. agalactiae isolates is illustrated in Table 3. The highest resistance rates were observed against tetracycline (87.3%), followed by erythromycin (33.3%), ofloxacin and levofloxacin (12.8%), azithromycin (7.7%), and clindamycin and chloramphenicol (5.1%). All isolates were susceptible (100%) to ampicillin, meropenem, vancomycin, cefotaxime, rifampin, and cefepime.
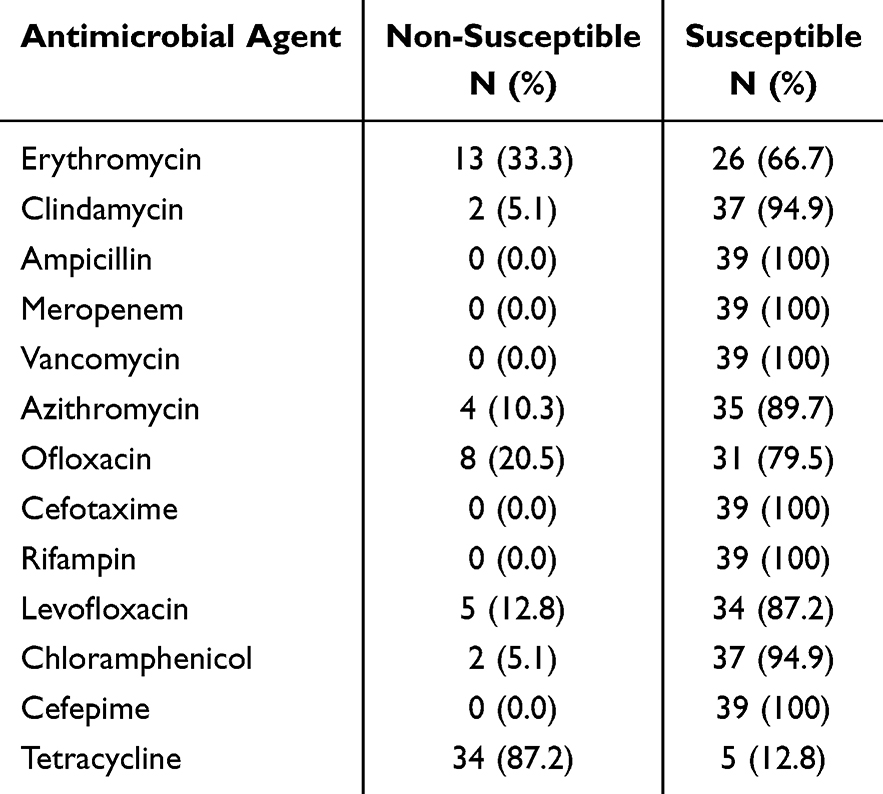 |
Table 3 Antimicrobial Susceptibility Profile of the Isolates Reported as Susceptible and Non-Susceptible |
Antimicrobial Resistance Genes
Resistance genes were identified at the following rates: ermB, ermTR, and mefE at 15.4% each, mefA at 10.3%, and linB at 5.1%. The association between resistance genes and antibiotic efficacy was examined only among those who showed resistance higher than 10% (Table 4). The linB gene was significantly associated with nonsusceptibility to erythromycin (Chi square = 4.216, P = 0.040), the mefE gene was significantly associated with nonsusceptibility to erythromycin (Chi square = 7.977, P = 0.005), and the mefA gene was significantly associated with susceptibility to tetracycline (Chi square = 5.512, P = 0.019) (Table 4).
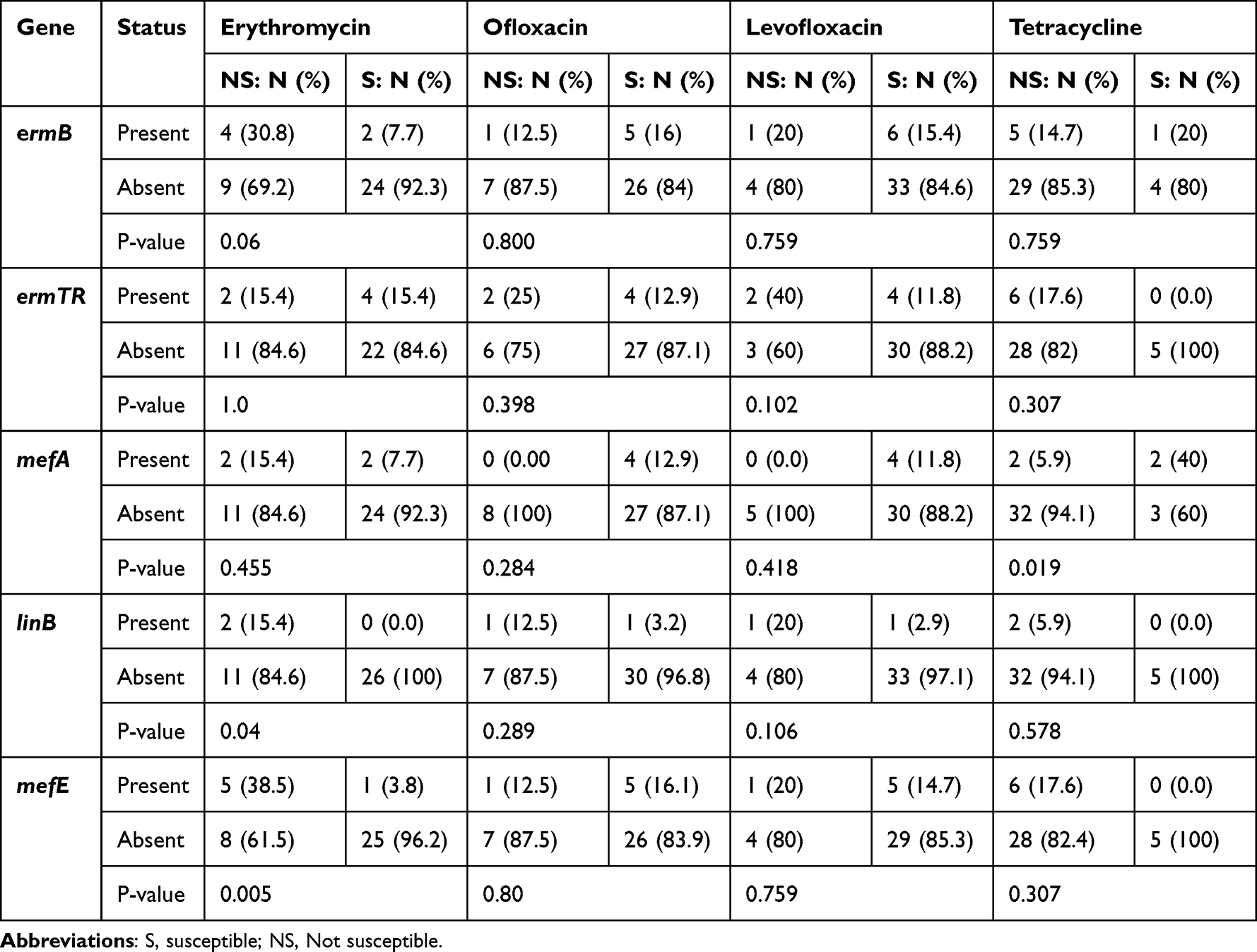 |
Table 4 Association Between Erythromycin and Clindamycin Resistance Genes and Susceptibility to Antimicrobial Agents (Only Ones That Showed Less Than 90% Sensitivity) |
Virulence Genes
ScpB and lmb were present in 92.3% and 97.4% of the isolates, respectively. ScpB was significantly associated with lmb (Chi square = 12.316, P < 0.001) (Table 5). There were no significant associations between virulence and resistance genes.
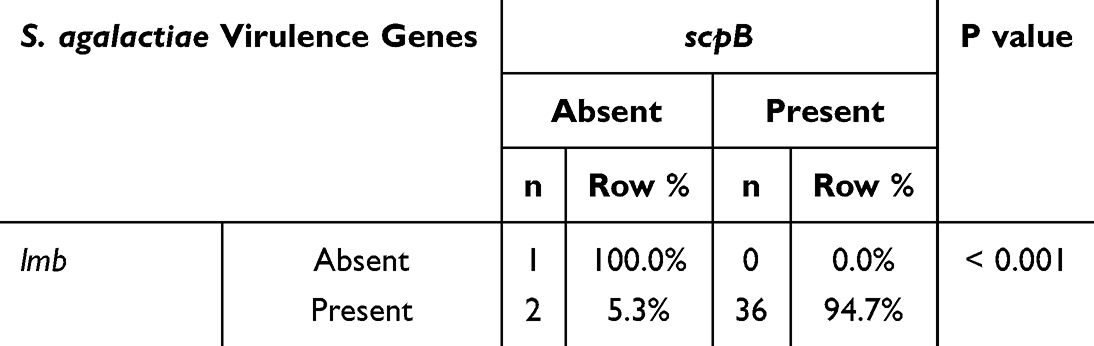 |
Table 5 Association Between S. agalactiae Virulence Genes |
Biofilm Production
Two methods measured the isolates’ ability to produce biofilms. Using the Congo red agar method, all isolates displayed positive results, i.e., black colonies. The tissue culture plate biofilm formation assay classified the isolates into three biofilm production categories based on quantitative data: moderate at 51.3% (20/39), weak at 33.3% (13/39), and strong at 15.4% (6/39). No significant associations were observed between the virulence genes scpB and lmb, and biofilm formation according to the tissue culture plate biofilm formation assay (data not shown).
Discussion
In the present study, S. agalactiae carriage was investigated among pregnant women in Jordan. The prevalence of S. agalactiae among the subjects was 11.3%. Carriage was not associated with women’s age, history of abortion, history of antimicrobial intake, or number of previous pregnancies.
The carriage rate reported herein is considered low. A study conducted in Korea in 2011 reported a comparably low rate of vaginal colonization of 8.3% among women at 35–37 weeks of gestation.30 A study from Iran in 2017 demonstrated a similar result of 11.8%.31 In South Africa and Ethiopia, the prevalence rates were 30.9% and 19%, respectively.4,32 In Egypt and Nigeria, the carriage rates were 25.3% and 19.7%, respectively.33,34 Several factors have been reported to influence S. agalactiae vaginal colonization, such as age, education, household monthly income, smoking, alcohol intake during pregnancy, body mass index (BMI) before pregnancy, subjective health status during pregnancy, history of previous infection with human papillomavirus, vulvitis, vaginal pH, sexual intercourse frequency during or pre-pregnancy, history of neonate sepsis, history of preterm labor, premature rupture of membranes, pelvic inflammatory diseases, previous infection with herpes simplex virus, vaginal discharge, vaginal candidiasis, rectal coitus, vaginal burning, and miscarriages in previous pregnancies.30,31 The high overall pregnancy count and generally elevated BMI of Jordanian women would be expected to result in a higher carriage rate than what was found. However, given the numerous potential confounders affecting S. agalactiae carriage, it is difficult to explain the low carriage rate reported in the current study. In addition, the data of the current study relied on a single low vaginal swab. While the standard for group B Streptococcus screening is a combined rectovaginal swab, which significantly increases detection sensitivity, the low carriage rate reported in the current study might be an underestimate due to the sampling method, which is a critical point for comparison with other studies.
The highest antimicrobial resistance among isolates was tetracycline (87.3%), followed by erythromycin (33.3%). On the other hand, the highest susceptibility was observed to ampicillin, vancomycin, rifampin, cefepime, and cefotaxime (100% each), and to clindamycin and chloramphenicol (94.9% each). Comparable results have been reported for S. agalactiae from South Africa, Czechia, Ethiopia, Kuwait, and Egypt. In South Africa, the isolates had tetracycline resistance rates of 94.5%, erythromycin resistance of 21.1%, and clindamycin resistance of 17.2%.4 In Czechia, the rates of resistance to tetracycline, erythromycin, and clindamycin were 83.9%, 3.8%, and 3.2%, respectively.35 In Ethiopia, the isolates had a clindamycin resistance rate of 3.2%, erythromycin 6.5%, and tetracycline 45.2%. In Egypt, the resistance rates against clindamycin, erythromycin, and cefotaxime were 23.7%, 13.2%, and 7.9%, respectively. In Kuwait, the resistance rates against tetracycline, erythromycin, and clindamycin were 89.5%, 12.6%, and 7%, respectively.16,33 As tetracycline is contraindicated in pregnant women due to significant risks of fetal development issues, the observed high resistance of S. agalactiae to tetracycline is of low practical significance. Differences in susceptibility rates across countries are likely attributable to variations in the prevalence of bacterial strains and resistance genes, as well as in the quality of health-care services and infection-control measures, including prescribed antimicrobials.
S. agalactiae virulence genes lmb and scpB were present in 97.4% and 92.3% of isolates, respectively. Similar results have been reported in Kuwait in 2013; a prevalence rate of 88.3% for each of lmb and scpB, in Malaysia in 2014; lmb at 96.1% and scpB at 94.2%, and in Lebanon in 2009; lmb at 96%, and scpB at 94.7%.8,36,37 The high prevalence of the two genes among vaginal isolates, as reported herein and in other reports, suggests an important role in vaginal colonization.
Among the isolates, ermB, ermTR, and mefE were the most prevalent, each at 15.4%, followed by mefA at 10.3% and linB at 5.1%. A study done in South Africa in 2015 reported that resistance to erythromycin and clindamycin was mainly associated with ermB, with 55% of isolates harboring ermB, 3.4% ermTR, 3.4% mefA, and 38% harboring ermB and linB genes together.4 In a 2016 study from Nigeria, the erythromycin resistance gene ermB was not detected in any of the isolates, whereas the mefA/E gene was carried by two of three macrolide-clindamycin-resistant isolates.34 Differences in the prevalence of resistance genes are likely attributable to differences in prevalent strains and antimicrobial agents’ usage patterns across countries.
Infections caused by biofilm producers are difficult to eliminate even with antimicrobial therapy, thus leading to increased morbidity and mortality. In the present study, isolates’ ability to generate biofilms was evaluated qualitatively using the Congo red agar method and quantitatively using the tissue culture plate biofilm formation assay. All S. agalactiae isolates were biofilm producers according to both methods. A 2012 study from Taiwan found that 95% of isolates were biofilm producers: 51% strong, 28% moderate, and 21% weak at an acidic pH of 4.5.38 A study from India demonstrated that strains isolated from asymptomatic carrier pregnant women had a higher capacity to produce biofilms than those from symptomatic women, which might explain why all isolates in the current study could produce biofilms, as all study subjects were asymptomatic carriers. The ability of the detected S. agalactiae isolates to produce biofilms indicates a likelihood of treatment failure or infection recurrence, despite the bacteria appearing susceptible to many antibiotics, as discussed above. This could also explain the observed comparable prevalence of S. agalactiae among antibiotic users and non-users reported in the current study.
The current study had the following strengths: it investigated the prevalence of S. agalactiae in a modestly large sample. Two important virulence genes were investigated to assess the potential virulence of the recovered isolates. The ability of isolates to produce biofilms was evaluated using two methods. The antimicrobial susceptibility profile and presence of several resistance genes were determined for all isolates.
Among the study limitations is that the study’s reliance on a single low vaginal swab. As the gold standard for group B Streptococcus screening is a combined rectovaginal swab, which significantly increases detection sensitivity. Using only vaginal swabs is a major limitation that may have led to an underestimation of the true S. agalactiae prevalence. Therefore, it is recommended that subsequent studies in the region adopt the combined rectovaginal swab collection method to provide a more accurate and reliable epidemiological baseline for Jordan. Another limitation is that the disk diffusion (Kirby-Bauer) method was used to test antibiotic susceptibility, which has some limitations compared to the recommended broth microdilution method. In addition, we did not use reference strains that harbor the examined genes as positive controls. Thus, future investigations should consider such limitations into account.
Conclusion
The overall carriage rate of S. agalactiae among asymptomatic pregnant women was relatively low (11.3%) compared to previous studies conducted in other countries, which could be attributed to sampling procedure. All isolates had the capacity to produce biofilms, which might complicate management of this bacteria even when using first line antibiotics. S. agalactiae virulence genes scpB and lmb were found among 92.3% and 97.4% of the isolates, respectively. The implementation of rigorous, standardized, and timely intervention to manage S. agalactiae in women who test positive is vital to reduce vertical transmission of this pathogen to newborns.
Data Sharing Statement
Data will be available upon reasonable request via emailing the corresponding author.
Consent for Publication
Written informed consent was obtained from the study participants.
Acknowledgments
Authors would like to thank Jordan University of Science and Technology for its support.
Funding
This study was funded by the Deanship of Research, Jordan University of Science and Technology (grant number 385/2016).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Harrison ML, Dickson BFR, Sharland M, Williams PCM. Beyond early- and late-onset neonatal sepsis definitions: what are the current causes of neonatal sepsis globally? A systematic review and meta-analysis of the evidence. Pediatr Infect Dis J. 2024;43(12):1182–9. doi:10.1097/INF.0000000000004485
2. Shen L, Huang M, Xie N. Experimental study on Streptococcus agalactiae genotype and erythromycin resistance in neonatal sepsis. Cellular Mol Biol. 2022;67(6):100–106. doi:10.14715/cmb/2021.67.6.14
3. Morgan JA, Zafar N, Cooper DB. Group B Streptococcus and pregnancy. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
4. Bolukaoto JY, Monyama CM, Chukwu MO, et al. Antibiotic resistance of Streptococcus agalactiae isolated from pregnant women in Garankuwa, South Africa. BMC Res Notes. 2015;8(1):364. doi:10.1186/s13104-015-1328-0
5. Megli CJ, Carlin SM, Giacobe EJ, Hillebrand GH, Hooven TA. Virulence and pathogenicity of group B Streptococcus: virulence factors and their roles in perinatal infection. Virulence. 2025;16(1):2451173. doi:10.1080/21505594.2025.2451173
6. HajiAhmadi P, Momtaz H, Tajbakhsh E. Molecular characterization of Streptococcus agalactiae strains isolated from pregnant women. Sci Rep. 2025;15(1):5887. doi:10.1038/s41598-025-86565-z
7. Wang Q, Huang Y, Liu X, et al. Characterization of clinical infection and drug resistance of group B streptococcus in Chengdu, China. Indian J Med Microbiol. 2024;52:100742. doi:10.1016/j.ijmmb.2024.100742
8. Udo EE, Boswihi SS, Al-Sweih N. Genotypes and virulence genes in group B streptococcus isolated in the maternity hospital, Kuwait. Med Principles Pract. 2013;22(5):453–457. doi:10.1159/000349932
9. Kamińska D, Ratajczak M, Nowak-Malczewska DM, et al. Macrolide and lincosamide resistance of Streptococcus agalactiae in pregnant women in Poland. Sci Rep. 2024;14(1):3877. doi:10.1038/s41598-024-54521-y
10. Hernandez LB, Cadona JS, Traverso F, Altamiranda SM, Bustamante AV, Sanso AM. Virulence profiles and antimicrobial resistance of Streptococcus agalactiae infective and colonizing strains from Argentina. Curr Microbiol. 2022;79(12):392. doi:10.1007/s00284-022-03050-w
11. Rajagopal L. Understanding the regulation of Group B Streptococcal virulence factors. Future Microbiol. 2009;4(2):201–221. doi:10.2217/17460913.4.2.201
12. Bobadilla FJ, Novosak MG, Cortese IJ, Delgado OD, Laczeski ME. Prevalence, serotypes and virulence genes of Streptococcus agalactiae isolated from pregnant women with 35-37 weeks of gestation. BMC Infect Dis. 2021;21(1):73. doi:10.1186/s12879-020-05603-5
13. Moulin P, Patron K, Cano C, et al. The Adc/Lmb system mediates zinc acquisition in Streptococcus agalactiae and contributes to bacterial growth and survival. J Bacteriol. 2016;198(24):3265–3277. doi:10.1128/JB.00614-16
14. Genovese C, D’Angeli F, Di Salvatore V, Tempera G, Nicolosi D. Streptococcus agalactiae in pregnant women: serotype and antimicrobial susceptibility patterns over five years in Eastern Sicily (Italy). European J Clin Microbiol Infect Dis. 2020;39(12):2387–2396. doi:10.1007/s10096-020-03992-8
15. Gygax SE, Schuyler JA, Kimmel LE, Trama JP, Mordechai E, Adelson ME. Erythromycin and clindamycin resistance in group B streptococcal clinical isolates. Antimicrob Agents Chemother. 2006;50(5):1875–1877. doi:10.1128/AAC.50.5.1875-1877.2006
16. Boswihi SS, Udo EE, Al-Sweih N. Serotypes and antibiotic resistance in Group B streptococcus isolated from patients at the maternity hospital, Kuwait. J Med Microbiol. 2012;61(Pt 1):126–131. doi:10.1099/jmm.0.035477-0
17. Rinaudo CD, Rosini R, Galeotti CL, et al. Specific involvement of pilus type 2a in biofilm formation in group B Streptococcus. PLoS One. 2010;5(2):e9216. doi:10.1371/journal.pone.0009216
18. Jabbour N, Morello E, Camiade E, Lartigue MF. Biofilm formation in Streptococcus agalactiae is inhibited by a small regulatory RNA regulated by the two-component system CiaRH. Microbiol Spectr. 2022;10(5):e0063522. doi:10.1128/spectrum.00635-22
19. Kaur H, Kumar P, Ray P, Kaur J, Chakraborti A. Biofilm formation in clinical isolates of group B streptococci from north India. Microb Pathogenesis. 2009;46(6):321–327. doi:10.1016/j.micpath.2009.04.004
20. Hoiby N, Bjarnsholt T, Givskov M, Molin S, Ciofu O. Antibiotic resistance of bacterial biofilms. Int J Antimicrob Agents. 2010;35(4):322–332. doi:10.1016/j.ijantimicag.2009.12.011
21. Alshengeti A. Group B Streptococcus among pregnant women and neonates in Saudi Arabia: a systemic review. Pathogens. 2022;11(9):1029. doi:10.3390/pathogens11091029
22. Hezam ALJedri ZA, Algabr MN, Qaid Al-Hajj NM, Ahmed Ali AM. Prevalence of Streptococcus agalactiae Infection among pregnant women in Sana’a City/Republic of Yemen and its implications for cervical cancer risk. Onkologia i Radioterapia. 2024;18(1).
23. Clouse K, Shehabi A, Suleimat AM, et al. High prevalence of Group B Streptococcus colonization among pregnant women in Amman, Jordan. BMC Pregnancy Childbirth. 2019;19(1):177. doi:10.1186/s12884-019-2317-4
24. Malek-Jafarian M, Hosseini FS, Ahmadi AR. Pattern of infection and antibiotic activity among Streptococcus agalactiae isolates from adults in Mashhad, Iran. Reports Biochemistry Mol Biol. 2015;3(2):89–93.
25. Sader HS, Fritsche TR, Jones RN. Daptomycin bactericidal activity and correlation between disk and broth microdilution method results in testing of Staphylococcus aureus strains with decreased susceptibility to vancomycin. Antimicrob Agents Chemother. 2006;50(7):2330–2336. doi:10.1128/AAC.01491-05
26. Dmitriev A, Shakleina E, Tkacikova L, Mikula I, Totolian A. Genetic heterogeneity of the pathogenic potentials of human and bovine group B streptococci. Folia microbiologica. 2002;47(3):291–295. doi:10.1007/BF02817655
27. Lopardo HA, Vidal P, Jeric P, et al. Six-month multicenter study on invasive infections due to group B streptococci in Argentina. J Clin Microbiol. 2003;41(10):4688–4694. doi:10.1128/JCM.41.10.4688-4694.2003
28. Freeman DJ, Falkiner FR, Keane CT. New method for detecting slime production by coagulase negative staphylococci. J Clin Pathol. 1989;42(8):872–874. doi:10.1136/jcp.42.8.872
29. Mathur T, Singhal S, Khan S, Upadhyay DJ, Fatma T, Rattan A. Detection of biofilm formation among the clinical isolates of Staphylococci: an evaluation of three different screening methods. Indian J Med Microbiol. 2006;24(1):25–29. doi:10.1016/S0255-0857(21)02466-X
30. Kim EJ, Oh KY, Kim MY, et al. Risk factors for group B Streptococcus colonization among pregnant women in Korea. Epidemiol Health. 2011;33:e2011010. doi:10.4178/epih/e2011010
31. Darabi R, Tadi S, Mohit M, et al. The prevalence and risk factors of group B streptococcus colonization in Iranian pregnant women. Electron Physician. 2017;9(5):4399–4404. doi:10.19082/4399
32. Mengist A, Kannan H, Abdissa A. Prevalence and antimicrobial susceptibility pattern of anorectal and vaginal group B Streptococci isolates among pregnant women in Jimma, Ethiopia. BMC Res Notes. 2016;9(1):351. doi:10.1186/s13104-016-2158-4
33. Shabayek SA, Abdalla SM, Abouzeid AM. Vaginal carriage and antibiotic susceptibility profile of group B Streptococcus during late pregnancy in Ismailia, Egypt. J Infect Public Health. 2009;2(2):86–90. doi:10.1016/j.jiph.2009.03.004
34. Elikwu CJ, Oduyebo O, König B. Antibiotic susceptibility profiles of group B streptococci (GBS) isolates from pregnant mothers in a tertiary institution in Nigeria. Inter J Infect Dis. 2014;21:348. doi:10.1016/j.ijid.2014.03.1138
35. Motlova J, Strakova L, Urbaskova P, Sak P, Sever T. Vaginal & rectal carriage of Streptococcus agalactiae in the Czech Republic: incidence, serotypes distribution & susceptibility to antibiotics. Indian J Med Res. 2004;119 Suppl:84–87.
36. Hannoun A, Shehab M, Khairallah MT, et al. Correlation between Group B Streptococcal genotypes, their antimicrobial resistance profiles, and virulence genes among pregnant women in Lebanon. Int J Microbiol. 2009;2009:796512. doi:10.1155/2009/796512
37. Eskandarian N, Ismail Z, Neela V, van Belkum A, Desa MN, Amin Nordin S. Antimicrobial susceptibility profiles, serotype distribution and virulence determinants among invasive, non-invasive and colonizing Streptococcus agalactiae (group B streptococcus) from Malaysian patients. Eur J Clin Microbiol Infect Dis. 2015;34(3):579–584. doi:10.1007/s10096-014-2265-x
38. Ho YR, Li CM, Yu CH, et al. The enhancement of biofilm formation in Group B streptococcal isolates at vaginal pH. Med Microbiol Immunol. 2013;202(2):105–115. doi:10.1007/s00430-012-0255-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.